Mrs. Brown's Case Study: Acute Exacerbation of Chronic Conditions
VerifiedAdded on 2022/10/02
|10
|1944
|88
Report
AI Summary
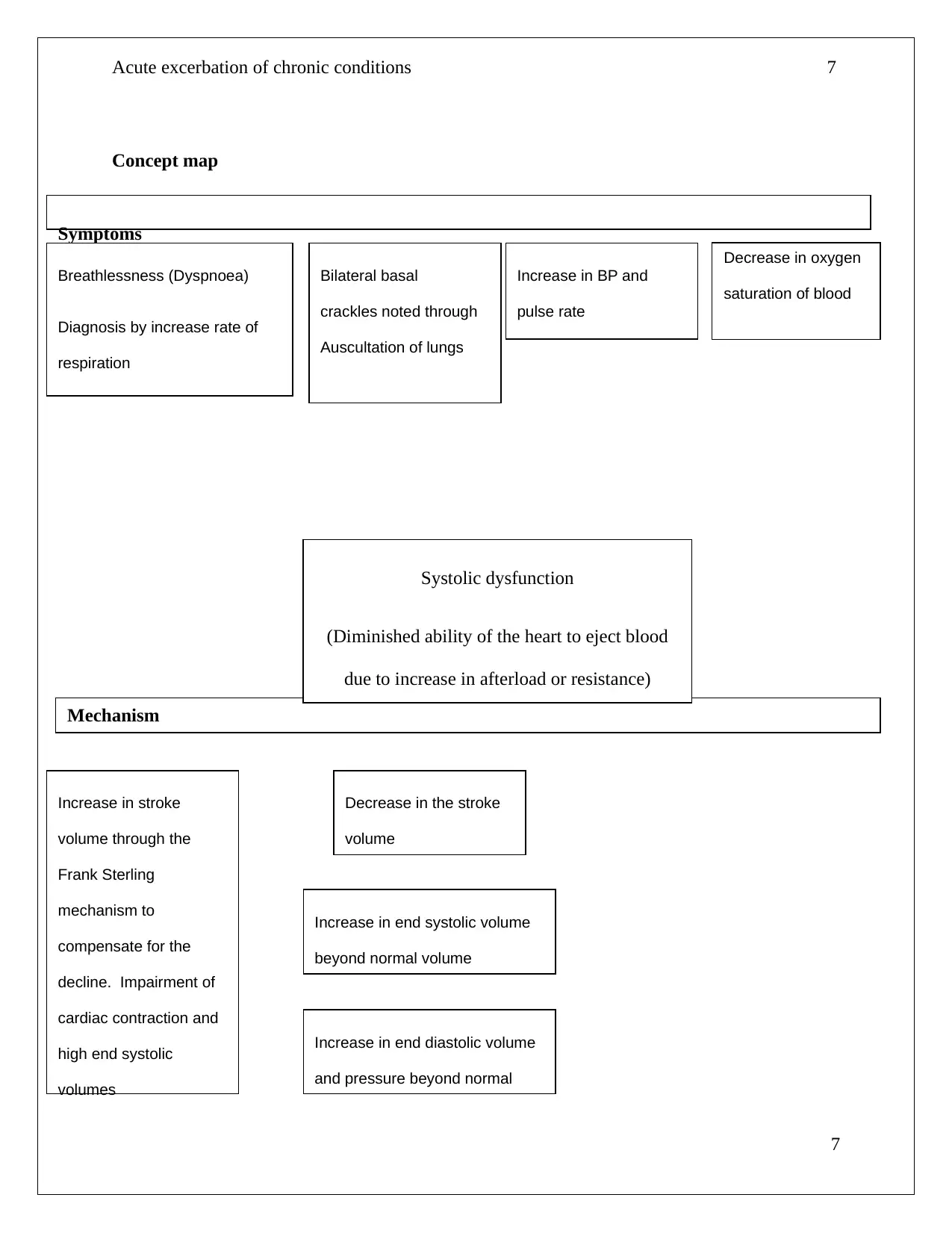
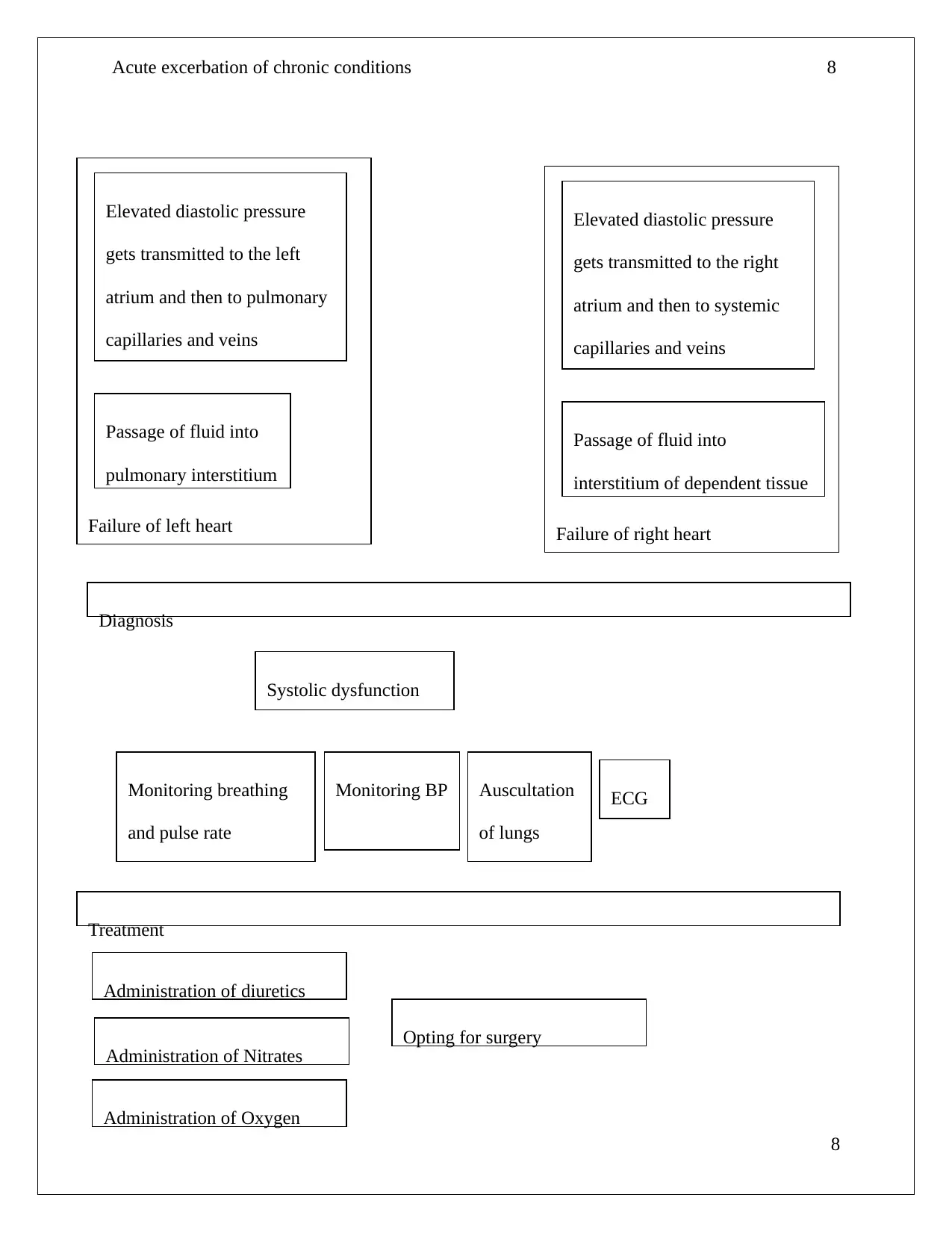
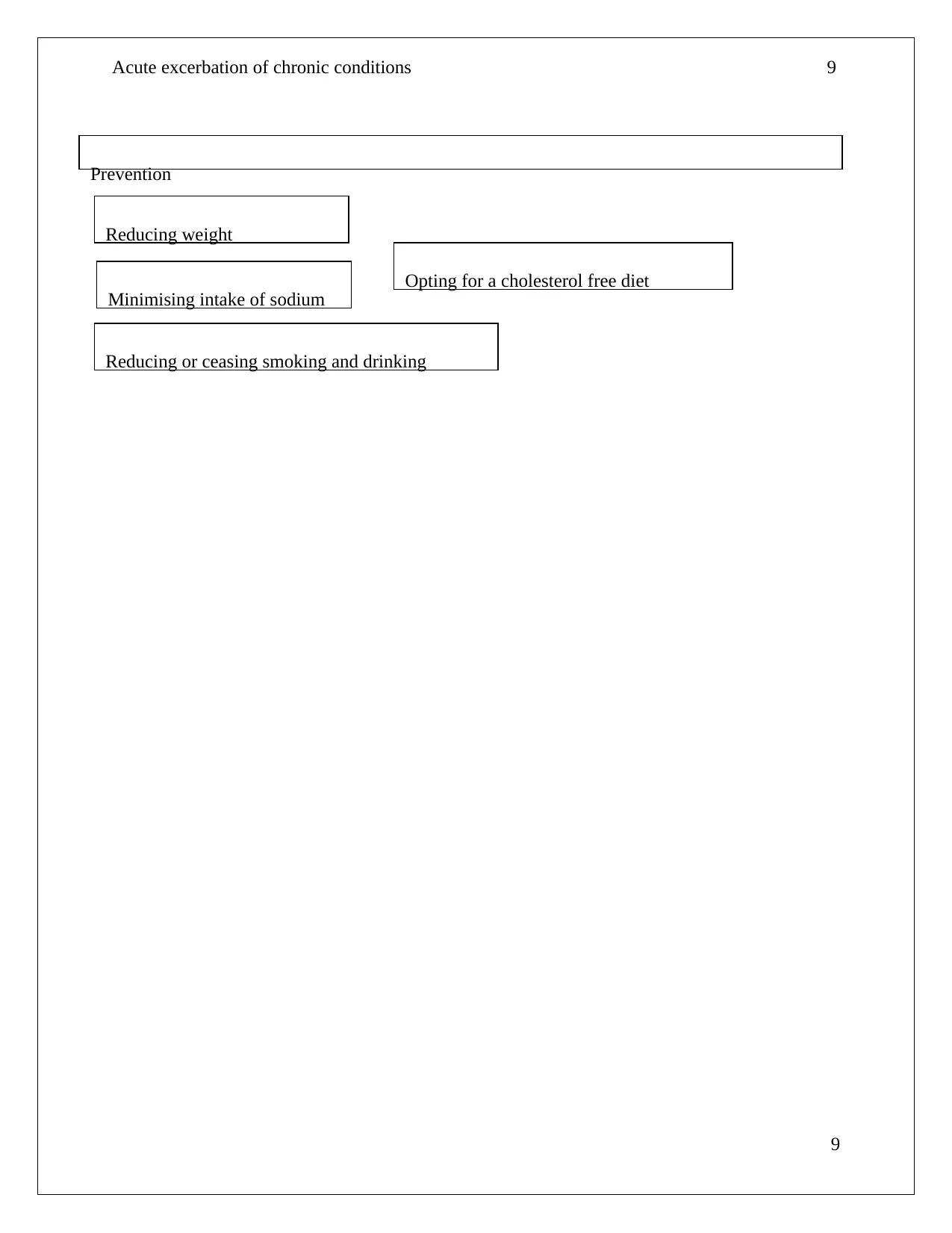
This report presents a case study of Mrs. Brown, who experienced an acute exacerbation of chronic heart failure. The report details her symptoms, including severe dyspnea, increased respiratory and pulse rates, low oxygen saturation, and high blood pressure. Through analysis of her vital signs, ECG readings (atrial fibrillation), and auscultation findings (bilateral crackles), the report diagnoses systolic dysfunction and acute decompensated heart failure (ADHF). It explores the pathogenesis of her condition, highlighting the role of increased afterload, reduced cardiac contractility, and tachycardia. The report also examines the patient's journey through the emergency department, emphasizing the importance of nurses in assessing and managing the condition. Finally, it discusses the administered treatments, including sublingual Glyceryl Trinitrate (GTN) and Furosemide (Lasix), and their mechanisms of action in managing the patient's condition.

1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.