Assessment and Management of Acute Pain and Deep Vein Thrombosis in a Trauma Patient
VerifiedAdded on 2023/06/14
|8
|1986
|413
AI Summary
This report discusses the case of a trauma patient who suffered from acute pain and was at risk of developing deep vein thrombosis. The report covers the assessment of the patient, the pathophysiology of acute pain and DVT, and the interventions and nursing priorities for pain management and DVT prevention.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Written Report
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
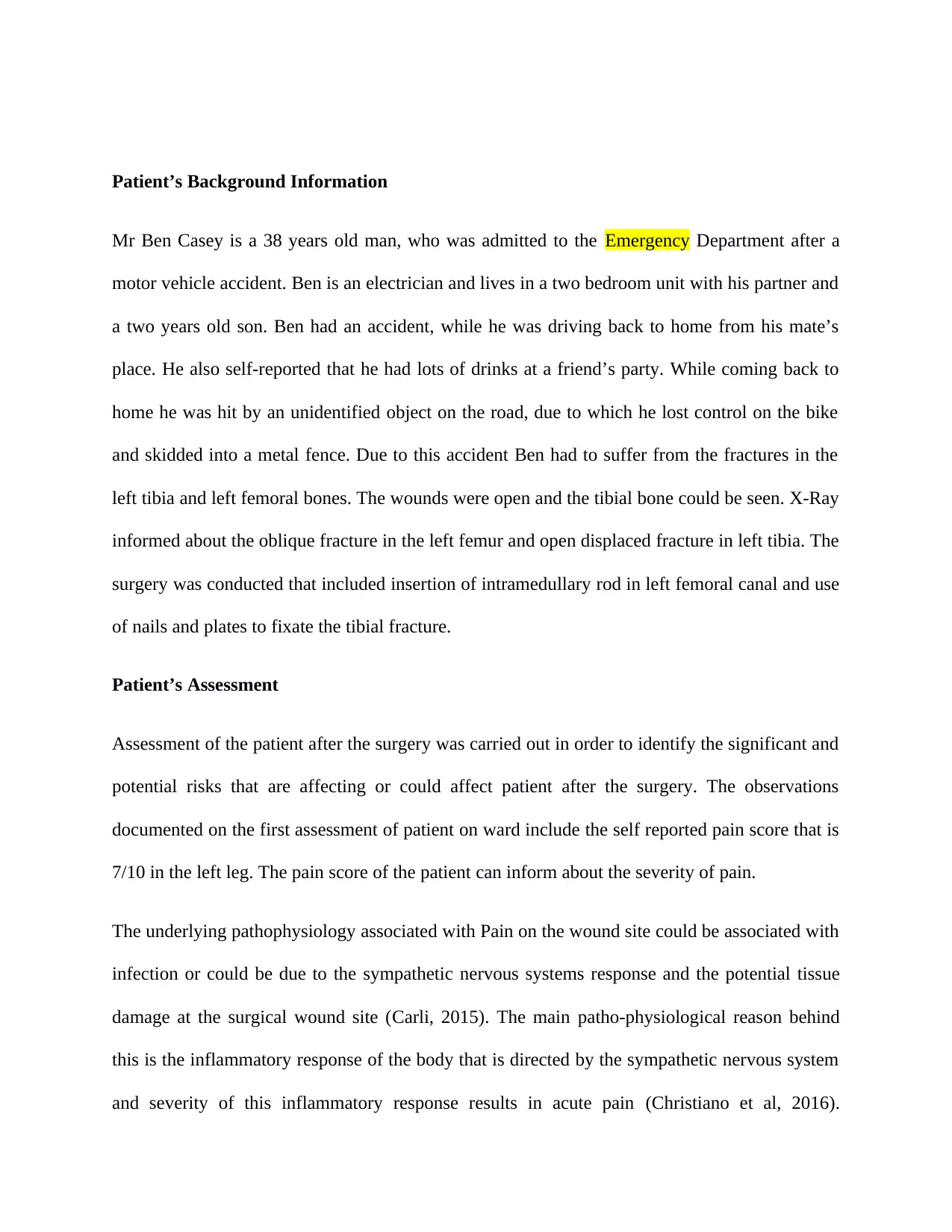
Patient’s Background Information
Mr Ben Casey is a 38 years old man, who was admitted to the Emergency Department after a
motor vehicle accident. Ben is an electrician and lives in a two bedroom unit with his partner and
a two years old son. Ben had an accident, while he was driving back to home from his mate’s
place. He also self-reported that he had lots of drinks at a friend’s party. While coming back to
home he was hit by an unidentified object on the road, due to which he lost control on the bike
and skidded into a metal fence. Due to this accident Ben had to suffer from the fractures in the
left tibia and left femoral bones. The wounds were open and the tibial bone could be seen. X-Ray
informed about the oblique fracture in the left femur and open displaced fracture in left tibia. The
surgery was conducted that included insertion of intramedullary rod in left femoral canal and use
of nails and plates to fixate the tibial fracture.
Patient’s Assessment
Assessment of the patient after the surgery was carried out in order to identify the significant and
potential risks that are affecting or could affect patient after the surgery. The observations
documented on the first assessment of patient on ward include the self reported pain score that is
7/10 in the left leg. The pain score of the patient can inform about the severity of pain.
The underlying pathophysiology associated with Pain on the wound site could be associated with
infection or could be due to the sympathetic nervous systems response and the potential tissue
damage at the surgical wound site (Carli, 2015). The main patho-physiological reason behind
this is the inflammatory response of the body that is directed by the sympathetic nervous system
and severity of this inflammatory response results in acute pain (Christiano et al, 2016).
Mr Ben Casey is a 38 years old man, who was admitted to the Emergency Department after a
motor vehicle accident. Ben is an electrician and lives in a two bedroom unit with his partner and
a two years old son. Ben had an accident, while he was driving back to home from his mate’s
place. He also self-reported that he had lots of drinks at a friend’s party. While coming back to
home he was hit by an unidentified object on the road, due to which he lost control on the bike
and skidded into a metal fence. Due to this accident Ben had to suffer from the fractures in the
left tibia and left femoral bones. The wounds were open and the tibial bone could be seen. X-Ray
informed about the oblique fracture in the left femur and open displaced fracture in left tibia. The
surgery was conducted that included insertion of intramedullary rod in left femoral canal and use
of nails and plates to fixate the tibial fracture.
Patient’s Assessment
Assessment of the patient after the surgery was carried out in order to identify the significant and
potential risks that are affecting or could affect patient after the surgery. The observations
documented on the first assessment of patient on ward include the self reported pain score that is
7/10 in the left leg. The pain score of the patient can inform about the severity of pain.
The underlying pathophysiology associated with Pain on the wound site could be associated with
infection or could be due to the sympathetic nervous systems response and the potential tissue
damage at the surgical wound site (Carli, 2015). The main patho-physiological reason behind
this is the inflammatory response of the body that is directed by the sympathetic nervous system
and severity of this inflammatory response results in acute pain (Christiano et al, 2016).
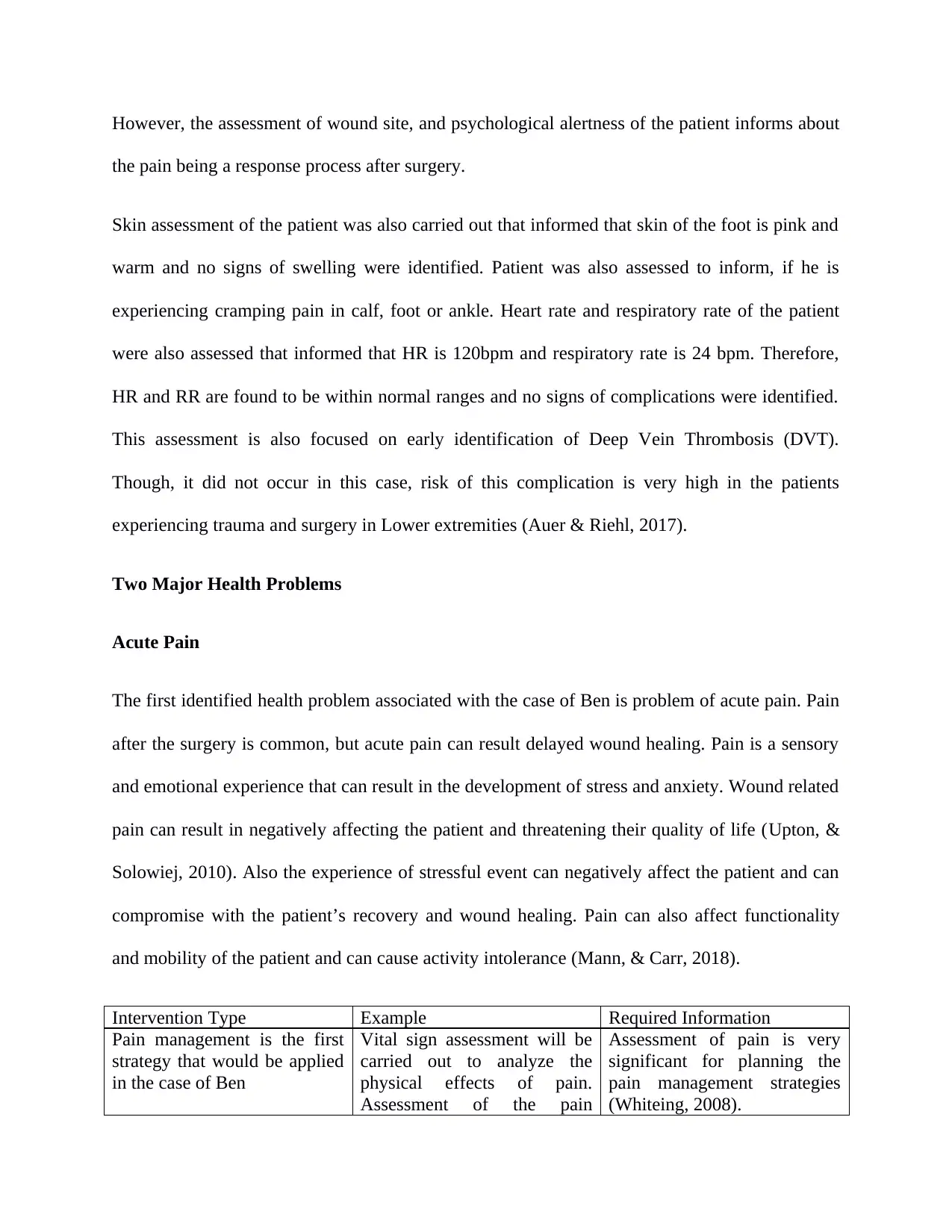
However, the assessment of wound site, and psychological alertness of the patient informs about
the pain being a response process after surgery.
Skin assessment of the patient was also carried out that informed that skin of the foot is pink and
warm and no signs of swelling were identified. Patient was also assessed to inform, if he is
experiencing cramping pain in calf, foot or ankle. Heart rate and respiratory rate of the patient
were also assessed that informed that HR is 120bpm and respiratory rate is 24 bpm. Therefore,
HR and RR are found to be within normal ranges and no signs of complications were identified.
This assessment is also focused on early identification of Deep Vein Thrombosis (DVT).
Though, it did not occur in this case, risk of this complication is very high in the patients
experiencing trauma and surgery in Lower extremities (Auer & Riehl, 2017).
Two Major Health Problems
Acute Pain
The first identified health problem associated with the case of Ben is problem of acute pain. Pain
after the surgery is common, but acute pain can result delayed wound healing. Pain is a sensory
and emotional experience that can result in the development of stress and anxiety. Wound related
pain can result in negatively affecting the patient and threatening their quality of life (Upton, &
Solowiej, 2010). Also the experience of stressful event can negatively affect the patient and can
compromise with the patient’s recovery and wound healing. Pain can also affect functionality
and mobility of the patient and can cause activity intolerance (Mann, & Carr, 2018).
Intervention Type Example Required Information
Pain management is the first
strategy that would be applied
in the case of Ben
Vital sign assessment will be
carried out to analyze the
physical effects of pain.
Assessment of the pain
Assessment of pain is very
significant for planning the
pain management strategies
(Whiteing, 2008).
the pain being a response process after surgery.
Skin assessment of the patient was also carried out that informed that skin of the foot is pink and
warm and no signs of swelling were identified. Patient was also assessed to inform, if he is
experiencing cramping pain in calf, foot or ankle. Heart rate and respiratory rate of the patient
were also assessed that informed that HR is 120bpm and respiratory rate is 24 bpm. Therefore,
HR and RR are found to be within normal ranges and no signs of complications were identified.
This assessment is also focused on early identification of Deep Vein Thrombosis (DVT).
Though, it did not occur in this case, risk of this complication is very high in the patients
experiencing trauma and surgery in Lower extremities (Auer & Riehl, 2017).
Two Major Health Problems
Acute Pain
The first identified health problem associated with the case of Ben is problem of acute pain. Pain
after the surgery is common, but acute pain can result delayed wound healing. Pain is a sensory
and emotional experience that can result in the development of stress and anxiety. Wound related
pain can result in negatively affecting the patient and threatening their quality of life (Upton, &
Solowiej, 2010). Also the experience of stressful event can negatively affect the patient and can
compromise with the patient’s recovery and wound healing. Pain can also affect functionality
and mobility of the patient and can cause activity intolerance (Mann, & Carr, 2018).
Intervention Type Example Required Information
Pain management is the first
strategy that would be applied
in the case of Ben
Vital sign assessment will be
carried out to analyze the
physical effects of pain.
Assessment of the pain
Assessment of pain is very
significant for planning the
pain management strategies
(Whiteing, 2008).
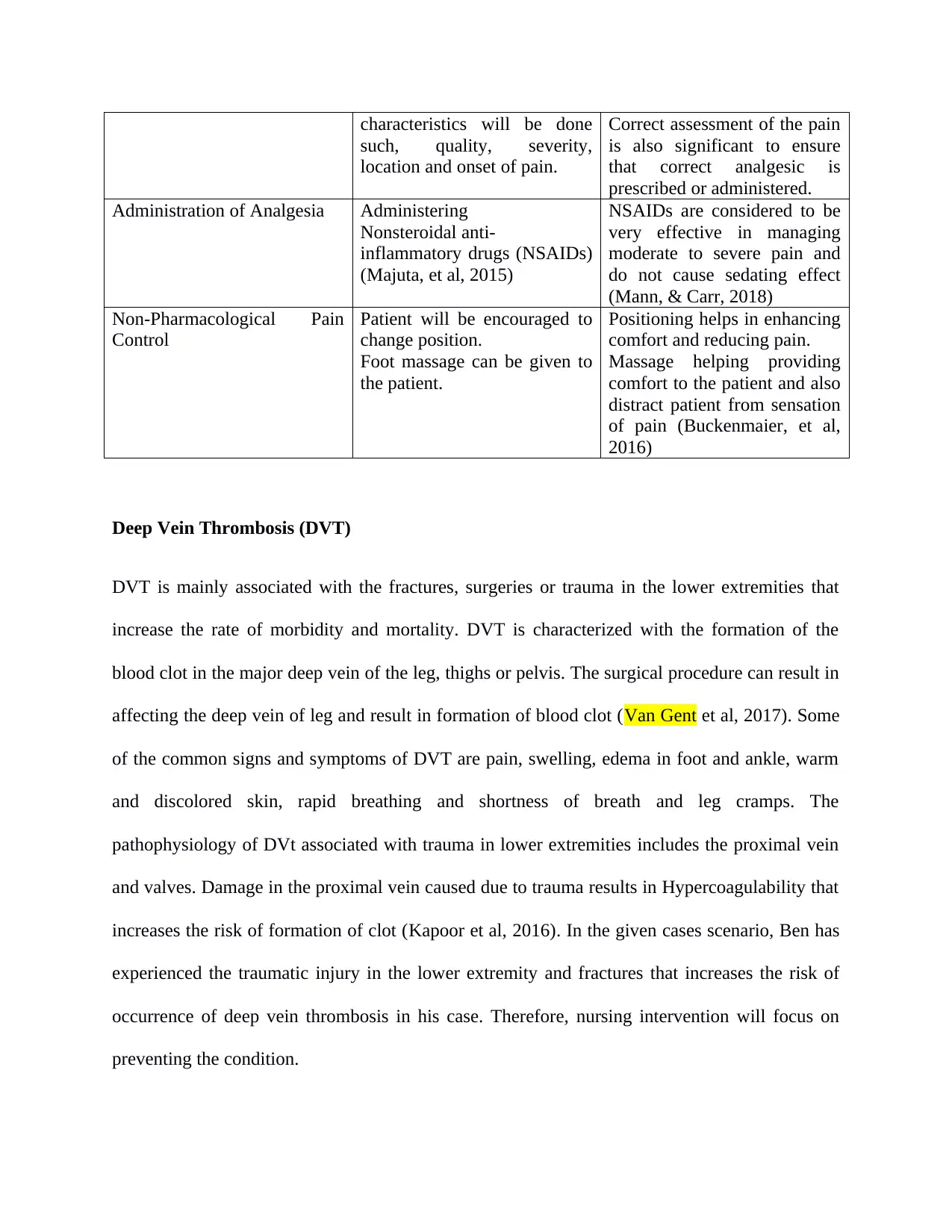
characteristics will be done
such, quality, severity,
location and onset of pain.
Correct assessment of the pain
is also significant to ensure
that correct analgesic is
prescribed or administered.
Administration of Analgesia Administering
Nonsteroidal anti-
inflammatory drugs (NSAIDs)
(Majuta, et al, 2015)
NSAIDs are considered to be
very effective in managing
moderate to severe pain and
do not cause sedating effect
(Mann, & Carr, 2018)
Non-Pharmacological Pain
Control
Patient will be encouraged to
change position.
Foot massage can be given to
the patient.
Positioning helps in enhancing
comfort and reducing pain.
Massage helping providing
comfort to the patient and also
distract patient from sensation
of pain (Buckenmaier, et al,
2016)
Deep Vein Thrombosis (DVT)
DVT is mainly associated with the fractures, surgeries or trauma in the lower extremities that
increase the rate of morbidity and mortality. DVT is characterized with the formation of the
blood clot in the major deep vein of the leg, thighs or pelvis. The surgical procedure can result in
affecting the deep vein of leg and result in formation of blood clot (Van Gent et al, 2017). Some
of the common signs and symptoms of DVT are pain, swelling, edema in foot and ankle, warm
and discolored skin, rapid breathing and shortness of breath and leg cramps. The
pathophysiology of DVt associated with trauma in lower extremities includes the proximal vein
and valves. Damage in the proximal vein caused due to trauma results in Hypercoagulability that
increases the risk of formation of clot (Kapoor et al, 2016). In the given cases scenario, Ben has
experienced the traumatic injury in the lower extremity and fractures that increases the risk of
occurrence of deep vein thrombosis in his case. Therefore, nursing intervention will focus on
preventing the condition.
such, quality, severity,
location and onset of pain.
Correct assessment of the pain
is also significant to ensure
that correct analgesic is
prescribed or administered.
Administration of Analgesia Administering
Nonsteroidal anti-
inflammatory drugs (NSAIDs)
(Majuta, et al, 2015)
NSAIDs are considered to be
very effective in managing
moderate to severe pain and
do not cause sedating effect
(Mann, & Carr, 2018)
Non-Pharmacological Pain
Control
Patient will be encouraged to
change position.
Foot massage can be given to
the patient.
Positioning helps in enhancing
comfort and reducing pain.
Massage helping providing
comfort to the patient and also
distract patient from sensation
of pain (Buckenmaier, et al,
2016)
Deep Vein Thrombosis (DVT)
DVT is mainly associated with the fractures, surgeries or trauma in the lower extremities that
increase the rate of morbidity and mortality. DVT is characterized with the formation of the
blood clot in the major deep vein of the leg, thighs or pelvis. The surgical procedure can result in
affecting the deep vein of leg and result in formation of blood clot (Van Gent et al, 2017). Some
of the common signs and symptoms of DVT are pain, swelling, edema in foot and ankle, warm
and discolored skin, rapid breathing and shortness of breath and leg cramps. The
pathophysiology of DVt associated with trauma in lower extremities includes the proximal vein
and valves. Damage in the proximal vein caused due to trauma results in Hypercoagulability that
increases the risk of formation of clot (Kapoor et al, 2016). In the given cases scenario, Ben has
experienced the traumatic injury in the lower extremity and fractures that increases the risk of
occurrence of deep vein thrombosis in his case. Therefore, nursing intervention will focus on
preventing the condition.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
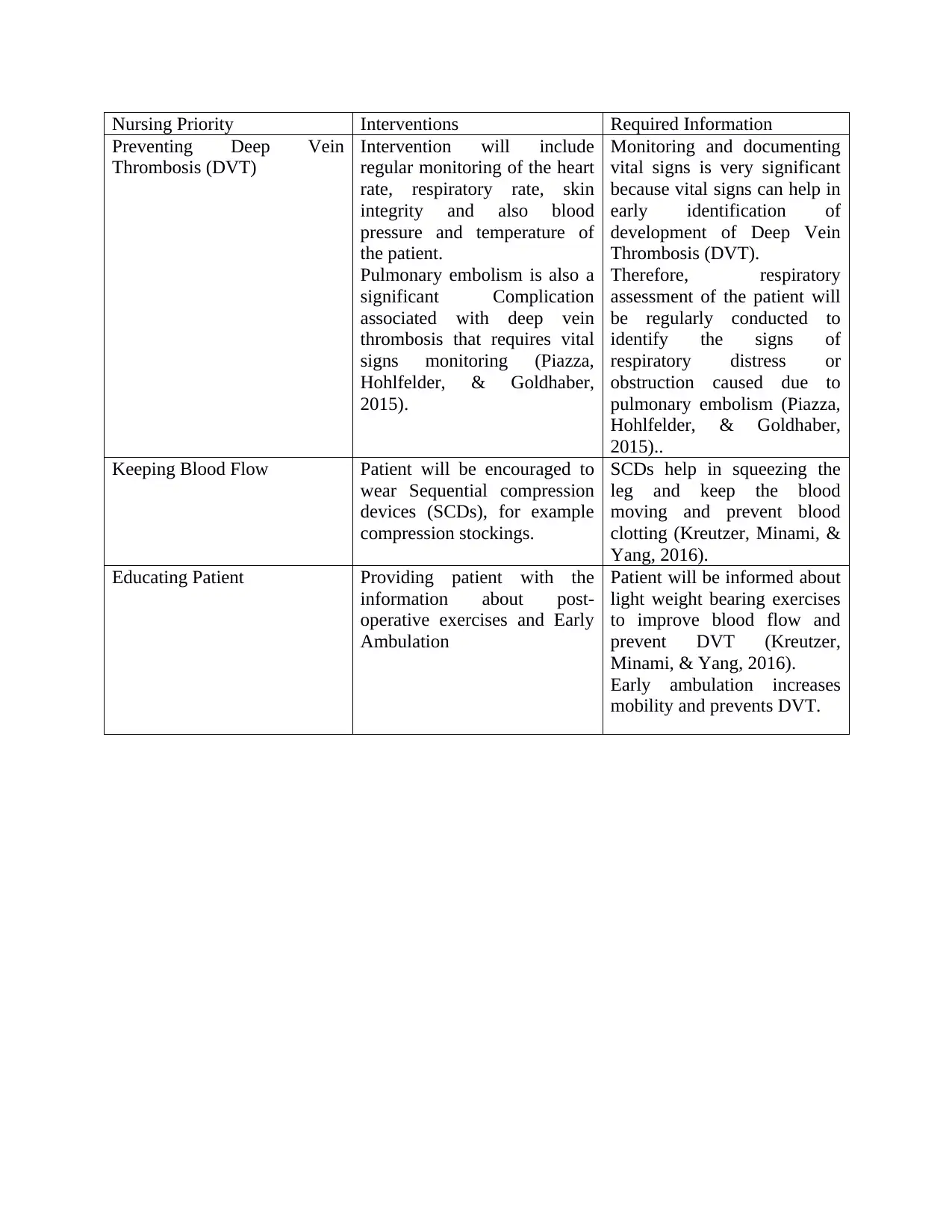
Nursing Priority Interventions Required Information
Preventing Deep Vein
Thrombosis (DVT)
Intervention will include
regular monitoring of the heart
rate, respiratory rate, skin
integrity and also blood
pressure and temperature of
the patient.
Pulmonary embolism is also a
significant Complication
associated with deep vein
thrombosis that requires vital
signs monitoring (Piazza,
Hohlfelder, & Goldhaber,
2015).
Monitoring and documenting
vital signs is very significant
because vital signs can help in
early identification of
development of Deep Vein
Thrombosis (DVT).
Therefore, respiratory
assessment of the patient will
be regularly conducted to
identify the signs of
respiratory distress or
obstruction caused due to
pulmonary embolism (Piazza,
Hohlfelder, & Goldhaber,
2015)..
Keeping Blood Flow Patient will be encouraged to
wear Sequential compression
devices (SCDs), for example
compression stockings.
SCDs help in squeezing the
leg and keep the blood
moving and prevent blood
clotting (Kreutzer, Minami, &
Yang, 2016).
Educating Patient Providing patient with the
information about post-
operative exercises and Early
Ambulation
Patient will be informed about
light weight bearing exercises
to improve blood flow and
prevent DVT (Kreutzer,
Minami, & Yang, 2016).
Early ambulation increases
mobility and prevents DVT.
Preventing Deep Vein
Thrombosis (DVT)
Intervention will include
regular monitoring of the heart
rate, respiratory rate, skin
integrity and also blood
pressure and temperature of
the patient.
Pulmonary embolism is also a
significant Complication
associated with deep vein
thrombosis that requires vital
signs monitoring (Piazza,
Hohlfelder, & Goldhaber,
2015).
Monitoring and documenting
vital signs is very significant
because vital signs can help in
early identification of
development of Deep Vein
Thrombosis (DVT).
Therefore, respiratory
assessment of the patient will
be regularly conducted to
identify the signs of
respiratory distress or
obstruction caused due to
pulmonary embolism (Piazza,
Hohlfelder, & Goldhaber,
2015)..
Keeping Blood Flow Patient will be encouraged to
wear Sequential compression
devices (SCDs), for example
compression stockings.
SCDs help in squeezing the
leg and keep the blood
moving and prevent blood
clotting (Kreutzer, Minami, &
Yang, 2016).
Educating Patient Providing patient with the
information about post-
operative exercises and Early
Ambulation
Patient will be informed about
light weight bearing exercises
to improve blood flow and
prevent DVT (Kreutzer,
Minami, & Yang, 2016).
Early ambulation increases
mobility and prevents DVT.
References
Auer, R., & Riehl, J (2017). The incidence of deep vein thrombosis and pulmonary embolism
after fracture of the tibia: An analysis of the National Trauma Databank. Journal of Clinical
Orthopaedics & Trauma, 8(1), 38-44. Available from:
http://www.journal-cot.com/article/S0976-5662(16)30060-1/abstract
Brown,D, Edwards, H,Seaton ,L & Buckley,T.,(eds) (2015). Lewis medical-surgical nursing:
assessment and management of clinical problems. 4th edn, Elservier Australia, Chatswood,
NSW.
Buckenmaier, C., Cambron, J., Werner, R., Buckenmaier, P., Deery, C., Schwartz, J., &
Whitridge, P (2016). Massage therapy for pain—call to action. Pain Medicine: The Official
Journal of the American Academy of Pain Medicine, 17(7), 1211. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4925169/
Carli, F (2015). Physiologic considerations of Enhanced Recovery After Surgery (ERAS)
programs: implications of the stress response. Canadian Journal of Anesthesia/Journal canadien
d'anesthésie, 62(2), 110-119. Available from: https://link.springer.com/article/10.1007/s12630-
014-0264-0
Christiano, A. V., Pean, C. A., Konda, S. R., & Egol, K. A (2016). Predictors of patient reported
pain after lower extremity nonunion surgery: the nicotine effect. The Iowa orthopaedic
journal, 36, 53. Available From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4910799/
Auer, R., & Riehl, J (2017). The incidence of deep vein thrombosis and pulmonary embolism
after fracture of the tibia: An analysis of the National Trauma Databank. Journal of Clinical
Orthopaedics & Trauma, 8(1), 38-44. Available from:
http://www.journal-cot.com/article/S0976-5662(16)30060-1/abstract
Brown,D, Edwards, H,Seaton ,L & Buckley,T.,(eds) (2015). Lewis medical-surgical nursing:
assessment and management of clinical problems. 4th edn, Elservier Australia, Chatswood,
NSW.
Buckenmaier, C., Cambron, J., Werner, R., Buckenmaier, P., Deery, C., Schwartz, J., &
Whitridge, P (2016). Massage therapy for pain—call to action. Pain Medicine: The Official
Journal of the American Academy of Pain Medicine, 17(7), 1211. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4925169/
Carli, F (2015). Physiologic considerations of Enhanced Recovery After Surgery (ERAS)
programs: implications of the stress response. Canadian Journal of Anesthesia/Journal canadien
d'anesthésie, 62(2), 110-119. Available from: https://link.springer.com/article/10.1007/s12630-
014-0264-0
Christiano, A. V., Pean, C. A., Konda, S. R., & Egol, K. A (2016). Predictors of patient reported
pain after lower extremity nonunion surgery: the nicotine effect. The Iowa orthopaedic
journal, 36, 53. Available From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4910799/
Kapoor, C. S., Mehta, A. K., Patel, K., & Golwala, P. P (2016). Prevalence of deep vein
thrombosis in patients with lower limb trauma. Journal of Clinical Orthopaedics & Trauma, 7,
220-224. Available from: http://www.journal-cot.com/article/S0976-5662(16)30143-6/abstract
Kreutzer, L., Minami, C., & Yang, A. (2016). Preventing venous thromboembolism after
surgery. Jama, 315(19), 2136-2136. Available from:
https://jamanetwork.com/journals/jama/fullarticle/2521971
Majuta, L. A., Longo, G., Fealk, M. N., McCaffrey, G., & Mantyh, P. W (2015). Orthopedic
surgery and bone fracture pain are both significantly attenuated by sustained blockade of nerve
growth factor. Pain, 156(1), 157. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4495732/
Mann, E., & Carr, E. (2018). Pain management. Foundation Studies for Caring: Using Student-
Centred Learning, 259. Available from: https://books.google.co.in/books?
hl=en&lr=&id=riFHDwAAQBAJ&oi=fnd&pg=PA259&dq=Mann,+E.,+%26+Carr,+E.+(2018).
+Pain+management.+Foundation+Studies+for+Caring:+Using+Student-Centred+Learning,
+259.&ots=9kE6b6SbOQ&sig=S5m9PLay1sTH6u0gjzM7fgw-wKE#v=onepage&q&f=false
[Accessed 4th April, 2018]
Piazza, G., Hohlfelder, B., & Goldhaber, S. Z. (2015) Pathophysiology of Deep Vein
Thrombosis and Pulmonary Embolism: Beyond Virchow’s Triad. In Handbook for Venous
Thromboembolism (pp. 15-20). Springer, Cham. Available from:
https://link.springer.com/chapter/10.1007/978-3-319-20843-5_3
Upton, D., & Solowiej, K (2010). Pain and stress as contributors to delayed wound
healing. Wound Practice & Research: Journal of the Australian Wound Management
thrombosis in patients with lower limb trauma. Journal of Clinical Orthopaedics & Trauma, 7,
220-224. Available from: http://www.journal-cot.com/article/S0976-5662(16)30143-6/abstract
Kreutzer, L., Minami, C., & Yang, A. (2016). Preventing venous thromboembolism after
surgery. Jama, 315(19), 2136-2136. Available from:
https://jamanetwork.com/journals/jama/fullarticle/2521971
Majuta, L. A., Longo, G., Fealk, M. N., McCaffrey, G., & Mantyh, P. W (2015). Orthopedic
surgery and bone fracture pain are both significantly attenuated by sustained blockade of nerve
growth factor. Pain, 156(1), 157. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4495732/
Mann, E., & Carr, E. (2018). Pain management. Foundation Studies for Caring: Using Student-
Centred Learning, 259. Available from: https://books.google.co.in/books?
hl=en&lr=&id=riFHDwAAQBAJ&oi=fnd&pg=PA259&dq=Mann,+E.,+%26+Carr,+E.+(2018).
+Pain+management.+Foundation+Studies+for+Caring:+Using+Student-Centred+Learning,
+259.&ots=9kE6b6SbOQ&sig=S5m9PLay1sTH6u0gjzM7fgw-wKE#v=onepage&q&f=false
[Accessed 4th April, 2018]
Piazza, G., Hohlfelder, B., & Goldhaber, S. Z. (2015) Pathophysiology of Deep Vein
Thrombosis and Pulmonary Embolism: Beyond Virchow’s Triad. In Handbook for Venous
Thromboembolism (pp. 15-20). Springer, Cham. Available from:
https://link.springer.com/chapter/10.1007/978-3-319-20843-5_3
Upton, D., & Solowiej, K (2010). Pain and stress as contributors to delayed wound
healing. Wound Practice & Research: Journal of the Australian Wound Management
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Association, 18(3), 114. Available from:
https://search.informit.com.au/documentSummary;dn=364536431309445;res=IELHEA
Van Gent, J. M., Calvo, R. Y., Zander, A. L., Olson, E. J., Sise, C. B., Sise, M. J., & Shackford,
S. R. (2017). Risk factors for deep vein thrombosis and pulmonary embolism after traumatic
injury: A competing risks analysis. Journal of trauma and acute care surgery, 83(6), 1154-1160.
Available from:
https://journals.lww.com/jtrauma/Abstract/2017/12000/Risk_factors_for_deep_vein_thrombosis
_and.23.aspx
Whiteing, N. L. (2008). Fractures: pathophysiology, treatment and nursing care. Nursing
Standard (through 2013), 23(2), 49. Available from:
https://search.proquest.com/openview/7132041950e359f4182fdefbda4cf169/1?pq-
origsite=gscholar&cbl=30130
https://search.informit.com.au/documentSummary;dn=364536431309445;res=IELHEA
Van Gent, J. M., Calvo, R. Y., Zander, A. L., Olson, E. J., Sise, C. B., Sise, M. J., & Shackford,
S. R. (2017). Risk factors for deep vein thrombosis and pulmonary embolism after traumatic
injury: A competing risks analysis. Journal of trauma and acute care surgery, 83(6), 1154-1160.
Available from:
https://journals.lww.com/jtrauma/Abstract/2017/12000/Risk_factors_for_deep_vein_thrombosis
_and.23.aspx
Whiteing, N. L. (2008). Fractures: pathophysiology, treatment and nursing care. Nursing
Standard (through 2013), 23(2), 49. Available from:
https://search.proquest.com/openview/7132041950e359f4182fdefbda4cf169/1?pq-
origsite=gscholar&cbl=30130
1 out of 8
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.