Analysis of Nursing Leadership Styles in Healthcare Settings
VerifiedAdded on 2022/11/15
|10
|8542
|470
Report
AI Summary
This report analyzes the research article "The association of leadership styles and empowerment with nurses’ organizational commitment in an acute health care setting: a cross-sectional study" by Asiri et al. The study, conducted in Saudi Arabia, investigated the influence of leadership styles (transformational, transactional, and laissez-faire) and psychological empowerment on nurses' organizational commitment within acute care units. The research employed a cross-sectional survey, collecting data from 332 nurses using validated questionnaires, including the Multifactor Leadership Questionnaire (MLQ), the Psychological Empowerment Scale, and the Three-Component Model of Employee Commitment. The findings revealed that nurses generally perceived their managers as not fully exhibiting transformational leadership behaviors, and commitment was negatively correlated with this style. However, commitment showed a positive correlation with transactional leadership. The study also identified significant associations between commitment and nurse nationality, as well as predictors like laissez-faire leadership and autonomy. The analysis suggests that leadership styles and employee empowerment play a crucial role in fostering organizational commitment among nurses, particularly in the context of Saudi Arabian healthcare settings, highlighting the importance of effective leadership in addressing challenges such as staff shortages and maintaining quality care.
R E S E A R C H A R T I C L E Open Access
The association of leadership styles and
empowerment with nurses’organizational
commitment in an acute health care
setting:a cross-sectionalstudy
Samirah A.Asiri1
, Wesley W.Rohrer2
, Khaled Al-Surimi4*
, Omar O.Da’ar3 and Anwar Ahmed5
Abstract
Background:The current challenges facing healthcare systems,in relation to the shortage of health professionals,
necessitates mangers and leaders to learn from different leadership styles and staff empowerment strategso as
to create a work environment that encourages nursing staff commitment to patients and their organizationThis
study intends to measure the effects of nurses’overallperception of the leadership style of their managers,and
psychologicalempowerment on their organizationalcommitment in acute care units,in NationalGuard Health
Affairs,Riyadh City,SaudiArabia.
Methods:This was a cross-sectionalsurvey,where the data was obtained from nurses at King Abdulaziz Medical
City.Hard copy questionnaires were distributed to 350 randomly selected nurses.Three hundred and thirty two
(332) were completed,representing a response rate of 95 %.Three validated survey instruments were used to
obtain the data:(1) The Multifactor Leadership Questionnaire (MLQ),formulated by Bass and Avolio (1997),(2) The
PsychologicalEmpowerment Scale developed by Spreitzer (1995) and (3) The Three-Component Modelof
Employee Commitment developed by Meyer and Allen (1997).A theoreticalmodelthat conceptually links
leadership,empowerment,and organizationalcommitment was used.The SPSS program version 19 was employed
to perform descriptive and inferentialstatistics including correlation and stepwise multiple regression analysis.
Results:Overallmost nurses perceived their immediate nursing managers as not displaying the ideallevelof
transformationalleadership (TFL) behaviors.Nurses’commitment appeared to be negatively correlated with TFL
style and perceived psychologicalempowerment.However,commitment was positively correlated with the
TransactionalLeadership (TAL) style.Analysis,also,showed that commitment is significantly associated with the
nurse’s nationality by region:North American (P = 0.001) and Arab (p = 0.027).The other important predictors of
commitment include TAL (P = 0.027),Laissez-faire Leadership (LFL (P = 0.012),and autonomy (P = 0.016).The linear
combination of these predictors explained 20 % of the variability of the nurses’commitment.
Conclusion:The study findings suggest that leadership styles and employee empowerment could play an
instrumentalrole in promoting organizationalcommitment of nurses working in acute health care settings,at least
in the SaudiArabian context.
Keywords:Transformationalleadership,Transactionalleadership,Organizationalcommitment,Psychological
empowerment
* Correspondence:kalsurimi@gmail.com
4Department of Health System and Quality Management,College of Public
Health and Health Informatics;King Abdullah InternationalMedicalResearch
Center,King Saud bin Abdulaziz University for Health Sciences,Ministry of
NationalGuard Health Affairs,Riyadh,SaudiArabia
Fulllist of author information is available at the end of the article
© 2016 Asiriet al.Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0
InternationalLicense (http://creativecommons.org/licenses/by/4.0/),which permits unrestricted use,distribution,and
reproduction in any medium,provided you give appropriate credit to the originalauthor(s) and the source,provide a link to
the Creative Commons license,and indicate if changes were made.The Creative Commons Public Domain Dedication waiver
(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.
Asiri et al.BMC Nursing (2016) 15:38
DOI10.1186/s12912-016-0161-7
The association of leadership styles and
empowerment with nurses’organizational
commitment in an acute health care
setting:a cross-sectionalstudy
Samirah A.Asiri1
, Wesley W.Rohrer2
, Khaled Al-Surimi4*
, Omar O.Da’ar3 and Anwar Ahmed5
Abstract
Background:The current challenges facing healthcare systems,in relation to the shortage of health professionals,
necessitates mangers and leaders to learn from different leadership styles and staff empowerment strategso as
to create a work environment that encourages nursing staff commitment to patients and their organizationThis
study intends to measure the effects of nurses’overallperception of the leadership style of their managers,and
psychologicalempowerment on their organizationalcommitment in acute care units,in NationalGuard Health
Affairs,Riyadh City,SaudiArabia.
Methods:This was a cross-sectionalsurvey,where the data was obtained from nurses at King Abdulaziz Medical
City.Hard copy questionnaires were distributed to 350 randomly selected nurses.Three hundred and thirty two
(332) were completed,representing a response rate of 95 %.Three validated survey instruments were used to
obtain the data:(1) The Multifactor Leadership Questionnaire (MLQ),formulated by Bass and Avolio (1997),(2) The
PsychologicalEmpowerment Scale developed by Spreitzer (1995) and (3) The Three-Component Modelof
Employee Commitment developed by Meyer and Allen (1997).A theoreticalmodelthat conceptually links
leadership,empowerment,and organizationalcommitment was used.The SPSS program version 19 was employed
to perform descriptive and inferentialstatistics including correlation and stepwise multiple regression analysis.
Results:Overallmost nurses perceived their immediate nursing managers as not displaying the ideallevelof
transformationalleadership (TFL) behaviors.Nurses’commitment appeared to be negatively correlated with TFL
style and perceived psychologicalempowerment.However,commitment was positively correlated with the
TransactionalLeadership (TAL) style.Analysis,also,showed that commitment is significantly associated with the
nurse’s nationality by region:North American (P = 0.001) and Arab (p = 0.027).The other important predictors of
commitment include TAL (P = 0.027),Laissez-faire Leadership (LFL (P = 0.012),and autonomy (P = 0.016).The linear
combination of these predictors explained 20 % of the variability of the nurses’commitment.
Conclusion:The study findings suggest that leadership styles and employee empowerment could play an
instrumentalrole in promoting organizationalcommitment of nurses working in acute health care settings,at least
in the SaudiArabian context.
Keywords:Transformationalleadership,Transactionalleadership,Organizationalcommitment,Psychological
empowerment
* Correspondence:kalsurimi@gmail.com
4Department of Health System and Quality Management,College of Public
Health and Health Informatics;King Abdullah InternationalMedicalResearch
Center,King Saud bin Abdulaziz University for Health Sciences,Ministry of
NationalGuard Health Affairs,Riyadh,SaudiArabia
Fulllist of author information is available at the end of the article
© 2016 Asiriet al.Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0
InternationalLicense (http://creativecommons.org/licenses/by/4.0/),which permits unrestricted use,distribution,and
reproduction in any medium,provided you give appropriate credit to the originalauthor(s) and the source,provide a link to
the Creative Commons license,and indicate if changes were made.The Creative Commons Public Domain Dedication waiver
(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.
Asiri et al.BMC Nursing (2016) 15:38
DOI10.1186/s12912-016-0161-7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Background
Acute care environments in hospitals are in a state of
continuous improvementand rapid change due to the
pressuresof reduced average length ofhospitalstays
(ALOS), cost-containment,unpredictability,and uncer-
tainty.Moreover,the shortage of nursing staff within the
hospitalincreasesthe difficulty ofmaintaining accept-
able health care standards.Also, by replacing nursing
positions,such asthe nurse manager,which requires
strong leadership and at least minimalmanagement ex-
perienceand training,with less-qualified health care
personnelhas led to a devalued nursing role within or-
ganizations[1]. Nursesmightperceive thatmanagers,
both with autocratic and weak leadership styles,present
barriers to effective nursing practice.Overly controlling
managersare likely to discourage individualinitiative
and creative thinking.Weak nurse managers,meanwhile,
may failto advocate for nurses’employment rights,the
respect they deserve within the health care team,to sup-
port their need for resources,and may failto effectively
negotiate and retain nursing positions.Thus,failed lead-
ership due to the absence ofqualified nurse managers
results in the nursing staffbecoming further disempow-
ered,demotivated and ultimately disengaged,less satis-
fied and committed [2].
Nursing managershave an essentialrole in hospital
management.This includes facilitating care,ensuring pa-
tient safety,enhancing the quality of work life of nurses,
and championing change processes that serve these ends
[3,4].This requires managers to empower their nurses
to perform their obligations using best practices.It, also,
requires managers to ensure the staffing nurses’ commit-
mentby means ofproviding an optimalwork environ-
ment whilst maintaining a high levelof quality care and
patient safety.Nurse empowerment is not only an essen-
tialrequirement,but it also affects work performance to
achieve these outcomes.In this context,Kanter (1993)
states thatWork Empowerment Theory is conceptually
consistentwith the nursing care processand can be
logically extended to supportnurses’interactions with
their patients,as empowered nurses will enable best care
practices for their patients,hence,resulting in optimal
patient care outcomes [5].However,it has been reported
thatthe relations between nurse managers and staffing
nurses have grown more strained,leading to less oppor-
tunity for nurses to communicate their concerns about
patient care and their own roles with their managers [6].
Previousstudies showed nursesperceive thatthey are
underrepresented in the organizationalhierarchy [4–6];
thus limiting their capacity to have meaningfulrole in
decision makingand influencingchangeto improve
organizationalprocesses that are relevant to the nurse’s
role,quality ofwork life and patientcare.Correspond-
ingly,these conditions affect not only the staffing nurses’
emotionaland physicalhealth outcomes,but also their
efficiency,productivity,performance and commitment.
Failing to providenurseswith a significantvoicein
health care system management,eventually leads to ad-
verse effects in the workplaceenvironmentand
organizationalculture and functioning,and this ultim-
ately results in lower-quality patient care [7].
The available literature provides considerable evidence
that nurses’limited participation in clinicaldecision-
makingis ineffectiveand harmfulto patientsafety.
There is evidence that nurses may also be overextending
themselves to ensure the quality of care under deterior-
ating working conditions [5].It has also been reported
thatlimited participation ofnurses in decision-making,
affecting their jobs and work environment,entails a cost
to the organization in terms of mistrust of hospital man-
agementand resentment[6];high levels ofstress,de-
creasedmorale,reducedjob satisfactionand lower
organizationalcommitment [2,5, 6, 8, 9].These condi-
tions collectivelywould, likely,contributeto nursing
burnoutand nurses leaving the organization and even
the profession.
Thus,as a priority,the role ofthe nurse manager,in
continually and effectively empowering staffin the care
process,is to ensure a work environmentand culture
thatencourages and sustains quality ofhealthcare and
patient safety.However,the relationship between leader-
ship style and behavior and employee commitment and
empowermenthas notbeen investigated in SaudiAra-
bian health care context.Furthermore,the work em-
powermentconstructitself has not been previously
tested within theSaudiArabian context.Hence,this
study aims primarily to test a model that links leadership
style and employee empowerment,and their impact on
organizational commitment among nurses working in an
acute healthcare setting in Riyadh,Saudi Arabia.
Methods
Study design,setting,and sampling
This study uses a cross-sectional survey investigating the
relationshipsamong leadership style,psychologicalem-
powerment,and organizationalcommitment.The study
was conducted at King Abdulaziz MedicalCity,Ministry
of NationalGuard Health Affairs,in Riyad,SaudiArabia
(KAMC-R). KAMC-R was established in May 1983 to pro-
vide medical,surgical,obstetrician,and criticalcare ser-
vices to NationalGuard employees and their dependents.
The services expanded over the following years to include
more than 1800 beds with specialized services like oncol-
ogy and transplant in addition to the original services.
Three hundred and fifty(350)questionnaireswere
randomly distributed to full time registered nursing staff
in the acute care units at KAMC-R.Of these 332 valid
Asiri et al.BMC Nursing (2016) 15:38 Page 2 of 10
Acute care environments in hospitals are in a state of
continuous improvementand rapid change due to the
pressuresof reduced average length ofhospitalstays
(ALOS), cost-containment,unpredictability,and uncer-
tainty.Moreover,the shortage of nursing staff within the
hospitalincreasesthe difficulty ofmaintaining accept-
able health care standards.Also, by replacing nursing
positions,such asthe nurse manager,which requires
strong leadership and at least minimalmanagement ex-
perienceand training,with less-qualified health care
personnelhas led to a devalued nursing role within or-
ganizations[1]. Nursesmightperceive thatmanagers,
both with autocratic and weak leadership styles,present
barriers to effective nursing practice.Overly controlling
managersare likely to discourage individualinitiative
and creative thinking.Weak nurse managers,meanwhile,
may failto advocate for nurses’employment rights,the
respect they deserve within the health care team,to sup-
port their need for resources,and may failto effectively
negotiate and retain nursing positions.Thus,failed lead-
ership due to the absence ofqualified nurse managers
results in the nursing staffbecoming further disempow-
ered,demotivated and ultimately disengaged,less satis-
fied and committed [2].
Nursing managershave an essentialrole in hospital
management.This includes facilitating care,ensuring pa-
tient safety,enhancing the quality of work life of nurses,
and championing change processes that serve these ends
[3,4].This requires managers to empower their nurses
to perform their obligations using best practices.It, also,
requires managers to ensure the staffing nurses’ commit-
mentby means ofproviding an optimalwork environ-
ment whilst maintaining a high levelof quality care and
patient safety.Nurse empowerment is not only an essen-
tialrequirement,but it also affects work performance to
achieve these outcomes.In this context,Kanter (1993)
states thatWork Empowerment Theory is conceptually
consistentwith the nursing care processand can be
logically extended to supportnurses’interactions with
their patients,as empowered nurses will enable best care
practices for their patients,hence,resulting in optimal
patient care outcomes [5].However,it has been reported
thatthe relations between nurse managers and staffing
nurses have grown more strained,leading to less oppor-
tunity for nurses to communicate their concerns about
patient care and their own roles with their managers [6].
Previousstudies showed nursesperceive thatthey are
underrepresented in the organizationalhierarchy [4–6];
thus limiting their capacity to have meaningfulrole in
decision makingand influencingchangeto improve
organizationalprocesses that are relevant to the nurse’s
role,quality ofwork life and patientcare.Correspond-
ingly,these conditions affect not only the staffing nurses’
emotionaland physicalhealth outcomes,but also their
efficiency,productivity,performance and commitment.
Failing to providenurseswith a significantvoicein
health care system management,eventually leads to ad-
verse effects in the workplaceenvironmentand
organizationalculture and functioning,and this ultim-
ately results in lower-quality patient care [7].
The available literature provides considerable evidence
that nurses’limited participation in clinicaldecision-
makingis ineffectiveand harmfulto patientsafety.
There is evidence that nurses may also be overextending
themselves to ensure the quality of care under deterior-
ating working conditions [5].It has also been reported
thatlimited participation ofnurses in decision-making,
affecting their jobs and work environment,entails a cost
to the organization in terms of mistrust of hospital man-
agementand resentment[6];high levels ofstress,de-
creasedmorale,reducedjob satisfactionand lower
organizationalcommitment [2,5, 6, 8, 9].These condi-
tions collectivelywould, likely,contributeto nursing
burnoutand nurses leaving the organization and even
the profession.
Thus,as a priority,the role ofthe nurse manager,in
continually and effectively empowering staffin the care
process,is to ensure a work environmentand culture
thatencourages and sustains quality ofhealthcare and
patient safety.However,the relationship between leader-
ship style and behavior and employee commitment and
empowermenthas notbeen investigated in SaudiAra-
bian health care context.Furthermore,the work em-
powermentconstructitself has not been previously
tested within theSaudiArabian context.Hence,this
study aims primarily to test a model that links leadership
style and employee empowerment,and their impact on
organizational commitment among nurses working in an
acute healthcare setting in Riyadh,Saudi Arabia.
Methods
Study design,setting,and sampling
This study uses a cross-sectional survey investigating the
relationshipsamong leadership style,psychologicalem-
powerment,and organizationalcommitment.The study
was conducted at King Abdulaziz MedicalCity,Ministry
of NationalGuard Health Affairs,in Riyad,SaudiArabia
(KAMC-R). KAMC-R was established in May 1983 to pro-
vide medical,surgical,obstetrician,and criticalcare ser-
vices to NationalGuard employees and their dependents.
The services expanded over the following years to include
more than 1800 beds with specialized services like oncol-
ogy and transplant in addition to the original services.
Three hundred and fifty(350)questionnaireswere
randomly distributed to full time registered nursing staff
in the acute care units at KAMC-R.Of these 332 valid
Asiri et al.BMC Nursing (2016) 15:38 Page 2 of 10
questionnaireswerecompleted and returned fordata
analysis,representing a 95 % response rate.
Instruments and reliability
Three recognized and validated questionnaires to obtain
the data that were used are:the 1997 Multifactor Leader-
ship Questionnaire (MLQ) developed by Bass and Avolio
[10],the 1995 PsychologicalEmpowermentScale devel-
oped by Spreitzer [11],and the 1997.Three-Component
Model of employee commitment developed by Meyer and
Allen [12].The three instruments address the nurses’per-
ception ofworkplace PsychologicalEmpowerment(PE),
Leadership Styles (LS),and levels oftheir Organizational
Commitment (OC).
The reliability ofthe three instrumentswas investi-
gated in a random sampleof 80 nurses.Internal
consistency was checked for the 44 items of the LS scale,
12 itemsof PE scale,and 18 itemsof the OC scale.
Cronbach’salpha measurescalculated were 0.94,0.94,
and 0.79,respectively.Acute care nurses were asked to
rate theirperceptionsof their immediate supervisors’
leadership style,and their own levelof commitmentto
the organization.In addition,demographic profiles in-
cluding characteristicssuch asgender,age,nationality
education level,yearsof experiencein nursing, and
number of years in current position were sought.
Statistical analyses
Data from the completed and returned surveyswere
compiled and analyzed using the SPSS statisticalsoft-
ware package (SPSS forWindows,version 19.0,SPSS,
Chicago,IL, USA).First,key variables from the concep-
tual framework were descriptively summarized.Counts
and percentageswere used to summarize categorical
variables(Table 1). Mean and standarddeviation
(Mean ± SD) were used to summarize continuous vari-
ables (Tables 2,3, 4 and 5).Then,inferentialstatistics
such as Pearson Correlation and Stepwise regression
were performed to makeinferencesfrom the study
sample to the broaderpopulation.ANOVA and post
hoc analysis were conducted to examine differences in
nurses’ commitment across various nationalities (Table 4
& Fig.1).Pearson Correlation coefficients were calculated
to measure the direction and strength ofthe linear rela-
tionship between nurses’commitmentacross leadership
and empowermentperception subtypes (Table 6).Step-
wise linear regression analysis was employed to identify
the main predictors of nurses’ commitment (Table 7).The
following predictorswere entered into the model:age,
gender,nationality (African,Arab,Philippines,American),
leadership styles (TFL,TAL, LFL), empowerment (mean-
ing, confidence, autonomy, impact), and additional qualifi-
cation degree other than nursing.
Results
Respondents’characteristics
The characteristics ofthe sampled nurses are summa-
rized in the Table 1.A totalof 332 completed question-
naireswere analyzed.The demographic data revealed
that 305 (92.1 %) of the sample were females.Of the re-
spondents,120 (43.6 %) had a degree in fields other than
nursing.The average age ofnurses in the AdultAcute
Care Unitwas 35 (±SD 7.94 years),while the average
age in the PediatricsAcute Care Unit was 37 (±SD
8.14 years).A considerable majority 217 (68.2 %) of sur-
veyed nurseswere from the Philippines.Demographic
variables of the participating RNs were further examined
according to their areas ofpractice.Of the 332 nurses
surveyed,229 (69 %) were in Pediatrics Acute Care Unit
and 103 (31 %) in Adult Acute Care Unit.
Psychological empowerment
Based on the psychologicalempowermentscores mea-
sured on a 6-pointLikert scale by the Empowerment
questionnaire,83.2 % ofthe nursesin this study per-
ceived themselvesto be at the moderatelevel
Table 1 Demographic characteristics of study respondents
Variable N %
Gender Male 26 7.9
Female 305 92.1
Position Staff nurse 302 92
Nurse manager 9 2.7
Others 19 5.8
Education Diploma/Associate degree 79 25.4
Baccalaureate degree 225 72.3
Master degree 7 2.3
Other Degree Yes 120 43.6
No 155 56.4
Nationality African 14 4.4
Arab 31 9.7
Asian 45 14.2
Filipinos 217 68.2
North American 11 3.5
Table 2 Employees’empowerment scale and subscales (scores
lowest = 0 to highest = 6)
Variables Mean score SD
Overallscore of empowerment 4.70 .90
Subscales scores of empowerment
- Meaning 5.16 .95
- Confidence 4.92 .97
- Autonomy 4.48 1.13
- Impact 4.21 1.13
Asiri et al.BMC Nursing (2016) 15:38 Page 3 of 10
analysis,representing a 95 % response rate.
Instruments and reliability
Three recognized and validated questionnaires to obtain
the data that were used are:the 1997 Multifactor Leader-
ship Questionnaire (MLQ) developed by Bass and Avolio
[10],the 1995 PsychologicalEmpowermentScale devel-
oped by Spreitzer [11],and the 1997.Three-Component
Model of employee commitment developed by Meyer and
Allen [12].The three instruments address the nurses’per-
ception ofworkplace PsychologicalEmpowerment(PE),
Leadership Styles (LS),and levels oftheir Organizational
Commitment (OC).
The reliability ofthe three instrumentswas investi-
gated in a random sampleof 80 nurses.Internal
consistency was checked for the 44 items of the LS scale,
12 itemsof PE scale,and 18 itemsof the OC scale.
Cronbach’salpha measurescalculated were 0.94,0.94,
and 0.79,respectively.Acute care nurses were asked to
rate theirperceptionsof their immediate supervisors’
leadership style,and their own levelof commitmentto
the organization.In addition,demographic profiles in-
cluding characteristicssuch asgender,age,nationality
education level,yearsof experiencein nursing, and
number of years in current position were sought.
Statistical analyses
Data from the completed and returned surveyswere
compiled and analyzed using the SPSS statisticalsoft-
ware package (SPSS forWindows,version 19.0,SPSS,
Chicago,IL, USA).First,key variables from the concep-
tual framework were descriptively summarized.Counts
and percentageswere used to summarize categorical
variables(Table 1). Mean and standarddeviation
(Mean ± SD) were used to summarize continuous vari-
ables (Tables 2,3, 4 and 5).Then,inferentialstatistics
such as Pearson Correlation and Stepwise regression
were performed to makeinferencesfrom the study
sample to the broaderpopulation.ANOVA and post
hoc analysis were conducted to examine differences in
nurses’ commitment across various nationalities (Table 4
& Fig.1).Pearson Correlation coefficients were calculated
to measure the direction and strength ofthe linear rela-
tionship between nurses’commitmentacross leadership
and empowermentperception subtypes (Table 6).Step-
wise linear regression analysis was employed to identify
the main predictors of nurses’ commitment (Table 7).The
following predictorswere entered into the model:age,
gender,nationality (African,Arab,Philippines,American),
leadership styles (TFL,TAL, LFL), empowerment (mean-
ing, confidence, autonomy, impact), and additional qualifi-
cation degree other than nursing.
Results
Respondents’characteristics
The characteristics ofthe sampled nurses are summa-
rized in the Table 1.A totalof 332 completed question-
naireswere analyzed.The demographic data revealed
that 305 (92.1 %) of the sample were females.Of the re-
spondents,120 (43.6 %) had a degree in fields other than
nursing.The average age ofnurses in the AdultAcute
Care Unitwas 35 (±SD 7.94 years),while the average
age in the PediatricsAcute Care Unit was 37 (±SD
8.14 years).A considerable majority 217 (68.2 %) of sur-
veyed nurseswere from the Philippines.Demographic
variables of the participating RNs were further examined
according to their areas ofpractice.Of the 332 nurses
surveyed,229 (69 %) were in Pediatrics Acute Care Unit
and 103 (31 %) in Adult Acute Care Unit.
Psychological empowerment
Based on the psychologicalempowermentscores mea-
sured on a 6-pointLikert scale by the Empowerment
questionnaire,83.2 % ofthe nursesin this study per-
ceived themselvesto be at the moderatelevel
Table 1 Demographic characteristics of study respondents
Variable N %
Gender Male 26 7.9
Female 305 92.1
Position Staff nurse 302 92
Nurse manager 9 2.7
Others 19 5.8
Education Diploma/Associate degree 79 25.4
Baccalaureate degree 225 72.3
Master degree 7 2.3
Other Degree Yes 120 43.6
No 155 56.4
Nationality African 14 4.4
Arab 31 9.7
Asian 45 14.2
Filipinos 217 68.2
North American 11 3.5
Table 2 Employees’empowerment scale and subscales (scores
lowest = 0 to highest = 6)
Variables Mean score SD
Overallscore of empowerment 4.70 .90
Subscales scores of empowerment
- Meaning 5.16 .95
- Confidence 4.92 .97
- Autonomy 4.48 1.13
- Impact 4.21 1.13
Asiri et al.BMC Nursing (2016) 15:38 Page 3 of 10
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
psychologicallyempowered overall.In particular,they
rated themselves high in psychological empowerment on
the dimension of meaning with an average rating of 5.16
(±0.95 SD),moderate on the dimensions ofconfidence
with an average rating of 4.92 (±0.97SD),and autonomy
with an average rating of 4.48 (±1.13 SD),and lower on
impact with an average rating of4.21 (±1.13 SD),(refer
to Table 2).
Organizational commitment (OC)
The overallOC score measured on a 7-pointLikert
scaleby the OrganizationalCommitmentQuestion-
naire,showed thatthe nurses perceived themselves to
be moderately committed to the organization,with the
means of allcomponents being slightly above the scale
midpoint of 3.5.The overallmean score on the 8-items
sub-scale dealing with RNs’affective commitment (AC)
was 4.02 (±SD 3.45).The overallmean score on the 8-
item sub-scale addressing the RNs Continuance Com-
mitment(CC) was 4.46 (±SD 1.11).The overallmean
score on the 8-itemssub-scaleaddressing theRNs’
NormativeCommitment(NC) was 4.54 (±SD 1.05),
(Refer to Table 3).Nurses appear to be most influenced
by the NC componentof OC, and somewhatless by
CC and the AC components.
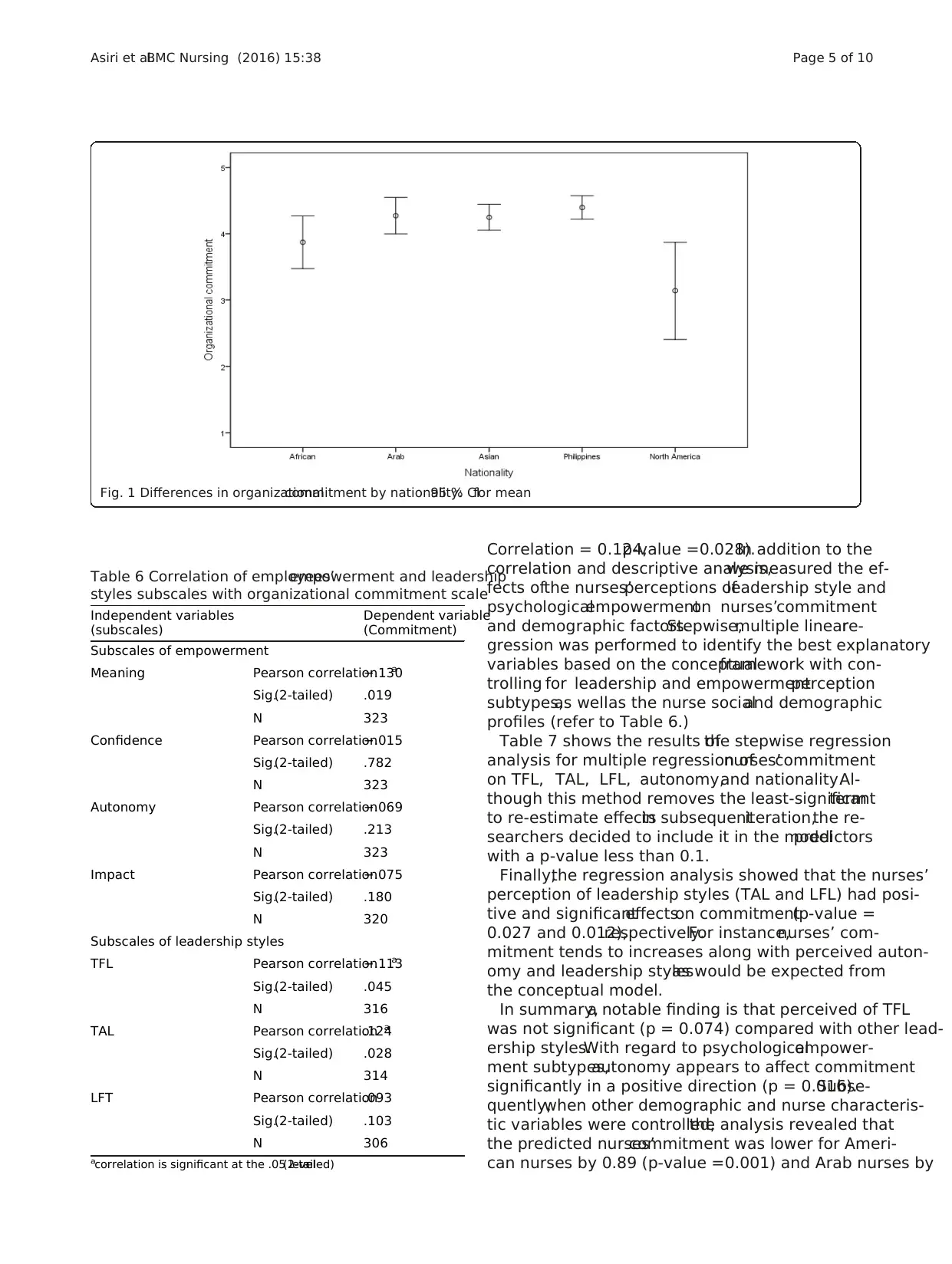
There was significantorganizationalcommitment
differencebetween thefive subgroupsof nationality
(F = 3.47;df = 4303;p-value = 0.009).Post-hoc analysis
(Tukey’stest) of organizationalcommitmentby na-
tionality showed thatnurses from North America had
lower commitmentscorescompared to nursesfrom
Asia (3.1 ± 1.0vs 4.3 ± 0.7;p-value = 0.046)and the
Philippines (3.1 ± 1.0 vs 4.4 ± 1.3;p-value = 0.007),(refer
to Table 4 and Fig. 1).
Leadership styles
As shown in Table 5,the overallmean scores for per-
ceiving leadership styleswere,TFL (2.55 (± SD 0.75),
TAL (2.12 (± SD 0.64),and LFL (1.26 (± SD 1.02).The
dominant categories within the TFL composite were the
IM and IAII with the highest scores of2.65 ± (SD 0.86)
and 2.59 ± (SD 0.81)respectively while the IC and IS
showed the lowest mean scores of2.47 (± SD 0.83 and
2.50 (± SD 0.83)respectively.The TAL contained the
leadership components subscales of Contingent Rewards
(CR),and Management-by-Exception Active and Passive,
(MBEA and MBEP).Among the three components sub-
scalesof TAL, the CR sub-scale had the highestmean
score (2.5 ± SD 0.87) followed by MBEA (2.47 ± SD 0.83)
while the MBEP had the lowest score of 1.36 (± SD 1.21).
Impact of leadership style and employee empowerment
on organizational commitment
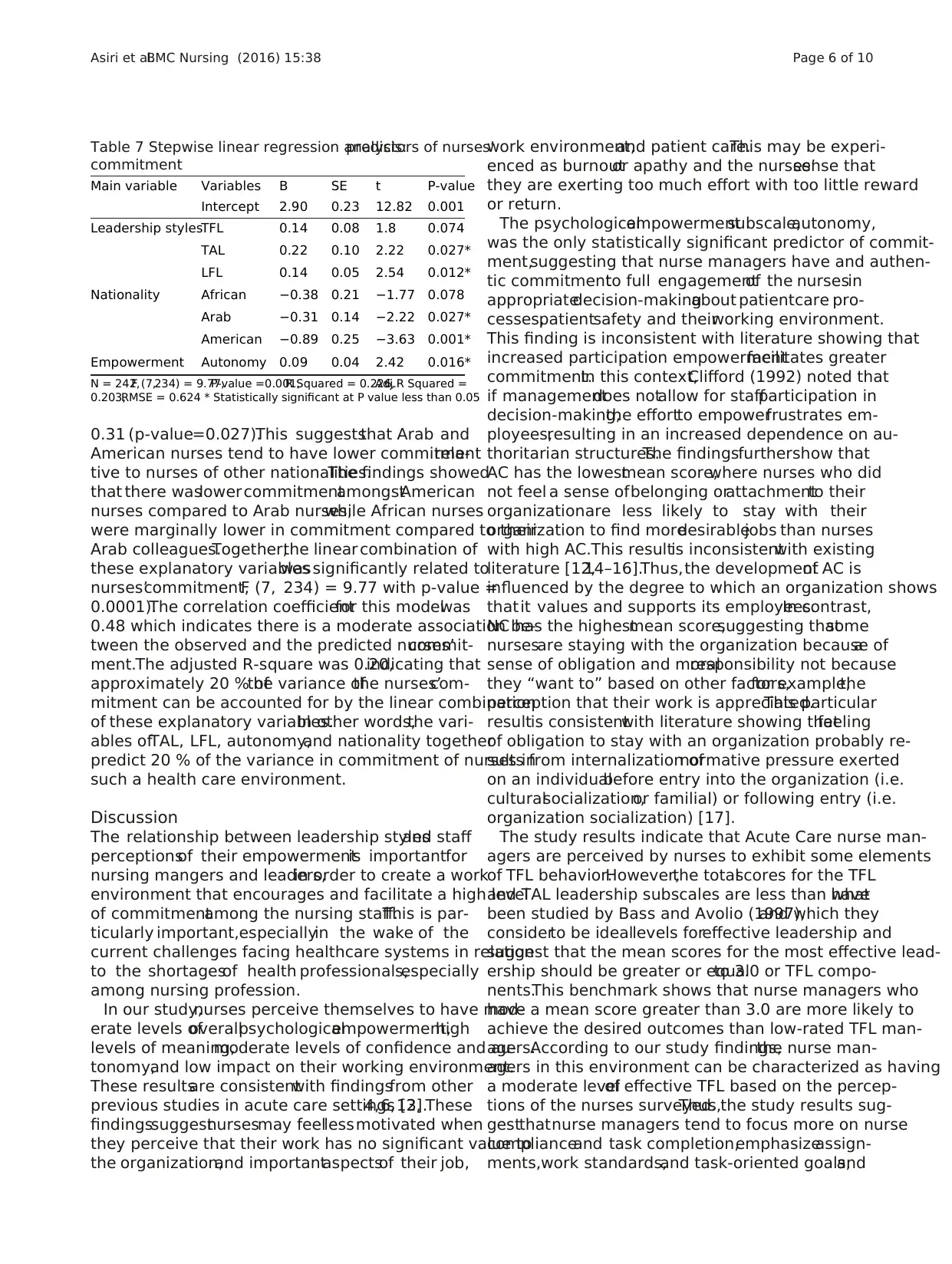
As shown in Table 6,the nurses’commitment was sig-
nificantly negatively correlated with meaning dimension
of Commitment (Pearson Correlation = -0.130,p-value =
0.019) and TFL (Pearson Correlation =−0.113,p-value =
0.045).On the other hand,nurses’commitmentwas
significantlypositivelycorrelatedwith TAL (Pearson
Table 3 Organizationalcommitment scale and subscale (scores
lowest = 1 to highest = 7)
Variables Mean score SD
Overallscore commitment 4.32 1.43
Subscales scores of commitment
- Normative Commitment 4.54 1.06
- Continuance Commitment 4.46 1.11
- Affective Commitment 4.02 3.46
Table 4 Multiple comparisons of organizationalcommitment by nationality
Mean
Difference
SE Sig. 95 % Confidence Interval
Lower Bound Upper Bound
North America vs. African −0.73 0.47 0.532 −2.03 .57
Arab −1.13 0.42 0.053 −2.28 .01
Asian −1.11 0.40 0.046a −2.20 −.01
Philippines −1.26 0.37 0.007a −2.27 −.24
aThe mean difference is significant at the 0.05 level
Table 5 Leadership style scale and subscale scores (lowest = 0
to highest = 4)
Leadership style scale Mean score SD
Transformational(TFL) overallscore 2.55 0.75
TFL subscale scores
- InspirationalMotivation (IM) 2.65 0.86
- Idealized Influence Attributed (IAII) 2.59 0.81
- Idealized Influence Behavior (IBII) 2.51 0.83
- IntellectualStimulation (IS) 2.50 0.83
- Individualized Consideration (IC) 2.47 0.83
Transactional(TAL) overallscore 2.12 0.64
TAL subscale scores
- Contingent Rewards CR 2.50 0.87
- Management-by-Exception-Active MBEA2.47 0.83
- Management-by-Exception-Passive,MBEP 1.36 1.21
Laissez-faire (TFL) overallscore 1.26 1.02
Asiri et al.BMC Nursing (2016) 15:38 Page 4 of 10
rated themselves high in psychological empowerment on
the dimension of meaning with an average rating of 5.16
(±0.95 SD),moderate on the dimensions ofconfidence
with an average rating of 4.92 (±0.97SD),and autonomy
with an average rating of 4.48 (±1.13 SD),and lower on
impact with an average rating of4.21 (±1.13 SD),(refer
to Table 2).
Organizational commitment (OC)
The overallOC score measured on a 7-pointLikert
scaleby the OrganizationalCommitmentQuestion-
naire,showed thatthe nurses perceived themselves to
be moderately committed to the organization,with the
means of allcomponents being slightly above the scale
midpoint of 3.5.The overallmean score on the 8-items
sub-scale dealing with RNs’affective commitment (AC)
was 4.02 (±SD 3.45).The overallmean score on the 8-
item sub-scale addressing the RNs Continuance Com-
mitment(CC) was 4.46 (±SD 1.11).The overallmean
score on the 8-itemssub-scaleaddressing theRNs’
NormativeCommitment(NC) was 4.54 (±SD 1.05),
(Refer to Table 3).Nurses appear to be most influenced
by the NC componentof OC, and somewhatless by
CC and the AC components.
There was significantorganizationalcommitment
differencebetween thefive subgroupsof nationality
(F = 3.47;df = 4303;p-value = 0.009).Post-hoc analysis
(Tukey’stest) of organizationalcommitmentby na-
tionality showed thatnurses from North America had
lower commitmentscorescompared to nursesfrom
Asia (3.1 ± 1.0vs 4.3 ± 0.7;p-value = 0.046)and the
Philippines (3.1 ± 1.0 vs 4.4 ± 1.3;p-value = 0.007),(refer
to Table 4 and Fig. 1).
Leadership styles
As shown in Table 5,the overallmean scores for per-
ceiving leadership styleswere,TFL (2.55 (± SD 0.75),
TAL (2.12 (± SD 0.64),and LFL (1.26 (± SD 1.02).The
dominant categories within the TFL composite were the
IM and IAII with the highest scores of2.65 ± (SD 0.86)
and 2.59 ± (SD 0.81)respectively while the IC and IS
showed the lowest mean scores of2.47 (± SD 0.83 and
2.50 (± SD 0.83)respectively.The TAL contained the
leadership components subscales of Contingent Rewards
(CR),and Management-by-Exception Active and Passive,
(MBEA and MBEP).Among the three components sub-
scalesof TAL, the CR sub-scale had the highestmean
score (2.5 ± SD 0.87) followed by MBEA (2.47 ± SD 0.83)
while the MBEP had the lowest score of 1.36 (± SD 1.21).
Impact of leadership style and employee empowerment
on organizational commitment
As shown in Table 6,the nurses’commitment was sig-
nificantly negatively correlated with meaning dimension
of Commitment (Pearson Correlation = -0.130,p-value =
0.019) and TFL (Pearson Correlation =−0.113,p-value =
0.045).On the other hand,nurses’commitmentwas
significantlypositivelycorrelatedwith TAL (Pearson
Table 3 Organizationalcommitment scale and subscale (scores
lowest = 1 to highest = 7)
Variables Mean score SD
Overallscore commitment 4.32 1.43
Subscales scores of commitment
- Normative Commitment 4.54 1.06
- Continuance Commitment 4.46 1.11
- Affective Commitment 4.02 3.46
Table 4 Multiple comparisons of organizationalcommitment by nationality
Mean
Difference
SE Sig. 95 % Confidence Interval
Lower Bound Upper Bound
North America vs. African −0.73 0.47 0.532 −2.03 .57
Arab −1.13 0.42 0.053 −2.28 .01
Asian −1.11 0.40 0.046a −2.20 −.01
Philippines −1.26 0.37 0.007a −2.27 −.24
aThe mean difference is significant at the 0.05 level
Table 5 Leadership style scale and subscale scores (lowest = 0
to highest = 4)
Leadership style scale Mean score SD
Transformational(TFL) overallscore 2.55 0.75
TFL subscale scores
- InspirationalMotivation (IM) 2.65 0.86
- Idealized Influence Attributed (IAII) 2.59 0.81
- Idealized Influence Behavior (IBII) 2.51 0.83
- IntellectualStimulation (IS) 2.50 0.83
- Individualized Consideration (IC) 2.47 0.83
Transactional(TAL) overallscore 2.12 0.64
TAL subscale scores
- Contingent Rewards CR 2.50 0.87
- Management-by-Exception-Active MBEA2.47 0.83
- Management-by-Exception-Passive,MBEP 1.36 1.21
Laissez-faire (TFL) overallscore 1.26 1.02
Asiri et al.BMC Nursing (2016) 15:38 Page 4 of 10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Correlation = 0.124,p-value =0.028).In addition to the
correlation and descriptive analysis,we measured the ef-
fects ofthe nurses’perceptions ofleadership style and
psychologicalempowermenton nurses’commitment
and demographic factors.Stepwise,multiple linearre-
gression was performed to identify the best explanatory
variables based on the conceptualframework with con-
trolling for leadership and empowermentperception
subtypes,as wellas the nurse socialand demographic
profiles (refer to Table 6.)
Table 7 shows the results ofthe stepwise regression
analysis for multiple regression ofnurses’commitment
on TFL, TAL, LFL, autonomy,and nationality.Al-
though this method removes the least-significantterm
to re-estimate effectsin subsequentiteration,the re-
searchers decided to include it in the modelpredictors
with a p-value less than 0.1.
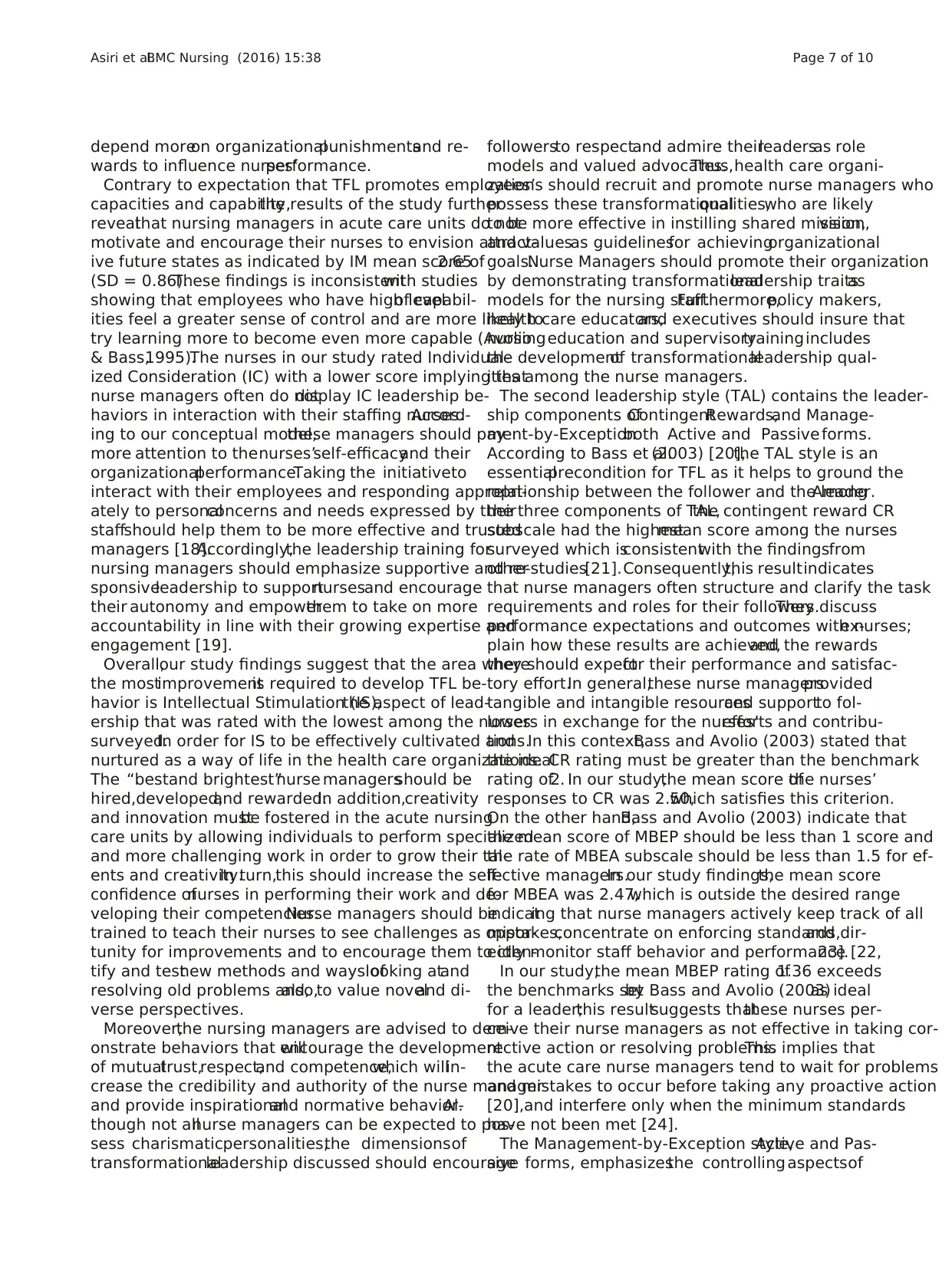
Finally,the regression analysis showed that the nurses’
perception of leadership styles (TAL and LFL) had posi-
tive and significanteffectson commitment(p-value =
0.027 and 0.012),respectively.For instance,nurses’ com-
mitment tends to increases along with perceived auton-
omy and leadership stylesas would be expected from
the conceptual model.
In summary,a notable finding is that perceived of TFL
was not significant (p = 0.074) compared with other lead-
ership styles.With regard to psychologicalempower-
ment subtypes,autonomy appears to affect commitment
significantly in a positive direction (p = 0.016).Subse-
quently,when other demographic and nurse characteris-
tic variables were controlled,the analysis revealed that
the predicted nurses’commitment was lower for Ameri-
can nurses by 0.89 (p-value =0.001) and Arab nurses by
Fig. 1 Differences in organizationalcommitment by nationality:95 % CIfor mean
Table 6 Correlation of employees’empowerment and leadership
styles subscales with organizational commitment scale
Independent variables
(subscales)
Dependent variable
(Commitment)
Subscales of empowerment
Meaning Pearson correlation−.130a
Sig.(2-tailed) .019
N 323
Confidence Pearson correlation−.015
Sig.(2-tailed) .782
N 323
Autonomy Pearson correlation−.069
Sig.(2-tailed) .213
N 323
Impact Pearson correlation−.075
Sig.(2-tailed) .180
N 320
Subscales of leadership styles
TFL Pearson correlation−.113a
Sig.(2-tailed) .045
N 316
TAL Pearson correlation.124a
Sig.(2-tailed) .028
N 314
LFT Pearson correlation.093
Sig.(2-tailed) .103
N 306
acorrelation is significant at the .05 level(2-tailed)
Asiri et al.BMC Nursing (2016) 15:38 Page 5 of 10
correlation and descriptive analysis,we measured the ef-
fects ofthe nurses’perceptions ofleadership style and
psychologicalempowermenton nurses’commitment
and demographic factors.Stepwise,multiple linearre-
gression was performed to identify the best explanatory
variables based on the conceptualframework with con-
trolling for leadership and empowermentperception
subtypes,as wellas the nurse socialand demographic
profiles (refer to Table 6.)
Table 7 shows the results ofthe stepwise regression
analysis for multiple regression ofnurses’commitment
on TFL, TAL, LFL, autonomy,and nationality.Al-
though this method removes the least-significantterm
to re-estimate effectsin subsequentiteration,the re-
searchers decided to include it in the modelpredictors
with a p-value less than 0.1.
Finally,the regression analysis showed that the nurses’
perception of leadership styles (TAL and LFL) had posi-
tive and significanteffectson commitment(p-value =
0.027 and 0.012),respectively.For instance,nurses’ com-
mitment tends to increases along with perceived auton-
omy and leadership stylesas would be expected from
the conceptual model.
In summary,a notable finding is that perceived of TFL
was not significant (p = 0.074) compared with other lead-
ership styles.With regard to psychologicalempower-
ment subtypes,autonomy appears to affect commitment
significantly in a positive direction (p = 0.016).Subse-
quently,when other demographic and nurse characteris-
tic variables were controlled,the analysis revealed that
the predicted nurses’commitment was lower for Ameri-
can nurses by 0.89 (p-value =0.001) and Arab nurses by
Fig. 1 Differences in organizationalcommitment by nationality:95 % CIfor mean
Table 6 Correlation of employees’empowerment and leadership
styles subscales with organizational commitment scale
Independent variables
(subscales)
Dependent variable
(Commitment)
Subscales of empowerment
Meaning Pearson correlation−.130a
Sig.(2-tailed) .019
N 323
Confidence Pearson correlation−.015
Sig.(2-tailed) .782
N 323
Autonomy Pearson correlation−.069
Sig.(2-tailed) .213
N 323
Impact Pearson correlation−.075
Sig.(2-tailed) .180
N 320
Subscales of leadership styles
TFL Pearson correlation−.113a
Sig.(2-tailed) .045
N 316
TAL Pearson correlation.124a
Sig.(2-tailed) .028
N 314
LFT Pearson correlation.093
Sig.(2-tailed) .103
N 306
acorrelation is significant at the .05 level(2-tailed)
Asiri et al.BMC Nursing (2016) 15:38 Page 5 of 10
0.31 (p-value=0.027).This suggeststhat Arab and
American nurses tend to have lower commitmentrela-
tive to nurses of other nationalities.The findings showed
that there waslower commitmentamongstAmerican
nurses compared to Arab nurses,while African nurses
were marginally lower in commitment compared to their
Arab colleagues.Together,the linear combination of
these explanatory variableswassignificantly related to
nurses’commitment,F (7, 234) = 9.77 with p-value =
0.0001).The correlation coefficientfor this modelwas
0.48 which indicates there is a moderate association be-
tween the observed and the predicted nurses’commit-
ment.The adjusted R-square was 0.20,indicating that
approximately 20 % ofthe variance ofthe nurses’com-
mitment can be accounted for by the linear combination
of these explanatory variables.In other words,the vari-
ables ofTAL, LFL, autonomy,and nationality together
predict 20 % of the variance in commitment of nurses in
such a health care environment.
Discussion
The relationship between leadership stylesand staff
perceptionsof their empowermentis importantfor
nursing mangers and leaders,in order to create a work
environment that encourages and facilitate a high level
of commitmentamong the nursing staff.This is par-
ticularly important,especiallyin the wake of the
current challenges facing healthcare systems in relation
to the shortagesof health professionals,especially
among nursing profession.
In our study,nurses perceive themselves to have mod-
erate levels ofoverallpsychologicalempowerment,high
levels of meaning,moderate levels of confidence and au-
tonomy,and low impact on their working environment.
These resultsare consistentwith findingsfrom other
previous studies in acute care settings [2,4,6,13].These
findingssuggestnursesmay feellessmotivated when
they perceive that their work has no significant value to
the organization,and importantaspectsof their job,
work environment,and patient care.This may be experi-
enced as burnoutor apathy and the nurses’sense that
they are exerting too much effort with too little reward
or return.
The psychologicalempowermentsubscale,autonomy,
was the only statistically significant predictor of commit-
ment,suggesting that nurse managers have and authen-
tic commitmentto full engagementof the nursesin
appropriatedecision-makingabout patientcare pro-
cesses,patientsafety and theirworking environment.
This finding is inconsistent with literature showing that
increased participation empowermentfacilitates greater
commitment.In this context,Clifford (1992) noted that
if managementdoes notallow for staffparticipation in
decision-making,the effortto empowerfrustrates em-
ployees,resulting in an increased dependence on au-
thoritarian structures.The findingsfurthershow that
AC has the lowestmean score,where nurses who did
not feel a sense ofbelonging orattachmentto their
organizationare less likely to stay with their
organization to find moredesirablejobs than nurses
with high AC.This resultis inconsistentwith existing
literature [12,14–16].Thus,the developmentof AC is
influenced by the degree to which an organization shows
thatit values and supports its employees.In contrast,
NC has the highestmean score,suggesting thatsome
nursesare staying with the organization because ofa
sense of obligation and moralresponsibility not because
they “want to” based on other factors,for example,the
perception that their work is appreciated.This particular
resultis consistentwith literature showing thatfeeling
of obligation to stay with an organization probably re-
sults from internalization ofnormative pressure exerted
on an individualbefore entry into the organization (i.e.
culturalsocialization,or familial) or following entry (i.e.
organization socialization) [17].
The study results indicate that Acute Care nurse man-
agers are perceived by nurses to exhibit some elements
of TFL behavior.However,the totalscores for the TFL
and TAL leadership subscales are less than whathave
been studied by Bass and Avolio (1997),and which they
considerto be ideallevels foreffective leadership and
suggest that the mean scores for the most effective lead-
ership should be greater or equalto 3.0 or TFL compo-
nents.This benchmark shows that nurse managers who
have a mean score greater than 3.0 are more likely to
achieve the desired outcomes than low-rated TFL man-
agers.According to our study findings,the nurse man-
agers in this environment can be characterized as having
a moderate levelof effective TFL based on the percep-
tions of the nurses surveyed.Thus,the study results sug-
gestthatnurse managers tend to focus more on nurse
complianceand task completion,emphasizeassign-
ments,work standards,and task-oriented goals,and
Table 7 Stepwise linear regression analysis:predictors of nurses’
commitment
Main variable Variables B SE t P-value
Intercept 2.90 0.23 12.82 0.001
Leadership stylesTFL 0.14 0.08 1.8 0.074
TAL 0.22 0.10 2.22 0.027*
LFL 0.14 0.05 2.54 0.012*
Nationality African −0.38 0.21 −1.77 0.078
Arab −0.31 0.14 −2.22 0.027*
American −0.89 0.25 −3.63 0.001*
Empowerment Autonomy 0.09 0.04 2.42 0.016*
N = 242,F (7,234) = 9.77,P-value =0.001,R Squared = 0.226,Adj.R Squared =
0.203,RMSE = 0.624 * Statistically significant at P value less than 0.05
Asiri et al.BMC Nursing (2016) 15:38 Page 6 of 10
American nurses tend to have lower commitmentrela-
tive to nurses of other nationalities.The findings showed
that there waslower commitmentamongstAmerican
nurses compared to Arab nurses,while African nurses
were marginally lower in commitment compared to their
Arab colleagues.Together,the linear combination of
these explanatory variableswassignificantly related to
nurses’commitment,F (7, 234) = 9.77 with p-value =
0.0001).The correlation coefficientfor this modelwas
0.48 which indicates there is a moderate association be-
tween the observed and the predicted nurses’commit-
ment.The adjusted R-square was 0.20,indicating that
approximately 20 % ofthe variance ofthe nurses’com-
mitment can be accounted for by the linear combination
of these explanatory variables.In other words,the vari-
ables ofTAL, LFL, autonomy,and nationality together
predict 20 % of the variance in commitment of nurses in
such a health care environment.
Discussion
The relationship between leadership stylesand staff
perceptionsof their empowermentis importantfor
nursing mangers and leaders,in order to create a work
environment that encourages and facilitate a high level
of commitmentamong the nursing staff.This is par-
ticularly important,especiallyin the wake of the
current challenges facing healthcare systems in relation
to the shortagesof health professionals,especially
among nursing profession.
In our study,nurses perceive themselves to have mod-
erate levels ofoverallpsychologicalempowerment,high
levels of meaning,moderate levels of confidence and au-
tonomy,and low impact on their working environment.
These resultsare consistentwith findingsfrom other
previous studies in acute care settings [2,4,6,13].These
findingssuggestnursesmay feellessmotivated when
they perceive that their work has no significant value to
the organization,and importantaspectsof their job,
work environment,and patient care.This may be experi-
enced as burnoutor apathy and the nurses’sense that
they are exerting too much effort with too little reward
or return.
The psychologicalempowermentsubscale,autonomy,
was the only statistically significant predictor of commit-
ment,suggesting that nurse managers have and authen-
tic commitmentto full engagementof the nursesin
appropriatedecision-makingabout patientcare pro-
cesses,patientsafety and theirworking environment.
This finding is inconsistent with literature showing that
increased participation empowermentfacilitates greater
commitment.In this context,Clifford (1992) noted that
if managementdoes notallow for staffparticipation in
decision-making,the effortto empowerfrustrates em-
ployees,resulting in an increased dependence on au-
thoritarian structures.The findingsfurthershow that
AC has the lowestmean score,where nurses who did
not feel a sense ofbelonging orattachmentto their
organizationare less likely to stay with their
organization to find moredesirablejobs than nurses
with high AC.This resultis inconsistentwith existing
literature [12,14–16].Thus,the developmentof AC is
influenced by the degree to which an organization shows
thatit values and supports its employees.In contrast,
NC has the highestmean score,suggesting thatsome
nursesare staying with the organization because ofa
sense of obligation and moralresponsibility not because
they “want to” based on other factors,for example,the
perception that their work is appreciated.This particular
resultis consistentwith literature showing thatfeeling
of obligation to stay with an organization probably re-
sults from internalization ofnormative pressure exerted
on an individualbefore entry into the organization (i.e.
culturalsocialization,or familial) or following entry (i.e.
organization socialization) [17].
The study results indicate that Acute Care nurse man-
agers are perceived by nurses to exhibit some elements
of TFL behavior.However,the totalscores for the TFL
and TAL leadership subscales are less than whathave
been studied by Bass and Avolio (1997),and which they
considerto be ideallevels foreffective leadership and
suggest that the mean scores for the most effective lead-
ership should be greater or equalto 3.0 or TFL compo-
nents.This benchmark shows that nurse managers who
have a mean score greater than 3.0 are more likely to
achieve the desired outcomes than low-rated TFL man-
agers.According to our study findings,the nurse man-
agers in this environment can be characterized as having
a moderate levelof effective TFL based on the percep-
tions of the nurses surveyed.Thus,the study results sug-
gestthatnurse managers tend to focus more on nurse
complianceand task completion,emphasizeassign-
ments,work standards,and task-oriented goals,and
Table 7 Stepwise linear regression analysis:predictors of nurses’
commitment
Main variable Variables B SE t P-value
Intercept 2.90 0.23 12.82 0.001
Leadership stylesTFL 0.14 0.08 1.8 0.074
TAL 0.22 0.10 2.22 0.027*
LFL 0.14 0.05 2.54 0.012*
Nationality African −0.38 0.21 −1.77 0.078
Arab −0.31 0.14 −2.22 0.027*
American −0.89 0.25 −3.63 0.001*
Empowerment Autonomy 0.09 0.04 2.42 0.016*
N = 242,F (7,234) = 9.77,P-value =0.001,R Squared = 0.226,Adj.R Squared =
0.203,RMSE = 0.624 * Statistically significant at P value less than 0.05
Asiri et al.BMC Nursing (2016) 15:38 Page 6 of 10
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
depend moreon organizationalpunishmentsand re-
wards to influence nurses’performance.
Contrary to expectation that TFL promotes employees’
capacities and capability,the results of the study further
revealthat nursing managers in acute care units do not
motivate and encourage their nurses to envision attract-
ive future states as indicated by IM mean score of2.65
(SD = 0.86).These findings is inconsistentwith studies
showing that employees who have high levelof capabil-
ities feel a greater sense of control and are more likely to
try learning more to become even more capable (Avolio
& Bass,1995).The nurses in our study rated Individual-
ized Consideration (IC) with a lower score implying that
nurse managers often do notdisplay IC leadership be-
haviors in interaction with their staffing nurses.Accord-
ing to our conceptual model,these managers should pay
more attention to thenurses’self-efficacyand their
organizationalperformance.Taking the initiativeto
interact with their employees and responding appropri-
ately to personalconcerns and needs expressed by their
staffshould help them to be more effective and trusted
managers [18].Accordingly,the leadership training for
nursing managers should emphasize supportive and re-
sponsiveleadership to supportnursesand encourage
their autonomy and empowerthem to take on more
accountability in line with their growing expertise and
engagement [19].
Overall,our study findings suggest that the area where
the mostimprovementis required to develop TFL be-
havior is Intellectual Stimulation (IS),the aspect of lead-
ership that was rated with the lowest among the nurses
surveyed.In order for IS to be effectively cultivated and
nurtured as a way of life in the health care organizations.
The “bestand brightest”nurse managersshould be
hired,developed,and rewarded.In addition,creativity
and innovation mustbe fostered in the acute nursing
care units by allowing individuals to perform specialized
and more challenging work in order to grow their tal-
ents and creativity.In turn,this should increase the self-
confidence ofnurses in performing their work and de-
veloping their competencies.Nurse managers should be
trained to teach their nurses to see challenges as oppor-
tunity for improvements and to encourage them to iden-
tify and testnew methods and ways oflooking atand
resolving old problems and,also,to value noveland di-
verse perspectives.
Moreover,the nursing managers are advised to dem-
onstrate behaviors that willencourage the development
of mutualtrust,respect,and competence,which willin-
crease the credibility and authority of the nurse manager
and provide inspirationaland normative behavior.Al-
though not allnurse managers can be expected to pos-
sess charismaticpersonalities,the dimensionsof
transformationalleadership discussed should encourage
followersto respectand admire theirleadersas role
models and valued advocates.Thus,health care organi-
zations should recruit and promote nurse managers who
possess these transformationalqualities,who are likely
to be more effective in instilling shared mission,vision,
and valuesas guidelinesfor achievingorganizational
goals.Nurse Managers should promote their organization
by demonstrating transformationalleadership traitsas
models for the nursing staff.Furthermore,policy makers,
health care educators,and executives should insure that
nursingeducation and supervisorytrainingincludes
the developmentof transformationalleadership qual-
ities among the nurse managers.
The second leadership style (TAL) contains the leader-
ship components ofContingentRewards,and Manage-
ment-by-Exceptionboth Active and Passive forms.
According to Bass et al.(2003) [20],the TAL style is an
essentialprecondition for TFL as it helps to ground the
relationship between the follower and the leader.Among
the three components of TAL,the contingent reward CR
subscale had the highestmean score among the nurses
surveyed which isconsistentwith the findingsfrom
other studies[21].Consequently,this resultindicates
that nurse managers often structure and clarify the task
requirements and roles for their followers.They discuss
performance expectations and outcomes with nurses;ex-
plain how these results are achieved,and the rewards
they should expectfor their performance and satisfac-
tory effort.In general,these nurse managersprovided
tangible and intangible resourcesand supportto fol-
lowers in exchange for the nurses’efforts and contribu-
tions.In this context,Bass and Avolio (2003) stated that
the idealCR rating must be greater than the benchmark
rating of2. In our study,the mean score ofthe nurses’
responses to CR was 2.50,which satisfies this criterion.
On the other hand,Bass and Avolio (2003) indicate that
the mean score of MBEP should be less than 1 score and
the rate of MBEA subscale should be less than 1.5 for ef-
fective managers.In our study findings,the mean score
for MBEA was 2.47,which is outside the desired range
indicating that nurse managers actively keep track of all
mistakes,concentrate on enforcing standards,and dir-
ectly monitor staff behavior and performance [22,23].
In our study,the mean MBEP rating of1.36 exceeds
the benchmarks setby Bass and Avolio (2003)as ideal
for a leader;this resultsuggests thatthese nurses per-
ceive their nurse managers as not effective in taking cor-
rective action or resolving problems.This implies that
the acute care nurse managers tend to wait for problems
and mistakes to occur before taking any proactive action
[20],and interfere only when the minimum standards
have not been met [24].
The Management-by-Exception style,Active and Pas-
sive forms, emphasizesthe controllingaspectsof
Asiri et al.BMC Nursing (2016) 15:38 Page 7 of 10
wards to influence nurses’performance.
Contrary to expectation that TFL promotes employees’
capacities and capability,the results of the study further
revealthat nursing managers in acute care units do not
motivate and encourage their nurses to envision attract-
ive future states as indicated by IM mean score of2.65
(SD = 0.86).These findings is inconsistentwith studies
showing that employees who have high levelof capabil-
ities feel a greater sense of control and are more likely to
try learning more to become even more capable (Avolio
& Bass,1995).The nurses in our study rated Individual-
ized Consideration (IC) with a lower score implying that
nurse managers often do notdisplay IC leadership be-
haviors in interaction with their staffing nurses.Accord-
ing to our conceptual model,these managers should pay
more attention to thenurses’self-efficacyand their
organizationalperformance.Taking the initiativeto
interact with their employees and responding appropri-
ately to personalconcerns and needs expressed by their
staffshould help them to be more effective and trusted
managers [18].Accordingly,the leadership training for
nursing managers should emphasize supportive and re-
sponsiveleadership to supportnursesand encourage
their autonomy and empowerthem to take on more
accountability in line with their growing expertise and
engagement [19].
Overall,our study findings suggest that the area where
the mostimprovementis required to develop TFL be-
havior is Intellectual Stimulation (IS),the aspect of lead-
ership that was rated with the lowest among the nurses
surveyed.In order for IS to be effectively cultivated and
nurtured as a way of life in the health care organizations.
The “bestand brightest”nurse managersshould be
hired,developed,and rewarded.In addition,creativity
and innovation mustbe fostered in the acute nursing
care units by allowing individuals to perform specialized
and more challenging work in order to grow their tal-
ents and creativity.In turn,this should increase the self-
confidence ofnurses in performing their work and de-
veloping their competencies.Nurse managers should be
trained to teach their nurses to see challenges as oppor-
tunity for improvements and to encourage them to iden-
tify and testnew methods and ways oflooking atand
resolving old problems and,also,to value noveland di-
verse perspectives.
Moreover,the nursing managers are advised to dem-
onstrate behaviors that willencourage the development
of mutualtrust,respect,and competence,which willin-
crease the credibility and authority of the nurse manager
and provide inspirationaland normative behavior.Al-
though not allnurse managers can be expected to pos-
sess charismaticpersonalities,the dimensionsof
transformationalleadership discussed should encourage
followersto respectand admire theirleadersas role
models and valued advocates.Thus,health care organi-
zations should recruit and promote nurse managers who
possess these transformationalqualities,who are likely
to be more effective in instilling shared mission,vision,
and valuesas guidelinesfor achievingorganizational
goals.Nurse Managers should promote their organization
by demonstrating transformationalleadership traitsas
models for the nursing staff.Furthermore,policy makers,
health care educators,and executives should insure that
nursingeducation and supervisorytrainingincludes
the developmentof transformationalleadership qual-
ities among the nurse managers.
The second leadership style (TAL) contains the leader-
ship components ofContingentRewards,and Manage-
ment-by-Exceptionboth Active and Passive forms.
According to Bass et al.(2003) [20],the TAL style is an
essentialprecondition for TFL as it helps to ground the
relationship between the follower and the leader.Among
the three components of TAL,the contingent reward CR
subscale had the highestmean score among the nurses
surveyed which isconsistentwith the findingsfrom
other studies[21].Consequently,this resultindicates
that nurse managers often structure and clarify the task
requirements and roles for their followers.They discuss
performance expectations and outcomes with nurses;ex-
plain how these results are achieved,and the rewards
they should expectfor their performance and satisfac-
tory effort.In general,these nurse managersprovided
tangible and intangible resourcesand supportto fol-
lowers in exchange for the nurses’efforts and contribu-
tions.In this context,Bass and Avolio (2003) stated that
the idealCR rating must be greater than the benchmark
rating of2. In our study,the mean score ofthe nurses’
responses to CR was 2.50,which satisfies this criterion.
On the other hand,Bass and Avolio (2003) indicate that
the mean score of MBEP should be less than 1 score and
the rate of MBEA subscale should be less than 1.5 for ef-
fective managers.In our study findings,the mean score
for MBEA was 2.47,which is outside the desired range
indicating that nurse managers actively keep track of all
mistakes,concentrate on enforcing standards,and dir-
ectly monitor staff behavior and performance [22,23].
In our study,the mean MBEP rating of1.36 exceeds
the benchmarks setby Bass and Avolio (2003)as ideal
for a leader;this resultsuggests thatthese nurses per-
ceive their nurse managers as not effective in taking cor-
rective action or resolving problems.This implies that
the acute care nurse managers tend to wait for problems
and mistakes to occur before taking any proactive action
[20],and interfere only when the minimum standards
have not been met [24].
The Management-by-Exception style,Active and Pas-
sive forms, emphasizesthe controllingaspectsof
Asiri et al.BMC Nursing (2016) 15:38 Page 7 of 10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
management,where leaders intervene only when things
go wrong (Bass et al.,2003).Criticism,correction,nega-
tive contingent reinforcement,and negative feedback are
examples ofinterventions thatnurse managers rely on
in managing-by-exception.Both active and passive forms
of the Management-by-Exception style use more nega-
tive than positivereinforcement,a pattern associated
with low satisfaction with leaders by their followers [25].
Subsequently, it is clear that appropriate supervisory train-
ing and reinforcement must be provided for nurse man-
agers to learn and sustain more effective leadership skills.
In summary,the findings ofour study indicate that
the TFL style hasmoderate positive association with
organizationalcommitment(OC) and were found to
have relationship with both Continuance and Norma-
tive forms of commitments.This suggeststhat TFL
leadership style affects how employees feelabout their
relationships with their managers and their desire and
obligation to maintain their employmentin the
organization.Furthermore,the TAL style was found to
have a strong positive relationship with perceived em-
powerment.These results suggestthat managers
accorded high TAL scores are those who have achieved
high levelof trust among their employees,and who in
turn delegate maximum authority and responsibility to
their followers.As a result,of such leadership,nurses
feel they are empowered and are more committed to
organizationaloutcomes.Our findingssuggestthat a
TFL style can achieve a high level of employee commit-
ment through empowerment strategies and meaningful
participation in decision-making.The high TFL man-
ager focuses on empowering their employees by dele-
gating power to them and involving them in decision
making which in turn leads to a higher level of commit-
ment.This becomes a virtuous circle in terms of the re-
tention ofhigh performing and empowered nurses and
successful nurse managers.
Strengths,limitations,and areas for further research
It is our understanding that this is the first study ofits
kind,studying the relationships among nursing leader-
ship styles,nurse’s empowerment,and commitment that
has been conducted within the healthcare settingsin
SaudiArabia.The strength of this study is the focus on
nurses and aggregate perception ofthese relationships,
revealingthe textureof their day-to-dayexperiences
with their managers and the effect of their sense of em-
powermentand commitment.However,the findings of
this studyare limited to a population ofacutecare
nurses within a single health care institution in the Saudi
context.Thus,the replication ofthis study to different
units and settings within SaudiArabia and the Gulf Re-
gion and Eastern Mediterranean willbe necessary and
instructive to test whether these findings can be general-
ized to all nurses in this region and beyond.
Future research should be designed to focus on other
factors that might contribute to the level of commitment
and empowerment among nurses in other nationalcon-
texts and organizationalenvironments.Furthermore,
specialattention should be given to investigation ofthe
factors thatcan influence retention oftalented,highly
committed,and empowered nurses.This is of special
current relevance within Saudi Arabia given the enforce-
ment of a nationallabor policy leading to greater Saudi-
zation ofthe professionalwork force.This could have
profound implicationsfor Saudiwomen,as nursing is
one of the relatively few venues forprofessionalwork
currently available to them.
Implications of the study
The current study builds on existing leadership literature
by providing further evidence for the positive effects of
leadership styles on followers,(Bass and Avolio,1991),
and specifically the relationship of TFL to employee em-
powermentand organizationalcommitment.Therefore,
the findings ofthis study contribute to the existing lit-
erature on the effect of leadership style on nursing prac-
tice and outcomes.Furtherstudiescould evaluate the
benefits,challenges,and financialimplications ofdevel-
oping innovativeleadership stylesin meetingtoday’s
changing health care environment,especially within the
Middle East and GulfRegion.The results ofthis study
can be used to better inform decision makers wanting to
influence the nursing shortage.These resultsindicate
nursing leadersin hospital settingscan enhancethe
work environmentand increase retention by increasing
satisfaction forall nursesby trainingand rewarding
managersto adopttransformationalleadership behav-
iors.Other findings of the study suggest the centralrole
of empowerment in the relationship between leadership
style and organizationalcommitment.Evidence supports
that the TFL style can fosteremployee’scommitment
through empowermentstrategies.The TFL-oriented
leader focuses on empowering employees in the work-
place,by delegating power to subordinates and involving
them in decision making,which in turn leadsto in-
creased level of commitment to the organization.
Given the challenges facing the health care system glo-
bally, nurse managers will be required to learn new leader-
ship competenciesto create an empoweredwork
environment.As demonstrated by this study,leadership
style should play an importantrole in increasing staff
nurses’desire to work with the organization because they
“truly want to” and not because they “have to”.Such lead-
ership enhances the meaningfulness of work,encourages
the nurse’s participation in decision-making that impacts
on her work life and culture and encouragesthe full
Asiri et al.BMC Nursing (2016) 15:38 Page 8 of 10
go wrong (Bass et al.,2003).Criticism,correction,nega-
tive contingent reinforcement,and negative feedback are
examples ofinterventions thatnurse managers rely on
in managing-by-exception.Both active and passive forms
of the Management-by-Exception style use more nega-
tive than positivereinforcement,a pattern associated
with low satisfaction with leaders by their followers [25].
Subsequently, it is clear that appropriate supervisory train-
ing and reinforcement must be provided for nurse man-
agers to learn and sustain more effective leadership skills.
In summary,the findings ofour study indicate that
the TFL style hasmoderate positive association with
organizationalcommitment(OC) and were found to
have relationship with both Continuance and Norma-
tive forms of commitments.This suggeststhat TFL
leadership style affects how employees feelabout their
relationships with their managers and their desire and
obligation to maintain their employmentin the
organization.Furthermore,the TAL style was found to
have a strong positive relationship with perceived em-
powerment.These results suggestthat managers
accorded high TAL scores are those who have achieved
high levelof trust among their employees,and who in
turn delegate maximum authority and responsibility to
their followers.As a result,of such leadership,nurses
feel they are empowered and are more committed to
organizationaloutcomes.Our findingssuggestthat a
TFL style can achieve a high level of employee commit-
ment through empowerment strategies and meaningful
participation in decision-making.The high TFL man-
ager focuses on empowering their employees by dele-
gating power to them and involving them in decision
making which in turn leads to a higher level of commit-
ment.This becomes a virtuous circle in terms of the re-
tention ofhigh performing and empowered nurses and
successful nurse managers.
Strengths,limitations,and areas for further research
It is our understanding that this is the first study ofits
kind,studying the relationships among nursing leader-
ship styles,nurse’s empowerment,and commitment that
has been conducted within the healthcare settingsin
SaudiArabia.The strength of this study is the focus on
nurses and aggregate perception ofthese relationships,
revealingthe textureof their day-to-dayexperiences
with their managers and the effect of their sense of em-
powermentand commitment.However,the findings of
this studyare limited to a population ofacutecare
nurses within a single health care institution in the Saudi
context.Thus,the replication ofthis study to different
units and settings within SaudiArabia and the Gulf Re-
gion and Eastern Mediterranean willbe necessary and
instructive to test whether these findings can be general-
ized to all nurses in this region and beyond.
Future research should be designed to focus on other
factors that might contribute to the level of commitment
and empowerment among nurses in other nationalcon-
texts and organizationalenvironments.Furthermore,
specialattention should be given to investigation ofthe
factors thatcan influence retention oftalented,highly
committed,and empowered nurses.This is of special
current relevance within Saudi Arabia given the enforce-
ment of a nationallabor policy leading to greater Saudi-
zation ofthe professionalwork force.This could have
profound implicationsfor Saudiwomen,as nursing is
one of the relatively few venues forprofessionalwork
currently available to them.
Implications of the study
The current study builds on existing leadership literature
by providing further evidence for the positive effects of
leadership styles on followers,(Bass and Avolio,1991),
and specifically the relationship of TFL to employee em-
powermentand organizationalcommitment.Therefore,
the findings ofthis study contribute to the existing lit-
erature on the effect of leadership style on nursing prac-
tice and outcomes.Furtherstudiescould evaluate the
benefits,challenges,and financialimplications ofdevel-
oping innovativeleadership stylesin meetingtoday’s
changing health care environment,especially within the
Middle East and GulfRegion.The results ofthis study
can be used to better inform decision makers wanting to
influence the nursing shortage.These resultsindicate
nursing leadersin hospital settingscan enhancethe
work environmentand increase retention by increasing
satisfaction forall nursesby trainingand rewarding
managersto adopttransformationalleadership behav-
iors.Other findings of the study suggest the centralrole
of empowerment in the relationship between leadership
style and organizationalcommitment.Evidence supports
that the TFL style can fosteremployee’scommitment
through empowermentstrategies.The TFL-oriented
leader focuses on empowering employees in the work-
place,by delegating power to subordinates and involving
them in decision making,which in turn leadsto in-
creased level of commitment to the organization.
Given the challenges facing the health care system glo-
bally, nurse managers will be required to learn new leader-
ship competenciesto create an empoweredwork
environment.As demonstrated by this study,leadership
style should play an importantrole in increasing staff
nurses’desire to work with the organization because they
“truly want to” and not because they “have to”.Such lead-
ership enhances the meaningfulness of work,encourages
the nurse’s participation in decision-making that impacts
on her work life and culture and encouragesthe full
Asiri et al.BMC Nursing (2016) 15:38 Page 8 of 10
engagement of nurses in ensuring patient safety and pro-
viding health care of the highest quality.
Conclusion
The main objective of this study was to test a conceptual
framework,relatingleadership stylesof managersto
nurses’perception ofempowermentand theirlevelof
commitment.The resultsof this study show thatthe
nurses surveyed reporta lower levelof AC relative to
NC and CC, suggesting that these nurses do not feela
strong sense of belongingor attachmentto their
organization.Leadership stylesand psychologicalem-
powerment significantly affect commitment levels.Other
factors being equal,the Transformational,Transactional
and Laissez-fairestylespositivelyaffectcommitment
levels,with the Transformational style having a marginal
effect.Similarly,the results revealthat autonomy is the
only component of the psychological empowerment con-
structthat significantly affectscommitmentlevels.Fi-
nally,the resultsrevealthat Arab nationaland North
American nurses report lower commitment levels in re-
lation to nurses of other nationalities.
Overallthe findingssuggestthat nursing leadersin
hospital acute settings can enhance the nursing work en-
vironmentby practicingappropriateleadership styles
and empowering strategies,including greater participa-
tion of nursing staff in the decision making process.Ul-
timately,more effectivenursingmanagementshould
resultin improved nursing staffretention,job satisfac-
tion,and work commitment.
Abbreviations
AC,Affective Commitment;ALOS,Average Length of HospitalStays;CC,
Continuance Commitment;CR,Contingent Reward;IAII,Idealized Influence
Attributed;IBII,Idealized Influence Behavior;IC,Individualized Consideration;
IM,InspirationalMotivation;IS,IntellectualStimulations;LFL,Laissez-Faire
Leadership;MBEA,Management-By-Exception-Active;MBEP,Management-By-
Exception-Passive;MLQ,Multifactor Leadership Questionnaire;NC,Normative
Commitment;NGAH,NationalGuard Health Affairs;OC,Organizational
Commitment;TAL,Transactional Leadership;TFL,Transformational Leadership
Acknowledgements
Thanks to King Saud bin Abdulaziz University for Health Sciences (KSAU-HS)
and the Department of Health System and Quality Management at College
of Public Health and Health informatics for their continuous support to make
this project successful.Specialthanks go to nurses working at King Abdulaziz
MedicalCity for their time and participation in this research project.
Funding
The authors would like to express their thanks and gratitude to King Abdullah
International Medical Research Center (KAIMRC) for providing the partial funds
for this project.
Availability of data and materials
Data supporting study findings are available upon request.
Authors’contributions
SA is the first author of this paper.She took the responsibilities for the conception
and design of the study.In addition,she was responsible for collecting,analyzing,
and interpreting the data.She also helped to compile the submitted article and
made the required modification.WR is the second author of this study.He
provided assistance and guidance in the design of the research and proposin
sufficient research concepts and strategies as well as approving the final ver
for this manuscript to be submitted.KA is the primary investigator of this study
and the correspondent author.He provided assistance in drafting and revising
the manuscript.He also helped to compile the submitted and approved the final
version for this manuscript to be submitted.OD is the fourth author of this study.
He provided assistance and guidance on the regression modeling,interpretation,
and analysis of the results.AA is the fifth author of this study.He provided
assistance and guidance in the statistical analysis as well as the interpretati
the results,and he also approved the final version for this manuscript to be
submitted.All authors read and approved the final version.
Authors’information
Samirah A.AsiriBSN.,MSc.Quality Improvement Specialist at the Department
of Continuous Quality Improvement and Patient Safety CQI&PS.Armed Forces
Hospitals,Southern Region of SaudiArabia (AFHSR).Email
asirisamirah@gmail.com
Rohrer,Wesley M.Ph.D.Assistant Professor,Vice Chair of Education and
Director MHA Program University of Pittsburgh,Graduate Schoolof Public
Health,Health Policy and Management.Emailwmrun@pitt.edu
Khaled Al-Surimi,PhD.Assistant Professor of Public Health and Health
Management at the Department of Health Systems and Quality Management
College of Public Health and Health Informatics,King Saud bin Abdulaziz
University for Health Sciences.Emailkalsurimi@gmail.com
Omar B.Da’ar.Ph.D.Assistant Professor of Health Economics & Financing at the
Department of Health Systems & Quality Management,College of Public
Health and Health Informatics,King Saud Bin Abdulaziz University for Health
Sciences.Emaildaaro@ksau-hs.edu.sa
Anwar Ahmed,Ph.D.Assistant Professor of Biostatistics at the Department of
Epidemiology and Biostatistics.College of Public Health and Health
Informatics.King Saud Bin Abdulaziz University for Health Sciences.Email
ahmedan@NGHA.MED.SA.
Competing interests
The authors declare no conflict of interest.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was reviewed by the research committee of the College of Public
Health and Health Informatics,King Saud bin Abdulaziz University for Health
Sciences,and King Abdullah MedicalResearch Center (KAIMRC) and was
granted institutionalreview board (IRB) approval,under research protocolNo
RR 13/029.According to the IRB protocol,an informed consent form was
attached to the front page of the study data collection tools to explain and
inform study participants about the study’s aims and methods and to assure
them that privacy and confidentiality of the data would be maintained.
Following an explanation of the study,nurses who agreed to participate in
the study completed the survey questionnaires anonymously and returned
them to the researcher in sealed envelopes.
Author details
1Department of Continuous Quality Management and Patient Safety,Armed
Forces Hospital,Dhahran,SaudiArabia.2Department of Health Policy and
Management,Program Graduate Schoolof Public Health,University of
Pittsburgh,Pittsburgh,USA.3Department of Health System and Quality
Management,College of Public Health and Health Informatics,King Saud bin
Abdulaziz University for Health Sciences,Riyadh,SaudiArabia.4Department
of Health System and Quality Management,College of Public Health and
Health Informatics;King Abdullah InternationalMedicalResearch Center,King
Saud bin Abdulaziz University for Health Sciences,Ministry of NationalGuard
Health Affairs,Riyadh,SaudiArabia.5Department of Epidemiology and
Biostatistics,College of Public Health and Health Informatics,King Saud bin
Abdulaziz University for Health Sciences,Riyadh,SaudiArabia.
Received:23 October 2014 Accepted:6 June 2016
Asiri et al.BMC Nursing (2016) 15:38 Page 9 of 10
viding health care of the highest quality.
Conclusion
The main objective of this study was to test a conceptual
framework,relatingleadership stylesof managersto
nurses’perception ofempowermentand theirlevelof
commitment.The resultsof this study show thatthe
nurses surveyed reporta lower levelof AC relative to
NC and CC, suggesting that these nurses do not feela
strong sense of belongingor attachmentto their
organization.Leadership stylesand psychologicalem-
powerment significantly affect commitment levels.Other
factors being equal,the Transformational,Transactional
and Laissez-fairestylespositivelyaffectcommitment
levels,with the Transformational style having a marginal
effect.Similarly,the results revealthat autonomy is the
only component of the psychological empowerment con-
structthat significantly affectscommitmentlevels.Fi-
nally,the resultsrevealthat Arab nationaland North
American nurses report lower commitment levels in re-
lation to nurses of other nationalities.
Overallthe findingssuggestthat nursing leadersin
hospital acute settings can enhance the nursing work en-
vironmentby practicingappropriateleadership styles
and empowering strategies,including greater participa-
tion of nursing staff in the decision making process.Ul-
timately,more effectivenursingmanagementshould
resultin improved nursing staffretention,job satisfac-
tion,and work commitment.
Abbreviations
AC,Affective Commitment;ALOS,Average Length of HospitalStays;CC,
Continuance Commitment;CR,Contingent Reward;IAII,Idealized Influence
Attributed;IBII,Idealized Influence Behavior;IC,Individualized Consideration;
IM,InspirationalMotivation;IS,IntellectualStimulations;LFL,Laissez-Faire
Leadership;MBEA,Management-By-Exception-Active;MBEP,Management-By-
Exception-Passive;MLQ,Multifactor Leadership Questionnaire;NC,Normative
Commitment;NGAH,NationalGuard Health Affairs;OC,Organizational
Commitment;TAL,Transactional Leadership;TFL,Transformational Leadership
Acknowledgements
Thanks to King Saud bin Abdulaziz University for Health Sciences (KSAU-HS)
and the Department of Health System and Quality Management at College
of Public Health and Health informatics for their continuous support to make
this project successful.Specialthanks go to nurses working at King Abdulaziz
MedicalCity for their time and participation in this research project.
Funding
The authors would like to express their thanks and gratitude to King Abdullah
International Medical Research Center (KAIMRC) for providing the partial funds
for this project.
Availability of data and materials
Data supporting study findings are available upon request.
Authors’contributions
SA is the first author of this paper.She took the responsibilities for the conception
and design of the study.In addition,she was responsible for collecting,analyzing,
and interpreting the data.She also helped to compile the submitted article and
made the required modification.WR is the second author of this study.He
provided assistance and guidance in the design of the research and proposin
sufficient research concepts and strategies as well as approving the final ver
for this manuscript to be submitted.KA is the primary investigator of this study
and the correspondent author.He provided assistance in drafting and revising
the manuscript.He also helped to compile the submitted and approved the final
version for this manuscript to be submitted.OD is the fourth author of this study.
He provided assistance and guidance on the regression modeling,interpretation,
and analysis of the results.AA is the fifth author of this study.He provided
assistance and guidance in the statistical analysis as well as the interpretati
the results,and he also approved the final version for this manuscript to be
submitted.All authors read and approved the final version.
Authors’information
Samirah A.AsiriBSN.,MSc.Quality Improvement Specialist at the Department
of Continuous Quality Improvement and Patient Safety CQI&PS.Armed Forces
Hospitals,Southern Region of SaudiArabia (AFHSR).Email
asirisamirah@gmail.com
Rohrer,Wesley M.Ph.D.Assistant Professor,Vice Chair of Education and
Director MHA Program University of Pittsburgh,Graduate Schoolof Public
Health,Health Policy and Management.Emailwmrun@pitt.edu
Khaled Al-Surimi,PhD.Assistant Professor of Public Health and Health
Management at the Department of Health Systems and Quality Management
College of Public Health and Health Informatics,King Saud bin Abdulaziz
University for Health Sciences.Emailkalsurimi@gmail.com
Omar B.Da’ar.Ph.D.Assistant Professor of Health Economics & Financing at the
Department of Health Systems & Quality Management,College of Public
Health and Health Informatics,King Saud Bin Abdulaziz University for Health
Sciences.Emaildaaro@ksau-hs.edu.sa
Anwar Ahmed,Ph.D.Assistant Professor of Biostatistics at the Department of
Epidemiology and Biostatistics.College of Public Health and Health
Informatics.King Saud Bin Abdulaziz University for Health Sciences.Email
ahmedan@NGHA.MED.SA.
Competing interests
The authors declare no conflict of interest.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was reviewed by the research committee of the College of Public
Health and Health Informatics,King Saud bin Abdulaziz University for Health
Sciences,and King Abdullah MedicalResearch Center (KAIMRC) and was
granted institutionalreview board (IRB) approval,under research protocolNo
RR 13/029.According to the IRB protocol,an informed consent form was
attached to the front page of the study data collection tools to explain and
inform study participants about the study’s aims and methods and to assure
them that privacy and confidentiality of the data would be maintained.
Following an explanation of the study,nurses who agreed to participate in
the study completed the survey questionnaires anonymously and returned
them to the researcher in sealed envelopes.
Author details
1Department of Continuous Quality Management and Patient Safety,Armed
Forces Hospital,Dhahran,SaudiArabia.2Department of Health Policy and
Management,Program Graduate Schoolof Public Health,University of
Pittsburgh,Pittsburgh,USA.3Department of Health System and Quality
Management,College of Public Health and Health Informatics,King Saud bin
Abdulaziz University for Health Sciences,Riyadh,SaudiArabia.4Department
of Health System and Quality Management,College of Public Health and
Health Informatics;King Abdullah InternationalMedicalResearch Center,King
Saud bin Abdulaziz University for Health Sciences,Ministry of NationalGuard
Health Affairs,Riyadh,SaudiArabia.5Department of Epidemiology and
Biostatistics,College of Public Health and Health Informatics,King Saud bin
Abdulaziz University for Health Sciences,Riyadh,SaudiArabia.
Received:23 October 2014 Accepted:6 June 2016
Asiri et al.BMC Nursing (2016) 15:38 Page 9 of 10
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
References
1. Ammer S.Despite impending and relatively growth:Factors influencing the
expansion of nurses involvement in health profession.J Riyadh Trading.
2001;4176(74):46.
2. Laschinger H,Finegan J,Shamian J,Almost J.Testing Karasek’s demand-
controlmodelof restructures healthcare settings.J Nurs Adm.2001;31(5):
233–43.
3. Everson-Bates S.First-line managers in the expanded role.J Nurs Adm.
1992;22(3):32–7.
4. McNees-Smith D.The influence of manager behaviour on nurses’job
satisfaction.J Nurs Adm.1997;27(9):47–55.
5. Shamian J,Lightstone E.Hospitalrestructuring initiatives in Canada.Med
Care.1997;35(10):OS62–9.
6. Blythe J,Baumann A,GiovannettiP.Nurses’experience of restructuring in
three Ontriao hospitals.J Nurs Adm.2001;first quarter((67):67–74.
7. Tillman HJ,Salyer J,Corley MC.Environmentalturbulence:Staff nurse
perspectives.J Nurs Adm.1997;27(11):1522.
8. Corey-Lisle P,Tarzian AJ,Cohen MZ,Trinkeff AM.Heallhcare reform:Its
effects on nurses.J Nurs Adm.1999;29(3):30–7.
9. Burke R,Greenglass ER.Hospitalrestructuring,work-family conflict,and
Psychology burnout among nursing staff.PscholHealth.2001;16(5):583–94.
10. Avolio BJ,Bass BM.Multifactor Leadership Questionnaire:Manualand
sample Set.3rd ed.Redwood:Mind Garden;2004.
11. Spreitzer G.Psychologicalempowerment in the workplace:Dimensions,
measurement,and validation.Acad Manage J.1995;38(5):1142–465.
12. Allen N,Meyer N.Affective,continuance,and normative commitment to
the organization:an examination of construct validity.J VocationalBehav.
1996;29:252–76.
13. McNees-Smith D.Job satisfaction,productivity and organizational
commitment.The result of Leadership.J Nurs Adm.1995;25(9):17–26.
14. Dunham B,Grube A,Castaneda B.Organizationalcommitment:The utility
of an integrative definition.J ApplPsychol.1994;79(3):370–80.
15. Schwappach DL,Meyer MassettiC,Gehring K.Communication barriers in
counselling foreign-language patients in public pharmacies:threats to
patient safety? Int J Clin Pharm.2012;34(5):765–72.
16. Meyer J,Allen N.Commitment in the workplace.Thousand Oaks:Sage
Publisher;1997.
17. Wiener Y.Commitment in organizations:A normative view.Acad Manage
Rev.1982;7(3):418–28.
18. Avolio BJ,Bass BM,Jung DI.Re-examining the components of
transformationaland transactionalleadership using the multifactor
leadership questionnaire.J Occup Organ Psychol.1999;72(4):441–62.
19. Kelloway EK,Barling J.Knowledge work as organizationalbehavior.Int J
Manag Rev.2000;2(287):304.
20. Bass BM,Avoilio BJ,Jung DI,Berson Y.Predicting uint performance by
assessing transformationaland transactionalleadership.J ApplPsychol.
2003;88(2):207–18.
21. LibsekalJ. Nursing leadership styles and their impact on leadership
outcomes.Minnesota:ProQuest Information and Learning Company;2006.
22. Antonakis J,Avolio BJ,Sivasubramaniam N.Context and Leadership:An
examination of the nine factor full-range leadership theory using the
Multifactor Leadership Questionnaire.J Leadersh Q.2003;14(3):261–95.
23. NguniS,Sleegers P,Denessen E.Transformationaland transactional
leadership effects on teachers’job satisfaction,organizationalcommitment,
and organizationalcitizenship behavior in primary schools:The Tanzanian
case.SchoolEffectiveness SchoolImprov.2006;17(2):145–77.
24. Northouse P.Leadership:Theory and practice.4th ed.Thousands Oaks:
Sage;2007.
25. Northouse P.Leadership:Theory and practice.2nd ed.Thousands Oaks:
Sage;2001.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript at
www.biomedcentral.com/submit
Submit your next manuscript to BioMed Central
and we will help you at every step:
Asiri et al.BMC Nursing (2016) 15:38 Page 10 of 10
1. Ammer S.Despite impending and relatively growth:Factors influencing the
expansion of nurses involvement in health profession.J Riyadh Trading.
2001;4176(74):46.
2. Laschinger H,Finegan J,Shamian J,Almost J.Testing Karasek’s demand-
controlmodelof restructures healthcare settings.J Nurs Adm.2001;31(5):
233–43.
3. Everson-Bates S.First-line managers in the expanded role.J Nurs Adm.
1992;22(3):32–7.
4. McNees-Smith D.The influence of manager behaviour on nurses’job
satisfaction.J Nurs Adm.1997;27(9):47–55.
5. Shamian J,Lightstone E.Hospitalrestructuring initiatives in Canada.Med
Care.1997;35(10):OS62–9.
6. Blythe J,Baumann A,GiovannettiP.Nurses’experience of restructuring in
three Ontriao hospitals.J Nurs Adm.2001;first quarter((67):67–74.
7. Tillman HJ,Salyer J,Corley MC.Environmentalturbulence:Staff nurse
perspectives.J Nurs Adm.1997;27(11):1522.
8. Corey-Lisle P,Tarzian AJ,Cohen MZ,Trinkeff AM.Heallhcare reform:Its
effects on nurses.J Nurs Adm.1999;29(3):30–7.
9. Burke R,Greenglass ER.Hospitalrestructuring,work-family conflict,and
Psychology burnout among nursing staff.PscholHealth.2001;16(5):583–94.
10. Avolio BJ,Bass BM.Multifactor Leadership Questionnaire:Manualand
sample Set.3rd ed.Redwood:Mind Garden;2004.
11. Spreitzer G.Psychologicalempowerment in the workplace:Dimensions,
measurement,and validation.Acad Manage J.1995;38(5):1142–465.
12. Allen N,Meyer N.Affective,continuance,and normative commitment to
the organization:an examination of construct validity.J VocationalBehav.
1996;29:252–76.
13. McNees-Smith D.Job satisfaction,productivity and organizational
commitment.The result of Leadership.J Nurs Adm.1995;25(9):17–26.
14. Dunham B,Grube A,Castaneda B.Organizationalcommitment:The utility
of an integrative definition.J ApplPsychol.1994;79(3):370–80.
15. Schwappach DL,Meyer MassettiC,Gehring K.Communication barriers in
counselling foreign-language patients in public pharmacies:threats to
patient safety? Int J Clin Pharm.2012;34(5):765–72.
16. Meyer J,Allen N.Commitment in the workplace.Thousand Oaks:Sage
Publisher;1997.
17. Wiener Y.Commitment in organizations:A normative view.Acad Manage
Rev.1982;7(3):418–28.
18. Avolio BJ,Bass BM,Jung DI.Re-examining the components of
transformationaland transactionalleadership using the multifactor
leadership questionnaire.J Occup Organ Psychol.1999;72(4):441–62.
19. Kelloway EK,Barling J.Knowledge work as organizationalbehavior.Int J
Manag Rev.2000;2(287):304.
20. Bass BM,Avoilio BJ,Jung DI,Berson Y.Predicting uint performance by
assessing transformationaland transactionalleadership.J ApplPsychol.
2003;88(2):207–18.
21. LibsekalJ. Nursing leadership styles and their impact on leadership
outcomes.Minnesota:ProQuest Information and Learning Company;2006.
22. Antonakis J,Avolio BJ,Sivasubramaniam N.Context and Leadership:An
examination of the nine factor full-range leadership theory using the
Multifactor Leadership Questionnaire.J Leadersh Q.2003;14(3):261–95.
23. NguniS,Sleegers P,Denessen E.Transformationaland transactional
leadership effects on teachers’job satisfaction,organizationalcommitment,
and organizationalcitizenship behavior in primary schools:The Tanzanian
case.SchoolEffectiveness SchoolImprov.2006;17(2):145–77.
24. Northouse P.Leadership:Theory and practice.4th ed.Thousands Oaks:
Sage;2007.
25. Northouse P.Leadership:Theory and practice.2nd ed.Thousands Oaks:
Sage;2001.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript at
www.biomedcentral.com/submit
Submit your next manuscript to BioMed Central
and we will help you at every step:
Asiri et al.BMC Nursing (2016) 15:38 Page 10 of 10
1 out of 10