A Mobile Health Solution to Improve Surgery Outcome
VerifiedAdded on 2022/10/19
|27
|10242
|180
AI Summary
This research paper proposes a mobile health solution to improve surgery outcome by incorporating surgical methods and manual things involved in the surgery to get a clear information of the surgical treatment. The aim is to create and implement certain technological facilities that can help doctors and patients ease their communication which will ultimately result in an improved health outcome of the patients.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Ravina Paresh Kaniyawala
Auckland University of Technology
Supervisor: Dr. Roopak Sinha
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Ravina Paresh Kaniyawala
Auckland University of Technology
Supervisor: Dr. Roopak Sinha
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
1. Introduction:
The modern world has witnessed an enormous growth in technology and scientific advancement
through the implementation of several mobile applications and smart gadgets that made life
easier and more convenient. Information technology plays a significant role in improving patient
care and with its advancements, it is widely used in all sectors including health care
organizations to provide an accurate and right care to the patients, access patient’s necessary
information, keep record, make communication between physician and patient more convenient,
ensure transparency in medical charge, provide the patient information and enable them to keep
tract on themselves with the help of mobile application, thereby increasing the overall outcome
of the patient’ health and ensuring patient’s satisfaction (Bowles, Dykes & Demiris, 2015). It
falls under the responsibility of the healthcare providers to assist patients with quality care during
pre-surgery, in the course of surgery and also post-surgery and therefore, a detail survey needs to
be brought into effect that aims at improving patient’s life by giving them facilities to track their
activities after surgery and enable them to directly report to the doctor so that they can be
monitored very closely (Lu et al., 2018). The m-health solution should be designed in such a
way so as to incorporate the surgical methods and manual things involved in the surgery to get a
clear information of the surgical treatment. It should contain the devices used in the surgery like
heart measuring device, body sensor and other smart gadgets so that patient’s activity can be
monitored after the surgery (Semple & Armstrong, 2016). The aim and purpose of this research
paper is to propose, create and implement certain technological facilities that can help doctors
and patient ease their communication which will ultimately result in an improved health outcome
of the patients.
The three research questions for this project are provided below:
1. What are the primary requirements from relevant industry and medical standards involved in
effecting and monitoring surgery- related health plans?
2. How can a mHealth platform be architected to meet the primary requirements identified in
RQ1?
3. How can a prototype of the mHealth platform identified in RQ2, consisting of a mobile app
for patients and a web interface for clinicians, be built?
1. Introduction:
The modern world has witnessed an enormous growth in technology and scientific advancement
through the implementation of several mobile applications and smart gadgets that made life
easier and more convenient. Information technology plays a significant role in improving patient
care and with its advancements, it is widely used in all sectors including health care
organizations to provide an accurate and right care to the patients, access patient’s necessary
information, keep record, make communication between physician and patient more convenient,
ensure transparency in medical charge, provide the patient information and enable them to keep
tract on themselves with the help of mobile application, thereby increasing the overall outcome
of the patient’ health and ensuring patient’s satisfaction (Bowles, Dykes & Demiris, 2015). It
falls under the responsibility of the healthcare providers to assist patients with quality care during
pre-surgery, in the course of surgery and also post-surgery and therefore, a detail survey needs to
be brought into effect that aims at improving patient’s life by giving them facilities to track their
activities after surgery and enable them to directly report to the doctor so that they can be
monitored very closely (Lu et al., 2018). The m-health solution should be designed in such a
way so as to incorporate the surgical methods and manual things involved in the surgery to get a
clear information of the surgical treatment. It should contain the devices used in the surgery like
heart measuring device, body sensor and other smart gadgets so that patient’s activity can be
monitored after the surgery (Semple & Armstrong, 2016). The aim and purpose of this research
paper is to propose, create and implement certain technological facilities that can help doctors
and patient ease their communication which will ultimately result in an improved health outcome
of the patients.
The three research questions for this project are provided below:
1. What are the primary requirements from relevant industry and medical standards involved in
effecting and monitoring surgery- related health plans?
2. How can a mHealth platform be architected to meet the primary requirements identified in
RQ1?
3. How can a prototype of the mHealth platform identified in RQ2, consisting of a mobile app
for patients and a web interface for clinicians, be built?

A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
2. Background:
Smart devices has been established that has changed people’s lives and made everything more
convenient. Recent studies have shown the implementation of Information Technology in
healthcare sectors and their association with improving patient’s life and therefore increases the
patient’s overall satisfaction. Patient’s experience and satisfaction is considered to be an
important outcome in medical health care and it makes the central pillars of health care quality
(Lu et al., 2018). The satisfaction is associated with the treatment and care they receive from the
medical practitioners that influence their perception about quality care. Therefore, the usage of
mobile health applications has helped to improve the quality of healthcare and it has been proven
that through the installation of several facilities like reminders and diagnostic information into
the mobile application can promote the patient’s experience, satisfaction and health (Lu et al.,
2018). In surgical care, there is a growing drift towards reducing the amount of days staying in
the hospital and indulging patients into self-care. However, expedited discharge can lead to poor
outcome of the patients thereby increasing the health complications. Therefore, to address this
challenge, mobile applications has been discovered and developed to facilitate monitoring and
support discharge of the patients ensuring quality care (Semple & Armstrong, 2016).
2. Background:
Smart devices has been established that has changed people’s lives and made everything more
convenient. Recent studies have shown the implementation of Information Technology in
healthcare sectors and their association with improving patient’s life and therefore increases the
patient’s overall satisfaction. Patient’s experience and satisfaction is considered to be an
important outcome in medical health care and it makes the central pillars of health care quality
(Lu et al., 2018). The satisfaction is associated with the treatment and care they receive from the
medical practitioners that influence their perception about quality care. Therefore, the usage of
mobile health applications has helped to improve the quality of healthcare and it has been proven
that through the installation of several facilities like reminders and diagnostic information into
the mobile application can promote the patient’s experience, satisfaction and health (Lu et al.,
2018). In surgical care, there is a growing drift towards reducing the amount of days staying in
the hospital and indulging patients into self-care. However, expedited discharge can lead to poor
outcome of the patients thereby increasing the health complications. Therefore, to address this
challenge, mobile applications has been discovered and developed to facilitate monitoring and
support discharge of the patients ensuring quality care (Semple & Armstrong, 2016).
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
3. Literature Review
3.1 Method of Literature Review
The purpose of this literature review is to discuss every aspects of this Mobile Health
Information Management system through conducting a systematic review of various secondary
data resources such as Books, Articles, Published Reports and others. Most of the resources
reviewed for this research are collected from online databases such as NCBI dataase, Google
Scholars, Biomedcentral and others. Several keywords have been used to collect the relevant
literatures on this topic such as biomedical mobile application, medical informatics application,
surgery applications for mobile devices and mobile health application.
Database of Secondary
resources
Key words used for research Boolean functions for
research
NCBI dataase
Google Scholars
Biomedcentral
Researchgate
biomedical mobile
application
medical informatics
application
surgery applications for
mobile devices and mobile
health application
-
“”
NOT
AND
OR
Capital letters
3.2 Systematic Research
Also referred to as mHealth, mobile health is an umbrella term that refers to the use of mobile
devices in the practice of public health and medicine. The term is generally used for referring to
mobile phones, computers, tablets, and smart watches, and has emerged in recent years as a
major segment of electronic health. Mobile health has been found imperative in breaking down
the obstructions of distance for countryside New Zealanders, for more than 16 years and efforts
are currently being taken by the government to ensure that health professionals and patients
obtain fairness of ‘face-to-face’ communication and access to necessary healthcare services
(Mhurchu et al., 2014). This was in accordance to Perera (2018) who stated that notwithstanding
the obtainability numerous actuator and sensor devices intended to co-perform, few of them can
be integrated in smart homes. Their findings suggested that Internet of Things and ICT are
associated with a range of benefits, including low-cost and low-power devices that can be used
for developing a network that comprises of interconnected smart objects. It has also been stated
by Dowdeswell, Sinha and Haemmerle (2016) that cyber-physical systems are able to exert a
control over multifaceted physical components and processes, at the time of cooperating in the
form of distributed network agents. Furthermore, owing to the complexity and scale of
interactions that are associated with cyber-physical systems, it is difficult to maintain and
implement traceability policies that are precise and easy to accomplish.
3. Literature Review
3.1 Method of Literature Review
The purpose of this literature review is to discuss every aspects of this Mobile Health
Information Management system through conducting a systematic review of various secondary
data resources such as Books, Articles, Published Reports and others. Most of the resources
reviewed for this research are collected from online databases such as NCBI dataase, Google
Scholars, Biomedcentral and others. Several keywords have been used to collect the relevant
literatures on this topic such as biomedical mobile application, medical informatics application,
surgery applications for mobile devices and mobile health application.
Database of Secondary
resources
Key words used for research Boolean functions for
research
NCBI dataase
Google Scholars
Biomedcentral
Researchgate
biomedical mobile
application
medical informatics
application
surgery applications for
mobile devices and mobile
health application
-
“”
NOT
AND
OR
Capital letters
3.2 Systematic Research
Also referred to as mHealth, mobile health is an umbrella term that refers to the use of mobile
devices in the practice of public health and medicine. The term is generally used for referring to
mobile phones, computers, tablets, and smart watches, and has emerged in recent years as a
major segment of electronic health. Mobile health has been found imperative in breaking down
the obstructions of distance for countryside New Zealanders, for more than 16 years and efforts
are currently being taken by the government to ensure that health professionals and patients
obtain fairness of ‘face-to-face’ communication and access to necessary healthcare services
(Mhurchu et al., 2014). This was in accordance to Perera (2018) who stated that notwithstanding
the obtainability numerous actuator and sensor devices intended to co-perform, few of them can
be integrated in smart homes. Their findings suggested that Internet of Things and ICT are
associated with a range of benefits, including low-cost and low-power devices that can be used
for developing a network that comprises of interconnected smart objects. It has also been stated
by Dowdeswell, Sinha and Haemmerle (2016) that cyber-physical systems are able to exert a
control over multifaceted physical components and processes, at the time of cooperating in the
form of distributed network agents. Furthermore, owing to the complexity and scale of
interactions that are associated with cyber-physical systems, it is difficult to maintain and
implement traceability policies that are precise and easy to accomplish.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
According to Grissinger (2016) automatic alerts can deliver an actual means of disseminating
indispensable information about a patient and the intervention to clinicians who are entitled with
the responsibility of prescribing, dispensing, and administering the intended treatment regimen.
These alerts are envisioned to upkeep medical decisions about the efficacy and safety of
pharmaceutical therapies. In addition, the alerts are characteristically communicated through
different cautionary posts that arrive on the screen of mobile health devices. Furthermore, no or
minimal acknowledgment or action, in relation to the alert on mobile device is generally
obligatory on the part of the users to continue. It has been affirmed by Sanger et al. (2014) that
surgical site infections (SSI) that occur after discharge of patients from hospitals have been
identified as a major reason behind morbidity, expenditure and concern for the patients.
Nonetheless, perceptions amid patients about the barriers that they encounter, at the time of
seeking care, in relation to post-discharge SSI have not been measured adequately. The
researchers conducted surveys and semi-structured interviews and found that some of the major
challenges that act as impediment in management of post-discharge surgical wound
complications encompass lack of adequate knowledge for wound nursing, absence of self-
efficacy for wound management at home, and lack of available communication with healthcare
providers. The researchers further elaborated on the fact that mHealth wound monitoring
application was considered extremely acceptable by the patients, and pronounced its potential to
deliver more recurrent, thorough, and expedient follow-up for wound monitoring. In addition, the
mHealth wound monitoring application was also found to lower post-discharge anxiety, when
compared to the existing practice. However, some of the major concerns related to mHealth
wound monitoring were inaccessibility of device and absence of timely response from the
healthcare providers.
In the words of Gunter et al. (2016) surgical patients are progressively spending their time in the
usage of mHealth platforms, with the aim of monitoring wound recovery, while communicating
with the healthcare providers during post-discharge period. Notwithstanding the extensive
eagerness for mHealth, lack of studies on user experience made the researchers explore the
patient usability of an image-based mHealth software for post-operative wound monitoring. The
researchers found that mean time spent by patients in training session and application completion
was 4.7 (2.1-12.8) minutes and 5.0 (1.4-16.6) minutes, respectively. Besides high user
satisfaction of 83.3 out of 100, 55.5% patients independently completed the application, with
maximum difficulty encountered at the time of taking digital imageries of surgical wounds. The
findings therefore, suggested that using a smartphone application increased satisfaction among
patients, in relation to their wound monitoring.
It has been established by Armstrong, Coyte, Brown, Beber and Semple (2017) that patients who
are subjected to ambulatory surgery can often follow-up their care through the use of mobile
health application, in comparison to conventional and in-person visits after their surgeries. They
conducted a randomised trial among 65 patients and found that patients who used the mobile
According to Grissinger (2016) automatic alerts can deliver an actual means of disseminating
indispensable information about a patient and the intervention to clinicians who are entitled with
the responsibility of prescribing, dispensing, and administering the intended treatment regimen.
These alerts are envisioned to upkeep medical decisions about the efficacy and safety of
pharmaceutical therapies. In addition, the alerts are characteristically communicated through
different cautionary posts that arrive on the screen of mobile health devices. Furthermore, no or
minimal acknowledgment or action, in relation to the alert on mobile device is generally
obligatory on the part of the users to continue. It has been affirmed by Sanger et al. (2014) that
surgical site infections (SSI) that occur after discharge of patients from hospitals have been
identified as a major reason behind morbidity, expenditure and concern for the patients.
Nonetheless, perceptions amid patients about the barriers that they encounter, at the time of
seeking care, in relation to post-discharge SSI have not been measured adequately. The
researchers conducted surveys and semi-structured interviews and found that some of the major
challenges that act as impediment in management of post-discharge surgical wound
complications encompass lack of adequate knowledge for wound nursing, absence of self-
efficacy for wound management at home, and lack of available communication with healthcare
providers. The researchers further elaborated on the fact that mHealth wound monitoring
application was considered extremely acceptable by the patients, and pronounced its potential to
deliver more recurrent, thorough, and expedient follow-up for wound monitoring. In addition, the
mHealth wound monitoring application was also found to lower post-discharge anxiety, when
compared to the existing practice. However, some of the major concerns related to mHealth
wound monitoring were inaccessibility of device and absence of timely response from the
healthcare providers.
In the words of Gunter et al. (2016) surgical patients are progressively spending their time in the
usage of mHealth platforms, with the aim of monitoring wound recovery, while communicating
with the healthcare providers during post-discharge period. Notwithstanding the extensive
eagerness for mHealth, lack of studies on user experience made the researchers explore the
patient usability of an image-based mHealth software for post-operative wound monitoring. The
researchers found that mean time spent by patients in training session and application completion
was 4.7 (2.1-12.8) minutes and 5.0 (1.4-16.6) minutes, respectively. Besides high user
satisfaction of 83.3 out of 100, 55.5% patients independently completed the application, with
maximum difficulty encountered at the time of taking digital imageries of surgical wounds. The
findings therefore, suggested that using a smartphone application increased satisfaction among
patients, in relation to their wound monitoring.
It has been established by Armstrong, Coyte, Brown, Beber and Semple (2017) that patients who
are subjected to ambulatory surgery can often follow-up their care through the use of mobile
health application, in comparison to conventional and in-person visits after their surgeries. They
conducted a randomised trial among 65 patients and found that patients who used the mobile
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
application were able to attend 0.66 in-person visits, in comparison 1.64 in-person visits that
were found among patients who attended in-person follow-up care regimen. In addition, patients
who used the mHealth application were found to send more emails to health care professionals
during the first 30 days following the surgery (mean, 0.65 vs 0.15; incidence rate ratio, 4.13;
95% CI, 1.55-10.99; P = .005), when compared in-person patient follow-up group. The benefits
of mHealth outcomes were also demonstrated by Symer, Abelson, Milsom, McClure and Yeo
(2017) who conducted a pilot study of a novel mHealth application among patients who were
subjected to major abdominal surgery. The researchers conducted the study amid 31 patients and
found that an estimated 83.9% patients were able to complete an application-associated task, for
minimum 70% of the time. Furthermore, 89% patients suggested that the mHealth application
was considerably easy to monitor health outcomes. Besides, 1.1 alerts were generated on an
average by the patients, and most often the patients were able to complete the single-item
photoaffective meter. This findings also suggested that use of mHealth application demonstrated
the potential to improve health outcomes among patients who underwent abdominal surgery.
It has also been suggested by Jaensson, Dahlberg and Nilsson (2018) females often display an
increased likelihood of manifesting poor recovery after anaesthesia, when compared to males.
The findings suggested that females aged less than 45 years reported suggestively high global
scores, in relation to SwQoR questionnaire, concomitant with poor recovery during 1-10 post-
operative days, when compared to females aged more than 45 years or older (P=.001 to P=.008).
In contrast, males aged less than 45 years demonstrated high scores during 2-6 postoperative
days, in comparison to those aged more (P=.001 to P=.006). Thus, the research findings
provided evidence for sex resemblances in postoperative recovery amid male and female patients
who were subjected to mHealth follow-up.
Wang et al. (2018) also confirmed the above findings by conducting a randomised controlled
trial to determine the impacts of a mobile healthcare application on the health outcomes of
patients who had been discharged after a stoma. The researchers found that stoma self‐efficacy
score and psychosocial adjustment amid patients who were subjected to home care through a
mobile application were meaningfully greater than the control group during follow‐up
(p < 0.05). Furthermore, the results also indicated that stoma complications reduced amid
patients who used the mobile application. This in turn provided evidence for the fact that home
care mobile application acts in the form of an effective intervention, for supporting the self-
efficacy and emotional adjustment of stoma patients, following their discharge. In other words,
mHealth applications help in ensuring continuity of care, in addition to delivering guidance to
the patients in a timely manner. DeAntonio et al. (2019) also presented findings that are in
accordance to those presented above. The researchers tried to explore the application of a
handheld telemedicine (TM) device amid pediatric surgical patients and found that there were no
differences to the TM care plan, after missed diagnoses, “in person” evaluations, additional
clinic visits, or visits to the emergency department among those who had been subjected to only
application were able to attend 0.66 in-person visits, in comparison 1.64 in-person visits that
were found among patients who attended in-person follow-up care regimen. In addition, patients
who used the mHealth application were found to send more emails to health care professionals
during the first 30 days following the surgery (mean, 0.65 vs 0.15; incidence rate ratio, 4.13;
95% CI, 1.55-10.99; P = .005), when compared in-person patient follow-up group. The benefits
of mHealth outcomes were also demonstrated by Symer, Abelson, Milsom, McClure and Yeo
(2017) who conducted a pilot study of a novel mHealth application among patients who were
subjected to major abdominal surgery. The researchers conducted the study amid 31 patients and
found that an estimated 83.9% patients were able to complete an application-associated task, for
minimum 70% of the time. Furthermore, 89% patients suggested that the mHealth application
was considerably easy to monitor health outcomes. Besides, 1.1 alerts were generated on an
average by the patients, and most often the patients were able to complete the single-item
photoaffective meter. This findings also suggested that use of mHealth application demonstrated
the potential to improve health outcomes among patients who underwent abdominal surgery.
It has also been suggested by Jaensson, Dahlberg and Nilsson (2018) females often display an
increased likelihood of manifesting poor recovery after anaesthesia, when compared to males.
The findings suggested that females aged less than 45 years reported suggestively high global
scores, in relation to SwQoR questionnaire, concomitant with poor recovery during 1-10 post-
operative days, when compared to females aged more than 45 years or older (P=.001 to P=.008).
In contrast, males aged less than 45 years demonstrated high scores during 2-6 postoperative
days, in comparison to those aged more (P=.001 to P=.006). Thus, the research findings
provided evidence for sex resemblances in postoperative recovery amid male and female patients
who were subjected to mHealth follow-up.
Wang et al. (2018) also confirmed the above findings by conducting a randomised controlled
trial to determine the impacts of a mobile healthcare application on the health outcomes of
patients who had been discharged after a stoma. The researchers found that stoma self‐efficacy
score and psychosocial adjustment amid patients who were subjected to home care through a
mobile application were meaningfully greater than the control group during follow‐up
(p < 0.05). Furthermore, the results also indicated that stoma complications reduced amid
patients who used the mobile application. This in turn provided evidence for the fact that home
care mobile application acts in the form of an effective intervention, for supporting the self-
efficacy and emotional adjustment of stoma patients, following their discharge. In other words,
mHealth applications help in ensuring continuity of care, in addition to delivering guidance to
the patients in a timely manner. DeAntonio et al. (2019) also presented findings that are in
accordance to those presented above. The researchers tried to explore the application of a
handheld telemedicine (TM) device amid pediatric surgical patients and found that there were no
differences to the TM care plan, after missed diagnoses, “in person” evaluations, additional
clinic visits, or visits to the emergency department among those who had been subjected to only
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
TM postoperative evaluations. However, most of the patients reported extreme satisfaction and
92% caregivers stated that they felt contented with TM-only post-operative assessment. These
data also indicated that use of TM among post-operative patients was effective and safe.
It has also been postulated by Slade Shantz and Veillette (2014) that mass production and
miniaturization of countless sensors have made conceivable the incorporation of output and
sensor applications in wearable platforms. Notwithstanding the customer emphasis of wearable
insurgency, particular surgical applications are being established in recent years that are
categorised as namely, assistive, augmentative, and assessment functions. Furthermore, the
researchers also state that use of augmentative and assistive mHealth technology will facilitate
enhanced communication between healthcare providers and patients, in addition to improving
clinical decision making related done by surgeons.
3.2.1 Literature review on previously made mHealth solution
a) monitoring the symptoms and sending alerts
There are certain ways in which the post-surgery patients’ symptoms are being monitored. SMS
and using the mHealth application were the most common ways for doing this. As suggested in
study by (Cleeland et al., 2011; Carrier et al., 2016; Debono et al., 2019; DeVito Dabbs et al.,
2016; Semple et al., 2015) the most monitored symptoms are temperature and pain. But even the
other symptoms monitored in these studies were nausea, dizziness, any shortness of breath,
constipation, weight, blood pressure output.
Four after surgery patient care monitoring system (Cleeland et al., 2011; Carrier et al., 2016;
DeVito Dabbs et al., 2016; Semple et al., 2015) sends some alerts to the clinic depending on the
patient response to application. If in any case some symptoms are not normal the medical teams
or the doctors will immediately response to such things.
In paper, (Semple et al., 2015) patient has been monitored and survey is being done in which
patient were asked to send some daily images of their recovery or wound after surgery so that
medical team can track the patient’s progress. The pictures send by patients seems to be normal
to the surgeon and then they cancel their follow up visit with the doctor.
One of the application had been developed by (Debono et al. -23) which could help in generating
the response from the doctors. The patients were supposed to push alarm of either green, orange
or red alarm depending on their emergency level of symptom (which can be pain, fever etc. )
During the survey it had been found that total of 31.7% of patient pressed either orange or red
alarm which require response and out of which 18 to some 19 patient who generated the alarm
for orange or red code, their response had been solved over just a call and not needed any
consultation.
Similarly, one another application by (Cleeland et al. -10) in which the alerts had been sent to
respected clinics in some of event like pain, breathing problem, less heart rating etc using some
pre-determined evaluation criteria.
TM postoperative evaluations. However, most of the patients reported extreme satisfaction and
92% caregivers stated that they felt contented with TM-only post-operative assessment. These
data also indicated that use of TM among post-operative patients was effective and safe.
It has also been postulated by Slade Shantz and Veillette (2014) that mass production and
miniaturization of countless sensors have made conceivable the incorporation of output and
sensor applications in wearable platforms. Notwithstanding the customer emphasis of wearable
insurgency, particular surgical applications are being established in recent years that are
categorised as namely, assistive, augmentative, and assessment functions. Furthermore, the
researchers also state that use of augmentative and assistive mHealth technology will facilitate
enhanced communication between healthcare providers and patients, in addition to improving
clinical decision making related done by surgeons.
3.2.1 Literature review on previously made mHealth solution
a) monitoring the symptoms and sending alerts
There are certain ways in which the post-surgery patients’ symptoms are being monitored. SMS
and using the mHealth application were the most common ways for doing this. As suggested in
study by (Cleeland et al., 2011; Carrier et al., 2016; Debono et al., 2019; DeVito Dabbs et al.,
2016; Semple et al., 2015) the most monitored symptoms are temperature and pain. But even the
other symptoms monitored in these studies were nausea, dizziness, any shortness of breath,
constipation, weight, blood pressure output.
Four after surgery patient care monitoring system (Cleeland et al., 2011; Carrier et al., 2016;
DeVito Dabbs et al., 2016; Semple et al., 2015) sends some alerts to the clinic depending on the
patient response to application. If in any case some symptoms are not normal the medical teams
or the doctors will immediately response to such things.
In paper, (Semple et al., 2015) patient has been monitored and survey is being done in which
patient were asked to send some daily images of their recovery or wound after surgery so that
medical team can track the patient’s progress. The pictures send by patients seems to be normal
to the surgeon and then they cancel their follow up visit with the doctor.
One of the application had been developed by (Debono et al. -23) which could help in generating
the response from the doctors. The patients were supposed to push alarm of either green, orange
or red alarm depending on their emergency level of symptom (which can be pain, fever etc. )
During the survey it had been found that total of 31.7% of patient pressed either orange or red
alarm which require response and out of which 18 to some 19 patient who generated the alarm
for orange or red code, their response had been solved over just a call and not needed any
consultation.
Similarly, one another application by (Cleeland et al. -10) in which the alerts had been sent to
respected clinics in some of event like pain, breathing problem, less heart rating etc using some
pre-determined evaluation criteria.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
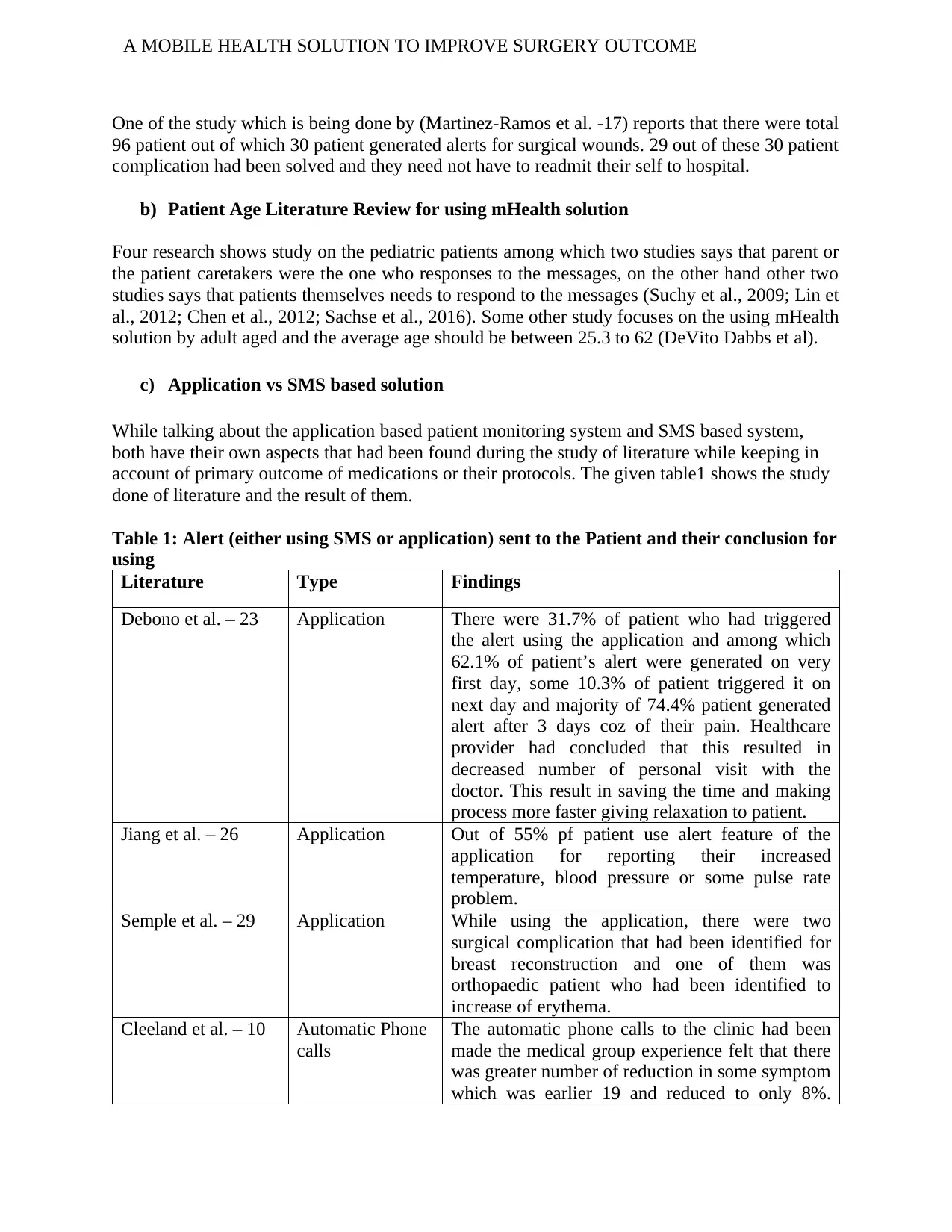
One of the study which is being done by (Martinez-Ramos et al. -17) reports that there were total
96 patient out of which 30 patient generated alerts for surgical wounds. 29 out of these 30 patient
complication had been solved and they need not have to readmit their self to hospital.
b) Patient Age Literature Review for using mHealth solution
Four research shows study on the pediatric patients among which two studies says that parent or
the patient caretakers were the one who responses to the messages, on the other hand other two
studies says that patients themselves needs to respond to the messages (Suchy et al., 2009; Lin et
al., 2012; Chen et al., 2012; Sachse et al., 2016). Some other study focuses on the using mHealth
solution by adult aged and the average age should be between 25.3 to 62 (DeVito Dabbs et al).
c) Application vs SMS based solution
While talking about the application based patient monitoring system and SMS based system,
both have their own aspects that had been found during the study of literature while keeping in
account of primary outcome of medications or their protocols. The given table1 shows the study
done of literature and the result of them.
Table 1: Alert (either using SMS or application) sent to the Patient and their conclusion for
using
Literature Type Findings
Debono et al. – 23 Application There were 31.7% of patient who had triggered
the alert using the application and among which
62.1% of patient’s alert were generated on very
first day, some 10.3% of patient triggered it on
next day and majority of 74.4% patient generated
alert after 3 days coz of their pain. Healthcare
provider had concluded that this resulted in
decreased number of personal visit with the
doctor. This result in saving the time and making
process more faster giving relaxation to patient.
Jiang et al. – 26 Application Out of 55% pf patient use alert feature of the
application for reporting their increased
temperature, blood pressure or some pulse rate
problem.
Semple et al. – 29 Application While using the application, there were two
surgical complication that had been identified for
breast reconstruction and one of them was
orthopaedic patient who had been identified to
increase of erythema.
Cleeland et al. – 10 Automatic Phone
calls
The automatic phone calls to the clinic had been
made the medical group experience felt that there
was greater number of reduction in some symptom
which was earlier 19 and reduced to only 8%.
One of the study which is being done by (Martinez-Ramos et al. -17) reports that there were total
96 patient out of which 30 patient generated alerts for surgical wounds. 29 out of these 30 patient
complication had been solved and they need not have to readmit their self to hospital.
b) Patient Age Literature Review for using mHealth solution
Four research shows study on the pediatric patients among which two studies says that parent or
the patient caretakers were the one who responses to the messages, on the other hand other two
studies says that patients themselves needs to respond to the messages (Suchy et al., 2009; Lin et
al., 2012; Chen et al., 2012; Sachse et al., 2016). Some other study focuses on the using mHealth
solution by adult aged and the average age should be between 25.3 to 62 (DeVito Dabbs et al).
c) Application vs SMS based solution
While talking about the application based patient monitoring system and SMS based system,
both have their own aspects that had been found during the study of literature while keeping in
account of primary outcome of medications or their protocols. The given table1 shows the study
done of literature and the result of them.
Table 1: Alert (either using SMS or application) sent to the Patient and their conclusion for
using
Literature Type Findings
Debono et al. – 23 Application There were 31.7% of patient who had triggered
the alert using the application and among which
62.1% of patient’s alert were generated on very
first day, some 10.3% of patient triggered it on
next day and majority of 74.4% patient generated
alert after 3 days coz of their pain. Healthcare
provider had concluded that this resulted in
decreased number of personal visit with the
doctor. This result in saving the time and making
process more faster giving relaxation to patient.
Jiang et al. – 26 Application Out of 55% pf patient use alert feature of the
application for reporting their increased
temperature, blood pressure or some pulse rate
problem.
Semple et al. – 29 Application While using the application, there were two
surgical complication that had been identified for
breast reconstruction and one of them was
orthopaedic patient who had been identified to
increase of erythema.
Cleeland et al. – 10 Automatic Phone
calls
The automatic phone calls to the clinic had been
made the medical group experience felt that there
was greater number of reduction in some symptom
which was earlier 19 and reduced to only 8%.
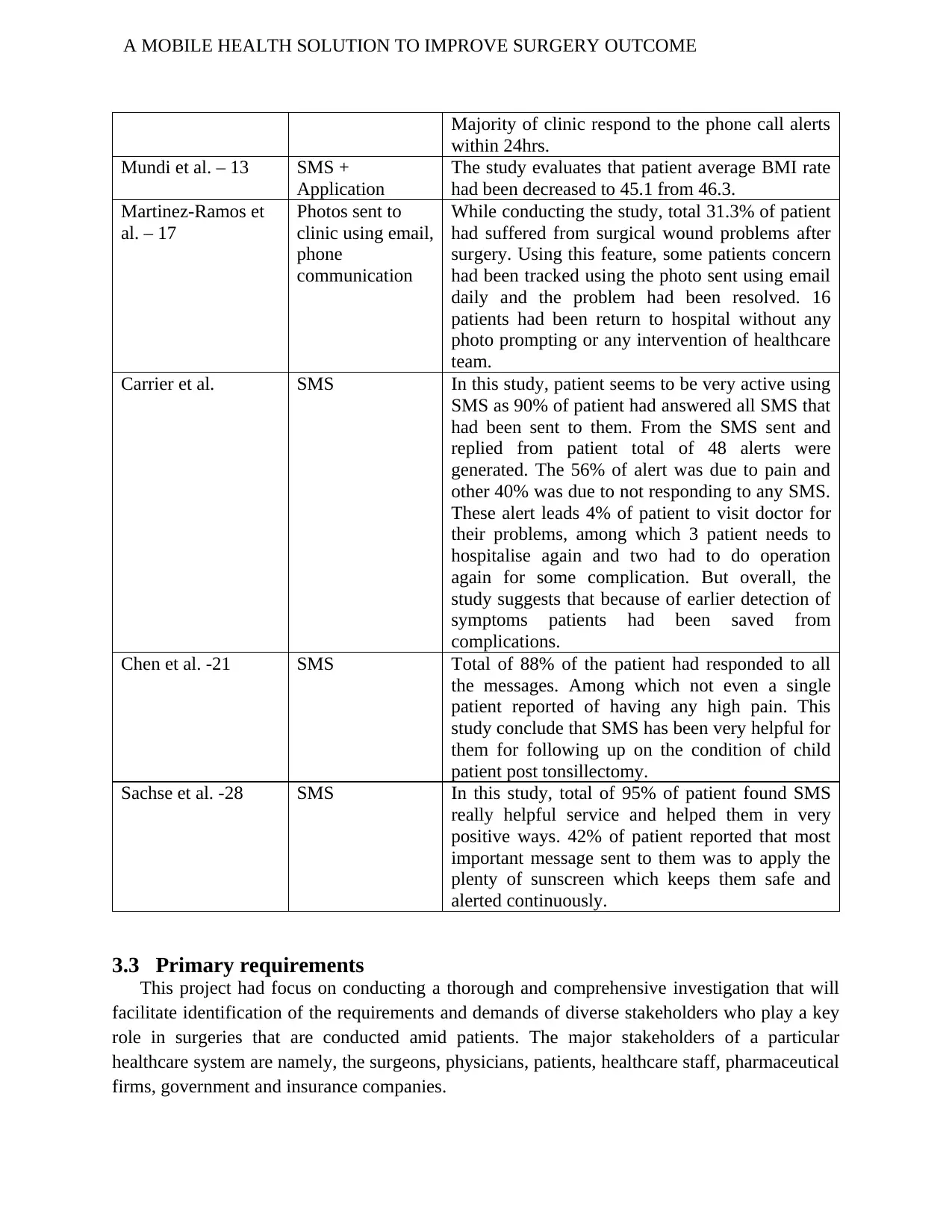
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Majority of clinic respond to the phone call alerts
within 24hrs.
Mundi et al. – 13 SMS +
Application
The study evaluates that patient average BMI rate
had been decreased to 45.1 from 46.3.
Martinez-Ramos et
al. – 17
Photos sent to
clinic using email,
phone
communication
While conducting the study, total 31.3% of patient
had suffered from surgical wound problems after
surgery. Using this feature, some patients concern
had been tracked using the photo sent using email
daily and the problem had been resolved. 16
patients had been return to hospital without any
photo prompting or any intervention of healthcare
team.
Carrier et al. SMS In this study, patient seems to be very active using
SMS as 90% of patient had answered all SMS that
had been sent to them. From the SMS sent and
replied from patient total of 48 alerts were
generated. The 56% of alert was due to pain and
other 40% was due to not responding to any SMS.
These alert leads 4% of patient to visit doctor for
their problems, among which 3 patient needs to
hospitalise again and two had to do operation
again for some complication. But overall, the
study suggests that because of earlier detection of
symptoms patients had been saved from
complications.
Chen et al. -21 SMS Total of 88% of the patient had responded to all
the messages. Among which not even a single
patient reported of having any high pain. This
study conclude that SMS has been very helpful for
them for following up on the condition of child
patient post tonsillectomy.
Sachse et al. -28 SMS In this study, total of 95% of patient found SMS
really helpful service and helped them in very
positive ways. 42% of patient reported that most
important message sent to them was to apply the
plenty of sunscreen which keeps them safe and
alerted continuously.
3.3 Primary requirements
This project had focus on conducting a thorough and comprehensive investigation that will
facilitate identification of the requirements and demands of diverse stakeholders who play a key
role in surgeries that are conducted amid patients. The major stakeholders of a particular
healthcare system are namely, the surgeons, physicians, patients, healthcare staff, pharmaceutical
firms, government and insurance companies.
Majority of clinic respond to the phone call alerts
within 24hrs.
Mundi et al. – 13 SMS +
Application
The study evaluates that patient average BMI rate
had been decreased to 45.1 from 46.3.
Martinez-Ramos et
al. – 17
Photos sent to
clinic using email,
phone
communication
While conducting the study, total 31.3% of patient
had suffered from surgical wound problems after
surgery. Using this feature, some patients concern
had been tracked using the photo sent using email
daily and the problem had been resolved. 16
patients had been return to hospital without any
photo prompting or any intervention of healthcare
team.
Carrier et al. SMS In this study, patient seems to be very active using
SMS as 90% of patient had answered all SMS that
had been sent to them. From the SMS sent and
replied from patient total of 48 alerts were
generated. The 56% of alert was due to pain and
other 40% was due to not responding to any SMS.
These alert leads 4% of patient to visit doctor for
their problems, among which 3 patient needs to
hospitalise again and two had to do operation
again for some complication. But overall, the
study suggests that because of earlier detection of
symptoms patients had been saved from
complications.
Chen et al. -21 SMS Total of 88% of the patient had responded to all
the messages. Among which not even a single
patient reported of having any high pain. This
study conclude that SMS has been very helpful for
them for following up on the condition of child
patient post tonsillectomy.
Sachse et al. -28 SMS In this study, total of 95% of patient found SMS
really helpful service and helped them in very
positive ways. 42% of patient reported that most
important message sent to them was to apply the
plenty of sunscreen which keeps them safe and
alerted continuously.
3.3 Primary requirements
This project had focus on conducting a thorough and comprehensive investigation that will
facilitate identification of the requirements and demands of diverse stakeholders who play a key
role in surgeries that are conducted amid patients. The major stakeholders of a particular
healthcare system are namely, the surgeons, physicians, patients, healthcare staff, pharmaceutical
firms, government and insurance companies.
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Hence, determining the role requirements of the stakeholders will provide an insight about
their expectations, in relation to surgical health outcomes of patients. In addition, the review will
also try to determine the manual and traditional approaches that are currently associated while
delivering optimal care services to patients undergoing surgeries. The prospect of mHealth
market is anticipated to grow in the coming decade, in addition to the fact that several
applications have already gained attention that focus on remote health monitoring of patients.
The review will also place due emphasis on analysing the strategies that can be adopted for
enhancing life of the patients, by providing them the opportunity to access technological
facilities, with the aim of helping them track their health status, following a surgery.
The project will also encompass presentation of a system architecture for demonstrating the
required needs of the stakeholder. This will be accomplished by development of a prototype of
mHealth system that will comprise of devices commonly used in surgery such as, heart
measuring device and body sensor. Implementation of this system architecture will ease
communication of patients with healthcare professionals, and demonstrate the efficacy of
mHealth platform for enhancing surgical outcomes.
From the detailed literature review in the previous section, we can identify our primary
requirements to make some prototype of system which will give additional facility and one roof
to make bridge for making communication possible between doctor and patient. To Conduct this
project of developing a mobile application for integrated surgical care the primary requirements
are:
Identifying the complicacies among patient of surgical department
Understanding the process of surgical treatments and interventions
Understanding the types of communication required among caregivers, doctors and
facilitators in surgical treatments
Conceptual operation of the application and their communication networks
Findings of equipment purchasing and software subscription
Final application coding, debugging and testing platform
Primary requirements for Application:
SMS alert for reporting to patient about their conditions
Emergency click notification system for both patient and doctor
Patient regular reports uploading using application to replace sending emails to doctor
Before surgery tips by doctor to follow for patient integrated in the application so patient
can keep themselves updated.
Checklist of activity done so, both patient and doctor can track them and do the analysis.
Monitoring patient’s heartrate and reporting after surgery to check the conditions.
Hence, determining the role requirements of the stakeholders will provide an insight about
their expectations, in relation to surgical health outcomes of patients. In addition, the review will
also try to determine the manual and traditional approaches that are currently associated while
delivering optimal care services to patients undergoing surgeries. The prospect of mHealth
market is anticipated to grow in the coming decade, in addition to the fact that several
applications have already gained attention that focus on remote health monitoring of patients.
The review will also place due emphasis on analysing the strategies that can be adopted for
enhancing life of the patients, by providing them the opportunity to access technological
facilities, with the aim of helping them track their health status, following a surgery.
The project will also encompass presentation of a system architecture for demonstrating the
required needs of the stakeholder. This will be accomplished by development of a prototype of
mHealth system that will comprise of devices commonly used in surgery such as, heart
measuring device and body sensor. Implementation of this system architecture will ease
communication of patients with healthcare professionals, and demonstrate the efficacy of
mHealth platform for enhancing surgical outcomes.
From the detailed literature review in the previous section, we can identify our primary
requirements to make some prototype of system which will give additional facility and one roof
to make bridge for making communication possible between doctor and patient. To Conduct this
project of developing a mobile application for integrated surgical care the primary requirements
are:
Identifying the complicacies among patient of surgical department
Understanding the process of surgical treatments and interventions
Understanding the types of communication required among caregivers, doctors and
facilitators in surgical treatments
Conceptual operation of the application and their communication networks
Findings of equipment purchasing and software subscription
Final application coding, debugging and testing platform
Primary requirements for Application:
SMS alert for reporting to patient about their conditions
Emergency click notification system for both patient and doctor
Patient regular reports uploading using application to replace sending emails to doctor
Before surgery tips by doctor to follow for patient integrated in the application so patient
can keep themselves updated.
Checklist of activity done so, both patient and doctor can track them and do the analysis.
Monitoring patient’s heartrate and reporting after surgery to check the conditions.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
4. Methodology
4.1 Selection of Methodology
Design science approach focuses on the expansion and presentation of artifacts, in addition to the
obvious purpose of refining the practical application of the artifact. mHealth technology
comprises of adaptable and mutable software, hardware, and human interfaces. In other words,
use of mHealth application provides several exclusive and thought-provoking design difficulties
that call for novel and original ideas. Furthermore, use of design science approach has been
found extremely pertinent to mHealth investigation, owing to the fact that it is based on the
development of innovative artifacts for solving real-world problems (Cronholm & Göbel, 2016).
This project was guided by the Information System Research (ISR) Framework that is based on
design science approach for informing growth and expansion of information system.
Incorporation of this system involved iteratively repeating the design and development cycle, till
an anticipated final artefact had been achieved.
4.1.1 First Cycle
Through the usage of the ISR Framework, three research cycles had been employed. The first
cycle referred to as the relevance cycle encompassed conducting an investigation to comprehend
the situation of the patients (end-users) by exploring their necessities through a sequence of
interactions such as, focus groups (Schnall, Rojas, Travers, Brown III & Bakken, 2014). For this
stage, literature review of the paper in which the feedback of users had been taken for healthcare
application features will be done for identifying the anticipated features, content, and function of
mHealth application.
On conducting a thematic analysis of the literature review of what user seeks in the application
and their responses, four major functional requirements were identified namely, (i) managing
medications, (ii) monitoring wound, (iii) easy communication with providers, and (iv) faster
recovery. The providers and patients also suggested that some of the functionalities and tools that
must be included in the mHealth application are notes, reminders/alerts, testimonials of lived
experiences, chat boxes/forums, games/virtual rewards, and personal outreach.
4.1.2 Second Cycle
The second phase involved the rigour cycle where a comprehensive assessment of artefacts and
theories underwrote design science and presentation realm knowledge base. This encompassed
conducting a systematic review of already existing studies (SLR), published in English, on or
after 2010 that were based on the implementation of mobile health applications for follow-up
care after surgical treatment.
4. Methodology
4.1 Selection of Methodology
Design science approach focuses on the expansion and presentation of artifacts, in addition to the
obvious purpose of refining the practical application of the artifact. mHealth technology
comprises of adaptable and mutable software, hardware, and human interfaces. In other words,
use of mHealth application provides several exclusive and thought-provoking design difficulties
that call for novel and original ideas. Furthermore, use of design science approach has been
found extremely pertinent to mHealth investigation, owing to the fact that it is based on the
development of innovative artifacts for solving real-world problems (Cronholm & Göbel, 2016).
This project was guided by the Information System Research (ISR) Framework that is based on
design science approach for informing growth and expansion of information system.
Incorporation of this system involved iteratively repeating the design and development cycle, till
an anticipated final artefact had been achieved.
4.1.1 First Cycle
Through the usage of the ISR Framework, three research cycles had been employed. The first
cycle referred to as the relevance cycle encompassed conducting an investigation to comprehend
the situation of the patients (end-users) by exploring their necessities through a sequence of
interactions such as, focus groups (Schnall, Rojas, Travers, Brown III & Bakken, 2014). For this
stage, literature review of the paper in which the feedback of users had been taken for healthcare
application features will be done for identifying the anticipated features, content, and function of
mHealth application.
On conducting a thematic analysis of the literature review of what user seeks in the application
and their responses, four major functional requirements were identified namely, (i) managing
medications, (ii) monitoring wound, (iii) easy communication with providers, and (iv) faster
recovery. The providers and patients also suggested that some of the functionalities and tools that
must be included in the mHealth application are notes, reminders/alerts, testimonials of lived
experiences, chat boxes/forums, games/virtual rewards, and personal outreach.
4.1.2 Second Cycle
The second phase involved the rigour cycle where a comprehensive assessment of artefacts and
theories underwrote design science and presentation realm knowledge base. This encompassed
conducting a systematic review of already existing studies (SLR), published in English, on or
after 2010 that were based on the implementation of mobile health applications for follow-up
care after surgical treatment.
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
4.1.3 Third Cycle – Design Cycle
The design cycle was the third phase, which was conducted with the primary objective of
enhancing the design and increased probability of technology acceptance. With the aim of
accomplishing objectives of this particular cycle, findings obtained from the previous parts of the
research were incorporated (Gorini et al., 2018). These comprised of a list of features, content,
and functions as deciphered from the focus groups, together with findings obtained from the
literature review.
An user-centered dispersed information design approach and participating action investigation
method for formulating the user-centered session activities. Two design sessions were
conducted, with each consecutive design sitting being established based on the evidence
collected from the preceding design session. The objective of the first session was to recognise
optimal features for enhancing surgical outcome needs of patients (Schnall, Rojas, Travers,
Brown III & Bakken, 2014). The patients discussed several topics and did not seek help from
existing mHealth prototypes or applications. The patients were asked to envisage the broad
categories, in the form of a distinct screen on mobile application. The themes obtained from
focus group were presented, followed by asking the participants the aspects that were related to
functionality of mHealth application. The second design session involved helping the
stakeholders sketch an interface for the anticipated mHealth application, This helped in
determining the preferences of the participants about mHealth application that can help improve
their surgical health outcomes.
5. System Architecture
This chapter shows the detail of system architecture for mHealth application. The first part of
this section will explain about the details of requirements, constraints, quality attributes, drivers
etc. For the use of system architecture the ADD process is being followed for which the template
suggested by (Clements et al., 2002) will be used. The usage of ADD template demonstrate
identifying the drivers for architecture, definition and proper documentation for the different
views for mHealth solution. Different views given in this chapter will demonstrate how it had
helped in the initial stages of creation of system architecture. ADD (Attribute Driven Design)
method make sure that the drivers and attribute define for the system will be matched at the end.
This process is followed to rectify that specification of prototype meets the project requirements.
5.1 Attribute Driven Design Methodology (ADD)
Write about the ADD process by giving some paper reference (one paragraph)
4.1.3 Third Cycle – Design Cycle
The design cycle was the third phase, which was conducted with the primary objective of
enhancing the design and increased probability of technology acceptance. With the aim of
accomplishing objectives of this particular cycle, findings obtained from the previous parts of the
research were incorporated (Gorini et al., 2018). These comprised of a list of features, content,
and functions as deciphered from the focus groups, together with findings obtained from the
literature review.
An user-centered dispersed information design approach and participating action investigation
method for formulating the user-centered session activities. Two design sessions were
conducted, with each consecutive design sitting being established based on the evidence
collected from the preceding design session. The objective of the first session was to recognise
optimal features for enhancing surgical outcome needs of patients (Schnall, Rojas, Travers,
Brown III & Bakken, 2014). The patients discussed several topics and did not seek help from
existing mHealth prototypes or applications. The patients were asked to envisage the broad
categories, in the form of a distinct screen on mobile application. The themes obtained from
focus group were presented, followed by asking the participants the aspects that were related to
functionality of mHealth application. The second design session involved helping the
stakeholders sketch an interface for the anticipated mHealth application, This helped in
determining the preferences of the participants about mHealth application that can help improve
their surgical health outcomes.
5. System Architecture
This chapter shows the detail of system architecture for mHealth application. The first part of
this section will explain about the details of requirements, constraints, quality attributes, drivers
etc. For the use of system architecture the ADD process is being followed for which the template
suggested by (Clements et al., 2002) will be used. The usage of ADD template demonstrate
identifying the drivers for architecture, definition and proper documentation for the different
views for mHealth solution. Different views given in this chapter will demonstrate how it had
helped in the initial stages of creation of system architecture. ADD (Attribute Driven Design)
method make sure that the drivers and attribute define for the system will be matched at the end.
This process is followed to rectify that specification of prototype meets the project requirements.
5.1 Attribute Driven Design Methodology (ADD)
Write about the ADD process by giving some paper reference (one paragraph)
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Attribute Design Methodology suggested by the Software Engineering Institute (SEI) is known
as a deliberate philosophy pursued bit by bit so as to plan the product engineering of a software
extended framework. (Dixon, 2016) This methodology mainly focus around defining the product
design, the mhealth framework is dependent on the structures' quality characteristic prerequisites.
This strategy involves different advances, they include: recognize candidate architectural drivers,
choose a design concept that satisfies the architectural drivers, guarantee to give strategies to
accomplish quality prerequisites and produce a total programming engineering for the apparatus
which tends to all the compositional drivers.
Inaddition, the above advances, ADD is a three-advance procedure which includes info,
procedure and yield stages and this phrasing will be taken in to work on during the structure of
the product engineering of the proposed Activity Diagram to the mhealth development
procedures. The software architecture and configuration procedure is as demonstrated in the
design process
Identification of architectural driver
The input requirements to ADD includes the primary functional requirements, quality attribute
requirements and the constraints. Functional requirements for this project will be explained by
use of the use cases which is considered with architecture in the mHealth architecture. The
quality credit prioritization going before the framework being fabricated is upheld by the Quality
Attribute Workshop (QAW) which is likewise endorsed by the SEI. Finally, business and
specific goals are managed by outside components.
5.1.1 Architecture Driver
This section clarifies the development of the mhealth application program. This section
additionally identifies and subtleties the highlights of the application. The engineering structure
format proposed by is pursued for the remainder of the section. The act of this format bolsters the
identification of design drivers, definition, and documentation of views and viewpoints of
mhealth application software and how different perspectives utilized backings the
accomplishment of various compositional drivers identified during the underlying phases of this
section. In addition the structure of the design of the instrument, this section subtleties different
other relative terms, for example, model, displaying, meta model, meta-demonstrating and
changes that are utilized to plan the apparatus. This section rehearses the Attribute-Driven
Design (ADD) technique to define the product engineering of the apparatus which uses the
recently referenced compositional drivers as the essential contributions of the building plan
method. This system is pursued to guarantee all the required drivers are utilized and are handled
with the help of different plan procedures, for example, the design examples and situations.
Primary Requirements:
As this project mainly focuses on the making communication possible between the doctor and
patient, the need of prototype should be managing the patient before and after surgery. The
software should provide the set of functionality that makes is possible for doctor and the user to
communicate with each other in an easy way within the mHealth solution. The application is to
be made for iPhone so the programming coding language to be used is swift. There are number
of requirements which had been identified from doing the literature review for the project
purpose and listed below.
Attribute Design Methodology suggested by the Software Engineering Institute (SEI) is known
as a deliberate philosophy pursued bit by bit so as to plan the product engineering of a software
extended framework. (Dixon, 2016) This methodology mainly focus around defining the product
design, the mhealth framework is dependent on the structures' quality characteristic prerequisites.
This strategy involves different advances, they include: recognize candidate architectural drivers,
choose a design concept that satisfies the architectural drivers, guarantee to give strategies to
accomplish quality prerequisites and produce a total programming engineering for the apparatus
which tends to all the compositional drivers.
Inaddition, the above advances, ADD is a three-advance procedure which includes info,
procedure and yield stages and this phrasing will be taken in to work on during the structure of
the product engineering of the proposed Activity Diagram to the mhealth development
procedures. The software architecture and configuration procedure is as demonstrated in the
design process
Identification of architectural driver
The input requirements to ADD includes the primary functional requirements, quality attribute
requirements and the constraints. Functional requirements for this project will be explained by
use of the use cases which is considered with architecture in the mHealth architecture. The
quality credit prioritization going before the framework being fabricated is upheld by the Quality
Attribute Workshop (QAW) which is likewise endorsed by the SEI. Finally, business and
specific goals are managed by outside components.
5.1.1 Architecture Driver
This section clarifies the development of the mhealth application program. This section
additionally identifies and subtleties the highlights of the application. The engineering structure
format proposed by is pursued for the remainder of the section. The act of this format bolsters the
identification of design drivers, definition, and documentation of views and viewpoints of
mhealth application software and how different perspectives utilized backings the
accomplishment of various compositional drivers identified during the underlying phases of this
section. In addition the structure of the design of the instrument, this section subtleties different
other relative terms, for example, model, displaying, meta model, meta-demonstrating and
changes that are utilized to plan the apparatus. This section rehearses the Attribute-Driven
Design (ADD) technique to define the product engineering of the apparatus which uses the
recently referenced compositional drivers as the essential contributions of the building plan
method. This system is pursued to guarantee all the required drivers are utilized and are handled
with the help of different plan procedures, for example, the design examples and situations.
Primary Requirements:
As this project mainly focuses on the making communication possible between the doctor and
patient, the need of prototype should be managing the patient before and after surgery. The
software should provide the set of functionality that makes is possible for doctor and the user to
communicate with each other in an easy way within the mHealth solution. The application is to
be made for iPhone so the programming coding language to be used is swift. There are number
of requirements which had been identified from doing the literature review for the project
purpose and listed below.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Requirement1: Application should have ability for patient to generate emergency alert in critical
situation.
Requirement2: Application should have ability for doctors to assign daily activity to assign to
the patient to take after surgery care.
Requirement3: Application should have ability for patient to report back the activity done daily.
Requirement4: Application should give functionality for patient to upload wound recovery
imaged within the application and not from email.
Quality Attribute Requirements:
About quality attribute Requirement (one para with reference)
In a general sense, the mhealth systems' utility is controlled by both the use and non-useful
necessities, these attributes incorporate ease of use, flexibility, execution, interoperability, and
security. Despite the fact that there had been an uneven accentuation on utilitarian prerequisites,
the usefulness of any framework isn't viewed as helpful or usable without the essential non-
practical necessities. (Dixon, 2016)As far as both architectural design and ADD, the non-
practical necessities are alluded to as Quality Attribute Requirements. Different helpful angles in
connection to mhealth application necessities are accomplished with the location of QARs. One
of the principle angles incorporates the direction gave during the structure and production of
value property situations which will be tended to after the identification and prioritization of the
QARs of this apparatus.
Any system non-functional requirements are being considered as the quality attribute
requirements. Like usability, security etc.
Why it is important in our paper? (1 paragraph)
The mhealth application tends to address the quality during the design structure of its
engineering and the device. Also, these QARs, some extra QARs are taken a look at, so as to
address the usefulness of the apparatus all in all. The QARs usefulness are interoperability,
convenience, understandability, versatility, likeness, modifiability, re-ease of use, accessibility,
testability, flexibility and execution of the framework, which are justified later in this segment.
These quality characteristic prerequisites are organized dependent on specific criteria as nitty-
gritty beneath.
Quality Attribute Priority:
Quality attribute prioritization helps process to achieve in better ways. It tells system architecture
to follow things on what extents. The priority levels are from 1 to so on and the level 1 shows the
highest level of priority.
Requirement1: Application should have ability for patient to generate emergency alert in critical
situation.
Requirement2: Application should have ability for doctors to assign daily activity to assign to
the patient to take after surgery care.
Requirement3: Application should have ability for patient to report back the activity done daily.
Requirement4: Application should give functionality for patient to upload wound recovery
imaged within the application and not from email.
Quality Attribute Requirements:
About quality attribute Requirement (one para with reference)
In a general sense, the mhealth systems' utility is controlled by both the use and non-useful
necessities, these attributes incorporate ease of use, flexibility, execution, interoperability, and
security. Despite the fact that there had been an uneven accentuation on utilitarian prerequisites,
the usefulness of any framework isn't viewed as helpful or usable without the essential non-
practical necessities. (Dixon, 2016)As far as both architectural design and ADD, the non-
practical necessities are alluded to as Quality Attribute Requirements. Different helpful angles in
connection to mhealth application necessities are accomplished with the location of QARs. One
of the principle angles incorporates the direction gave during the structure and production of
value property situations which will be tended to after the identification and prioritization of the
QARs of this apparatus.
Any system non-functional requirements are being considered as the quality attribute
requirements. Like usability, security etc.
Why it is important in our paper? (1 paragraph)
The mhealth application tends to address the quality during the design structure of its
engineering and the device. Also, these QARs, some extra QARs are taken a look at, so as to
address the usefulness of the apparatus all in all. The QARs usefulness are interoperability,
convenience, understandability, versatility, likeness, modifiability, re-ease of use, accessibility,
testability, flexibility and execution of the framework, which are justified later in this segment.
These quality characteristic prerequisites are organized dependent on specific criteria as nitty-
gritty beneath.
Quality Attribute Priority:
Quality attribute prioritization helps process to achieve in better ways. It tells system architecture
to follow things on what extents. The priority levels are from 1 to so on and the level 1 shows the
highest level of priority.
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
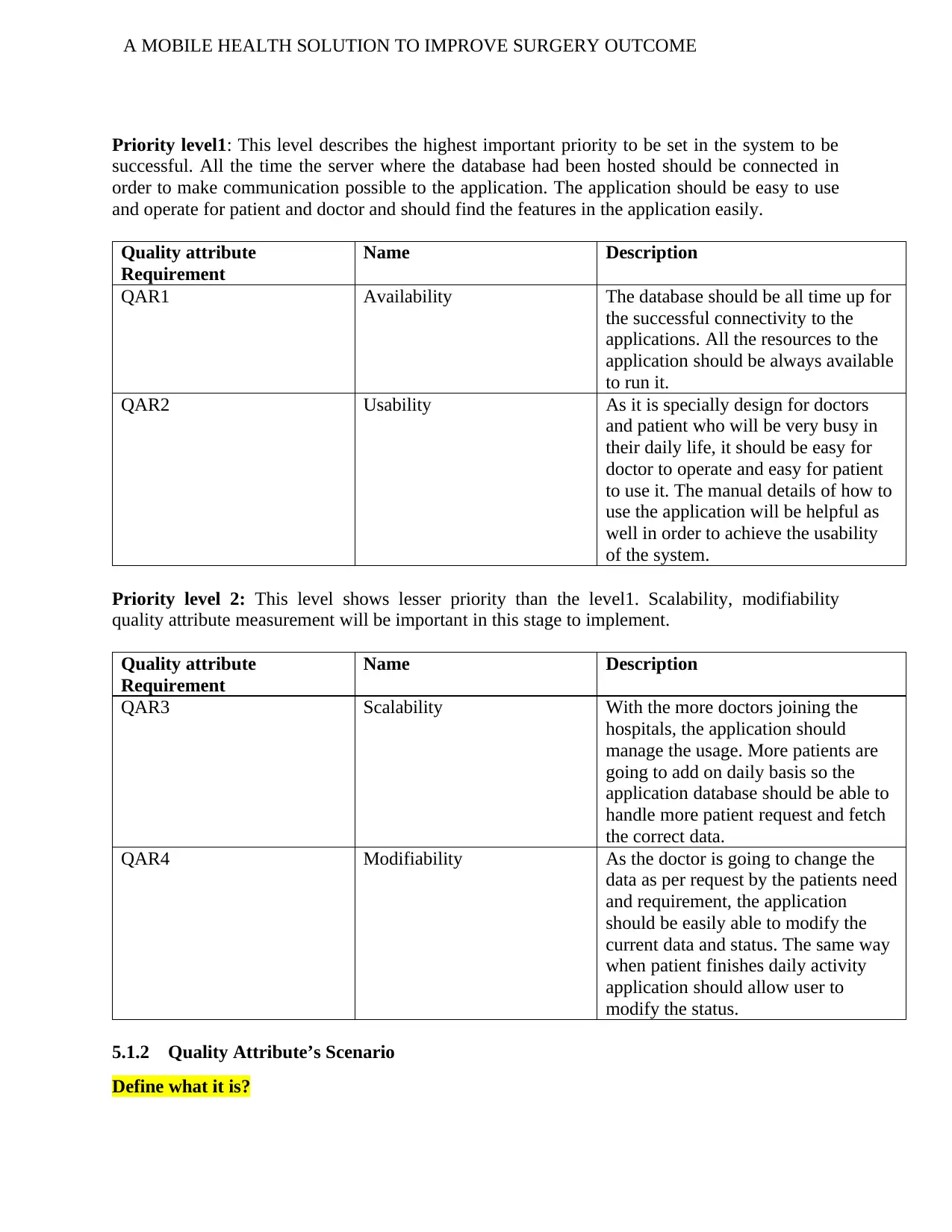
Priority level1: This level describes the highest important priority to be set in the system to be
successful. All the time the server where the database had been hosted should be connected in
order to make communication possible to the application. The application should be easy to use
and operate for patient and doctor and should find the features in the application easily.
Quality attribute
Requirement
Name Description
QAR1 Availability The database should be all time up for
the successful connectivity to the
applications. All the resources to the
application should be always available
to run it.
QAR2 Usability As it is specially design for doctors
and patient who will be very busy in
their daily life, it should be easy for
doctor to operate and easy for patient
to use it. The manual details of how to
use the application will be helpful as
well in order to achieve the usability
of the system.
Priority level 2: This level shows lesser priority than the level1. Scalability, modifiability
quality attribute measurement will be important in this stage to implement.
Quality attribute
Requirement
Name Description
QAR3 Scalability With the more doctors joining the
hospitals, the application should
manage the usage. More patients are
going to add on daily basis so the
application database should be able to
handle more patient request and fetch
the correct data.
QAR4 Modifiability As the doctor is going to change the
data as per request by the patients need
and requirement, the application
should be easily able to modify the
current data and status. The same way
when patient finishes daily activity
application should allow user to
modify the status.
5.1.2 Quality Attribute’s Scenario
Define what it is?
Priority level1: This level describes the highest important priority to be set in the system to be
successful. All the time the server where the database had been hosted should be connected in
order to make communication possible to the application. The application should be easy to use
and operate for patient and doctor and should find the features in the application easily.
Quality attribute
Requirement
Name Description
QAR1 Availability The database should be all time up for
the successful connectivity to the
applications. All the resources to the
application should be always available
to run it.
QAR2 Usability As it is specially design for doctors
and patient who will be very busy in
their daily life, it should be easy for
doctor to operate and easy for patient
to use it. The manual details of how to
use the application will be helpful as
well in order to achieve the usability
of the system.
Priority level 2: This level shows lesser priority than the level1. Scalability, modifiability
quality attribute measurement will be important in this stage to implement.
Quality attribute
Requirement
Name Description
QAR3 Scalability With the more doctors joining the
hospitals, the application should
manage the usage. More patients are
going to add on daily basis so the
application database should be able to
handle more patient request and fetch
the correct data.
QAR4 Modifiability As the doctor is going to change the
data as per request by the patients need
and requirement, the application
should be easily able to modify the
current data and status. The same way
when patient finishes daily activity
application should allow user to
modify the status.
5.1.2 Quality Attribute’s Scenario
Define what it is?
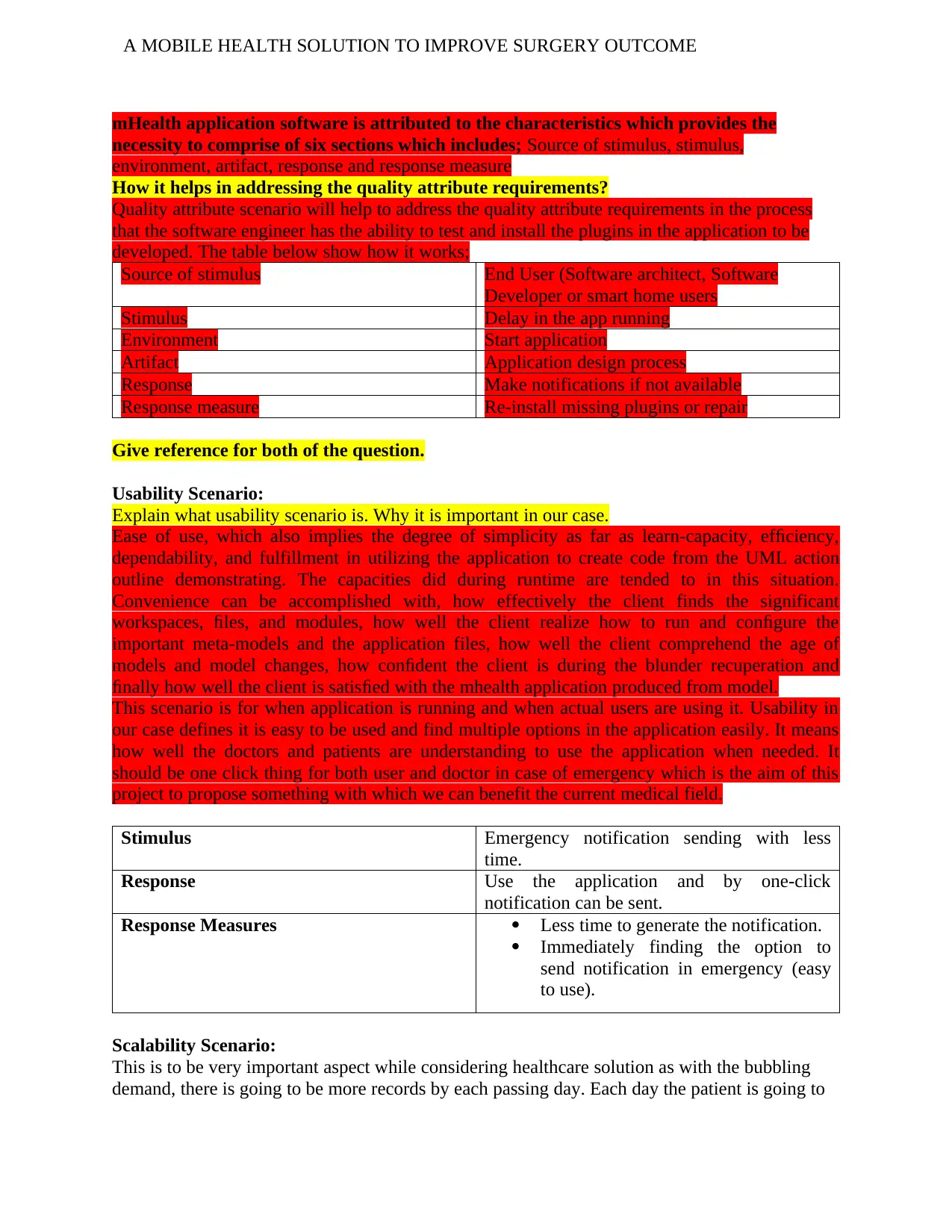
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
mHealth application software is attributed to the characteristics which provides the
necessity to comprise of six sections which includes; Source of stimulus, stimulus,
environment, artifact, response and response measure
How it helps in addressing the quality attribute requirements?
Quality attribute scenario will help to address the quality attribute requirements in the process
that the software engineer has the ability to test and install the plugins in the application to be
developed. The table below show how it works;
Source of stimulus End User (Software architect, Software
Developer or smart home users
Stimulus Delay in the app running
Environment Start application
Artifact Application design process
Response Make notifications if not available
Response measure Re-install missing plugins or repair
Give reference for both of the question.
Usability Scenario:
Explain what usability scenario is. Why it is important in our case.
Ease of use, which also implies the degree of simplicity as far as learn-capacity, efficiency,
dependability, and fulfillment in utilizing the application to create code from the UML action
outline demonstrating. The capacities did during runtime are tended to in this situation.
Convenience can be accomplished with, how effectively the client finds the significant
workspaces, files, and modules, how well the client realize how to run and configure the
important meta-models and the application files, how well the client comprehend the age of
models and model changes, how confident the client is during the blunder recuperation and
finally how well the client is satisfied with the mhealth application produced from model.
This scenario is for when application is running and when actual users are using it. Usability in
our case defines it is easy to be used and find multiple options in the application easily. It means
how well the doctors and patients are understanding to use the application when needed. It
should be one click thing for both user and doctor in case of emergency which is the aim of this
project to propose something with which we can benefit the current medical field.
Stimulus Emergency notification sending with less
time.
Response Use the application and by one-click
notification can be sent.
Response Measures Less time to generate the notification.
Immediately finding the option to
send notification in emergency (easy
to use).
Scalability Scenario:
This is to be very important aspect while considering healthcare solution as with the bubbling
demand, there is going to be more records by each passing day. Each day the patient is going to
mHealth application software is attributed to the characteristics which provides the
necessity to comprise of six sections which includes; Source of stimulus, stimulus,
environment, artifact, response and response measure
How it helps in addressing the quality attribute requirements?
Quality attribute scenario will help to address the quality attribute requirements in the process
that the software engineer has the ability to test and install the plugins in the application to be
developed. The table below show how it works;
Source of stimulus End User (Software architect, Software
Developer or smart home users
Stimulus Delay in the app running
Environment Start application
Artifact Application design process
Response Make notifications if not available
Response measure Re-install missing plugins or repair
Give reference for both of the question.
Usability Scenario:
Explain what usability scenario is. Why it is important in our case.
Ease of use, which also implies the degree of simplicity as far as learn-capacity, efficiency,
dependability, and fulfillment in utilizing the application to create code from the UML action
outline demonstrating. The capacities did during runtime are tended to in this situation.
Convenience can be accomplished with, how effectively the client finds the significant
workspaces, files, and modules, how well the client realize how to run and configure the
important meta-models and the application files, how well the client comprehend the age of
models and model changes, how confident the client is during the blunder recuperation and
finally how well the client is satisfied with the mhealth application produced from model.
This scenario is for when application is running and when actual users are using it. Usability in
our case defines it is easy to be used and find multiple options in the application easily. It means
how well the doctors and patients are understanding to use the application when needed. It
should be one click thing for both user and doctor in case of emergency which is the aim of this
project to propose something with which we can benefit the current medical field.
Stimulus Emergency notification sending with less
time.
Response Use the application and by one-click
notification can be sent.
Response Measures Less time to generate the notification.
Immediately finding the option to
send notification in emergency (easy
to use).
Scalability Scenario:
This is to be very important aspect while considering healthcare solution as with the bubbling
demand, there is going to be more records by each passing day. Each day the patient is going to
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
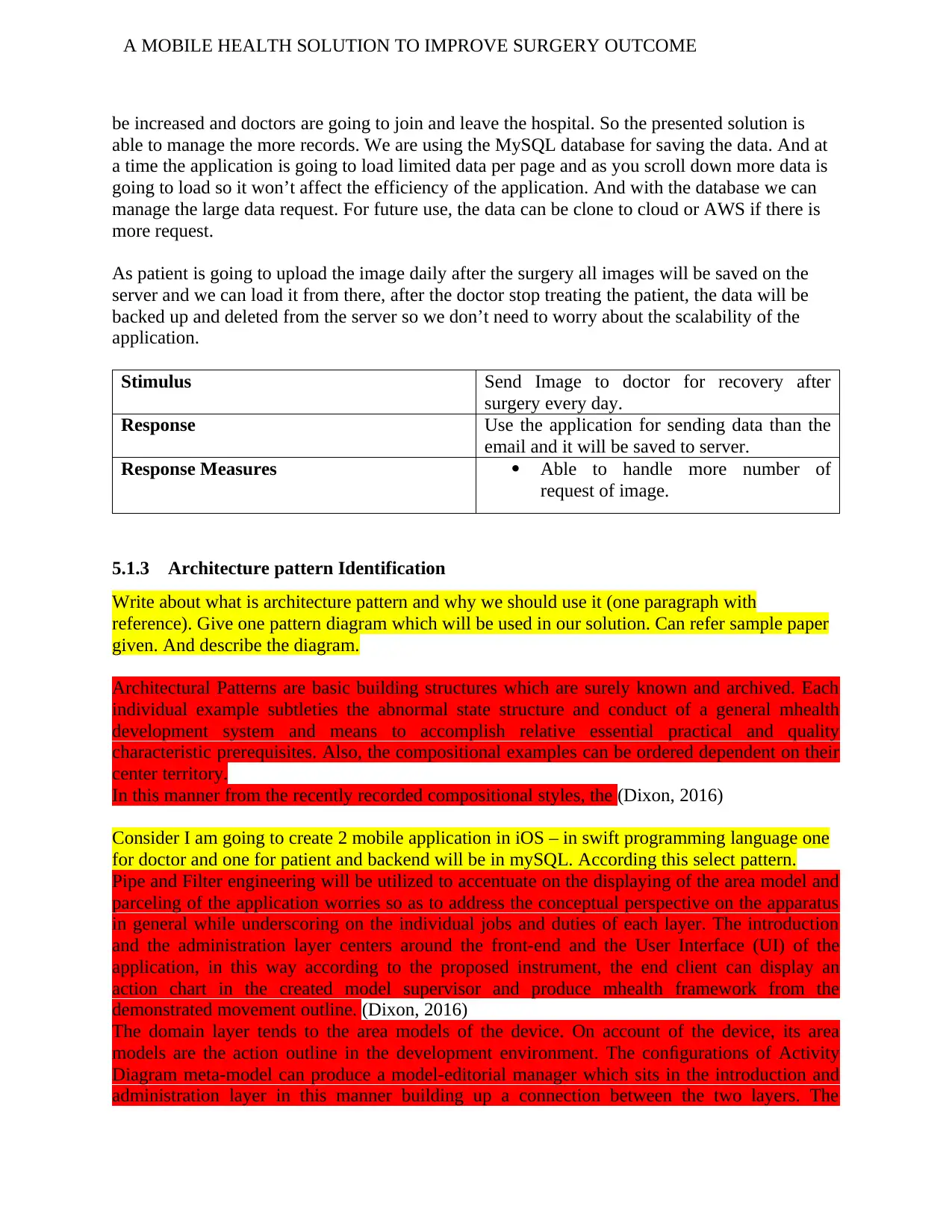
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
be increased and doctors are going to join and leave the hospital. So the presented solution is
able to manage the more records. We are using the MySQL database for saving the data. And at
a time the application is going to load limited data per page and as you scroll down more data is
going to load so it won’t affect the efficiency of the application. And with the database we can
manage the large data request. For future use, the data can be clone to cloud or AWS if there is
more request.
As patient is going to upload the image daily after the surgery all images will be saved on the
server and we can load it from there, after the doctor stop treating the patient, the data will be
backed up and deleted from the server so we don’t need to worry about the scalability of the
application.
Stimulus Send Image to doctor for recovery after
surgery every day.
Response Use the application for sending data than the
email and it will be saved to server.
Response Measures Able to handle more number of
request of image.
5.1.3 Architecture pattern Identification
Write about what is architecture pattern and why we should use it (one paragraph with
reference). Give one pattern diagram which will be used in our solution. Can refer sample paper
given. And describe the diagram.
Architectural Patterns are basic building structures which are surely known and archived. Each
individual example subtleties the abnormal state structure and conduct of a general mhealth
development system and means to accomplish relative essential practical and quality
characteristic prerequisites. Also, the compositional examples can be ordered dependent on their
center territory.
In this manner from the recently recorded compositional styles, the (Dixon, 2016)
Consider I am going to create 2 mobile application in iOS – in swift programming language one
for doctor and one for patient and backend will be in mySQL. According this select pattern.
Pipe and Filter engineering will be utilized to accentuate on the displaying of the area model and
parceling of the application worries so as to address the conceptual perspective on the apparatus
in general while underscoring on the individual jobs and duties of each layer. The introduction
and the administration layer centers around the front-end and the User Interface (UI) of the
application, in this way according to the proposed instrument, the end client can display an
action chart in the created model supervisor and produce mhealth framework from the
demonstrated movement outline. (Dixon, 2016)
The domain layer tends to the area models of the device. On account of the device, its area
models are the action outline in the development environment. The configurations of Activity
Diagram meta-model can produce a model-editorial manager which sits in the introduction and
administration layer in this manner building up a connection between the two layers. The
be increased and doctors are going to join and leave the hospital. So the presented solution is
able to manage the more records. We are using the MySQL database for saving the data. And at
a time the application is going to load limited data per page and as you scroll down more data is
going to load so it won’t affect the efficiency of the application. And with the database we can
manage the large data request. For future use, the data can be clone to cloud or AWS if there is
more request.
As patient is going to upload the image daily after the surgery all images will be saved on the
server and we can load it from there, after the doctor stop treating the patient, the data will be
backed up and deleted from the server so we don’t need to worry about the scalability of the
application.
Stimulus Send Image to doctor for recovery after
surgery every day.
Response Use the application for sending data than the
email and it will be saved to server.
Response Measures Able to handle more number of
request of image.
5.1.3 Architecture pattern Identification
Write about what is architecture pattern and why we should use it (one paragraph with
reference). Give one pattern diagram which will be used in our solution. Can refer sample paper
given. And describe the diagram.
Architectural Patterns are basic building structures which are surely known and archived. Each
individual example subtleties the abnormal state structure and conduct of a general mhealth
development system and means to accomplish relative essential practical and quality
characteristic prerequisites. Also, the compositional examples can be ordered dependent on their
center territory.
In this manner from the recently recorded compositional styles, the (Dixon, 2016)
Consider I am going to create 2 mobile application in iOS – in swift programming language one
for doctor and one for patient and backend will be in mySQL. According this select pattern.
Pipe and Filter engineering will be utilized to accentuate on the displaying of the area model and
parceling of the application worries so as to address the conceptual perspective on the apparatus
in general while underscoring on the individual jobs and duties of each layer. The introduction
and the administration layer centers around the front-end and the User Interface (UI) of the
application, in this way according to the proposed instrument, the end client can display an
action chart in the created model supervisor and produce mhealth framework from the
demonstrated movement outline. (Dixon, 2016)
The domain layer tends to the area models of the device. On account of the device, its area
models are the action outline in the development environment. The configurations of Activity
Diagram meta-model can produce a model-editorial manager which sits in the introduction and
administration layer in this manner building up a connection between the two layers. The
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
framework layer empowers the application to associate with the outside frameworks backing
getting, putting away and giving information when mentioned. Since the proposed device doesn't
include with any information stockpiling and trade, the ATL change procedure is incorporated
into this layer since it includes a model mapping and giving the mhealth application to the area
model when mentioned to help and finish the code age process.
5.1.4 Architecture Tactic Identification
Describe what is Tactic and how it is used? With reference.
Technique and strategies are two unique things. When you plan business technique you pick
strategies that will accomplish your vital objectives. Technique alludes to a bearing toward an
objective. Strategies are the moves made to help that technique. Most organizations manage five
kinds of procedure and the strategies used to accomplish key objectives: item, estimating,
showcasing, and operational and money related methodologies. Since the plan of the proposed
UML to code age apparatus doesn't have any outer partners engaged with the prerequisite
specification, the inference of the QARs is completely founded on the ADD and other relative
techniques, for example, the QAW. (Dixon, 2016)
QAR Stimulus Tactics
QAR1 Emergency notification sending with
less time.
This can be achieved by giving push
notification generation and message
sending within the application by just
one click.
This can be done by using the push
notification in iOS phone.
QAR2 Send Image for recovery after surgery
every day.
This can be done within the
application as application gives the
feature of uploading the image every
day and which will be managed by
status code. The image will be
uploaded on the server every time. We
can manage it using Restoration.
5.2 Architecture Tools:
For creating the small proto-type of the system, we are going to code in swift language for
creating the mobile application. To support the communication possible between the mobile and
the data we are going to have the database in MySQL. As we have two modules the patient and
the doctor module, we will have two mobile application. In order to make communication
possible we need to host the database on some server. The server will give connectivity so the
activity can be possible live in the application.
framework layer empowers the application to associate with the outside frameworks backing
getting, putting away and giving information when mentioned. Since the proposed device doesn't
include with any information stockpiling and trade, the ATL change procedure is incorporated
into this layer since it includes a model mapping and giving the mhealth application to the area
model when mentioned to help and finish the code age process.
5.1.4 Architecture Tactic Identification
Describe what is Tactic and how it is used? With reference.
Technique and strategies are two unique things. When you plan business technique you pick
strategies that will accomplish your vital objectives. Technique alludes to a bearing toward an
objective. Strategies are the moves made to help that technique. Most organizations manage five
kinds of procedure and the strategies used to accomplish key objectives: item, estimating,
showcasing, and operational and money related methodologies. Since the plan of the proposed
UML to code age apparatus doesn't have any outer partners engaged with the prerequisite
specification, the inference of the QARs is completely founded on the ADD and other relative
techniques, for example, the QAW. (Dixon, 2016)
QAR Stimulus Tactics
QAR1 Emergency notification sending with
less time.
This can be achieved by giving push
notification generation and message
sending within the application by just
one click.
This can be done by using the push
notification in iOS phone.
QAR2 Send Image for recovery after surgery
every day.
This can be done within the
application as application gives the
feature of uploading the image every
day and which will be managed by
status code. The image will be
uploaded on the server every time. We
can manage it using Restoration.
5.2 Architecture Tools:
For creating the small proto-type of the system, we are going to code in swift language for
creating the mobile application. To support the communication possible between the mobile and
the data we are going to have the database in MySQL. As we have two modules the patient and
the doctor module, we will have two mobile application. In order to make communication
possible we need to host the database on some server. The server will give connectivity so the
activity can be possible live in the application.
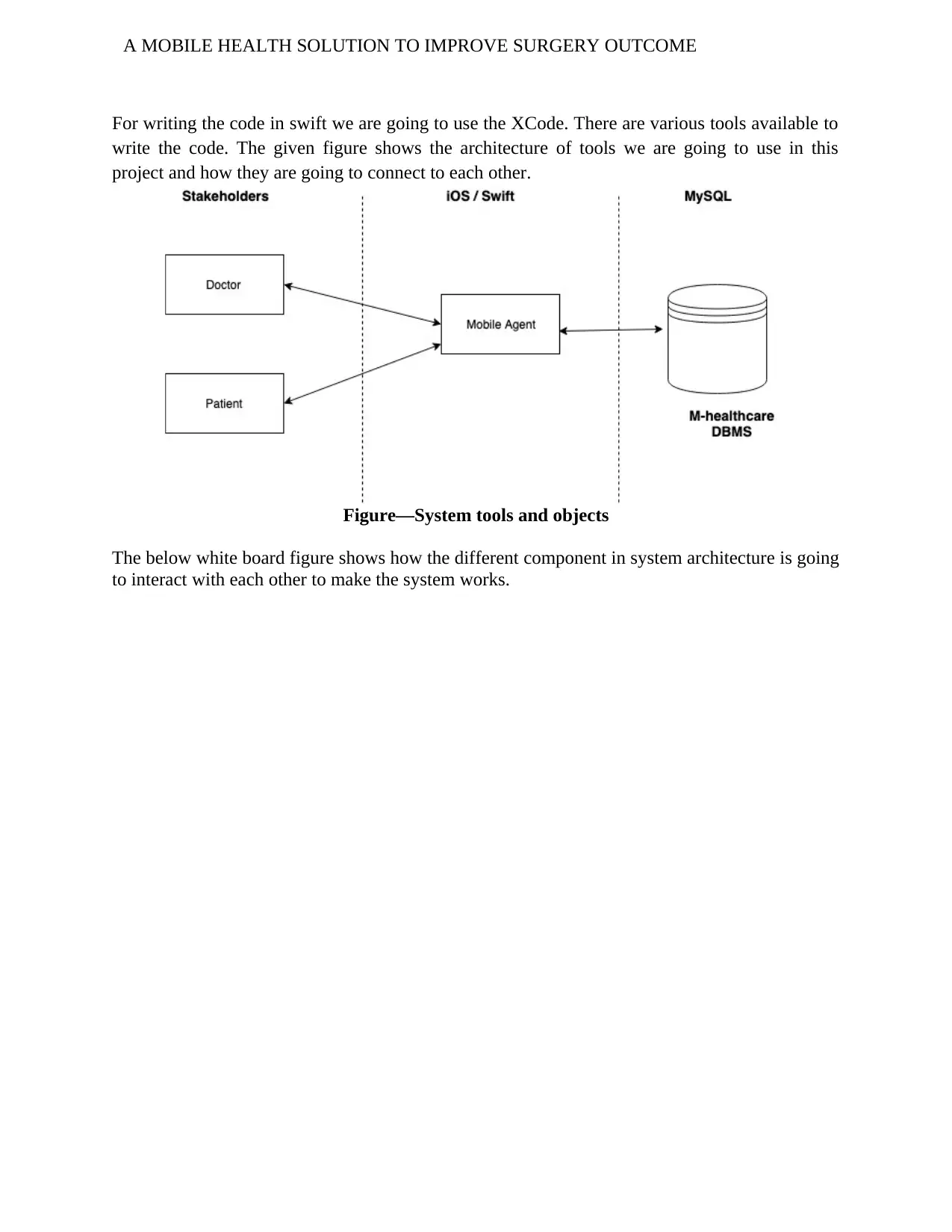
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
For writing the code in swift we are going to use the XCode. There are various tools available to
write the code. The given figure shows the architecture of tools we are going to use in this
project and how they are going to connect to each other.
Figure—System tools and objects
The below white board figure shows how the different component in system architecture is going
to interact with each other to make the system works.
For writing the code in swift we are going to use the XCode. There are various tools available to
write the code. The given figure shows the architecture of tools we are going to use in this
project and how they are going to connect to each other.
Figure—System tools and objects
The below white board figure shows how the different component in system architecture is going
to interact with each other to make the system works.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
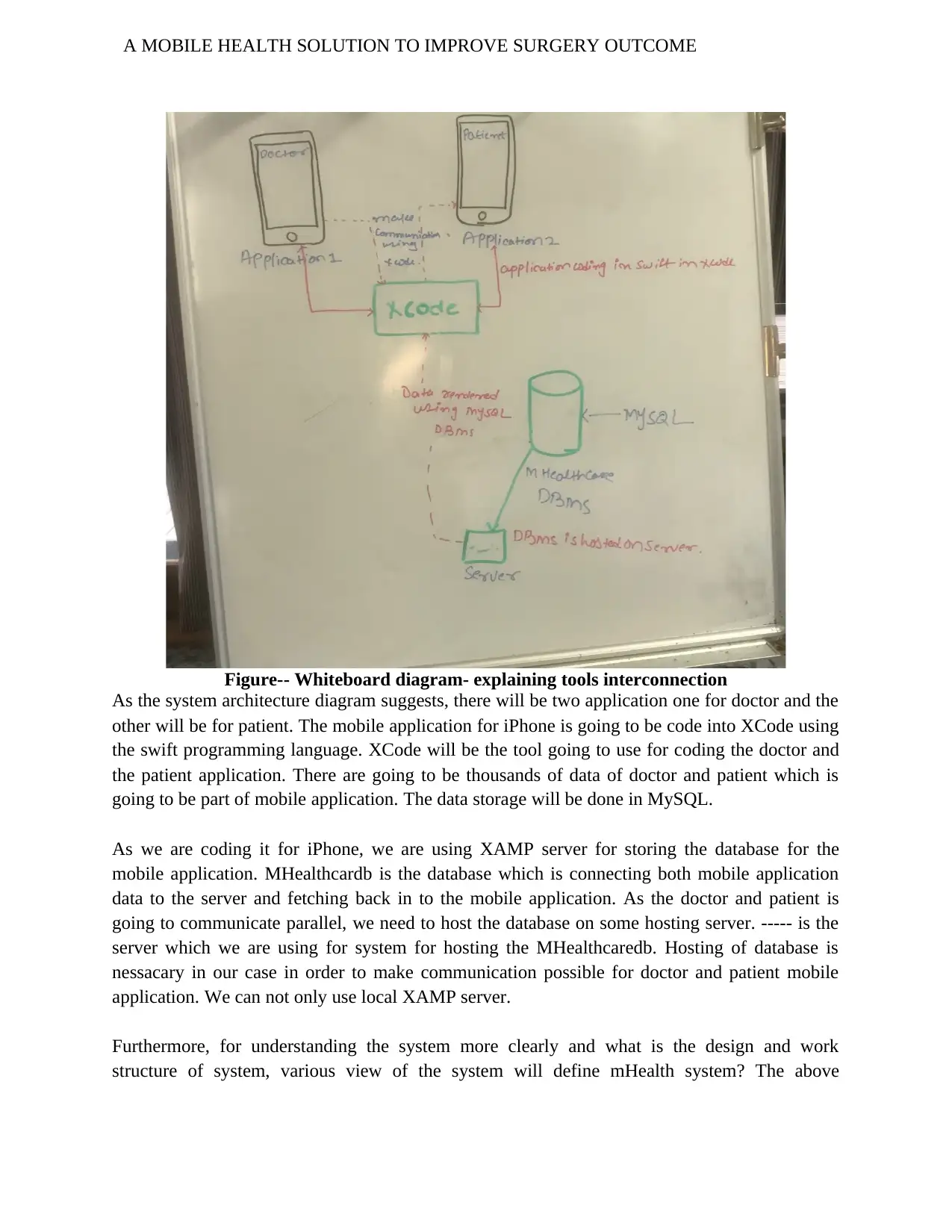
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Figure-- Whiteboard diagram- explaining tools interconnection
As the system architecture diagram suggests, there will be two application one for doctor and the
other will be for patient. The mobile application for iPhone is going to be code into XCode using
the swift programming language. XCode will be the tool going to use for coding the doctor and
the patient application. There are going to be thousands of data of doctor and patient which is
going to be part of mobile application. The data storage will be done in MySQL.
As we are coding it for iPhone, we are using XAMP server for storing the database for the
mobile application. MHealthcardb is the database which is connecting both mobile application
data to the server and fetching back in to the mobile application. As the doctor and patient is
going to communicate parallel, we need to host the database on some hosting server. ----- is the
server which we are using for system for hosting the MHealthcaredb. Hosting of database is
nessacary in our case in order to make communication possible for doctor and patient mobile
application. We can not only use local XAMP server.
Furthermore, for understanding the system more clearly and what is the design and work
structure of system, various view of the system will define mHealth system? The above
Figure-- Whiteboard diagram- explaining tools interconnection
As the system architecture diagram suggests, there will be two application one for doctor and the
other will be for patient. The mobile application for iPhone is going to be code into XCode using
the swift programming language. XCode will be the tool going to use for coding the doctor and
the patient application. There are going to be thousands of data of doctor and patient which is
going to be part of mobile application. The data storage will be done in MySQL.
As we are coding it for iPhone, we are using XAMP server for storing the database for the
mobile application. MHealthcardb is the database which is connecting both mobile application
data to the server and fetching back in to the mobile application. As the doctor and patient is
going to communicate parallel, we need to host the database on some hosting server. ----- is the
server which we are using for system for hosting the MHealthcaredb. Hosting of database is
nessacary in our case in order to make communication possible for doctor and patient mobile
application. We can not only use local XAMP server.
Furthermore, for understanding the system more clearly and what is the design and work
structure of system, various view of the system will define mHealth system? The above
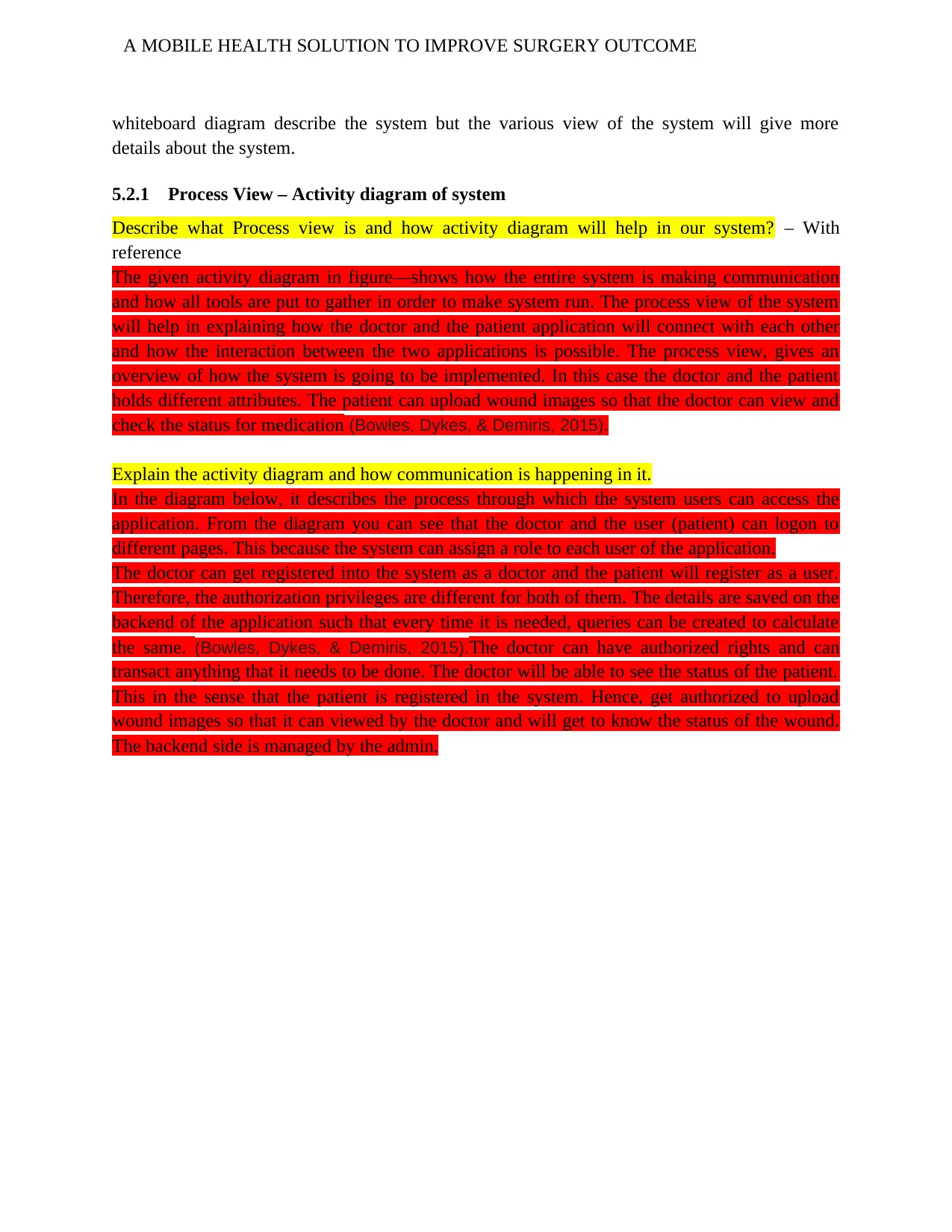
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
whiteboard diagram describe the system but the various view of the system will give more
details about the system.
5.2.1 Process View – Activity diagram of system
Describe what Process view is and how activity diagram will help in our system? – With
reference
The given activity diagram in figure—shows how the entire system is making communication
and how all tools are put to gather in order to make system run. The process view of the system
will help in explaining how the doctor and the patient application will connect with each other
and how the interaction between the two applications is possible. The process view, gives an
overview of how the system is going to be implemented. In this case the doctor and the patient
holds different attributes. The patient can upload wound images so that the doctor can view and
check the status for medication (Bowles, Dykes, & Demiris, 2015).
Explain the activity diagram and how communication is happening in it.
In the diagram below, it describes the process through which the system users can access the
application. From the diagram you can see that the doctor and the user (patient) can logon to
different pages. This because the system can assign a role to each user of the application.
The doctor can get registered into the system as a doctor and the patient will register as a user.
Therefore, the authorization privileges are different for both of them. The details are saved on the
backend of the application such that every time it is needed, queries can be created to calculate
the same. (Bowles, Dykes, & Demiris, 2015).The doctor can have authorized rights and can
transact anything that it needs to be done. The doctor will be able to see the status of the patient.
This in the sense that the patient is registered in the system. Hence, get authorized to upload
wound images so that it can viewed by the doctor and will get to know the status of the wound.
The backend side is managed by the admin.
whiteboard diagram describe the system but the various view of the system will give more
details about the system.
5.2.1 Process View – Activity diagram of system
Describe what Process view is and how activity diagram will help in our system? – With
reference
The given activity diagram in figure—shows how the entire system is making communication
and how all tools are put to gather in order to make system run. The process view of the system
will help in explaining how the doctor and the patient application will connect with each other
and how the interaction between the two applications is possible. The process view, gives an
overview of how the system is going to be implemented. In this case the doctor and the patient
holds different attributes. The patient can upload wound images so that the doctor can view and
check the status for medication (Bowles, Dykes, & Demiris, 2015).
Explain the activity diagram and how communication is happening in it.
In the diagram below, it describes the process through which the system users can access the
application. From the diagram you can see that the doctor and the user (patient) can logon to
different pages. This because the system can assign a role to each user of the application.
The doctor can get registered into the system as a doctor and the patient will register as a user.
Therefore, the authorization privileges are different for both of them. The details are saved on the
backend of the application such that every time it is needed, queries can be created to calculate
the same. (Bowles, Dykes, & Demiris, 2015).The doctor can have authorized rights and can
transact anything that it needs to be done. The doctor will be able to see the status of the patient.
This in the sense that the patient is registered in the system. Hence, get authorized to upload
wound images so that it can viewed by the doctor and will get to know the status of the wound.
The backend side is managed by the admin.
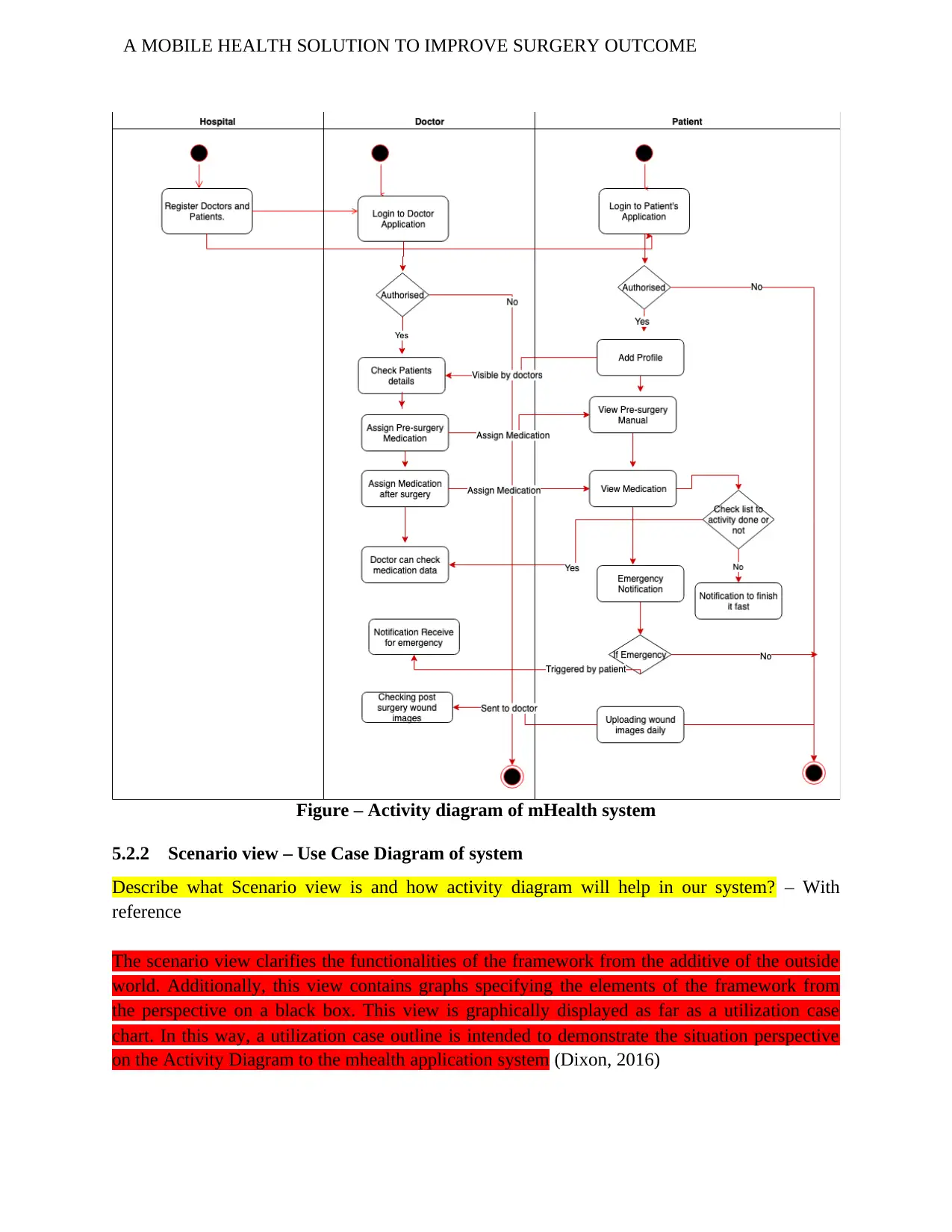
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Figure – Activity diagram of mHealth system
5.2.2 Scenario view – Use Case Diagram of system
Describe what Scenario view is and how activity diagram will help in our system? – With
reference
The scenario view clarifies the functionalities of the framework from the additive of the outside
world. Additionally, this view contains graphs specifying the elements of the framework from
the perspective on a black box. This view is graphically displayed as far as a utilization case
chart. In this way, a utilization case outline is intended to demonstrate the situation perspective
on the Activity Diagram to the mhealth application system (Dixon, 2016)
Figure – Activity diagram of mHealth system
5.2.2 Scenario view – Use Case Diagram of system
Describe what Scenario view is and how activity diagram will help in our system? – With
reference
The scenario view clarifies the functionalities of the framework from the additive of the outside
world. Additionally, this view contains graphs specifying the elements of the framework from
the perspective on a black box. This view is graphically displayed as far as a utilization case
chart. In this way, a utilization case outline is intended to demonstrate the situation perspective
on the Activity Diagram to the mhealth application system (Dixon, 2016)
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
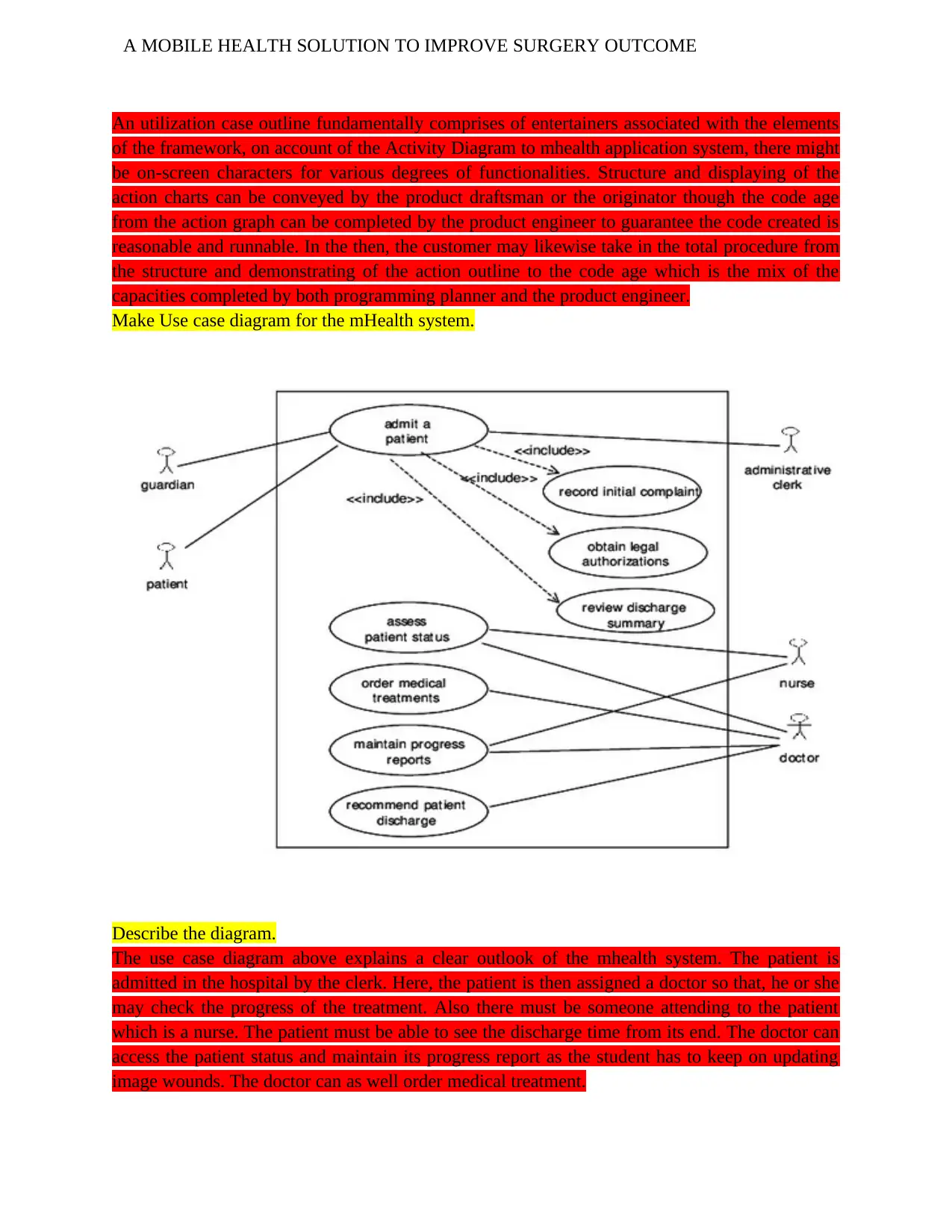
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
An utilization case outline fundamentally comprises of entertainers associated with the elements
of the framework, on account of the Activity Diagram to mhealth application system, there might
be on-screen characters for various degrees of functionalities. Structure and displaying of the
action charts can be conveyed by the product draftsman or the originator though the code age
from the action graph can be completed by the product engineer to guarantee the code created is
reasonable and runnable. In the then, the customer may likewise take in the total procedure from
the structure and demonstrating of the action outline to the code age which is the mix of the
capacities completed by both programming planner and the product engineer.
Make Use case diagram for the mHealth system.
Describe the diagram.
The use case diagram above explains a clear outlook of the mhealth system. The patient is
admitted in the hospital by the clerk. Here, the patient is then assigned a doctor so that, he or she
may check the progress of the treatment. Also there must be someone attending to the patient
which is a nurse. The patient must be able to see the discharge time from its end. The doctor can
access the patient status and maintain its progress report as the student has to keep on updating
image wounds. The doctor can as well order medical treatment.
An utilization case outline fundamentally comprises of entertainers associated with the elements
of the framework, on account of the Activity Diagram to mhealth application system, there might
be on-screen characters for various degrees of functionalities. Structure and displaying of the
action charts can be conveyed by the product draftsman or the originator though the code age
from the action graph can be completed by the product engineer to guarantee the code created is
reasonable and runnable. In the then, the customer may likewise take in the total procedure from
the structure and demonstrating of the action outline to the code age which is the mix of the
capacities completed by both programming planner and the product engineer.
Make Use case diagram for the mHealth system.
Describe the diagram.
The use case diagram above explains a clear outlook of the mhealth system. The patient is
admitted in the hospital by the clerk. Here, the patient is then assigned a doctor so that, he or she
may check the progress of the treatment. Also there must be someone attending to the patient
which is a nurse. The patient must be able to see the discharge time from its end. The doctor can
access the patient status and maintain its progress report as the student has to keep on updating
image wounds. The doctor can as well order medical treatment.

A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
4. Architecture Creation
References:
Bowles, K., Dykes, P., & Demiris, G. (2015). The Use of Health Information Technology to
Improve Care and Outcomes for Older Adults. Research in Gerontological Nursing, 8(1), 5-10.
doi:10.3928/19404921-20121222-01
Lu, C., Hu, Y., Xie, J., Fu, Q., Leigh, I., Governor, S., & Wang, G. (2018). The Use of Mobile
Health Applications to Improve Patient Experience: Cross-Sectional Study in Chinese Public
Hospitals. JMIR mHealth and uHealth, 6(5), e126. doi:10.2196/mhealth.9145
Semple, J., & Armstrong, K. (2016). Mobile applications for postoperative monitoring after
discharge. Canadian Medical Association Journal, 189(1), E22-E24. doi:10.1503/cmaj.160195
DeAntonio, J. H., Kang, H. S., Cockrell, H. C., Rothstein, W., Oiticica, C., & Lanning, D. A.
(2019). Utilization of a handheld telemedicine device in postoperative pediatric surgical
care. Journal of pediatric surgery, 54(5), 1005-1008.
https://doi.org/10.1016/j.jpedsurg.2019.01.032
Dowdeswell, B., Sinha, R., & Haemmerle, E. (2016, November). TORUS: Tracing complex
requirements for large cyber-physical systems. In 2016 21st International Conference on
Engineering of Complex Computer Systems (ICECCS) (pp. 23-32). IEEE.
DOI: 10.1109/ICECCS.2016.013
Gorini, A., Mazzocco, K., Triberti, S., Sebri, V., Savioni, L., & Pravettoni, G. (2018). A P5
approach to m-health: design suggestions for advanced mobile health technology. Frontiers in
psychology, 9. doi: 10.3389/fpsyg.2018.02066
Grissinger, M. (2016). Small effort, big payoff: Automated maximum dose alerts with hard
stops. Pharmacy and Therapeutics, 41(2), 82.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4745632/pdf/ptj4102082.pdf
Gunter, R., Fernandes-Taylor, S., Mahnke, A., Awoyinka, L., Schroeder, C., Wiseman, J., ... &
Kent, K. C. (2016). Evaluating patient usability of an image-based mobile health platform for
postoperative wound monitoring. JMIR mHealth and uHealth, 4(3), e113.
doi:10.2196/mhealth.6023
Jaensson, M., Dahlberg, K., & Nilsson, U. (2018). Sex similarities in postoperative recovery and
health care contacts within 14 days with mhealth follow-up: secondary analysis of a randomized
controlled trial. JMIR Perioperative Medicine, 1(1), e2. doi:10.2196/periop.9874
Kuhrmann, M., Diebold, P., Münch, J., Tell, P., Garousi, V., Felderer, M., Trektere, K.,
McCaffery, F., Linssen, O., Hanser, E. and Prause, C.R., (2017), July. Hybrid software and
system development in practice: waterfall, scrum, and beyond. In Proceedings of the 2017
International Conference on Software and System Process (30-39). ACM.
4. Architecture Creation
References:
Bowles, K., Dykes, P., & Demiris, G. (2015). The Use of Health Information Technology to
Improve Care and Outcomes for Older Adults. Research in Gerontological Nursing, 8(1), 5-10.
doi:10.3928/19404921-20121222-01
Lu, C., Hu, Y., Xie, J., Fu, Q., Leigh, I., Governor, S., & Wang, G. (2018). The Use of Mobile
Health Applications to Improve Patient Experience: Cross-Sectional Study in Chinese Public
Hospitals. JMIR mHealth and uHealth, 6(5), e126. doi:10.2196/mhealth.9145
Semple, J., & Armstrong, K. (2016). Mobile applications for postoperative monitoring after
discharge. Canadian Medical Association Journal, 189(1), E22-E24. doi:10.1503/cmaj.160195
DeAntonio, J. H., Kang, H. S., Cockrell, H. C., Rothstein, W., Oiticica, C., & Lanning, D. A.
(2019). Utilization of a handheld telemedicine device in postoperative pediatric surgical
care. Journal of pediatric surgery, 54(5), 1005-1008.
https://doi.org/10.1016/j.jpedsurg.2019.01.032
Dowdeswell, B., Sinha, R., & Haemmerle, E. (2016, November). TORUS: Tracing complex
requirements for large cyber-physical systems. In 2016 21st International Conference on
Engineering of Complex Computer Systems (ICECCS) (pp. 23-32). IEEE.
DOI: 10.1109/ICECCS.2016.013
Gorini, A., Mazzocco, K., Triberti, S., Sebri, V., Savioni, L., & Pravettoni, G. (2018). A P5
approach to m-health: design suggestions for advanced mobile health technology. Frontiers in
psychology, 9. doi: 10.3389/fpsyg.2018.02066
Grissinger, M. (2016). Small effort, big payoff: Automated maximum dose alerts with hard
stops. Pharmacy and Therapeutics, 41(2), 82.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4745632/pdf/ptj4102082.pdf
Gunter, R., Fernandes-Taylor, S., Mahnke, A., Awoyinka, L., Schroeder, C., Wiseman, J., ... &
Kent, K. C. (2016). Evaluating patient usability of an image-based mobile health platform for
postoperative wound monitoring. JMIR mHealth and uHealth, 4(3), e113.
doi:10.2196/mhealth.6023
Jaensson, M., Dahlberg, K., & Nilsson, U. (2018). Sex similarities in postoperative recovery and
health care contacts within 14 days with mhealth follow-up: secondary analysis of a randomized
controlled trial. JMIR Perioperative Medicine, 1(1), e2. doi:10.2196/periop.9874
Kuhrmann, M., Diebold, P., Münch, J., Tell, P., Garousi, V., Felderer, M., Trektere, K.,
McCaffery, F., Linssen, O., Hanser, E. and Prause, C.R., (2017), July. Hybrid software and
system development in practice: waterfall, scrum, and beyond. In Proceedings of the 2017
International Conference on Software and System Process (30-39). ACM.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Mhurchu, C. N., Whittaker, R., McRobbie, H., Ball, K., Crawford, D., Michie, J., ... & Myers, K.
(2014). Feasibility, acceptability and potential effectiveness of a mobile health (mHealth) weight
management programme for New Zealand adults. BMC obesity, 1(1), 10.
https://doi.org/10.1186/2052-9538-1-10
Pedersen, P.M., Black Duck Software Inc, (2016). Methods and systems for managing software
development. U.S. Patent 9,489,687.
Cleeland, C., Wang, X., Shi, Q., Mendoza, T., Wright, S., Berry, M., Malveaux, D., Shah, P.,
Gning, I., Hofstetter, W., Putnam, J. and Vaporciyan, A. (2011). Automated Symptom Alerts
Reduce Postoperative Symptom Severity After Cancer Surgery: A Randomized Controlled
Clinical Trial. Journal of Clinical Oncology, 29(8), pp.994-1000.
Carrier, G., Cotte, E., Beyer-Berjot, L., Faucheron, J., Joris, J. and Slim, K. (2016). Post-
discharge follow-up using text messaging within an enhanced recovery program after colorectal
surgery. Journal of Visceral Surgery, 153(4), pp.249-252.
Debono, B., Bousquet, P., Sabatier, P., Plas, J., Lescure, J. and Hamel, O.
(2019). Postoperative monitoring with a mobile application after ambulatory lumbar discectomy:
an effective tool for spine surgeons.
DeVito Dabbs, A., Song, M., Myers, B., Li, R., Hawkins, R., Pilewski, J., Bermudez, C.,
Aubrecht, J., Begey, A., Connolly, M., Alrawashdeh, M. and Dew, M. (2016). A Randomized
Controlled Trial of a Mobile Health Intervention to Promote Self-Management After Lung
Transplantation. American Journal of Transplantation, 16(7), pp.2172-2180.
Semple, J., Sharpe, S., Murnaghan, M., Theodoropoulos, J. and Metcalfe, K. (2015). Using a
Mobile App for Monitoring Post-Operative Quality of Recovery of Patients at Home: A Feasibility
Study. JMIR mHealth and uHealth, 3(1), p.e18.
Martínez-Ramos, C., Cerdán, M. T., & Lopez, R. S. (2009). Mobile phone–based telemedicine
system for the home follow-up of patients undergoing ambulatory surgery. Telemedicine and e-
Health, 15(6), 531-537.
Perera, N. (2018). Automatic conversion of activity diagrams into flexible smart home
apps (Doctoral dissertation, Auckland University of Technology).
http://hdl.handle.net/10292/11602
Sanger, P. C., Hartzler, A., Han, S. M., Armstrong, C. A., Stewart, M. R., Lordon, R. J., ... &
Evans, H. L. (2014). Patient perspectives on post-discharge surgical site infections: towards a
patient-centered mobile health solution. PLoS One, 9(12), e114016.
https://doi.org/10.1371/journal.pone.0114016
Suchy, F. J., Iyer, K., & Kerkar, N. (2009). Improved Adherence and Outcomes for Pediatric
Liver Transplant Recipients by Using Text Messaging.
Lin, H., Chen, W., Luo, L., Congdon, N., Zhang, X., Zhong, X., ... & Deng, D. (2012).
Effectiveness of a short message reminder in increasing compliance with pediatric cataract
treatment: a randomized trial. Ophthalmology, 119(12), 2463-2470.
Mhurchu, C. N., Whittaker, R., McRobbie, H., Ball, K., Crawford, D., Michie, J., ... & Myers, K.
(2014). Feasibility, acceptability and potential effectiveness of a mobile health (mHealth) weight
management programme for New Zealand adults. BMC obesity, 1(1), 10.
https://doi.org/10.1186/2052-9538-1-10
Pedersen, P.M., Black Duck Software Inc, (2016). Methods and systems for managing software
development. U.S. Patent 9,489,687.
Cleeland, C., Wang, X., Shi, Q., Mendoza, T., Wright, S., Berry, M., Malveaux, D., Shah, P.,
Gning, I., Hofstetter, W., Putnam, J. and Vaporciyan, A. (2011). Automated Symptom Alerts
Reduce Postoperative Symptom Severity After Cancer Surgery: A Randomized Controlled
Clinical Trial. Journal of Clinical Oncology, 29(8), pp.994-1000.
Carrier, G., Cotte, E., Beyer-Berjot, L., Faucheron, J., Joris, J. and Slim, K. (2016). Post-
discharge follow-up using text messaging within an enhanced recovery program after colorectal
surgery. Journal of Visceral Surgery, 153(4), pp.249-252.
Debono, B., Bousquet, P., Sabatier, P., Plas, J., Lescure, J. and Hamel, O.
(2019). Postoperative monitoring with a mobile application after ambulatory lumbar discectomy:
an effective tool for spine surgeons.
DeVito Dabbs, A., Song, M., Myers, B., Li, R., Hawkins, R., Pilewski, J., Bermudez, C.,
Aubrecht, J., Begey, A., Connolly, M., Alrawashdeh, M. and Dew, M. (2016). A Randomized
Controlled Trial of a Mobile Health Intervention to Promote Self-Management After Lung
Transplantation. American Journal of Transplantation, 16(7), pp.2172-2180.
Semple, J., Sharpe, S., Murnaghan, M., Theodoropoulos, J. and Metcalfe, K. (2015). Using a
Mobile App for Monitoring Post-Operative Quality of Recovery of Patients at Home: A Feasibility
Study. JMIR mHealth and uHealth, 3(1), p.e18.
Martínez-Ramos, C., Cerdán, M. T., & Lopez, R. S. (2009). Mobile phone–based telemedicine
system for the home follow-up of patients undergoing ambulatory surgery. Telemedicine and e-
Health, 15(6), 531-537.
Perera, N. (2018). Automatic conversion of activity diagrams into flexible smart home
apps (Doctoral dissertation, Auckland University of Technology).
http://hdl.handle.net/10292/11602
Sanger, P. C., Hartzler, A., Han, S. M., Armstrong, C. A., Stewart, M. R., Lordon, R. J., ... &
Evans, H. L. (2014). Patient perspectives on post-discharge surgical site infections: towards a
patient-centered mobile health solution. PLoS One, 9(12), e114016.
https://doi.org/10.1371/journal.pone.0114016
Suchy, F. J., Iyer, K., & Kerkar, N. (2009). Improved Adherence and Outcomes for Pediatric
Liver Transplant Recipients by Using Text Messaging.
Lin, H., Chen, W., Luo, L., Congdon, N., Zhang, X., Zhong, X., ... & Deng, D. (2012).
Effectiveness of a short message reminder in increasing compliance with pediatric cataract
treatment: a randomized trial. Ophthalmology, 119(12), 2463-2470.
A MOBILE HEALTH SOLUTION TO IMPROVE SURGERY OUTCOME
Chen, Y., Chin, M., Greenberg, S., Johnstone, C., & McGuinness, J. (2012). Post‐tonsillectomy
pain in 24 children–utilising short message service (SMS) to assess postoperative
outcomes. Clinical otolaryngology, 37(5), 412-414.
Sachse, M. M., Böttcher, S., Pape, L., Wagner, G., Mehls, O., Klaus, G., ... & Zeeb, H. (2016).
Face-to-face sun protection training and text messages improve sun protection behaviour in
adolescent organ transplant recipients: HIPPOlino feasibility study. Acta dermato-
venereologica, 96(3), 341-345.
Schnall, R., Rojas, M., Travers, J., Brown III, W., & Bakken, S. (2014). Use of design science for
informing the development of a mobile app for persons living with HIV. In AMIA Annual
Symposium Proceedings (Vol. 2014, p. 1037). American Medical Informatics Association.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4419902/pdf/1970979.pdf
Slade Shantz, J. A., & Veillette, C. J. (2014). The application of wearable technology in surgery:
ensuring the positive impact of the wearable revolution on surgical patients. Frontiers in
surgery, 1, 39. https://doi.org/10.3389/fsurg.2014.00039
Symer, M. M., Abelson, J. S., Milsom, J., McClure, B., & Yeo, H. L. (2017). A mobile health
application to track patients after gastrointestinal surgery: results from a pilot study. Journal of
Gastrointestinal Surgery, 21(9), 1500-1505. https://doi.org/10.1007/s11605-017-3482-2
Wang, Q. Q., Zhao, J., Huo, X. R., Wu, L., Yang, L. F., Li, J. Y., & Wang, J. (2018). Effects of a
home care mobile app on the outcomes of discharged patients with a stoma: A randomised
controlled trial. Journal of clinical nursing, 27(19-20), 3592-3602.
https://doi.org/10.1111/jocn.14515
Dixon, B. (2016). Health Information Exchange. Academic Pr.
Chen, Y., Chin, M., Greenberg, S., Johnstone, C., & McGuinness, J. (2012). Post‐tonsillectomy
pain in 24 children–utilising short message service (SMS) to assess postoperative
outcomes. Clinical otolaryngology, 37(5), 412-414.
Sachse, M. M., Böttcher, S., Pape, L., Wagner, G., Mehls, O., Klaus, G., ... & Zeeb, H. (2016).
Face-to-face sun protection training and text messages improve sun protection behaviour in
adolescent organ transplant recipients: HIPPOlino feasibility study. Acta dermato-
venereologica, 96(3), 341-345.
Schnall, R., Rojas, M., Travers, J., Brown III, W., & Bakken, S. (2014). Use of design science for
informing the development of a mobile app for persons living with HIV. In AMIA Annual
Symposium Proceedings (Vol. 2014, p. 1037). American Medical Informatics Association.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4419902/pdf/1970979.pdf
Slade Shantz, J. A., & Veillette, C. J. (2014). The application of wearable technology in surgery:
ensuring the positive impact of the wearable revolution on surgical patients. Frontiers in
surgery, 1, 39. https://doi.org/10.3389/fsurg.2014.00039
Symer, M. M., Abelson, J. S., Milsom, J., McClure, B., & Yeo, H. L. (2017). A mobile health
application to track patients after gastrointestinal surgery: results from a pilot study. Journal of
Gastrointestinal Surgery, 21(9), 1500-1505. https://doi.org/10.1007/s11605-017-3482-2
Wang, Q. Q., Zhao, J., Huo, X. R., Wu, L., Yang, L. F., Li, J. Y., & Wang, J. (2018). Effects of a
home care mobile app on the outcomes of discharged patients with a stoma: A randomised
controlled trial. Journal of clinical nursing, 27(19-20), 3592-3602.
https://doi.org/10.1111/jocn.14515
Dixon, B. (2016). Health Information Exchange. Academic Pr.
1 out of 27
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.