Australian Pharmaceutical Benefit Scheme
VerifiedAdded on 2023/06/12
|12
|2752
|158
AI Summary
The Australian Pharmaceutical Benefit Scheme (PBS) offers free medication to pensioners and subsidizes over 211 million prescriptions. The PBS advisory committee assesses and recommends which drugs should be listed. Australia is one of the biggest consumers of medicine due to the high prevalence of chronic diseases. The government contributes a large amount of funds to the healthcare system, and there is private health insurance available. Both prescription and non-prescription forms of medication are common in the Australian healthcare system. Challenges faced by the PBS include preauthorization, price renegotiations, and post-market surveillance.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 1
Australian Pharmaceutical Benefit Scheme
Student’s Name
Professor’s Name
Institutional Affiliation
Date
Contents
Australian Pharmaceutical Benefit Scheme
Student’s Name
Professor’s Name
Institutional Affiliation
Date
Contents
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 2
Consumption of medicine in Australia............................................................................................3
Introduction..................................................................................................................................3
Consumption rates for medicine..................................................................................................4
Cost of medicine consumption.....................................................................................................5
Types of medicine consumed.......................................................................................................7
Conclusion...................................................................................................................................8
References........................................................................................................................................9
Consumption of medicine in Australia............................................................................................3
Introduction..................................................................................................................................3
Consumption rates for medicine..................................................................................................4
Cost of medicine consumption.....................................................................................................5
Types of medicine consumed.......................................................................................................7
Conclusion...................................................................................................................................8
References........................................................................................................................................9
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 3
Consumption of medicine in Australia
Introduction
The Idea of developing PBS in Australia began in1944though it was rejected by the
court. It began its main operations in1948. It was restricted to offering free medication to the
pensioners and around one hundred and thirty-nine vaccines as well as lifesaving medicines to
the entire public. It became very strong when it was first established under the law in1953 under
the national health act and it is one of the major aspects of the national medicine policy. In 1960
PBS was made an all-encompassing scheme allowing access to a good range of different
medicines in Australia. By 2014 the pharmaceutical benefits scheme had registered and
subsidized more than two hundred and eleven million prescriptions. The medicines are
approximated to have cost the government of Australia more than nine billion dollars. This
amount is about twenty-one percent of the total health expenditure. Van Boeckel, et al 2014).
The advisory committee of the pharmaceutical benefits scheme is obligated to assess all
the medication and then recommend which should be listed by the PBS and which should not.
The committee was set up by the government but not part of the PBS. The committee also
recommends which drugs should be withdrawn from the PBS list in case there are any safety
concerns. (Gleeson, et al 2015).
The medication must be listed with the Australian therapeutic good register before they
are accepted for listing in the pharmaceutical benefits scheme. The medication companies must
apply for the listing of the drugs with the therapeutic goods administration. Clinical trials
evidence is a requirement and must, therefore, be provided in order to ensure the health safety of
the patient who may use the drugs. The medication must attain the set quality standards and must
Consumption of medicine in Australia
Introduction
The Idea of developing PBS in Australia began in1944though it was rejected by the
court. It began its main operations in1948. It was restricted to offering free medication to the
pensioners and around one hundred and thirty-nine vaccines as well as lifesaving medicines to
the entire public. It became very strong when it was first established under the law in1953 under
the national health act and it is one of the major aspects of the national medicine policy. In 1960
PBS was made an all-encompassing scheme allowing access to a good range of different
medicines in Australia. By 2014 the pharmaceutical benefits scheme had registered and
subsidized more than two hundred and eleven million prescriptions. The medicines are
approximated to have cost the government of Australia more than nine billion dollars. This
amount is about twenty-one percent of the total health expenditure. Van Boeckel, et al 2014).
The advisory committee of the pharmaceutical benefits scheme is obligated to assess all
the medication and then recommend which should be listed by the PBS and which should not.
The committee was set up by the government but not part of the PBS. The committee also
recommends which drugs should be withdrawn from the PBS list in case there are any safety
concerns. (Gleeson, et al 2015).
The medication must be listed with the Australian therapeutic good register before they
are accepted for listing in the pharmaceutical benefits scheme. The medication companies must
apply for the listing of the drugs with the therapeutic goods administration. Clinical trials
evidence is a requirement and must, therefore, be provided in order to ensure the health safety of
the patient who may use the drugs. The medication must attain the set quality standards and must
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 4
be cost-effective compared to all other types of medicine offered in the market. (Walkom, et al
2013).
According to the national health act, the pharmacist must be approved to dispense
medicine from particular pharmacies. The government pays a portion of the cost to the
pharmacist and the patient are charged the remaining amount. Under the PBS, the amount of
money that a patient is supposed to pay towards the medication cost of the pharmacies are set to
protect the public. In 2015 a maximum of 37.70 dollars was paid by the pensioners, while the
cohesion patients paid an average of 6.10dollars per prescription. (Schaffer, et al 2015).
According to the national health act, the pharmacist must be approved to dispense medicine from
particular pharmacies. The government pays a portion of the cost to the pharmacist and the
patient are charged the remaining amount. Under the PBS, the amount of money that a patient is
supposed to pay towards the medication cost of the pharmacies are set to protect the public. In
2015 a maximum of 37.70 dollars was paid by the pensioners, while the cohesion patients paid
an average of 6.10dollars per prescription. (Schaffer, et al 2015).
be cost-effective compared to all other types of medicine offered in the market. (Walkom, et al
2013).
According to the national health act, the pharmacist must be approved to dispense
medicine from particular pharmacies. The government pays a portion of the cost to the
pharmacist and the patient are charged the remaining amount. Under the PBS, the amount of
money that a patient is supposed to pay towards the medication cost of the pharmacies are set to
protect the public. In 2015 a maximum of 37.70 dollars was paid by the pensioners, while the
cohesion patients paid an average of 6.10dollars per prescription. (Schaffer, et al 2015).
According to the national health act, the pharmacist must be approved to dispense medicine from
particular pharmacies. The government pays a portion of the cost to the pharmacist and the
patient are charged the remaining amount. Under the PBS, the amount of money that a patient is
supposed to pay towards the medication cost of the pharmacies are set to protect the public. In
2015 a maximum of 37.70 dollars was paid by the pensioners, while the cohesion patients paid
an average of 6.10dollars per prescription. (Schaffer, et al 2015).
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 5
Consumption rates for medicine
Australia is ranked as one of the greatest consumer of medicine though it has one of the
biggest life expectancies the country has some challenges of diseases like cancer, coronary heart
diseases, stroke, diabetes, kidney diseases, respiratory diseases dementia, incontinence and so
many others that are among the leading causes of deaths in Australia. A report of 2014 from the
NHS revealed that around 1,2 million people were diagnosed with diabetes, an average of 11
million cases of chronic conditions such as cancer, arthritis, and asthma were reported in the
same year 11 million cases of obesity were also noted among the people aged 188 and above.
This is about 63%of the adult population in the country. This kind of statistics has forced the
government to invest a lot in medication making them be among the biggest users of medication.
The Australian government has also set up a safety net scheme to ensure that the citizens
who may be having high medications needs are well protected. In 2015 if a patient or the close
family had spent around 1453.90 dollars on the PBS prescription, the remaining part of the year
cost the 6.10 per prescription. After the pensioners and other cohesion patients who own a card
reached the net threshold of 366 dollars expenditure index. (Karanges, et al 2016)
A national medication policy was set by the government of Australia to put formulate a
good framework of improving the health standards in the country.it improves the outcomes of
health by ensuring that the Australians access and use the right medication for the various health-
related problems. The main aim of the policy is to meet needs of health care services and
medication as well as the economic objectives. (Mellish, et al 2015).
Consumption rates for medicine
Australia is ranked as one of the greatest consumer of medicine though it has one of the
biggest life expectancies the country has some challenges of diseases like cancer, coronary heart
diseases, stroke, diabetes, kidney diseases, respiratory diseases dementia, incontinence and so
many others that are among the leading causes of deaths in Australia. A report of 2014 from the
NHS revealed that around 1,2 million people were diagnosed with diabetes, an average of 11
million cases of chronic conditions such as cancer, arthritis, and asthma were reported in the
same year 11 million cases of obesity were also noted among the people aged 188 and above.
This is about 63%of the adult population in the country. This kind of statistics has forced the
government to invest a lot in medication making them be among the biggest users of medication.
The Australian government has also set up a safety net scheme to ensure that the citizens
who may be having high medications needs are well protected. In 2015 if a patient or the close
family had spent around 1453.90 dollars on the PBS prescription, the remaining part of the year
cost the 6.10 per prescription. After the pensioners and other cohesion patients who own a card
reached the net threshold of 366 dollars expenditure index. (Karanges, et al 2016)
A national medication policy was set by the government of Australia to put formulate a
good framework of improving the health standards in the country.it improves the outcomes of
health by ensuring that the Australians access and use the right medication for the various health-
related problems. The main aim of the policy is to meet needs of health care services and
medication as well as the economic objectives. (Mellish, et al 2015).
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 6
Cost of medicine consumption
The government of Australia together with the territory and state government to share the
responsibilities and roles in the healthcare system. The public health centre is controlled and
funded by the Australian government. There are also private sectors owned by private sectors but
are licensed and controlled by the government health laws. The health cost in Australia in 2013-
2014 Australian health budget was approximate to be $155 billion, which is equivalent to 9.8%
of gross domestic income product. This was compared with the previous year's budget of $150
billion. Among the $155 billion health budget, $59 million was spent on the hospital in Australia.
This health expenditure in the Australian healthcare system on hospitals was constant for over
the previous 10 years at about 40% (Dobbin, 2014).
The cost of pharmaceutical via the pharmaceutical benefits scheme (PBS) included the
primary healthcare group which was $10.1 billion in the 2013- 2014 health budget. The
Australian government contributed $105 billion which was equivalent to 68% of the total
expenditure in the year 2013- 2014 health budget. This shows that the Australian government
contributes a large amount of fund in the medical services. The state and territory government of
Australia provides most of the funds in the community health services, which is estimated to be
$6.2 billion. The total expenditure contributed by non- government sectors in 2013- 2014 was
approximately $billion which was nearly 18% of the health budget. Most the funds for non-
subsidized medicines for example medication offered over the counter, under co-payment
medicines and private prescription came from individuals which were about $ 9.0 billion in the
year 2015 the rate of healthcare expenditure increased by 1.75% according to the report from the
department of health. (Lai, et al 2013).
Cost of medicine consumption
The government of Australia together with the territory and state government to share the
responsibilities and roles in the healthcare system. The public health centre is controlled and
funded by the Australian government. There are also private sectors owned by private sectors but
are licensed and controlled by the government health laws. The health cost in Australia in 2013-
2014 Australian health budget was approximate to be $155 billion, which is equivalent to 9.8%
of gross domestic income product. This was compared with the previous year's budget of $150
billion. Among the $155 billion health budget, $59 million was spent on the hospital in Australia.
This health expenditure in the Australian healthcare system on hospitals was constant for over
the previous 10 years at about 40% (Dobbin, 2014).
The cost of pharmaceutical via the pharmaceutical benefits scheme (PBS) included the
primary healthcare group which was $10.1 billion in the 2013- 2014 health budget. The
Australian government contributed $105 billion which was equivalent to 68% of the total
expenditure in the year 2013- 2014 health budget. This shows that the Australian government
contributes a large amount of fund in the medical services. The state and territory government of
Australia provides most of the funds in the community health services, which is estimated to be
$6.2 billion. The total expenditure contributed by non- government sectors in 2013- 2014 was
approximately $billion which was nearly 18% of the health budget. Most the funds for non-
subsidized medicines for example medication offered over the counter, under co-payment
medicines and private prescription came from individuals which were about $ 9.0 billion in the
year 2015 the rate of healthcare expenditure increased by 1.75% according to the report from the
department of health. (Lai, et al 2013).
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 7
The significant increase rate was as a result of the introduction of new generic medicines which
influenced the negotiable prices of the pharmaceutical drugs through the listing of the generic
medicines in (PBS) and also availing them to the market. The decrease in the health cost did not
reflect inadequate services as the number of subsidized drugs distributed during this period had
risen from 2008 million in 2012 to 223 million in 2013. The changes that occurred in the private
health sector insurance rebated the share of funds that was were provided by Australian
government through reduction scheme. These changes lead to the increased proportion of cost
from private health insurers from 7.4% in 2012 to 8.3% 1n 2013. (Blanch, et al 2014).
There is private health insurance available for individuals who wish to cover the cost of
hospital admission bills as the private patient or for covering other subordinate health services. In
2015, 11.3 million Australian people which were 47% of the total population had been insured
with private patient hospital cover and around 13.4 million that is 56% had applied for general
treatment cover. Through Medicare system, the Australian government covered a portion of
hospital admission bills for the private patient. (Stephenson, et al2013). The government
intervention strategies within the healthcare system of Australia in both public and the private
patient is the main reason for the standardization of the medical cost in Australia. In addition, the
Australian government together with the state and territory government roles in the healthcare
system has contributed to the ease of healthcare in Australian people. The overall health sector in
Australian which is collectively called the Health Council is responsible for providing a forum of
health services through cooperation and regulation on primary and secondary healthcare issues
and in considering the increase in cost pressure. The drug utilization in Australia can be used to
monitor the impact of pharmacy economy. Golley, et al 2015).
The significant increase rate was as a result of the introduction of new generic medicines which
influenced the negotiable prices of the pharmaceutical drugs through the listing of the generic
medicines in (PBS) and also availing them to the market. The decrease in the health cost did not
reflect inadequate services as the number of subsidized drugs distributed during this period had
risen from 2008 million in 2012 to 223 million in 2013. The changes that occurred in the private
health sector insurance rebated the share of funds that was were provided by Australian
government through reduction scheme. These changes lead to the increased proportion of cost
from private health insurers from 7.4% in 2012 to 8.3% 1n 2013. (Blanch, et al 2014).
There is private health insurance available for individuals who wish to cover the cost of
hospital admission bills as the private patient or for covering other subordinate health services. In
2015, 11.3 million Australian people which were 47% of the total population had been insured
with private patient hospital cover and around 13.4 million that is 56% had applied for general
treatment cover. Through Medicare system, the Australian government covered a portion of
hospital admission bills for the private patient. (Stephenson, et al2013). The government
intervention strategies within the healthcare system of Australia in both public and the private
patient is the main reason for the standardization of the medical cost in Australia. In addition, the
Australian government together with the state and territory government roles in the healthcare
system has contributed to the ease of healthcare in Australian people. The overall health sector in
Australian which is collectively called the Health Council is responsible for providing a forum of
health services through cooperation and regulation on primary and secondary healthcare issues
and in considering the increase in cost pressure. The drug utilization in Australia can be used to
monitor the impact of pharmacy economy. Golley, et al 2015).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 8
Types of medicine consumed
Both prescription and non- prescription forms of medication are common in Australian
healthcare system. The prescribed forms of medication require medical or doctor's instructions
and advice. These prescribed forms of medication include pain relievers, heart problems and
blood pressure medication. On the other hand, the non- prescribed do not need proceedings from
medical professional prescription or advice, they include vitamins, minerals and herbal
medication. These types of medication do elude government rebate. The drug prescription is
dispensed under government subsidization schemes or as private prescription these schemes
include; Repatriation Pharmaceutical Benefits Scheme (RPBS) and Pharmaceutical Benefits
Scheme (PBS). When a new medicine is discovered in Australia, it must then get approved for
market distribution by the company according to the rules of the Therapeutic Goods Act 1989.
The company then had the drug included on the PBS. The table A below shows examples of
medicine that have been commonly used in Australia in 2015 and over the previous years. These
drugs included the subsidized prescription count of the top 10 drugs distributed in the Australian
community. (Cooter, & Pickstone, 2013).
Types of medicine consumed
Both prescription and non- prescription forms of medication are common in Australian
healthcare system. The prescribed forms of medication require medical or doctor's instructions
and advice. These prescribed forms of medication include pain relievers, heart problems and
blood pressure medication. On the other hand, the non- prescribed do not need proceedings from
medical professional prescription or advice, they include vitamins, minerals and herbal
medication. These types of medication do elude government rebate. The drug prescription is
dispensed under government subsidization schemes or as private prescription these schemes
include; Repatriation Pharmaceutical Benefits Scheme (RPBS) and Pharmaceutical Benefits
Scheme (PBS). When a new medicine is discovered in Australia, it must then get approved for
market distribution by the company according to the rules of the Therapeutic Goods Act 1989.
The company then had the drug included on the PBS. The table A below shows examples of
medicine that have been commonly used in Australia in 2015 and over the previous years. These
drugs included the subsidized prescription count of the top 10 drugs distributed in the Australian
community. (Cooter, & Pickstone, 2013).
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 9
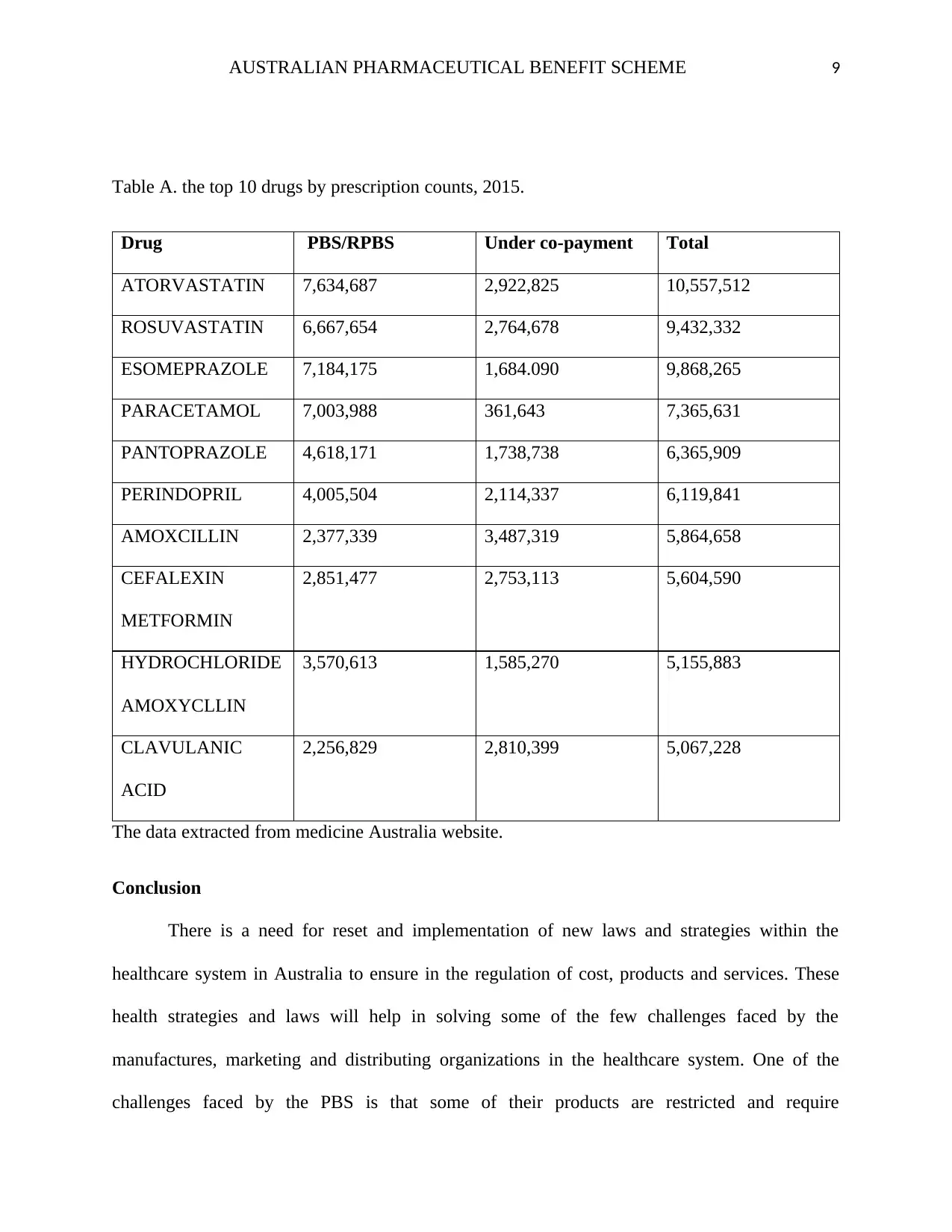
Table A. the top 10 drugs by prescription counts, 2015.
Drug PBS/RPBS Under co-payment Total
ATORVASTATIN 7,634,687 2,922,825 10,557,512
ROSUVASTATIN 6,667,654 2,764,678 9,432,332
ESOMEPRAZOLE 7,184,175 1,684.090 9,868,265
PARACETAMOL 7,003,988 361,643 7,365,631
PANTOPRAZOLE 4,618,171 1,738,738 6,365,909
PERINDOPRIL 4,005,504 2,114,337 6,119,841
AMOXCILLIN 2,377,339 3,487,319 5,864,658
CEFALEXIN
METFORMIN
2,851,477 2,753,113 5,604,590
HYDROCHLORIDE
AMOXYCLLIN
3,570,613 1,585,270 5,155,883
CLAVULANIC
ACID
2,256,829 2,810,399 5,067,228
The data extracted from medicine Australia website.
Conclusion
There is a need for reset and implementation of new laws and strategies within the
healthcare system in Australia to ensure in the regulation of cost, products and services. These
health strategies and laws will help in solving some of the few challenges faced by the
manufactures, marketing and distributing organizations in the healthcare system. One of the
challenges faced by the PBS is that some of their products are restricted and require
Table A. the top 10 drugs by prescription counts, 2015.
Drug PBS/RPBS Under co-payment Total
ATORVASTATIN 7,634,687 2,922,825 10,557,512
ROSUVASTATIN 6,667,654 2,764,678 9,432,332
ESOMEPRAZOLE 7,184,175 1,684.090 9,868,265
PARACETAMOL 7,003,988 361,643 7,365,631
PANTOPRAZOLE 4,618,171 1,738,738 6,365,909
PERINDOPRIL 4,005,504 2,114,337 6,119,841
AMOXCILLIN 2,377,339 3,487,319 5,864,658
CEFALEXIN
METFORMIN
2,851,477 2,753,113 5,604,590
HYDROCHLORIDE
AMOXYCLLIN
3,570,613 1,585,270 5,155,883
CLAVULANIC
ACID
2,256,829 2,810,399 5,067,228
The data extracted from medicine Australia website.
Conclusion
There is a need for reset and implementation of new laws and strategies within the
healthcare system in Australia to ensure in the regulation of cost, products and services. These
health strategies and laws will help in solving some of the few challenges faced by the
manufactures, marketing and distributing organizations in the healthcare system. One of the
challenges faced by the PBS is that some of their products are restricted and require
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 10
preauthorization over medical registration. PBS experiences problems in the fields of price
renegotiations. It has weakness in terms of efficiency in the post-market surveillance. Challenges
arise when there are weaknesses in incentives in the manufacturer's line of pricing agreement this
may result in the production of poor quality medicines. The patient's co-payment also brings a
negative impact on equity and efficiency of PBS. Lack of standardized cost-effectiveness
according to the government regulation policy on PBS. The studies that are sponsored by some
pharmaceutical producers may give report result that favours their sponsors more than research
supported by the other sources. The introduction of new generic medicines to the market also
becomes a challenge among the manufactures as it alters price levels.
References
Blanch, B., Pearson, S. A., & Haber, P. S. (2014). An overview of the patterns of prescription
opioid use, costs and related harms in Australia. British journal of clinical pharmacology,
preauthorization over medical registration. PBS experiences problems in the fields of price
renegotiations. It has weakness in terms of efficiency in the post-market surveillance. Challenges
arise when there are weaknesses in incentives in the manufacturer's line of pricing agreement this
may result in the production of poor quality medicines. The patient's co-payment also brings a
negative impact on equity and efficiency of PBS. Lack of standardized cost-effectiveness
according to the government regulation policy on PBS. The studies that are sponsored by some
pharmaceutical producers may give report result that favours their sponsors more than research
supported by the other sources. The introduction of new generic medicines to the market also
becomes a challenge among the manufactures as it alters price levels.
References
Blanch, B., Pearson, S. A., & Haber, P. S. (2014). An overview of the patterns of prescription
opioid use, costs and related harms in Australia. British journal of clinical pharmacology,
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 11
78(5), 1159-1166.Cooter, R., & Pickstone, J. (Eds.). (2013). Companion encyclopedia of
medicine in the twentieth century. Routledge.
Dobbin, M. (2014). Pharmaceutical drug misuse in Australia. Australian Prescriber, 37(3), 79-81.
Gleeson, D. H., Moir, H., & Lopert, R. (2015). Costs to Australian taxpayers of pharmaceutical
monopolies and proposals to extend them in the Trans-Pacific Partnership Agreement.
The Medical Journal of Australia, 202(6), 306-308.
Golley, S., Corsini, N., Topping, D., Morell, M., & Mohr, P. (2015). Motivations for avoiding
wheat consumption in Australia: results from a population survey. Public Health
Nutrition, 18(3), 490-499.
Karanges, E. A., Blanch, B., Buckley, N. A., & Pearson, S. A. (2016). Twenty‐five years of
prescription opioid use in Australia: a whole‐of‐population analysis using pharmaceutical
claims. British journal of clinical pharmacology, 82(1), 255-267.
Lai, F. Y., Bruno, R., Hall, W., Gartner, C., Ort, C., Kirkbride, P., ... & Mueller, J. F. (2013).
Profiles of illicit drug use during annual key holiday and control periods in Australia:
wastewater analysis in an urban, a semi‐rural and a vacation area. Addiction, 108(3), 556-
565.
Mellish, L., Karanges, E. A., Litchfield, M. J., Schaffer, A. L., Blanch, B., Daniels, B. J., ... &
Pearson, S. A. (2015). The Australian Pharmaceutical Benefits Scheme data collection: a
practical guide for researchers. BMC research notes, 8(1), 634.
78(5), 1159-1166.Cooter, R., & Pickstone, J. (Eds.). (2013). Companion encyclopedia of
medicine in the twentieth century. Routledge.
Dobbin, M. (2014). Pharmaceutical drug misuse in Australia. Australian Prescriber, 37(3), 79-81.
Gleeson, D. H., Moir, H., & Lopert, R. (2015). Costs to Australian taxpayers of pharmaceutical
monopolies and proposals to extend them in the Trans-Pacific Partnership Agreement.
The Medical Journal of Australia, 202(6), 306-308.
Golley, S., Corsini, N., Topping, D., Morell, M., & Mohr, P. (2015). Motivations for avoiding
wheat consumption in Australia: results from a population survey. Public Health
Nutrition, 18(3), 490-499.
Karanges, E. A., Blanch, B., Buckley, N. A., & Pearson, S. A. (2016). Twenty‐five years of
prescription opioid use in Australia: a whole‐of‐population analysis using pharmaceutical
claims. British journal of clinical pharmacology, 82(1), 255-267.
Lai, F. Y., Bruno, R., Hall, W., Gartner, C., Ort, C., Kirkbride, P., ... & Mueller, J. F. (2013).
Profiles of illicit drug use during annual key holiday and control periods in Australia:
wastewater analysis in an urban, a semi‐rural and a vacation area. Addiction, 108(3), 556-
565.
Mellish, L., Karanges, E. A., Litchfield, M. J., Schaffer, A. L., Blanch, B., Daniels, B. J., ... &
Pearson, S. A. (2015). The Australian Pharmaceutical Benefits Scheme data collection: a
practical guide for researchers. BMC research notes, 8(1), 634.
AUSTRALIAN PHARMACEUTICAL BENEFIT SCHEME 12
Schaffer, A. L., Buckley, N. A., Dobbins, T. A., Banks, E., & Pearson, S. A. (2015). The crux of
the matter: did the ABC's Catalyst program change statin use in Australia?. The Medical
Journal of Australia, 202(11), 591-594.
Stephenson, C. P., Karanges, E., & McGregor, I. S. (2013). Trends in the utilisation of
psychotropic medications in Australia from 2000 to 2011. Australian & New Zealand
Journal of Psychiatry, 47(1), 74-87.
Van Boeckel, T. P., Gandra, S., Ashok, A., Caudron, Q., Grenfell, B. T., Levin, S. A., &
Laxminarayan, R. (2014). Global antibiotic consumption 2000 to 2010: an analysis of
national pharmaceutical sales data. The Lancet Infectious Diseases, 14(8), 742-750.
Walkom, E. J., Loxton, D., & Robertson, J. (2013). Costs of medicines and health care: a
concern for Australian women across the ages. BMC health services research, 13(1), 484.
Schaffer, A. L., Buckley, N. A., Dobbins, T. A., Banks, E., & Pearson, S. A. (2015). The crux of
the matter: did the ABC's Catalyst program change statin use in Australia?. The Medical
Journal of Australia, 202(11), 591-594.
Stephenson, C. P., Karanges, E., & McGregor, I. S. (2013). Trends in the utilisation of
psychotropic medications in Australia from 2000 to 2011. Australian & New Zealand
Journal of Psychiatry, 47(1), 74-87.
Van Boeckel, T. P., Gandra, S., Ashok, A., Caudron, Q., Grenfell, B. T., Levin, S. A., &
Laxminarayan, R. (2014). Global antibiotic consumption 2000 to 2010: an analysis of
national pharmaceutical sales data. The Lancet Infectious Diseases, 14(8), 742-750.
Walkom, E. J., Loxton, D., & Robertson, J. (2013). Costs of medicines and health care: a
concern for Australian women across the ages. BMC health services research, 13(1), 484.
1 out of 12
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.