NURBN2016 Case Study: Melanie Johnson's Chronic Renal Failure
VerifiedAdded on 2023/01/04
|12
|3346
|43
Case Study
AI Summary
This case study focuses on Melanie Johnson, a 55-year-old woman diagnosed with chronic renal failure. It details the anatomy and physiology of the renal system, the pathophysiology of chronic renal failure, and the differences between acute and chronic kidney disease. The study explores Melanie's risk factors, complications such as anemia and cardiovascular issues, and treatment modalities including drugs like Valsartan and Eprex. It also discusses hemodialysis, nursing considerations, and the significance of Melanie's GFR and Hb levels. The teach-back method for patient education is highlighted, emphasizing the importance of dietary management and fluid intake. The assignment solution provides a comprehensive overview of Melanie's condition and its management.

1
Running head: STUDY CASE
Student's Name:
Student Number:
Institutional Affiliation:
Date
1.1
Running head: STUDY CASE
Student's Name:
Student Number:
Institutional Affiliation:
Date
1.1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
STUDY
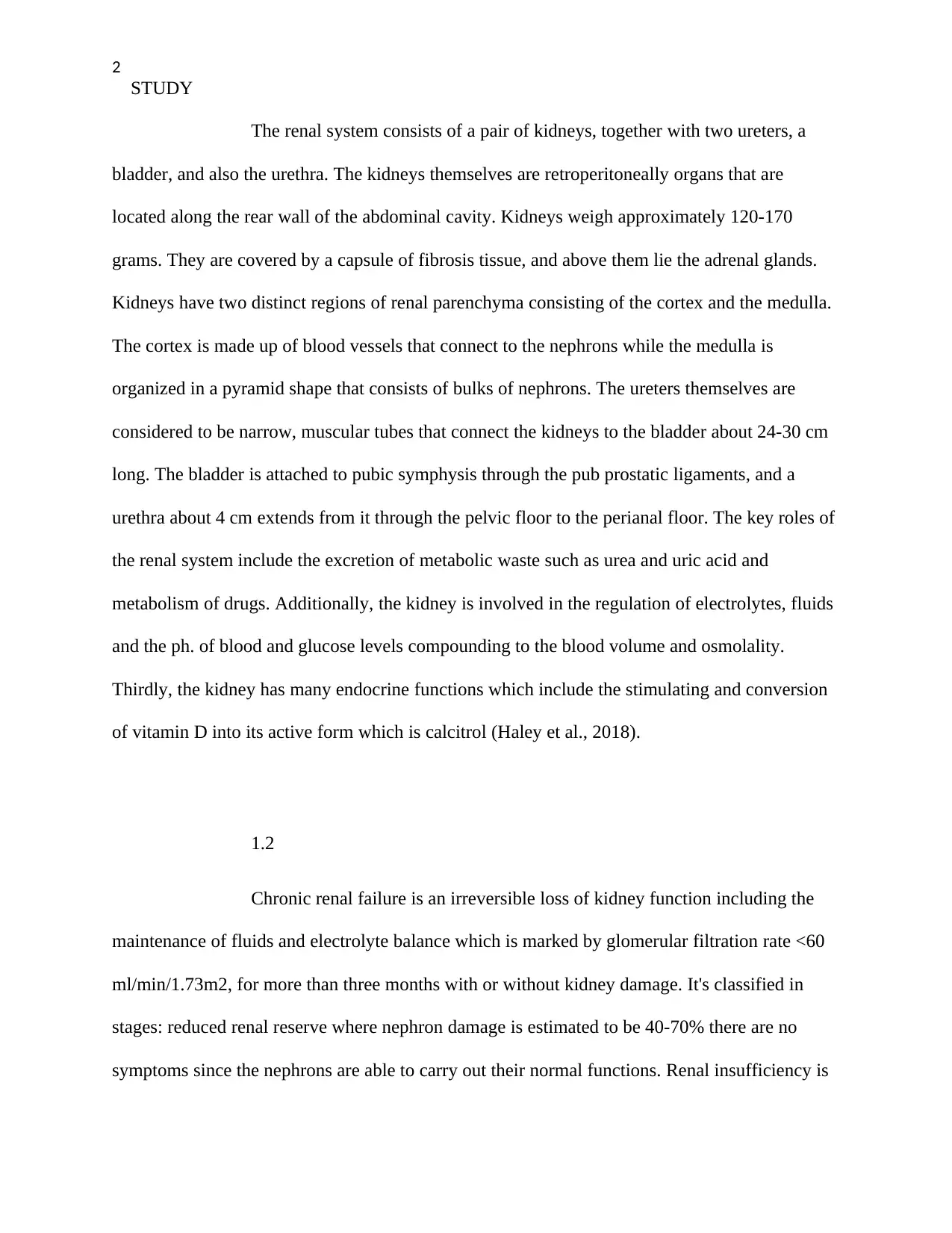
The renal system consists of a pair of kidneys, together with two ureters, a
bladder, and also the urethra. The kidneys themselves are retroperitoneally organs that are
located along the rear wall of the abdominal cavity. Kidneys weigh approximately 120-170
grams. They are covered by a capsule of fibrosis tissue, and above them lie the adrenal glands.
Kidneys have two distinct regions of renal parenchyma consisting of the cortex and the medulla.
The cortex is made up of blood vessels that connect to the nephrons while the medulla is
organized in a pyramid shape that consists of bulks of nephrons. The ureters themselves are
considered to be narrow, muscular tubes that connect the kidneys to the bladder about 24-30 cm
long. The bladder is attached to pubic symphysis through the pub prostatic ligaments, and a
urethra about 4 cm extends from it through the pelvic floor to the perianal floor. The key roles of
the renal system include the excretion of metabolic waste such as urea and uric acid and
metabolism of drugs. Additionally, the kidney is involved in the regulation of electrolytes, fluids
and the ph. of blood and glucose levels compounding to the blood volume and osmolality.
Thirdly, the kidney has many endocrine functions which include the stimulating and conversion
of vitamin D into its active form which is calcitrol (Haley et al., 2018).
1.2
Chronic renal failure is an irreversible loss of kidney function including the
maintenance of fluids and electrolyte balance which is marked by glomerular filtration rate <60
ml/min/1.73m2, for more than three months with or without kidney damage. It's classified in
stages: reduced renal reserve where nephron damage is estimated to be 40-70% there are no
symptoms since the nephrons are able to carry out their normal functions. Renal insufficiency is
STUDY
The renal system consists of a pair of kidneys, together with two ureters, a
bladder, and also the urethra. The kidneys themselves are retroperitoneally organs that are
located along the rear wall of the abdominal cavity. Kidneys weigh approximately 120-170
grams. They are covered by a capsule of fibrosis tissue, and above them lie the adrenal glands.
Kidneys have two distinct regions of renal parenchyma consisting of the cortex and the medulla.
The cortex is made up of blood vessels that connect to the nephrons while the medulla is
organized in a pyramid shape that consists of bulks of nephrons. The ureters themselves are
considered to be narrow, muscular tubes that connect the kidneys to the bladder about 24-30 cm
long. The bladder is attached to pubic symphysis through the pub prostatic ligaments, and a
urethra about 4 cm extends from it through the pelvic floor to the perianal floor. The key roles of
the renal system include the excretion of metabolic waste such as urea and uric acid and
metabolism of drugs. Additionally, the kidney is involved in the regulation of electrolytes, fluids
and the ph. of blood and glucose levels compounding to the blood volume and osmolality.
Thirdly, the kidney has many endocrine functions which include the stimulating and conversion
of vitamin D into its active form which is calcitrol (Haley et al., 2018).
1.2
Chronic renal failure is an irreversible loss of kidney function including the
maintenance of fluids and electrolyte balance which is marked by glomerular filtration rate <60
ml/min/1.73m2, for more than three months with or without kidney damage. It's classified in
stages: reduced renal reserve where nephron damage is estimated to be 40-70% there are no
symptoms since the nephrons are able to carry out their normal functions. Renal insufficiency is
3
STUDY
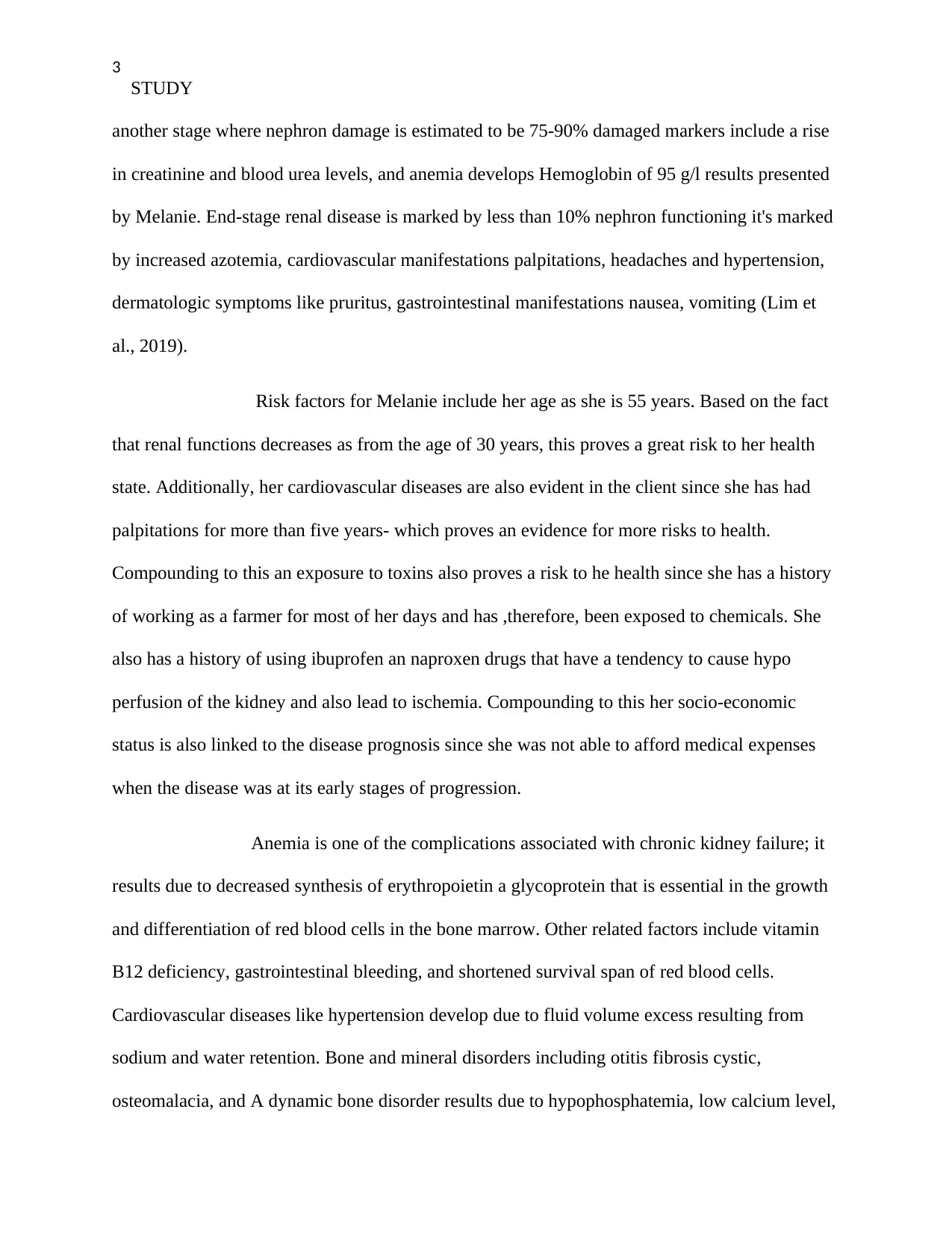
another stage where nephron damage is estimated to be 75-90% damaged markers include a rise
in creatinine and blood urea levels, and anemia develops Hemoglobin of 95 g/l results presented
by Melanie. End-stage renal disease is marked by less than 10% nephron functioning it's marked
by increased azotemia, cardiovascular manifestations palpitations, headaches and hypertension,
dermatologic symptoms like pruritus, gastrointestinal manifestations nausea, vomiting (Lim et
al., 2019).
Risk factors for Melanie include her age as she is 55 years. Based on the fact
that renal functions decreases as from the age of 30 years, this proves a great risk to her health
state. Additionally, her cardiovascular diseases are also evident in the client since she has had
palpitations for more than five years- which proves an evidence for more risks to health.
Compounding to this an exposure to toxins also proves a risk to he health since she has a history
of working as a farmer for most of her days and has ,therefore, been exposed to chemicals. She
also has a history of using ibuprofen an naproxen drugs that have a tendency to cause hypo
perfusion of the kidney and also lead to ischemia. Compounding to this her socio-economic
status is also linked to the disease prognosis since she was not able to afford medical expenses
when the disease was at its early stages of progression.
Anemia is one of the complications associated with chronic kidney failure; it
results due to decreased synthesis of erythropoietin a glycoprotein that is essential in the growth
and differentiation of red blood cells in the bone marrow. Other related factors include vitamin
B12 deficiency, gastrointestinal bleeding, and shortened survival span of red blood cells.
Cardiovascular diseases like hypertension develop due to fluid volume excess resulting from
sodium and water retention. Bone and mineral disorders including otitis fibrosis cystic,
osteomalacia, and A dynamic bone disorder results due to hypophosphatemia, low calcium level,
STUDY
another stage where nephron damage is estimated to be 75-90% damaged markers include a rise
in creatinine and blood urea levels, and anemia develops Hemoglobin of 95 g/l results presented
by Melanie. End-stage renal disease is marked by less than 10% nephron functioning it's marked
by increased azotemia, cardiovascular manifestations palpitations, headaches and hypertension,
dermatologic symptoms like pruritus, gastrointestinal manifestations nausea, vomiting (Lim et
al., 2019).
Risk factors for Melanie include her age as she is 55 years. Based on the fact
that renal functions decreases as from the age of 30 years, this proves a great risk to her health
state. Additionally, her cardiovascular diseases are also evident in the client since she has had
palpitations for more than five years- which proves an evidence for more risks to health.
Compounding to this an exposure to toxins also proves a risk to he health since she has a history
of working as a farmer for most of her days and has ,therefore, been exposed to chemicals. She
also has a history of using ibuprofen an naproxen drugs that have a tendency to cause hypo
perfusion of the kidney and also lead to ischemia. Compounding to this her socio-economic
status is also linked to the disease prognosis since she was not able to afford medical expenses
when the disease was at its early stages of progression.
Anemia is one of the complications associated with chronic kidney failure; it
results due to decreased synthesis of erythropoietin a glycoprotein that is essential in the growth
and differentiation of red blood cells in the bone marrow. Other related factors include vitamin
B12 deficiency, gastrointestinal bleeding, and shortened survival span of red blood cells.
Cardiovascular diseases like hypertension develop due to fluid volume excess resulting from
sodium and water retention. Bone and mineral disorders including otitis fibrosis cystic,
osteomalacia, and A dynamic bone disorder results due to hypophosphatemia, low calcium level,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
STUDY
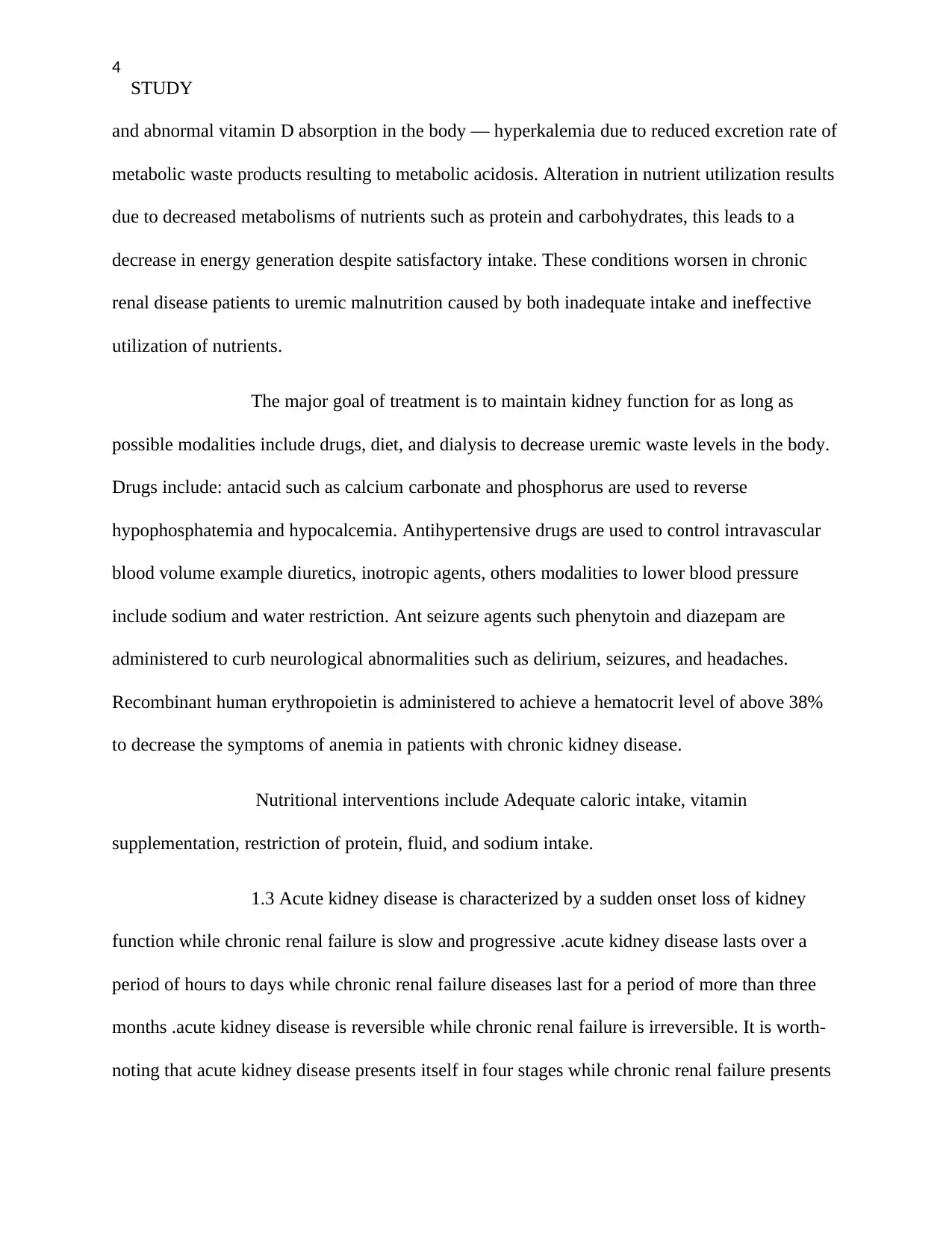
and abnormal vitamin D absorption in the body — hyperkalemia due to reduced excretion rate of
metabolic waste products resulting to metabolic acidosis. Alteration in nutrient utilization results
due to decreased metabolisms of nutrients such as protein and carbohydrates, this leads to a
decrease in energy generation despite satisfactory intake. These conditions worsen in chronic
renal disease patients to uremic malnutrition caused by both inadequate intake and ineffective
utilization of nutrients.
The major goal of treatment is to maintain kidney function for as long as
possible modalities include drugs, diet, and dialysis to decrease uremic waste levels in the body.
Drugs include: antacid such as calcium carbonate and phosphorus are used to reverse
hypophosphatemia and hypocalcemia. Antihypertensive drugs are used to control intravascular
blood volume example diuretics, inotropic agents, others modalities to lower blood pressure
include sodium and water restriction. Ant seizure agents such phenytoin and diazepam are
administered to curb neurological abnormalities such as delirium, seizures, and headaches.
Recombinant human erythropoietin is administered to achieve a hematocrit level of above 38%
to decrease the symptoms of anemia in patients with chronic kidney disease.
Nutritional interventions include Adequate caloric intake, vitamin
supplementation, restriction of protein, fluid, and sodium intake.
1.3 Acute kidney disease is characterized by a sudden onset loss of kidney
function while chronic renal failure is slow and progressive .acute kidney disease lasts over a
period of hours to days while chronic renal failure diseases last for a period of more than three
months .acute kidney disease is reversible while chronic renal failure is irreversible. It is worth-
noting that acute kidney disease presents itself in four stages while chronic renal failure presents
STUDY
and abnormal vitamin D absorption in the body — hyperkalemia due to reduced excretion rate of
metabolic waste products resulting to metabolic acidosis. Alteration in nutrient utilization results
due to decreased metabolisms of nutrients such as protein and carbohydrates, this leads to a
decrease in energy generation despite satisfactory intake. These conditions worsen in chronic
renal disease patients to uremic malnutrition caused by both inadequate intake and ineffective
utilization of nutrients.
The major goal of treatment is to maintain kidney function for as long as
possible modalities include drugs, diet, and dialysis to decrease uremic waste levels in the body.
Drugs include: antacid such as calcium carbonate and phosphorus are used to reverse
hypophosphatemia and hypocalcemia. Antihypertensive drugs are used to control intravascular
blood volume example diuretics, inotropic agents, others modalities to lower blood pressure
include sodium and water restriction. Ant seizure agents such phenytoin and diazepam are
administered to curb neurological abnormalities such as delirium, seizures, and headaches.
Recombinant human erythropoietin is administered to achieve a hematocrit level of above 38%
to decrease the symptoms of anemia in patients with chronic kidney disease.
Nutritional interventions include Adequate caloric intake, vitamin
supplementation, restriction of protein, fluid, and sodium intake.
1.3 Acute kidney disease is characterized by a sudden onset loss of kidney
function while chronic renal failure is slow and progressive .acute kidney disease lasts over a
period of hours to days while chronic renal failure diseases last for a period of more than three
months .acute kidney disease is reversible while chronic renal failure is irreversible. It is worth-
noting that acute kidney disease presents itself in four stages while chronic renal failure presents
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
STUDY
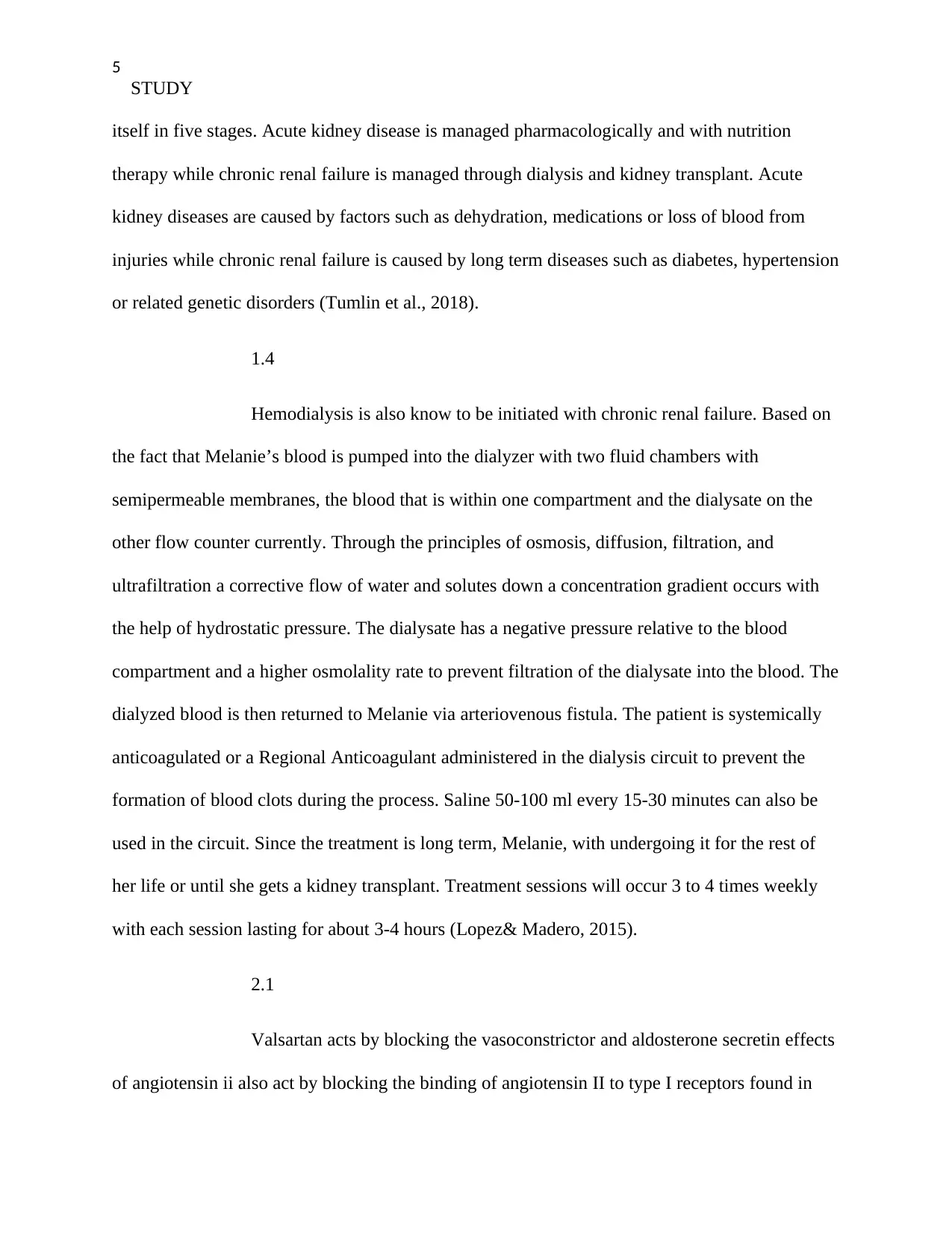
itself in five stages. Acute kidney disease is managed pharmacologically and with nutrition
therapy while chronic renal failure is managed through dialysis and kidney transplant. Acute
kidney diseases are caused by factors such as dehydration, medications or loss of blood from
injuries while chronic renal failure is caused by long term diseases such as diabetes, hypertension
or related genetic disorders (Tumlin et al., 2018).
1.4
Hemodialysis is also know to be initiated with chronic renal failure. Based on
the fact that Melanie’s blood is pumped into the dialyzer with two fluid chambers with
semipermeable membranes, the blood that is within one compartment and the dialysate on the
other flow counter currently. Through the principles of osmosis, diffusion, filtration, and
ultrafiltration a corrective flow of water and solutes down a concentration gradient occurs with
the help of hydrostatic pressure. The dialysate has a negative pressure relative to the blood
compartment and a higher osmolality rate to prevent filtration of the dialysate into the blood. The
dialyzed blood is then returned to Melanie via arteriovenous fistula. The patient is systemically
anticoagulated or a Regional Anticoagulant administered in the dialysis circuit to prevent the
formation of blood clots during the process. Saline 50-100 ml every 15-30 minutes can also be
used in the circuit. Since the treatment is long term, Melanie, with undergoing it for the rest of
her life or until she gets a kidney transplant. Treatment sessions will occur 3 to 4 times weekly
with each session lasting for about 3-4 hours (Lopez& Madero, 2015).
2.1
Valsartan acts by blocking the vasoconstrictor and aldosterone secretin effects
of angiotensin ii also act by blocking the binding of angiotensin II to type I receptors found in
STUDY
itself in five stages. Acute kidney disease is managed pharmacologically and with nutrition
therapy while chronic renal failure is managed through dialysis and kidney transplant. Acute
kidney diseases are caused by factors such as dehydration, medications or loss of blood from
injuries while chronic renal failure is caused by long term diseases such as diabetes, hypertension
or related genetic disorders (Tumlin et al., 2018).
1.4
Hemodialysis is also know to be initiated with chronic renal failure. Based on
the fact that Melanie’s blood is pumped into the dialyzer with two fluid chambers with
semipermeable membranes, the blood that is within one compartment and the dialysate on the
other flow counter currently. Through the principles of osmosis, diffusion, filtration, and
ultrafiltration a corrective flow of water and solutes down a concentration gradient occurs with
the help of hydrostatic pressure. The dialysate has a negative pressure relative to the blood
compartment and a higher osmolality rate to prevent filtration of the dialysate into the blood. The
dialyzed blood is then returned to Melanie via arteriovenous fistula. The patient is systemically
anticoagulated or a Regional Anticoagulant administered in the dialysis circuit to prevent the
formation of blood clots during the process. Saline 50-100 ml every 15-30 minutes can also be
used in the circuit. Since the treatment is long term, Melanie, with undergoing it for the rest of
her life or until she gets a kidney transplant. Treatment sessions will occur 3 to 4 times weekly
with each session lasting for about 3-4 hours (Lopez& Madero, 2015).
2.1
Valsartan acts by blocking the vasoconstrictor and aldosterone secretin effects
of angiotensin ii also act by blocking the binding of angiotensin II to type I receptors found in
6
STUDY
tissues The drug is used in the treatment of Hypertension a condition characterized by
persistence increased in blood pressures above 140/90mmHg. Side effects of the drug include
central nervous system effects dizziness insomnia, drowsiness, and fatigue. Cardiovascular
system, myocardial infarction, cerebrovascular accident, hypotension, angina pectoris.
Gastrointestinal system hepatotoxicity, diarrhea, nausea, and vomiting. Genitourinary system
impotence, renal failure, and nephrotoxicity (Pianta et al., 2015; Whalen, 2018).
Nursing considerations
Assessment of blood pressure and pulse note the rate, duration, and rhythm
every quarter-hourly while she's lying, sitting or walking. Check the levels of blood urea
nitrogen, creatinine, liver function tests, and bilirubin levels before administering the drug to
prevent hyper toxicity. Perform a daily facial assessment for angioedema, shortness of breath,
and edema on the feet to rule out renal failure. A skin turgor assessment is key to check the
hydration status by checking the mucous membrane and correct volume depletion before
administering the drug therapy.
Eprex is an erythropoietin synthetic drug that has biological activity as the
endogenous hormone in the human body. Acts by inducing erythropoiesis by stimulating the
differentiation and division of erythroid progenitor cells in the bone marrow. It also stimulates
the release of reticulocytes from the bone marrow to the bloodstream. Its administered to patients
with chronic renal failure and blood cancers.
Central nervous system-related side effects include seizures, headaches,
fatigue and dizziness .cardiovascular effects, hypertensive encephalopathy, congestive heart
failure, myocardial infarction, stroke, and deep venous thrombosis may result. Integumentary:
STUDY
tissues The drug is used in the treatment of Hypertension a condition characterized by
persistence increased in blood pressures above 140/90mmHg. Side effects of the drug include
central nervous system effects dizziness insomnia, drowsiness, and fatigue. Cardiovascular
system, myocardial infarction, cerebrovascular accident, hypotension, angina pectoris.
Gastrointestinal system hepatotoxicity, diarrhea, nausea, and vomiting. Genitourinary system
impotence, renal failure, and nephrotoxicity (Pianta et al., 2015; Whalen, 2018).
Nursing considerations
Assessment of blood pressure and pulse note the rate, duration, and rhythm
every quarter-hourly while she's lying, sitting or walking. Check the levels of blood urea
nitrogen, creatinine, liver function tests, and bilirubin levels before administering the drug to
prevent hyper toxicity. Perform a daily facial assessment for angioedema, shortness of breath,
and edema on the feet to rule out renal failure. A skin turgor assessment is key to check the
hydration status by checking the mucous membrane and correct volume depletion before
administering the drug therapy.
Eprex is an erythropoietin synthetic drug that has biological activity as the
endogenous hormone in the human body. Acts by inducing erythropoiesis by stimulating the
differentiation and division of erythroid progenitor cells in the bone marrow. It also stimulates
the release of reticulocytes from the bone marrow to the bloodstream. Its administered to patients
with chronic renal failure and blood cancers.
Central nervous system-related side effects include seizures, headaches,
fatigue and dizziness .cardiovascular effects, hypertensive encephalopathy, congestive heart
failure, myocardial infarction, stroke, and deep venous thrombosis may result. Integumentary:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
STUDY
pruritus and rush on the injection site. Musculoskeletal effects include myalgia, arthralgia, and
bone pain (Tamura et al., 2016).
Nursing considerations
The assessment of the renal values is essential in studies of blood urea,
nitrogen, urinalysis, creatinine, input and also the output evaluation. Evaluation of the vital signs
by checking the blood pressure levels and the levels of hematocrit rises in order to avert
hypertensive encephalopathy. Progressive monitoring of the patient in terms of assessing the
patient seizure and hematocrit levels is essential within the span of two weeks accompanied by
monitoring any increases in blood pressure that may be noted within the period after 90 days of
using the treatment modalities. Health teaching to Melanie and the family to report immediately
to the hospital in case she develops signs of chest pain, pain in the calf muscles, numbness in the
face, legs and arms, and, inability to speak (Meersch et al., 2018).
2.2
The GFR from Melanie was found to be 10ml/min/1.73m2 while her Hb was
found to be 95g/l -a lot of information can be derived from this. Based on the fact that the
glomerular filtration rate is used to asses the functioning of the kidney, and its ability to assess
how much blood is capable of passing through the kidney during each minute- valuable
information can be collected from it. The glomeruli filtration rate measures how much blood
passes through the kidney each minute and can provide substantial information regarding the
normal functioning of the kidney (Kaufman, Basit & Knohl, 2019; Karger et al., 2017). The
STUDY
pruritus and rush on the injection site. Musculoskeletal effects include myalgia, arthralgia, and
bone pain (Tamura et al., 2016).
Nursing considerations
The assessment of the renal values is essential in studies of blood urea,
nitrogen, urinalysis, creatinine, input and also the output evaluation. Evaluation of the vital signs
by checking the blood pressure levels and the levels of hematocrit rises in order to avert
hypertensive encephalopathy. Progressive monitoring of the patient in terms of assessing the
patient seizure and hematocrit levels is essential within the span of two weeks accompanied by
monitoring any increases in blood pressure that may be noted within the period after 90 days of
using the treatment modalities. Health teaching to Melanie and the family to report immediately
to the hospital in case she develops signs of chest pain, pain in the calf muscles, numbness in the
face, legs and arms, and, inability to speak (Meersch et al., 2018).
2.2
The GFR from Melanie was found to be 10ml/min/1.73m2 while her Hb was
found to be 95g/l -a lot of information can be derived from this. Based on the fact that the
glomerular filtration rate is used to asses the functioning of the kidney, and its ability to assess
how much blood is capable of passing through the kidney during each minute- valuable
information can be collected from it. The glomeruli filtration rate measures how much blood
passes through the kidney each minute and can provide substantial information regarding the
normal functioning of the kidney (Kaufman, Basit & Knohl, 2019; Karger et al., 2017). The
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
STUDY
normal glomerular filtration rate ranges from 90 to 120ml/min/1.73m2. However, it is important
to note that older people will have lower than normal GFR degrees due to the fact that it
decreases markedly with age. In the case of the patient, it is clear that there are signs of chronic
kidney disease based on the fact that the GFR is lower than 15/mL/min/1.73m2, and thus, kidney
failure is imminent. Immediate medical attention is needed. Additionally, the Hb levels of the
patient are also indicative of kidney problems based on the levels they are at (Dalal & Sehdev,
2019; Feteh et al., 2016).
3. How Melanie can manage her chronic renal failure.
What the teach-back method is
The teach-back method refers to a method through which is employed by a
health care provider to assess whether a patient can comprehend what he or she is being taught at
a particular instance. When a patient fully comprehends what they are being taught at a specific
point in time, they are capable of teaching-back the same information they are being taught. The
teach-back method is useful in assessing whether a patient is fully capable of using this
information in helping other patients suffering from the same situation or in the overall
management of the condition in question. The teach-back method is also useful in identifying
any gaps that may be present in the teaching process of the patient (Correia et al., 2019).
Educating the client
By using the teach-back method in educating Melanie on proper feeding and
diet, several facts will have to be allayed to her. Firstly, I would allay some of the important facts
associated with a diet that needs to be known in addition to the management of fluid intake, as it
may prove appropriate. It would prove crucial, however, to use easily understandable language
STUDY
normal glomerular filtration rate ranges from 90 to 120ml/min/1.73m2. However, it is important
to note that older people will have lower than normal GFR degrees due to the fact that it
decreases markedly with age. In the case of the patient, it is clear that there are signs of chronic
kidney disease based on the fact that the GFR is lower than 15/mL/min/1.73m2, and thus, kidney
failure is imminent. Immediate medical attention is needed. Additionally, the Hb levels of the
patient are also indicative of kidney problems based on the levels they are at (Dalal & Sehdev,
2019; Feteh et al., 2016).
3. How Melanie can manage her chronic renal failure.
What the teach-back method is
The teach-back method refers to a method through which is employed by a
health care provider to assess whether a patient can comprehend what he or she is being taught at
a particular instance. When a patient fully comprehends what they are being taught at a specific
point in time, they are capable of teaching-back the same information they are being taught. The
teach-back method is useful in assessing whether a patient is fully capable of using this
information in helping other patients suffering from the same situation or in the overall
management of the condition in question. The teach-back method is also useful in identifying
any gaps that may be present in the teaching process of the patient (Correia et al., 2019).
Educating the client
By using the teach-back method in educating Melanie on proper feeding and
diet, several facts will have to be allayed to her. Firstly, I would allay some of the important facts
associated with a diet that needs to be known in addition to the management of fluid intake, as it
may prove appropriate. It would prove crucial, however, to use easily understandable language
9
STUDY
while avoiding the use of jargons or words that bear a lot of scientific weight. The use of a diet
that has low-fat and also diary products is crucial for this patient in addition to the use of fish
poultry, beans, and seeds. It is also crucial that the patient avoids high caloric foods in his or her
diet in addition to foods that may contain additives of various forms. The main reason why the
client should avoid such foods is based on the fact that such foods would lead to anomalies due
to the stress from excessive need to excrete them from the body system (Klompas et al., 2019).
I will then move forward to ask the patient to explain the concept in their own
words. The patient will have to explain why it is necessary to avoid specific foods and drinks,
which may evidently affect the performance of the kidney in performing its duties in excretion.
The patient will have to explain the concepts explained and taught in his or her own words.
I will then move forward to assess the gaps that exist in my patient's
understanding of the process of kidney functioning and excretion and fill these gaps as
necessary. The filling of the gaps through clarifying concepts taught will enable me to drive the
point clearly to my patient. In the event that my patient does not comprehend the concepts
taught, I will have to re-educate the patient using specific tools such as charts and other
appropriate teaching methods. I will progressively move to asses the patients understanding of
kidney function in excretion until my patient is capable of understanding, comprehending and
explaining the concepts explained (Luo et al., 2018; Xu et al., 2015).
STUDY
while avoiding the use of jargons or words that bear a lot of scientific weight. The use of a diet
that has low-fat and also diary products is crucial for this patient in addition to the use of fish
poultry, beans, and seeds. It is also crucial that the patient avoids high caloric foods in his or her
diet in addition to foods that may contain additives of various forms. The main reason why the
client should avoid such foods is based on the fact that such foods would lead to anomalies due
to the stress from excessive need to excrete them from the body system (Klompas et al., 2019).
I will then move forward to ask the patient to explain the concept in their own
words. The patient will have to explain why it is necessary to avoid specific foods and drinks,
which may evidently affect the performance of the kidney in performing its duties in excretion.
The patient will have to explain the concepts explained and taught in his or her own words.
I will then move forward to assess the gaps that exist in my patient's
understanding of the process of kidney functioning and excretion and fill these gaps as
necessary. The filling of the gaps through clarifying concepts taught will enable me to drive the
point clearly to my patient. In the event that my patient does not comprehend the concepts
taught, I will have to re-educate the patient using specific tools such as charts and other
appropriate teaching methods. I will progressively move to asses the patients understanding of
kidney function in excretion until my patient is capable of understanding, comprehending and
explaining the concepts explained (Luo et al., 2018; Xu et al., 2015).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

10
STUDY
References
Correia, C. P., Martins, A., Oliveira, J., Andrade, S., & Almeida, J. (2019). Systemic
Amyloidosis with Renal Failure: A Challenging Diagnosis of SAPHO
Syndrome. European journal of case reports in internal medicine, 6(4).
Dalal, R., & Sehdev, J. S. (2019). Physiology, Renal, Blood Flow and Filtration. In StatPearls
[Internet]. StatPearls Publishing.
Feteh, V. F., Choukem, S. P., Kengne, A. P., Nebongo, D. N., & Ngowe-Ngowe, M. (2016).
Anemia in type 2 diabetic patients and correlation with kidney function in a
tertiary care sub-Saharan African hospital: a cross-sectional study. BMC
nephrology, 17(1), 29.
Haley, P. A., Zabaneh, I. D., Bandak, D. N., & Iskapalli, M. S. (2018). The Resolution of
Thyroid Storm Using Plasma Exchange and Continuous Renal Replacement
Therapy. Journal of Advances in Biology & Biotechnology, 1-4.
Kaufman, D. P., Basit, H., & Knohl, S. J. (2019). Physiology, Glomerular Filtration Rate (GFR).
In StatPearls [Internet]. StatPearls Publishing.
STUDY
References
Correia, C. P., Martins, A., Oliveira, J., Andrade, S., & Almeida, J. (2019). Systemic
Amyloidosis with Renal Failure: A Challenging Diagnosis of SAPHO
Syndrome. European journal of case reports in internal medicine, 6(4).
Dalal, R., & Sehdev, J. S. (2019). Physiology, Renal, Blood Flow and Filtration. In StatPearls
[Internet]. StatPearls Publishing.
Feteh, V. F., Choukem, S. P., Kengne, A. P., Nebongo, D. N., & Ngowe-Ngowe, M. (2016).
Anemia in type 2 diabetic patients and correlation with kidney function in a
tertiary care sub-Saharan African hospital: a cross-sectional study. BMC
nephrology, 17(1), 29.
Haley, P. A., Zabaneh, I. D., Bandak, D. N., & Iskapalli, M. S. (2018). The Resolution of
Thyroid Storm Using Plasma Exchange and Continuous Renal Replacement
Therapy. Journal of Advances in Biology & Biotechnology, 1-4.
Kaufman, D. P., Basit, H., & Knohl, S. J. (2019). Physiology, Glomerular Filtration Rate (GFR).
In StatPearls [Internet]. StatPearls Publishing.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11
STUDY
Karger, A. B., Inker, L. A., Coresh, J., Levey, A. S., & Eckfeldt, J. H. (2017). Novel filtration
markers for GFR estimation. EJIFCC, 28(4), 277.
Klompas, A. M., Albright, R. C., Maltais, S., & Demirci, O. (2019). Acute renal failure due to
bilateral renal vein thromboses: A rare complication of heparin-induced
thrombocytopenia. Annals of cardiac anaesthesia, 22(2), 204.
Lim, C. C., Chee, M. L., Cheng, C. Y., Kwek, J. L., Foo, M., Wong, T. Y., & Sabanayagam, C.
(2019). Simplified end stage renal failure risk prediction model for the low-
risk general population with chronic kidney disease. PloS one, 14(2),
e0212590.
Lopez-Giacoman, S., & Madero, M. (2015). Biomarkers in chronic kidney disease, from kidney
function to kidney damage. World journal of nephrology, 4(1), 57.
Luo, K., Fu, S., Fang, W., & Xu, G. (2018). Correction: The optimal time of initiation of renal
replacement therapy in acute kidney injury: A meta-analysis. Oncotarget, 9(5),
6657.
Meersch, M., Zarbock, A., & Küllmar, M. (2018). Renal biomarkers for the initiation of renal
replacement therapy—is this the future?. Journal of thoracic
disease, 10(Suppl 26), S3229.
Pianta, T. J., Endre, Z. H., Pickering, J. W., Buckley, N. A., & Peake, P. W. (2015). Kinetic
estimation of GFR improves prediction of dialysis and recovery after kidney
transplantation. PLoS One, 10(5), e0125669.
STUDY
Karger, A. B., Inker, L. A., Coresh, J., Levey, A. S., & Eckfeldt, J. H. (2017). Novel filtration
markers for GFR estimation. EJIFCC, 28(4), 277.
Klompas, A. M., Albright, R. C., Maltais, S., & Demirci, O. (2019). Acute renal failure due to
bilateral renal vein thromboses: A rare complication of heparin-induced
thrombocytopenia. Annals of cardiac anaesthesia, 22(2), 204.
Lim, C. C., Chee, M. L., Cheng, C. Y., Kwek, J. L., Foo, M., Wong, T. Y., & Sabanayagam, C.
(2019). Simplified end stage renal failure risk prediction model for the low-
risk general population with chronic kidney disease. PloS one, 14(2),
e0212590.
Lopez-Giacoman, S., & Madero, M. (2015). Biomarkers in chronic kidney disease, from kidney
function to kidney damage. World journal of nephrology, 4(1), 57.
Luo, K., Fu, S., Fang, W., & Xu, G. (2018). Correction: The optimal time of initiation of renal
replacement therapy in acute kidney injury: A meta-analysis. Oncotarget, 9(5),
6657.
Meersch, M., Zarbock, A., & Küllmar, M. (2018). Renal biomarkers for the initiation of renal
replacement therapy—is this the future?. Journal of thoracic
disease, 10(Suppl 26), S3229.
Pianta, T. J., Endre, Z. H., Pickering, J. W., Buckley, N. A., & Peake, P. W. (2015). Kinetic
estimation of GFR improves prediction of dialysis and recovery after kidney
transplantation. PLoS One, 10(5), e0125669.
12
STUDY
Tamura, M. K., Vittinghoff, E., Yang, J., Go, A. S., Seliger, S. L., Kusek, J. W., ... & Ordonez, J.
(2016). Anemia and risk for cognitive decline in chronic kidney disease. BMC
nephrology, 17(1), 13.
Tumlin, J. A., Murugan, R., Deane, A. M., Ostermann, M., Busse, L. W., Ham, K. R., ... &
Finkel, K. W. (2018). Outcomes in patients with vasodilatory shock and renal
replacement therapy treated with intravenous angiotensin II. Critical care
medicine, 46(6), 949.
Whalen, K. (2015). Pharmacology: Lippincott illustrated reviews. Lippincott Williams &
Wilkins.
Xu, D., Murakoshi, N., Sairenchi, T., Irie, F., Igarashi, M., Nogami, A., ... & Ota, H. (2015).
Anemia and reduced kidney function as risk factors for new onset of atrial
fibrillation (from the Ibaraki prefectural health study). The American journal
of cardiology, 115(3), 328-333.
STUDY
Tamura, M. K., Vittinghoff, E., Yang, J., Go, A. S., Seliger, S. L., Kusek, J. W., ... & Ordonez, J.
(2016). Anemia and risk for cognitive decline in chronic kidney disease. BMC
nephrology, 17(1), 13.
Tumlin, J. A., Murugan, R., Deane, A. M., Ostermann, M., Busse, L. W., Ham, K. R., ... &
Finkel, K. W. (2018). Outcomes in patients with vasodilatory shock and renal
replacement therapy treated with intravenous angiotensin II. Critical care
medicine, 46(6), 949.
Whalen, K. (2015). Pharmacology: Lippincott illustrated reviews. Lippincott Williams &
Wilkins.
Xu, D., Murakoshi, N., Sairenchi, T., Irie, F., Igarashi, M., Nogami, A., ... & Ota, H. (2015).
Anemia and reduced kidney function as risk factors for new onset of atrial
fibrillation (from the Ibaraki prefectural health study). The American journal
of cardiology, 115(3), 328-333.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.