Abortion Health Law USA Topic 2022
VerifiedAdded on 2022/10/19
|15
|2797
|31
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Running head: ABORTION 0
HEALTH LAW
JULY 30, 2019
STUDENT DETAILS:
HEALTH LAW
JULY 30, 2019
STUDENT DETAILS:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
ABORTION 1
The abortion is old as well as worldwide practice. The abortion has taken various forms
in the social context, political context, as well as traditional context. There are different laws on
the abortion in different nations. These laws vary from country to country. In some nations, this
is available to the females on demand. On the other hand, it is outlawed in some countries. The
liberalization of abortion is a matter of deep arguments. Most of the times, the liberalization of
abortion is challenged. The governments struggle to make the balance between the right of
unborn fetuses and the right of pregnant females. The imagining health policies info-graphic
assesses the state policies in relation to abortion as well as the intersection with clinical practices.
In the following parts, the intersection of state abortion policy and clinical practice is discussed
and critically examined.
In USA, the abortion is a secure as well as general medical process for the females. In
2015, over ninety per cent of reported abortions occurred in the first trimester. The rate of
abortion has decreased. From 2006 to 2015, it is decreased to twenty six per cent among women
aged fifteen years to forty-four years. When services of abortion are regulated by similar
approaches and legislations that govern the medical services, various states have passed the
abortion related regulations. The abortion related regulations may restrict the access of females
to the abortion services (Francome, 2017). These laws may endanger the quality of care. There
are 27 states, which require the females seeking abortion to wait eighteen hours or more before
getting the abortion. Further, numerous require females to be counselled on the matters
unconfirmed by medical agreements or evidence, like wrongly telling women that abortion
increases the risks of breast cancer. More recently, many states have established particular
requirements for the doctors and clinics who render the medication abortion, with thirty-four
The abortion is old as well as worldwide practice. The abortion has taken various forms
in the social context, political context, as well as traditional context. There are different laws on
the abortion in different nations. These laws vary from country to country. In some nations, this
is available to the females on demand. On the other hand, it is outlawed in some countries. The
liberalization of abortion is a matter of deep arguments. Most of the times, the liberalization of
abortion is challenged. The governments struggle to make the balance between the right of
unborn fetuses and the right of pregnant females. The imagining health policies info-graphic
assesses the state policies in relation to abortion as well as the intersection with clinical practices.
In the following parts, the intersection of state abortion policy and clinical practice is discussed
and critically examined.
In USA, the abortion is a secure as well as general medical process for the females. In
2015, over ninety per cent of reported abortions occurred in the first trimester. The rate of
abortion has decreased. From 2006 to 2015, it is decreased to twenty six per cent among women
aged fifteen years to forty-four years. When services of abortion are regulated by similar
approaches and legislations that govern the medical services, various states have passed the
abortion related regulations. The abortion related regulations may restrict the access of females
to the abortion services (Francome, 2017). These laws may endanger the quality of care. There
are 27 states, which require the females seeking abortion to wait eighteen hours or more before
getting the abortion. Further, numerous require females to be counselled on the matters
unconfirmed by medical agreements or evidence, like wrongly telling women that abortion
increases the risks of breast cancer. More recently, many states have established particular
requirements for the doctors and clinics who render the medication abortion, with thirty-four
ABORTION 2
authorizing that only the licensed physician distribute abortion pill. Further, seventeen of the
states require that the physicians should be present physically. They block the utilisation of
telemedicine to increase the access to abortion. Almost twenty states have the laws to enforce the
prison sentence on the clinicians if they make abortions past certain state-developed
gestational restrictions (Grossman, 2017).
Further, the legislations and regulations related to the abortion state that abortion could
also have the bad impacts on the capability to obtain care. In year 2014, the fifty-seven per cent
of the females of generative age lived in one of twenty-seven states regarded hostile to the rights
of abortion. On the other hand, thirty-one per cent of females had lived in the thirteen states in
year 2000. Increasingly, the restrictive policies in relation to access to the abortion service
possibly play the role in obtainability. The number of non-hospital abortion clinics that render
ninety-five per cent of abortion, reduced six per cent form year 2011 to 2014. This reduction can
be attributable to the limiting laws aimed at closing clinic that in order may force the patients for
travelling (Piazaa, 2017).
Furthermore, the Ohio and Texas are regarded hostile to the abortion rights, and render
illustrations of how abortion limitations and settings may influence where and how the females
get services. Texas enacted HB 2 in year 2013. It includes various kinds of targeted regulations
of abortion provider restrictions. It involves the provisions that provider has hospital declaring
rights. It provides the requirement of the physical standard of ambulatory surgery centre. In the
state, the abortion rendering has dropped from forty-one to twenty-two in 6 months after the laws
were enacted. It can have declined further since that period. The decreased number of workers
has translated to the restricted appointment obtainability among the remaining providers. Waiting
period of two weeks to three weeks for the abortion have been documented at certain amenities.
authorizing that only the licensed physician distribute abortion pill. Further, seventeen of the
states require that the physicians should be present physically. They block the utilisation of
telemedicine to increase the access to abortion. Almost twenty states have the laws to enforce the
prison sentence on the clinicians if they make abortions past certain state-developed
gestational restrictions (Grossman, 2017).
Further, the legislations and regulations related to the abortion state that abortion could
also have the bad impacts on the capability to obtain care. In year 2014, the fifty-seven per cent
of the females of generative age lived in one of twenty-seven states regarded hostile to the rights
of abortion. On the other hand, thirty-one per cent of females had lived in the thirteen states in
year 2000. Increasingly, the restrictive policies in relation to access to the abortion service
possibly play the role in obtainability. The number of non-hospital abortion clinics that render
ninety-five per cent of abortion, reduced six per cent form year 2011 to 2014. This reduction can
be attributable to the limiting laws aimed at closing clinic that in order may force the patients for
travelling (Piazaa, 2017).
Furthermore, the Ohio and Texas are regarded hostile to the abortion rights, and render
illustrations of how abortion limitations and settings may influence where and how the females
get services. Texas enacted HB 2 in year 2013. It includes various kinds of targeted regulations
of abortion provider restrictions. It involves the provisions that provider has hospital declaring
rights. It provides the requirement of the physical standard of ambulatory surgery centre. In the
state, the abortion rendering has dropped from forty-one to twenty-two in 6 months after the laws
were enacted. It can have declined further since that period. The decreased number of workers
has translated to the restricted appointment obtainability among the remaining providers. Waiting
period of two weeks to three weeks for the abortion have been documented at certain amenities.
ABORTION 3
In addition, the average one-way distance to the nearest abortion providers have enhanced from
seventeen miles to seventy miles that is particularly important if females should have the trips in
excess of once (Gomez, et. al, 2016). The females who are looking for the abortion in Texas,
have stated that a closure of various clinics has led to the confusion regarding where to get the
extra care, enhanced cost as well as travel for care, and sometimes forced them to suspend or
decline attaining the care. Additionally, Ohio that has various limitations in a place as Texas saw
a closure of minimum six of the eighteen abortion hospitals between year 2011 and 2014,
following the application of severe hospital transfer agreement TRAP laws as same as the Texas
hospital declaring privilege requirements. United with gestational age limit restrictions as well as
the in person waiting period of twenty-four hours, the laws can have driven the females to travel
to neighbouring Michigan to get the services related to abortion, as subjective report suggests
(Conti, et. al, 2016).
Independently, the limitations like those in Ohio and Texas cannot evidently breach the
basic rights of females to abortion. However, in a case of Whole Woman's Health v. Hellerstedt,
the Supreme Court of America upturned the two provisions of Texas law HB 2. It was held by
the Supreme Court that the hospitals declaring privileges and ambulatory surgical centres
necessities together made the constitutionally impermissible undue load by creating the
significant problems in a way of females looking for the abortion (Mucciaroni, Ferraiolo &
Rubado, 2019). In the subsequent period, the Supreme Court repudiated the judicial reviews to
due petitions from Wisconsin as well as Mississippi to re-establish confessing privilege laws as
same as in Texas. The Mississippi laws will have only closed the abortion hospitals in a state. By
rejecting to consider the matters, the Court protected the assistance for a concept that the
meeting of limitations that force the females to travel to get the abortion, can be the unauthorised
In addition, the average one-way distance to the nearest abortion providers have enhanced from
seventeen miles to seventy miles that is particularly important if females should have the trips in
excess of once (Gomez, et. al, 2016). The females who are looking for the abortion in Texas,
have stated that a closure of various clinics has led to the confusion regarding where to get the
extra care, enhanced cost as well as travel for care, and sometimes forced them to suspend or
decline attaining the care. Additionally, Ohio that has various limitations in a place as Texas saw
a closure of minimum six of the eighteen abortion hospitals between year 2011 and 2014,
following the application of severe hospital transfer agreement TRAP laws as same as the Texas
hospital declaring privilege requirements. United with gestational age limit restrictions as well as
the in person waiting period of twenty-four hours, the laws can have driven the females to travel
to neighbouring Michigan to get the services related to abortion, as subjective report suggests
(Conti, et. al, 2016).
Independently, the limitations like those in Ohio and Texas cannot evidently breach the
basic rights of females to abortion. However, in a case of Whole Woman's Health v. Hellerstedt,
the Supreme Court of America upturned the two provisions of Texas law HB 2. It was held by
the Supreme Court that the hospitals declaring privileges and ambulatory surgical centres
necessities together made the constitutionally impermissible undue load by creating the
significant problems in a way of females looking for the abortion (Mucciaroni, Ferraiolo &
Rubado, 2019). In the subsequent period, the Supreme Court repudiated the judicial reviews to
due petitions from Wisconsin as well as Mississippi to re-establish confessing privilege laws as
same as in Texas. The Mississippi laws will have only closed the abortion hospitals in a state. By
rejecting to consider the matters, the Court protected the assistance for a concept that the
meeting of limitations that force the females to travel to get the abortion, can be the unauthorised
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
ABORTION 4
impairment to female's rights to access security as well as lawful abortion care. Notwithstanding
the rulings, various hospitals in Texas have continued to be closed (Medoff, 2016).
Moreover, in the fields wherever the services related to abortion are becoming
progressively complex to access (involving Ohio and Texas), media report documents that
females travel somewhere else to get service. However, it is very significant to know the
experience of females who travel for abortion care (Bessett, et. al, 2017). This will be helpful in
knowing the breadth of obstacles, beyond the persons related to specific state level limitations of
abortion, which such female encounters as well as any related concerns (Jones, Ingerick &
Jerman, 2018).
Furthermore, for various females, the scope of the abortion coverage under their health
insurance, is reliant on where they alive. Since 1977, the Hyde amendments have intensely
limited the coverage of abortion under Medicaid as well as different central programs.
Progressively, various states have passed the rules to limit abortion coverage in a private
insurance marketplace (Kreitzer, 2015). At this time, twenty-six states have the legislations,
which limit the insurance coverage of abortion in private ACA market plan. Further, the eleven
of those states also restrict the abortion coverage in all states administrated plans. The state
policies of the abortion as well as the interaction with clinical practices can be understand
through the following charts-
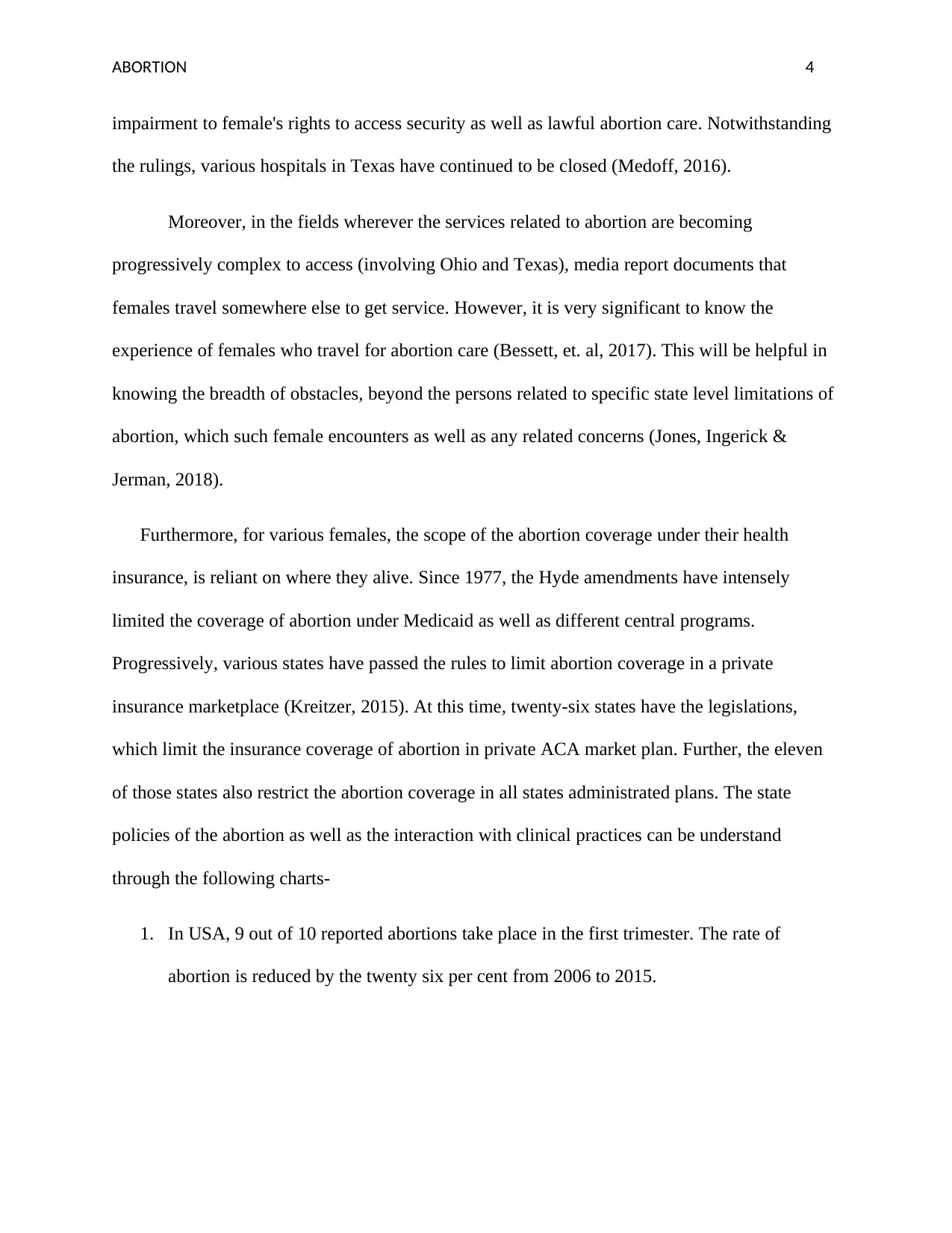
1. In USA, 9 out of 10 reported abortions take place in the first trimester. The rate of
abortion is reduced by the twenty six per cent from 2006 to 2015.
impairment to female's rights to access security as well as lawful abortion care. Notwithstanding
the rulings, various hospitals in Texas have continued to be closed (Medoff, 2016).
Moreover, in the fields wherever the services related to abortion are becoming
progressively complex to access (involving Ohio and Texas), media report documents that
females travel somewhere else to get service. However, it is very significant to know the
experience of females who travel for abortion care (Bessett, et. al, 2017). This will be helpful in
knowing the breadth of obstacles, beyond the persons related to specific state level limitations of
abortion, which such female encounters as well as any related concerns (Jones, Ingerick &
Jerman, 2018).
Furthermore, for various females, the scope of the abortion coverage under their health
insurance, is reliant on where they alive. Since 1977, the Hyde amendments have intensely
limited the coverage of abortion under Medicaid as well as different central programs.
Progressively, various states have passed the rules to limit abortion coverage in a private
insurance marketplace (Kreitzer, 2015). At this time, twenty-six states have the legislations,
which limit the insurance coverage of abortion in private ACA market plan. Further, the eleven
of those states also restrict the abortion coverage in all states administrated plans. The state
policies of the abortion as well as the interaction with clinical practices can be understand
through the following charts-
1. In USA, 9 out of 10 reported abortions take place in the first trimester. The rate of
abortion is reduced by the twenty six per cent from 2006 to 2015.
ABORTION 5
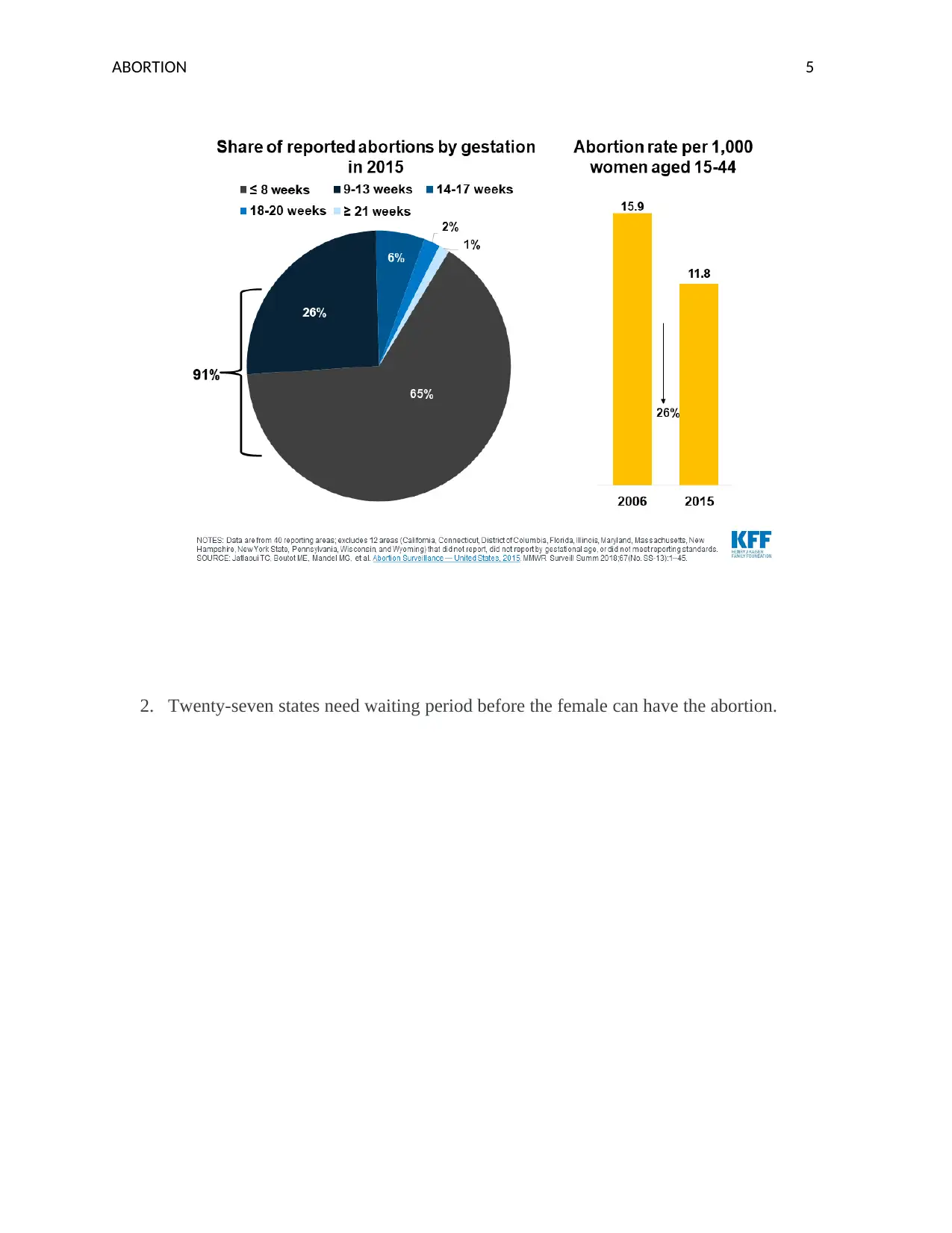
2. Twenty-seven states need waiting period before the female can have the abortion.
2. Twenty-seven states need waiting period before the female can have the abortion.
ABORTION 6
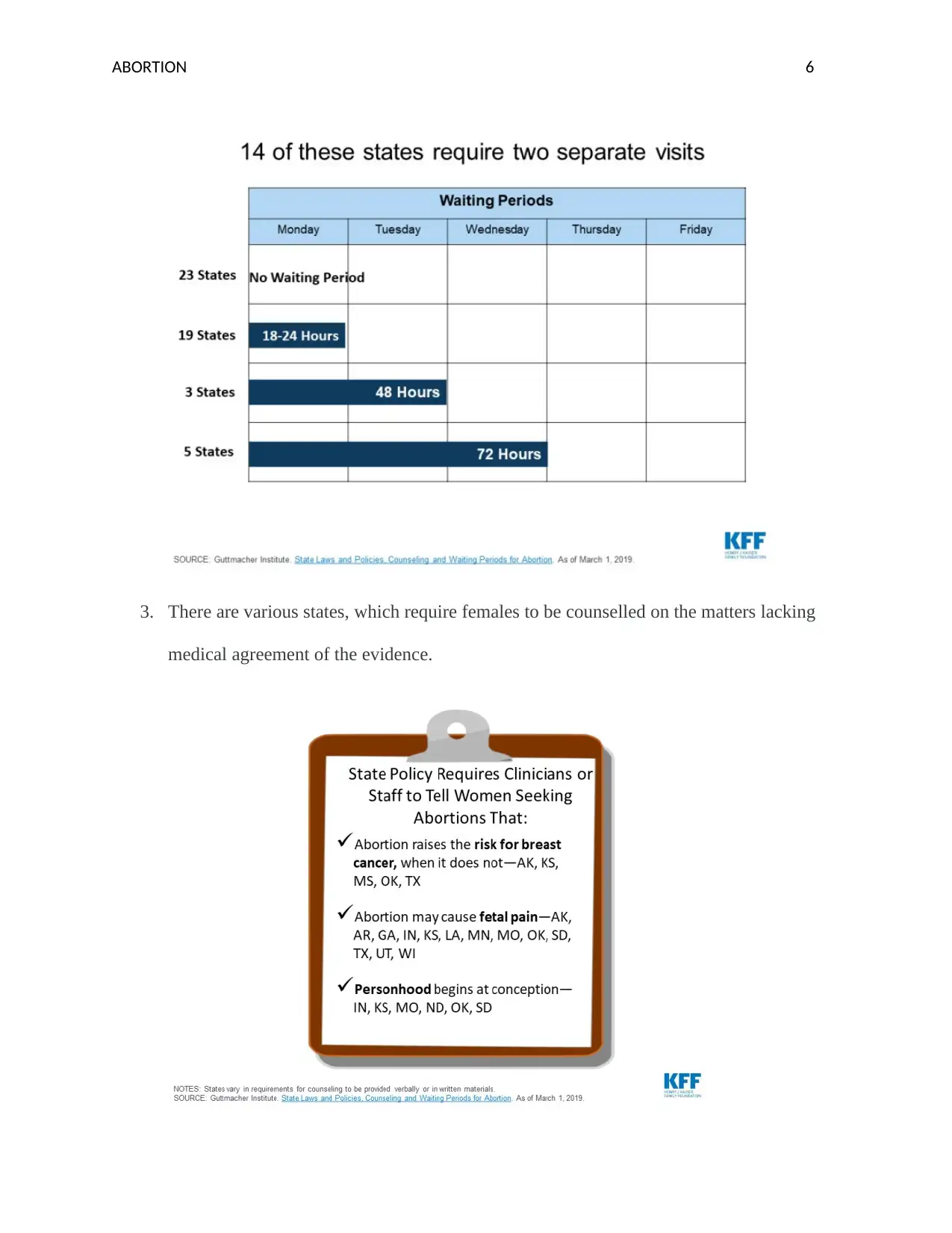
3. There are various states, which require females to be counselled on the matters lacking
medical agreement of the evidence.
3. There are various states, which require females to be counselled on the matters lacking
medical agreement of the evidence.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
ABORTION 7
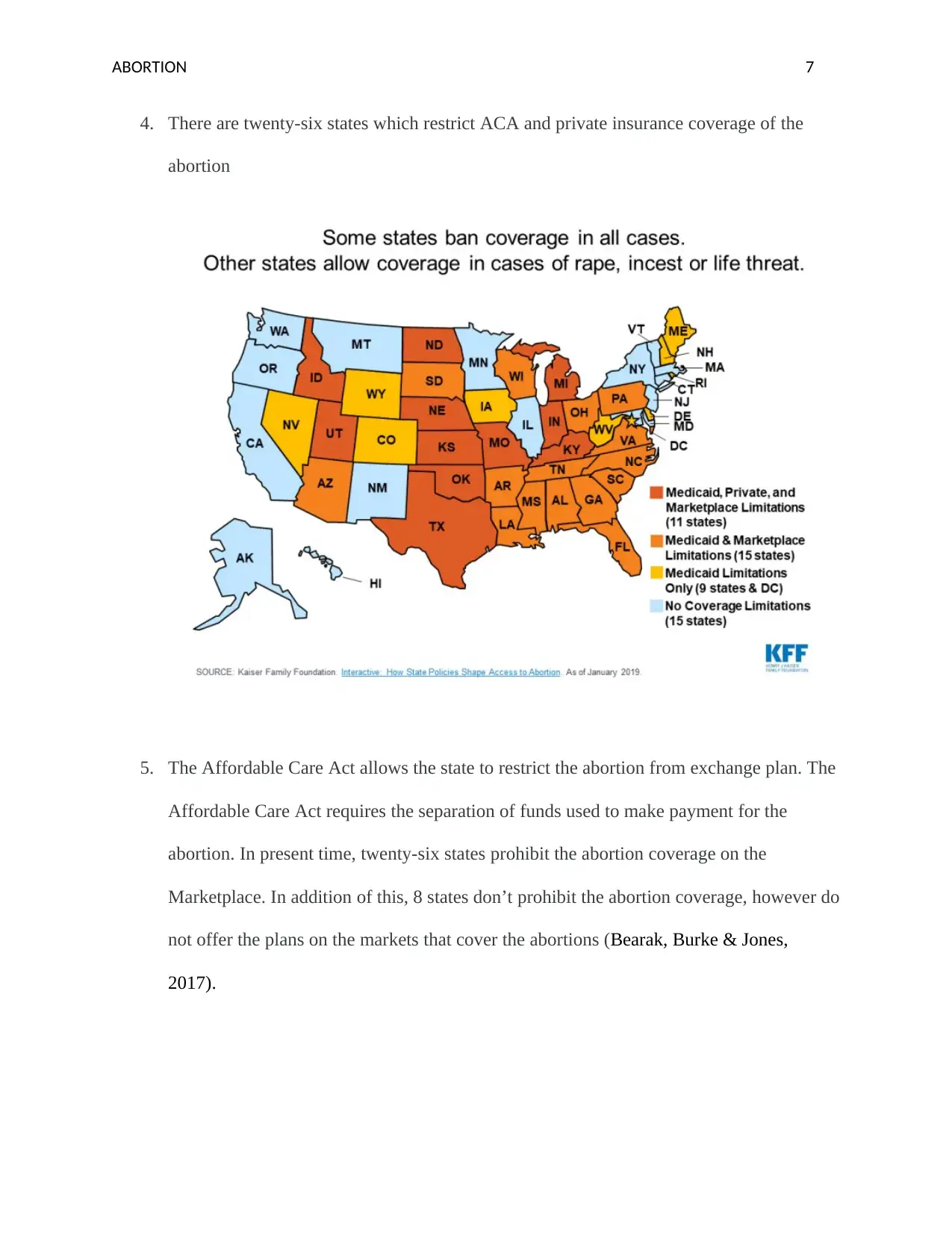
4. There are twenty-six states which restrict ACA and private insurance coverage of the
abortion
5. The Affordable Care Act allows the state to restrict the abortion from exchange plan. The
Affordable Care Act requires the separation of funds used to make payment for the
abortion. In present time, twenty-six states prohibit the abortion coverage on the
Marketplace. In addition of this, 8 states don’t prohibit the abortion coverage, however do
not offer the plans on the markets that cover the abortions (Bearak, Burke & Jones,
2017).
4. There are twenty-six states which restrict ACA and private insurance coverage of the
abortion
5. The Affordable Care Act allows the state to restrict the abortion from exchange plan. The
Affordable Care Act requires the separation of funds used to make payment for the
abortion. In present time, twenty-six states prohibit the abortion coverage on the
Marketplace. In addition of this, 8 states don’t prohibit the abortion coverage, however do
not offer the plans on the markets that cover the abortions (Bearak, Burke & Jones,
2017).
ABORTION 8
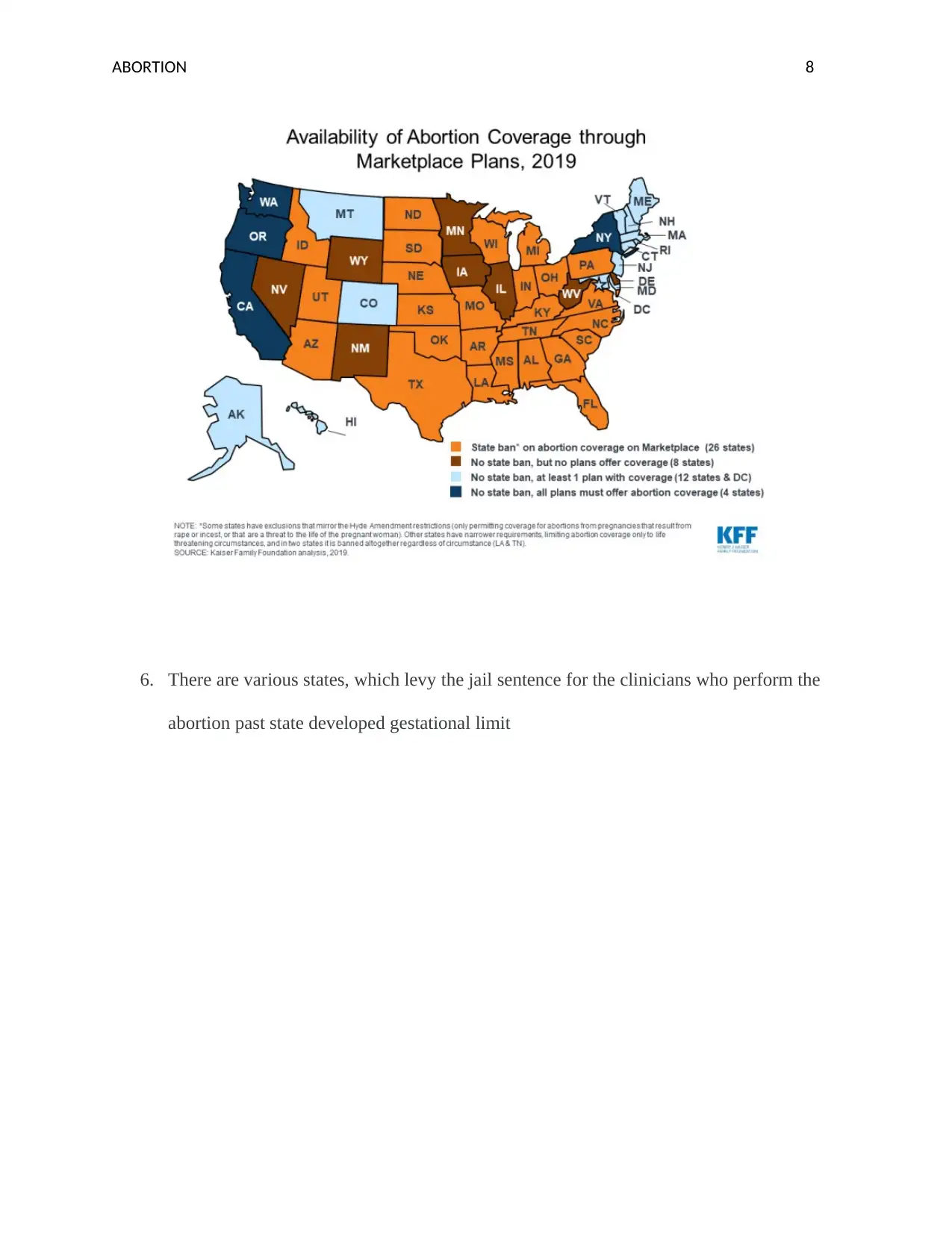
6. There are various states, which levy the jail sentence for the clinicians who perform the
abortion past state developed gestational limit
6. There are various states, which levy the jail sentence for the clinicians who perform the
abortion past state developed gestational limit
ABORTION 9
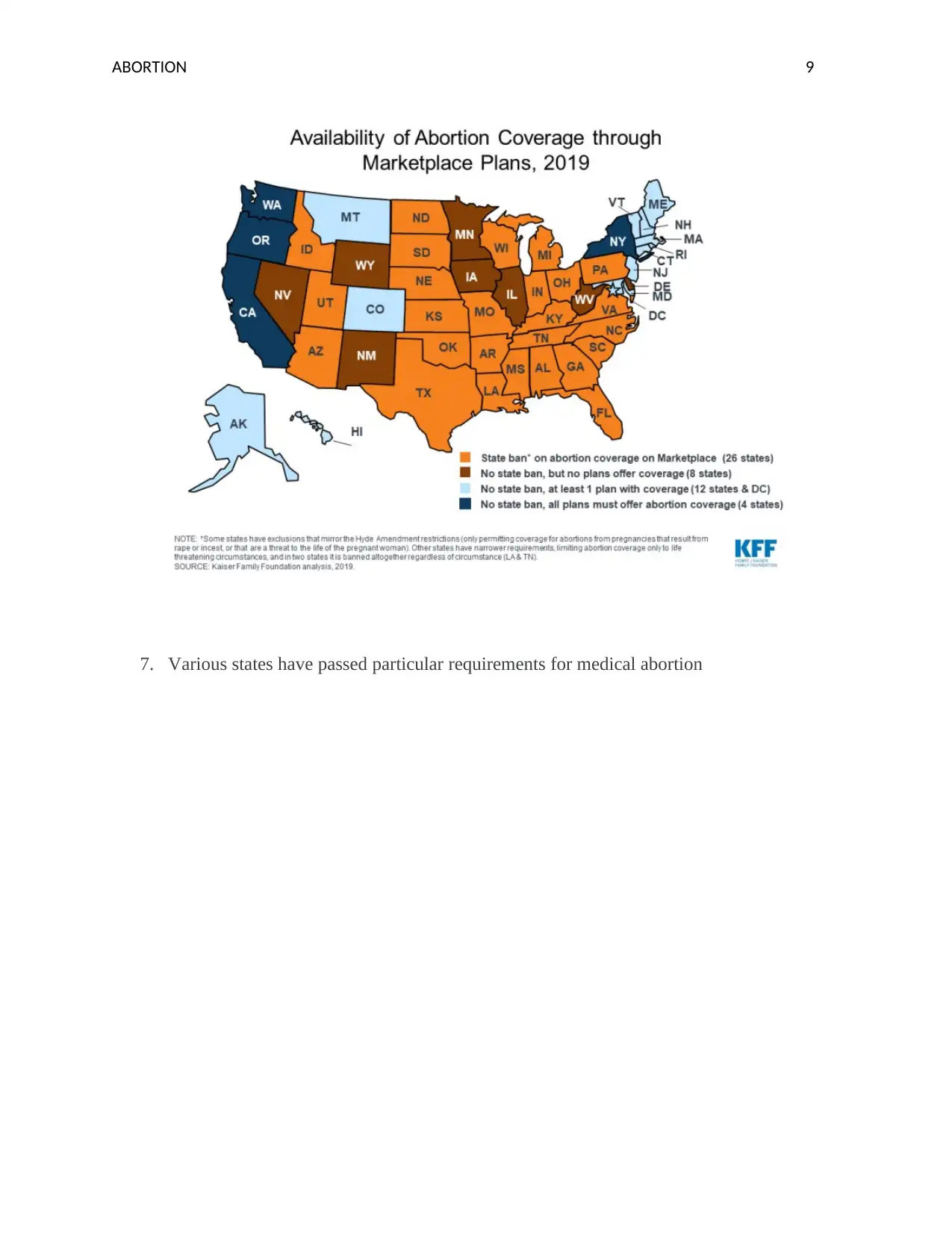
7. Various states have passed particular requirements for medical abortion
7. Various states have passed particular requirements for medical abortion
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

ABORTION 10
Additionally, the abortion is not well unified in the primary care in USA, and even
amongst obstetrician gynaecologists, there is the absence of providers providing the abortion
care. The prospective providers face various obstacles. The main obstacle is absence of the
training. From the year 1996, the Accreditation Council for Graduate Medical Education has
required obstetrics as well as gynecology position program to involve the training related to
abortion. These programs do not render all the types of training. These residency programs only
render the training on separate basis. The only good way is to address the lack of training is to
command this in the state law. The California passed the laws in year 2002 that mirrors the
Accreditation Council for Graduate Medical Education certification requirements. Furthermore,
Additionally, the abortion is not well unified in the primary care in USA, and even
amongst obstetrician gynaecologists, there is the absence of providers providing the abortion
care. The prospective providers face various obstacles. The main obstacle is absence of the
training. From the year 1996, the Accreditation Council for Graduate Medical Education has
required obstetrics as well as gynecology position program to involve the training related to
abortion. These programs do not render all the types of training. These residency programs only
render the training on separate basis. The only good way is to address the lack of training is to
command this in the state law. The California passed the laws in year 2002 that mirrors the
Accreditation Council for Graduate Medical Education certification requirements. Furthermore,
ABORTION 11
the state may go by needing the training for abortion care for the wider ranges of the doctors,
such as family medicine as well as the internal medicine clinicians (Upadhyay, 2017).
The other way to enhance the amalgamation of abortion provider is to permit advanced
practice clinicians to render medicine as well as medical abortion care in first trimester. The law
passed by California expands the provisions to nurse doctors, authorised nurse-midwives, as well
as the surgeon assistant (Freedman, et. al, 2017). This law was passed after the five-year pilot
program to determine that APCs render the high quality as well as secure services related to
abortion comparable with the physician. There are certain states, where the litigation can also be
the helpful tool. For instance, the matters challenging physician-only abortion provision laws are
due in Montana and Maine. In USA, the persons are progressively accessing the health related
products as well as the services in new manners. These new ways can be online drugstores,
computer-generated telehealth advices and the apps, which help the persons to manage the
various issues of health.
In addition, the telemedicine is a proper and secure manner of increasing access to
medication abortion. The telemedicine is already accessible in minimum ten states. However,
seventeen states properly or clearly prohibit the provisions of medication abortion through the
clinicians who are not available in person with the patients. By stimulating the prohibitions as
well as supporting the telemedicine performances, the local lawmakers may ease the access to
underserved groups, increase access to other group of the patients, and fill gap made by the
progressively hostile policy atmosphere. In order to make sure the reasonable access to the
model of care, policy makers should also mandate that Medicaid and individual insurance plan
not only contain the abortion care, however also contain telehealth service to a similar scope as
the care in person.
the state may go by needing the training for abortion care for the wider ranges of the doctors,
such as family medicine as well as the internal medicine clinicians (Upadhyay, 2017).
The other way to enhance the amalgamation of abortion provider is to permit advanced
practice clinicians to render medicine as well as medical abortion care in first trimester. The law
passed by California expands the provisions to nurse doctors, authorised nurse-midwives, as well
as the surgeon assistant (Freedman, et. al, 2017). This law was passed after the five-year pilot
program to determine that APCs render the high quality as well as secure services related to
abortion comparable with the physician. There are certain states, where the litigation can also be
the helpful tool. For instance, the matters challenging physician-only abortion provision laws are
due in Montana and Maine. In USA, the persons are progressively accessing the health related
products as well as the services in new manners. These new ways can be online drugstores,
computer-generated telehealth advices and the apps, which help the persons to manage the
various issues of health.
In addition, the telemedicine is a proper and secure manner of increasing access to
medication abortion. The telemedicine is already accessible in minimum ten states. However,
seventeen states properly or clearly prohibit the provisions of medication abortion through the
clinicians who are not available in person with the patients. By stimulating the prohibitions as
well as supporting the telemedicine performances, the local lawmakers may ease the access to
underserved groups, increase access to other group of the patients, and fill gap made by the
progressively hostile policy atmosphere. In order to make sure the reasonable access to the
model of care, policy makers should also mandate that Medicaid and individual insurance plan
not only contain the abortion care, however also contain telehealth service to a similar scope as
the care in person.
ABORTION 12
In conclusion, it can say that the abortion is a very difficult factor of the human rights and
procreative health care. This is authoritative that the policymaker works toward decreasing all
the barriers to the services of abortion. It can also see that the other way is to increase the access
to abortion. It will be helpful for promoting the approaches as well as strategies that support the
people who self-handle the abortion. In this way, the medication abortion may be properly as
well as securely self-handled. In USA, there are certain females who have opted to self-handle
the abortion. These trends would be possibly enhanced in upcoming periods to come, both as the
responses to reducing the access as well as because secured and proper self-management offers
increased secrecy as well as sovereignty for the various persons.
In conclusion, it can say that the abortion is a very difficult factor of the human rights and
procreative health care. This is authoritative that the policymaker works toward decreasing all
the barriers to the services of abortion. It can also see that the other way is to increase the access
to abortion. It will be helpful for promoting the approaches as well as strategies that support the
people who self-handle the abortion. In this way, the medication abortion may be properly as
well as securely self-handled. In USA, there are certain females who have opted to self-handle
the abortion. These trends would be possibly enhanced in upcoming periods to come, both as the
responses to reducing the access as well as because secured and proper self-management offers
increased secrecy as well as sovereignty for the various persons.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
ABORTION 13
References
Bearak, J. M., Burke, K. L., & Jones, R. K. (2017). Disparities and change over time in distance
women would need to travel to have an abortion in the USA: a spatial analysis. The
Lancet Public Health, 2(11), e493-e500.
Bessett, D., Gerdts, C., Littman, L. L., Kavanaugh, M. L., & Norris, A. (2015). Does state-level
context matter for individuals' knowledge about abortion, legality and health?
Challenging the ‘red states v. blue states’ hypothesis. Culture, health & sexuality, 17(6),
733-746.
Conti, J. A., Brant, A. R., Shumaker, H. D., & Reeves, M. F. (2016). Update on abortion
policy. Current Opinion in Obstetrics and Gynecology, 28(6), 517-521.
Francome, C. (2017). Abortion in the USA and the UK. Routledge.
Freedman, L., Langton, C., Landy, U., Ly, E., & Rocca, C. (2017). Abortion care policies and
enforcement in US obstetrics–gynecology teaching hospitals: a national
survey. Contraception, 96(4), 265.
Gomez, I., Sobel, L., Salganicoff, A., Jankiewicz, A., & Rousseau, D. (2016). Intersection of
State Abortion Policy and Clinical Practice. Jama, 316(14), 1438-1438.
References
Bearak, J. M., Burke, K. L., & Jones, R. K. (2017). Disparities and change over time in distance
women would need to travel to have an abortion in the USA: a spatial analysis. The
Lancet Public Health, 2(11), e493-e500.
Bessett, D., Gerdts, C., Littman, L. L., Kavanaugh, M. L., & Norris, A. (2015). Does state-level
context matter for individuals' knowledge about abortion, legality and health?
Challenging the ‘red states v. blue states’ hypothesis. Culture, health & sexuality, 17(6),
733-746.
Conti, J. A., Brant, A. R., Shumaker, H. D., & Reeves, M. F. (2016). Update on abortion
policy. Current Opinion in Obstetrics and Gynecology, 28(6), 517-521.
Francome, C. (2017). Abortion in the USA and the UK. Routledge.
Freedman, L., Langton, C., Landy, U., Ly, E., & Rocca, C. (2017). Abortion care policies and
enforcement in US obstetrics–gynecology teaching hospitals: a national
survey. Contraception, 96(4), 265.
Gomez, I., Sobel, L., Salganicoff, A., Jankiewicz, A., & Rousseau, D. (2016). Intersection of
State Abortion Policy and Clinical Practice. Jama, 316(14), 1438-1438.
ABORTION 14
Grossman, D. (2017). Sexual and reproductive health under the Trump presidency: policy
change threatens women in the USA and worldwide. J Fam Plann Reprod Health
Care, 43(2), 89-91.
Jones, R. K., Ingerick, M., & Jerman, J. (2018). Differences in abortion service delivery in
hostile, middle-ground, and supportive states in 2014. Women's Health Issues, 28(3),
212-218.
Kreitzer, R. J. (2015). Politics and morality in state abortion policy. State Politics & Policy
Quarterly, 15(1), 41-66.
Medoff, M. H. (2016). State abortion policy and unintended birth rates in the United
States. Social Indicators Research, 129(2), 589-600.
Mucciaroni, G., Ferraiolo, K., & Rubado, M. E. (2019). Framing morality policy issues: state
legislative debates on abortion restrictions. Policy Sciences, 52(2), 171-189.
Piazza, J. A. (2017). The determinants of domestic right-wing terrorism in the USA: Economic
grievance, societal change and political resentment. Conflict management and peace
science, 34(1), 52-80.
Upadhyay, U. D. (2017). Innovative models are needed for equitable abortion access in the
USA. The Lancet Public Health, 2(11), e484-e485.
Grossman, D. (2017). Sexual and reproductive health under the Trump presidency: policy
change threatens women in the USA and worldwide. J Fam Plann Reprod Health
Care, 43(2), 89-91.
Jones, R. K., Ingerick, M., & Jerman, J. (2018). Differences in abortion service delivery in
hostile, middle-ground, and supportive states in 2014. Women's Health Issues, 28(3),
212-218.
Kreitzer, R. J. (2015). Politics and morality in state abortion policy. State Politics & Policy
Quarterly, 15(1), 41-66.
Medoff, M. H. (2016). State abortion policy and unintended birth rates in the United
States. Social Indicators Research, 129(2), 589-600.
Mucciaroni, G., Ferraiolo, K., & Rubado, M. E. (2019). Framing morality policy issues: state
legislative debates on abortion restrictions. Policy Sciences, 52(2), 171-189.
Piazza, J. A. (2017). The determinants of domestic right-wing terrorism in the USA: Economic
grievance, societal change and political resentment. Conflict management and peace
science, 34(1), 52-80.
Upadhyay, U. D. (2017). Innovative models are needed for equitable abortion access in the
USA. The Lancet Public Health, 2(11), e484-e485.
1 out of 15
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.