Case Study: Analysis of Systolic Heart Failure in HV3 Assessment
VerifiedAdded on 2022/09/27
|8
|2025
|23
Case Study
AI Summary
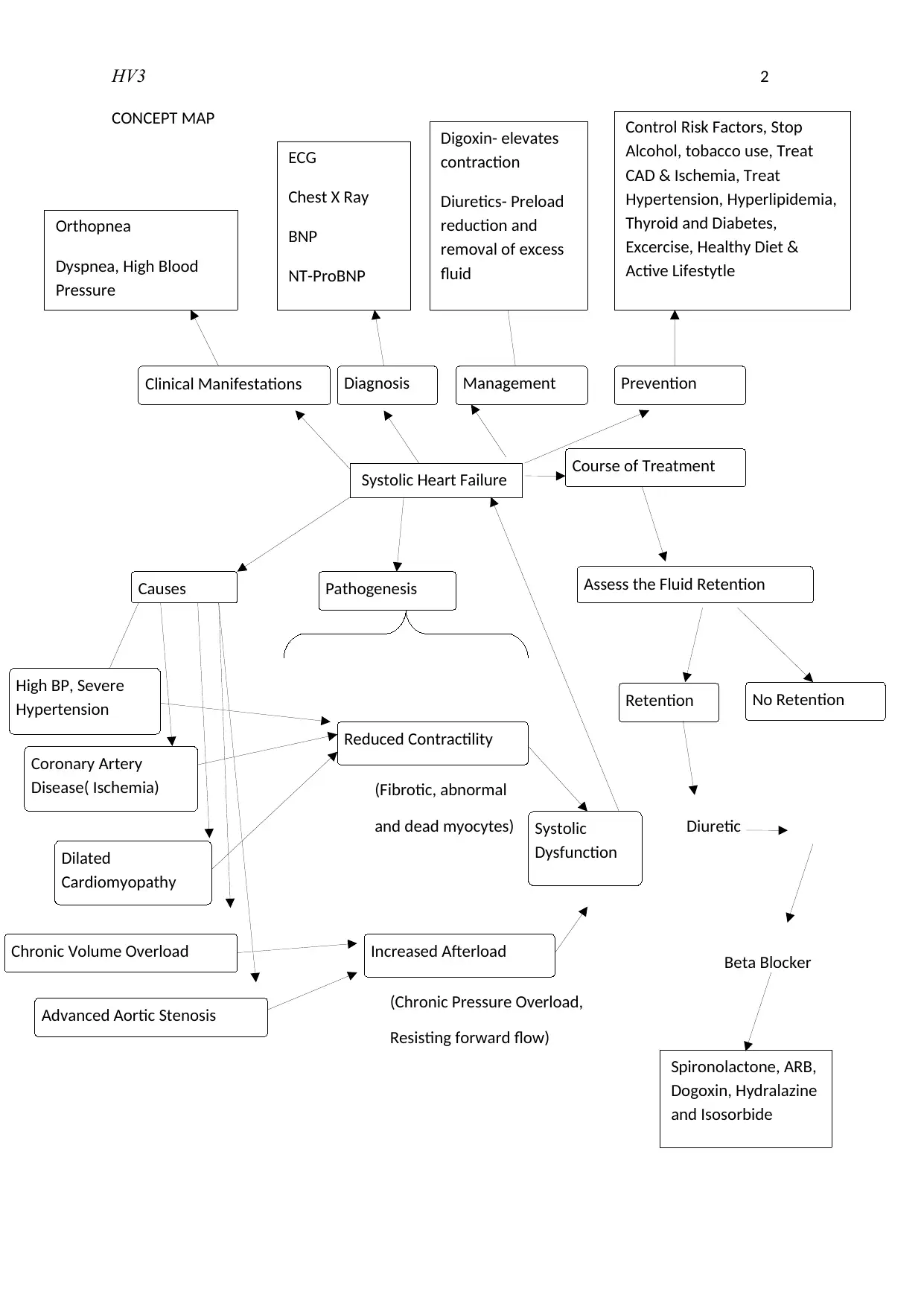
This assignment presents a case study on a patient experiencing systolic heart failure. It explores the pathogenesis of the condition, detailing how reduced cardiac function and external factors impact oxygen utilization in muscle cells. The case study analyzes the patient's clinical manifestations, including dyspnea, tachycardia, and low oxygen saturation, linking them to underlying conditions like hypertension and atrial fibrillation. The document also covers two crucial nursing strategies: regular monitoring of vital signs and exercise training, highlighting their role in managing the patient's condition. Furthermore, it explains the mechanism of action of two key medications, IV Furosemide and Sublingual Glyceryl Trinitrate, in treating heart failure symptoms. The document concludes with a comprehensive list of references supporting the analysis and recommendations.


1 out of 8
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.