NSG2101 Case Study: Patient with Congestive Heart and Renal Failure
VerifiedAdded on 2023/04/20
|12
|3791
|341
Case Study
AI Summary
This case study analyzes the case of a 68-year-old female patient admitted to the emergency department with congestive heart failure (CHF) and a history of chronic renal failure (CRF). The assessment includes the patient's medical history, current vital signs, physical examination findings, and laboratory results. The analysis delves into the pathophysiology of CHF and CRF, exploring their interrelation and the impact on the patient's signs and symptoms. The case study identifies two priority nursing problems: decreased cardiac output and a deficiency of cognitive information. For each problem, the study establishes short-term and long-term goals, evidence-based nursing interventions, and expected outcomes. The nursing care plan includes monitoring vital signs, managing fluid intake, administering diuretics, and providing patient education. The assignment follows the Clinical Reasoning Cycle, including patient situation, cue collection, information processing, identifying nursing problems, establishing goals, and developing interventions. The case study highlights the importance of understanding the complex interplay between cardiac and renal function in providing effective patient care. This assignment, contributed by a student, is available on Desklib, a platform offering AI-powered study tools for students.
1
Case study assessment
Name
University
Tutor
Date
Case study assessment
Name
University
Tutor
Date
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
Patient situation
This assessment is based on patient M.G aged 68 years old female having admission to
the emergency department with a diagnosis of congestive heart failure. She was discharged in
the hospital one and a half weeks ago and has just visited back due to complications arising
from her breathing ability and difficulty in walking. The patient assessment indicates inability
in following her fluid management and salt intake, further she has not been following her
medication correctly. Her past medical history indicates the presence of hypertension, chronic
renal failure, and anterior myocardial infection 4 years ago. Family history assessment shows
that she has lost both her parents, while she has a sister who is alive and well as well as a
brother age 62 years and 70 years respectively. The brother has been diagnosed with coronary
heart disease and hypertension. She has two children and six grandchildren.
Collecting information
Her medical assessments reveal that the blood pressure during discharge was bp140/90
while two weeks before discharge was BP156/94, which led to the commencement of
hydrochlorothiazide 25 mg PO. During patient admission, her pulse rate was irregular at 122,
BP 160/100, respiratory rate 26, temperature 37.3 Celsius degrees, and oxygen saturation
93% on room air. The patient presented with widespread palpitation on chest auscultation
examination in both lungs. Chest x-ray reveals widespread consolidation and cardiomegaly.
The apical pulse is elevated, skin assessment shows pink color while peripheral edema
present at a score of 2.
Electrolyte assessment indicates elevated potassium levels of 5.5mEq/l against normal
levels of 3.5-5.0 mEq/l which indicates mild hyperkalemia. Creatine assessment on the
functionality of the kidney shows impaired function. The patient creatine levels are 4.5mg/dl
against normal ranges of 0.6 to 1.2 ml/dL. The blood urea nitrogen indicates elevated levels
of signifying stress levels with a high of 43 mg/dl against normal ranges of around 7 to 20
mg/dL. Further CXR Assesment shows cardiomegaly presence signifying enlarged heart,
while a pulmonary score of a grade of 2 indicating fluid accumulation.
Patient situation
This assessment is based on patient M.G aged 68 years old female having admission to
the emergency department with a diagnosis of congestive heart failure. She was discharged in
the hospital one and a half weeks ago and has just visited back due to complications arising
from her breathing ability and difficulty in walking. The patient assessment indicates inability
in following her fluid management and salt intake, further she has not been following her
medication correctly. Her past medical history indicates the presence of hypertension, chronic
renal failure, and anterior myocardial infection 4 years ago. Family history assessment shows
that she has lost both her parents, while she has a sister who is alive and well as well as a
brother age 62 years and 70 years respectively. The brother has been diagnosed with coronary
heart disease and hypertension. She has two children and six grandchildren.
Collecting information
Her medical assessments reveal that the blood pressure during discharge was bp140/90
while two weeks before discharge was BP156/94, which led to the commencement of
hydrochlorothiazide 25 mg PO. During patient admission, her pulse rate was irregular at 122,
BP 160/100, respiratory rate 26, temperature 37.3 Celsius degrees, and oxygen saturation
93% on room air. The patient presented with widespread palpitation on chest auscultation
examination in both lungs. Chest x-ray reveals widespread consolidation and cardiomegaly.
The apical pulse is elevated, skin assessment shows pink color while peripheral edema
present at a score of 2.
Electrolyte assessment indicates elevated potassium levels of 5.5mEq/l against normal
levels of 3.5-5.0 mEq/l which indicates mild hyperkalemia. Creatine assessment on the
functionality of the kidney shows impaired function. The patient creatine levels are 4.5mg/dl
against normal ranges of 0.6 to 1.2 ml/dL. The blood urea nitrogen indicates elevated levels
of signifying stress levels with a high of 43 mg/dl against normal ranges of around 7 to 20
mg/dL. Further CXR Assesment shows cardiomegaly presence signifying enlarged heart,
while a pulmonary score of a grade of 2 indicating fluid accumulation.
3
Process information
Pathophysiology Congestive Cardiac Failure
Congestive heart failure occurs due to the inability of the heart to pump the blood
normally. Heart failure state reflects a pathophysiologic state where abnormal cardiac
function occurs. Heart failure can be linked to myocardial failure which leads to circulatory
failure. The pathophysiological occurrence of CHF occurs due to the state of the inability of
the heart to be able to acquire the normal maintenance of oxygen delivered. It indicates the
systematic response in an attempt to compensate for the inadequacy occurring. The stroke
volume is further assessed based on the preload and afterload in the left ventricular valves
(Harjola, et al., 2017).
The occurring significance of the heart in the reaction of the heart muscle through the
overload or damage reducing the efficiency of the heart leading to lower output levels while
myocardial dysfunction defined by the systolic and diastolic, acute or chronic depicts changes
of the heart. In assessing heart failure, various mechanisms take place which is activated
depending on the heart failure duration. Neurohormonal reflexes like the adrenergic system,
renal, peripheral alterations, and renin-angiotensin systems aim at restoring the cardiac output
and terminating the perfusion of tissue perfusions. The occurrence of stroke volume cannot
be removed from the left ventricle thus shifting the pressure-volume on to the systolic failure.
Filing of adequate cannot be achieved due to the occurrence of stiffness in the diastolic
region, thus shifting the diastolic pressure-volume curving upward without effects on the
diastolic pressure increasing without effects on the systolic volume-pressure curve, leading to
diastolic failure. The left ventricle heart failure often reflects the dominance of heart failure
syndrome while the right heart develops as an isolated failure, the occurrence of bi-
ventricular syndrome indicates an end-stage clinical assessment of the heart failure state
(Münzel, 2015).
In fluid mechanism congestion, the presence of cardiac dysfunction often leads to a
serious state of the neruo humoral pathway which entails changes on the nervous system,
vasopressin system; arginine activation and aldosterone system is activated by the negative
consequences of the heart failure on the delivery of oxygen to the peripheral tissues. The
activation of neurohumoral leads to impairment of sodium excretion regulation through eh
kidney organs which leads to increased levels of sodium and fluid accumulation, thus
Process information
Pathophysiology Congestive Cardiac Failure
Congestive heart failure occurs due to the inability of the heart to pump the blood
normally. Heart failure state reflects a pathophysiologic state where abnormal cardiac
function occurs. Heart failure can be linked to myocardial failure which leads to circulatory
failure. The pathophysiological occurrence of CHF occurs due to the state of the inability of
the heart to be able to acquire the normal maintenance of oxygen delivered. It indicates the
systematic response in an attempt to compensate for the inadequacy occurring. The stroke
volume is further assessed based on the preload and afterload in the left ventricular valves
(Harjola, et al., 2017).
The occurring significance of the heart in the reaction of the heart muscle through the
overload or damage reducing the efficiency of the heart leading to lower output levels while
myocardial dysfunction defined by the systolic and diastolic, acute or chronic depicts changes
of the heart. In assessing heart failure, various mechanisms take place which is activated
depending on the heart failure duration. Neurohormonal reflexes like the adrenergic system,
renal, peripheral alterations, and renin-angiotensin systems aim at restoring the cardiac output
and terminating the perfusion of tissue perfusions. The occurrence of stroke volume cannot
be removed from the left ventricle thus shifting the pressure-volume on to the systolic failure.
Filing of adequate cannot be achieved due to the occurrence of stiffness in the diastolic
region, thus shifting the diastolic pressure-volume curving upward without effects on the
diastolic pressure increasing without effects on the systolic volume-pressure curve, leading to
diastolic failure. The left ventricle heart failure often reflects the dominance of heart failure
syndrome while the right heart develops as an isolated failure, the occurrence of bi-
ventricular syndrome indicates an end-stage clinical assessment of the heart failure state
(Münzel, 2015).
In fluid mechanism congestion, the presence of cardiac dysfunction often leads to a
serious state of the neruo humoral pathway which entails changes on the nervous system,
vasopressin system; arginine activation and aldosterone system is activated by the negative
consequences of the heart failure on the delivery of oxygen to the peripheral tissues. The
activation of neurohumoral leads to impairment of sodium excretion regulation through eh
kidney organs which leads to increased levels of sodium and fluid accumulation, thus
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
increasing cardiac filling pressures and congestion of the venous is observed recurrent
(McKie et al., 2011). The occurrence of venous congestion has often been indicated in
cardiac failure, it plays a crucial role in the overall pathophysiological process of cardiac
failure.
The association of cardiac function and renal dysfunction referred to as cardio-renal
syndrome occurs in CCF. The congestion of the venous is the key hemodynamic determinant
for the development of renal dysfunction and low index of cardiac functionality. The
increased occurrence of central pressure of the venous and low index of the cardiac is
particularly not favorable for renal function (Nijs et al., 2015).
The resultant effect of congestive heart failure leads to reduce contraction force due to
overloading of the ventricular. This leads to failure of ventricle lading with blood in the heart
muscle contraction reducing leading to reduced ability of the cross-link actin and myosin in
stretching the muscles of the heart (Arrigo, Parissis, Akiyama & Mebazaa, 2016).
Chronic renal failure
Chronic renal failure indicates the gradual loss of the kidney function. The kidney
performs filtration of waste and fluids from blood which is then excreted inform of urine. In
chronic disease advance stages, elevated levels of fluid, electrolytes and waste often build up
in the body. This occurs as a result of a progressive decline in kidney function ability. The
occurrence of modulation and adaptation occur at glomerular functionality which keeps the
kidney function normal, the remaining glomerular experience rise in pressure due to
hyperfiltration (Malek & Nematbakhsh, 2015).
The consequential release of the cytokines and growth factors yield hypertrophy and
hyperplasia, while the function of glomerular is hampered, leading to excess demand on
them. This leads to increase levels of permeability and proteinuria, while there is increased
permeability and proteinuria. The increased concentrations in the proximal tube lead to direct
nephrotoxins which deteriorate the state of the kidney function (DiLullo et al., 2015).
Chronic renal failure leads to the reduced ability of excretory functionality, leading to
accumulation of endogenous and other extraneous substances. This leads to
pharmacodynamic changes due to increased metabolic concentration leading to maximal
concentration capacity of the kidney is reduced.
increasing cardiac filling pressures and congestion of the venous is observed recurrent
(McKie et al., 2011). The occurrence of venous congestion has often been indicated in
cardiac failure, it plays a crucial role in the overall pathophysiological process of cardiac
failure.
The association of cardiac function and renal dysfunction referred to as cardio-renal
syndrome occurs in CCF. The congestion of the venous is the key hemodynamic determinant
for the development of renal dysfunction and low index of cardiac functionality. The
increased occurrence of central pressure of the venous and low index of the cardiac is
particularly not favorable for renal function (Nijs et al., 2015).
The resultant effect of congestive heart failure leads to reduce contraction force due to
overloading of the ventricular. This leads to failure of ventricle lading with blood in the heart
muscle contraction reducing leading to reduced ability of the cross-link actin and myosin in
stretching the muscles of the heart (Arrigo, Parissis, Akiyama & Mebazaa, 2016).
Chronic renal failure
Chronic renal failure indicates the gradual loss of the kidney function. The kidney
performs filtration of waste and fluids from blood which is then excreted inform of urine. In
chronic disease advance stages, elevated levels of fluid, electrolytes and waste often build up
in the body. This occurs as a result of a progressive decline in kidney function ability. The
occurrence of modulation and adaptation occur at glomerular functionality which keeps the
kidney function normal, the remaining glomerular experience rise in pressure due to
hyperfiltration (Malek & Nematbakhsh, 2015).
The consequential release of the cytokines and growth factors yield hypertrophy and
hyperplasia, while the function of glomerular is hampered, leading to excess demand on
them. This leads to increase levels of permeability and proteinuria, while there is increased
permeability and proteinuria. The increased concentrations in the proximal tube lead to direct
nephrotoxins which deteriorate the state of the kidney function (DiLullo et al., 2015).
Chronic renal failure leads to the reduced ability of excretory functionality, leading to
accumulation of endogenous and other extraneous substances. This leads to
pharmacodynamic changes due to increased metabolic concentration leading to maximal
concentration capacity of the kidney is reduced.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
The reduced secretory ability of the renal results from the endocrinal balance while
decreased levels of erythropoietin lead to lowered levels of erythrocytes causing renal anemia
and reduction of functional erythrocytes occurring due to hemolysis. Production of vitamin D
is impaired while the excretion of phosphate is reduced. The occurrence of renal osteopathy
leads to disruption of bone metabolisms and disruption of bone mass leading to a decreased
reduction of bone metabolisms. Thirst feelings occur a leading a to increase in sodium
excretion levels. The function of the glomeruli dictates the levels of water and electrolytes in
the body. The occurrence of hypertension, pulmonary edema occurs due to overhydration.
The excretion of water and salt occur with critical glomerular damage leading to utilization of
diuretics (Schrezenmeier et al., 2017).
With the consequential adaption of the glomeruli, the tubular transport mechanism
occurs to prevent the onset of hyperkalemia through elevated potassium secretion. The
hypokalemia effect occurs due to hyperstimulation and resorption capacity. The occurrence
of acidosis can occur due to hypokalemia effect. The ability of kidneys to sufficiently
eliminate the protons due to reduced function of the glomerular filtration process. The
metabolic acidosis leads to elevated levels of calcium release and improves renal osteopathy
leading to more gastrointestinal problems and impairing protein metabolism.
Association of CCF& CRF
Congestive heart failure is associated with the chronic renal disease with an association
of about one-quarter of patients of the former developing kidney disease. Congestive heart
failure prevalence increases significantly as the renal function ability deteriorates and enteral
end stage, with evidence showing about 65%-70% of the congestive heart failure cases
progressing to a kidney disease state. There is growing evidence on the chronic renal disease
as a major contributor to severe cardiac impairment and vice versa. Exacerbate congestive
failure often leads to elevated rapid decline of renal function (Kato, Steinberg & Gladwin,
2017).
The patient electrolyte assessment indicted high levels. The eventual occurrence of
chronic renal failure leads to an inability of the maintenance of electrolyte balances leading to
increased levels of potassium in the body. The potassium functions by maintaining the level
of electrolyte in the body and the pH levels. Elevated levels of hypokalemia can lead to
cardiac arrhythmias and even death and often in critical stage leads to mortality. Kidney state
The reduced secretory ability of the renal results from the endocrinal balance while
decreased levels of erythropoietin lead to lowered levels of erythrocytes causing renal anemia
and reduction of functional erythrocytes occurring due to hemolysis. Production of vitamin D
is impaired while the excretion of phosphate is reduced. The occurrence of renal osteopathy
leads to disruption of bone metabolisms and disruption of bone mass leading to a decreased
reduction of bone metabolisms. Thirst feelings occur a leading a to increase in sodium
excretion levels. The function of the glomeruli dictates the levels of water and electrolytes in
the body. The occurrence of hypertension, pulmonary edema occurs due to overhydration.
The excretion of water and salt occur with critical glomerular damage leading to utilization of
diuretics (Schrezenmeier et al., 2017).
With the consequential adaption of the glomeruli, the tubular transport mechanism
occurs to prevent the onset of hyperkalemia through elevated potassium secretion. The
hypokalemia effect occurs due to hyperstimulation and resorption capacity. The occurrence
of acidosis can occur due to hypokalemia effect. The ability of kidneys to sufficiently
eliminate the protons due to reduced function of the glomerular filtration process. The
metabolic acidosis leads to elevated levels of calcium release and improves renal osteopathy
leading to more gastrointestinal problems and impairing protein metabolism.
Association of CCF& CRF
Congestive heart failure is associated with the chronic renal disease with an association
of about one-quarter of patients of the former developing kidney disease. Congestive heart
failure prevalence increases significantly as the renal function ability deteriorates and enteral
end stage, with evidence showing about 65%-70% of the congestive heart failure cases
progressing to a kidney disease state. There is growing evidence on the chronic renal disease
as a major contributor to severe cardiac impairment and vice versa. Exacerbate congestive
failure often leads to elevated rapid decline of renal function (Kato, Steinberg & Gladwin,
2017).
The patient electrolyte assessment indicted high levels. The eventual occurrence of
chronic renal failure leads to an inability of the maintenance of electrolyte balances leading to
increased levels of potassium in the body. The potassium functions by maintaining the level
of electrolyte in the body and the pH levels. Elevated levels of hypokalemia can lead to
cardiac arrhythmias and even death and often in critical stage leads to mortality. Kidney state
6
of the patient reflects elevated levels of potassium with a dynamic association of cardiorenal
syndrome affecting the heart (Ter Maaten et al., 2016).
Creatine levels assessment indicates the function of the kidneys. Elevated levels of
creatine signals imparted damage on the kidney. The kidneys roles are to filter the blood
through the use of nephrons which most of the fluid is reabsorbed back into the blood.
Impaired ability of the kidney leads to low creatine clearance levels. The creatine level
assesses the kidney function. Further, elevated levels of serum in the blood lead to toxic
effects and heavy load on the blood, leading to low cardiac offload thus initiative congestive
heart symptoms.
Blood urea nitrogen assesses the levels of waste in the blood. High levels of BUN
indicate a lowered level of kidney function and heart failure. The elevated levels of BUN for
the patient reflect malfunction of the kidney and secondary failure of congestive failure. The
protein metabolic products are not efficiently removed in the blood due to the slow function
ability of the kidney thus elevating the levels of BUN in the blood (Evrard et al., 2015).
The CXR X rays of the patient indicating the presence of cardiomegaly signify the
elevated occurrence of blood pressure while pulmonary edema depicting the presence of fluid
in the chest worsening breathing problems (Bartunek et al., 2016).The overall patient vital
indicators show elevated levels. There is an increase on pulse rate due to breathing problems,
high blood pressure, reduced respiratory rate, elevated temperature levels, low oxygen
saturation levels, increased apical pulse and atrial fibrillation on heart functionality
assessments status. The associative risks factors for developing CCF and CRF entail high
blood pressures, diabetes, medication drugs, heart attack, obesity, hypertension, and
congenital heart defects all depicting the patient status.
of the patient reflects elevated levels of potassium with a dynamic association of cardiorenal
syndrome affecting the heart (Ter Maaten et al., 2016).
Creatine levels assessment indicates the function of the kidneys. Elevated levels of
creatine signals imparted damage on the kidney. The kidneys roles are to filter the blood
through the use of nephrons which most of the fluid is reabsorbed back into the blood.
Impaired ability of the kidney leads to low creatine clearance levels. The creatine level
assesses the kidney function. Further, elevated levels of serum in the blood lead to toxic
effects and heavy load on the blood, leading to low cardiac offload thus initiative congestive
heart symptoms.
Blood urea nitrogen assesses the levels of waste in the blood. High levels of BUN
indicate a lowered level of kidney function and heart failure. The elevated levels of BUN for
the patient reflect malfunction of the kidney and secondary failure of congestive failure. The
protein metabolic products are not efficiently removed in the blood due to the slow function
ability of the kidney thus elevating the levels of BUN in the blood (Evrard et al., 2015).
The CXR X rays of the patient indicating the presence of cardiomegaly signify the
elevated occurrence of blood pressure while pulmonary edema depicting the presence of fluid
in the chest worsening breathing problems (Bartunek et al., 2016).The overall patient vital
indicators show elevated levels. There is an increase on pulse rate due to breathing problems,
high blood pressure, reduced respiratory rate, elevated temperature levels, low oxygen
saturation levels, increased apical pulse and atrial fibrillation on heart functionality
assessments status. The associative risks factors for developing CCF and CRF entail high
blood pressures, diabetes, medication drugs, heart attack, obesity, hypertension, and
congenital heart defects all depicting the patient status.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
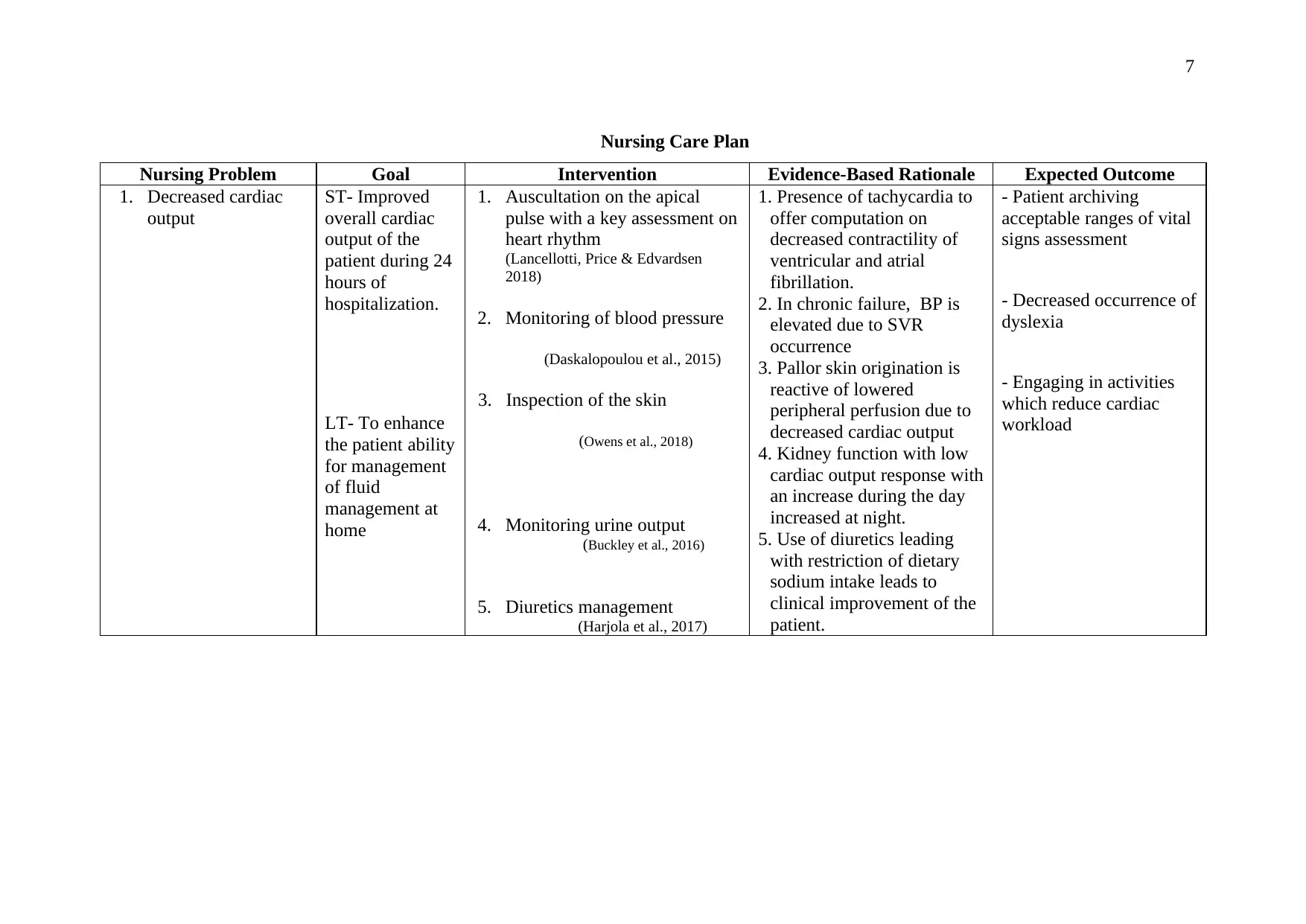
Nursing Care Plan
Nursing Problem Goal Intervention Evidence-Based Rationale Expected Outcome
1. Decreased cardiac
output
ST- Improved
overall cardiac
output of the
patient during 24
hours of
hospitalization.
LT- To enhance
the patient ability
for management
of fluid
management at
home
1. Auscultation on the apical
pulse with a key assessment on
heart rhythm
(Lancellotti, Price & Edvardsen
2018)
2. Monitoring of blood pressure
(Daskalopoulou et al., 2015)
3. Inspection of the skin
(Owens et al., 2018)
4. Monitoring urine output
(Buckley et al., 2016)
5. Diuretics management
(Harjola et al., 2017)
1. Presence of tachycardia to
offer computation on
decreased contractility of
ventricular and atrial
fibrillation.
2. In chronic failure, BP is
elevated due to SVR
occurrence
3. Pallor skin origination is
reactive of lowered
peripheral perfusion due to
decreased cardiac output
4. Kidney function with low
cardiac output response with
an increase during the day
increased at night.
5. Use of diuretics leading
with restriction of dietary
sodium intake leads to
clinical improvement of the
patient.
- Patient archiving
acceptable ranges of vital
signs assessment
- Decreased occurrence of
dyslexia
- Engaging in activities
which reduce cardiac
workload
Nursing Care Plan
Nursing Problem Goal Intervention Evidence-Based Rationale Expected Outcome
1. Decreased cardiac
output
ST- Improved
overall cardiac
output of the
patient during 24
hours of
hospitalization.
LT- To enhance
the patient ability
for management
of fluid
management at
home
1. Auscultation on the apical
pulse with a key assessment on
heart rhythm
(Lancellotti, Price & Edvardsen
2018)
2. Monitoring of blood pressure
(Daskalopoulou et al., 2015)
3. Inspection of the skin
(Owens et al., 2018)
4. Monitoring urine output
(Buckley et al., 2016)
5. Diuretics management
(Harjola et al., 2017)
1. Presence of tachycardia to
offer computation on
decreased contractility of
ventricular and atrial
fibrillation.
2. In chronic failure, BP is
elevated due to SVR
occurrence
3. Pallor skin origination is
reactive of lowered
peripheral perfusion due to
decreased cardiac output
4. Kidney function with low
cardiac output response with
an increase during the day
increased at night.
5. Use of diuretics leading
with restriction of dietary
sodium intake leads to
clinical improvement of the
patient.
- Patient archiving
acceptable ranges of vital
signs assessment
- Decreased occurrence of
dyslexia
- Engaging in activities
which reduce cardiac
workload
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
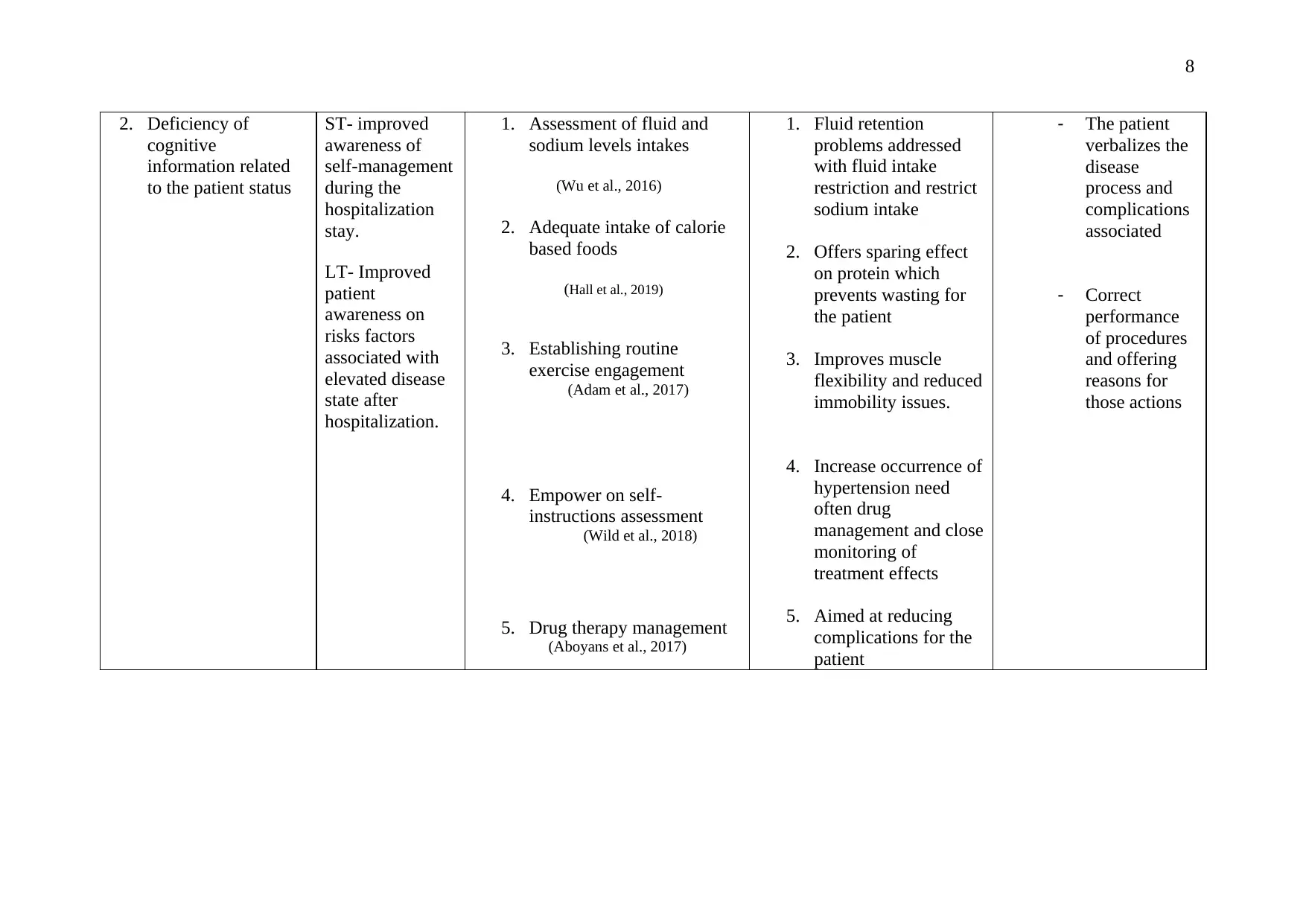
2. Deficiency of
cognitive
information related
to the patient status
ST- improved
awareness of
self-management
during the
hospitalization
stay.
LT- Improved
patient
awareness on
risks factors
associated with
elevated disease
state after
hospitalization.
1. Assessment of fluid and
sodium levels intakes
(Wu et al., 2016)
2. Adequate intake of calorie
based foods
(Hall et al., 2019)
3. Establishing routine
exercise engagement
(Adam et al., 2017)
4. Empower on self-
instructions assessment
(Wild et al., 2018)
5. Drug therapy management
(Aboyans et al., 2017)
1. Fluid retention
problems addressed
with fluid intake
restriction and restrict
sodium intake
2. Offers sparing effect
on protein which
prevents wasting for
the patient
3. Improves muscle
flexibility and reduced
immobility issues.
4. Increase occurrence of
hypertension need
often drug
management and close
monitoring of
treatment effects
5. Aimed at reducing
complications for the
patient
- The patient
verbalizes the
disease
process and
complications
associated
- Correct
performance
of procedures
and offering
reasons for
those actions
2. Deficiency of
cognitive
information related
to the patient status
ST- improved
awareness of
self-management
during the
hospitalization
stay.
LT- Improved
patient
awareness on
risks factors
associated with
elevated disease
state after
hospitalization.
1. Assessment of fluid and
sodium levels intakes
(Wu et al., 2016)
2. Adequate intake of calorie
based foods
(Hall et al., 2019)
3. Establishing routine
exercise engagement
(Adam et al., 2017)
4. Empower on self-
instructions assessment
(Wild et al., 2018)
5. Drug therapy management
(Aboyans et al., 2017)
1. Fluid retention
problems addressed
with fluid intake
restriction and restrict
sodium intake
2. Offers sparing effect
on protein which
prevents wasting for
the patient
3. Improves muscle
flexibility and reduced
immobility issues.
4. Increase occurrence of
hypertension need
often drug
management and close
monitoring of
treatment effects
5. Aimed at reducing
complications for the
patient
- The patient
verbalizes the
disease
process and
complications
associated
- Correct
performance
of procedures
and offering
reasons for
those actions

9
Reflection
My overall assessment of this essay case study has strengthened my core skills and
improved learning outcomes on human physiology process. Learning the functioning of the
overall kidney process and heart function through patient assessment is critical. Application
of my nursing skills in offering nursing diagnosis plays a key role in ensuring successful
patient assessment. There is a need to further improve my nursing skills in order to offer a
high level of nursing care.
Reflection
My overall assessment of this essay case study has strengthened my core skills and
improved learning outcomes on human physiology process. Learning the functioning of the
overall kidney process and heart function through patient assessment is critical. Application
of my nursing skills in offering nursing diagnosis plays a key role in ensuring successful
patient assessment. There is a need to further improve my nursing skills in order to offer a
high level of nursing care.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10
References
Harjola, V. P., Mullens, W., Banaszewski, M., Bauersachs, J., Brunner‐La Rocca, H. P.,
Chioncel, O., ... & Fuhrmann, V. (2017). Organ dysfunction, injury and failure in acute
heart failure: from pathophysiology to diagnosis and management. A review on behalf
of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the
European Society of Cardiology (ESC). European journal of heart failure, 19(7), 821-
836.
Münzel, T., Gori, T., Keaney Jr, J. F., Maack, C., & Daiber, A. (2015). Pathophysiological
role of oxidative stress in systolic and diastolic heart failure and its therapeutic
implications. European heart journal, 36(38), 2555-2564.
Nijst, P., Verbrugge, F. H., Grieten, L., Dupont, M., Steels, P., Tang, W. W., & Mullens, W.
(2015). The pathophysiological role of interstitial sodium in heart failure. Journal of the
American College of Cardiology, 65(4), 378-388.
Arrigo, M., Parissis, J. T., Akiyama, E., & Mebazaa, A. (2016). Understanding acute heart
failure: pathophysiology and diagnosis. European Heart Journal Supplements,
18(suppl_G), G11-G18.
Malek, M., & Nematbakhsh, M. (2015). Renal ischemia/reperfusion injury; from
pathophysiology to treatment. Journal of renal injury prevention, 4(2), 20.
Di Lullo, L., Gorini, A., Russo, D., Santoboni, A., & Ronco, C. (2015). Left ventricular
hypertrophy in chronic kidney disease patients: from pathophysiology to treatment.
Cardiorenal medicine, 5(4), 254-266.
Schrezenmeier, E. V., Barasch, J., Budde, K., Westhoff, T., & Schmidt‐Ott, K. M. (2017).
Biomarkers in acute kidney injury–pathophysiological basis and clinical performance.
Acta physiologica, 219(3), 556-574.
Kato, G. J., Steinberg, M. H., & Gladwin, M. T. (2017). Intravascular hemolysis and the
pathophysiology of sickle cell disease. The Journal of clinical investigation, 127(3),
750-760.
References
Harjola, V. P., Mullens, W., Banaszewski, M., Bauersachs, J., Brunner‐La Rocca, H. P.,
Chioncel, O., ... & Fuhrmann, V. (2017). Organ dysfunction, injury and failure in acute
heart failure: from pathophysiology to diagnosis and management. A review on behalf
of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the
European Society of Cardiology (ESC). European journal of heart failure, 19(7), 821-
836.
Münzel, T., Gori, T., Keaney Jr, J. F., Maack, C., & Daiber, A. (2015). Pathophysiological
role of oxidative stress in systolic and diastolic heart failure and its therapeutic
implications. European heart journal, 36(38), 2555-2564.
Nijst, P., Verbrugge, F. H., Grieten, L., Dupont, M., Steels, P., Tang, W. W., & Mullens, W.
(2015). The pathophysiological role of interstitial sodium in heart failure. Journal of the
American College of Cardiology, 65(4), 378-388.
Arrigo, M., Parissis, J. T., Akiyama, E., & Mebazaa, A. (2016). Understanding acute heart
failure: pathophysiology and diagnosis. European Heart Journal Supplements,
18(suppl_G), G11-G18.
Malek, M., & Nematbakhsh, M. (2015). Renal ischemia/reperfusion injury; from
pathophysiology to treatment. Journal of renal injury prevention, 4(2), 20.
Di Lullo, L., Gorini, A., Russo, D., Santoboni, A., & Ronco, C. (2015). Left ventricular
hypertrophy in chronic kidney disease patients: from pathophysiology to treatment.
Cardiorenal medicine, 5(4), 254-266.
Schrezenmeier, E. V., Barasch, J., Budde, K., Westhoff, T., & Schmidt‐Ott, K. M. (2017).
Biomarkers in acute kidney injury–pathophysiological basis and clinical performance.
Acta physiologica, 219(3), 556-574.
Kato, G. J., Steinberg, M. H., & Gladwin, M. T. (2017). Intravascular hemolysis and the
pathophysiology of sickle cell disease. The Journal of clinical investigation, 127(3),
750-760.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11
Ter Maaten, J. M., Damman, K., Verhaar, M. C., Paulus, W. J., Duncker, D. J., Cheng, C., ...
& Voors, A. A. (2016). Connecting heart failure with preserved ejection fraction and
renal dysfunction: the role of endothelial dysfunction and inflammation. European
journal of heart failure, 18(6), 588-598.
Evrard, S., Delanaye, P., Kamel, S., Cristol, J. P., Cavalier, E., Arnaud, J., ... & Cavalier, E.
(2015). Vascular calcification: from pathophysiology to biomarkers. Clinica Chimica
Acta, 438, 401-414.
Bartunek, J., Davison, B., Sherman, W., Povsic, T., Henry, T. D., Gersh, B., ... & Homsy, C.
(2016). Congestive heart failure cardiopoietic regenerative therapy (CHART‐1) trial
design. European journal of heart failure, 18(2), 160-168.
Lancellotti, P., Price, S., & Edvardsen, T. (2018). Association of CardiovascularImaging and
the Acute Cardiovascular Care Association. Eur HeartJ Cardiovasc Imaging 2015; 16:
119–46. National Institute for Health and Care Excellence. Nice Guidelines (CG 187)
2014: Acute Heart Failure: Diagnosing and Managing Acute Heart Failure in Adults.
2014. Available at https://www. nice. org. Diagnosis and Treatment in Internal
Medicine, 67, 49.
Daskalopoulou, S. S., Rabi, D. M., Zarnke, K. B., Dasgupta, K., Nerenberg, K., Cloutier,
L., ... & McKay, D. W. (2015). The 2015 Canadian Hypertension Education Program
recommendations for blood pressure measurement, diagnosis, assessment of risk,
prevention, and treatment of hypertension. Canadian Journal of Cardiology, 31(5),
549-568.
Owens, L., Warfield, T., MacDonald, R., & Krenzischek, E. (2018). Using Alternative Light
Source Technology to Enhance Visual Inspection of the Skin. Journal of Wound
Ostomy & Continence Nursing, 45(4), 356-358.
Buckley, L. F., Carter, D. M., Matta, L., Cheng, J. W., Stevens, C., Belenkiy, R. M., ... &
Stevenson, L. W. (2016). Intravenous diuretic therapy for the management of heart
failure and volume overload in a multidisciplinary outpatient unit. JACC: Heart
Failure, 4(1), 1-8.
Ter Maaten, J. M., Damman, K., Verhaar, M. C., Paulus, W. J., Duncker, D. J., Cheng, C., ...
& Voors, A. A. (2016). Connecting heart failure with preserved ejection fraction and
renal dysfunction: the role of endothelial dysfunction and inflammation. European
journal of heart failure, 18(6), 588-598.
Evrard, S., Delanaye, P., Kamel, S., Cristol, J. P., Cavalier, E., Arnaud, J., ... & Cavalier, E.
(2015). Vascular calcification: from pathophysiology to biomarkers. Clinica Chimica
Acta, 438, 401-414.
Bartunek, J., Davison, B., Sherman, W., Povsic, T., Henry, T. D., Gersh, B., ... & Homsy, C.
(2016). Congestive heart failure cardiopoietic regenerative therapy (CHART‐1) trial
design. European journal of heart failure, 18(2), 160-168.
Lancellotti, P., Price, S., & Edvardsen, T. (2018). Association of CardiovascularImaging and
the Acute Cardiovascular Care Association. Eur HeartJ Cardiovasc Imaging 2015; 16:
119–46. National Institute for Health and Care Excellence. Nice Guidelines (CG 187)
2014: Acute Heart Failure: Diagnosing and Managing Acute Heart Failure in Adults.
2014. Available at https://www. nice. org. Diagnosis and Treatment in Internal
Medicine, 67, 49.
Daskalopoulou, S. S., Rabi, D. M., Zarnke, K. B., Dasgupta, K., Nerenberg, K., Cloutier,
L., ... & McKay, D. W. (2015). The 2015 Canadian Hypertension Education Program
recommendations for blood pressure measurement, diagnosis, assessment of risk,
prevention, and treatment of hypertension. Canadian Journal of Cardiology, 31(5),
549-568.
Owens, L., Warfield, T., MacDonald, R., & Krenzischek, E. (2018). Using Alternative Light
Source Technology to Enhance Visual Inspection of the Skin. Journal of Wound
Ostomy & Continence Nursing, 45(4), 356-358.
Buckley, L. F., Carter, D. M., Matta, L., Cheng, J. W., Stevens, C., Belenkiy, R. M., ... &
Stevenson, L. W. (2016). Intravenous diuretic therapy for the management of heart
failure and volume overload in a multidisciplinary outpatient unit. JACC: Heart
Failure, 4(1), 1-8.
12
Harjola, V. P., Mullens, W., Banaszewski, M., Bauersachs, J., Brunner‐La Rocca, H. P.,
Chioncel, O., ... & Fuhrmann, V. (2017). Organ dysfunction, injury and failure in acute
heart failure: from pathophysiology to diagnosis and management. A review on behalf
of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the
European Society of Cardiology (ESC). European journal of heart failure, 19(7), 821-
836.
Wu, L. W., Chen, W. L., Liaw, F. Y., Sun, Y. S., Yang, H. F., Wang, C. C., ... & Tsao, Y. T.
(2016). Association between fluid intake and kidney function, and survival outcomes
analysis: a nationwide population-based study. BMJ open, 6(5), e010708.
Hall, J. A., Fritsch, D. A., Jewell, D. E., Burris, P. A., & Gross, K. L. (2019). Cats with IRIS
stage 1 and 2 chronic kidney disease maintain body weight and lean muscle mass when
fed food having increased caloric density, and enhanced concentrations of carnitine and
essential amino acids. Veterinary Record, 184(6), 190-190.
Adam, J. K., Singh, S., Nasr, M., & Krishna, S. B. N. (2017). Impact of airogym exercise on
solute removal and oedema on end-stage kidney disease patients: a randomised
controlled trial. Medical Technology SA, 31(1), 1-8.
Wild, M. G., Ostini, R., Harrington, M., Cavanaugh, K. L., & Wallston, K. A. (2018).
Validation of the shortened Perceived Medical Condition Self-Management Scale in
patients with chronic disease. Psychological assessment, 30(10), 1300.
Aboyans, V., Ricco, J. B., Bartelink, M. L. E., Björck, M., Brodmann, M., Cohnert, T., ... &
Espinola-Klein, C. (2017). 2017 ESC Guidelines on the Diagnosis and Treatment of
Peripheral Arterial Diseases, in collaboration with the European Society for Vascular
Surgery (ESVS) Document covering atherosclerotic disease of extracranial carotid and
vertebral, mesenteric, renal, upper and lower extremity arteries Endorsed by: the
European Stroke Organization (ESO) The Task Force for the Diagnosis and Treatment
of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the
European Society for Vascular .... European heart journal, 39(9), 763-816.
Harjola, V. P., Mullens, W., Banaszewski, M., Bauersachs, J., Brunner‐La Rocca, H. P.,
Chioncel, O., ... & Fuhrmann, V. (2017). Organ dysfunction, injury and failure in acute
heart failure: from pathophysiology to diagnosis and management. A review on behalf
of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the
European Society of Cardiology (ESC). European journal of heart failure, 19(7), 821-
836.
Wu, L. W., Chen, W. L., Liaw, F. Y., Sun, Y. S., Yang, H. F., Wang, C. C., ... & Tsao, Y. T.
(2016). Association between fluid intake and kidney function, and survival outcomes
analysis: a nationwide population-based study. BMJ open, 6(5), e010708.
Hall, J. A., Fritsch, D. A., Jewell, D. E., Burris, P. A., & Gross, K. L. (2019). Cats with IRIS
stage 1 and 2 chronic kidney disease maintain body weight and lean muscle mass when
fed food having increased caloric density, and enhanced concentrations of carnitine and
essential amino acids. Veterinary Record, 184(6), 190-190.
Adam, J. K., Singh, S., Nasr, M., & Krishna, S. B. N. (2017). Impact of airogym exercise on
solute removal and oedema on end-stage kidney disease patients: a randomised
controlled trial. Medical Technology SA, 31(1), 1-8.
Wild, M. G., Ostini, R., Harrington, M., Cavanaugh, K. L., & Wallston, K. A. (2018).
Validation of the shortened Perceived Medical Condition Self-Management Scale in
patients with chronic disease. Psychological assessment, 30(10), 1300.
Aboyans, V., Ricco, J. B., Bartelink, M. L. E., Björck, M., Brodmann, M., Cohnert, T., ... &
Espinola-Klein, C. (2017). 2017 ESC Guidelines on the Diagnosis and Treatment of
Peripheral Arterial Diseases, in collaboration with the European Society for Vascular
Surgery (ESVS) Document covering atherosclerotic disease of extracranial carotid and
vertebral, mesenteric, renal, upper and lower extremity arteries Endorsed by: the
European Stroke Organization (ESO) The Task Force for the Diagnosis and Treatment
of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the
European Society for Vascular .... European heart journal, 39(9), 763-816.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.