Assessment Task 1: Obesity in Low Socio-Economic Groups, HSH703
VerifiedAdded on 2023/01/18
|16
|3802
|81
Report
AI Summary
This report, prepared for the HSH703 unit, explores the significant health issue of obesity within low socio-economic groups, focusing on Australia's context. It begins by defining obesity and outlining its global and Australian prevalence, supported by statistical data from various sources. The report then delves into the specific challenges faced by low socio-economic groups, examining the interplay of lifestyle factors, psycho-socio-cultural determinants, and the Iceberg Model to understand the root causes of obesity within this population. Furthermore, the report analyzes the integration of health concerns into Municipal Public Health and Wellbeing Plans (MPHWP), particularly in the City of Whittlesea, and how these plans address the determinants of health. The report highlights the MPHWP's approaches to enhance healthier eating, promote active living, and improve mental health, providing a comprehensive overview of strategies to combat obesity and improve health outcomes for vulnerable populations. The report concludes by emphasizing the importance of a multifaceted approach to address obesity, considering the need for affordable housing, safe environments, and financial wellbeing to reduce stress and prevent obesity. The report uses various academic resources to support its findings.

ASSESMENT TASK 1
Assessment task 1
Obesity among low socio-economic groups
HSH703: Unit name
Unit chair: Name of unit chair
Author: Your name and ID
Date submitted: dd/mm/yy
Word count: 2435 words
Assessment task 1
Obesity among low socio-economic groups
HSH703: Unit name
Unit chair: Name of unit chair
Author: Your name and ID
Date submitted: dd/mm/yy
Word count: 2435 words
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
ASSESMENT TASK 2
Table of contents
Introduction…………………………………………………………………………………3
Obesity globally……………………………………………………………………………. 3
Obesity in Australia………………………………………………………………………... 5
Obesity among the low socio-economic status groups……………………………………. 7
Integration of MPHWP……………………………………………………………………. 9
Conclusion…………………………………………………………………………………. 11
References…………………………………………………………………………………..13
Table of contents
Introduction…………………………………………………………………………………3
Obesity globally……………………………………………………………………………. 3
Obesity in Australia………………………………………………………………………... 5
Obesity among the low socio-economic status groups……………………………………. 7
Integration of MPHWP……………………………………………………………………. 9
Conclusion…………………………………………………………………………………. 11
References…………………………………………………………………………………..13
ASSESMENT TASK 3
Introduction
Obesity can be described as an excessive accumulation of body fat presenting health
risks. It is measured by determining body mass index via body weight divided by the square
of body height. A body mass index greater or equal to thirty is defined as obesity. It is a
significant factor exposing the body to chronic conditions such as cancer, cardiovascular
diseases, and diabetes (Baum, 2002, pp. 356). Australia was established to be among the top
states with obesity. It is an epidemic with its frequency increasing over and over (Australian
Bureau of Statistics, “more than two thirds of Australians now overweight or obese” 2018).
The country has the third greatest pervasiveness of adults with overweight body mass indexes
(AIHW, 2017, pp. 40). In this, a plan aimed to note down wellbeing and health statuses of all
residents especially among low socio-economic status groups (World Health Organization,
“obesity”, 2019). The program is to ensure that the needs in terms of health for all societies
are addressed (ilonakickbusch, 2008, pp. 59).
Obesity globally
Obesity prevalence has been increasing gradually year after years with increased
consumption of foods dense in energy and with high-fat content. Also decreased physical
activity now that the need to engage in physical work has been gradually eliminated by
technology World Health Organization, “health promotion”, 2019) among many others. The
World Health Organization provides some estimated statistics that more than two billion
adults within ages eighteen and above in 2016 alone were overweight (Ilona, 2003, pp. 385).
Among the overweight ones, there were a rough six hundred and fifty million adults who had
obesity conditions. Among the two billion adults, thirty-nine percent of men and forty percent
of women were overweight. Among the six hundred and fifty million who were estimated to
Introduction
Obesity can be described as an excessive accumulation of body fat presenting health
risks. It is measured by determining body mass index via body weight divided by the square
of body height. A body mass index greater or equal to thirty is defined as obesity. It is a
significant factor exposing the body to chronic conditions such as cancer, cardiovascular
diseases, and diabetes (Baum, 2002, pp. 356). Australia was established to be among the top
states with obesity. It is an epidemic with its frequency increasing over and over (Australian
Bureau of Statistics, “more than two thirds of Australians now overweight or obese” 2018).
The country has the third greatest pervasiveness of adults with overweight body mass indexes
(AIHW, 2017, pp. 40). In this, a plan aimed to note down wellbeing and health statuses of all
residents especially among low socio-economic status groups (World Health Organization,
“obesity”, 2019). The program is to ensure that the needs in terms of health for all societies
are addressed (ilonakickbusch, 2008, pp. 59).
Obesity globally
Obesity prevalence has been increasing gradually year after years with increased
consumption of foods dense in energy and with high-fat content. Also decreased physical
activity now that the need to engage in physical work has been gradually eliminated by
technology World Health Organization, “health promotion”, 2019) among many others. The
World Health Organization provides some estimated statistics that more than two billion
adults within ages eighteen and above in 2016 alone were overweight (Ilona, 2003, pp. 385).
Among the overweight ones, there were a rough six hundred and fifty million adults who had
obesity conditions. Among the two billion adults, thirty-nine percent of men and forty percent
of women were overweight. Among the six hundred and fifty million who were estimated to
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
ASSESMENT TASK 4
have obesity, eleven percent were men, and fifteen percent were women. Between the years
1974 and 2016, obesity cases have tripled (World Health Organization, “obesity”, 2019).
Globally, children aged below five years estimated, to sum up to forty-one million
roughly had been diagnosed with either obesity or an overweight condition. Obesity was well
known to exist in high-income countries. However, the current state of affairs shows that the
middle-income countries are affected but even worse in acquiring the conditions are the low-
income countries (World Health Organization, “obesity and overweight”, 2015). Africa alone
recorded an appreciation of almost fifty percent of overweight children in ages five years and
below since the year 2000 (World Health Organization, “obesity and overweight”, 2015). In
Asia, more than three hundred and fifty million adolescents and children had been diagnosed
with obesity or overweight conditions in 2016 (WHO, 2016).
These statistics reveal an appreciating rate of pervasiveness concerning obesity and
underweight conditions among adolescents and children between ages five to nineteen. The
appreciation rates have changed from almost four percent in the 1970s to nineteen percent in
2016 affecting both boys and girls (WHO “obesity and overweight”, 2019). Eighteen percent
of girls had been diagnosed with either of the conditions whereas nineteen percent of boys
had been diagnosed with either of the conditions (WHO “obesity and overweight”, 2019). In
2016 however, more one hundred and twenty-four million were found to be obese. That is six
percent of girls and eight percent boys. Deaths reported from either obesity or overweight
conditions have occurred as a result of cardiovascular diseases, diabetic conditions or
resultant cancers (WHO, 2016).
Obesity in Australia
According to the United States Journal of Human Biology and Economics, Australia
records more significant effects of obesity among women between ages sixty to seventy-four
have obesity, eleven percent were men, and fifteen percent were women. Between the years
1974 and 2016, obesity cases have tripled (World Health Organization, “obesity”, 2019).
Globally, children aged below five years estimated, to sum up to forty-one million
roughly had been diagnosed with either obesity or an overweight condition. Obesity was well
known to exist in high-income countries. However, the current state of affairs shows that the
middle-income countries are affected but even worse in acquiring the conditions are the low-
income countries (World Health Organization, “obesity and overweight”, 2015). Africa alone
recorded an appreciation of almost fifty percent of overweight children in ages five years and
below since the year 2000 (World Health Organization, “obesity and overweight”, 2015). In
Asia, more than three hundred and fifty million adolescents and children had been diagnosed
with obesity or overweight conditions in 2016 (WHO, 2016).
These statistics reveal an appreciating rate of pervasiveness concerning obesity and
underweight conditions among adolescents and children between ages five to nineteen. The
appreciation rates have changed from almost four percent in the 1970s to nineteen percent in
2016 affecting both boys and girls (WHO “obesity and overweight”, 2019). Eighteen percent
of girls had been diagnosed with either of the conditions whereas nineteen percent of boys
had been diagnosed with either of the conditions (WHO “obesity and overweight”, 2019). In
2016 however, more one hundred and twenty-four million were found to be obese. That is six
percent of girls and eight percent boys. Deaths reported from either obesity or overweight
conditions have occurred as a result of cardiovascular diseases, diabetic conditions or
resultant cancers (WHO, 2016).
Obesity in Australia
According to the United States Journal of Human Biology and Economics, Australia
records more significant effects of obesity among women between ages sixty to seventy-four
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
ASSESMENT TASK 5
and for men with ages above seventy-five (ABS “National Health Survey: key results”,
2018). The Australian Bureau of Statistics conducted a study in 2005, and the results were
astonishing. The obesity rate between the years 2004 and 2005 had risen by 2.5 million. That
is from a population of five million for the years 1989 to 1990, six million for the year 1995,
seven million for the year 2001 lastly, 7.5 million for the years 2004 to 2005. Additionally,
the World Health Organization determined that in the year 2007, roughly 67.4 percent of
adults living in Australia was diagnosed with the overweight condition ranking third among
the primary English speaking nations and twenty-first globally. In 2005, the World Health
Organization determined that more than twenty percent of adults in Australia had an obesity
condition. The rates have then significantly changed to nearly twenty-eight percent for the
year 2010 (WHO, 2013). National Health survey for the year 2005 revealed that almost fifty-
four percent of Australians were found to be overweight and eighteen percent of these were
diagnosed with obesity. In 2016, some astonishing numbers were then established. The
percentages had risen to sixty-five percent of Australians being overweight and twenty-nine
percent being obese.
In 2017, statistics revealed that thirty percent of Australians (adults, kids, and
adolescents) were found to have obesity conditions (ABS, 2017). The figures show a near
double from the numbers recorded in years 1995, that is roughly ten percent of Australians
were obese and twenty-eight percent of them were overweight) from which there were cases
where individuals did not give the actual height and weight measures which the two primary
measurements used to determine the body mass index. Victoria from the report showed a low
obesity prevalence clocking at seventeen percent of the total population. Australia according
to the Organization for Economic Co-operation and Development in 2013, had been
identified to be the third in obesity rates among selected Organization for Economic Co-
operation and Development countries (“obesity and overweight”, 2015).
and for men with ages above seventy-five (ABS “National Health Survey: key results”,
2018). The Australian Bureau of Statistics conducted a study in 2005, and the results were
astonishing. The obesity rate between the years 2004 and 2005 had risen by 2.5 million. That
is from a population of five million for the years 1989 to 1990, six million for the year 1995,
seven million for the year 2001 lastly, 7.5 million for the years 2004 to 2005. Additionally,
the World Health Organization determined that in the year 2007, roughly 67.4 percent of
adults living in Australia was diagnosed with the overweight condition ranking third among
the primary English speaking nations and twenty-first globally. In 2005, the World Health
Organization determined that more than twenty percent of adults in Australia had an obesity
condition. The rates have then significantly changed to nearly twenty-eight percent for the
year 2010 (WHO, 2013). National Health survey for the year 2005 revealed that almost fifty-
four percent of Australians were found to be overweight and eighteen percent of these were
diagnosed with obesity. In 2016, some astonishing numbers were then established. The
percentages had risen to sixty-five percent of Australians being overweight and twenty-nine
percent being obese.
In 2017, statistics revealed that thirty percent of Australians (adults, kids, and
adolescents) were found to have obesity conditions (ABS, 2017). The figures show a near
double from the numbers recorded in years 1995, that is roughly ten percent of Australians
were obese and twenty-eight percent of them were overweight) from which there were cases
where individuals did not give the actual height and weight measures which the two primary
measurements used to determine the body mass index. Victoria from the report showed a low
obesity prevalence clocking at seventeen percent of the total population. Australia according
to the Organization for Economic Co-operation and Development in 2013, had been
identified to be the third in obesity rates among selected Organization for Economic Co-
operation and Development countries (“obesity and overweight”, 2015).
ASSESMENT TASK 6
The southern regions of Australia were distinguishable with prevalence rates of
roughly twenty percent (“National Health Survey: key results”, 2018). Sixty-one percent of
adults were diagnosed with either obesity or overweight conditions (“more than two thirds of
Australians now overweight or obese”, 2018). Among these, sixty-seven percent of the male
gender along with fifty-five percent of females had been determined to be obese or
overweight. Adults identified to be obese were twenty-six percent whereas thirty-five percent
were overweight (AIHW, 2017, pp. 40). Individuals found to have obesity conditions
between ages eighteen to twenty-four were twelve percent and adults aging fifty-five years to
sixty-four years diagnosed with either obesity or overweight conditions clocked at thirty-five
percent according to The Australian Bureau of Statistics in 2011 (ABS, 2011).
The southern regions of Australia were distinguishable with prevalence rates of
roughly twenty percent (“National Health Survey: key results”, 2018). Sixty-one percent of
adults were diagnosed with either obesity or overweight conditions (“more than two thirds of
Australians now overweight or obese”, 2018). Among these, sixty-seven percent of the male
gender along with fifty-five percent of females had been determined to be obese or
overweight. Adults identified to be obese were twenty-six percent whereas thirty-five percent
were overweight (AIHW, 2017, pp. 40). Individuals found to have obesity conditions
between ages eighteen to twenty-four were twelve percent and adults aging fifty-five years to
sixty-four years diagnosed with either obesity or overweight conditions clocked at thirty-five
percent according to The Australian Bureau of Statistics in 2011 (ABS, 2011).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
ASSESMENT TASK 7
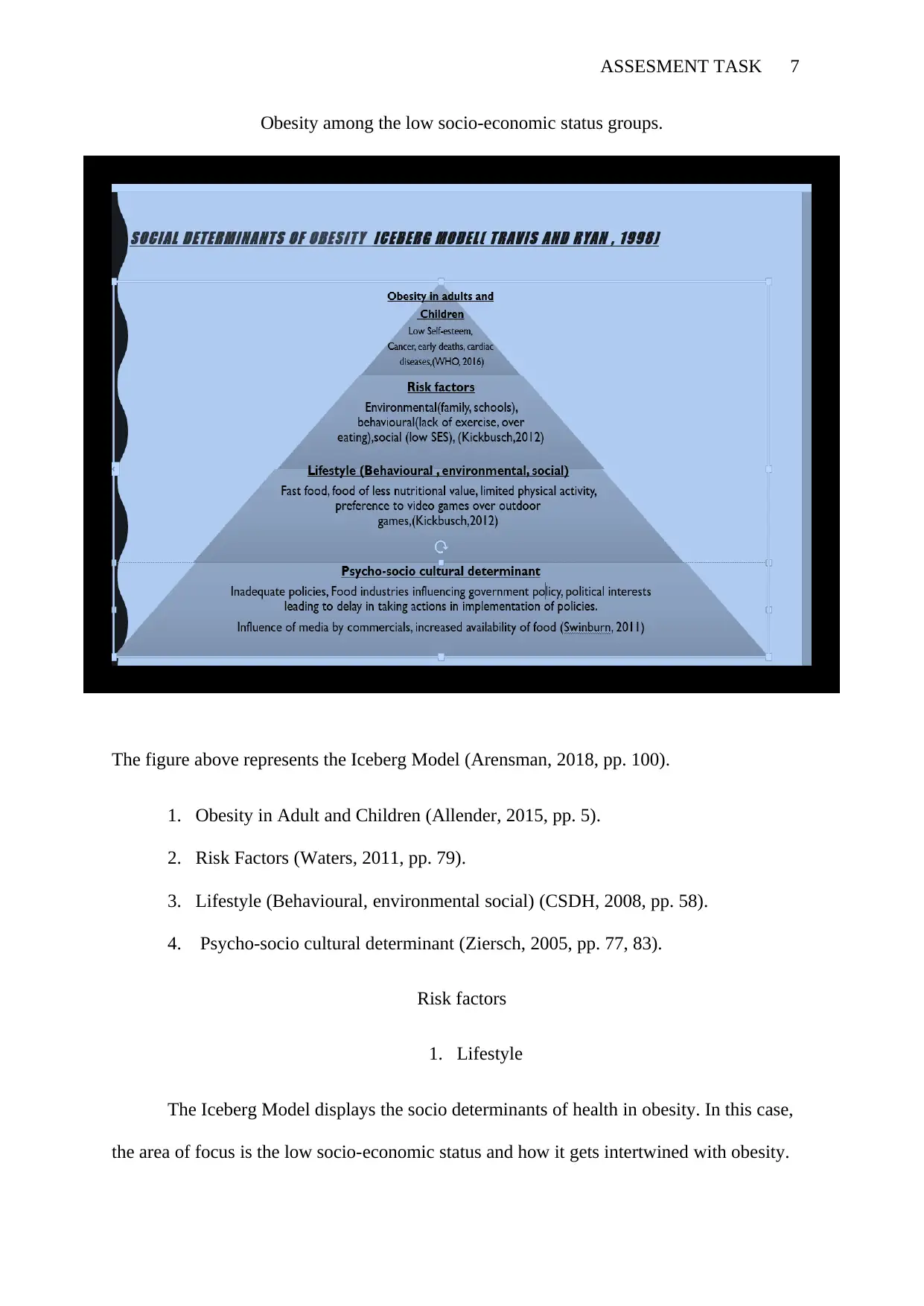
Obesity among the low socio-economic status groups.
The figure above represents the Iceberg Model (Arensman, 2018, pp. 100).
1. Obesity in Adult and Children (Allender, 2015, pp. 5).
2. Risk Factors (Waters, 2011, pp. 79).
3. Lifestyle (Behavioural, environmental social) (CSDH, 2008, pp. 58).
4. Psycho-socio cultural determinant (Ziersch, 2005, pp. 77, 83).
Risk factors
1. Lifestyle
The Iceberg Model displays the socio determinants of health in obesity. In this case,
the area of focus is the low socio-economic status and how it gets intertwined with obesity.
Obesity among the low socio-economic status groups.
The figure above represents the Iceberg Model (Arensman, 2018, pp. 100).
1. Obesity in Adult and Children (Allender, 2015, pp. 5).
2. Risk Factors (Waters, 2011, pp. 79).
3. Lifestyle (Behavioural, environmental social) (CSDH, 2008, pp. 58).
4. Psycho-socio cultural determinant (Ziersch, 2005, pp. 77, 83).
Risk factors
1. Lifestyle
The Iceberg Model displays the socio determinants of health in obesity. In this case,
the area of focus is the low socio-economic status and how it gets intertwined with obesity.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
ASSESMENT TASK 8
Despite the universal pervasiveness rates for obesity increasing by almost double over the
years from 1974 to 2013, prevalent obesity rates in middle-income countries and low-income
countries have been noted to be more significant than those in high-income countries
(ctgreport.pmc.gov.au, 2019, PP. 122). Technology and industrialization have resulted in
transitions in lifestyle, and many low-income and middle-income countries have had the
benefits of an increased life expectancy. Nonetheless, the same changes have led to an
increase in the uptake of high-calorie diets as well as high-fat foods.
2. Psycho-socio cultural determinant
The same has also resulted in decreasing in physical activity reflecting what was seen
in the high-income countries some time back. This has led to attention shifting to focus on the
vitality of social inequities concerning body health (Baum, 2010, pp. 320). Obesity has been
seen to get a hold in crucial moments such as in the transition period from childhood to
adolescence (Allender, 2015, pp. 8). This brings in the importance of understanding what role
a low socio-economic status as a psycho-socio cultural determinant plays in the obesity
pervasiveness rates in the human body and social life.
Focusing on the above, it can be established that a significant direct and indirect
impact of socioeconomic status reflects on the body mass index through stress
psychologically resulting in increased emotional eating. This proves the relationship that
exists between low socioeconomic status and obesity. Individuals from the low-income
countries as well as middle-income countries experience a substantial amount of
psychological distress either due to financial matters such as a significant budget countered
with a low-income source, lack of basic needs among others (Baum, 2005, pp. 79). The
distress then results in the individuals obtaining a coping stratagem which involves increased
Despite the universal pervasiveness rates for obesity increasing by almost double over the
years from 1974 to 2013, prevalent obesity rates in middle-income countries and low-income
countries have been noted to be more significant than those in high-income countries
(ctgreport.pmc.gov.au, 2019, PP. 122). Technology and industrialization have resulted in
transitions in lifestyle, and many low-income and middle-income countries have had the
benefits of an increased life expectancy. Nonetheless, the same changes have led to an
increase in the uptake of high-calorie diets as well as high-fat foods.
2. Psycho-socio cultural determinant
The same has also resulted in decreasing in physical activity reflecting what was seen
in the high-income countries some time back. This has led to attention shifting to focus on the
vitality of social inequities concerning body health (Baum, 2010, pp. 320). Obesity has been
seen to get a hold in crucial moments such as in the transition period from childhood to
adolescence (Allender, 2015, pp. 8). This brings in the importance of understanding what role
a low socio-economic status as a psycho-socio cultural determinant plays in the obesity
pervasiveness rates in the human body and social life.
Focusing on the above, it can be established that a significant direct and indirect
impact of socioeconomic status reflects on the body mass index through stress
psychologically resulting in increased emotional eating. This proves the relationship that
exists between low socioeconomic status and obesity. Individuals from the low-income
countries as well as middle-income countries experience a substantial amount of
psychological distress either due to financial matters such as a significant budget countered
with a low-income source, lack of basic needs among others (Baum, 2005, pp. 79). The
distress then results in the individuals obtaining a coping stratagem which involves increased
ASSESMENT TASK 9
emotional eating which leads to overweight conditions as they gradually transform to obesity
(Waters, 2011, pp. 79).
Integration of MPHWP
Integrating health concerns in an MPHWP means that healthcare is everybody's
business, not just an agenda upheld by health planners. Integration gets everyone thinking of
how the community's healthcare can be improved. In this case, obesity is addressed above
features in the low socio-economic status. It has been integrated into policy and planning
contexts. The first field of obesity has been discussed is in the mandate to enhance healthier
eating as well as enhance active living; additionally, improving mental health has been
addressed at a state level (Breton, 2010, pp. 87).
Furthermore, it has been discussed in regional prevention planning partnerships. The
approach emphasizes local needs as well as local priorities. Thirdly, health and human
services planning have integrated obesity by addressing appropriate infrastructure and
services. Additionally, community demographics have combined the rising concern on
obesity with regards to psychological distress based on financial matters. The wellbeing has
noticed increased obesity rates, physical inactivity, reduced food consumption, food
insecurity which are all interlinked to obesity among the low socioeconomic statuses
(Sturmberg, 2014, pp. 72).
Determinants.
The MPHWP addresses the determining factors in several ways. First, in the
continued areas for a health planning section, the plan seeks to establish appropriate and
affordable housing. Affordability based on housing results to better living affordability and
better financial well-being. This along with lowered transport costs as well as reduced energy
emotional eating which leads to overweight conditions as they gradually transform to obesity
(Waters, 2011, pp. 79).
Integration of MPHWP
Integrating health concerns in an MPHWP means that healthcare is everybody's
business, not just an agenda upheld by health planners. Integration gets everyone thinking of
how the community's healthcare can be improved. In this case, obesity is addressed above
features in the low socio-economic status. It has been integrated into policy and planning
contexts. The first field of obesity has been discussed is in the mandate to enhance healthier
eating as well as enhance active living; additionally, improving mental health has been
addressed at a state level (Breton, 2010, pp. 87).
Furthermore, it has been discussed in regional prevention planning partnerships. The
approach emphasizes local needs as well as local priorities. Thirdly, health and human
services planning have integrated obesity by addressing appropriate infrastructure and
services. Additionally, community demographics have combined the rising concern on
obesity with regards to psychological distress based on financial matters. The wellbeing has
noticed increased obesity rates, physical inactivity, reduced food consumption, food
insecurity which are all interlinked to obesity among the low socioeconomic statuses
(Sturmberg, 2014, pp. 72).
Determinants.
The MPHWP addresses the determining factors in several ways. First, in the
continued areas for a health planning section, the plan seeks to establish appropriate and
affordable housing. Affordability based on housing results to better living affordability and
better financial well-being. This along with lowered transport costs as well as reduced energy
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
ASSESMENT TASK 10
costs as well as a low price for basic utilities will allow individuals from the low-income
class as well as middle-income class to have decreased distress levels avoiding, therefore,
preventing obesity (whittlesea.vic.gov.au, 2017, pp. 9-14). Also, focus area one discussed in
the plan addresses creating a safe and welcoming surrounding. The outcomes from the
implementation will result in a long term depreciating psychological distress and depression
which are risk factors attributing to obesity (Kickbusch I. Healthy societies, 2008, pp. 59).
Additionally, implementing safe and sustainable travel means which lies under focus
area two will address obesity not only among low socio-economic statuses but among all
groups of individuals (Swinburn, 2007, pp. 306). The outcome of implementing the plan
concerning safe travel means will be an appreciating number of individuals engaging in
active transport modes such as walking and cycling (Morley, 2016, pp. 129) These will allow
individuals to engage in physical activity. Increased physical activity decrease in obesity
prevalence rates (AIHW, 2017, pp. 40). Focus area three addresses increased employment
and financial well-being. The outcomes for implementing the plan concerning focus area
three will be appreciating affordable, appropriate and accessible housing
(whittlesea.vic.gov.au, 2017, pp. 31).
Financial stress results in pain resulting in obesity, but the program will offer
economic well-being, therefore, reduced distress (CSDH, 2008, pp. 68). The fourth focus area
addresses the facilitation of available green open space all through the lifetime of any person.
The outcomes of implementing the plan with regards to focus area four will mean an
achieved long term physical activity. That is for adults, children, and adolescents. Secondly,
it will result in an improvement in physical health (Australian Government, “closing the
gap”, 2019). The results for this will be diminished cases of cardiovascular diseases and
decreased cases of blood pressure as well as diabetic conditions. Thirdly, it will result in an
improvement in mental health which will lead to diminished depression and depreciating
costs as well as a low price for basic utilities will allow individuals from the low-income
class as well as middle-income class to have decreased distress levels avoiding, therefore,
preventing obesity (whittlesea.vic.gov.au, 2017, pp. 9-14). Also, focus area one discussed in
the plan addresses creating a safe and welcoming surrounding. The outcomes from the
implementation will result in a long term depreciating psychological distress and depression
which are risk factors attributing to obesity (Kickbusch I. Healthy societies, 2008, pp. 59).
Additionally, implementing safe and sustainable travel means which lies under focus
area two will address obesity not only among low socio-economic statuses but among all
groups of individuals (Swinburn, 2007, pp. 306). The outcome of implementing the plan
concerning safe travel means will be an appreciating number of individuals engaging in
active transport modes such as walking and cycling (Morley, 2016, pp. 129) These will allow
individuals to engage in physical activity. Increased physical activity decrease in obesity
prevalence rates (AIHW, 2017, pp. 40). Focus area three addresses increased employment
and financial well-being. The outcomes for implementing the plan concerning focus area
three will be appreciating affordable, appropriate and accessible housing
(whittlesea.vic.gov.au, 2017, pp. 31).
Financial stress results in pain resulting in obesity, but the program will offer
economic well-being, therefore, reduced distress (CSDH, 2008, pp. 68). The fourth focus area
addresses the facilitation of available green open space all through the lifetime of any person.
The outcomes of implementing the plan with regards to focus area four will mean an
achieved long term physical activity. That is for adults, children, and adolescents. Secondly,
it will result in an improvement in physical health (Australian Government, “closing the
gap”, 2019). The results for this will be diminished cases of cardiovascular diseases and
decreased cases of blood pressure as well as diabetic conditions. Thirdly, it will result in an
improvement in mental health which will lead to diminished depression and depreciating
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
ASSESMENT TASK 11
psychological distress (WHO Global Health Promotion Conferences ,“Health promotion”,
2019).
Lastly, at a community level, the members will enjoy an increased social cohesion.
Risk factors such as physical inactivity and physical distress were seen to cause obesity
prevalence for middle and low-income earners who are the sources to the majority of the low
socio-economic status groups (Lfe, 2013, pp. 62). The plan has fully solved these concerns
and has even offered other means to reduce obesity among other groups apart from one part.
Cycling and walking more (City of Whittlesea, “HEALTH AND WELLBEING
PARTNERSHIP PLAN”, 2017) will mean lateness to work causing cases of firing among
many so the distress will somehow still exist. The plan would also suggest that the council
engages in all developments without involving the private sector. Participating in a
partnership where the investors have to be persuaded to invest in a lowly returning business
would seem quite impossible.
Conclusion
As seen above, obesity is evolving to get to the low-income and middle-income
countries contrary to what many would expect. It will continue to root itself among them
because is that population will increase amidst a gradually decreasing quantity of natural
resources. This will mean that investors will have to go a mile farther to come up with ways
of sustaining the countries resulting in the people digging deeper into their pockets to pay up
for services. Employers will also keep off taking in more staff because cash inflow will be
deficient with more resources going into finding new resources.
A financial strain will continue to exist, and the results will always be psychological
distress which will result in obesity prevalence (Patrick R, 2011, pp. 58). The plan, in this
case, suggests a way to make the cost of living cheaper reducing psychological distress
psychological distress (WHO Global Health Promotion Conferences ,“Health promotion”,
2019).
Lastly, at a community level, the members will enjoy an increased social cohesion.
Risk factors such as physical inactivity and physical distress were seen to cause obesity
prevalence for middle and low-income earners who are the sources to the majority of the low
socio-economic status groups (Lfe, 2013, pp. 62). The plan has fully solved these concerns
and has even offered other means to reduce obesity among other groups apart from one part.
Cycling and walking more (City of Whittlesea, “HEALTH AND WELLBEING
PARTNERSHIP PLAN”, 2017) will mean lateness to work causing cases of firing among
many so the distress will somehow still exist. The plan would also suggest that the council
engages in all developments without involving the private sector. Participating in a
partnership where the investors have to be persuaded to invest in a lowly returning business
would seem quite impossible.
Conclusion
As seen above, obesity is evolving to get to the low-income and middle-income
countries contrary to what many would expect. It will continue to root itself among them
because is that population will increase amidst a gradually decreasing quantity of natural
resources. This will mean that investors will have to go a mile farther to come up with ways
of sustaining the countries resulting in the people digging deeper into their pockets to pay up
for services. Employers will also keep off taking in more staff because cash inflow will be
deficient with more resources going into finding new resources.
A financial strain will continue to exist, and the results will always be psychological
distress which will result in obesity prevalence (Patrick R, 2011, pp. 58). The plan, in this
case, suggests a way to make the cost of living cheaper reducing psychological distress

ASSESMENT TASK 12
which, in turn, minimize obesity prevalence rates. Physical activity has also been enhanced
diminishing obesity prevalence but remains quite inefficient concerning factors such as work
time and emergency need for a faster transport means.
which, in turn, minimize obesity prevalence rates. Physical activity has also been enhanced
diminishing obesity prevalence but remains quite inefficient concerning factors such as work
time and emergency need for a faster transport means.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 16