Australian Pharmaceutical Benefits Scheme
VerifiedAdded on 2023/01/23
|12
|2632
|37
AI Summary
This report critically reviews the characteristics of the Australian Pharmaceutical Benefits Scheme (PBS) and discusses the issues associated with it. It explores medication consumption in Australia, types of medicines consumed, and problems with the PBS. The report concludes with recommendations for improving affordability and accessibility.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Name of the Student:
Name of the University:
Author note:
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Name of the Student:
Name of the University:
Author note:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Executive Summary
The need to ensure accessibility and affordability in terms of basic medication and healthcare
services forms the underlying background of the Australian Pharmaceutical Benefits Scheme
(PBS). The purpose of this report is to critically review PBS characteristics.
Statins, antiretroviral drugs and cancer drugs are the most used drugs in Australia.
Major medications have been removed from PBS subsidy list.
The safety net rule increases medication costs during emergencies and for remote
communities.
Despite PBS, Australia continues to experience high medication cost.
Hence, to conclude, it is recommended that the government review the high PBS costs and
explore options to enhance affordability for disadvantaged groups.
Executive Summary
The need to ensure accessibility and affordability in terms of basic medication and healthcare
services forms the underlying background of the Australian Pharmaceutical Benefits Scheme
(PBS). The purpose of this report is to critically review PBS characteristics.
Statins, antiretroviral drugs and cancer drugs are the most used drugs in Australia.
Major medications have been removed from PBS subsidy list.
The safety net rule increases medication costs during emergencies and for remote
communities.
Despite PBS, Australia continues to experience high medication cost.
Hence, to conclude, it is recommended that the government review the high PBS costs and
explore options to enhance affordability for disadvantaged groups.
2AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Table of Contents
Introduction..........................................................................................................................2
Discussion............................................................................................................................2
Costs and Reasons of Medication Consumption in Australia.........................................2
Types of Medicines Consumed.......................................................................................4
Pharmaceutical Benefits Scheme: Problems...................................................................5
Concluding Recommendations........................................................................................7
References............................................................................................................................9
Table of Contents
Introduction..........................................................................................................................2
Discussion............................................................................................................................2
Costs and Reasons of Medication Consumption in Australia.........................................2
Types of Medicines Consumed.......................................................................................4
Pharmaceutical Benefits Scheme: Problems...................................................................5
Concluding Recommendations........................................................................................7
References............................................................................................................................9
3AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Introduction
The Australian Pharmaceutical Benefits Scheme (PBS) was developed to provide access
to wide range of drugs to Australian citizens at however, subsidized price. PBS has been subject
to nationwide public scrutiny and criticism, due to the rise in its subsequent subsidized costs. The
PBS is regulated by the National Health (Pharmaceutical Benefits) Regulations 1960 and
National Health Act (Paige et al., 2015). The following report will discuss on medicine
consumption in Australia and the key issues associated with PBS and recommendations which
may aid in possible improvements of the same.
Discussion
Costs and Reasons of Medication Consumption in Australia
The medicinal group of statins record highest cost and usage followed by medicines for
treatment of neurological complications and antiretroviral drugs required for the management of
hepatic conditions like Hepatitis C (Mellish, 2015). Taking insights from the report published by
the Australian Institute of Health and Welfare, medicines like statins, required for the treatment
of high circulatory cholesterol levels and cardiovascular abnormalities have undergone
dispensing in volumes higher than other drugs, amounting to approximately 10 million
prescriptions annual across the years ranging from 2016 to 2017 (Paola, 2019). Of these,
Atorvastatin has been reported to yield the highest usage with an alarming cost of $19. Such high
costs continue to sound ironic considering the presence of PBS whose agenda lies in the
subsidizing the costs of medications for the general public (ABC News. (2019). Followed by
statin usage, antiretroviral drugs for the treatment of Hepatitis C have been recorded to yield
Introduction
The Australian Pharmaceutical Benefits Scheme (PBS) was developed to provide access
to wide range of drugs to Australian citizens at however, subsidized price. PBS has been subject
to nationwide public scrutiny and criticism, due to the rise in its subsequent subsidized costs. The
PBS is regulated by the National Health (Pharmaceutical Benefits) Regulations 1960 and
National Health Act (Paige et al., 2015). The following report will discuss on medicine
consumption in Australia and the key issues associated with PBS and recommendations which
may aid in possible improvements of the same.
Discussion
Costs and Reasons of Medication Consumption in Australia
The medicinal group of statins record highest cost and usage followed by medicines for
treatment of neurological complications and antiretroviral drugs required for the management of
hepatic conditions like Hepatitis C (Mellish, 2015). Taking insights from the report published by
the Australian Institute of Health and Welfare, medicines like statins, required for the treatment
of high circulatory cholesterol levels and cardiovascular abnormalities have undergone
dispensing in volumes higher than other drugs, amounting to approximately 10 million
prescriptions annual across the years ranging from 2016 to 2017 (Paola, 2019). Of these,
Atorvastatin has been reported to yield the highest usage with an alarming cost of $19. Such high
costs continue to sound ironic considering the presence of PBS whose agenda lies in the
subsidizing the costs of medications for the general public (ABC News. (2019). Followed by
statin usage, antiretroviral drugs for the treatment of Hepatitis C have been recorded to yield
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
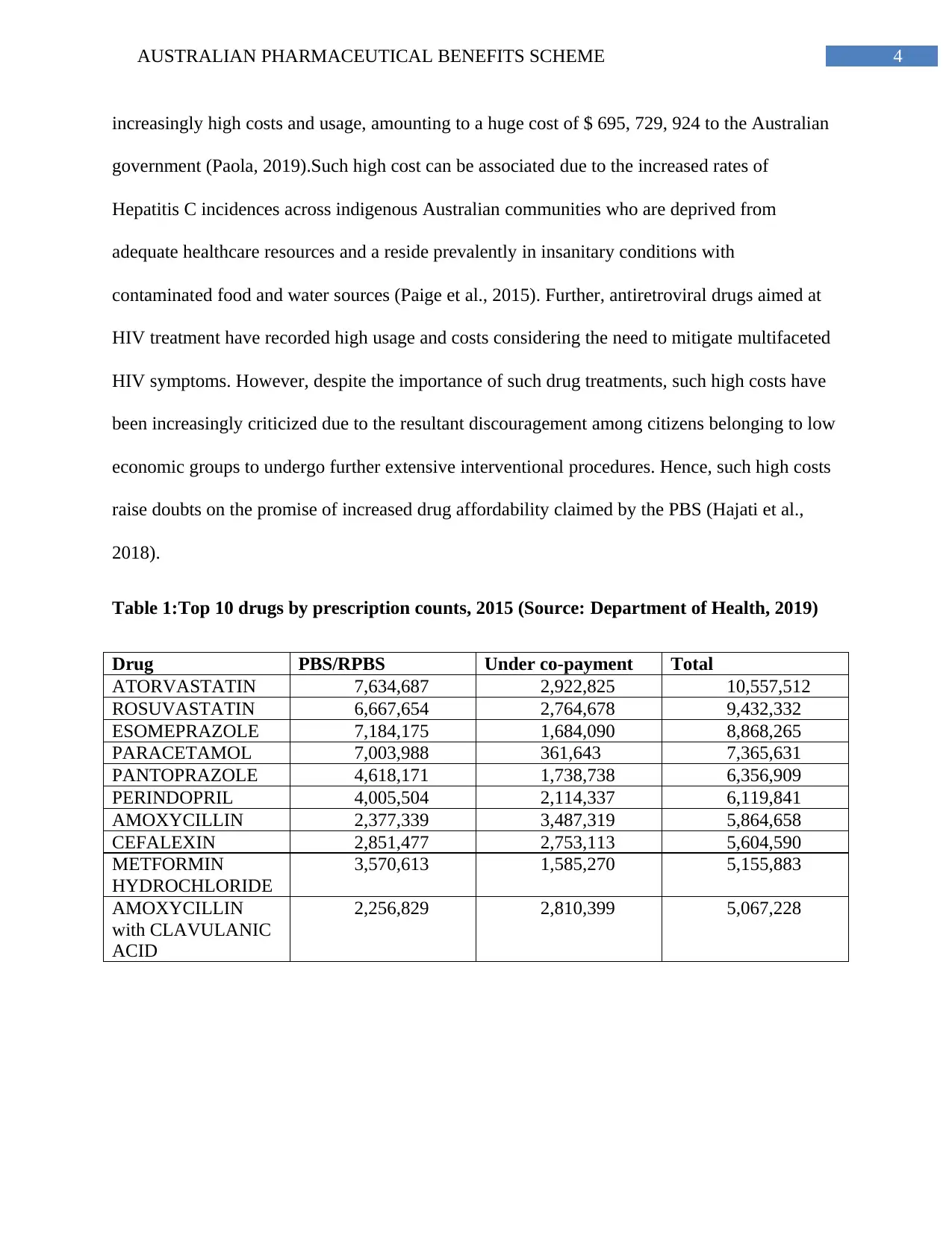
increasingly high costs and usage, amounting to a huge cost of $ 695, 729, 924 to the Australian
government (Paola, 2019).Such high cost can be associated due to the increased rates of
Hepatitis C incidences across indigenous Australian communities who are deprived from
adequate healthcare resources and a reside prevalently in insanitary conditions with
contaminated food and water sources (Paige et al., 2015). Further, antiretroviral drugs aimed at
HIV treatment have recorded high usage and costs considering the need to mitigate multifaceted
HIV symptoms. However, despite the importance of such drug treatments, such high costs have
been increasingly criticized due to the resultant discouragement among citizens belonging to low
economic groups to undergo further extensive interventional procedures. Hence, such high costs
raise doubts on the promise of increased drug affordability claimed by the PBS (Hajati et al.,
2018).
Table 1:Top 10 drugs by prescription counts, 2015 (Source: Department of Health, 2019)
Drug PBS/RPBS Under co-payment Total
ATORVASTATIN 7,634,687 2,922,825 10,557,512
ROSUVASTATIN 6,667,654 2,764,678 9,432,332
ESOMEPRAZOLE 7,184,175 1,684,090 8,868,265
PARACETAMOL 7,003,988 361,643 7,365,631
PANTOPRAZOLE 4,618,171 1,738,738 6,356,909
PERINDOPRIL 4,005,504 2,114,337 6,119,841
AMOXYCILLIN 2,377,339 3,487,319 5,864,658
CEFALEXIN 2,851,477 2,753,113 5,604,590
METFORMIN
HYDROCHLORIDE
3,570,613 1,585,270 5,155,883
AMOXYCILLIN
with CLAVULANIC
ACID
2,256,829 2,810,399 5,067,228
increasingly high costs and usage, amounting to a huge cost of $ 695, 729, 924 to the Australian
government (Paola, 2019).Such high cost can be associated due to the increased rates of
Hepatitis C incidences across indigenous Australian communities who are deprived from
adequate healthcare resources and a reside prevalently in insanitary conditions with
contaminated food and water sources (Paige et al., 2015). Further, antiretroviral drugs aimed at
HIV treatment have recorded high usage and costs considering the need to mitigate multifaceted
HIV symptoms. However, despite the importance of such drug treatments, such high costs have
been increasingly criticized due to the resultant discouragement among citizens belonging to low
economic groups to undergo further extensive interventional procedures. Hence, such high costs
raise doubts on the promise of increased drug affordability claimed by the PBS (Hajati et al.,
2018).
Table 1:Top 10 drugs by prescription counts, 2015 (Source: Department of Health, 2019)
Drug PBS/RPBS Under co-payment Total
ATORVASTATIN 7,634,687 2,922,825 10,557,512
ROSUVASTATIN 6,667,654 2,764,678 9,432,332
ESOMEPRAZOLE 7,184,175 1,684,090 8,868,265
PARACETAMOL 7,003,988 361,643 7,365,631
PANTOPRAZOLE 4,618,171 1,738,738 6,356,909
PERINDOPRIL 4,005,504 2,114,337 6,119,841
AMOXYCILLIN 2,377,339 3,487,319 5,864,658
CEFALEXIN 2,851,477 2,753,113 5,604,590
METFORMIN
HYDROCHLORIDE
3,570,613 1,585,270 5,155,883
AMOXYCILLIN
with CLAVULANIC
ACID
2,256,829 2,810,399 5,067,228
5AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Types of Medicines Consumed
As per the report on Australian Statistics of Medicine (See Table 1 and Table 2),
published by the Department of Health, the following drugs, which have been funded by the
PBS, are generally used extensively and recommended in terms of prescriptions, between the
years 2013 to 2015: drugs for the alimentary tract, for blood formation, for management of
cardiovascular impairments, dermatological drugs, drugs for the genitourinary system, hormonal
preparations, anti-infection drugs, anti-neoplastic drugs, drugs for the musculoskeletal system,
products combating parasites, medicines for the respiratory system and as well as for ensuring
functioning of sensory organs. Of these, drugs for the cardiovascular system, as discussed
previously have recorded highest prescription counts amounting to be 70, 372, 716 in 2013, 68,
145, 369 in 2014 and 66, 613, 110 in 2015 (Department of Health, 2019).Taking insights from
the research by Schilling et al., (2017), which aimed to explore the differences in statin
prescription and usage between Australia and New Zealand, the high uses can be attributed to the
fact that while an absolute risk model is used to prescribe statins, Australian recommendations
involve prescription considering multiple patient risk factors such as LDL cholesterol, total
cholesterol and diabetes.
As researched by Mc Rae et al., (2017), while most drugs have been prescribed and
subsided by the PBS, cancer associated drugs have not undergone PBS prescription and hence
are not discounted. Considering the significant rates of cancer incidences in Australia, this can be
considered as a key disadvantage of PBS. Cancer is chronic and debilitating health condition
with detrimental long term metabolic, psychological and physiological impacts hence requiring
huge financial costs and hindrances to accessibility by patients. Hence, as postulated by Currie,
Chiarella and Buckley (2019), considering the expensive nature of anti-carcinogenic drugs, PBS
Types of Medicines Consumed
As per the report on Australian Statistics of Medicine (See Table 1 and Table 2),
published by the Department of Health, the following drugs, which have been funded by the
PBS, are generally used extensively and recommended in terms of prescriptions, between the
years 2013 to 2015: drugs for the alimentary tract, for blood formation, for management of
cardiovascular impairments, dermatological drugs, drugs for the genitourinary system, hormonal
preparations, anti-infection drugs, anti-neoplastic drugs, drugs for the musculoskeletal system,
products combating parasites, medicines for the respiratory system and as well as for ensuring
functioning of sensory organs. Of these, drugs for the cardiovascular system, as discussed
previously have recorded highest prescription counts amounting to be 70, 372, 716 in 2013, 68,
145, 369 in 2014 and 66, 613, 110 in 2015 (Department of Health, 2019).Taking insights from
the research by Schilling et al., (2017), which aimed to explore the differences in statin
prescription and usage between Australia and New Zealand, the high uses can be attributed to the
fact that while an absolute risk model is used to prescribe statins, Australian recommendations
involve prescription considering multiple patient risk factors such as LDL cholesterol, total
cholesterol and diabetes.
As researched by Mc Rae et al., (2017), while most drugs have been prescribed and
subsided by the PBS, cancer associated drugs have not undergone PBS prescription and hence
are not discounted. Considering the significant rates of cancer incidences in Australia, this can be
considered as a key disadvantage of PBS. Cancer is chronic and debilitating health condition
with detrimental long term metabolic, psychological and physiological impacts hence requiring
huge financial costs and hindrances to accessibility by patients. Hence, as postulated by Currie,
Chiarella and Buckley (2019), considering the expensive nature of anti-carcinogenic drugs, PBS
6AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
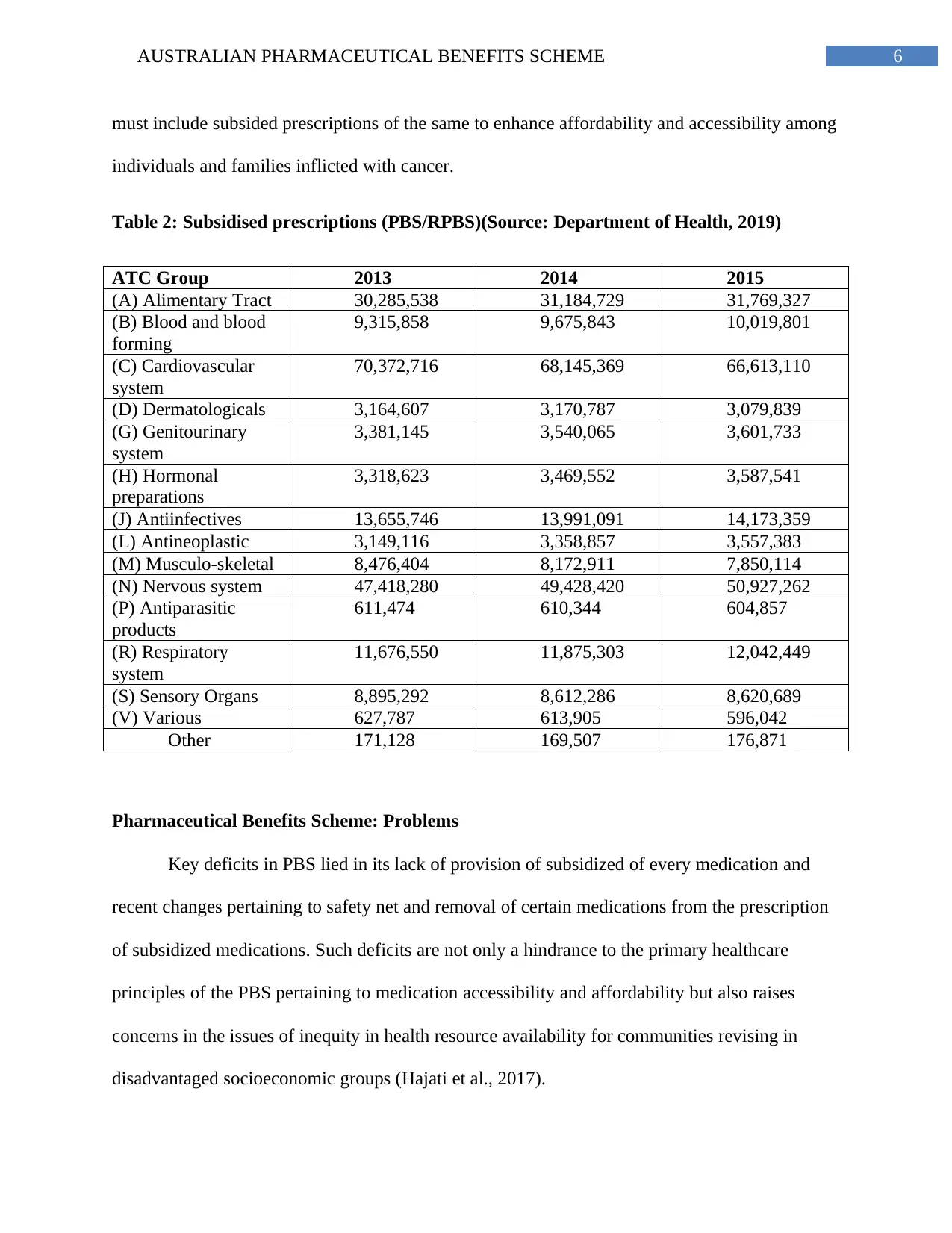
must include subsided prescriptions of the same to enhance affordability and accessibility among
individuals and families inflicted with cancer.
Table 2: Subsidised prescriptions (PBS/RPBS)(Source: Department of Health, 2019)
ATC Group 2013 2014 2015
(A) Alimentary Tract 30,285,538 31,184,729 31,769,327
(B) Blood and blood
forming
9,315,858 9,675,843 10,019,801
(C) Cardiovascular
system
70,372,716 68,145,369 66,613,110
(D) Dermatologicals 3,164,607 3,170,787 3,079,839
(G) Genitourinary
system
3,381,145 3,540,065 3,601,733
(H) Hormonal
preparations
3,318,623 3,469,552 3,587,541
(J) Antiinfectives 13,655,746 13,991,091 14,173,359
(L) Antineoplastic 3,149,116 3,358,857 3,557,383
(M) Musculo-skeletal 8,476,404 8,172,911 7,850,114
(N) Nervous system 47,418,280 49,428,420 50,927,262
(P) Antiparasitic
products
611,474 610,344 604,857
(R) Respiratory
system
11,676,550 11,875,303 12,042,449
(S) Sensory Organs 8,895,292 8,612,286 8,620,689
(V) Various 627,787 613,905 596,042
Other 171,128 169,507 176,871
Pharmaceutical Benefits Scheme: Problems
Key deficits in PBS lied in its lack of provision of subsidized of every medication and
recent changes pertaining to safety net and removal of certain medications from the prescription
of subsidized medications. Such deficits are not only a hindrance to the primary healthcare
principles of the PBS pertaining to medication accessibility and affordability but also raises
concerns in the issues of inequity in health resource availability for communities revising in
disadvantaged socioeconomic groups (Hajati et al., 2017).
must include subsided prescriptions of the same to enhance affordability and accessibility among
individuals and families inflicted with cancer.
Table 2: Subsidised prescriptions (PBS/RPBS)(Source: Department of Health, 2019)
ATC Group 2013 2014 2015
(A) Alimentary Tract 30,285,538 31,184,729 31,769,327
(B) Blood and blood
forming
9,315,858 9,675,843 10,019,801
(C) Cardiovascular
system
70,372,716 68,145,369 66,613,110
(D) Dermatologicals 3,164,607 3,170,787 3,079,839
(G) Genitourinary
system
3,381,145 3,540,065 3,601,733
(H) Hormonal
preparations
3,318,623 3,469,552 3,587,541
(J) Antiinfectives 13,655,746 13,991,091 14,173,359
(L) Antineoplastic 3,149,116 3,358,857 3,557,383
(M) Musculo-skeletal 8,476,404 8,172,911 7,850,114
(N) Nervous system 47,418,280 49,428,420 50,927,262
(P) Antiparasitic
products
611,474 610,344 604,857
(R) Respiratory
system
11,676,550 11,875,303 12,042,449
(S) Sensory Organs 8,895,292 8,612,286 8,620,689
(V) Various 627,787 613,905 596,042
Other 171,128 169,507 176,871
Pharmaceutical Benefits Scheme: Problems
Key deficits in PBS lied in its lack of provision of subsidized of every medication and
recent changes pertaining to safety net and removal of certain medications from the prescription
of subsidized medications. Such deficits are not only a hindrance to the primary healthcare
principles of the PBS pertaining to medication accessibility and affordability but also raises
concerns in the issues of inequity in health resource availability for communities revising in
disadvantaged socioeconomic groups (Hajati et al., 2017).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
As researched by Mellish et al., (2015), one of key problems associated with the PBS are
the relevant absence of certain groups of drugs in the prescribed list of subsidized medications.
Drugs for cancer have not been included in the PBS list of subsidized medications, which can be
considered as a key disadvantage. Cancer medications and associated treatment interventions are
not only expensive but are also difficult for patients to acquire in terms of accessibility. Further,
as researched by Datta Gupta and Wilson (2018), the lack of adequate subsidies on cancer drugs
not only hinder affordability and accessibility for the mainstream public but also result in
alarming consequences and dilemmas for patients belonging to disadvantaged socioeconomic
groups suffering from cancer. Such issues in absence of subsidies often hinder eagerness
towards further engagement in treatment across such patient groups.
Additionally, as researched by Schilling et al., (2017), a key issue of concern can be
observed in the revision of the subsidized list of medications during the year 2016. In 2016, a
wide range of medications were removed from the list of PBS medications which were
subsidized. These included aspirin, electrolytes, laxatives, Panadol Osteo, supplements for folic
acid and iron, skin allergies, reflux, urine test drops, antacids and injections for Vitamin B12.
While such amendments may lead to benefits of cost saving for taxpayers and at an estimated
value of $87 million annually, such raises questions on the impact it will exert for financial
underprivileged individuals and groups who are dependent on the availability of subsidized
medications. As researched by Paige et al., (2015), most of these medications, especially aspirin,
electrolytes or iron and folic acid supplements are basic medications for management or
cardiovascular conditions and general life sustenance which every and any individual may
require, especially considering the high rates of disease and morbidity in across communities
As researched by Mellish et al., (2015), one of key problems associated with the PBS are
the relevant absence of certain groups of drugs in the prescribed list of subsidized medications.
Drugs for cancer have not been included in the PBS list of subsidized medications, which can be
considered as a key disadvantage. Cancer medications and associated treatment interventions are
not only expensive but are also difficult for patients to acquire in terms of accessibility. Further,
as researched by Datta Gupta and Wilson (2018), the lack of adequate subsidies on cancer drugs
not only hinder affordability and accessibility for the mainstream public but also result in
alarming consequences and dilemmas for patients belonging to disadvantaged socioeconomic
groups suffering from cancer. Such issues in absence of subsidies often hinder eagerness
towards further engagement in treatment across such patient groups.
Additionally, as researched by Schilling et al., (2017), a key issue of concern can be
observed in the revision of the subsidized list of medications during the year 2016. In 2016, a
wide range of medications were removed from the list of PBS medications which were
subsidized. These included aspirin, electrolytes, laxatives, Panadol Osteo, supplements for folic
acid and iron, skin allergies, reflux, urine test drops, antacids and injections for Vitamin B12.
While such amendments may lead to benefits of cost saving for taxpayers and at an estimated
value of $87 million annually, such raises questions on the impact it will exert for financial
underprivileged individuals and groups who are dependent on the availability of subsidized
medications. As researched by Paige et al., (2015), most of these medications, especially aspirin,
electrolytes or iron and folic acid supplements are basic medications for management or
cardiovascular conditions and general life sustenance which every and any individual may
require, especially considering the high rates of disease and morbidity in across communities
8AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
residing in low socioeconomic groups. Hence, removal of major medication groups from
subsidies defeats the very purpose the PBS was built upon.
As researched by McRae et al., (2017), an additional issue which can be considered as a
major shortcoming of PBS is the amendment to include a Safety Net 20 day Rule. This revision
of the PBS was undertaken to prevent citizens from availing repeat medication prescriptions of
PBS before than the recommended period. Hence as per the Safety Net 20 day Rule, the supply
of a repeat prescription of drugs within 20 days of the first prescription will not allow citizens to
avail subscriptions but undergo normal charges of patient contribution. This change is a major
issue in terms of the accessibility and affordability of required medications for patients residing
in remote locations or requiring immediate treatment. Often, as researched Paola (2019), availing
of a quick, repeat prescription not only aids in the timely management of emergencies but also
saves time and travel costs for communities located in remote areas by preventing the need to
visit a distant chemist. Hence, such a safety net rule deprives such communities from financial
benefits and turns out to an unnecessarily high expenditure under uncontrolled circumstances for
patients encountering emergencies.
Concluding Recommendations
As researched by Currie, Chiarella and Buckley, 2019), the amendments of revised
medication list and the safety net rule can be considered as advantageous in terms of reducing the
costs for tax payers. However, in criticism, it must be noted that basic healthcare is a right for all
and must be equitable in terms of availability and distribution. Hence, it is recommended that
PBS amendments incorporate specialized considerations for communities in remotes,
economically underprivileged communities and socially disadvantaged communities such as
Aboriginals (Datta Gupta& Wilson, 2018). Further, as per the news article published by ABC
residing in low socioeconomic groups. Hence, removal of major medication groups from
subsidies defeats the very purpose the PBS was built upon.
As researched by McRae et al., (2017), an additional issue which can be considered as a
major shortcoming of PBS is the amendment to include a Safety Net 20 day Rule. This revision
of the PBS was undertaken to prevent citizens from availing repeat medication prescriptions of
PBS before than the recommended period. Hence as per the Safety Net 20 day Rule, the supply
of a repeat prescription of drugs within 20 days of the first prescription will not allow citizens to
avail subscriptions but undergo normal charges of patient contribution. This change is a major
issue in terms of the accessibility and affordability of required medications for patients residing
in remote locations or requiring immediate treatment. Often, as researched Paola (2019), availing
of a quick, repeat prescription not only aids in the timely management of emergencies but also
saves time and travel costs for communities located in remote areas by preventing the need to
visit a distant chemist. Hence, such a safety net rule deprives such communities from financial
benefits and turns out to an unnecessarily high expenditure under uncontrolled circumstances for
patients encountering emergencies.
Concluding Recommendations
As researched by Currie, Chiarella and Buckley, 2019), the amendments of revised
medication list and the safety net rule can be considered as advantageous in terms of reducing the
costs for tax payers. However, in criticism, it must be noted that basic healthcare is a right for all
and must be equitable in terms of availability and distribution. Hence, it is recommended that
PBS amendments incorporate specialized considerations for communities in remotes,
economically underprivileged communities and socially disadvantaged communities such as
Aboriginals (Datta Gupta& Wilson, 2018). Further, as per the news article published by ABC
9AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
news, the report by Grattan institute highlighted that medication costs in Australia are almost 14
times higher as compared to that in New Zealand, Canada and the United Kingdom(ABC News.
(2019). While comparisons with other nationalities defeats the consideration of the unique
socioeconomic situation of a concerned country, it is however recommended that the government
take note of these comparisons to rectify and restore the true principle of medication coverage
underlying the PBS. Hence, PBS issues in terms of high prices, limited prescription of
medications and safety net rule must be suited to unique needs of disadvantaged communities
and clinical emergencies.
news, the report by Grattan institute highlighted that medication costs in Australia are almost 14
times higher as compared to that in New Zealand, Canada and the United Kingdom(ABC News.
(2019). While comparisons with other nationalities defeats the consideration of the unique
socioeconomic situation of a concerned country, it is however recommended that the government
take note of these comparisons to rectify and restore the true principle of medication coverage
underlying the PBS. Hence, PBS issues in terms of high prices, limited prescription of
medications and safety net rule must be suited to unique needs of disadvantaged communities
and clinical emergencies.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
References
ABC News. (2019). Australians paying 14 times more for prescription drugs. Retrieved from
https://www.abc.net.au/news/2013-12-02/australians-paying-14-times-more-for-
prescription-drugs/5128028.
Currie, J., Chiarella, M., & Buckley, T. (2019). Privately practising nurse practitioners’ provision
of care subsidised through the Medicare Benefits Schedule and the Pharmaceutical
Benefits Scheme in Australia: results from a national survey. Australian Health Review,
43(1), 55-61.doi: https://doi.org/10.1071/AH17130.
Datta Gupta, A., & Wilson, D. H. (2018). Botulinum toxin for spasticity: A case for change to
the Pharmaceutical Benefits Scheme. Medical Journal of Australia, 208(9), 379-381.doi:
https://doi.org/10.5694/mja17.00841.
Department of Health. (2019). Pharmaceutical Benefits Scheme (PBS) | Australian Statistics on
Medicines 2015. Retrieved from http://www.pbs.gov.au/info/statistics/asm/asm-2015.
Hajati, F., Atlantis, E., Bell, K. J., &Girosi, F. (2018). Patterns and trends of potentially
inappropriate high-density lipoprotein cholesterol testing in Australian adults at high risk
of cardiovascular disease from 2008 to 2014: analysis of linked individual patient data
from the Australian Medicare Benefits Schedule and Pharmaceutical Benefits Scheme.
BMJ open, 8(3), e019041.doi: http://dx.doi.org/10.1136/bmjopen-2017-019041.
McRae, I., van Gool, K., Hall, J., & Yen, L. (2017). Role of Cost on Failure to Access Prescribed
Pharmaceuticals: The Case of Statins. Applied health economics and health policy, 15(5),
625-634.doi: https://doi.org/10.1007/s40258-017-0336-8.
References
ABC News. (2019). Australians paying 14 times more for prescription drugs. Retrieved from
https://www.abc.net.au/news/2013-12-02/australians-paying-14-times-more-for-
prescription-drugs/5128028.
Currie, J., Chiarella, M., & Buckley, T. (2019). Privately practising nurse practitioners’ provision
of care subsidised through the Medicare Benefits Schedule and the Pharmaceutical
Benefits Scheme in Australia: results from a national survey. Australian Health Review,
43(1), 55-61.doi: https://doi.org/10.1071/AH17130.
Datta Gupta, A., & Wilson, D. H. (2018). Botulinum toxin for spasticity: A case for change to
the Pharmaceutical Benefits Scheme. Medical Journal of Australia, 208(9), 379-381.doi:
https://doi.org/10.5694/mja17.00841.
Department of Health. (2019). Pharmaceutical Benefits Scheme (PBS) | Australian Statistics on
Medicines 2015. Retrieved from http://www.pbs.gov.au/info/statistics/asm/asm-2015.
Hajati, F., Atlantis, E., Bell, K. J., &Girosi, F. (2018). Patterns and trends of potentially
inappropriate high-density lipoprotein cholesterol testing in Australian adults at high risk
of cardiovascular disease from 2008 to 2014: analysis of linked individual patient data
from the Australian Medicare Benefits Schedule and Pharmaceutical Benefits Scheme.
BMJ open, 8(3), e019041.doi: http://dx.doi.org/10.1136/bmjopen-2017-019041.
McRae, I., van Gool, K., Hall, J., & Yen, L. (2017). Role of Cost on Failure to Access Prescribed
Pharmaceuticals: The Case of Statins. Applied health economics and health policy, 15(5),
625-634.doi: https://doi.org/10.1007/s40258-017-0336-8.
11AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Mellish, L., Karanges, E. A., Litchfield, M. J., Schaffer, A. L., Blanch, B., Daniels, B. J., ... &
Pearson, S. A. (2015). The Australian Pharmaceutical Benefits Scheme data collection: a
practical guide for researchers. BMC research notes, 8(1), 634.doi:
https://doi.org/10.1186/s13104-015-1616-8.
Paige, E., Kemp-Casey, A., Korda, R., & Banks, E. (2015). Using Australian Pharmaceutical
Benefits Scheme data for pharmacoepidemiological research: challenges and
approaches.doi: https://doi.org/10.17061/phrp2541546.
Paola, S. (2019). 10 latest stats on medicine use in Australia | AJP. Retrieved from
https://ajp.com.au/news/10-latest-stats-on-medicine-use-in-australia/.
Schilling, C., Knight, J., Mortimer, D., Petrie, D., Clarke, P., Chalmers, J., ...& Jackson, R.
(2017). Australian general practitioners initiate statin therapy primarily on the basis of
lipid levels; New Zealand general practitioners use absolute risk. Health Policy, 121(12),
1233-1239.doi: https://doi.org/10.1016/j.healthpol.2017.09.022.
Mellish, L., Karanges, E. A., Litchfield, M. J., Schaffer, A. L., Blanch, B., Daniels, B. J., ... &
Pearson, S. A. (2015). The Australian Pharmaceutical Benefits Scheme data collection: a
practical guide for researchers. BMC research notes, 8(1), 634.doi:
https://doi.org/10.1186/s13104-015-1616-8.
Paige, E., Kemp-Casey, A., Korda, R., & Banks, E. (2015). Using Australian Pharmaceutical
Benefits Scheme data for pharmacoepidemiological research: challenges and
approaches.doi: https://doi.org/10.17061/phrp2541546.
Paola, S. (2019). 10 latest stats on medicine use in Australia | AJP. Retrieved from
https://ajp.com.au/news/10-latest-stats-on-medicine-use-in-australia/.
Schilling, C., Knight, J., Mortimer, D., Petrie, D., Clarke, P., Chalmers, J., ...& Jackson, R.
(2017). Australian general practitioners initiate statin therapy primarily on the basis of
lipid levels; New Zealand general practitioners use absolute risk. Health Policy, 121(12),
1233-1239.doi: https://doi.org/10.1016/j.healthpol.2017.09.022.
1 out of 12
Related Documents



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.