A Study of Premature Menopause Among Urban Women in Sydney, Australia
VerifiedAdded on 2021/06/16
|27
|6244
|39
Report
AI Summary
This research proposal outlines a study investigating premature menopause among urban women aged 30-45 in the Great Western Sydney region of Australia. The study aims to address the research problem of early or premature menopause, focusing on causes, contributory factors, symptoms, and potential treatments, with the goal of bridging knowledge gaps and informing policy makers. The proposal reviews existing literature on premature menopause, including its causes (genetic disorders, autoimmune diseases, infections, etc.), clinical features, and consequences. It poses specific research questions regarding the relationship between puberty delays and early menopause, the impact of natural and induced causes, the effectiveness of treatments like oocyte donation and hormone replacement therapy, and the consistency of signs and symptoms. The research will identify women aged 30-45 and explore the factors, signs, symptoms, and interventions associated with premature menopause, including ethnicity and age. This research seeks to contribute valuable insights into this critical women's health issue.
Assignment 2 – Research Proposal, 2018
Student name: Student ID:
Title
STUDY OF PREMATURE MENOPAUSE AMONG URBAN WOMEN AGED 30 TO 45
YEARS IN GREAT WESTERN SYDNEY REGION, AUSTRALIA
Research problem
Early or premature menopause among women has been of major concern. The causes,
contributory factors, symptoms and treatment have not been well understood by most
premenopausal women who would otherwise bear children at that age (Moen, M, 2010).
The motivation in this premenopausal women study is to bridge the gap of knowledge on
what causes premature menopause, symptoms, social factors and how it can be prevented
or treated. This will go a long way to help planners and policy makers to have substantial
information about premature menopause.
What is already known
Premature menopause is a condition whereby women below 40 years stop receiving
Student name: Student ID:
Title
STUDY OF PREMATURE MENOPAUSE AMONG URBAN WOMEN AGED 30 TO 45
YEARS IN GREAT WESTERN SYDNEY REGION, AUSTRALIA
Research problem
Early or premature menopause among women has been of major concern. The causes,
contributory factors, symptoms and treatment have not been well understood by most
premenopausal women who would otherwise bear children at that age (Moen, M, 2010).
The motivation in this premenopausal women study is to bridge the gap of knowledge on
what causes premature menopause, symptoms, social factors and how it can be prevented
or treated. This will go a long way to help planners and policy makers to have substantial
information about premature menopause.
What is already known
Premature menopause is a condition whereby women below 40 years stop receiving
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
menstrual periods and hence lose fertility. Onset of premature menopause is presented with
amenorrhea, rise in gonadotrophic levels and oestrogen deficiency. Menopause can happen
in two ways it can be natural or induced that is through chemotherapy or surgical
oophorectomy (Faddy, M, 2016).
According to Okeke, et al, premature menopausal is a condition that affects about 1% of
women below 40 years. It presents itself in primary and secondary amenorrhea whereby
primary amenorrhea takes about 10-28% and secondary amenorrhea takes 4-18 %. This
shows that primary amenorrhea takes a large percentage of premature menopause due to
problems in development. Development problems occur when there is ovarian failure,
uterine absence and puberty delays. Secondary amenorrhea occurs due to disturbances in
hormone and formation of a scar inside the uterine. Although causes of premature
menopause have not been established but what causes the condition can be established. The
article gives causes including: genetic disorders, smoking, autoimmune diseases,
infections, iatrogenic, surgery, drugs and pathophysiology. Genetic disorders cause
premature menopause through dysgenesis of the ovary and sex chromosomes
abnormalities. Dysgenesis of the ovary accounts to 30% of all cases, this is because that is
where the actual menstrual cycle happens. Alteration in chromosomes due to abnormalities
accounts for 10-20% of all cases whereby X sex chromosomes is involved (Okeke, T,
2013). The article by Okeke highlights the common chromosomal abnormalities that may
mark onset of premature menopause including: pure gonadal dysgenesis , Turners
Syndrome, familial and trisomy 13 and trisomy 18. Cases whereby there is genetic
alteration of metabolism factors to cause 17 alpha-hydroxylase deficiencies, galactosaemia
and myotonic dystrophy can contribute to the condition. Genetics can also cause alteration
amenorrhea, rise in gonadotrophic levels and oestrogen deficiency. Menopause can happen
in two ways it can be natural or induced that is through chemotherapy or surgical
oophorectomy (Faddy, M, 2016).
According to Okeke, et al, premature menopausal is a condition that affects about 1% of
women below 40 years. It presents itself in primary and secondary amenorrhea whereby
primary amenorrhea takes about 10-28% and secondary amenorrhea takes 4-18 %. This
shows that primary amenorrhea takes a large percentage of premature menopause due to
problems in development. Development problems occur when there is ovarian failure,
uterine absence and puberty delays. Secondary amenorrhea occurs due to disturbances in
hormone and formation of a scar inside the uterine. Although causes of premature
menopause have not been established but what causes the condition can be established. The
article gives causes including: genetic disorders, smoking, autoimmune diseases,
infections, iatrogenic, surgery, drugs and pathophysiology. Genetic disorders cause
premature menopause through dysgenesis of the ovary and sex chromosomes
abnormalities. Dysgenesis of the ovary accounts to 30% of all cases, this is because that is
where the actual menstrual cycle happens. Alteration in chromosomes due to abnormalities
accounts for 10-20% of all cases whereby X sex chromosomes is involved (Okeke, T,
2013). The article by Okeke highlights the common chromosomal abnormalities that may
mark onset of premature menopause including: pure gonadal dysgenesis , Turners
Syndrome, familial and trisomy 13 and trisomy 18. Cases whereby there is genetic
alteration of metabolism factors to cause 17 alpha-hydroxylase deficiencies, galactosaemia
and myotonic dystrophy can contribute to the condition. Genetics can also cause alteration
to the immune system as to cause mucocutaneous fungal infections, Ataxia telangiectasia
and Di George syndrome this can also contribute to the condition (Okeke, T, 2013).
Autoimmune diseases account 30-60% of cases which present itself through thyroid
diseases, mumps, hyperparathyroidism, adrenal insufficiency and Addison’s diseases. This
shows follicle infiltration with plasma cells and lymphocytes as seen through ovarian
biopsy. Infections like mumps have contributed to premature menopause; mumps presents
itself best during fetal and pubertal periods this can lead to failure of the ovary.3% of some
premature menstruation cases is caused by pelvic tuberculosis this leads to synechiae of the
intrauterine and endometrium destruction. Smoking cases premature menopause through
polycyclic hydrocarbon contained in cigarette smoke. Radiation can also cause premature
menopause through radiations and chemotherapy. Irradiation of megavoltage of about
4500-5000 radiations cause failure in the ovary and also lose dose radiation through
domestic microwave appliances. Chemotherapeutic agents like alkylating agents,
actimomycin, methotrexate, 6 mercaptopurine and Adriamycin can induce ovarian organ
failure. Surgery can also cause premature menopause this is though bilateral oophorectomy
to prevent ovarian cancer and also hysterectomy interferes with ovarian blood supply and
functional endocrine contribution between uterus and ovary. Surgery alone accounts for
15-50% of cases. In some aspect of premature menopause cases of ovarian suppression and
failure can be seen especially by drugs like alkylating agents. Clinical features that has
identified premature menopause include: vaginal dryness and dyspareunia, urinary tract
one can feel frequency, urgency, incontinence and atrophic cystitis. Other symptoms that
mark premature menopause comprise: headache, cancer phobia, anxiety, hot flushes,
irritability, night sweats, depression, irritability, skin atrophy, joint pains and inability to
and Di George syndrome this can also contribute to the condition (Okeke, T, 2013).
Autoimmune diseases account 30-60% of cases which present itself through thyroid
diseases, mumps, hyperparathyroidism, adrenal insufficiency and Addison’s diseases. This
shows follicle infiltration with plasma cells and lymphocytes as seen through ovarian
biopsy. Infections like mumps have contributed to premature menopause; mumps presents
itself best during fetal and pubertal periods this can lead to failure of the ovary.3% of some
premature menstruation cases is caused by pelvic tuberculosis this leads to synechiae of the
intrauterine and endometrium destruction. Smoking cases premature menopause through
polycyclic hydrocarbon contained in cigarette smoke. Radiation can also cause premature
menopause through radiations and chemotherapy. Irradiation of megavoltage of about
4500-5000 radiations cause failure in the ovary and also lose dose radiation through
domestic microwave appliances. Chemotherapeutic agents like alkylating agents,
actimomycin, methotrexate, 6 mercaptopurine and Adriamycin can induce ovarian organ
failure. Surgery can also cause premature menopause this is though bilateral oophorectomy
to prevent ovarian cancer and also hysterectomy interferes with ovarian blood supply and
functional endocrine contribution between uterus and ovary. Surgery alone accounts for
15-50% of cases. In some aspect of premature menopause cases of ovarian suppression and
failure can be seen especially by drugs like alkylating agents. Clinical features that has
identified premature menopause include: vaginal dryness and dyspareunia, urinary tract
one can feel frequency, urgency, incontinence and atrophic cystitis. Other symptoms that
mark premature menopause comprise: headache, cancer phobia, anxiety, hot flushes,
irritability, night sweats, depression, irritability, skin atrophy, joint pains and inability to
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
concentrate (Okeke, T, 2013).
According to Australian menopause society, information sheet, they look at early
menopause from perspectives of premature and unexpected ovarian failure. The result of
ovarian failure leads to a number of consequences. When the ovary stops to work in the
body they stop producing eggs and producing secondary female hormones namely
oestrogen and progesterone. This leads to loss of bearing capacity in many women. Failure
to produce hormones leads to stop of menstrual periods (Maclennan, A 2017). The
deficient oestrogen cause hot flushes, mood change due to hormonal imbalance,
disturbances when someone is sleeping, lead to stops of production of vaginal fluids
resulting to dry vagina. Cases whereby a woman has had premature menopause emotional
turmoil may set in. This is clearly seen whereby a woman feeling sad, jealous other
women’s pregnancies. The article proceeds to give the long-term consequences of
premature menopause which are osteoporosis which speeds up the arteries hardening. The
hardening of arteries may predispose someone to heart attack or stroke.
According to guideline of the Europe society of human reproduction and embryology they
give a clear outline on how to manage women with premature ovarian insufficiency. This
spells out good news on how to manage premature menopause. The article gives some
interventions that can be done case of loss of fertility this include: oocyte donation is one
of the best fertility interventions (Luborsky, J, 2013). Cases whereby there is bone loss,
women are advised to take a balanced diet to ensure sufficient intake of calcium and
vitamin D. The article cites oestrogen replacement to prevent osteoporosis and this help
maintain bones. Additionally, women may consider taking a combined oral contraceptive if
deemed appropriate. The article proceeds to tackle the issue of cardiovascular health in
According to Australian menopause society, information sheet, they look at early
menopause from perspectives of premature and unexpected ovarian failure. The result of
ovarian failure leads to a number of consequences. When the ovary stops to work in the
body they stop producing eggs and producing secondary female hormones namely
oestrogen and progesterone. This leads to loss of bearing capacity in many women. Failure
to produce hormones leads to stop of menstrual periods (Maclennan, A 2017). The
deficient oestrogen cause hot flushes, mood change due to hormonal imbalance,
disturbances when someone is sleeping, lead to stops of production of vaginal fluids
resulting to dry vagina. Cases whereby a woman has had premature menopause emotional
turmoil may set in. This is clearly seen whereby a woman feeling sad, jealous other
women’s pregnancies. The article proceeds to give the long-term consequences of
premature menopause which are osteoporosis which speeds up the arteries hardening. The
hardening of arteries may predispose someone to heart attack or stroke.
According to guideline of the Europe society of human reproduction and embryology they
give a clear outline on how to manage women with premature ovarian insufficiency. This
spells out good news on how to manage premature menopause. The article gives some
interventions that can be done case of loss of fertility this include: oocyte donation is one
of the best fertility interventions (Luborsky, J, 2013). Cases whereby there is bone loss,
women are advised to take a balanced diet to ensure sufficient intake of calcium and
vitamin D. The article cites oestrogen replacement to prevent osteoporosis and this help
maintain bones. Additionally, women may consider taking a combined oral contraceptive if
deemed appropriate. The article proceeds to tackle the issue of cardiovascular health in
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
premature ovarian insufficiency, it deals through hormone replacement therapy which
should be started early to prevent a future risk of getting cardiovascular disease. This
should be done constantly until a woman reaches natural menopause age. Cases whereby
the woman has Turner Syndrome, the person should be assessed on their blood pressure,
smoking, weight, lipid profile, fasting plasma glucose and HbA1c.The article provides also
intervention such as psychological and lifestyle support to improve their quality of life. The
article tackles the issue of sexual and genito-urinary function in the following ways: it cites
adequate oestrogen replacement for making sexual function normal. This helps treat
dyspareunia. Counseling should be given to women with premature ovarian insufficiency
on the need of supplementing testerone for long term efficacy and safety. On the issue of
genito-urinary, there should administration of hormone replacement therapy through local
estrogens. Additionally, lubricants can be used to treat vaginal dryness and dyspareunia for
women who are not using hormone replacement therapy. On the issue of inducing puberty
to premature ovarian therapy, women should take transdermal estradiol to induce puberty
(Luborsky, J, 2013).
The international journal of obstetrics and gynecology carried out a study using a sample of
4868 women to determine the cognitive and dementia in premature menopause women
later in life. The study was done in a timeline of two, four and seven years. The study
found out there is no notable association between dementia risk and premature menopause.
The study further gave some future consequences of premature ovarian failure which were
affects verbal fluency of women, poor performance which were not different on normal
menopausal women (Woad, K, 2016). This study adds to existing knowledge on influence
should be started early to prevent a future risk of getting cardiovascular disease. This
should be done constantly until a woman reaches natural menopause age. Cases whereby
the woman has Turner Syndrome, the person should be assessed on their blood pressure,
smoking, weight, lipid profile, fasting plasma glucose and HbA1c.The article provides also
intervention such as psychological and lifestyle support to improve their quality of life. The
article tackles the issue of sexual and genito-urinary function in the following ways: it cites
adequate oestrogen replacement for making sexual function normal. This helps treat
dyspareunia. Counseling should be given to women with premature ovarian insufficiency
on the need of supplementing testerone for long term efficacy and safety. On the issue of
genito-urinary, there should administration of hormone replacement therapy through local
estrogens. Additionally, lubricants can be used to treat vaginal dryness and dyspareunia for
women who are not using hormone replacement therapy. On the issue of inducing puberty
to premature ovarian therapy, women should take transdermal estradiol to induce puberty
(Luborsky, J, 2013).
The international journal of obstetrics and gynecology carried out a study using a sample of
4868 women to determine the cognitive and dementia in premature menopause women
later in life. The study was done in a timeline of two, four and seven years. The study
found out there is no notable association between dementia risk and premature menopause.
The study further gave some future consequences of premature ovarian failure which were
affects verbal fluency of women, poor performance which were not different on normal
menopausal women (Woad, K, 2016). This study adds to existing knowledge on influence
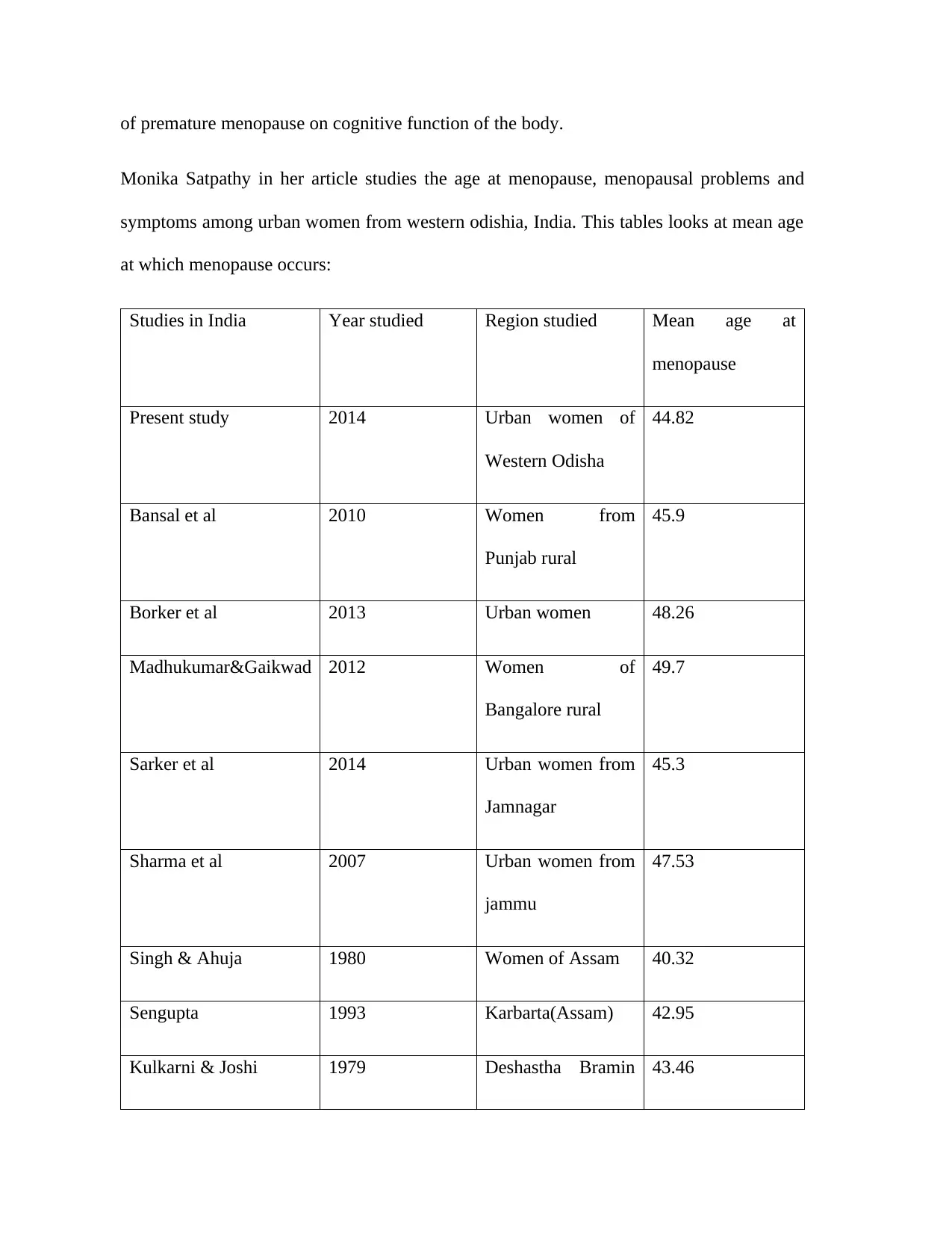
of premature menopause on cognitive function of the body.
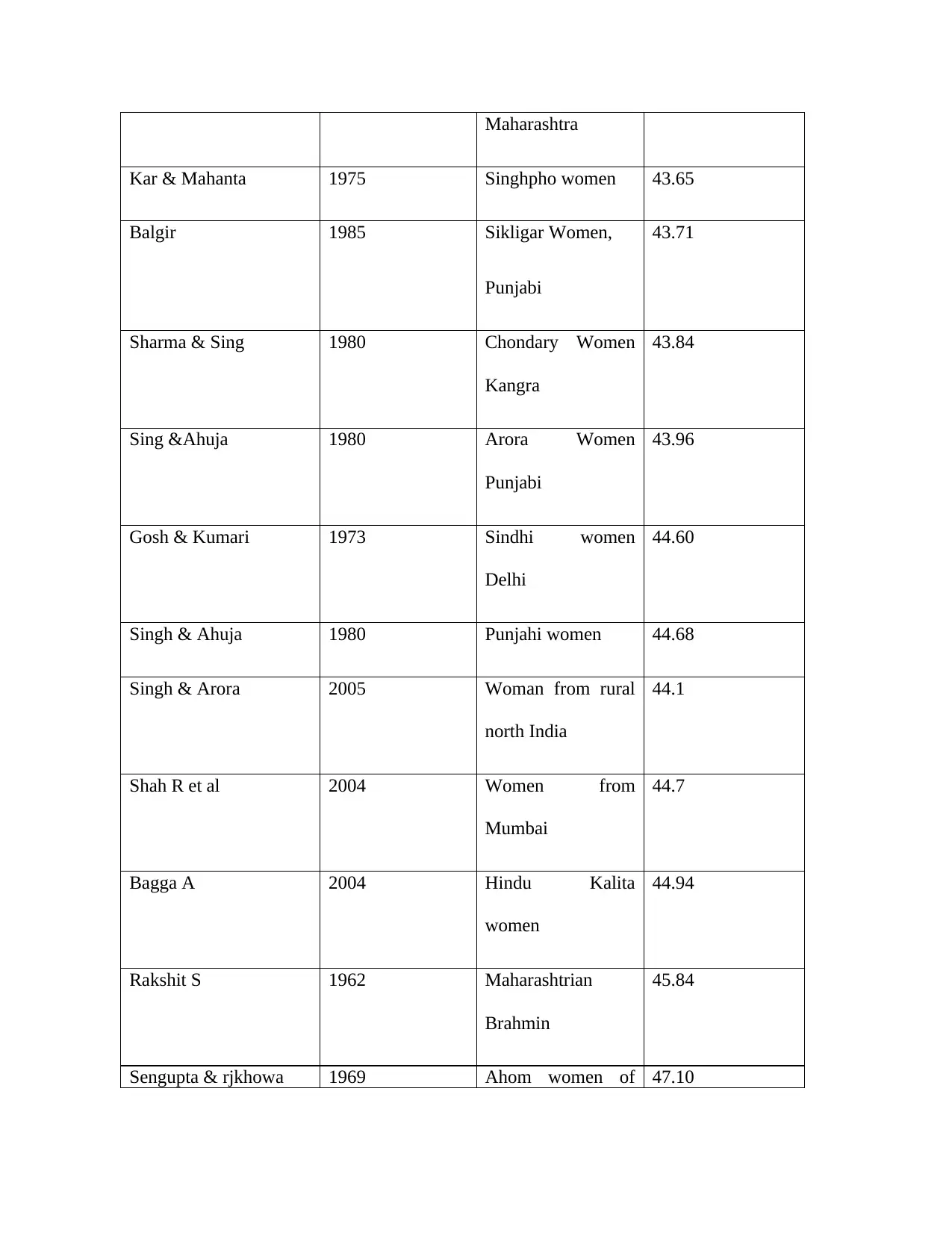
Monika Satpathy in her article studies the age at menopause, menopausal problems and
symptoms among urban women from western odishia, India. This tables looks at mean age
at which menopause occurs:
Studies in India Year studied Region studied Mean age at
menopause
Present study 2014 Urban women of
Western Odisha
44.82
Bansal et al 2010 Women from
Punjab rural
45.9
Borker et al 2013 Urban women 48.26
Madhukumar&Gaikwad 2012 Women of
Bangalore rural
49.7
Sarker et al 2014 Urban women from
Jamnagar
45.3
Sharma et al 2007 Urban women from
jammu
47.53
Singh & Ahuja 1980 Women of Assam 40.32
Sengupta 1993 Karbarta(Assam) 42.95
Kulkarni & Joshi 1979 Deshastha Bramin 43.46
Monika Satpathy in her article studies the age at menopause, menopausal problems and
symptoms among urban women from western odishia, India. This tables looks at mean age
at which menopause occurs:
Studies in India Year studied Region studied Mean age at
menopause
Present study 2014 Urban women of
Western Odisha
44.82
Bansal et al 2010 Women from
Punjab rural
45.9
Borker et al 2013 Urban women 48.26
Madhukumar&Gaikwad 2012 Women of
Bangalore rural
49.7
Sarker et al 2014 Urban women from
Jamnagar
45.3
Sharma et al 2007 Urban women from
jammu
47.53
Singh & Ahuja 1980 Women of Assam 40.32
Sengupta 1993 Karbarta(Assam) 42.95
Kulkarni & Joshi 1979 Deshastha Bramin 43.46
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Maharashtra
Kar & Mahanta 1975 Singhpho women 43.65
Balgir 1985 Sikligar Women,
Punjabi
43.71
Sharma & Sing 1980 Chondary Women
Kangra
43.84
Sing &Ahuja 1980 Arora Women
Punjabi
43.96
Gosh & Kumari 1973 Sindhi women
Delhi
44.60
Singh & Ahuja 1980 Punjahi women 44.68
Singh & Arora 2005 Woman from rural
north India
44.1
Shah R et al 2004 Women from
Mumbai
44.7
Bagga A 2004 Hindu Kalita
women
44.94
Rakshit S 1962 Maharashtrian
Brahmin
45.84
Sengupta & rjkhowa 1969 Ahom women of 47.10
Kar & Mahanta 1975 Singhpho women 43.65
Balgir 1985 Sikligar Women,
Punjabi
43.71
Sharma & Sing 1980 Chondary Women
Kangra
43.84
Sing &Ahuja 1980 Arora Women
Punjabi
43.96
Gosh & Kumari 1973 Sindhi women
Delhi
44.60
Singh & Ahuja 1980 Punjahi women 44.68
Singh & Arora 2005 Woman from rural
north India
44.1
Shah R et al 2004 Women from
Mumbai
44.7
Bagga A 2004 Hindu Kalita
women
44.94
Rakshit S 1962 Maharashtrian
Brahmin
45.84
Sengupta & rjkhowa 1969 Ahom women of 47.10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Dibrugarh in
Kaw et al 1994 Assam 47.50
Mastana 1996 Assam women 47.68
Sharma & Sing 1980 Among iabanas
North West India
Brahmin Women
Himachial
48.84
Kim YH et al 2003 Urban area of
Korea
48.29
Malachara JM et al 2002 State of Mexico 48.0
Mckinalay et al 1992 South East Asian
Women
51
Oldenhave &
Netelenbos
1994 Developed
countries
51
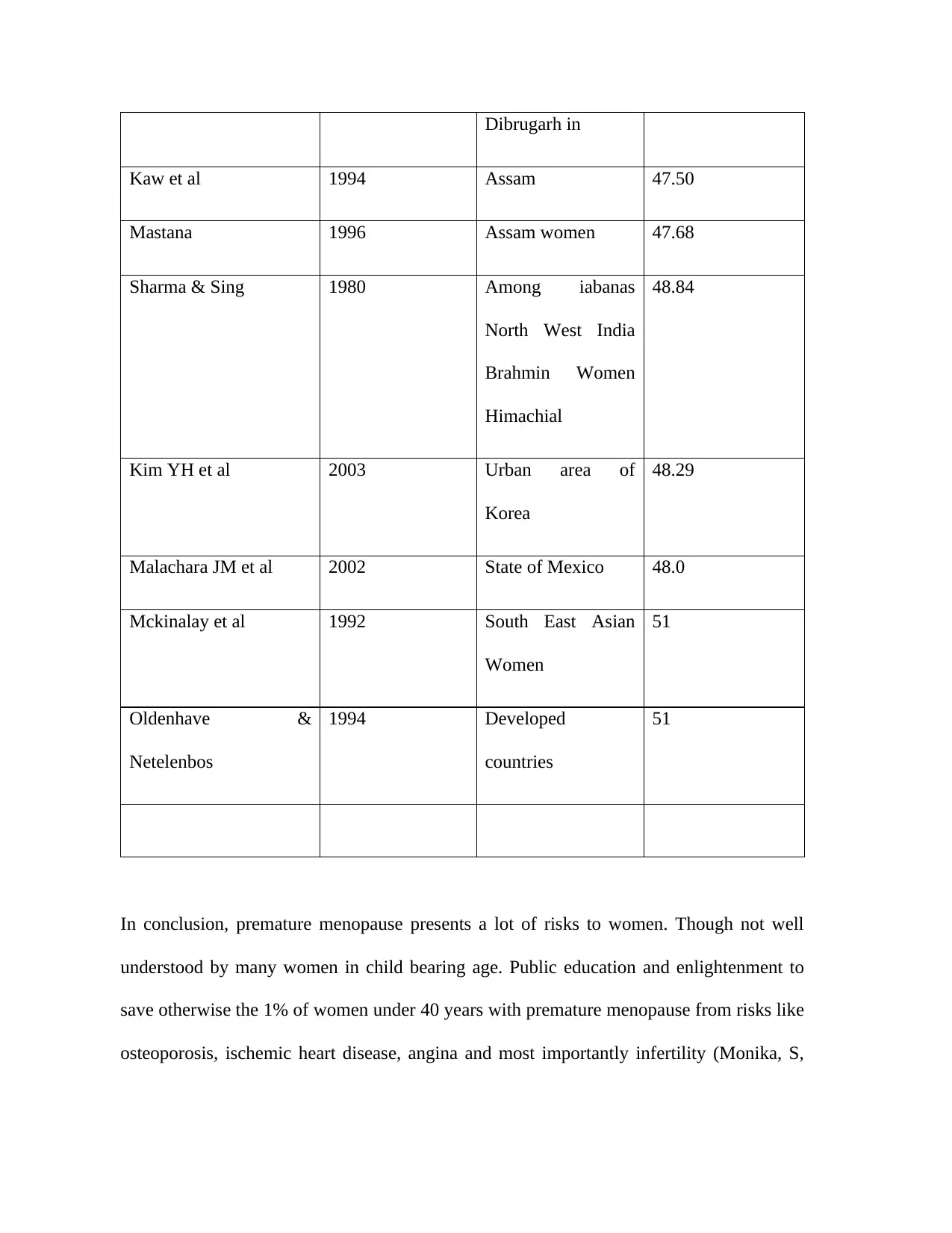
In conclusion, premature menopause presents a lot of risks to women. Though not well
understood by many women in child bearing age. Public education and enlightenment to
save otherwise the 1% of women under 40 years with premature menopause from risks like
osteoporosis, ischemic heart disease, angina and most importantly infertility (Monika, S,
Kaw et al 1994 Assam 47.50
Mastana 1996 Assam women 47.68
Sharma & Sing 1980 Among iabanas
North West India
Brahmin Women
Himachial
48.84
Kim YH et al 2003 Urban area of
Korea
48.29
Malachara JM et al 2002 State of Mexico 48.0
Mckinalay et al 1992 South East Asian
Women
51
Oldenhave &
Netelenbos
1994 Developed
countries
51
In conclusion, premature menopause presents a lot of risks to women. Though not well
understood by many women in child bearing age. Public education and enlightenment to
save otherwise the 1% of women under 40 years with premature menopause from risks like
osteoporosis, ischemic heart disease, angina and most importantly infertility (Monika, S,
2011).
Gap in knowledge
Many articles have been written on menopause in women but few focuses on premature
menopause on women who pass through a period of fluctuation in endocrine systems and
events that unfold with it. Premature menopause impacts a lot of change in women’s entire
body systems (Jain, R, 2016). Many studies have been brought forward in causal and
management of premature menopause if all of them are taken in consideration it becomes
too complex to predict and leads to conflicting conclusions in menopause research. The
areas of study which have not been research on exhaustively include:
Puberty delays among young women directly related to early menopause in women
aged 30-40 years.
Natural causes of premature menopause accounting for high incidence of
premature ovarian deficiency.
Induced causes of premature menopause affecting ovaries directly in
premenopausal women.
Chemotherapy affects directly ovarian function in premature menopause in
women.
Oocyte and ovary donation is effective in managing infertility in women with
premature ovary inefficiency.
Earliest age that premature menopause appears is before 30 years in women.
Hormone replacement therapy highly effective in managing premature ovarian
Gap in knowledge
Many articles have been written on menopause in women but few focuses on premature
menopause on women who pass through a period of fluctuation in endocrine systems and
events that unfold with it. Premature menopause impacts a lot of change in women’s entire
body systems (Jain, R, 2016). Many studies have been brought forward in causal and
management of premature menopause if all of them are taken in consideration it becomes
too complex to predict and leads to conflicting conclusions in menopause research. The
areas of study which have not been research on exhaustively include:
Puberty delays among young women directly related to early menopause in women
aged 30-40 years.
Natural causes of premature menopause accounting for high incidence of
premature ovarian deficiency.
Induced causes of premature menopause affecting ovaries directly in
premenopausal women.
Chemotherapy affects directly ovarian function in premature menopause in
women.
Oocyte and ovary donation is effective in managing infertility in women with
premature ovary inefficiency.
Earliest age that premature menopause appears is before 30 years in women.
Hormone replacement therapy highly effective in managing premature ovarian
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
deficiency (Kritz, S, 2013).
Signs and symptoms of premature menopause in women is consistent in all women
with premature ovarian efficiency.
Research question
The research questions for this study include:
Are puberty delays among young women directly related to early menopause in
women aged 30-40 years?
Do natural causes of premature menopause account for high incidence of premature
ovarian deficiency?
What Induced causes of premature menopause affect ovary directly in premenopausal
women? (Faddy, M, 2016)
How does chemotherapy affect ovary functioning in premature menopause in women?
Is oocyte and ovary donation effective in managing infertility in women with
premature ovary inefficiency?
What is the earliest age that premature menopause appears in premenopausal women
aged 30 years and below in women?
Is hormone replacement therapy effective in managing premature ovarian deficiency?
Are signs and symptoms of premature menopause in women consistent in all women
with premature ovarian inefficiency?
Signs and symptoms of premature menopause in women is consistent in all women
with premature ovarian efficiency.
Research question
The research questions for this study include:
Are puberty delays among young women directly related to early menopause in
women aged 30-40 years?
Do natural causes of premature menopause account for high incidence of premature
ovarian deficiency?
What Induced causes of premature menopause affect ovary directly in premenopausal
women? (Faddy, M, 2016)
How does chemotherapy affect ovary functioning in premature menopause in women?
Is oocyte and ovary donation effective in managing infertility in women with
premature ovary inefficiency?
What is the earliest age that premature menopause appears in premenopausal women
aged 30 years and below in women?
Is hormone replacement therapy effective in managing premature ovarian deficiency?
Are signs and symptoms of premature menopause in women consistent in all women
with premature ovarian inefficiency?
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
What needs to be known
In the research I will identify women aged between 30-45 years, since it is the age gap
most perceived to have premature menopause. I will identify what natural and induced
factors mainly cause premature menopause in women. I will identify both unique and
consistent signs and symptoms of premature menopause (Hou, N, 2016). I will also
identify what commonest intervention they receive to manage premature menopause.
The participants will be required to tell the researcher their age and ethnicity. After
identifying a woman with premature menopause, I will ask her about how premature
menopause presented itself i.e. was it natural or induced. If it was induced was the uterus
taken out by surgery. If yes, was the ovary taken too. Age and time when the surgical
operation was conducted to determine when the premature menopause set in. I will ask
when the participant had her last menstrual period in the premenopausal women and did
they complain about it. In the research I will also enquire from the participant how the
signs and symptoms presented themselves during premature menopause. I will ask the
participant to tell me what interventions she received when premature menopause set in.
The participant will tell me if it was hormone therapy or medication (Faubin, C, 2015).
Finally, I will ask the participant if she still experiences the symptoms and how she feels
about it.
Project aims and expected benefits
The project aims are:
To determine how puberty delays among young women is directly related to early
In the research I will identify women aged between 30-45 years, since it is the age gap
most perceived to have premature menopause. I will identify what natural and induced
factors mainly cause premature menopause in women. I will identify both unique and
consistent signs and symptoms of premature menopause (Hou, N, 2016). I will also
identify what commonest intervention they receive to manage premature menopause.
The participants will be required to tell the researcher their age and ethnicity. After
identifying a woman with premature menopause, I will ask her about how premature
menopause presented itself i.e. was it natural or induced. If it was induced was the uterus
taken out by surgery. If yes, was the ovary taken too. Age and time when the surgical
operation was conducted to determine when the premature menopause set in. I will ask
when the participant had her last menstrual period in the premenopausal women and did
they complain about it. In the research I will also enquire from the participant how the
signs and symptoms presented themselves during premature menopause. I will ask the
participant to tell me what interventions she received when premature menopause set in.
The participant will tell me if it was hormone therapy or medication (Faubin, C, 2015).
Finally, I will ask the participant if she still experiences the symptoms and how she feels
about it.
Project aims and expected benefits
The project aims are:
To determine how puberty delays among young women is directly related to early
menopause in women aged 30-40 years.
To establish the natural causes of premature menopause that account for high
incidences of premature ovarian deficiency.
To find out Induced causes of premature menopause that affect ovary directly in
premenopausal women.
To assess chemotherapeutical factors that affect ovary functioning in premature
menopause in women (Rocca, W, 2012).
To find out if oocyte and ovary donation is effective in managing infertility in
women with premature ovary inefficiency.
To establish the earliest age that premature menopause appears in premenopausal
women aged 30 years and below.
To find out if hormone replacement therapy is effective in managing premature
ovarian deficiency.
To establish signs and symptoms of premature menopause in women with
premature ovarian efficiency?
The study findings will help in developing new approaches for management of premature
menopause. The research will help generate ideas for management and attitudes towards
premature menopause. Project recommendations will contribute towards reaching the
reproductive health development goals by bridging the gap in knowledge in premature
menopause (Ewertz, M, 2011).
To establish the natural causes of premature menopause that account for high
incidences of premature ovarian deficiency.
To find out Induced causes of premature menopause that affect ovary directly in
premenopausal women.
To assess chemotherapeutical factors that affect ovary functioning in premature
menopause in women (Rocca, W, 2012).
To find out if oocyte and ovary donation is effective in managing infertility in
women with premature ovary inefficiency.
To establish the earliest age that premature menopause appears in premenopausal
women aged 30 years and below.
To find out if hormone replacement therapy is effective in managing premature
ovarian deficiency.
To establish signs and symptoms of premature menopause in women with
premature ovarian efficiency?
The study findings will help in developing new approaches for management of premature
menopause. The research will help generate ideas for management and attitudes towards
premature menopause. Project recommendations will contribute towards reaching the
reproductive health development goals by bridging the gap in knowledge in premature
menopause (Ewertz, M, 2011).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 27

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.