EBP Report: Antibiotic Therapy Effects on Necrotizing Enterocolitis
VerifiedAdded on 2023/04/11
|14
|1493
|282
Report
AI Summary
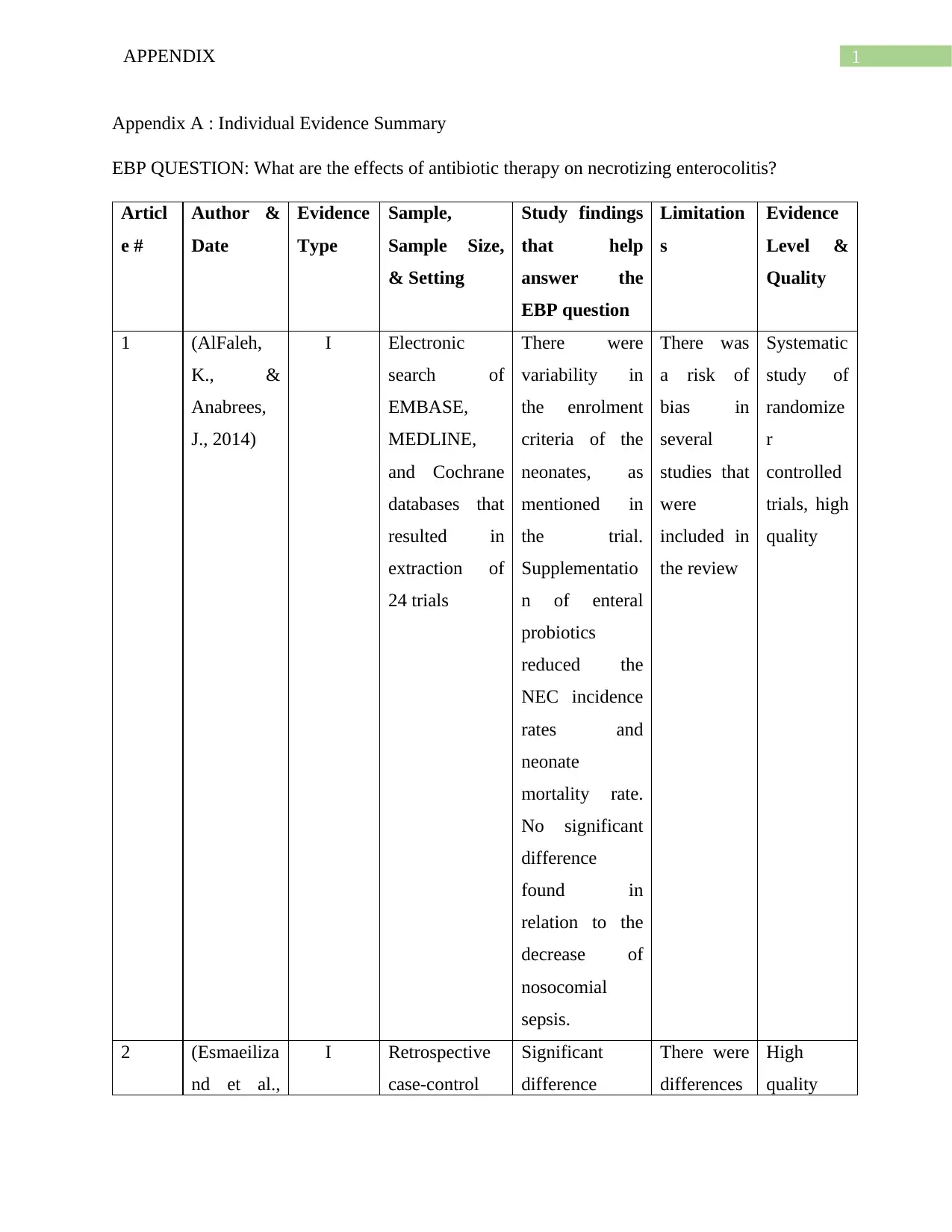
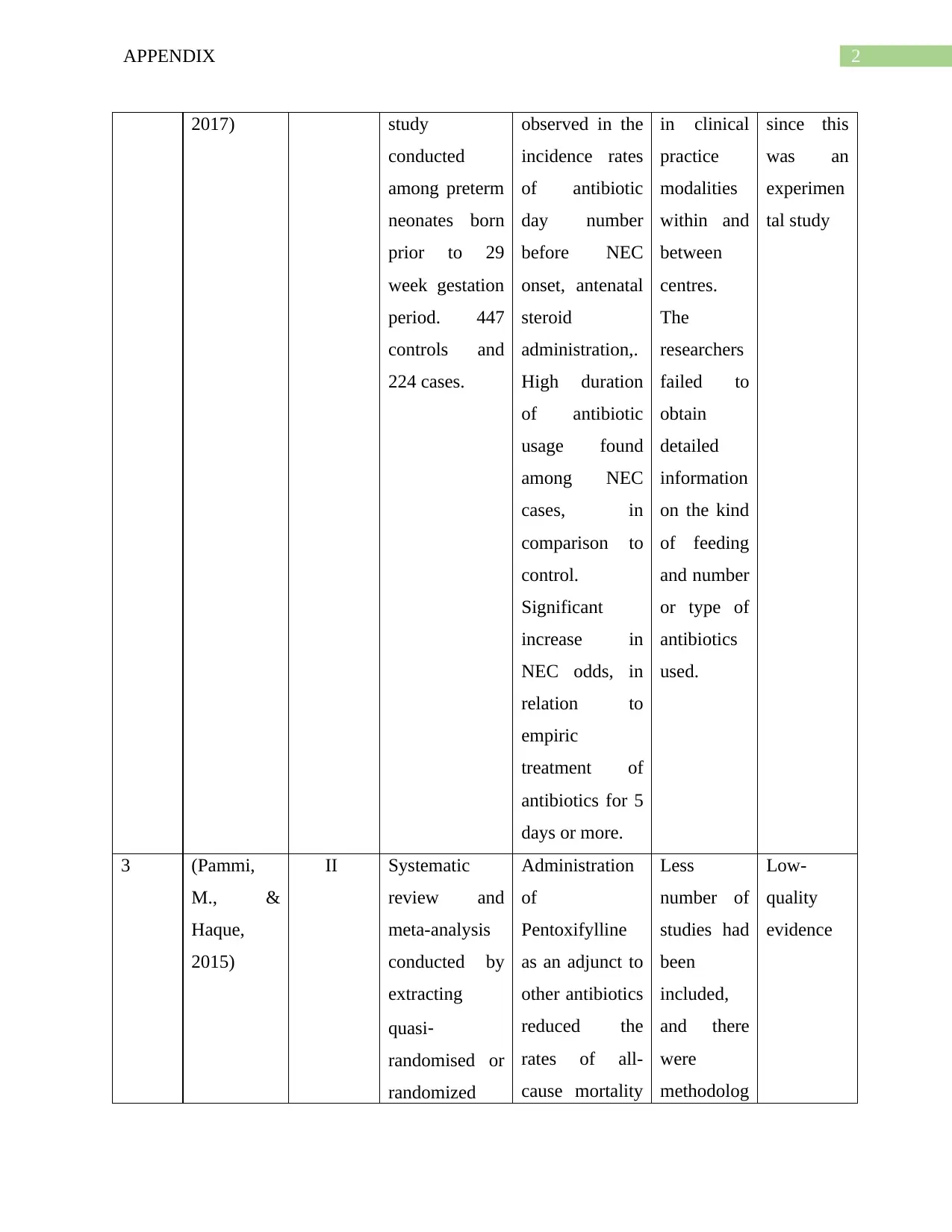
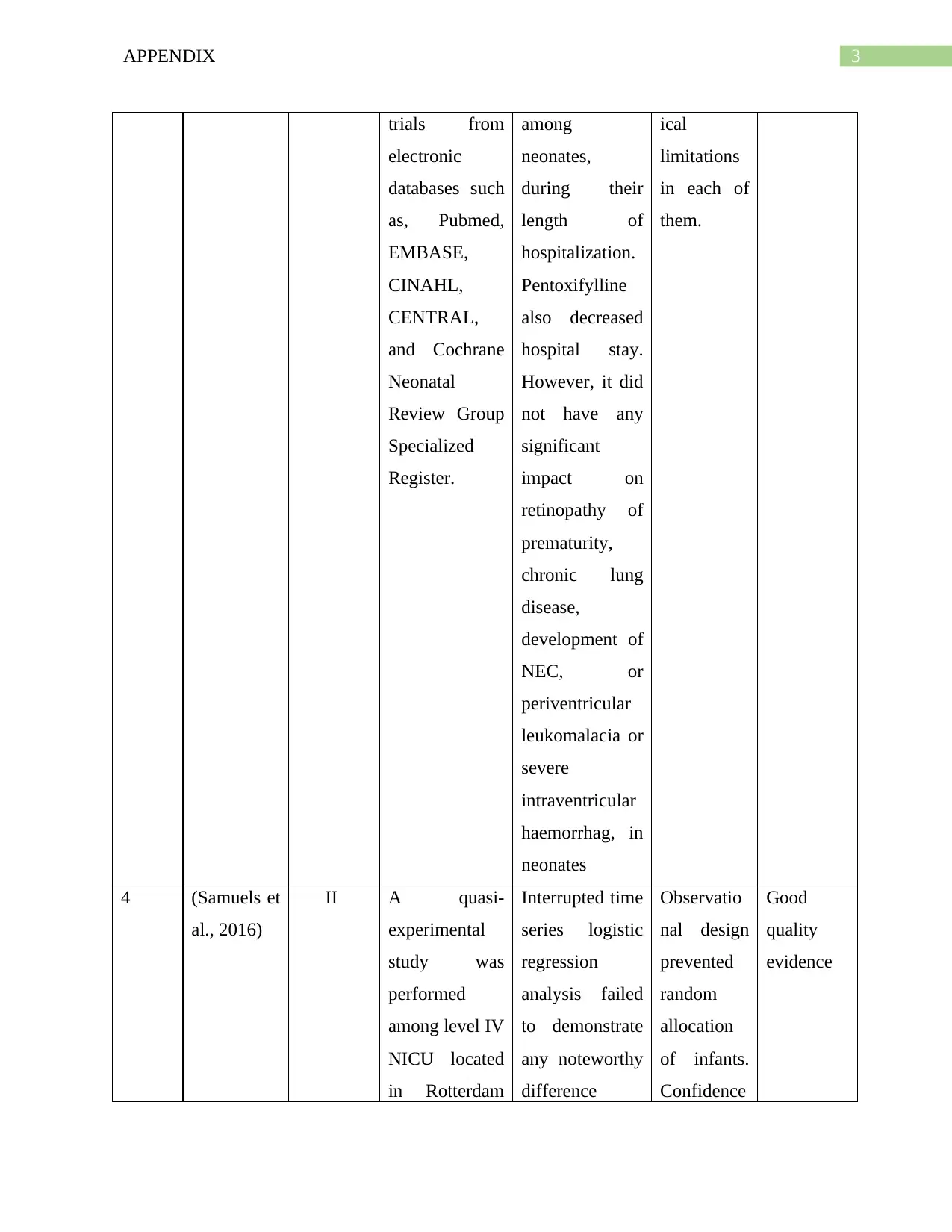
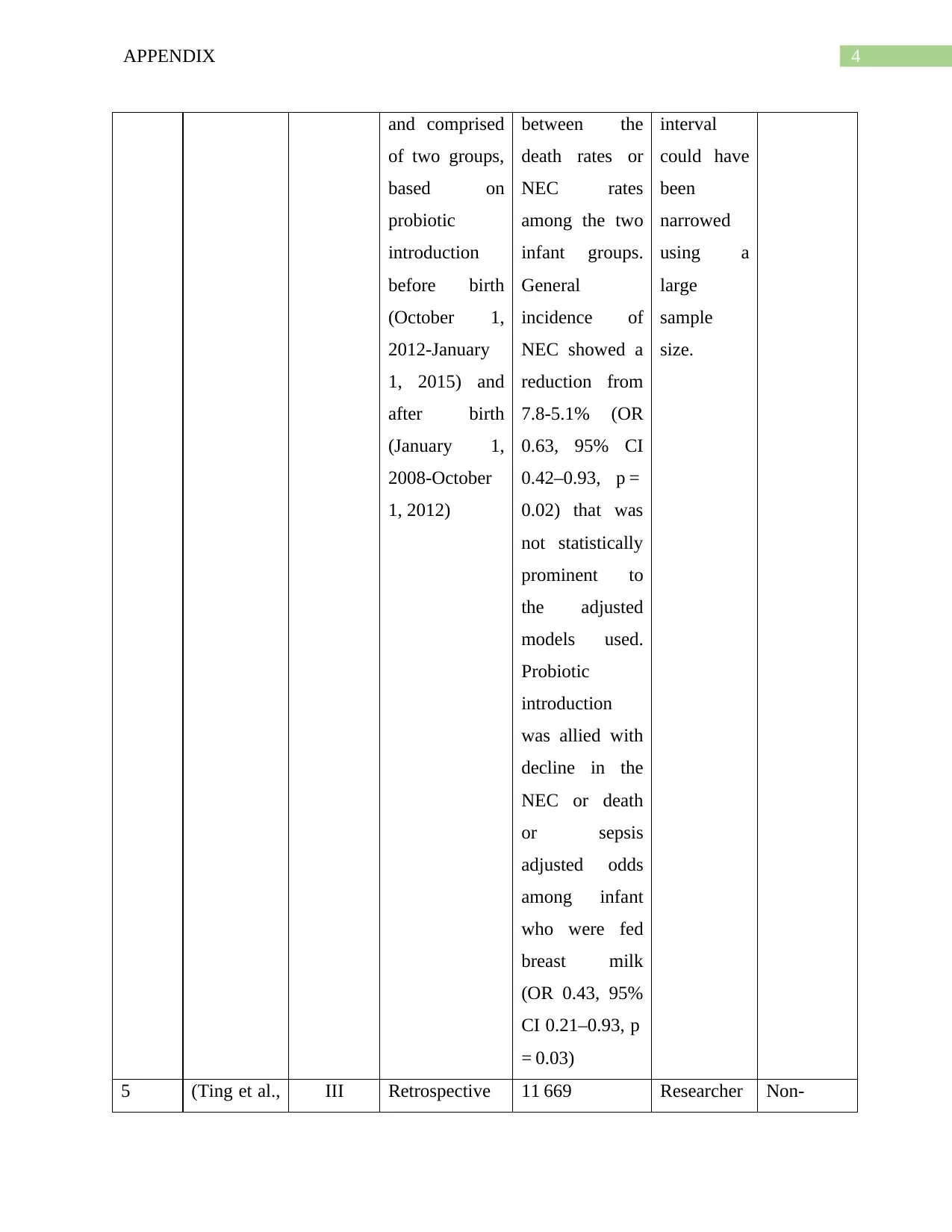
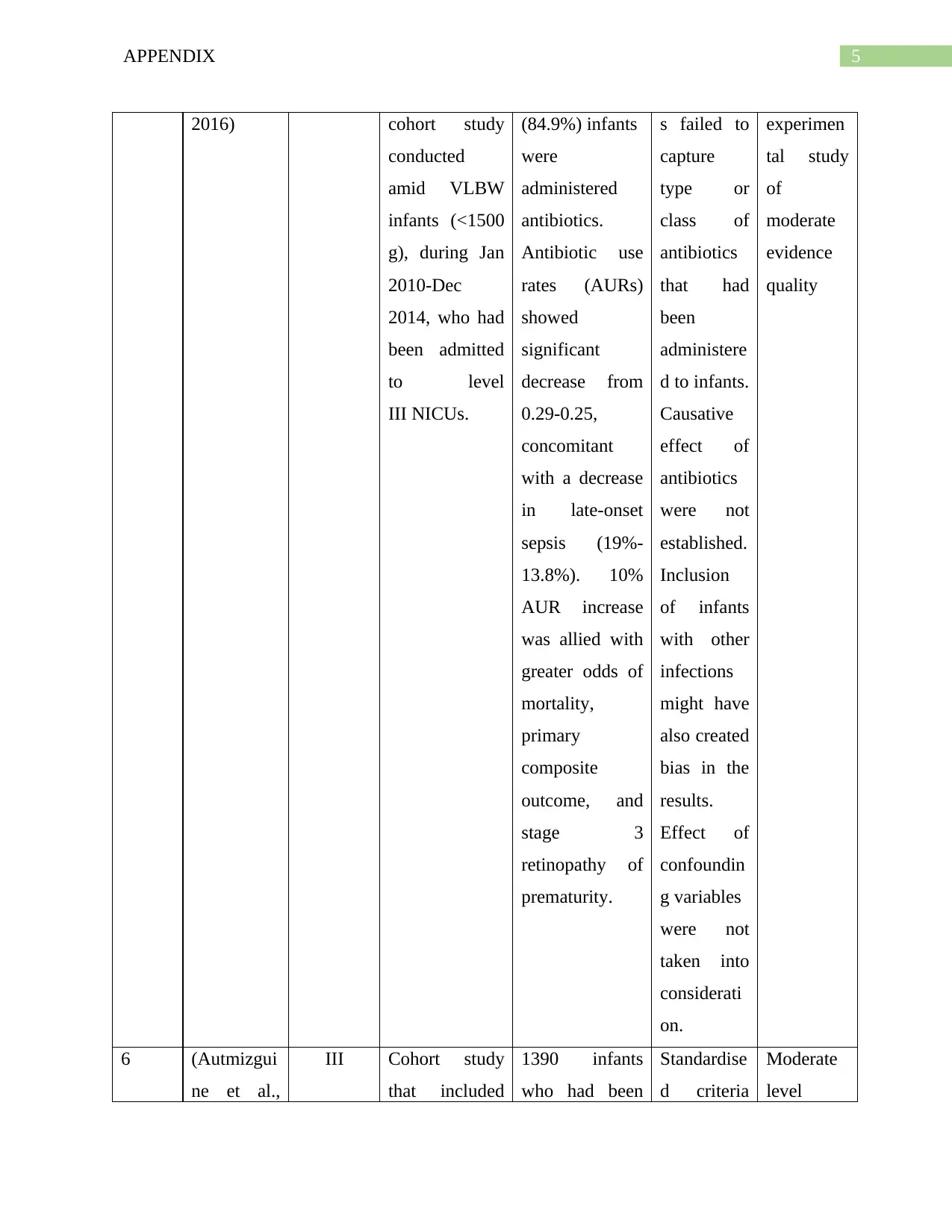
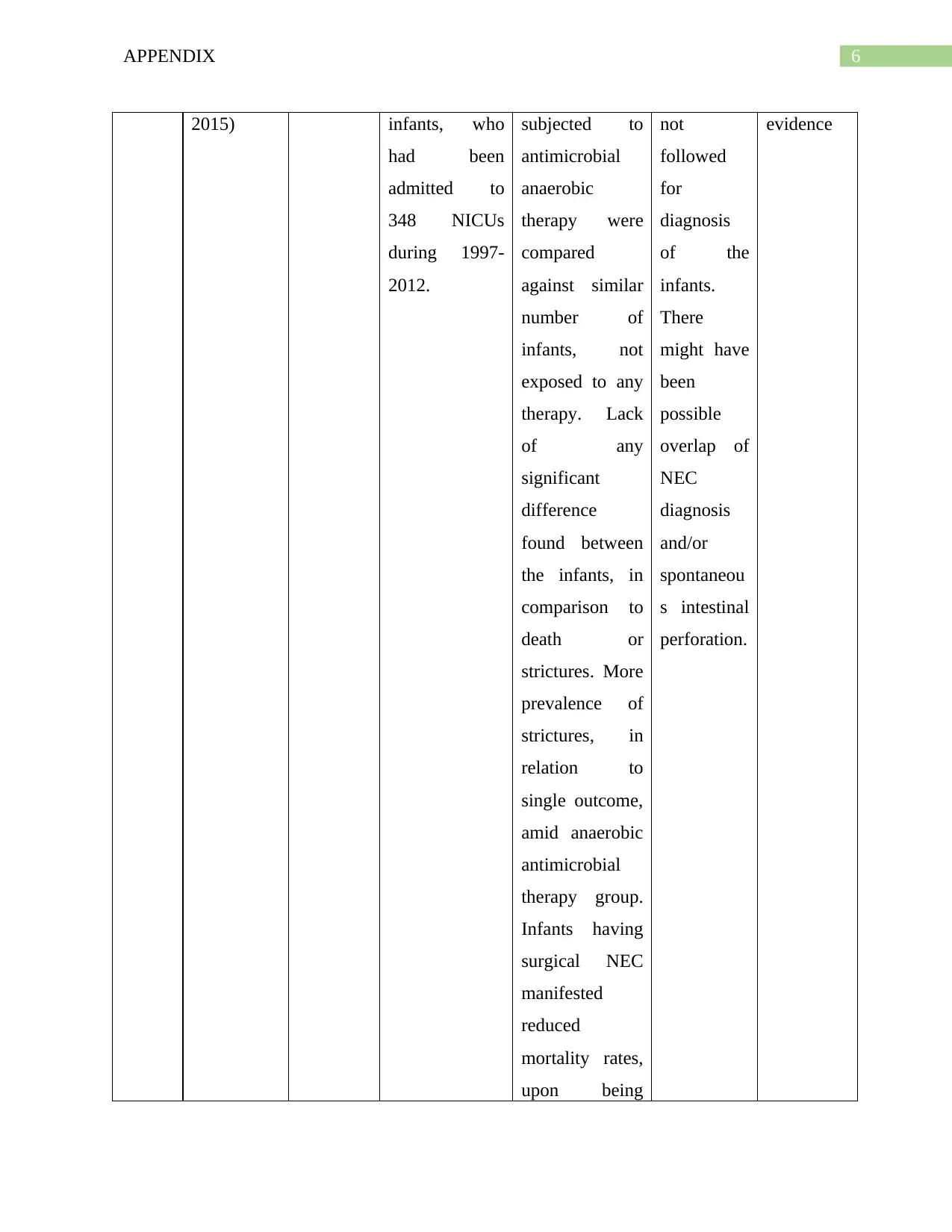
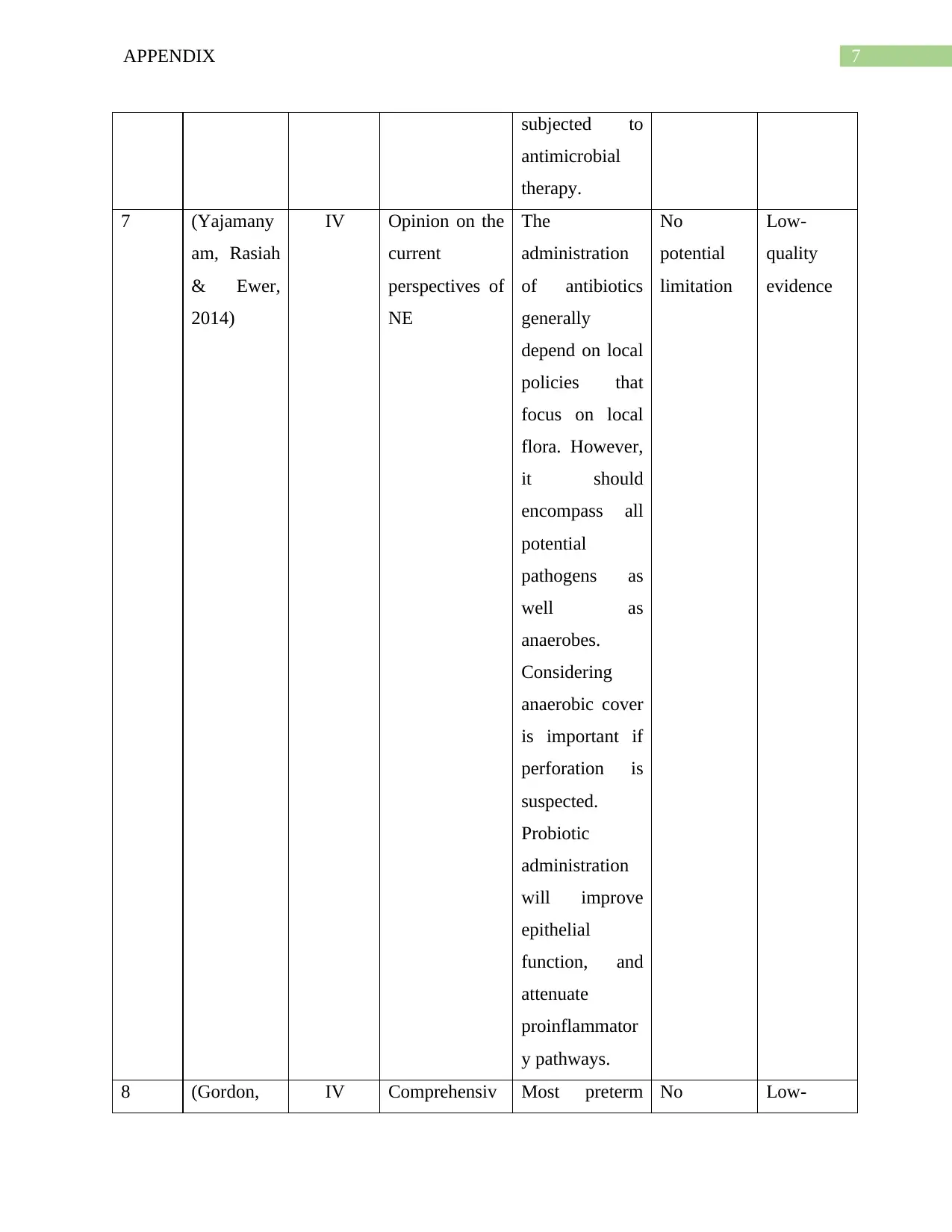
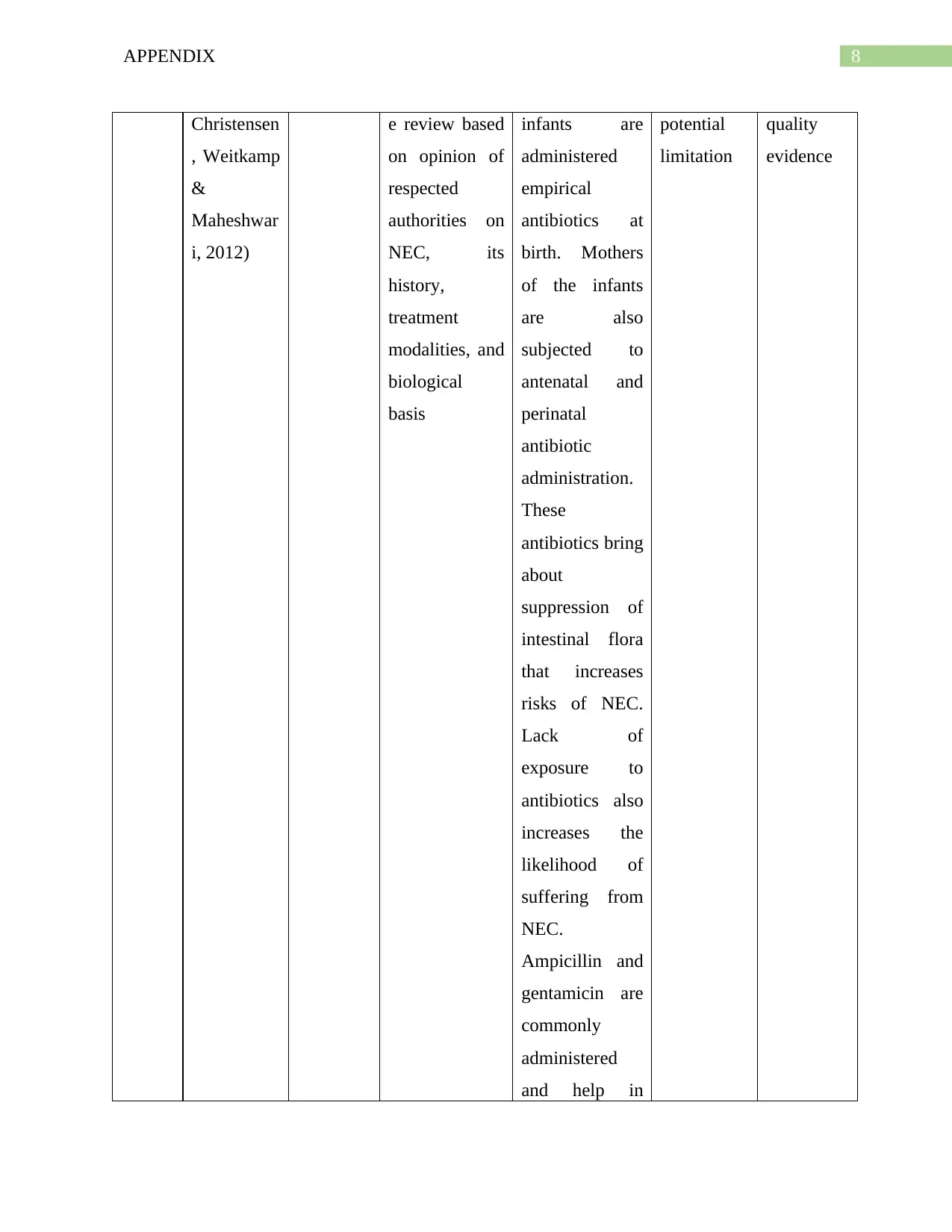
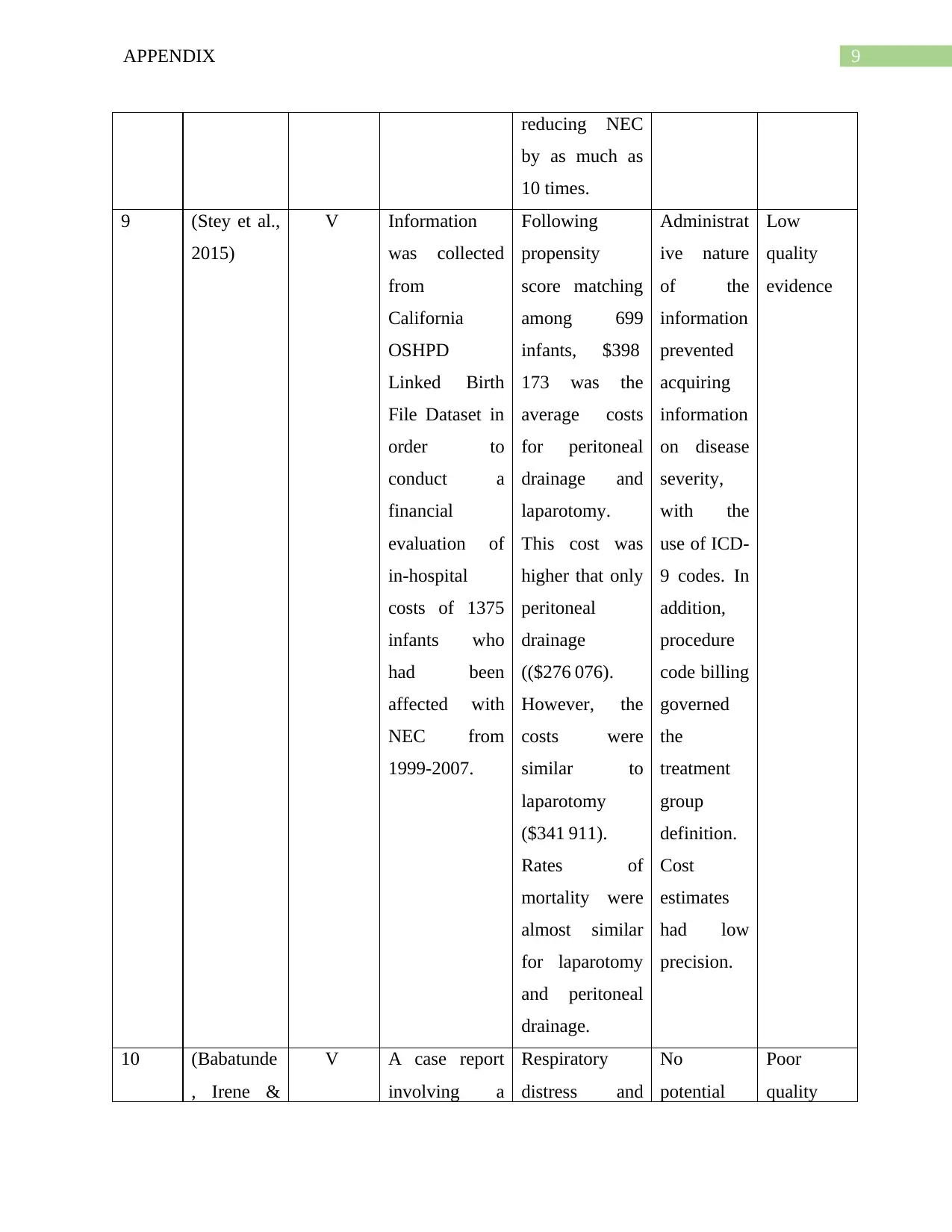
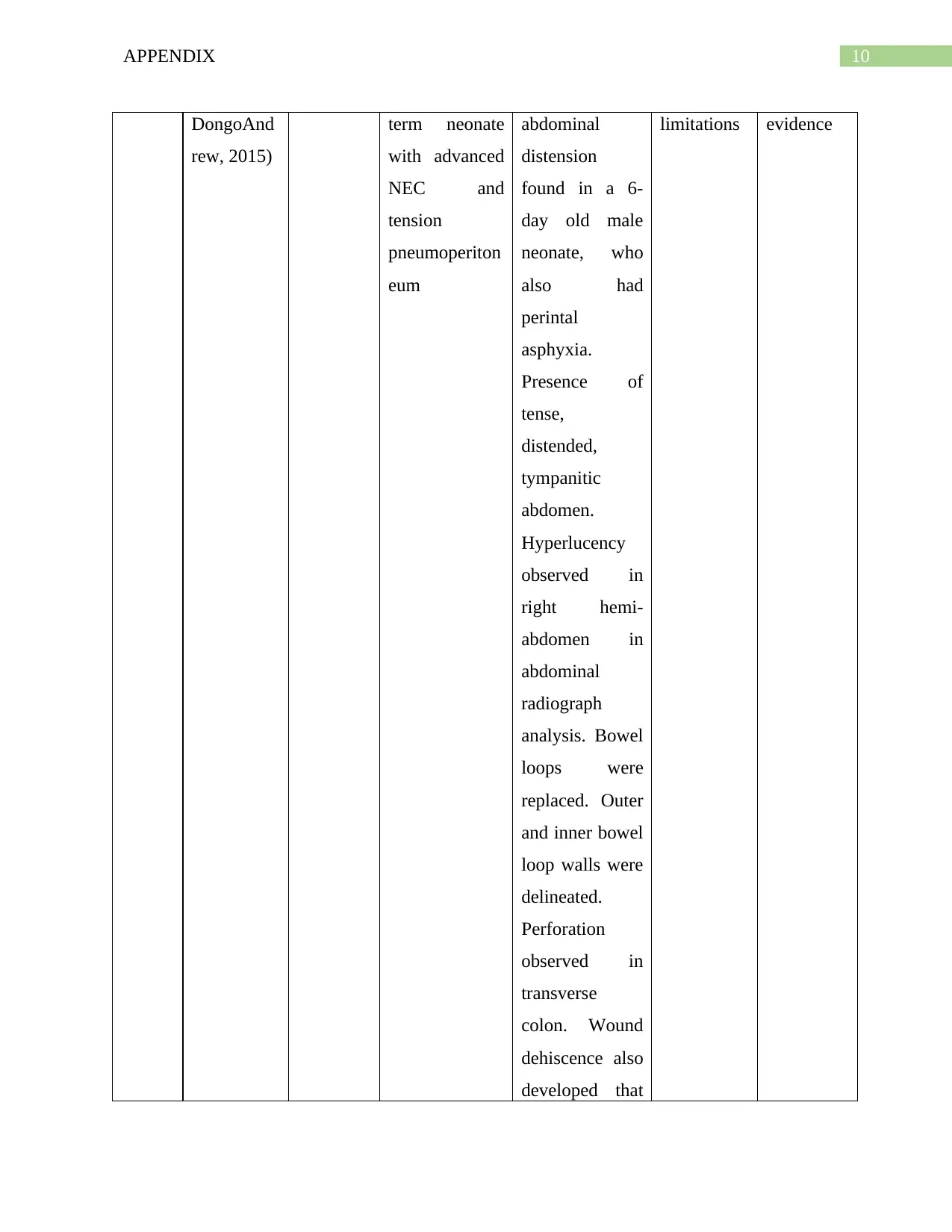
This report summarizes the evidence regarding the effects of antibiotic therapy on necrotizing enterocolitis (NEC) in neonates. It includes a table summarizing individual evidence from various studies, including systematic reviews, meta-analyses, retrospective cohort studies, and case reports. The studies examine the impact of antibiotic usage, the role of probiotics, and other interventions like pentoxifylline on NEC incidence, mortality, and associated complications. Limitations of the included studies, such as methodological issues, sample size limitations, and potential biases, are also discussed. The report also touches upon the current perspectives on antibiotic administration and the importance of considering anaerobic coverage. The report concludes by addressing the PICO question regarding the effectiveness of different parenteral antibiotics in preventing NEC progression and sequelae, emphasizing the importance of this issue due to the potential for severe outcomes like perforation, sepsis, and neonatal death if NEC is left untreated. Desklib provides access to similar solved assignments.

1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.