Global Anemia Prevalence in Women and Children: 1995 to 2011
VerifiedAdded on 2023/06/03
|20
|3942
|210
Report
AI Summary
This report investigates the prevalence of anemia in women and children worldwide between 1995 and 2011. Key findings reveal that average iron deficiency is highest among children under 5 years old compared to pregnant women and women of reproductive age. Statistical analysis, including t-tests and ANOVA, confirms significant differences in iron deficiency across these groups. The study also explores the correlation between micronutrient deficiency rates in preschool children and dietary diversity, as well as GDP per capita. Results indicate that higher micronutrient deficiency rates are observed in countries with poor dietary diversity and low GDP per capita. The report concludes with a discussion of these findings and their implications for public health interventions.

Fundamentals of science data
Student Name:
Instructor Name:
Course Number:
7 October 2018
Student Name:
Instructor Name:
Course Number:
7 October 2018
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of Contents
Abstract............................................................................................................................................4
Introduction......................................................................................................................................5
Literature Review............................................................................................................................6
Research Questions..........................................................................................................................7
Research Hypothesis........................................................................................................................7
Results..............................................................................................................................................9
Descriptive Analysis....................................................................................................................9
Inferential Analysis....................................................................................................................10
Hypothesis 1:..........................................................................................................................10
Hypothesis 2:..........................................................................................................................12
Hypothesis 3:..........................................................................................................................14
Hypothesis 4:..........................................................................................................................16
Conclusion.....................................................................................................................................18
References......................................................................................................................................19
Abstract............................................................................................................................................4
Introduction......................................................................................................................................5
Literature Review............................................................................................................................6
Research Questions..........................................................................................................................7
Research Hypothesis........................................................................................................................7
Results..............................................................................................................................................9
Descriptive Analysis....................................................................................................................9
Inferential Analysis....................................................................................................................10
Hypothesis 1:..........................................................................................................................10
Hypothesis 2:..........................................................................................................................12
Hypothesis 3:..........................................................................................................................14
Hypothesis 4:..........................................................................................................................16
Conclusion.....................................................................................................................................18
References......................................................................................................................................19
List of Tables
Table 1: Descriptive Statistics.........................................................................................................9
Table 2: t-Test: Two-Sample Assuming Equal Variances............................................................10
Table 3: ANOVA test (Single Factor)...........................................................................................12
Table 4: Correlation test................................................................................................................15
Table 5: Correlation test................................................................................................................16
List of Figures
Figure 1: Chart on average iron deficiency...................................................................................11
Figure 2: Chart on average iron deficiency...................................................................................14
Figure 3: A scatter plot of HHI versus share of energy.................................................................15
Figure 4: A scatter plot of HHI versus GDP per capita.................................................................17
Table 1: Descriptive Statistics.........................................................................................................9
Table 2: t-Test: Two-Sample Assuming Equal Variances............................................................10
Table 3: ANOVA test (Single Factor)...........................................................................................12
Table 4: Correlation test................................................................................................................15
Table 5: Correlation test................................................................................................................16
List of Figures
Figure 1: Chart on average iron deficiency...................................................................................11
Figure 2: Chart on average iron deficiency...................................................................................14
Figure 3: A scatter plot of HHI versus share of energy.................................................................15
Figure 4: A scatter plot of HHI versus GDP per capita.................................................................17
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Abstract
The main purpose of this study was to investigate the Prevalence of anaemia in women and
children- all over the world from 1995-2011. The following were the key findings that came out
of the study;
The average iron deficiency in pregnant women was found to be 40.56 (SD = 1.41), the
iron deficiency was highest among children aged less than 5 years old (M = 44.98, SD =
1.33) and lowest among women in the reproductive age, that is, women aged between 15-
49 years old (M = 31.28, SD = 1.19).
The average iron deficiency is highest among children aged less than 5 years of age as
compared to the pregnant women all over the world.
The average iron deficiency is highest among the pregnant women as compared to the
women of reproductive age (aged between 15 – 49 years old) all over the world.
The average micronutrient deficiency rates in pre-school children are higher in countries
with poor dietary diversity than countries with good dietary diversity.
The average micronutrient deficiency rates in pre-school children is higher in Countries
with low GDP per capita (with less incomes) than countries with high GDP per capita
(with high incomes).
The main purpose of this study was to investigate the Prevalence of anaemia in women and
children- all over the world from 1995-2011. The following were the key findings that came out
of the study;
The average iron deficiency in pregnant women was found to be 40.56 (SD = 1.41), the
iron deficiency was highest among children aged less than 5 years old (M = 44.98, SD =
1.33) and lowest among women in the reproductive age, that is, women aged between 15-
49 years old (M = 31.28, SD = 1.19).
The average iron deficiency is highest among children aged less than 5 years of age as
compared to the pregnant women all over the world.
The average iron deficiency is highest among the pregnant women as compared to the
women of reproductive age (aged between 15 – 49 years old) all over the world.
The average micronutrient deficiency rates in pre-school children are higher in countries
with poor dietary diversity than countries with good dietary diversity.
The average micronutrient deficiency rates in pre-school children is higher in Countries
with low GDP per capita (with less incomes) than countries with high GDP per capita
(with high incomes).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Introduction
Anemia refers to a condition where the number of red blood cells or on the other hand their
oxygen-conveying limit isn't sufficient to meet ordinary physiologic demands (Tortora &
Grabowski, 2000) . Deficiency of iron is strongly believed to be the main cause of anemia
around the world (Stoltzfus , 2003), however lack of different vitamins, infections, inflammation,
and inherited hemoglobin disorders can likewise cause anemia (Totin, et al., 2002; Grantham-
McGregor & Ani, 2001; Lozoff , et al., 2003).
Based on the anemia cause, the consequences or rather the outcomes of the condition are
possibly long-lasting and serious. The results of deficiency of iron anemia—including disabled
psychological also, motor development (Kwong, et al., 2004; Scholz , et al., 1997) and expanded
helplessness to poisoning (Wright , et al., 2003; Kwong , et al., 2004) in youthful kids and
debilitated aerobic capacity and decreased work efficiency (Lozoff , et al., 2003; Totin, et al.,
2002) in grown-ups—have been broadly researched, yet anemia coming as a result of other
deficiencies in nutrition or inflammation can likewise reflect harmful wellbeing conditions. This
study sought to analyze the prevalence of anemia as well as iron deficiency among pregnant
women, women of reproductive age and children below five years old.
Anemia refers to a condition where the number of red blood cells or on the other hand their
oxygen-conveying limit isn't sufficient to meet ordinary physiologic demands (Tortora &
Grabowski, 2000) . Deficiency of iron is strongly believed to be the main cause of anemia
around the world (Stoltzfus , 2003), however lack of different vitamins, infections, inflammation,
and inherited hemoglobin disorders can likewise cause anemia (Totin, et al., 2002; Grantham-
McGregor & Ani, 2001; Lozoff , et al., 2003).
Based on the anemia cause, the consequences or rather the outcomes of the condition are
possibly long-lasting and serious. The results of deficiency of iron anemia—including disabled
psychological also, motor development (Kwong, et al., 2004; Scholz , et al., 1997) and expanded
helplessness to poisoning (Wright , et al., 2003; Kwong , et al., 2004) in youthful kids and
debilitated aerobic capacity and decreased work efficiency (Lozoff , et al., 2003; Totin, et al.,
2002) in grown-ups—have been broadly researched, yet anemia coming as a result of other
deficiencies in nutrition or inflammation can likewise reflect harmful wellbeing conditions. This
study sought to analyze the prevalence of anemia as well as iron deficiency among pregnant
women, women of reproductive age and children below five years old.
Literature Review
Conceivable reasons for nutritional anemia, inadequate folate is related with an expanded danger
of defects in neural tube and may likewise be related with antagonistic pregnancy results,
cardiovascular ailment, melancholy, and dementia, while vitamin B-12 inadequacy might be
related with an increased danger of coronary illness and neuropathy (Sadeghian , et al., 2006;
Mischoulon & Raab , 2007). Anemia that results from deficiency in vitamin A might be
connected with impeded insusceptibility, development, and vision (Sherry , et al., 2001). Iron
deficiency can likewise demonstrate irritation caused by an assortment of conditions, including
disease, or then again it might happen in chronic diseases, for example, chronic renal ailment or
endocrine issues that can result in diminished erythropoiesis (Lozoff , et al., 2003).
Prior information demonstrated that the predominance of anemia declined in the 1980s in US
preschool kids, yet not among ladies of childbearing age (Kwong, et al., 2004; Sherry , et al.,
2001).The present weight of sickliness in these 2 high-hazard bunches in the United States is
indistinct. In the present investigation, we utilized information from 2 ongoing National Health
and Nourishment Examination Surveys (NHANES 1988 – 1994 and 1999 – 2002) to look at late
changes in complete weakness predominance. We additionally examined between-study changes
in the predominance of a few sorts of frailty, including paleness related with iron inadequacy,
folate lack, vitamin B-12 insufficiency, vitamin An inadequacy, high blood lead, and irritation to
evaluate regardless of whether these components assumed a job in any watched changes in
absolute sickliness. Distinguishing proof of a probable reason for changes in sickliness could
feature existing general wellbeing mediations that have been fruitful or could recognize new
intercessions that may be considered.
Conceivable reasons for nutritional anemia, inadequate folate is related with an expanded danger
of defects in neural tube and may likewise be related with antagonistic pregnancy results,
cardiovascular ailment, melancholy, and dementia, while vitamin B-12 inadequacy might be
related with an increased danger of coronary illness and neuropathy (Sadeghian , et al., 2006;
Mischoulon & Raab , 2007). Anemia that results from deficiency in vitamin A might be
connected with impeded insusceptibility, development, and vision (Sherry , et al., 2001). Iron
deficiency can likewise demonstrate irritation caused by an assortment of conditions, including
disease, or then again it might happen in chronic diseases, for example, chronic renal ailment or
endocrine issues that can result in diminished erythropoiesis (Lozoff , et al., 2003).
Prior information demonstrated that the predominance of anemia declined in the 1980s in US
preschool kids, yet not among ladies of childbearing age (Kwong, et al., 2004; Sherry , et al.,
2001).The present weight of sickliness in these 2 high-hazard bunches in the United States is
indistinct. In the present investigation, we utilized information from 2 ongoing National Health
and Nourishment Examination Surveys (NHANES 1988 – 1994 and 1999 – 2002) to look at late
changes in complete weakness predominance. We additionally examined between-study changes
in the predominance of a few sorts of frailty, including paleness related with iron inadequacy,
folate lack, vitamin B-12 insufficiency, vitamin An inadequacy, high blood lead, and irritation to
evaluate regardless of whether these components assumed a job in any watched changes in
absolute sickliness. Distinguishing proof of a probable reason for changes in sickliness could
feature existing general wellbeing mediations that have been fruitful or could recognize new
intercessions that may be considered.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Research Questions
The following are the research questions that this study sought to answer;
Is there significant difference of iron deficiency between children (<5 year old) and
pregnant women all over the world? Is there significant difference of iron deficiency between children (<5 year old), pregnant
women and women of reproductive age (15-49 year old) all over the world?
Are the Micronutrient deficiency rates in pre-school children are higher in countries with
poor dietary diversity?
Do countries with low GDP per capita (with less incomes) have high micronutrient
deficiency rates in pre-school children?
Research Hypothesis
From the above research questions, the following research hypothesis were tested;
1. Null Hypothesis (H0): There is no significant difference in the average iron deficiency
between children (<5 year old) and pregnant women all over the world.
Alternative Hypothesis (HA): There is significant difference in the average iron deficiency
between children (<5 year old) and pregnant women all over the world.
2. Null Hypothesis (H0): There is no significant difference in the average iron deficiency
between children (<5 year old), pregnant women and women of reproductive age (15-49
year old) all over the world.
The following are the research questions that this study sought to answer;
Is there significant difference of iron deficiency between children (<5 year old) and
pregnant women all over the world? Is there significant difference of iron deficiency between children (<5 year old), pregnant
women and women of reproductive age (15-49 year old) all over the world?
Are the Micronutrient deficiency rates in pre-school children are higher in countries with
poor dietary diversity?
Do countries with low GDP per capita (with less incomes) have high micronutrient
deficiency rates in pre-school children?
Research Hypothesis
From the above research questions, the following research hypothesis were tested;
1. Null Hypothesis (H0): There is no significant difference in the average iron deficiency
between children (<5 year old) and pregnant women all over the world.
Alternative Hypothesis (HA): There is significant difference in the average iron deficiency
between children (<5 year old) and pregnant women all over the world.
2. Null Hypothesis (H0): There is no significant difference in the average iron deficiency
between children (<5 year old), pregnant women and women of reproductive age (15-49
year old) all over the world.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Alternative Hypothesis (HA): There is significant difference in the average iron deficiency
between children (<5 year old), pregnant women and women of reproductive age (15-49
year old) all over the world.
3. Null Hypothesis (H0): There is no significant difference in the average micronutrient
deficiency rates in pre-school children between countries with poor dietary diversity and
countries with good dietary diversity
Alternative Hypothesis (HA): The average micronutrient deficiency rates in pre-school
children are higher in countries with poor dietary diversity than countries with good
dietary diversity.
4. Null Hypothesis (H0): There is no significant difference in the average micronutrient
deficiency rates in pre-school children between Countries with low GDP per capita (with
less incomes) and countries with high GDP per capita (with high incomes)
Alternative Hypothesis (HA): The average micronutrient deficiency rates in pre-school
children is higher in Countries with low GDP per capita (with less incomes) than
countries with high GDP per capita (with high incomes).
between children (<5 year old), pregnant women and women of reproductive age (15-49
year old) all over the world.
3. Null Hypothesis (H0): There is no significant difference in the average micronutrient
deficiency rates in pre-school children between countries with poor dietary diversity and
countries with good dietary diversity
Alternative Hypothesis (HA): The average micronutrient deficiency rates in pre-school
children are higher in countries with poor dietary diversity than countries with good
dietary diversity.
4. Null Hypothesis (H0): There is no significant difference in the average micronutrient
deficiency rates in pre-school children between Countries with low GDP per capita (with
less incomes) and countries with high GDP per capita (with high incomes)
Alternative Hypothesis (HA): The average micronutrient deficiency rates in pre-school
children is higher in Countries with low GDP per capita (with less incomes) than
countries with high GDP per capita (with high incomes).
Results
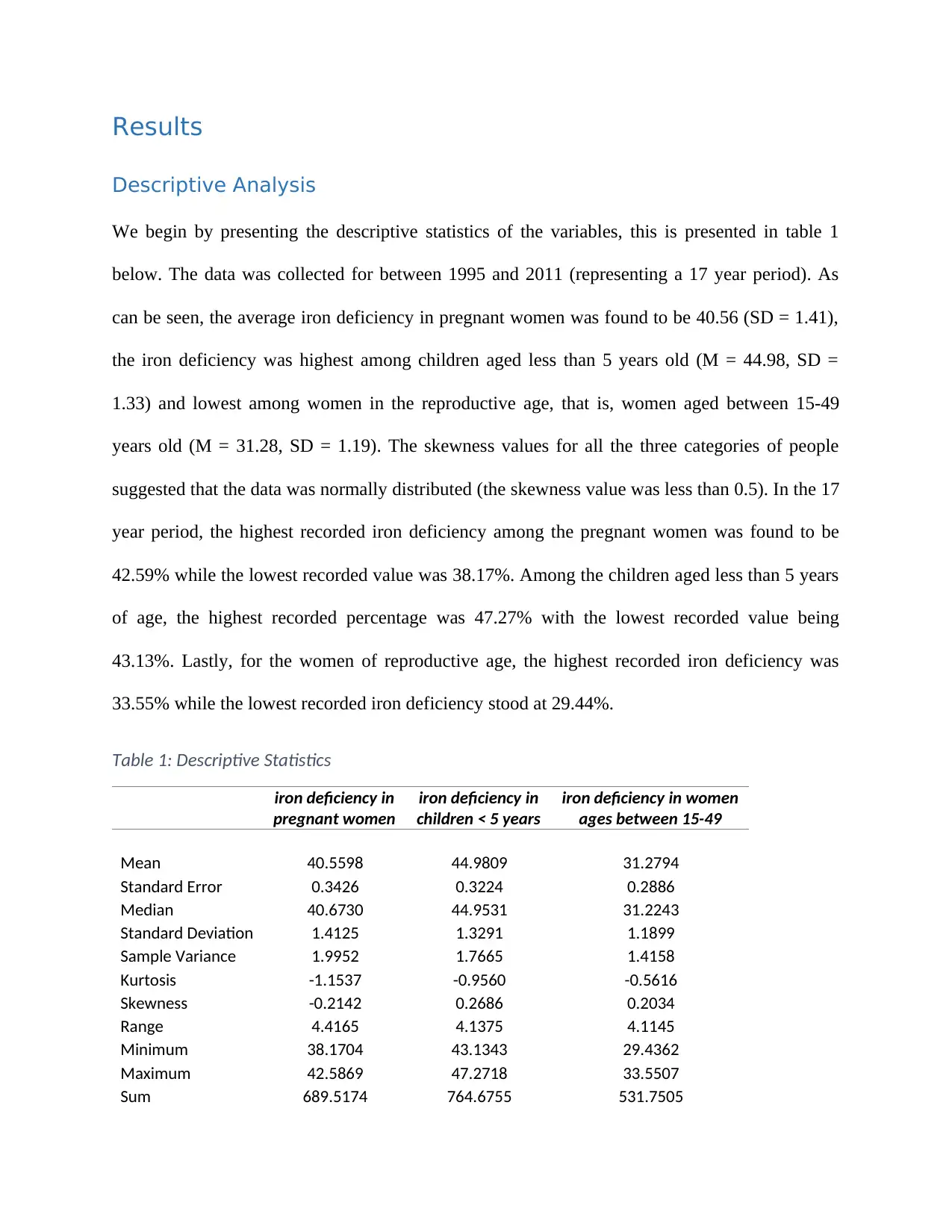
Descriptive Analysis
We begin by presenting the descriptive statistics of the variables, this is presented in table 1
below. The data was collected for between 1995 and 2011 (representing a 17 year period). As
can be seen, the average iron deficiency in pregnant women was found to be 40.56 (SD = 1.41),
the iron deficiency was highest among children aged less than 5 years old (M = 44.98, SD =
1.33) and lowest among women in the reproductive age, that is, women aged between 15-49
years old (M = 31.28, SD = 1.19). The skewness values for all the three categories of people
suggested that the data was normally distributed (the skewness value was less than 0.5). In the 17
year period, the highest recorded iron deficiency among the pregnant women was found to be
42.59% while the lowest recorded value was 38.17%. Among the children aged less than 5 years
of age, the highest recorded percentage was 47.27% with the lowest recorded value being
43.13%. Lastly, for the women of reproductive age, the highest recorded iron deficiency was
33.55% while the lowest recorded iron deficiency stood at 29.44%.
Table 1: Descriptive Statistics
iron deficiency in
pregnant women
iron deficiency in
children < 5 years
iron deficiency in women
ages between 15-49
Mean 40.5598 44.9809 31.2794
Standard Error 0.3426 0.3224 0.2886
Median 40.6730 44.9531 31.2243
Standard Deviation 1.4125 1.3291 1.1899
Sample Variance 1.9952 1.7665 1.4158
Kurtosis -1.1537 -0.9560 -0.5616
Skewness -0.2142 0.2686 0.2034
Range 4.4165 4.1375 4.1145
Minimum 38.1704 43.1343 29.4362
Maximum 42.5869 47.2718 33.5507
Sum 689.5174 764.6755 531.7505
Descriptive Analysis
We begin by presenting the descriptive statistics of the variables, this is presented in table 1
below. The data was collected for between 1995 and 2011 (representing a 17 year period). As
can be seen, the average iron deficiency in pregnant women was found to be 40.56 (SD = 1.41),
the iron deficiency was highest among children aged less than 5 years old (M = 44.98, SD =
1.33) and lowest among women in the reproductive age, that is, women aged between 15-49
years old (M = 31.28, SD = 1.19). The skewness values for all the three categories of people
suggested that the data was normally distributed (the skewness value was less than 0.5). In the 17
year period, the highest recorded iron deficiency among the pregnant women was found to be
42.59% while the lowest recorded value was 38.17%. Among the children aged less than 5 years
of age, the highest recorded percentage was 47.27% with the lowest recorded value being
43.13%. Lastly, for the women of reproductive age, the highest recorded iron deficiency was
33.55% while the lowest recorded iron deficiency stood at 29.44%.
Table 1: Descriptive Statistics
iron deficiency in
pregnant women
iron deficiency in
children < 5 years
iron deficiency in women
ages between 15-49
Mean 40.5598 44.9809 31.2794
Standard Error 0.3426 0.3224 0.2886
Median 40.6730 44.9531 31.2243
Standard Deviation 1.4125 1.3291 1.1899
Sample Variance 1.9952 1.7665 1.4158
Kurtosis -1.1537 -0.9560 -0.5616
Skewness -0.2142 0.2686 0.2034
Range 4.4165 4.1375 4.1145
Minimum 38.1704 43.1343 29.4362
Maximum 42.5869 47.2718 33.5507
Sum 689.5174 764.6755 531.7505
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Count 17.0000 17.0000 17.0000
Inferential Analysis
This study sought to test 4 research hypothesis which would subsequently answer the four
research questions that were earlier given.
Hypothesis 1:
The hypothesis tested is give below;
Null Hypothesis (H0): There is no significant difference in the average iron deficiency between
children (<5 year old) and pregnant women all over the world.
Alternative Hypothesis (HA): There is significant difference in the average iron deficiency
between children (<5 year old) and pregnant women all over the world.
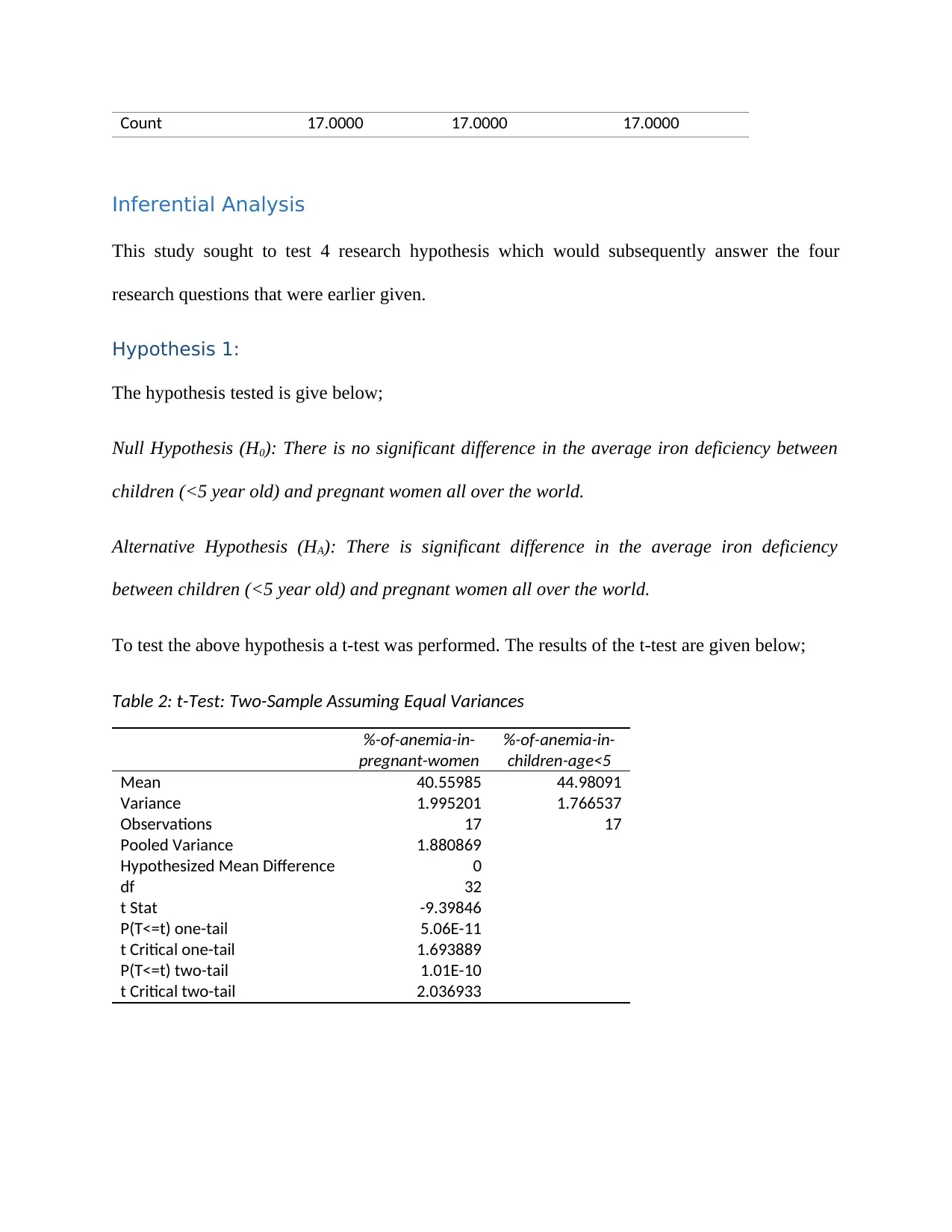
To test the above hypothesis a t-test was performed. The results of the t-test are given below;
Table 2: t-Test: Two-Sample Assuming Equal Variances
%-of-anemia-in-
pregnant-women
%-of-anemia-in-
children-age<5
Mean 40.55985 44.98091
Variance 1.995201 1.766537
Observations 17 17
Pooled Variance 1.880869
Hypothesized Mean Difference 0
df 32
t Stat -9.39846
P(T<=t) one-tail 5.06E-11
t Critical one-tail 1.693889
P(T<=t) two-tail 1.01E-10
t Critical two-tail 2.036933
Inferential Analysis
This study sought to test 4 research hypothesis which would subsequently answer the four
research questions that were earlier given.
Hypothesis 1:
The hypothesis tested is give below;
Null Hypothesis (H0): There is no significant difference in the average iron deficiency between
children (<5 year old) and pregnant women all over the world.
Alternative Hypothesis (HA): There is significant difference in the average iron deficiency
between children (<5 year old) and pregnant women all over the world.
To test the above hypothesis a t-test was performed. The results of the t-test are given below;
Table 2: t-Test: Two-Sample Assuming Equal Variances
%-of-anemia-in-
pregnant-women
%-of-anemia-in-
children-age<5
Mean 40.55985 44.98091
Variance 1.995201 1.766537
Observations 17 17
Pooled Variance 1.880869
Hypothesized Mean Difference 0
df 32
t Stat -9.39846
P(T<=t) one-tail 5.06E-11
t Critical one-tail 1.693889
P(T<=t) two-tail 1.01E-10
t Critical two-tail 2.036933
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
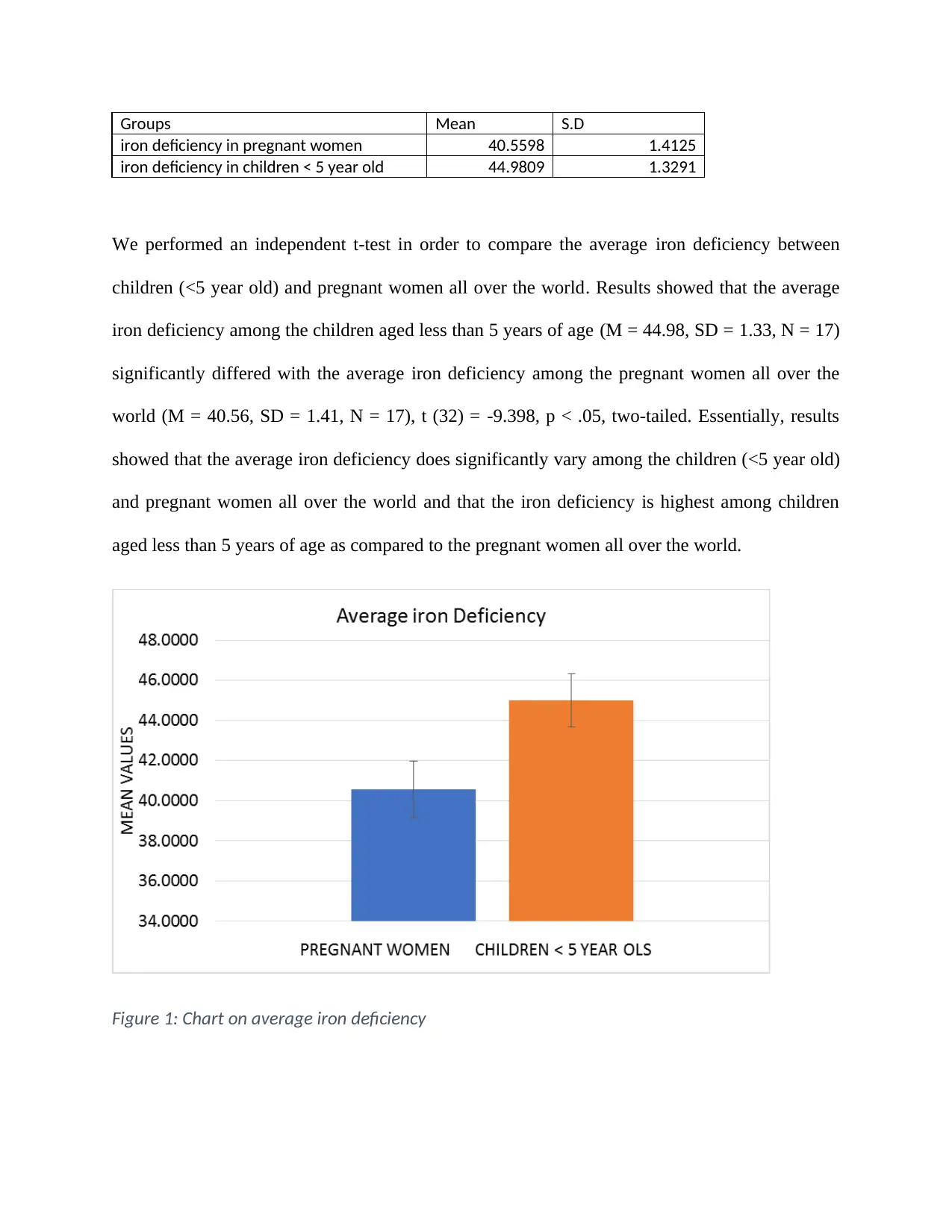
Groups Mean S.D
iron deficiency in pregnant women 40.5598 1.4125
iron deficiency in children < 5 year old 44.9809 1.3291
We performed an independent t-test in order to compare the average iron deficiency between
children (<5 year old) and pregnant women all over the world. Results showed that the average
iron deficiency among the children aged less than 5 years of age (M = 44.98, SD = 1.33, N = 17)
significantly differed with the average iron deficiency among the pregnant women all over the
world (M = 40.56, SD = 1.41, N = 17), t (32) = -9.398, p < .05, two-tailed. Essentially, results
showed that the average iron deficiency does significantly vary among the children (<5 year old)
and pregnant women all over the world and that the iron deficiency is highest among children
aged less than 5 years of age as compared to the pregnant women all over the world.
Figure 1: Chart on average iron deficiency
iron deficiency in pregnant women 40.5598 1.4125
iron deficiency in children < 5 year old 44.9809 1.3291
We performed an independent t-test in order to compare the average iron deficiency between
children (<5 year old) and pregnant women all over the world. Results showed that the average
iron deficiency among the children aged less than 5 years of age (M = 44.98, SD = 1.33, N = 17)
significantly differed with the average iron deficiency among the pregnant women all over the
world (M = 40.56, SD = 1.41, N = 17), t (32) = -9.398, p < .05, two-tailed. Essentially, results
showed that the average iron deficiency does significantly vary among the children (<5 year old)
and pregnant women all over the world and that the iron deficiency is highest among children
aged less than 5 years of age as compared to the pregnant women all over the world.
Figure 1: Chart on average iron deficiency
Hypothesis 2:
The hypothesis tested is give below;
Null Hypothesis (H0): There is no significant difference in the average iron deficiency among
children (<5 year old), pregnant women and women of reproductive age (15-49 year old) all
over the world.
Alternative Hypothesis (HA): There is significant difference in the average iron deficiency among
children (<5 year old), pregnant women and women of reproductive age (15-49 year old) all
over the world.
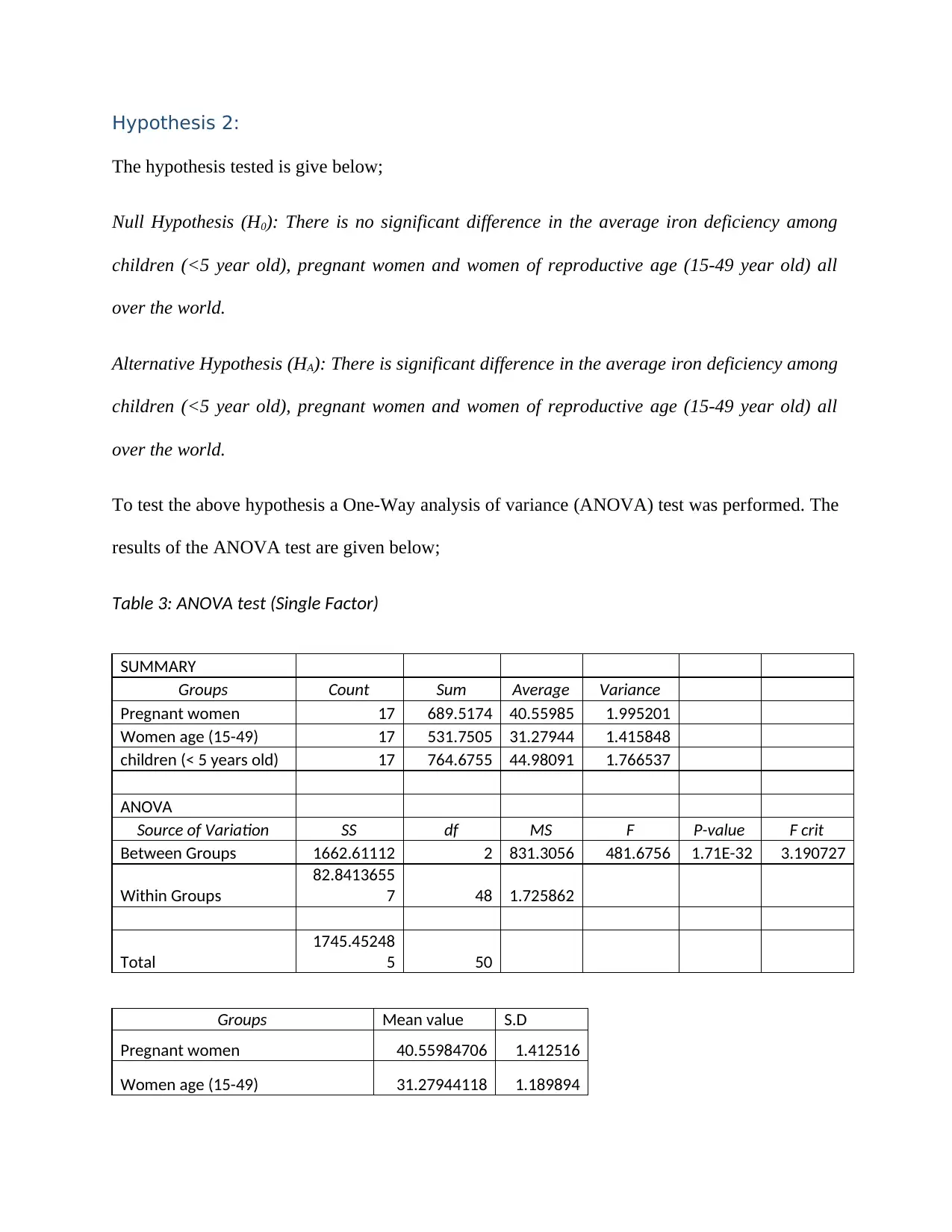
To test the above hypothesis a One-Way analysis of variance (ANOVA) test was performed. The
results of the ANOVA test are given below;
Table 3: ANOVA test (Single Factor)
SUMMARY
Groups Count Sum Average Variance
Pregnant women 17 689.5174 40.55985 1.995201
Women age (15-49) 17 531.7505 31.27944 1.415848
children (< 5 years old) 17 764.6755 44.98091 1.766537
ANOVA
Source of Variation SS df MS F P-value F crit
Between Groups 1662.61112 2 831.3056 481.6756 1.71E-32 3.190727
Within Groups
82.8413655
7 48 1.725862
Total
1745.45248
5 50
Groups Mean value S.D
Pregnant women 40.55984706 1.412516
Women age (15-49) 31.27944118 1.189894
The hypothesis tested is give below;
Null Hypothesis (H0): There is no significant difference in the average iron deficiency among
children (<5 year old), pregnant women and women of reproductive age (15-49 year old) all
over the world.
Alternative Hypothesis (HA): There is significant difference in the average iron deficiency among
children (<5 year old), pregnant women and women of reproductive age (15-49 year old) all
over the world.
To test the above hypothesis a One-Way analysis of variance (ANOVA) test was performed. The
results of the ANOVA test are given below;
Table 3: ANOVA test (Single Factor)
SUMMARY
Groups Count Sum Average Variance
Pregnant women 17 689.5174 40.55985 1.995201
Women age (15-49) 17 531.7505 31.27944 1.415848
children (< 5 years old) 17 764.6755 44.98091 1.766537
ANOVA
Source of Variation SS df MS F P-value F crit
Between Groups 1662.61112 2 831.3056 481.6756 1.71E-32 3.190727
Within Groups
82.8413655
7 48 1.725862
Total
1745.45248
5 50
Groups Mean value S.D
Pregnant women 40.55984706 1.412516
Women age (15-49) 31.27944118 1.189894
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 20

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.