Case Study: Investigating Binge Drinking and Stroke in Driscoville
VerifiedAdded on 2023/06/12
|10
|1385
|286
Case Study
AI Summary
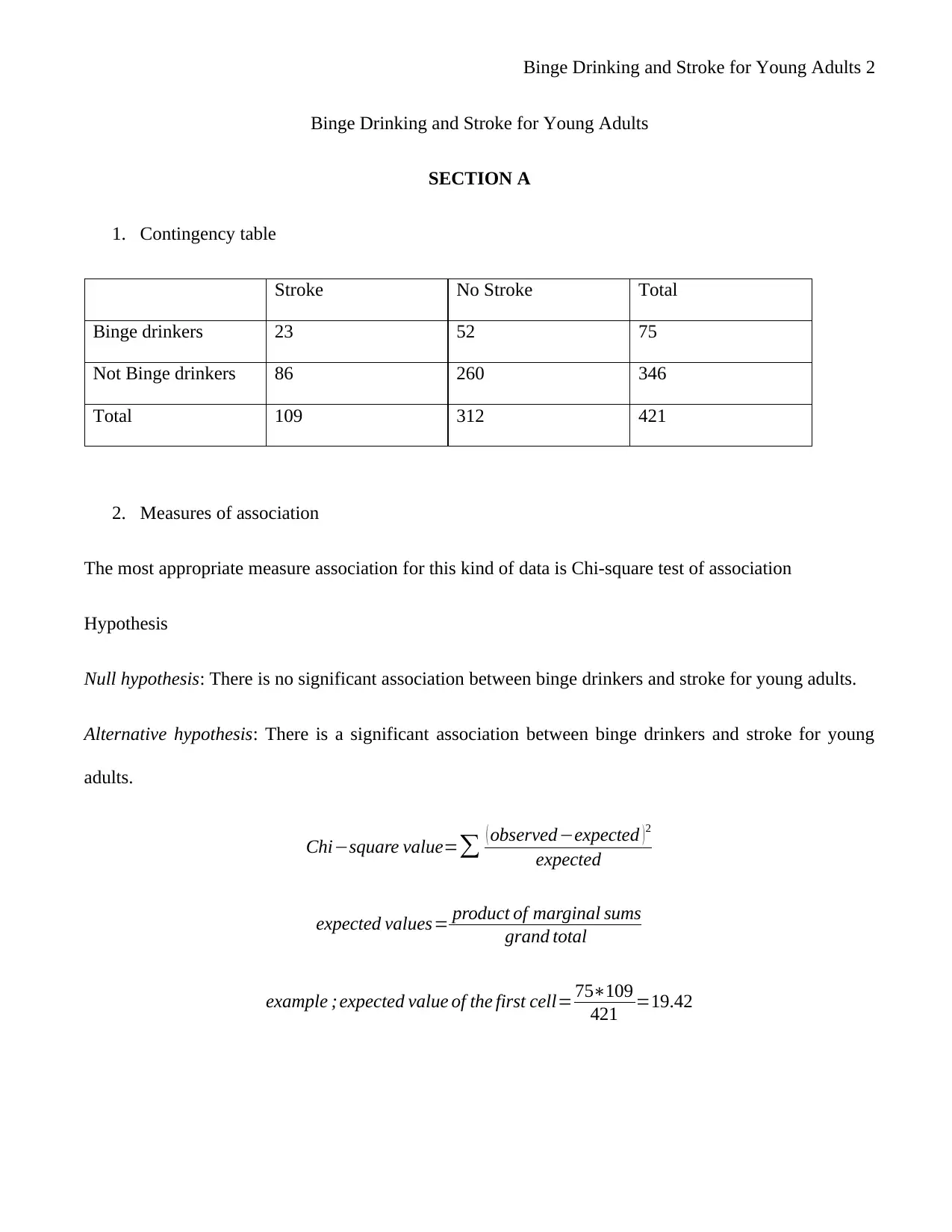
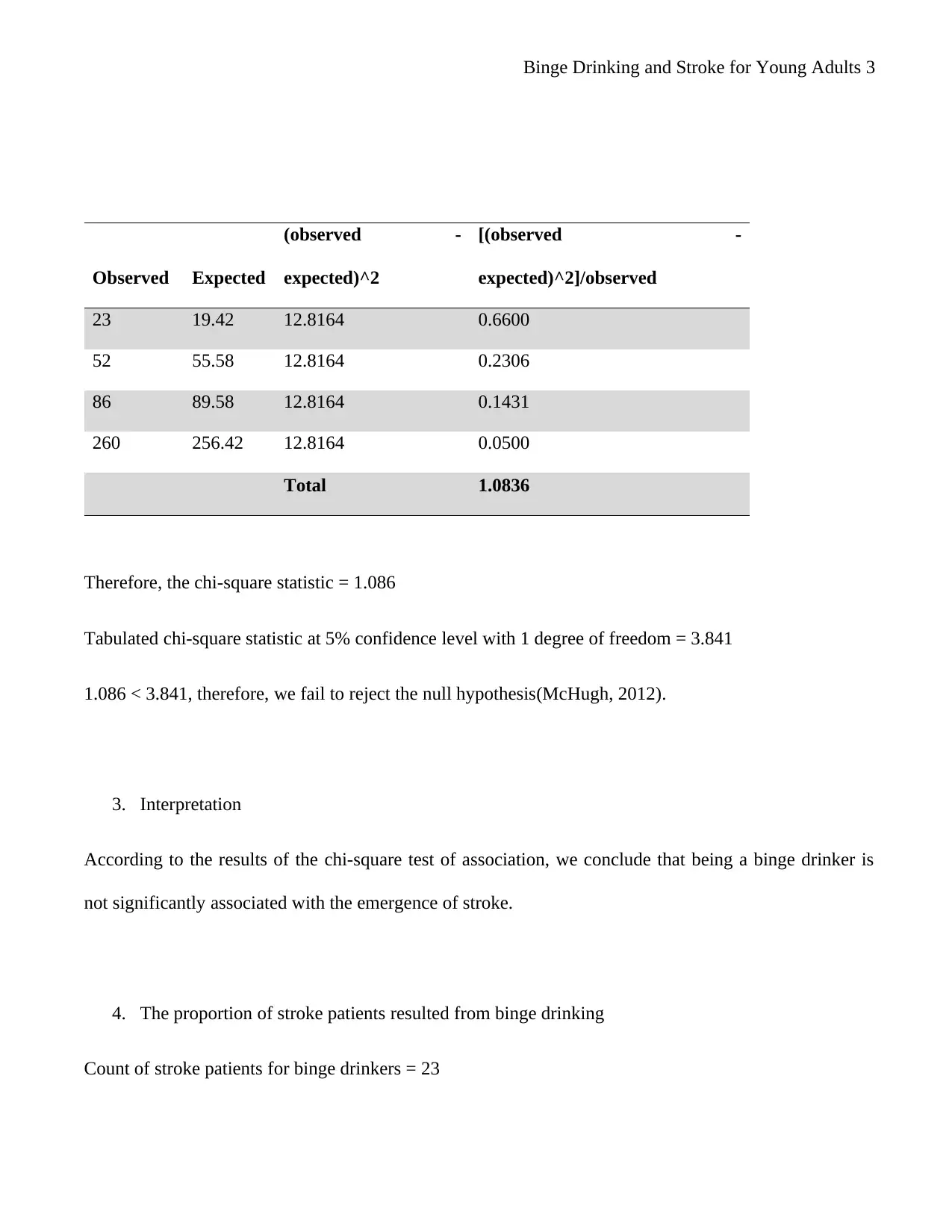
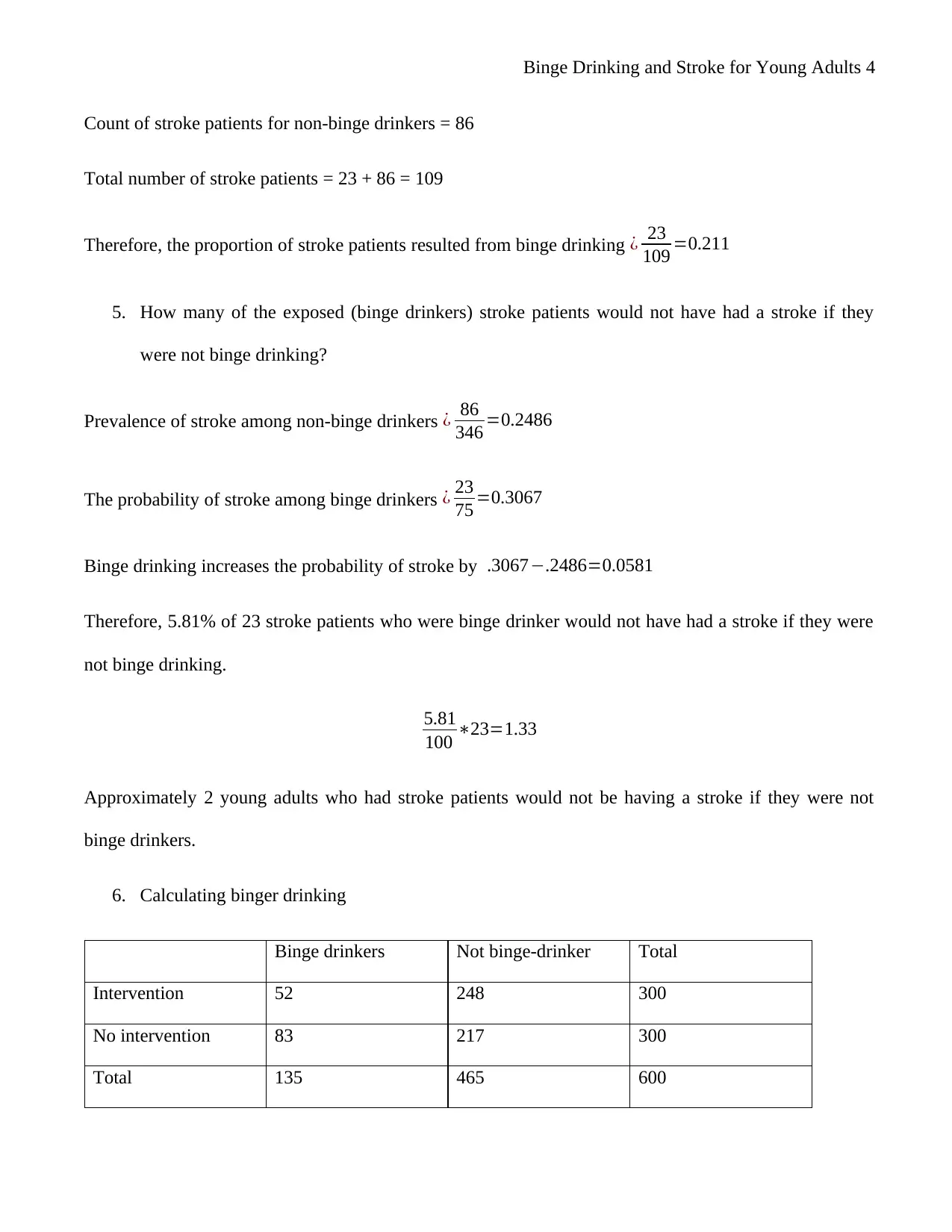
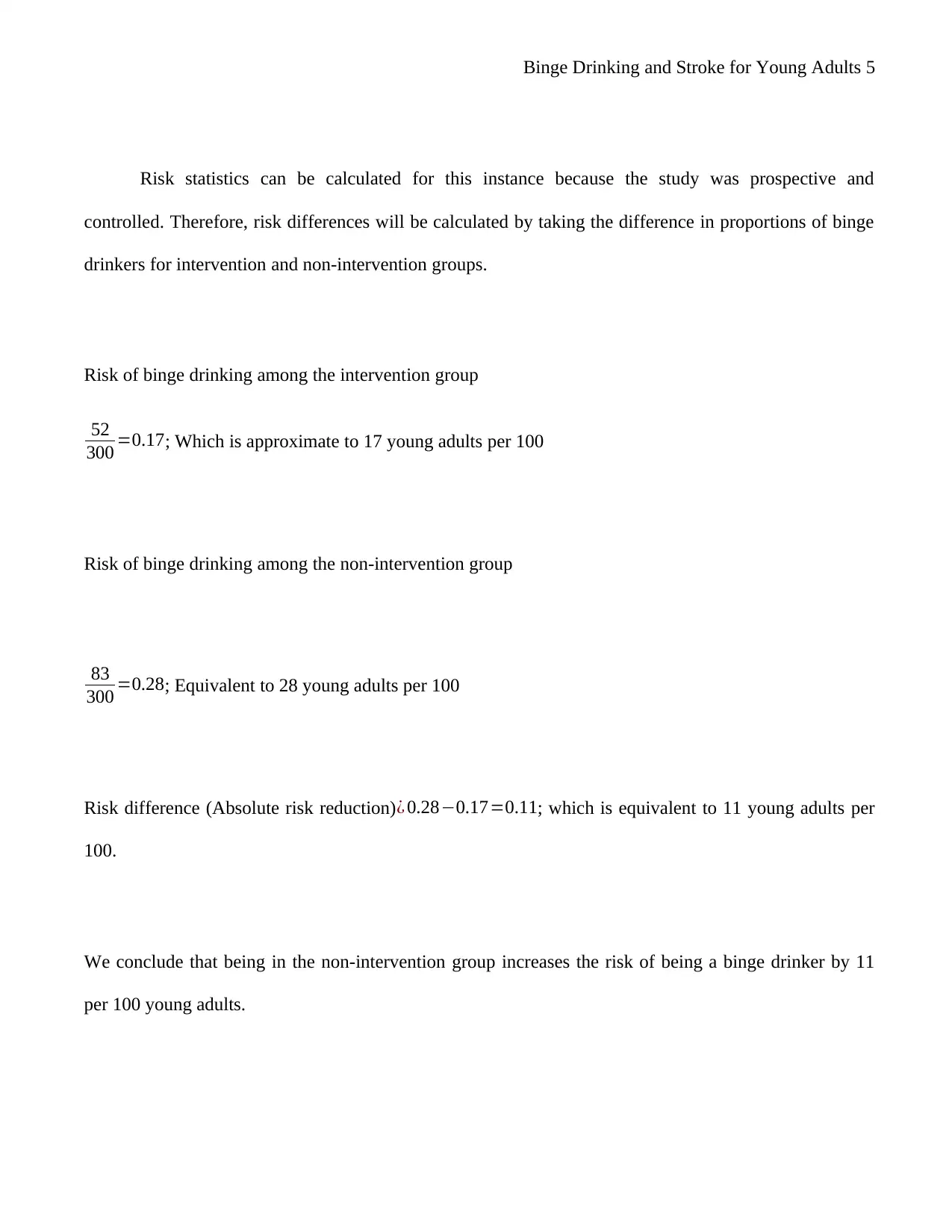
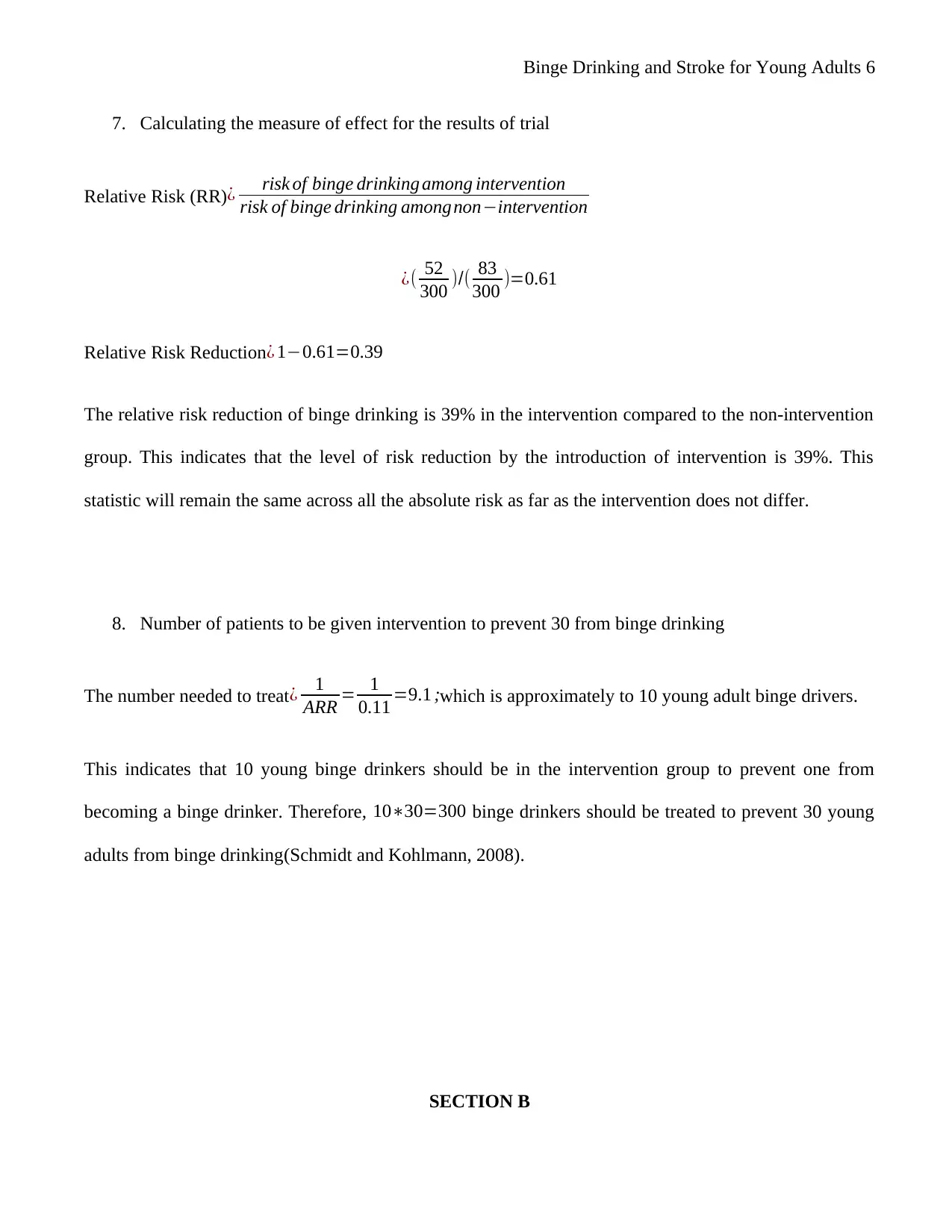
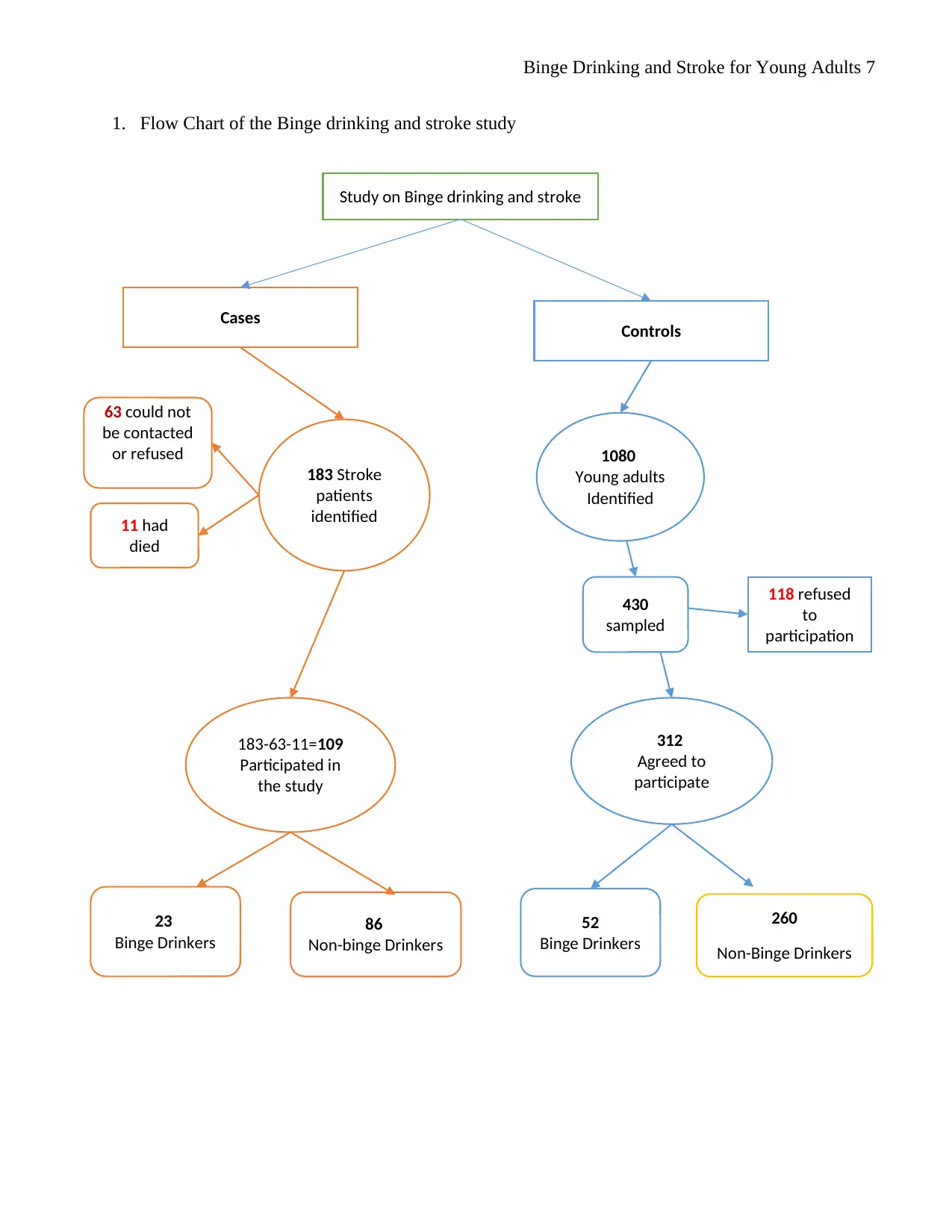
This case study examines the relationship between binge drinking and stroke in young adults within the fictitious country of Driscoville. The analysis includes a contingency table and chi-square test to assess the association between binge drinking and stroke, concluding that there is no significant association based on the provided data. The study calculates the proportion of stroke patients resulting from binge drinking and estimates the number of stroke patients who might not have had a stroke if they were not binge drinkers. Furthermore, it evaluates the impact of an intervention on binge drinking rates, calculating risk differences, relative risk reduction, and the number needed to treat to prevent binge drinking. The study also discusses the strengths and weaknesses of the case-control study design, particularly focusing on potential selection biases. The findings suggest that while binge drinking may increase the probability of stroke, the intervention strategy can reduce the risk of binge drinking among young adults. The document is available on Desklib, a platform offering study tools and solved assignments for students.

1 out of 10
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.