Antibiotic Use in Children's Ear Infections
VerifiedAdded on 2020/04/07
|15
|3469
|457
AI Summary
This assignment delves into the topic of antibiotic use in treating ear infections in children. It examines the existing medical guidelines, analyzes research studies on the efficacy of antibiotics for different types of ear infections, and explores the potential drawbacks of overprescribing antibiotics, such as disruption of the gut microbiome and the rise of antibiotic resistance.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Antibiotics and ear problems
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

Table of Contents
Introduction..............................................................................................................................................3
Antibiotics for children.............................................................................................................................3
Role of antibiotics for treating AOM.......................................................................................................4
Oral antibiotics vs. antibiotic eardrops.....................................................................................................5
Critical Appraisal Skills Programme........................................................................................................6
Why are more kids impacted by Otitis media then adults?......................................................................6
Cure of Otitis media.................................................................................................................................7
Management.............................................................................................................................................8
Recommendations..................................................................................................................................10
Conclusion..............................................................................................................................................11
References..............................................................................................................................................11
Appendices.............................................................................................................................................13
Introduction..............................................................................................................................................3
Antibiotics for children.............................................................................................................................3
Role of antibiotics for treating AOM.......................................................................................................4
Oral antibiotics vs. antibiotic eardrops.....................................................................................................5
Critical Appraisal Skills Programme........................................................................................................6
Why are more kids impacted by Otitis media then adults?......................................................................6
Cure of Otitis media.................................................................................................................................7
Management.............................................................................................................................................8
Recommendations..................................................................................................................................10
Conclusion..............................................................................................................................................11
References..............................................................................................................................................11
Appendices.............................................................................................................................................13
Introduction
The topic chosen for the study is “antibiotics and ear problems” and the article chosen for the
study is named as- “Use of Antibiotics in Preventing Recurrent Acute Otitis Media and in
Treating Otitis Media with Effusion” (Williams, 1993). This topic has been chosen for kids who
have chronic suppurations Otitis media (CSOM), so that the impact of antibiotics can be seen on
those kids. This article has been used for showing the efficiency of antibiotics for prophylaxis of
recurring Otitis medium and cure of Otitis media with effusion (OME) in kids.
Antibiotics for children
Antibiotics seem to be useful yet the recurring Otitis medium has meagre impact. OME has
impact in short run but it isn't effective in long run ("Use of antibiotics in young children may
disrupt gut microbiome", 2015). Also this article has limitations since the group of patients
which can be benefited was not rightly identified. Even though there has been huge amount of
expenditure by US pediatric population for the cost of Otitis media, still the treatment of these
conditions cannot be taken as a dependable one. In case of the recurring acute Otitis media, the
impact of antibiotics cannot be known ("Antibiotics not effective for children with infected
eczema", 2016). There are certain set of pediatricians who believe that antibiotics are more
effective and the other set believes that century has a long lasting effect. In case of recurring
AOM, The issue seems to be of choice, decision, and timing of antibiotic prophylaxis. This study
undertook meta–analysis of the role of antibiotics for the cure of OME and in prophylaxis of
recurring AOM.
The Otitis media states that child has some fluid or liquid on the backside of his or her eardrum.
These can be segregated into two types known as acute Otitis media (AOM) and Otitis media
The topic chosen for the study is “antibiotics and ear problems” and the article chosen for the
study is named as- “Use of Antibiotics in Preventing Recurrent Acute Otitis Media and in
Treating Otitis Media with Effusion” (Williams, 1993). This topic has been chosen for kids who
have chronic suppurations Otitis media (CSOM), so that the impact of antibiotics can be seen on
those kids. This article has been used for showing the efficiency of antibiotics for prophylaxis of
recurring Otitis medium and cure of Otitis media with effusion (OME) in kids.
Antibiotics for children
Antibiotics seem to be useful yet the recurring Otitis medium has meagre impact. OME has
impact in short run but it isn't effective in long run ("Use of antibiotics in young children may
disrupt gut microbiome", 2015). Also this article has limitations since the group of patients
which can be benefited was not rightly identified. Even though there has been huge amount of
expenditure by US pediatric population for the cost of Otitis media, still the treatment of these
conditions cannot be taken as a dependable one. In case of the recurring acute Otitis media, the
impact of antibiotics cannot be known ("Antibiotics not effective for children with infected
eczema", 2016). There are certain set of pediatricians who believe that antibiotics are more
effective and the other set believes that century has a long lasting effect. In case of recurring
AOM, The issue seems to be of choice, decision, and timing of antibiotic prophylaxis. This study
undertook meta–analysis of the role of antibiotics for the cure of OME and in prophylaxis of
recurring AOM.
The Otitis media states that child has some fluid or liquid on the backside of his or her eardrum.
These can be segregated into two types known as acute Otitis media (AOM) and Otitis media
with effusion (OME) (Are Children Overprescribed Antibiotics?, 2008). In a cute won the fluid
is having infection or virus or any kind of bacteria that leads to fever or pain. The update is
media with diffusion is one where the flu it is not infected and doesn't give any kind of pain. It is
important for the doctor to find out what kind of Otitis media it is. It can be caused by blocking
of any to connecting the mid of ear with the nose (Bhutta, 2014). In case this to gets blockage
then the fluid collection can be seen at the back of the eardrum. In case there is bacteria
developed within this fluid then this can be very painful and most of the times it is not due to
bacteria but do you to any virus.
The general time when this kind of infection or Otitis media occurs is during the winters and this
kind of problem is more seen in kids going to day-care. Even if a child catches any upper
respiratory infection or a cold then also this can happen. But it has to be kept in mind that water
going inside the ear doesn't lead to Otitis media.
Role of antibiotics for treating AOM
Antibiotics are just useful in specific instances of AOM. If the kid is of two ears are lesser of age
or kids with very severe and re-occurring pain or has high fever of more than 102°F then
antibiotics can be utilised for reduction in pain and bringing back the body temperature to
normal. However this would also take around 2 to 3 days (Slovis, 2012). In the children who are
bigger than two years of age over the kids who have almost no symptom then it is preferable that
antibiotics are not utilized for AOM. These antibiotics usually have Side effects like diarrhea,
upsetting of stomach and body rashes. These side effects can be seen when any kid who has been
treated with antibiotics for this ear infection gets harsh infections by antibiotic resistant bacteria.
Therefore doctors generally avoid using antibiotics and recommend these only for kids who have
high fever or severe pain in that ear (Pichichero, 2015). In such cases, the patient is treated with
is having infection or virus or any kind of bacteria that leads to fever or pain. The update is
media with diffusion is one where the flu it is not infected and doesn't give any kind of pain. It is
important for the doctor to find out what kind of Otitis media it is. It can be caused by blocking
of any to connecting the mid of ear with the nose (Bhutta, 2014). In case this to gets blockage
then the fluid collection can be seen at the back of the eardrum. In case there is bacteria
developed within this fluid then this can be very painful and most of the times it is not due to
bacteria but do you to any virus.
The general time when this kind of infection or Otitis media occurs is during the winters and this
kind of problem is more seen in kids going to day-care. Even if a child catches any upper
respiratory infection or a cold then also this can happen. But it has to be kept in mind that water
going inside the ear doesn't lead to Otitis media.
Role of antibiotics for treating AOM
Antibiotics are just useful in specific instances of AOM. If the kid is of two ears are lesser of age
or kids with very severe and re-occurring pain or has high fever of more than 102°F then
antibiotics can be utilised for reduction in pain and bringing back the body temperature to
normal. However this would also take around 2 to 3 days (Slovis, 2012). In the children who are
bigger than two years of age over the kids who have almost no symptom then it is preferable that
antibiotics are not utilized for AOM. These antibiotics usually have Side effects like diarrhea,
upsetting of stomach and body rashes. These side effects can be seen when any kid who has been
treated with antibiotics for this ear infection gets harsh infections by antibiotic resistant bacteria.
Therefore doctors generally avoid using antibiotics and recommend these only for kids who have
high fever or severe pain in that ear (Pichichero, 2015). In such cases, the patient is treated with
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
medication for pain. Even in case of OME, the antibiotics are not advantages because the middle
of the ear isn't impacted by the fluid (Macneil, 2006).
The study conducted by Leach et al and published in 2008, the study was for formed in
aboriginal societies where majority of kids have reoccurring mid ears ailment from very early
age. So these results could also be utilized for different groups which have higher rates of Otis
media with effusion (Leach, Morris & Mathews, 2008).
This study showed that Aboriginal infants who have OME and who have been continuously
getting amoxicillin the ones who have normal ears, lesser perforations and fewer pneumococcal
carriage. There had been no major rise in resistant pneumococcal on NCHi in amoxicillin kids in
comparison to the kids who are flexible and we have got continuous pediatric observation
with antibiotic cure for symptomatic ailments. These studies have one thing in common which is
that the utilization of long run on antibiotics would not be significant when the ailment is not
severe.
Oral antibiotics vs. antibiotic eardrops
As for the studies, there are various side effects and disadvantages due to which people avoid
using antibiotics. An antibiotic is a strong medicine which is used for killing bacteria but for the
infections in ear, eardrops can be more effective in comparison to oral medicines. These oral
antibiotics have more chances of causing resistant bacteria out of the ear. Also in upcoming
times these drugs might stop working. So in future it can make the ailment to be more difficult
and very expensive to be treated.
The eardrops in form of antibiotics remove the bacteria weaker and in a more complete manner
rather than oral antibiotics. So the antibiotic ear drops are more effective because these do not
of the ear isn't impacted by the fluid (Macneil, 2006).
The study conducted by Leach et al and published in 2008, the study was for formed in
aboriginal societies where majority of kids have reoccurring mid ears ailment from very early
age. So these results could also be utilized for different groups which have higher rates of Otis
media with effusion (Leach, Morris & Mathews, 2008).
This study showed that Aboriginal infants who have OME and who have been continuously
getting amoxicillin the ones who have normal ears, lesser perforations and fewer pneumococcal
carriage. There had been no major rise in resistant pneumococcal on NCHi in amoxicillin kids in
comparison to the kids who are flexible and we have got continuous pediatric observation
with antibiotic cure for symptomatic ailments. These studies have one thing in common which is
that the utilization of long run on antibiotics would not be significant when the ailment is not
severe.
Oral antibiotics vs. antibiotic eardrops
As for the studies, there are various side effects and disadvantages due to which people avoid
using antibiotics. An antibiotic is a strong medicine which is used for killing bacteria but for the
infections in ear, eardrops can be more effective in comparison to oral medicines. These oral
antibiotics have more chances of causing resistant bacteria out of the ear. Also in upcoming
times these drugs might stop working. So in future it can make the ailment to be more difficult
and very expensive to be treated.
The eardrops in form of antibiotics remove the bacteria weaker and in a more complete manner
rather than oral antibiotics. So the antibiotic ear drops are more effective because these do not
get in the bloodstream and the medicine directly goes to the infected area. When a comparison
has to be made between oral antibiotics and antibiotic ear drop then the ear drops have lesser side
effects. The side-effects of using oral antibiotics include headache, vomiting and nausea, recipe
allergic reactions, diarrhoea, stomach ache, rashes on the body etc. (Brunk, 2011).
Critical Appraisal Skills Programme
The CASP tool utilized in the study, for the literature review, is Randomised Controlled Trial
(RCT). It is a kind of interventional or experimental learning plan. The participants were
indiscriminately assigned to be given the antibiotics being tested or a control cure (generally in
RCT, it is the typical treatment or a placebo). All the sections of the study were then recorded
and the sum or severity of the illness was considered in the intervention group and evaluated
along the control group.
Why are more kids impacted by Otitis media then adults?
There are various causes for which kids are prone to have this disease of Otitis media rather than
adults. First, the kids have less resistance and they find it more difficult to fight with infections.
This happens since there are immune system is still under development. One more causes that
impacts their immunity is there eustachian tube. This tube is a tiny message which links the open
area of the throat with the mid of the ear. It is straighter and smaller in kids rather than in other
therefore it plays a major role in Otitis media (Office, 2015).
The eustachian tube is generally closed however it opens on a regular basis for ventilating a
replenishing the air in the mid ear. This tube also makes equilibrium of ear pressure in the mid
ear by responding to the environmental changes. But the two which is blocked due to swelling of
its lining or which has a blockage due to mucus caused by cold or any other reason can't open for
has to be made between oral antibiotics and antibiotic ear drop then the ear drops have lesser side
effects. The side-effects of using oral antibiotics include headache, vomiting and nausea, recipe
allergic reactions, diarrhoea, stomach ache, rashes on the body etc. (Brunk, 2011).
Critical Appraisal Skills Programme
The CASP tool utilized in the study, for the literature review, is Randomised Controlled Trial
(RCT). It is a kind of interventional or experimental learning plan. The participants were
indiscriminately assigned to be given the antibiotics being tested or a control cure (generally in
RCT, it is the typical treatment or a placebo). All the sections of the study were then recorded
and the sum or severity of the illness was considered in the intervention group and evaluated
along the control group.
Why are more kids impacted by Otitis media then adults?
There are various causes for which kids are prone to have this disease of Otitis media rather than
adults. First, the kids have less resistance and they find it more difficult to fight with infections.
This happens since there are immune system is still under development. One more causes that
impacts their immunity is there eustachian tube. This tube is a tiny message which links the open
area of the throat with the mid of the ear. It is straighter and smaller in kids rather than in other
therefore it plays a major role in Otitis media (Office, 2015).
The eustachian tube is generally closed however it opens on a regular basis for ventilating a
replenishing the air in the mid ear. This tube also makes equilibrium of ear pressure in the mid
ear by responding to the environmental changes. But the two which is blocked due to swelling of
its lining or which has a blockage due to mucus caused by cold or any other reason can't open for
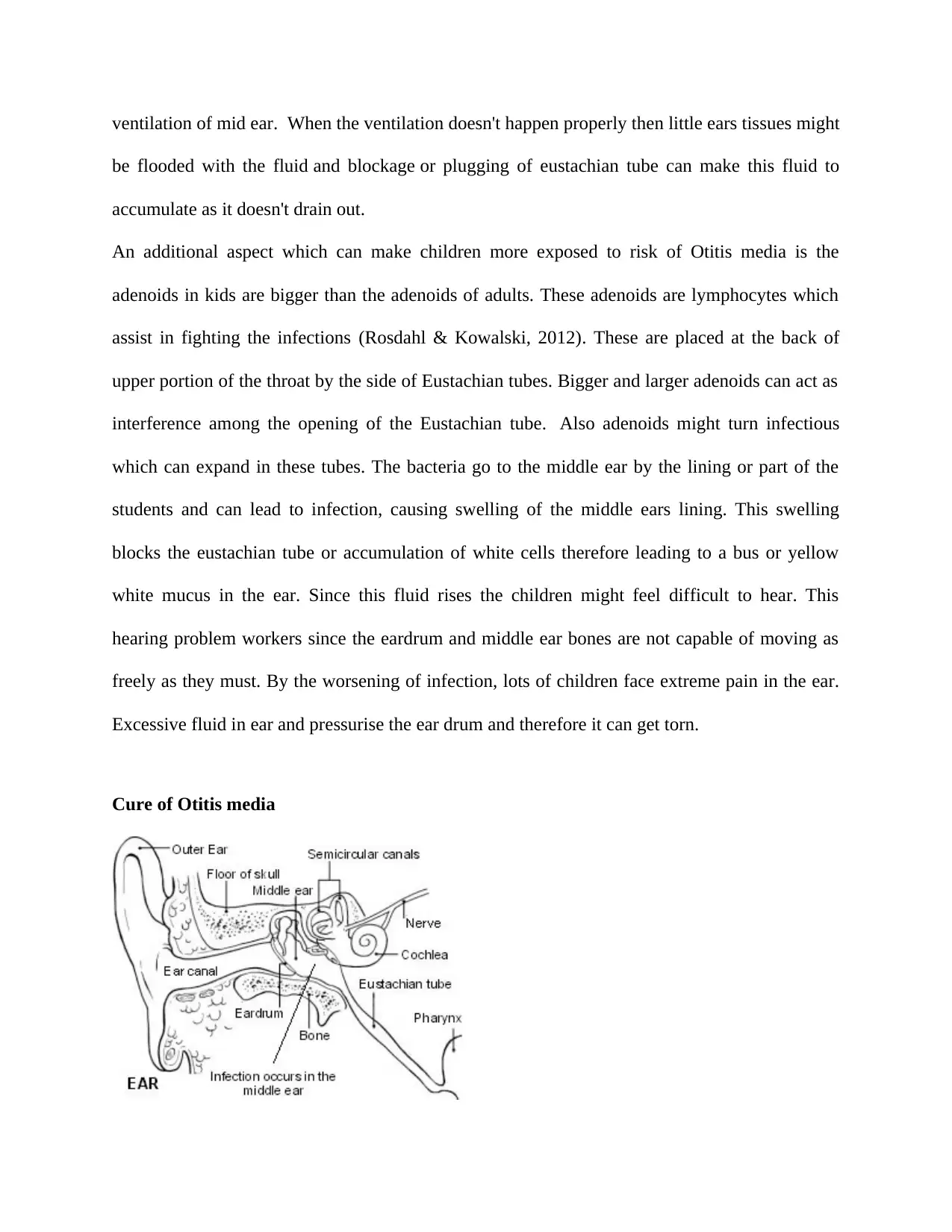
ventilation of mid ear. When the ventilation doesn't happen properly then little ears tissues might
be flooded with the fluid and blockage or plugging of eustachian tube can make this fluid to
accumulate as it doesn't drain out.
An additional aspect which can make children more exposed to risk of Otitis media is the
adenoids in kids are bigger than the adenoids of adults. These adenoids are lymphocytes which
assist in fighting the infections (Rosdahl & Kowalski, 2012). These are placed at the back of
upper portion of the throat by the side of Eustachian tubes. Bigger and larger adenoids can act as
interference among the opening of the Eustachian tube. Also adenoids might turn infectious
which can expand in these tubes. The bacteria go to the middle ear by the lining or part of the
students and can lead to infection, causing swelling of the middle ears lining. This swelling
blocks the eustachian tube or accumulation of white cells therefore leading to a bus or yellow
white mucus in the ear. Since this fluid rises the children might feel difficult to hear. This
hearing problem workers since the eardrum and middle ear bones are not capable of moving as
freely as they must. By the worsening of infection, lots of children face extreme pain in the ear.
Excessive fluid in ear and pressurise the ear drum and therefore it can get torn.
Cure of Otitis media
be flooded with the fluid and blockage or plugging of eustachian tube can make this fluid to
accumulate as it doesn't drain out.
An additional aspect which can make children more exposed to risk of Otitis media is the
adenoids in kids are bigger than the adenoids of adults. These adenoids are lymphocytes which
assist in fighting the infections (Rosdahl & Kowalski, 2012). These are placed at the back of
upper portion of the throat by the side of Eustachian tubes. Bigger and larger adenoids can act as
interference among the opening of the Eustachian tube. Also adenoids might turn infectious
which can expand in these tubes. The bacteria go to the middle ear by the lining or part of the
students and can lead to infection, causing swelling of the middle ears lining. This swelling
blocks the eustachian tube or accumulation of white cells therefore leading to a bus or yellow
white mucus in the ear. Since this fluid rises the children might feel difficult to hear. This
hearing problem workers since the eardrum and middle ear bones are not capable of moving as
freely as they must. By the worsening of infection, lots of children face extreme pain in the ear.
Excessive fluid in ear and pressurise the ear drum and therefore it can get torn.
Cure of Otitis media
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Source: "Acute Otitis Media in Children. Ear infection information. Patient", 2017
It brings a severe pain in the ear. Lots of physicians might suggest utilising the antibiotic in case
the middle ear infection is severe. In case the child experiences been, physician might also
suggest any pain relieving medication. It is important to follow the instructions of the physician.
Once the antibiotics are started then full course has to be followed. Most of the physicians want
the child to come back for a follow-up check up for examining if the infection has been
removed. And it has been seen in many cases that lots of bacteria can make Otitis media and
these bacteria also have resistance to a few antibiotics. This means whenever antibiotics are
provided for cold, flu, viral infections or cough then the body stops responding to these
antibiotics. That means that unneccesarry antibiotics in a body make the treatments to be less
effective with respect to infections. Therefore many sets of antibiotics might need to be tried for
getting this ear infection cleared. Also these antibiotics have many side-effects. After even the
clearing of infection, fluid might stay in the middle ear for many months. The middle ear fluid
that isn't infectious goes away after 3 to 6 weeks (Abou-halawa, Khan and Alrobaee, 2012).
There is one more kind of antibiotic which can be given by physicians, which is to quicken the
removal of fluid from the ear of the child. In case this fluid is present for more than three months
and also causes hearing loss then there are due to be inserted in the affected region of the ear.
This kind of operation is known as myringotomy and it can be done by surgeon who is generally
an otolaryngologist.
Management
Major cases of AOM and Otitis media get resolved quickly. Devoid of any particular treatment,
the symptoms get better in 24 hours and 60% of the kids and recovery is seen within three days
It brings a severe pain in the ear. Lots of physicians might suggest utilising the antibiotic in case
the middle ear infection is severe. In case the child experiences been, physician might also
suggest any pain relieving medication. It is important to follow the instructions of the physician.
Once the antibiotics are started then full course has to be followed. Most of the physicians want
the child to come back for a follow-up check up for examining if the infection has been
removed. And it has been seen in many cases that lots of bacteria can make Otitis media and
these bacteria also have resistance to a few antibiotics. This means whenever antibiotics are
provided for cold, flu, viral infections or cough then the body stops responding to these
antibiotics. That means that unneccesarry antibiotics in a body make the treatments to be less
effective with respect to infections. Therefore many sets of antibiotics might need to be tried for
getting this ear infection cleared. Also these antibiotics have many side-effects. After even the
clearing of infection, fluid might stay in the middle ear for many months. The middle ear fluid
that isn't infectious goes away after 3 to 6 weeks (Abou-halawa, Khan and Alrobaee, 2012).
There is one more kind of antibiotic which can be given by physicians, which is to quicken the
removal of fluid from the ear of the child. In case this fluid is present for more than three months
and also causes hearing loss then there are due to be inserted in the affected region of the ear.
This kind of operation is known as myringotomy and it can be done by surgeon who is generally
an otolaryngologist.
Management
Major cases of AOM and Otitis media get resolved quickly. Devoid of any particular treatment,
the symptoms get better in 24 hours and 60% of the kids and recovery is seen within three days
in around 80% of the kids. Whereas enough analgesia has to be given in each of
the case, Antibiotics must be avoided for the Miles – two – moderate cases and when there is no
surety of the diagnosis in patients below the age of two ears.
It is also suggested by many studies that most of the children should not be given antibiotics are
delayed intimated prescriptions. No antibiotics perception means that there is awareness that
antibiotics would create less difference to the symptoms but would have even more side-effects.
It would also cause body to be resistant against the antibiotics.
Delayed antibiotics prescription means that antibiotics have to be given only if there is no
improvement in the symptoms in the four days of father on in case there is any key worsening at
any point of time. For both of these prescriptions the review list necessary in case of
deteriorating situation or in case the symptoms do not improve in four days of their start.
But these antibiotics prescriptions can be given to certain as given below:
To the kids who are systemically you'll don't need any admission to the clinic or hospital, to the
kids and high risk of congregation due to the long, kidney, liver, heart or neuromuscular ailment,
to the kids who are immunocompromised, to the kids who have symptoms for more than 4 days
with no sign of improvement (Milne, 2007).
In case the antibiotics are needed, five days course of amoxicillin can be given and in case the
kids are allergic to penicillin then five days course of erythromycin or clarithromycin must be
given.
It is also suggested that antibiotics are not important for treating complicated AOM in an
otherwise fit kid. For management of AOM, it is important to utilise a complete strategy by
prescribing any antibiotic only when it is needed clinically. It is also important that the parents
and guardian of the child are explained regarding the advantages and side-effects of intimated
the case, Antibiotics must be avoided for the Miles – two – moderate cases and when there is no
surety of the diagnosis in patients below the age of two ears.
It is also suggested by many studies that most of the children should not be given antibiotics are
delayed intimated prescriptions. No antibiotics perception means that there is awareness that
antibiotics would create less difference to the symptoms but would have even more side-effects.
It would also cause body to be resistant against the antibiotics.
Delayed antibiotics prescription means that antibiotics have to be given only if there is no
improvement in the symptoms in the four days of father on in case there is any key worsening at
any point of time. For both of these prescriptions the review list necessary in case of
deteriorating situation or in case the symptoms do not improve in four days of their start.
But these antibiotics prescriptions can be given to certain as given below:
To the kids who are systemically you'll don't need any admission to the clinic or hospital, to the
kids and high risk of congregation due to the long, kidney, liver, heart or neuromuscular ailment,
to the kids who are immunocompromised, to the kids who have symptoms for more than 4 days
with no sign of improvement (Milne, 2007).
In case the antibiotics are needed, five days course of amoxicillin can be given and in case the
kids are allergic to penicillin then five days course of erythromycin or clarithromycin must be
given.
It is also suggested that antibiotics are not important for treating complicated AOM in an
otherwise fit kid. For management of AOM, it is important to utilise a complete strategy by
prescribing any antibiotic only when it is needed clinically. It is also important that the parents
and guardian of the child are explained regarding the advantages and side-effects of intimated
while thinking about a watchful waiting method. Generally the parents consider the return of
watchful waiting rather than use of antibiotics. The utilisation of antihistamines and
decongestants must be discouraged do you to their in adequate impact and safety issues,
particularly in the kids of two ears and below. The benefits of antibiotics are very less in
uncomplicated ailments.
A Cochrane Study of 8 RCTs (randomised controlled trials) – 6 double-blinded with 2287 kids in
all was used to compare antibiotics with place of for uncomplicated AOM in otherwise healthy
kids ("The journal of Family practice", 2017). This study reflected that kids who were cured by
use of antibiotics are less likely to suffer with pain in 24 hours beyond start of treatment, in
comparison to kids who were untreated. But 7% lesser kids who got antibiotics had been for 2 to
7 days then the untreated kids. So it could be seen that kids who were given antibiotics did not
see any key reduction in recurrence of AOM, rather there were issues of rice in the area, rashes
and nausea. The study also showed a moderate rise in failure rate of placebo cure for kids below
the age of two ears and for the kids with bilateral ailments. So there was a concluding thought
that the possible advantages and rest of antibiotics for AOM are very less.
Recommendations
It is suggested that studies have to be carried out which gave validation for shorter and clearance
of a fusion been useful for improving the speech development and also the validation of long run
treatment producing prolonged the remission of effusion. Due studies need to be done because
there are particular alternate surgical treatments available for Otitis medium.
watchful waiting rather than use of antibiotics. The utilisation of antihistamines and
decongestants must be discouraged do you to their in adequate impact and safety issues,
particularly in the kids of two ears and below. The benefits of antibiotics are very less in
uncomplicated ailments.
A Cochrane Study of 8 RCTs (randomised controlled trials) – 6 double-blinded with 2287 kids in
all was used to compare antibiotics with place of for uncomplicated AOM in otherwise healthy
kids ("The journal of Family practice", 2017). This study reflected that kids who were cured by
use of antibiotics are less likely to suffer with pain in 24 hours beyond start of treatment, in
comparison to kids who were untreated. But 7% lesser kids who got antibiotics had been for 2 to
7 days then the untreated kids. So it could be seen that kids who were given antibiotics did not
see any key reduction in recurrence of AOM, rather there were issues of rice in the area, rashes
and nausea. The study also showed a moderate rise in failure rate of placebo cure for kids below
the age of two ears and for the kids with bilateral ailments. So there was a concluding thought
that the possible advantages and rest of antibiotics for AOM are very less.
Recommendations
It is suggested that studies have to be carried out which gave validation for shorter and clearance
of a fusion been useful for improving the speech development and also the validation of long run
treatment producing prolonged the remission of effusion. Due studies need to be done because
there are particular alternate surgical treatments available for Otitis medium.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Conclusion
Also studies showed that there has been concern over the antibiotic resistance. It is known that
antibiotics must not be started without the advice of any specialist (Masum & Fakir, 2011). The
article which has been shared also suggest that short course of antibiotics is useful for short-term
clearing of its usual. But since OME involves Eustachian tube dysfunction in all so therefore in
few cases the better-than-expected is present in the mid ear. Therefore it is recommended that
one must not expect that small course of antibiotics will be useful for providing long
lasting effects. For antibiotics to be the accepted treatment for OME there has to be some success
shown in fulfilling the objective of cure – restoring normal hearing for longer period so that
development takes place in a normal way.
References
Abou-halawa, A., Khan, M. and Alrobaee, A. (2012). Otomycosis with Perforated Tympanic
Membrane : Self Medication with Topical Antifungal Solution versus Medicated Ear Wick.
International Journal of Health Sciences, 6(1), pp.73-77.
Antibiotics not effective for children with infected eczema. (2016). Clinical Pharmacist.
Are Children Overprescribed Antibiotics?. (2008). American Journal of Nursing, 98(6), p.54.
Bhutta, Z. (2014). Antibiotics to promote growth in children?. BMJ, 348(apr15 15), pp.g2624-
g2624.
Brunk, D. (2011). Trials Give Nod to Antibiotics With Certain AOM. Family Practice News,
41(2), p.7.
Friedrich, M. (2011). Antibiotics for Otitis Media. JAMA, 305(7), p.663.
Also studies showed that there has been concern over the antibiotic resistance. It is known that
antibiotics must not be started without the advice of any specialist (Masum & Fakir, 2011). The
article which has been shared also suggest that short course of antibiotics is useful for short-term
clearing of its usual. But since OME involves Eustachian tube dysfunction in all so therefore in
few cases the better-than-expected is present in the mid ear. Therefore it is recommended that
one must not expect that small course of antibiotics will be useful for providing long
lasting effects. For antibiotics to be the accepted treatment for OME there has to be some success
shown in fulfilling the objective of cure – restoring normal hearing for longer period so that
development takes place in a normal way.
References
Abou-halawa, A., Khan, M. and Alrobaee, A. (2012). Otomycosis with Perforated Tympanic
Membrane : Self Medication with Topical Antifungal Solution versus Medicated Ear Wick.
International Journal of Health Sciences, 6(1), pp.73-77.
Antibiotics not effective for children with infected eczema. (2016). Clinical Pharmacist.
Are Children Overprescribed Antibiotics?. (2008). American Journal of Nursing, 98(6), p.54.
Bhutta, Z. (2014). Antibiotics to promote growth in children?. BMJ, 348(apr15 15), pp.g2624-
g2624.
Brunk, D. (2011). Trials Give Nod to Antibiotics With Certain AOM. Family Practice News,
41(2), p.7.
Friedrich, M. (2011). Antibiotics for Otitis Media. JAMA, 305(7), p.663.
Leach, A., Morris, P. and Mathews, J. (2008). Compared to placebo, long-term antibiotics
resolve otitis media with effusion (OME) and prevent acute otitis media with perforation
(AOMwiP) in a high-risk population: A randomized controlled trial. BMC Pediatrics, 8(1).
Macneil, J. (2006). Use Antibiotics in Toddlers With Bilateral AOM. Pediatric News, 40(7),
p.14.
Masum, S. and Fakir, M. (2011). Systemic Antibiotics Versus Topical Treatments for Chronic
Discharging Ears with Underlying Eardrum Perforations. Journal of Dhaka Medical College,
19(2).
Mdedge.com. (2017). The journal of Family practice. [online] Available at:
http://www.mdedge.com/jfponline/article/65210/pediatrics/should-you-use-antibiotics-treat-
acute-otitis-media-children [Accessed 20 Sep. 2017].
Milne, A. (2007). Summary of ‘Systemic antibiotics versus topical treatments for chronically
discharging ears with underlying eardrum perforations’. Evidence-Based Child Health: A
Cochrane Review Journal, 2(2), pp.691-692.
Office, A. (2015). Acknowledgement to Reviewers of Antibiotics in 2014. Antibiotics, 4(1),
pp.42-43.
Patient.info. (2017). Acute Otitis Media In Children. Ear infection information. Patient. [online]
Available at: https://patient.info/in/doctor/acute-otitis-media-in-children [Accessed 20 Sep.
2017].
Pichichero, M. (2015). Antibiotics for Acute Otitis Media. JAMA, 313(3), p.294.
resolve otitis media with effusion (OME) and prevent acute otitis media with perforation
(AOMwiP) in a high-risk population: A randomized controlled trial. BMC Pediatrics, 8(1).
Macneil, J. (2006). Use Antibiotics in Toddlers With Bilateral AOM. Pediatric News, 40(7),
p.14.
Masum, S. and Fakir, M. (2011). Systemic Antibiotics Versus Topical Treatments for Chronic
Discharging Ears with Underlying Eardrum Perforations. Journal of Dhaka Medical College,
19(2).
Mdedge.com. (2017). The journal of Family practice. [online] Available at:
http://www.mdedge.com/jfponline/article/65210/pediatrics/should-you-use-antibiotics-treat-
acute-otitis-media-children [Accessed 20 Sep. 2017].
Milne, A. (2007). Summary of ‘Systemic antibiotics versus topical treatments for chronically
discharging ears with underlying eardrum perforations’. Evidence-Based Child Health: A
Cochrane Review Journal, 2(2), pp.691-692.
Office, A. (2015). Acknowledgement to Reviewers of Antibiotics in 2014. Antibiotics, 4(1),
pp.42-43.
Patient.info. (2017). Acute Otitis Media In Children. Ear infection information. Patient. [online]
Available at: https://patient.info/in/doctor/acute-otitis-media-in-children [Accessed 20 Sep.
2017].
Pichichero, M. (2015). Antibiotics for Acute Otitis Media. JAMA, 313(3), p.294.

Rosdahl, C. and Kowalski, M. (2012). Textbook of basic nursing. Philadelphia: Wolters Kluwer
Health/Lippincott Williams & Wilkins.
Slovis, N. (2012). Equine otitis media-interna. Equine Veterinary Education, 24(6), pp.276-278.
Use of antibiotics in young children may disrupt gut microbiome. (2015). The Pharmaceutical
Journal.
Williams, R. (1993). Use of Antibiotics in Preventing Recurrent Acute Otitis Media and in
Treating Otitis Media With Effusion. JAMA, 270(11), p.1344.
Appendices
Health/Lippincott Williams & Wilkins.
Slovis, N. (2012). Equine otitis media-interna. Equine Veterinary Education, 24(6), pp.276-278.
Use of antibiotics in young children may disrupt gut microbiome. (2015). The Pharmaceutical
Journal.
Williams, R. (1993). Use of Antibiotics in Preventing Recurrent Acute Otitis Media and in
Treating Otitis Media With Effusion. JAMA, 270(11), p.1344.
Appendices
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

1 out of 15




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.