Australia's Pharmaceutical Landscape
VerifiedAdded on 2020/02/24
|14
|2124
|56
AI Summary
This assignment examines the complexities of the pharmaceutical landscape in Australia. It delves into issues surrounding drug pricing, accessibility, and affordability, highlighting the impact on patients' well-being and the healthcare system's sustainability. The document specifically addresses the Pharmaceutical Benefits Scheme (PBS), its effectiveness in ensuring equitable access to medications, and the need for reforms to address rising costs and promote greater affordability.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
The Australian Pharmaceutical Benefits Scheme and the Consumption of Medicines in
Australia
Name of the Student
Name of the University
Author Note
The Australian Pharmaceutical Benefits Scheme and the Consumption of Medicines in
Australia
Name of the Student
Name of the University
Author Note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Highest consumption rates of medicines occurs mostly in Australia in comparison to
the other countries round the world. The Pharmaceutical Benefits Scheme (PBS) scheme is
designed to fund the medical costing of the general community. The scheme is thought to be
helpful because it provides the general race of the Australian population to get an easy access
of the commonly prescribed medicines which are widely available in the market, affordable
and at the same time have acceptable standards. However, the cost of the PBS that has been
exclusively designed to help the ex-service men women in Australia is increasing each year
(Duckett et al., 2013). The following essay sheds lights on the cost of the medicine
consumption in Australia via detailed analysis of the PBS scheme. The essay also tries to
elucidate the shortcomings of the PBS and the possible recommendation.
The Scenario of the Cost of Medicine Consumption in Australia
In order to speak about the cost of the medicine consumption in Australia, the first
thing which comes into consideration is PBS. The Pharmaceutical Benefit Scheme (PBS) is
one of the major schemes that define the various aspects of the Australian health care system.
The Government of Australia have subsidised the cost of the broad range of the prescript
medications for all the residents of Australia who possess the Medical cards (Blanch, Pearson
& Haber, 2014). The consumers in the country only pays a set form of price that are been
protected from the high costs by the arrangements of the safety nets. The major part of the
medicines are that comes under the Pharmaceutical Benefit Scheme are generally dispensed
through the pharmacies of the community. However, some of the medicines does not comes
under PBS, are only available at the country hospitals.
The government with all its persuasions have been observing the growth of the
Pharmaceutical Benefits Scheme (PBS). In past ten years between 1994 to 1995 and 2004 to
2005, the costs of the PBS have grown nearly about 13 percent every year. The growths have
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Highest consumption rates of medicines occurs mostly in Australia in comparison to
the other countries round the world. The Pharmaceutical Benefits Scheme (PBS) scheme is
designed to fund the medical costing of the general community. The scheme is thought to be
helpful because it provides the general race of the Australian population to get an easy access
of the commonly prescribed medicines which are widely available in the market, affordable
and at the same time have acceptable standards. However, the cost of the PBS that has been
exclusively designed to help the ex-service men women in Australia is increasing each year
(Duckett et al., 2013). The following essay sheds lights on the cost of the medicine
consumption in Australia via detailed analysis of the PBS scheme. The essay also tries to
elucidate the shortcomings of the PBS and the possible recommendation.
The Scenario of the Cost of Medicine Consumption in Australia
In order to speak about the cost of the medicine consumption in Australia, the first
thing which comes into consideration is PBS. The Pharmaceutical Benefit Scheme (PBS) is
one of the major schemes that define the various aspects of the Australian health care system.
The Government of Australia have subsidised the cost of the broad range of the prescript
medications for all the residents of Australia who possess the Medical cards (Blanch, Pearson
& Haber, 2014). The consumers in the country only pays a set form of price that are been
protected from the high costs by the arrangements of the safety nets. The major part of the
medicines are that comes under the Pharmaceutical Benefit Scheme are generally dispensed
through the pharmacies of the community. However, some of the medicines does not comes
under PBS, are only available at the country hospitals.
The government with all its persuasions have been observing the growth of the
Pharmaceutical Benefits Scheme (PBS). In past ten years between 1994 to 1995 and 2004 to
2005, the costs of the PBS have grown nearly about 13 percent every year. The growths have
2
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
also slowed down and the average annual growth rates have fallen down by 4.86 percent from
the year 2005 -06 to the year 2013-14 (Chrysant, 2016). The more recent form of the
expenditure has revised its expenditure and it has slowed down in the recent years. The
Parliament Budget office has predicted that the rise in the growth will be around 4 to 5
percent annually for the longer term. The slower form of growth in the expenditure of PBS
have been attributed in the parts that have the impacts on the discrete policies of pricing and
the co payments and the safety nets that have been introduced in the year 2005.
Despite having the overall trend towards the huge form of contractions in the growth
of Pharmaceutical Benefits Scheme, there is several number of programs of the
Pharmaceutical Benefits Scheme that have been showing the average rates of the growth
(Chrysant, 2016). Most importantly, the efficient funding for Chemotherapy has an annual
growth rate about 62.61%. Moreover, the highly specialized forms of the drug program have
an increased form of the growth of about 6.38% annually (Lal et al., 2017). This form of the
increase has been noted in the recent form of the reports that have been trending on the
increase in the growth by the department of the Health and by Medicines, Australia. This
report has suggested that these programs have been largely unaffected by the vast amount of
the changes of the co payments that have been introduced in the year 2005.
The drugs that are been listed under the Pharmaceutical Benefits scheme should be
clinically very much cost effective. However, some of the drugs are used for the treatments of
the rare form of the diseases that does not meet all of these criteria (Lal et al., 2017).
However, it has been observed that the medicines are clinically very effective, they are
expensive at a prohibitive rate and rarely very much cost effective. The Life Saving Drugs
Program (LSDP) bestows significant financial assistance to the patients who are in an urgent
need of expensive and ‘life saving’ drugs which are not listed under the PBS.
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
also slowed down and the average annual growth rates have fallen down by 4.86 percent from
the year 2005 -06 to the year 2013-14 (Chrysant, 2016). The more recent form of the
expenditure has revised its expenditure and it has slowed down in the recent years. The
Parliament Budget office has predicted that the rise in the growth will be around 4 to 5
percent annually for the longer term. The slower form of growth in the expenditure of PBS
have been attributed in the parts that have the impacts on the discrete policies of pricing and
the co payments and the safety nets that have been introduced in the year 2005.
Despite having the overall trend towards the huge form of contractions in the growth
of Pharmaceutical Benefits Scheme, there is several number of programs of the
Pharmaceutical Benefits Scheme that have been showing the average rates of the growth
(Chrysant, 2016). Most importantly, the efficient funding for Chemotherapy has an annual
growth rate about 62.61%. Moreover, the highly specialized forms of the drug program have
an increased form of the growth of about 6.38% annually (Lal et al., 2017). This form of the
increase has been noted in the recent form of the reports that have been trending on the
increase in the growth by the department of the Health and by Medicines, Australia. This
report has suggested that these programs have been largely unaffected by the vast amount of
the changes of the co payments that have been introduced in the year 2005.
The drugs that are been listed under the Pharmaceutical Benefits scheme should be
clinically very much cost effective. However, some of the drugs are used for the treatments of
the rare form of the diseases that does not meet all of these criteria (Lal et al., 2017).
However, it has been observed that the medicines are clinically very effective, they are
expensive at a prohibitive rate and rarely very much cost effective. The Life Saving Drugs
Program (LSDP) bestows significant financial assistance to the patients who are in an urgent
need of expensive and ‘life saving’ drugs which are not listed under the PBS.
3
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
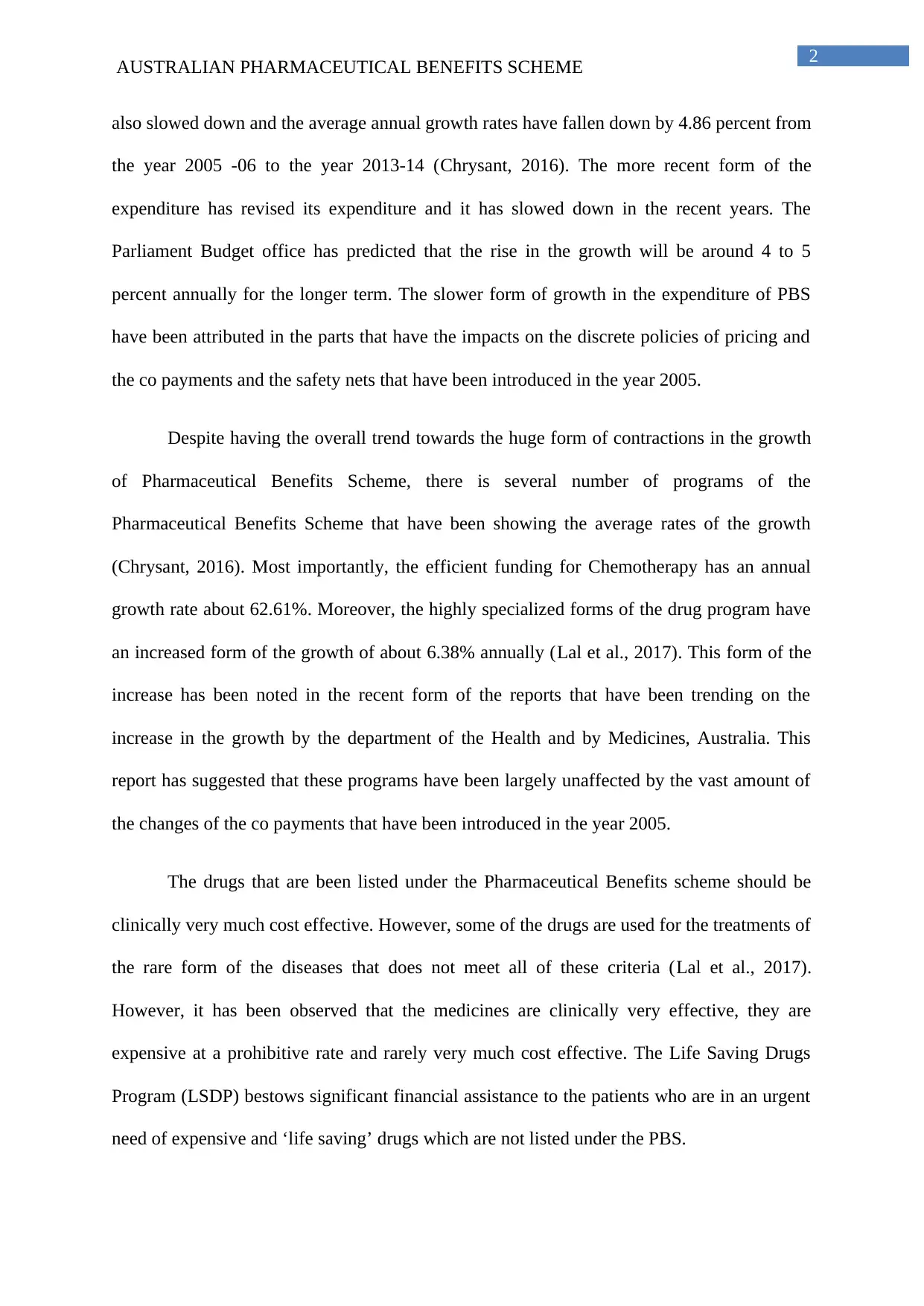
Figure 1: The table shows the annual price increase of the Drugs
Source: http://tommytoy.typepad.com/.a/6a0133f3a4072c970b014e5f20aa6f970c-popup
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Figure 1: The table shows the annual price increase of the Drugs
Source: http://tommytoy.typepad.com/.a/6a0133f3a4072c970b014e5f20aa6f970c-popup
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
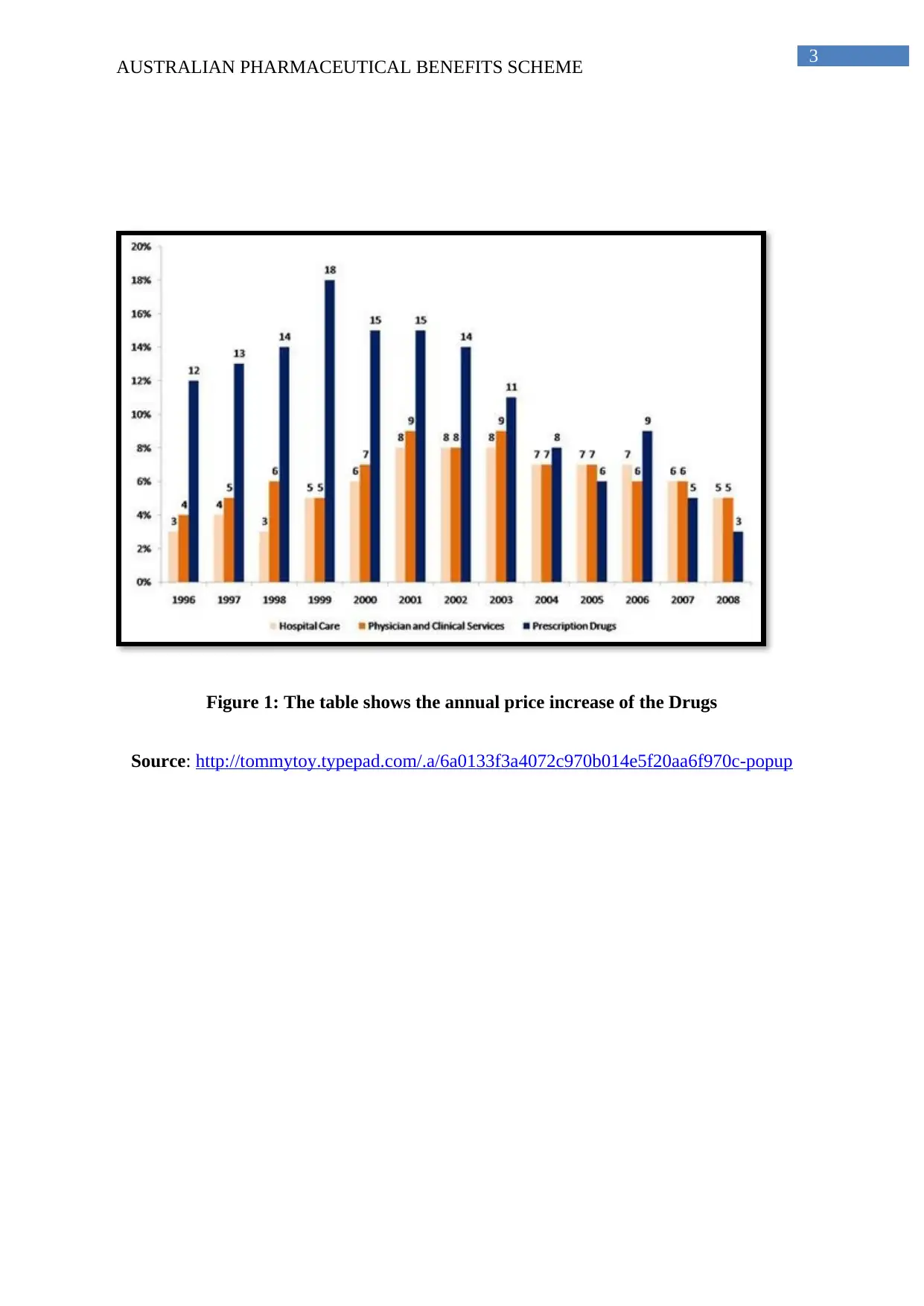
Source: http://tommytoy.typepad.com/.a/6a0133f3a4072c970b0147e27b6fab970b-popup
Figure 2: The table shows the US and the Europe Drug company trackers
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Source: http://tommytoy.typepad.com/.a/6a0133f3a4072c970b0147e27b6fab970b-popup
Figure 2: The table shows the US and the Europe Drug company trackers
5
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
6
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
8
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
9
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Pharmaceutical Benefits Scheme of Australia: In the Australian sub-continent, the
community prescription or private prescription that are dispensed from the non-public
hospitals are either funded by the patients or by the private health insurer under which the
patient’s health scheme is being covered. Sometimes the cost of these medicines prescribed in
such private prescriptions is also funded by the two subsidised schemes funded exclusively
by the Australian government--- the Pharmaceutical Benefits Scheme (PBS) and the
Repatriation Pharmaceutical Benefits Scheme (RPBS). PBS scheme is designed to fund the
medical costing of the general community and RPBS scheme is designed exclusively by for
retired servicemen and women. The schemes are thought to be helpful because it provides the
general race of the Australian population to get an easy access of the commonly prescribed
medicines which are widely available in the market, affordable and at the same time have
acceptable standards.
Australia records highest incidence of cancer in the world (Gleeson, Tienhaara &
Faunce, 2012; Torre et al., 2012). The cost of More than 100 cancer medicines are been
subsidised under the PBS of Australia. Moreover, the Community Affairs Reference
Committee is constantly examining the list of the cancer drugs in order to keep these life
saving medicines affordable and available to patients in the face of the escalating cost to the
government. It is due to the PBS scheme that Australia has been successful in providing some
of the best cancer survival outcomes round the world. Affordable and timely access to the
new and improved cancer drugs is the key to this success and credit for this goes to the
subsidised rate provided by the government under the PBS (Scheme, 2014).
The according to a report published by The Guardian on 18th September 2015,
“Cancer medicines account for one in every six dollars expended through the Scheme, up
from one in eight dollars in 2012-13”. However, several questions have been raised against
the procedure that has been implemented by the Pharmaceutical Benefits Advisory
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Pharmaceutical Benefits Scheme of Australia: In the Australian sub-continent, the
community prescription or private prescription that are dispensed from the non-public
hospitals are either funded by the patients or by the private health insurer under which the
patient’s health scheme is being covered. Sometimes the cost of these medicines prescribed in
such private prescriptions is also funded by the two subsidised schemes funded exclusively
by the Australian government--- the Pharmaceutical Benefits Scheme (PBS) and the
Repatriation Pharmaceutical Benefits Scheme (RPBS). PBS scheme is designed to fund the
medical costing of the general community and RPBS scheme is designed exclusively by for
retired servicemen and women. The schemes are thought to be helpful because it provides the
general race of the Australian population to get an easy access of the commonly prescribed
medicines which are widely available in the market, affordable and at the same time have
acceptable standards.
Australia records highest incidence of cancer in the world (Gleeson, Tienhaara &
Faunce, 2012; Torre et al., 2012). The cost of More than 100 cancer medicines are been
subsidised under the PBS of Australia. Moreover, the Community Affairs Reference
Committee is constantly examining the list of the cancer drugs in order to keep these life
saving medicines affordable and available to patients in the face of the escalating cost to the
government. It is due to the PBS scheme that Australia has been successful in providing some
of the best cancer survival outcomes round the world. Affordable and timely access to the
new and improved cancer drugs is the key to this success and credit for this goes to the
subsidised rate provided by the government under the PBS (Scheme, 2014).
The according to a report published by The Guardian on 18th September 2015,
“Cancer medicines account for one in every six dollars expended through the Scheme, up
from one in eight dollars in 2012-13”. However, several questions have been raised against
the procedure that has been implemented by the Pharmaceutical Benefits Advisory
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Committee (PBAC) in drafting the medicine subsidy recommendations in the scheme.
According to the recent report published by committee, a thorough review of the cancer
medicine data is an urgent requirement. Moreover, they also stated that PBAC must publicly
make this cancer drug submission so that the community who is actually hiring this
subsidised benefits can provided their reviews and join into a discussion centring real
benefits, harm and the cost of these life saving drugs.
In holding such discussion , the real challenge is explaining or finding the actual yet
acceptable reason behind the escalating cost of these life saving cancer drugs and how or
what basis of calculations their cost is being subsidised. The PBS scheme subsidise the
medicine on the basis of their cost however, they did not take into account the efficacy of the
medicines. Under the efficacy of the medicines there lies two principal factors; one is how
often the medicine is being used (demand in the market) and what outcome it is providing to
the patient and its side-effects (the success rate of the medicine). In short, the PBS must align
the prices if the cancer medicine as per the patient’s outcome. There has been a huge
transformation in the field of the cancer research with the advent of new yet effective
medicines in recent years. Now if the thought process of PBS is aligned on the financial
rewards associated with the medicines, overlooking the efficacy, then there is a risk to
innovation (Blanch, Pearson & Haber, 2014; Vitry & Roughead, 2014)
PBS scheme in order to cover more and more cancer drugs under the subsidised
schemes, they must excluded the painkillers and antacids form the subsidised charts.
However, painkillers and antacids are too required in a high rate by the general community
but these are different varieties of these medicines available in the market and are quite
affordable. On the other hand, the cancer drugs are life savings, there are only single variety
and are always on affordable by the general community, ex-servicemen and women. Thus the
committee members, working under the PBs scheme must work together to make the system
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Committee (PBAC) in drafting the medicine subsidy recommendations in the scheme.
According to the recent report published by committee, a thorough review of the cancer
medicine data is an urgent requirement. Moreover, they also stated that PBAC must publicly
make this cancer drug submission so that the community who is actually hiring this
subsidised benefits can provided their reviews and join into a discussion centring real
benefits, harm and the cost of these life saving drugs.
In holding such discussion , the real challenge is explaining or finding the actual yet
acceptable reason behind the escalating cost of these life saving cancer drugs and how or
what basis of calculations their cost is being subsidised. The PBS scheme subsidise the
medicine on the basis of their cost however, they did not take into account the efficacy of the
medicines. Under the efficacy of the medicines there lies two principal factors; one is how
often the medicine is being used (demand in the market) and what outcome it is providing to
the patient and its side-effects (the success rate of the medicine). In short, the PBS must align
the prices if the cancer medicine as per the patient’s outcome. There has been a huge
transformation in the field of the cancer research with the advent of new yet effective
medicines in recent years. Now if the thought process of PBS is aligned on the financial
rewards associated with the medicines, overlooking the efficacy, then there is a risk to
innovation (Blanch, Pearson & Haber, 2014; Vitry & Roughead, 2014)
PBS scheme in order to cover more and more cancer drugs under the subsidised
schemes, they must excluded the painkillers and antacids form the subsidised charts.
However, painkillers and antacids are too required in a high rate by the general community
but these are different varieties of these medicines available in the market and are quite
affordable. On the other hand, the cancer drugs are life savings, there are only single variety
and are always on affordable by the general community, ex-servicemen and women. Thus the
committee members, working under the PBs scheme must work together to make the system
11
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
more equitable. The government must also come forward and examine all the available
pathways inn order t accelerate the registration and listing of the newly discovered cancer
drugs for this they must cite the assessments performed by the other overseas regulators
(Davey, 2017; Clarke, 2012).
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
more equitable. The government must also come forward and examine all the available
pathways inn order t accelerate the registration and listing of the newly discovered cancer
drugs for this they must cite the assessments performed by the other overseas regulators
(Davey, 2017; Clarke, 2012).
12
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Reference List
Australian Statistics on Medicines 2015. (2017) (1st ed., pp. 1,2). Australia. Retrieved from
http://www.pbs.gov.au/statistics/asm/2015/australian-statistics-on-medicines-2015.pdf
Blanch, B., Pearson, S. A., & Haber, P. S. (2014). An overview of the patterns of prescription
opioid use, costs and related harms in Australia. British journal of clinical
pharmacology, 78(5), 1159-1166.
Chrysant, S. G. (2016). The clinical significance and costs of herbs and food supplements
used by complementary and alternative medicine for the treatment of cardiovascular
diseases and hypertension. Journal of human hypertension, 30(1), 1.
Clarke, P. M. (2012). Challenges and opportunities for the Pharmaceutical Benefits
Scheme. The Medical journal of Australia, 196(3), 153-154.
Davey, M. (2017). Pharmaceutical Benefits Scheme becoming unsustainable, says Senate
committee. the Guardian. Retrieved 1 September 2017, from
https://www.theguardian.com/society/2015/sep/18/pharmaceutical-benefits-scheme-
becoming-unsustainable-says-senate-committee
Duckett, S. J., Breadon, P., Ginnivan, L., & Venkataraman, P. (2013). Australia's bad drug
deal: high pharmaceutical prices. Melbourne: Grattan Institute.
Gleeson, D., Tienhaara, K., & Faunce, T. (2012). Challenges to Australia's national health
policy from trade and investment agreements.
Iyengar, S., Tay-Teo, K., Vogler, S., Beyer, P., Wiktor, S., de Joncheere, K., & Hill, S.
(2016). Prices, costs, and affordability of new medicines for hepatitis C in 30
countries: an economic analysis. PLoS Medicine, 13(5), e1002032.
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Reference List
Australian Statistics on Medicines 2015. (2017) (1st ed., pp. 1,2). Australia. Retrieved from
http://www.pbs.gov.au/statistics/asm/2015/australian-statistics-on-medicines-2015.pdf
Blanch, B., Pearson, S. A., & Haber, P. S. (2014). An overview of the patterns of prescription
opioid use, costs and related harms in Australia. British journal of clinical
pharmacology, 78(5), 1159-1166.
Chrysant, S. G. (2016). The clinical significance and costs of herbs and food supplements
used by complementary and alternative medicine for the treatment of cardiovascular
diseases and hypertension. Journal of human hypertension, 30(1), 1.
Clarke, P. M. (2012). Challenges and opportunities for the Pharmaceutical Benefits
Scheme. The Medical journal of Australia, 196(3), 153-154.
Davey, M. (2017). Pharmaceutical Benefits Scheme becoming unsustainable, says Senate
committee. the Guardian. Retrieved 1 September 2017, from
https://www.theguardian.com/society/2015/sep/18/pharmaceutical-benefits-scheme-
becoming-unsustainable-says-senate-committee
Duckett, S. J., Breadon, P., Ginnivan, L., & Venkataraman, P. (2013). Australia's bad drug
deal: high pharmaceutical prices. Melbourne: Grattan Institute.
Gleeson, D., Tienhaara, K., & Faunce, T. (2012). Challenges to Australia's national health
policy from trade and investment agreements.
Iyengar, S., Tay-Teo, K., Vogler, S., Beyer, P., Wiktor, S., de Joncheere, K., & Hill, S.
(2016). Prices, costs, and affordability of new medicines for hepatitis C in 30
countries: an economic analysis. PLoS Medicine, 13(5), e1002032.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Lal, A., Mantilla-Herrera, A. M., Veerman, L., Backholer, K., Sacks, G., Moodie, M., ... &
Peeters, A. (2017). Modelled health benefits of a sugar-sweetened beverage tax across
different socioeconomic groups in Australia: A cost-effectiveness and equity
analysis. PLoS medicine, 14(6), e1002326.
Scheme, P. B. (2014). Australian Government.
Torre, L. A., Bray, F., Siegel, R. L., Ferlay, J., Lortet‐Tieulent, J., & Jemal, A. (2015). Global
cancer statistics, 2012. CA: a cancer journal for clinicians, 65(2), 87-108.
Vitry, A., & Roughead, E. (2014). Managed entry agreements for pharmaceuticals in
Australia. Health Policy, 117(3), 345-352.
AUSTRALIAN PHARMACEUTICAL BENEFITS SCHEME
Lal, A., Mantilla-Herrera, A. M., Veerman, L., Backholer, K., Sacks, G., Moodie, M., ... &
Peeters, A. (2017). Modelled health benefits of a sugar-sweetened beverage tax across
different socioeconomic groups in Australia: A cost-effectiveness and equity
analysis. PLoS medicine, 14(6), e1002326.
Scheme, P. B. (2014). Australian Government.
Torre, L. A., Bray, F., Siegel, R. L., Ferlay, J., Lortet‐Tieulent, J., & Jemal, A. (2015). Global
cancer statistics, 2012. CA: a cancer journal for clinicians, 65(2), 87-108.
Vitry, A., & Roughead, E. (2014). Managed entry agreements for pharmaceuticals in
Australia. Health Policy, 117(3), 345-352.
1 out of 14
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.