Implementing Effective Discharge Plan for Tom
VerifiedAdded on 2021/04/17
|11
|3150
|74
AI Summary
The assignment requires considering multiple aspects to reduce clinical complications and prevent deterioration in patients with co-morbid conditions like cardiovascular conditions and external factors such as cigarette smoking and anaesthesia. An effective discharge plan was implemented for Tom, taking into account various references from medical literature.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Acute Care Across the Lifespan-
Nursing
Nursing
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Introduction:
Tom is a 72 years old gentleman who underwent left sigmoid colectomy. Also, he has a
medical histories of hypertension and hyperlipidaemia and consuming medications for this.
He has history of 40 years of smoking. Nursing care plan for the first 24 hours will be
demonstrated with physical and psychosocial needs of Tom. As Tom has a multiple
conditions, there is possibility of several clinical complications postoperative. These are
mainly due to the smoking, cardiovascular conditions and anaesthesia during the surgery. It
will be discussed in the essay. Smooth transition to the society can be achieved by
implementing suitable discharge plan.
Tom is a 72 years old gentleman who underwent left sigmoid colectomy. Also, he has a
medical histories of hypertension and hyperlipidaemia and consuming medications for this.
He has history of 40 years of smoking. Nursing care plan for the first 24 hours will be
demonstrated with physical and psychosocial needs of Tom. As Tom has a multiple
conditions, there is possibility of several clinical complications postoperative. These are
mainly due to the smoking, cardiovascular conditions and anaesthesia during the surgery. It
will be discussed in the essay. Smooth transition to the society can be achieved by
implementing suitable discharge plan.
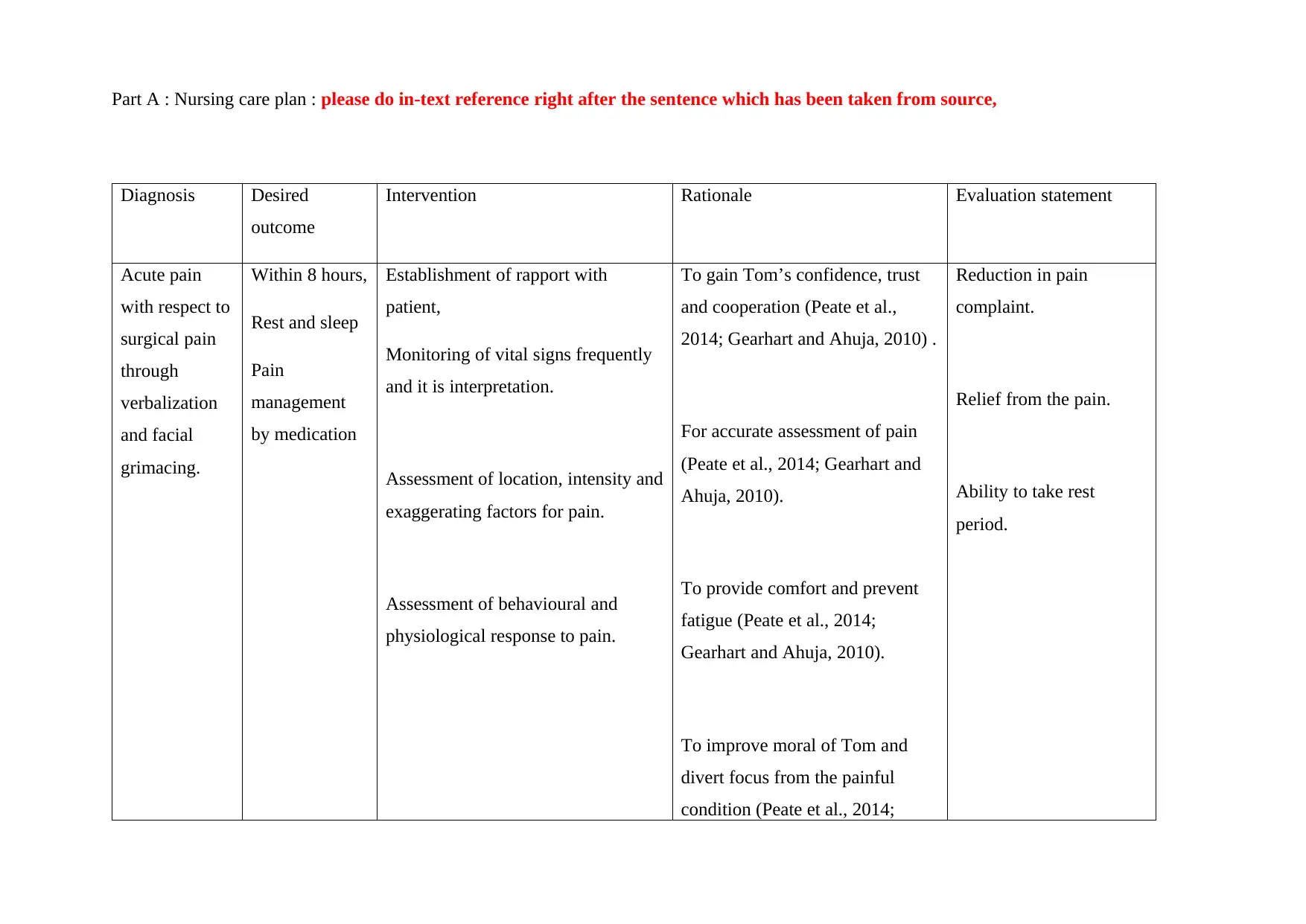
Part A : Nursing care plan : please do in-text reference right after the sentence which has been taken from source,
Diagnosis Desired
outcome
Intervention Rationale Evaluation statement
Acute pain
with respect to
surgical pain
through
verbalization
and facial
grimacing.
Within 8 hours,
Rest and sleep
Pain
management
by medication
Establishment of rapport with
patient,
Monitoring of vital signs frequently
and it is interpretation.
Assessment of location, intensity and
exaggerating factors for pain.
Assessment of behavioural and
physiological response to pain.
To gain Tom’s confidence, trust
and cooperation (Peate et al.,
2014; Gearhart and Ahuja, 2010) .
For accurate assessment of pain
(Peate et al., 2014; Gearhart and
Ahuja, 2010).
To provide comfort and prevent
fatigue (Peate et al., 2014;
Gearhart and Ahuja, 2010).
To improve moral of Tom and
divert focus from the painful
condition (Peate et al., 2014;
Reduction in pain
complaint.
Relief from the pain.
Ability to take rest
period.
Diagnosis Desired
outcome
Intervention Rationale Evaluation statement
Acute pain
with respect to
surgical pain
through
verbalization
and facial
grimacing.
Within 8 hours,
Rest and sleep
Pain
management
by medication
Establishment of rapport with
patient,
Monitoring of vital signs frequently
and it is interpretation.
Assessment of location, intensity and
exaggerating factors for pain.
Assessment of behavioural and
physiological response to pain.
To gain Tom’s confidence, trust
and cooperation (Peate et al.,
2014; Gearhart and Ahuja, 2010) .
For accurate assessment of pain
(Peate et al., 2014; Gearhart and
Ahuja, 2010).
To provide comfort and prevent
fatigue (Peate et al., 2014;
Gearhart and Ahuja, 2010).
To improve moral of Tom and
divert focus from the painful
condition (Peate et al., 2014;
Reduction in pain
complaint.
Relief from the pain.
Ability to take rest
period.
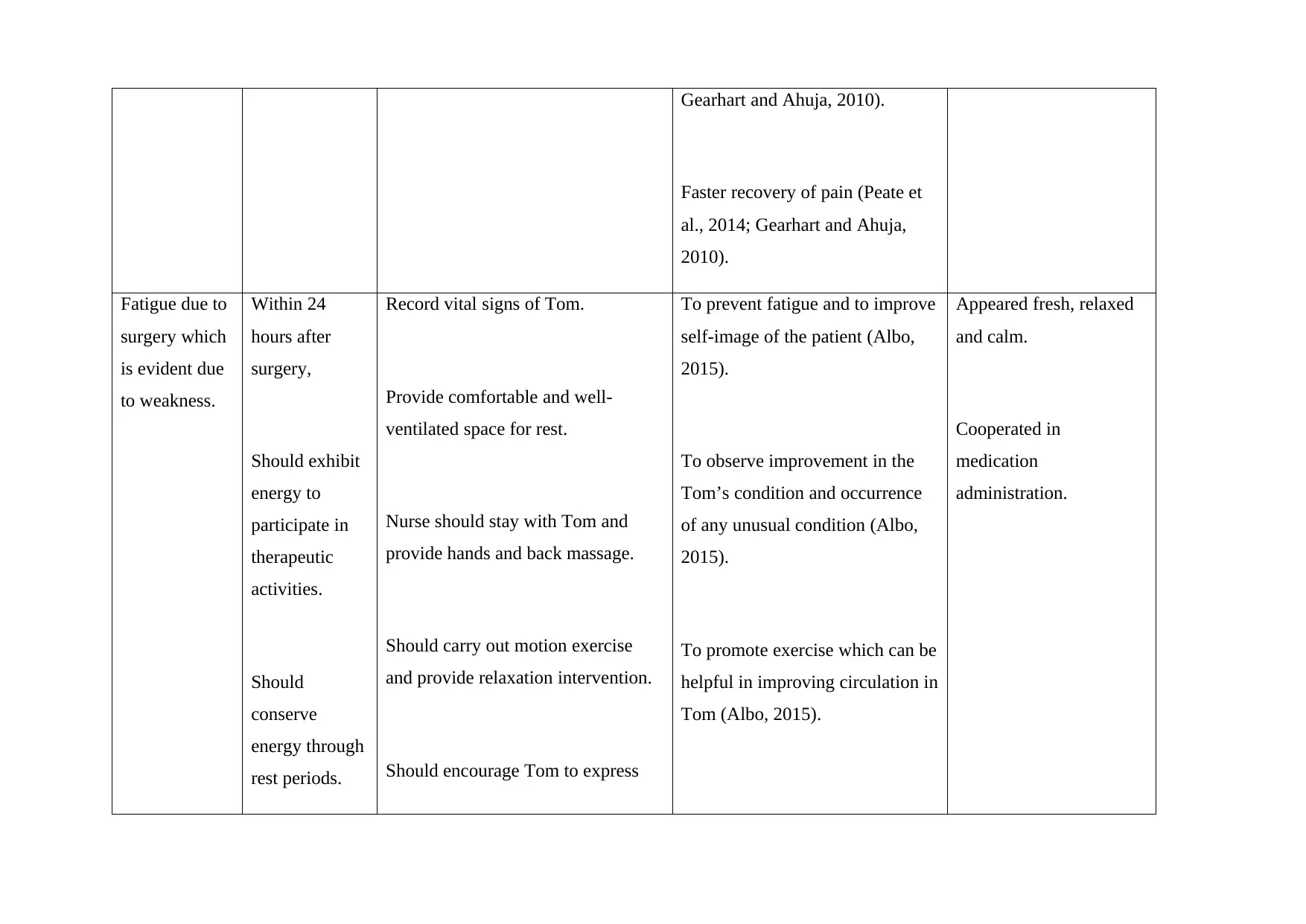
Gearhart and Ahuja, 2010).
Faster recovery of pain (Peate et
al., 2014; Gearhart and Ahuja,
2010).
Fatigue due to
surgery which
is evident due
to weakness.
Within 24
hours after
surgery,
Should exhibit
energy to
participate in
therapeutic
activities.
Should
conserve
energy through
rest periods.
Record vital signs of Tom.
Provide comfortable and well-
ventilated space for rest.
Nurse should stay with Tom and
provide hands and back massage.
Should carry out motion exercise
and provide relaxation intervention.
Should encourage Tom to express
To prevent fatigue and to improve
self-image of the patient (Albo,
2015).
To observe improvement in the
Tom’s condition and occurrence
of any unusual condition (Albo,
2015).
To promote exercise which can be
helpful in improving circulation in
Tom (Albo, 2015).
Appeared fresh, relaxed
and calm.
Cooperated in
medication
administration.
Faster recovery of pain (Peate et
al., 2014; Gearhart and Ahuja,
2010).
Fatigue due to
surgery which
is evident due
to weakness.
Within 24
hours after
surgery,
Should exhibit
energy to
participate in
therapeutic
activities.
Should
conserve
energy through
rest periods.
Record vital signs of Tom.
Provide comfortable and well-
ventilated space for rest.
Nurse should stay with Tom and
provide hands and back massage.
Should carry out motion exercise
and provide relaxation intervention.
Should encourage Tom to express
To prevent fatigue and to improve
self-image of the patient (Albo,
2015).
To observe improvement in the
Tom’s condition and occurrence
of any unusual condition (Albo,
2015).
To promote exercise which can be
helpful in improving circulation in
Tom (Albo, 2015).
Appeared fresh, relaxed
and calm.
Cooperated in
medication
administration.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
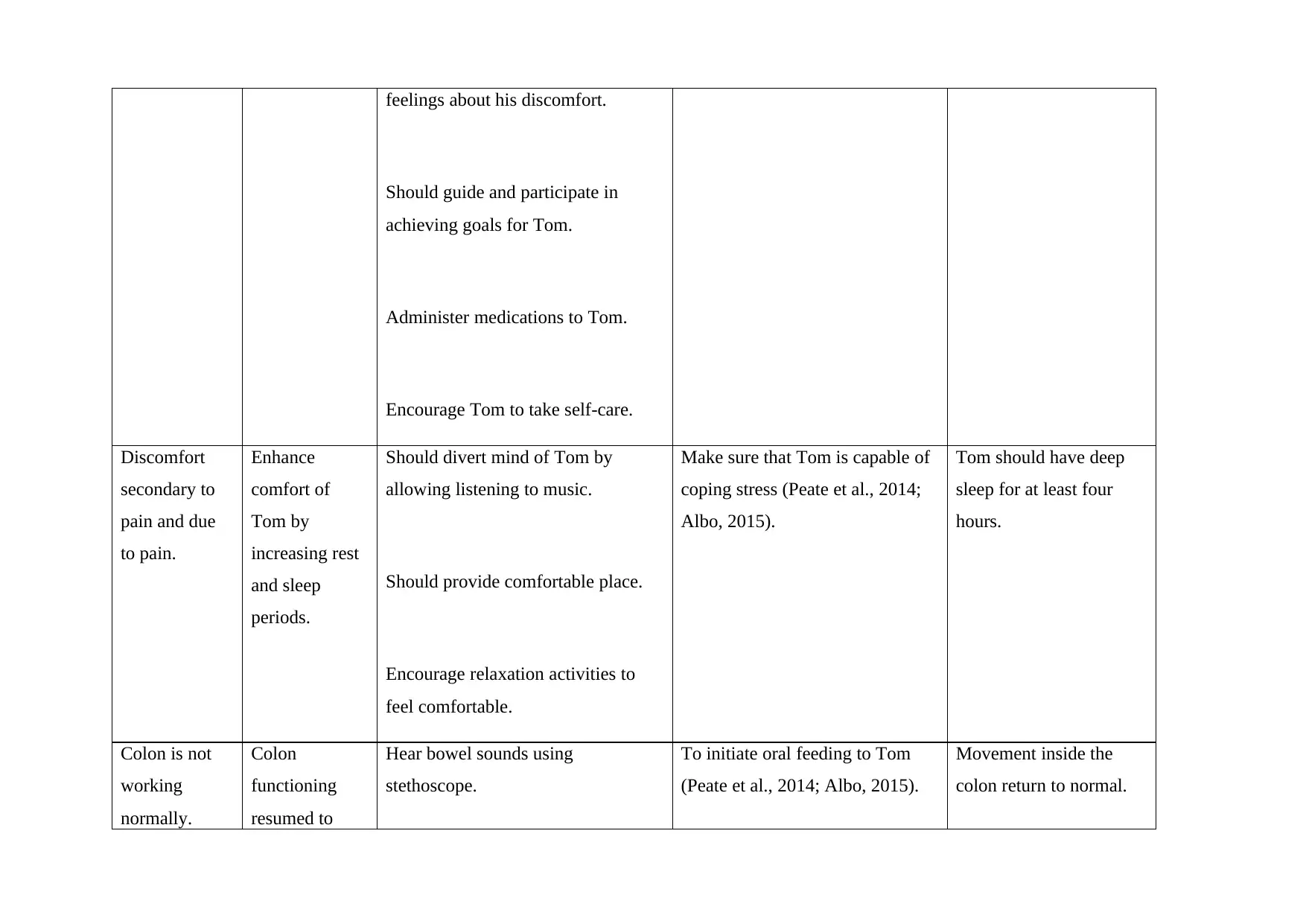
feelings about his discomfort.
Should guide and participate in
achieving goals for Tom.
Administer medications to Tom.
Encourage Tom to take self-care.
Discomfort
secondary to
pain and due
to pain.
Enhance
comfort of
Tom by
increasing rest
and sleep
periods.
Should divert mind of Tom by
allowing listening to music.
Should provide comfortable place.
Encourage relaxation activities to
feel comfortable.
Make sure that Tom is capable of
coping stress (Peate et al., 2014;
Albo, 2015).
Tom should have deep
sleep for at least four
hours.
Colon is not
working
normally.
Colon
functioning
resumed to
Hear bowel sounds using
stethoscope.
To initiate oral feeding to Tom
(Peate et al., 2014; Albo, 2015).
Movement inside the
colon return to normal.
Should guide and participate in
achieving goals for Tom.
Administer medications to Tom.
Encourage Tom to take self-care.
Discomfort
secondary to
pain and due
to pain.
Enhance
comfort of
Tom by
increasing rest
and sleep
periods.
Should divert mind of Tom by
allowing listening to music.
Should provide comfortable place.
Encourage relaxation activities to
feel comfortable.
Make sure that Tom is capable of
coping stress (Peate et al., 2014;
Albo, 2015).
Tom should have deep
sleep for at least four
hours.
Colon is not
working
normally.
Colon
functioning
resumed to
Hear bowel sounds using
stethoscope.
To initiate oral feeding to Tom
(Peate et al., 2014; Albo, 2015).
Movement inside the
colon return to normal.
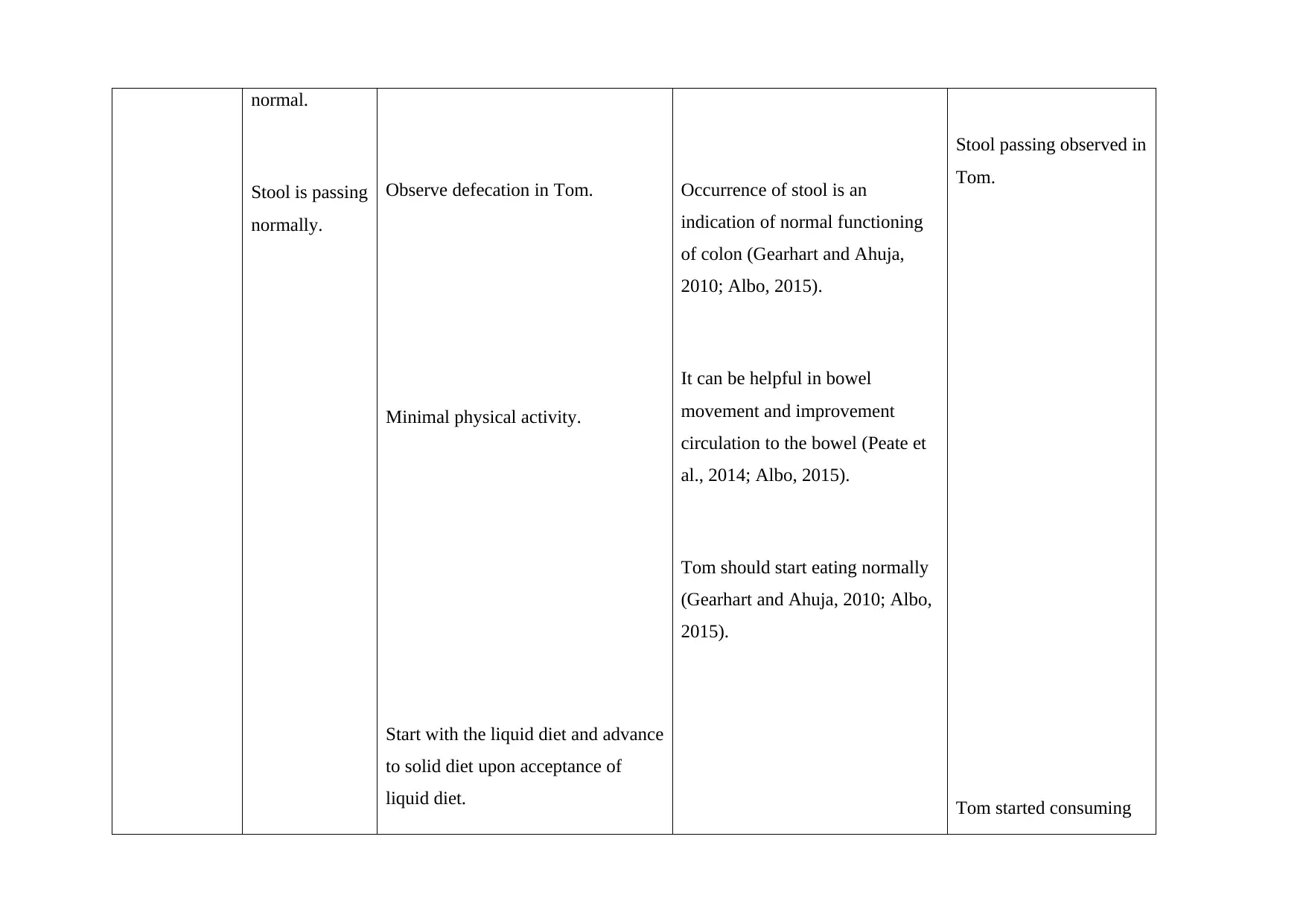
normal.
Stool is passing
normally.
Observe defecation in Tom.
Minimal physical activity.
Start with the liquid diet and advance
to solid diet upon acceptance of
liquid diet.
Occurrence of stool is an
indication of normal functioning
of colon (Gearhart and Ahuja,
2010; Albo, 2015).
It can be helpful in bowel
movement and improvement
circulation to the bowel (Peate et
al., 2014; Albo, 2015).
Tom should start eating normally
(Gearhart and Ahuja, 2010; Albo,
2015).
Stool passing observed in
Tom.
Tom started consuming
Stool is passing
normally.
Observe defecation in Tom.
Minimal physical activity.
Start with the liquid diet and advance
to solid diet upon acceptance of
liquid diet.
Occurrence of stool is an
indication of normal functioning
of colon (Gearhart and Ahuja,
2010; Albo, 2015).
It can be helpful in bowel
movement and improvement
circulation to the bowel (Peate et
al., 2014; Albo, 2015).
Tom should start eating normally
(Gearhart and Ahuja, 2010; Albo,
2015).
Stool passing observed in
Tom.
Tom started consuming
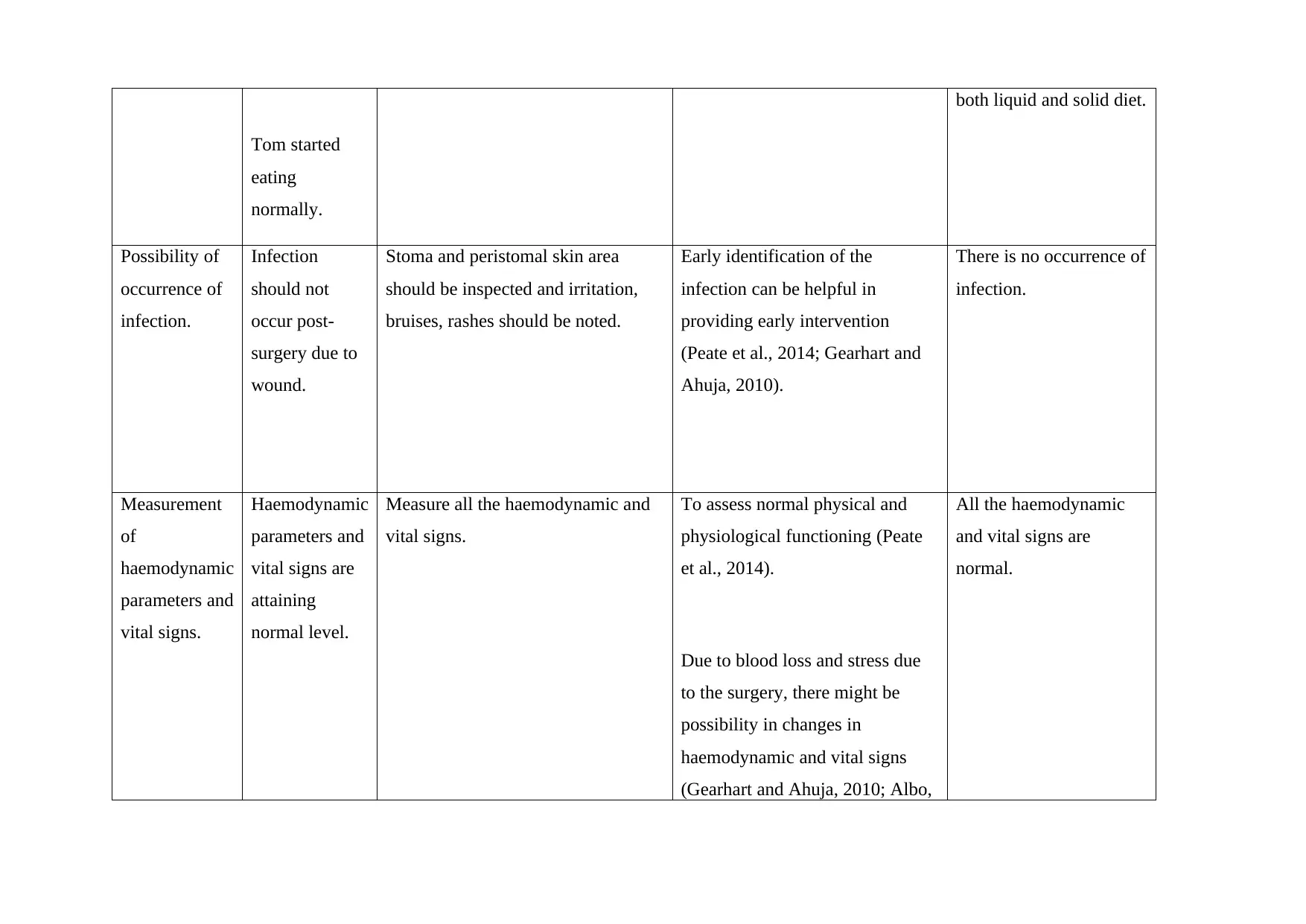
Tom started
eating
normally.
both liquid and solid diet.
Possibility of
occurrence of
infection.
Infection
should not
occur post-
surgery due to
wound.
Stoma and peristomal skin area
should be inspected and irritation,
bruises, rashes should be noted.
Early identification of the
infection can be helpful in
providing early intervention
(Peate et al., 2014; Gearhart and
Ahuja, 2010).
There is no occurrence of
infection.
Measurement
of
haemodynamic
parameters and
vital signs.
Haemodynamic
parameters and
vital signs are
attaining
normal level.
Measure all the haemodynamic and
vital signs.
To assess normal physical and
physiological functioning (Peate
et al., 2014).
Due to blood loss and stress due
to the surgery, there might be
possibility in changes in
haemodynamic and vital signs
(Gearhart and Ahuja, 2010; Albo,
All the haemodynamic
and vital signs are
normal.
eating
normally.
both liquid and solid diet.
Possibility of
occurrence of
infection.
Infection
should not
occur post-
surgery due to
wound.
Stoma and peristomal skin area
should be inspected and irritation,
bruises, rashes should be noted.
Early identification of the
infection can be helpful in
providing early intervention
(Peate et al., 2014; Gearhart and
Ahuja, 2010).
There is no occurrence of
infection.
Measurement
of
haemodynamic
parameters and
vital signs.
Haemodynamic
parameters and
vital signs are
attaining
normal level.
Measure all the haemodynamic and
vital signs.
To assess normal physical and
physiological functioning (Peate
et al., 2014).
Due to blood loss and stress due
to the surgery, there might be
possibility in changes in
haemodynamic and vital signs
(Gearhart and Ahuja, 2010; Albo,
All the haemodynamic
and vital signs are
normal.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2015).
Part B : Needs 800-1000 words
Smoking cessation should be there prior to surgery. Smoking can produce sudden and long-
term increase in the blood pressure, increase in heart rate, increased chances of blood clots,
doubled chances of stroke and more chances of blood vessel damage. Hence, it is advisable to
stop smoking at least 8 weeks prior to surgery and if not possible ate least 8 hours prior to
surgery. If smoking doesn’t stop prior to surgery, there is possibility that anaesthesia would
not exhibit desired effect. Hydrocarbons present in the cigarette smoke can produce multiple
effects like injury to arterial endothelium, initiation of atherosclerotic process, reduced level
of high-density lipoproteins and plaque formation. In addition to this nicotine present in the
cigarette can stimulate catecholamines release, augmented heart rate and hypertension.
Augmented levels of carbon monoxide present in the cigarette smoke can drastically reduce
myocardial oxygen delivery. Cigarette smoke can increase oxidative stress which can lead to
leucocyte activation and platelet activation, lipid peroxidation and release of adhesion and
inflammatory molecules (Messner and Bernhard, 2014). All these conditions can exaggerate
cardiovascular conditions. Moreover, anaesthesia exhibit opposite effect on cardiovascular
parameters like reduction in blood pressure and heart rate. In smokers, there can be
possibility of interference in the pulse oximeter reading and requirement of deep anaesthesia
(Zachariah and Basker, 2012).
Smoking can exhibit, respiratory problems and cardiovascular problems both during and after
anaesthesia. This respiratory problem includes interference in the oxygen uptake which
results in the higher arterial to end tidal carbon dioxide differences. Hence, during first 24
hours, there is more requirement of oxygen therapy and analgesics. Smoking can also exhibit
diverse effects on muscle relaxants. Hence, proper anaesthesia cannot be given in smoking
person during surgery. Due to smoking, there might be requirement of ventilator, which can
lead to pneumonia. Smoking can result in reduced blood flow which can affect healing
process at the surgery spot and also it can lead to increased chances of infection. In smokers it
is evident that increased production of Hb, red blood cells and fibrinogen. It can lead to rise
in the haematocrit and blood viscosity. It can lead increased thrombotic incidence (Mahlmann
et al., 2013; Scholes et al., 2009).
Incision during surgery during can produce wound. Smoking can interfere with the wound
healing because for wound healing basic requirement in oxygen. In smokers, there can be
increased levels of carbon monoxide and reduced levels of oxygen in their blood. Due to this
Smoking cessation should be there prior to surgery. Smoking can produce sudden and long-
term increase in the blood pressure, increase in heart rate, increased chances of blood clots,
doubled chances of stroke and more chances of blood vessel damage. Hence, it is advisable to
stop smoking at least 8 weeks prior to surgery and if not possible ate least 8 hours prior to
surgery. If smoking doesn’t stop prior to surgery, there is possibility that anaesthesia would
not exhibit desired effect. Hydrocarbons present in the cigarette smoke can produce multiple
effects like injury to arterial endothelium, initiation of atherosclerotic process, reduced level
of high-density lipoproteins and plaque formation. In addition to this nicotine present in the
cigarette can stimulate catecholamines release, augmented heart rate and hypertension.
Augmented levels of carbon monoxide present in the cigarette smoke can drastically reduce
myocardial oxygen delivery. Cigarette smoke can increase oxidative stress which can lead to
leucocyte activation and platelet activation, lipid peroxidation and release of adhesion and
inflammatory molecules (Messner and Bernhard, 2014). All these conditions can exaggerate
cardiovascular conditions. Moreover, anaesthesia exhibit opposite effect on cardiovascular
parameters like reduction in blood pressure and heart rate. In smokers, there can be
possibility of interference in the pulse oximeter reading and requirement of deep anaesthesia
(Zachariah and Basker, 2012).
Smoking can exhibit, respiratory problems and cardiovascular problems both during and after
anaesthesia. This respiratory problem includes interference in the oxygen uptake which
results in the higher arterial to end tidal carbon dioxide differences. Hence, during first 24
hours, there is more requirement of oxygen therapy and analgesics. Smoking can also exhibit
diverse effects on muscle relaxants. Hence, proper anaesthesia cannot be given in smoking
person during surgery. Due to smoking, there might be requirement of ventilator, which can
lead to pneumonia. Smoking can result in reduced blood flow which can affect healing
process at the surgery spot and also it can lead to increased chances of infection. In smokers it
is evident that increased production of Hb, red blood cells and fibrinogen. It can lead to rise
in the haematocrit and blood viscosity. It can lead increased thrombotic incidence (Mahlmann
et al., 2013; Scholes et al., 2009).
Incision during surgery during can produce wound. Smoking can interfere with the wound
healing because for wound healing basic requirement in oxygen. In smokers, there can be
increased levels of carbon monoxide and reduced levels of oxygen in their blood. Due to this
reduced level of oxygen in the blood, there can be reduced supply of oxygen at the wound
site. It can lead to deprived wound healing due to reduced capability to repair and build cells.
Oxygen at the wound site can also be helpful in the providing energy and preventing
infection at the wound site. It is evident from the studies that smoking can exaggerate pain
sensitivity during and post-surgery. Hence, in smokers requirement of anaesthetic and
analgesia is more as compared to the non-smokers. Administration of anaesthetic and
analgesia in more quantity as compared to the optimum level can lead to adverse events and
toxic effects. Hence, it can lead to further deterioration of the patient undergoing surgery
(Zanaty, 2014). Most of the patient undergoing right sigmoid colectomy can exhibit persistent
vomiting and nausea after surgery. This condition can be exaggerated due to smoking
because more frequency of nausea and vomiting in smokers as compared to the non-smokers
in patients undergoing right sigmoid colectomy. Augmented frequency of vomiting can lead
to the dehydration in the patient and further deterioration of the patient can occur. Smoking
impairs immune system and also anaesthesia also can impair immune system. Hence, if
anaesthesia is given to people with smoking there is increased risk of infection. Due to
infections, there can be occurrence of tracheitis, bronchitis and pneumonia. tracheitis,
bronchitis and pneumonia can occur due to S. aureus, H. influenzae and S. pneumoniae
infections respectively. Moreover, Tom is undergoing surgery. Incision made during the
surgery can augment possibility of infection (Guérin et al., 2015). Due to smoking there is
possibility of pneumonia in Tom and compromised immune system can exaggerate
pneumonia which can lead to sepsis in Tom. Since, this is an open sigmoid colectomy, there
are more chance of blood loss during surgery. Due to this blood loos, there can be reduced
blood supply to tissues and organs (Hwang et al., 2014). It can lead to reduced supply of
oxygen which can result in the increased respiratory rate to compensate oxygen demand.
Increased respiratory rate have prognostic significance in the augmented chances of infection,
pneumonia and sepsis. Sepsis can lead to organ deterioration in Tom. Nurse need to assess
respiratory rate, oxygen saturation, heart rate, blood pressure and temperature in Tom
because alteration in these parameters can lead to organ damage and deterioration of Tom.
Nurse should assess fluid balance, pain, skin colour and reactivity in Tom. In case of
deterioration, there would be alteration in all these parameters for Tom. Nurse can prevent
deterioration in the Tom by increasing frequency of observation and medical interventions,
by obtaining emergency assistance and shifting patient to the next level of care (Bohm et al.,
2015).
site. It can lead to deprived wound healing due to reduced capability to repair and build cells.
Oxygen at the wound site can also be helpful in the providing energy and preventing
infection at the wound site. It is evident from the studies that smoking can exaggerate pain
sensitivity during and post-surgery. Hence, in smokers requirement of anaesthetic and
analgesia is more as compared to the non-smokers. Administration of anaesthetic and
analgesia in more quantity as compared to the optimum level can lead to adverse events and
toxic effects. Hence, it can lead to further deterioration of the patient undergoing surgery
(Zanaty, 2014). Most of the patient undergoing right sigmoid colectomy can exhibit persistent
vomiting and nausea after surgery. This condition can be exaggerated due to smoking
because more frequency of nausea and vomiting in smokers as compared to the non-smokers
in patients undergoing right sigmoid colectomy. Augmented frequency of vomiting can lead
to the dehydration in the patient and further deterioration of the patient can occur. Smoking
impairs immune system and also anaesthesia also can impair immune system. Hence, if
anaesthesia is given to people with smoking there is increased risk of infection. Due to
infections, there can be occurrence of tracheitis, bronchitis and pneumonia. tracheitis,
bronchitis and pneumonia can occur due to S. aureus, H. influenzae and S. pneumoniae
infections respectively. Moreover, Tom is undergoing surgery. Incision made during the
surgery can augment possibility of infection (Guérin et al., 2015). Due to smoking there is
possibility of pneumonia in Tom and compromised immune system can exaggerate
pneumonia which can lead to sepsis in Tom. Since, this is an open sigmoid colectomy, there
are more chance of blood loss during surgery. Due to this blood loos, there can be reduced
blood supply to tissues and organs (Hwang et al., 2014). It can lead to reduced supply of
oxygen which can result in the increased respiratory rate to compensate oxygen demand.
Increased respiratory rate have prognostic significance in the augmented chances of infection,
pneumonia and sepsis. Sepsis can lead to organ deterioration in Tom. Nurse need to assess
respiratory rate, oxygen saturation, heart rate, blood pressure and temperature in Tom
because alteration in these parameters can lead to organ damage and deterioration of Tom.
Nurse should assess fluid balance, pain, skin colour and reactivity in Tom. In case of
deterioration, there would be alteration in all these parameters for Tom. Nurse can prevent
deterioration in the Tom by increasing frequency of observation and medical interventions,
by obtaining emergency assistance and shifting patient to the next level of care (Bohm et al.,
2015).
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Part C :
Discharge plan:
There should be participation of different stakeholders in the discharge plan of Tom. These
include discharge co-ordinator, medical officer, pharmacist, dietician, social worker and
specialist nurses. Discharge co-ordinator plays role in co-ordinating different members
involved in the discharge planning. Medical officer provides clinical management to the
patient. Pharmacist review prescription. Social worker can assist patient in addressing issues
like social, financial and family issues. Nurses provide accurate information about health
status of patient to the medical officer. Dietician helps to plan nutritious diet for the patient.
There should be smooth transition of Tom to the society. Tom need to live normal life after
discharge from the hospital. Tom’s dressings need to be removed prior to discharge. At home
Tom might not be able to remove dressing and removal of dressing would be helpful in
assessing infection in Tom. Tom’s wound should be healed completely. Nurse should assess
wound healing in Tom. He can assess it by assessing unusual sensations to touch like
numbness, tingling and itching. Hard lumpy formation reflects new tissue formation. If
wound didn’t heal completely, there might be possibility of infection in Tom. Tom should
have normal bowel movement after discharge. Mild laxative needs to be administered to him.
Laxative would be helpful in improving bowel movement because in colectomy there would
be less functioning and less bowel movement. For few days, consumption of oral fluids is
encouraged. To maintain proper diet and nutritional balance. Oral fluids are encouraged for
few days. Maintenance of normal diet would be helpful in speedy recovery (Dobradin et al.,
2013; Stefanou et al., 2012).
Management of medications for hypertension and hyperlipidaemia. To assist Tom to comply
with prescribed medications in required dosage and dose. Providing clear instruction about
medication consumption in verbal and written form. Nurse should educate Tom about the
adverse effects of medications. It would be helpful for the Tom to understand benefits and
adverse effects of medicines. It would also be helpful in understanding importance of
adherence to the medication. Tom referral after discharge. Tom should be aware of all the
planned appointments after discharge, hence he can make maximum benefits of it. Tom
Discharge plan:
There should be participation of different stakeholders in the discharge plan of Tom. These
include discharge co-ordinator, medical officer, pharmacist, dietician, social worker and
specialist nurses. Discharge co-ordinator plays role in co-ordinating different members
involved in the discharge planning. Medical officer provides clinical management to the
patient. Pharmacist review prescription. Social worker can assist patient in addressing issues
like social, financial and family issues. Nurses provide accurate information about health
status of patient to the medical officer. Dietician helps to plan nutritious diet for the patient.
There should be smooth transition of Tom to the society. Tom need to live normal life after
discharge from the hospital. Tom’s dressings need to be removed prior to discharge. At home
Tom might not be able to remove dressing and removal of dressing would be helpful in
assessing infection in Tom. Tom’s wound should be healed completely. Nurse should assess
wound healing in Tom. He can assess it by assessing unusual sensations to touch like
numbness, tingling and itching. Hard lumpy formation reflects new tissue formation. If
wound didn’t heal completely, there might be possibility of infection in Tom. Tom should
have normal bowel movement after discharge. Mild laxative needs to be administered to him.
Laxative would be helpful in improving bowel movement because in colectomy there would
be less functioning and less bowel movement. For few days, consumption of oral fluids is
encouraged. To maintain proper diet and nutritional balance. Oral fluids are encouraged for
few days. Maintenance of normal diet would be helpful in speedy recovery (Dobradin et al.,
2013; Stefanou et al., 2012).
Management of medications for hypertension and hyperlipidaemia. To assist Tom to comply
with prescribed medications in required dosage and dose. Providing clear instruction about
medication consumption in verbal and written form. Nurse should educate Tom about the
adverse effects of medications. It would be helpful for the Tom to understand benefits and
adverse effects of medicines. It would also be helpful in understanding importance of
adherence to the medication. Tom referral after discharge. Tom should be aware of all the
planned appointments after discharge, hence he can make maximum benefits of it. Tom
1 out of 11
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.