Article Analysis 1: Analysis of Research Articles on Bipolar Disorder
VerifiedAdded on 2022/10/14
|5
|1614
|326
Homework Assignment
AI Summary
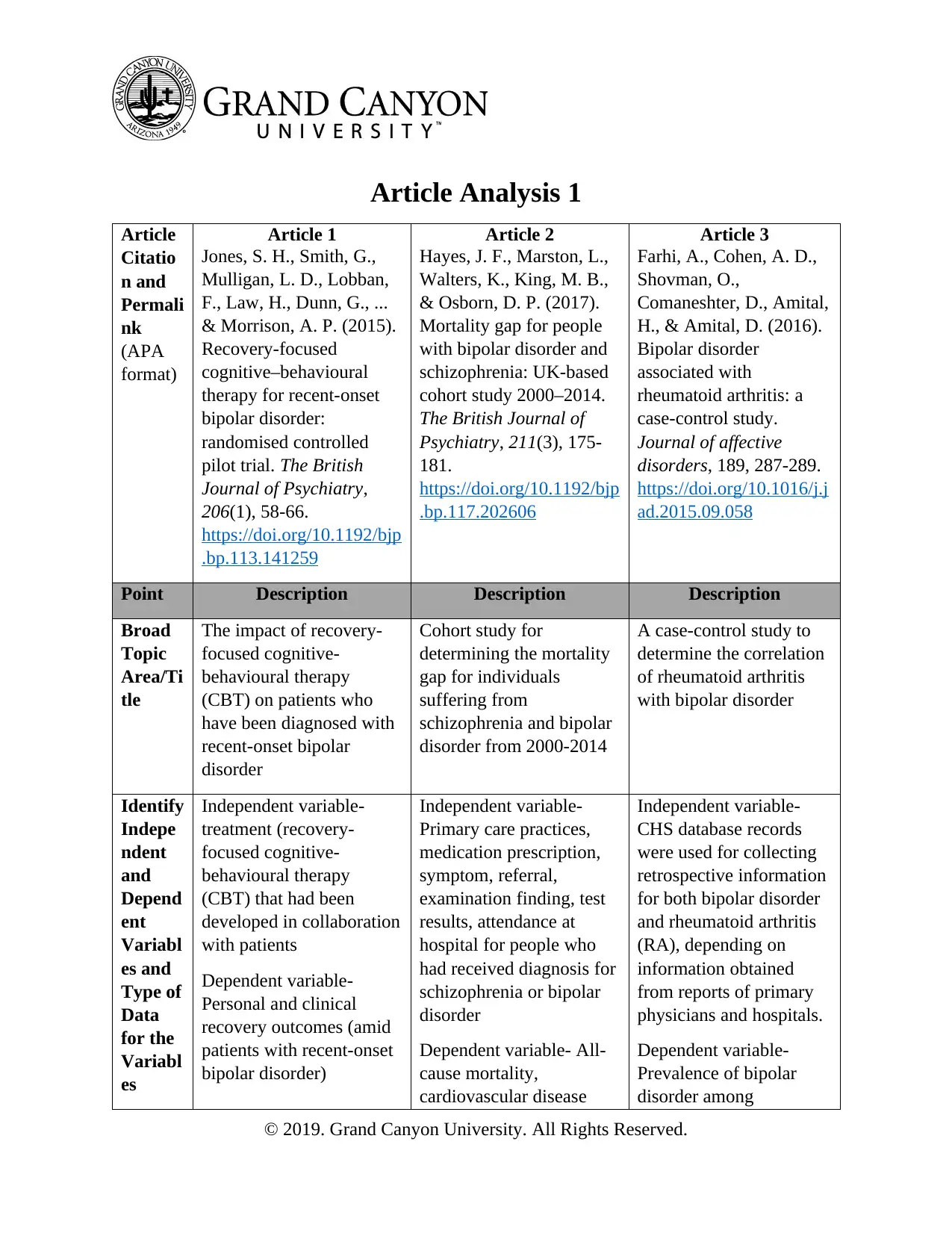
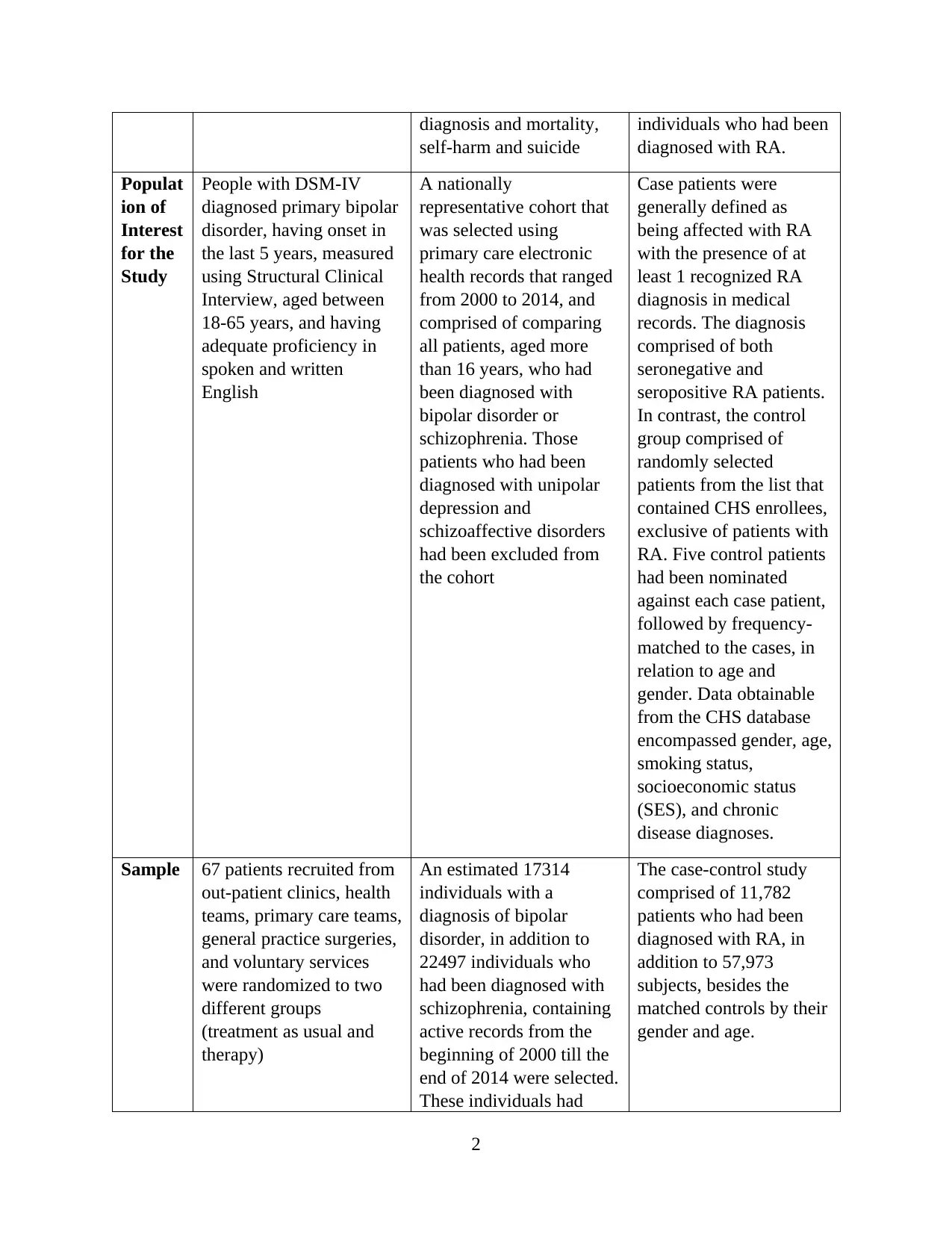
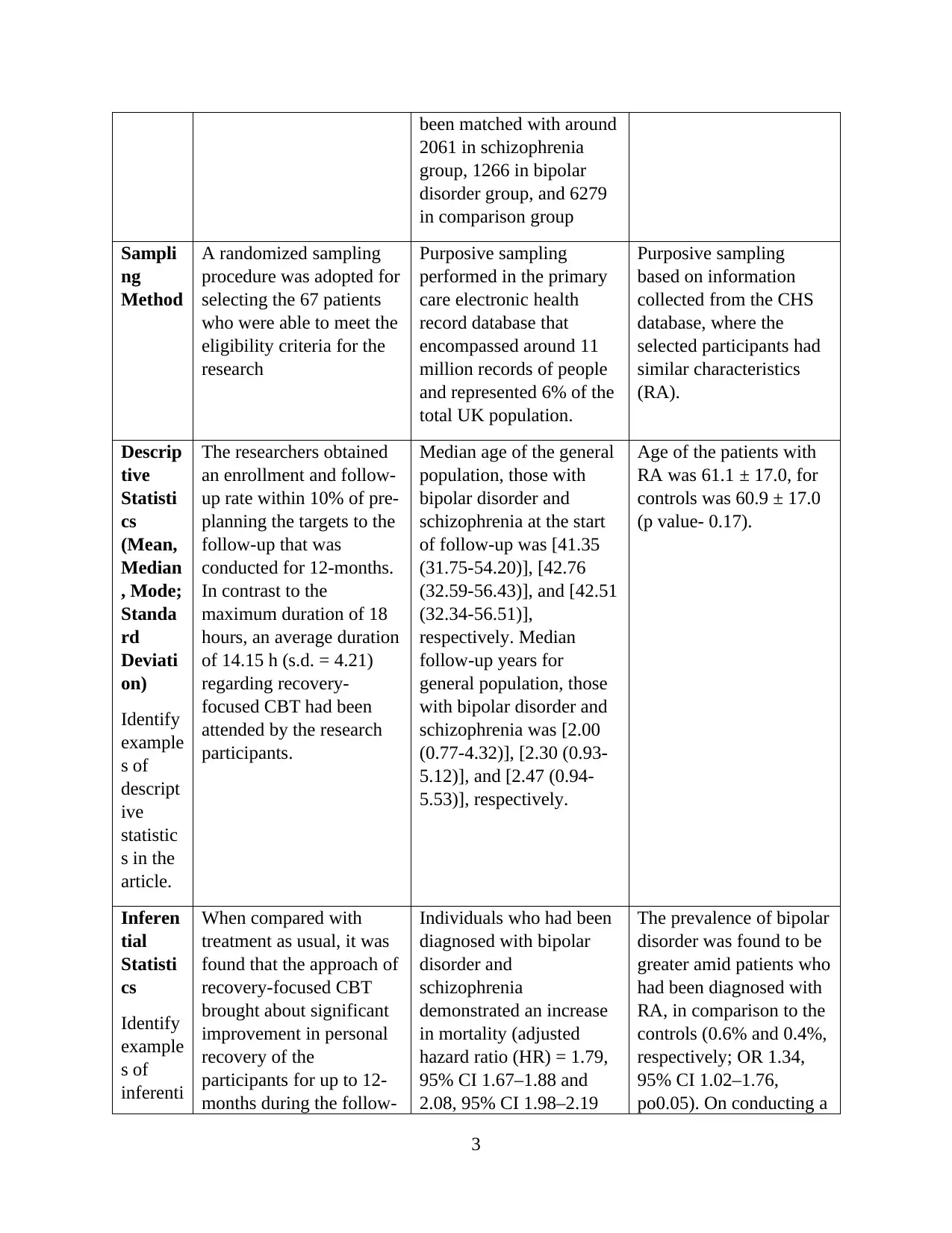
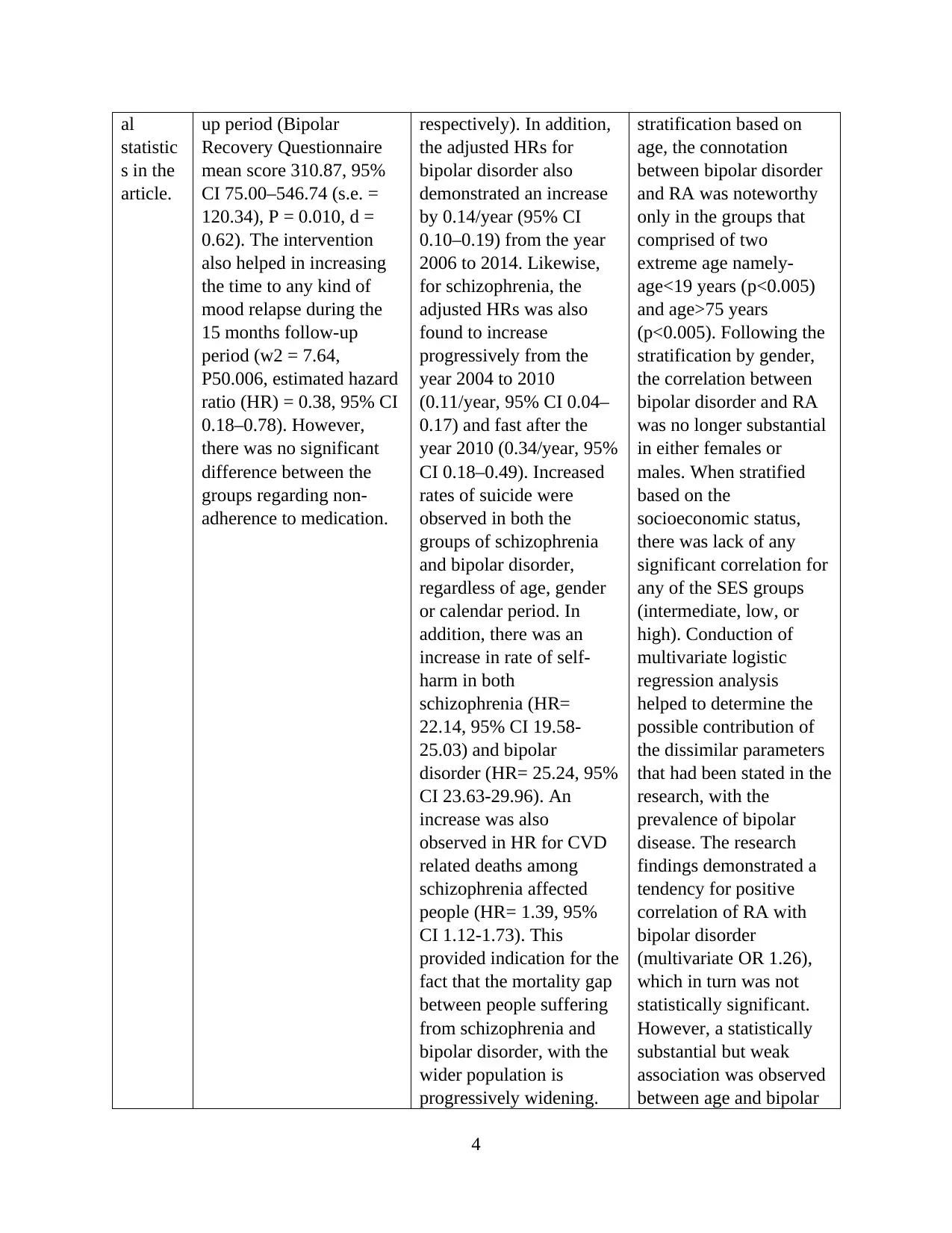
This assignment presents an analysis of three research articles related to bipolar disorder. The first article investigates the impact of recovery-focused cognitive-behavioral therapy (CBT) on patients with recent-onset bipolar disorder, examining independent and dependent variables, and employing a randomized sampling method with 67 patients. The second article is a cohort study determining the mortality gap for individuals with bipolar disorder and schizophrenia, utilizing a nationally representative cohort and analyzing data from primary care electronic health records. The third article is a case-control study exploring the correlation between bipolar disorder and rheumatoid arthritis (RA), using data from a CHS database. The assignment requires the identification of independent and dependent variables, the population of interest, sampling methods, and examples of both descriptive and inferential statistics from each article. The analysis reveals insights into treatment effectiveness, mortality risks, and potential associations between bipolar disorder and RA, as well as the application of various statistical methods in healthcare research.
1 out of 5
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.