Business Case: Analysis of MIKRS for Hospital Implementation
VerifiedAdded on 2023/03/31
|16
|4136
|264
Report
AI Summary
This business case report examines the implementation of minimally invasive total knee replacement (MIKRS) surgery within a hospital setting. It begins with a literature review highlighting the procedure's significance, followed by an assessment of its risks, benefits, and clinical factors, including patient safety and efficacy. The report then delves into cost considerations, stakeholder communication strategies, value for money, and funding requirements. The analysis covers population-specific risks, wound healing complications, lighting issues, surgeon expertise, regulatory and ethical complications, and HR considerations associated with MIKRS. Recommendations are provided to improve the procedure, focusing on collaborative decision-making among surgeons and rheumatologists, informed patient consent, and comprehensive staff training to ensure successful and ethical implementation.

Running head: BUSINESS CASE
Business Case
Name of the Student
Name of the University
Author Note
Business Case
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
BUSINESS CASE
Introduction
Total knee replacement popularly known as knee arthroplasty is a widely employed
orthopaedic procedure that is used to replace the worn or the damaged surfaces of the
knee (Kim et al, 2015). The following is a business case for implementation of the project of
minimally invasive total knee replacement surgery under the hospital settings. The business
case will start will a brief review of literature highlighting the importance of the minimally
invasive total knee replacement surgery. This will be followed by the risks and benefits of
this surgical procedure in order to evaluate its therapeutic importance. Clinical factors
including safety of the patients and the efficacy of the procedure will be discussed after
that. At the end, the business case will highlight the costs, communication strategy planning
with the stakeholders, value of money along with the required funding. Recommendation in
order to improvise the procedure will be done based on the data illustrated in the business
case.
Minimally invasive knee replacement surgery
Total knee replacement popularly known as knee arthroplasty is a widely employed
orthopaedic procedure that is used to replace the worn or the damaged surfaces of the
knee. Replacing these damaged surfaces with the help of prosthesis or implants helps to
provide relief from pain and enables the healthcare service users to return back of normal
life and independence to conduct the activities of daily living (ADL) (Kim et al, 2015). The
traditional approach for the knee replacement employs long yet vertical incision placed at
the centre of the knee in order to view or access the joint. The minimally invasive total knee
replacement surgery makes use of a different approach. Here the orthopaedic employs
shorter incision and different yet less-invasive approach to expose the joint – with an aim to
reduce the post-operative pain and speeding the post-operative recovery (Kim et al, 2015).
Minimally invasive technique makes incision that is half (4 to 6 inches) as long as traditional
knee replacement (8 to 10 inches) and ensures that les muscles incur damage. A smaller
incision allows less damage of the tissue. In general techniques employed in minimally
invasive knee replacement is known as “quadriceps sparing” that helps to avoid trauma over
the quadriceps tendon and associated muscles present in front of the thighs. Other notable
BUSINESS CASE
Introduction
Total knee replacement popularly known as knee arthroplasty is a widely employed
orthopaedic procedure that is used to replace the worn or the damaged surfaces of the
knee (Kim et al, 2015). The following is a business case for implementation of the project of
minimally invasive total knee replacement surgery under the hospital settings. The business
case will start will a brief review of literature highlighting the importance of the minimally
invasive total knee replacement surgery. This will be followed by the risks and benefits of
this surgical procedure in order to evaluate its therapeutic importance. Clinical factors
including safety of the patients and the efficacy of the procedure will be discussed after
that. At the end, the business case will highlight the costs, communication strategy planning
with the stakeholders, value of money along with the required funding. Recommendation in
order to improvise the procedure will be done based on the data illustrated in the business
case.
Minimally invasive knee replacement surgery
Total knee replacement popularly known as knee arthroplasty is a widely employed
orthopaedic procedure that is used to replace the worn or the damaged surfaces of the
knee. Replacing these damaged surfaces with the help of prosthesis or implants helps to
provide relief from pain and enables the healthcare service users to return back of normal
life and independence to conduct the activities of daily living (ADL) (Kim et al, 2015). The
traditional approach for the knee replacement employs long yet vertical incision placed at
the centre of the knee in order to view or access the joint. The minimally invasive total knee
replacement surgery makes use of a different approach. Here the orthopaedic employs
shorter incision and different yet less-invasive approach to expose the joint – with an aim to
reduce the post-operative pain and speeding the post-operative recovery (Kim et al, 2015).
Minimally invasive technique makes incision that is half (4 to 6 inches) as long as traditional
knee replacement (8 to 10 inches) and ensures that les muscles incur damage. A smaller
incision allows less damage of the tissue. In general techniques employed in minimally
invasive knee replacement is known as “quadriceps sparing” that helps to avoid trauma over
the quadriceps tendon and associated muscles present in front of the thighs. Other notable
2
BUSINESS CASE
minimally invasive techniques like “midvastus” and “subvastus” also make small incisions in
the muscle. This small incision helps to reduce the severity of the peri-operative pain and
reduce the time of recovery or overall length of stay at the hospital (Tria & Scuderi, 2015).
Lloyd, Wainwright and Middleton (2015) stated that hospital stay of minimally invasive knee
replacement is same like that of the total replacement surgery (1 to 4 days). However, in the
minimally invasive knee replacement surgery (MIKRS) physical rehabilitation holds prime
importance like physical exercise that helps to increase the range of motion in the body and
to restore the strength of the muscles. As per the Oxford Knee Score, MIKRS is effective as it
provides a 15-year of survival data for anteromedial osteoarthritis and spontaneous
osteonecrosis of the knee (Pandit et al., 2015).
Risks associated with the technique
Population specific risks
There are certain disadvantages of the conduction of the MIKRS. Unlike the
traditional knee replacement, MIKRS is not suitable for all the patients. MIKRS is mainly
conducted over thinner, younger and healthier individual who are motivated in order to
take part in the rehabilitation process. MIKRS is less suitable for people who are over-weight
and who have already undergone knee surgeries. Moreover, patients who have significant
knee deformity or patients who are extremely muscular or have health related problems
that slow down the process of wound healing have high risks from MIKRS (Lloyd,
Wainwright & Middleton, 2015). Watts et al. (2015) have argued in their study that people
who have high level of blood glucose are not suitable for MIKRS as it creates a barrier in
spontaneous yet fast healing of wound. Watts et al. (2015) have further counter argued his
own findings stating that traditionally knee replacement surgery incur more deep wound
and thus creating fatal threats for the diabetic patients further.
Complications with wound healing
For the promotion of the faster wound healing, mini-medial parapatellar is used. It
helps in the generation of minimal skin lesions. In this technique, the incision into the
quadriceps tendon is restricted to 4 cm and thus ensuring faster wound healing. Moreover,
this approach requires less training than that other minimally invasive techniques and is
easy to extend in condition where the lack of exposure is a problem during the conduction
BUSINESS CASE
minimally invasive techniques like “midvastus” and “subvastus” also make small incisions in
the muscle. This small incision helps to reduce the severity of the peri-operative pain and
reduce the time of recovery or overall length of stay at the hospital (Tria & Scuderi, 2015).
Lloyd, Wainwright and Middleton (2015) stated that hospital stay of minimally invasive knee
replacement is same like that of the total replacement surgery (1 to 4 days). However, in the
minimally invasive knee replacement surgery (MIKRS) physical rehabilitation holds prime
importance like physical exercise that helps to increase the range of motion in the body and
to restore the strength of the muscles. As per the Oxford Knee Score, MIKRS is effective as it
provides a 15-year of survival data for anteromedial osteoarthritis and spontaneous
osteonecrosis of the knee (Pandit et al., 2015).
Risks associated with the technique
Population specific risks
There are certain disadvantages of the conduction of the MIKRS. Unlike the
traditional knee replacement, MIKRS is not suitable for all the patients. MIKRS is mainly
conducted over thinner, younger and healthier individual who are motivated in order to
take part in the rehabilitation process. MIKRS is less suitable for people who are over-weight
and who have already undergone knee surgeries. Moreover, patients who have significant
knee deformity or patients who are extremely muscular or have health related problems
that slow down the process of wound healing have high risks from MIKRS (Lloyd,
Wainwright & Middleton, 2015). Watts et al. (2015) have argued in their study that people
who have high level of blood glucose are not suitable for MIKRS as it creates a barrier in
spontaneous yet fast healing of wound. Watts et al. (2015) have further counter argued his
own findings stating that traditionally knee replacement surgery incur more deep wound
and thus creating fatal threats for the diabetic patients further.
Complications with wound healing
For the promotion of the faster wound healing, mini-medial parapatellar is used. It
helps in the generation of minimal skin lesions. In this technique, the incision into the
quadriceps tendon is restricted to 4 cm and thus ensuring faster wound healing. Moreover,
this approach requires less training than that other minimally invasive techniques and is
easy to extend in condition where the lack of exposure is a problem during the conduction
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
BUSINESS CASE
of the operation (Rudolf & Capobianco, 2014). At present, this technique is performed with
further limitation in the incision of 2 cm and this is comparable with the quadriceps sparing
and also helps t extract same clinical results. Mini-subvastus approach has no quadriceps
incision. Here the muscle is raised across the anterior aspect of the femur and then
retracted laterally. This approach is particularly suitable for the individuals who have
problems in wound healing. However, it is not suitable of people who are over-weight
(Picard et al., 2018).
Problem with adequate lightening
Scuderi et al. (2014) stated that in order to conduct MIKRS, proper lightening is
required n order recognize the proper area and depth of incision. However, lightening
apparatus affixed over the surgeon’s helmet either directly or by use of the retractor fail to
provide proper illumination. The condition becomes more challenging while handling over-
weight patients with more muscle mass. Skin issues are other limiting structures for MIKRS.
This technique requires stretching at both the extremities of the incision. This stretching of
the skin generates ischaemic areas that take long time recovery. In such cases, fat pad
resection (15% of the skin injury rate) is replaced by infrapatellar fat pad preservation (3%
chances of the skin injury). Picard et al. (2018) highlighted in their study that small skin
incision in the MISKS occurs in horizontal skin tension line. Long-term stretches on the
elastic fibres result in the loss of recoil because of the fragmentation of the elastin and this
compromise the closure and process of fast wound healing. The conditions are more severe
among the older adults.
Special expertise
Pandit et al. (2017) stated that a surgeon performing a MIKRS requires advanced
training. This is because in traditional surgery the tibia (shinbone) is dislocated from the
femur (thighbone) before fitting the prosthetics with the bones. In contrary, in minimally
invasive surgery, tibia may not be dislocated from the femur. More specialised expertise is
required in order to operate minimally invasive surgery. Minimally invasive surgery also
differs in the exact location of incision along with the shape of the incision. Mainly curved
incision is made in order to clear out the soft tissues and the muscles to make room for the
conduction of the surgical procedure. Thus, demanding gamut experience of the
orthopaedic surgeon along to locate the exact location of the incision depending upon the
BUSINESS CASE
of the operation (Rudolf & Capobianco, 2014). At present, this technique is performed with
further limitation in the incision of 2 cm and this is comparable with the quadriceps sparing
and also helps t extract same clinical results. Mini-subvastus approach has no quadriceps
incision. Here the muscle is raised across the anterior aspect of the femur and then
retracted laterally. This approach is particularly suitable for the individuals who have
problems in wound healing. However, it is not suitable of people who are over-weight
(Picard et al., 2018).
Problem with adequate lightening
Scuderi et al. (2014) stated that in order to conduct MIKRS, proper lightening is
required n order recognize the proper area and depth of incision. However, lightening
apparatus affixed over the surgeon’s helmet either directly or by use of the retractor fail to
provide proper illumination. The condition becomes more challenging while handling over-
weight patients with more muscle mass. Skin issues are other limiting structures for MIKRS.
This technique requires stretching at both the extremities of the incision. This stretching of
the skin generates ischaemic areas that take long time recovery. In such cases, fat pad
resection (15% of the skin injury rate) is replaced by infrapatellar fat pad preservation (3%
chances of the skin injury). Picard et al. (2018) highlighted in their study that small skin
incision in the MISKS occurs in horizontal skin tension line. Long-term stretches on the
elastic fibres result in the loss of recoil because of the fragmentation of the elastin and this
compromise the closure and process of fast wound healing. The conditions are more severe
among the older adults.
Special expertise
Pandit et al. (2017) stated that a surgeon performing a MIKRS requires advanced
training. This is because in traditional surgery the tibia (shinbone) is dislocated from the
femur (thighbone) before fitting the prosthetics with the bones. In contrary, in minimally
invasive surgery, tibia may not be dislocated from the femur. More specialised expertise is
required in order to operate minimally invasive surgery. Minimally invasive surgery also
differs in the exact location of incision along with the shape of the incision. Mainly curved
incision is made in order to clear out the soft tissues and the muscles to make room for the
conduction of the surgical procedure. Thus, demanding gamut experience of the
orthopaedic surgeon along to locate the exact location of the incision depending upon the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
BUSINESS CASE
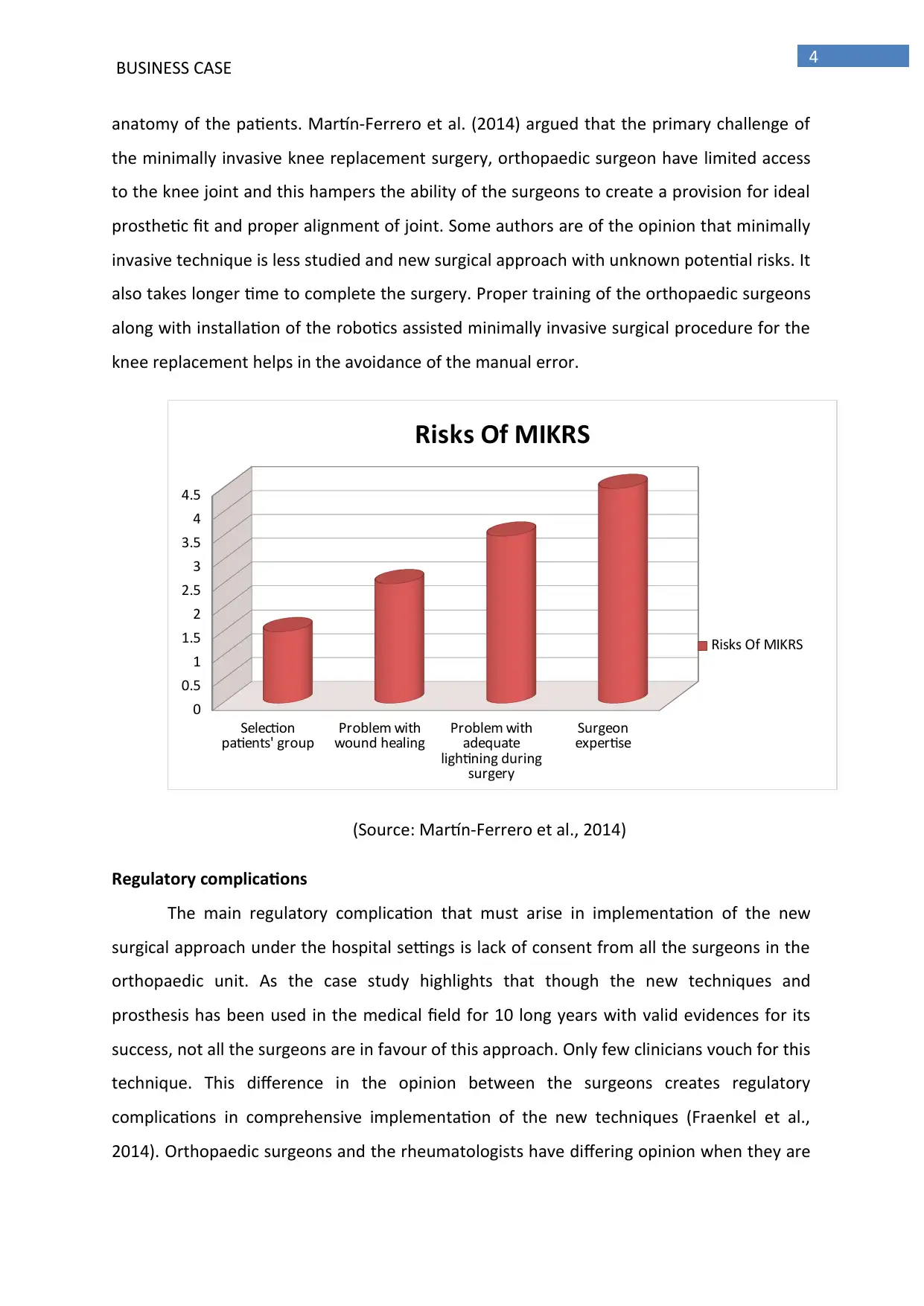
anatomy of the patients. Martín-Ferrero et al. (2014) argued that the primary challenge of
the minimally invasive knee replacement surgery, orthopaedic surgeon have limited access
to the knee joint and this hampers the ability of the surgeons to create a provision for ideal
prosthetic fit and proper alignment of joint. Some authors are of the opinion that minimally
invasive technique is less studied and new surgical approach with unknown potential risks. It
also takes longer time to complete the surgery. Proper training of the orthopaedic surgeons
along with installation of the robotics assisted minimally invasive surgical procedure for the
knee replacement helps in the avoidance of the manual error.
Selection
patients' group Problem with
wound healing Problem with
adequate
lightining during
surgery
Surgeon
expertise
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Risks Of MIKRS
Risks Of MIKRS
(Source: Martín-Ferrero et al., 2014)
Regulatory complications
The main regulatory complication that must arise in implementation of the new
surgical approach under the hospital settings is lack of consent from all the surgeons in the
orthopaedic unit. As the case study highlights that though the new techniques and
prosthesis has been used in the medical field for 10 long years with valid evidences for its
success, not all the surgeons are in favour of this approach. Only few clinicians vouch for this
technique. This difference in the opinion between the surgeons creates regulatory
complications in comprehensive implementation of the new techniques (Fraenkel et al.,
2014). Orthopaedic surgeons and the rheumatologists have differing opinion when they are
BUSINESS CASE
anatomy of the patients. Martín-Ferrero et al. (2014) argued that the primary challenge of
the minimally invasive knee replacement surgery, orthopaedic surgeon have limited access
to the knee joint and this hampers the ability of the surgeons to create a provision for ideal
prosthetic fit and proper alignment of joint. Some authors are of the opinion that minimally
invasive technique is less studied and new surgical approach with unknown potential risks. It
also takes longer time to complete the surgery. Proper training of the orthopaedic surgeons
along with installation of the robotics assisted minimally invasive surgical procedure for the
knee replacement helps in the avoidance of the manual error.
Selection
patients' group Problem with
wound healing Problem with
adequate
lightining during
surgery
Surgeon
expertise
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Risks Of MIKRS
Risks Of MIKRS
(Source: Martín-Ferrero et al., 2014)
Regulatory complications
The main regulatory complication that must arise in implementation of the new
surgical approach under the hospital settings is lack of consent from all the surgeons in the
orthopaedic unit. As the case study highlights that though the new techniques and
prosthesis has been used in the medical field for 10 long years with valid evidences for its
success, not all the surgeons are in favour of this approach. Only few clinicians vouch for this
technique. This difference in the opinion between the surgeons creates regulatory
complications in comprehensive implementation of the new techniques (Fraenkel et al.,
2014). Orthopaedic surgeons and the rheumatologists have differing opinion when they are
5
BUSINESS CASE
asked to recommend for the patients in the conduction of the knee replacement surgery in
order to improve the activities of daily living, reduce pain and improving other functional
limitations. Both the characteristics of the patient and physicians (orthopaedic surgeons and
rheumatologists) influence the recommendations of the surgical procedures. Difference in
the line of the decision making among the surgeons and the rheumatologists create
regulatory problems in proposing for proper yet best fit surgery for the patient’s recovery
on time. Moreover, difference in the opinion of the surgeons and the rheumatologists
hamper the overall patients’ decision making process (Smieliauskas, 2016).
Recommendations
In order reduce the difference opinion group discussion must be held among the
doctors (orthopaedic surgeons) and rheumatologist. Mosadeghrad (2014) are of the opinion
that effective group discussion among the multidisciplinary teams helps in the proper
exchange of the information and thereby helping to avoid the conflict of interest and at the
same time helps to increase the patients’ safety. Facilitation of the proper interaction
between the stakeholders (multidisciplinary team + hospital authority) is highlighted in the
communication planning below.
Ethical complications
There are significant ethical issues inherent towards the introduction of surgical
innovation in a health care organisation in the field of the orthopaedics. For the treatment
of the decaying bones in osteo-arthritis, traditional knee replacement approach is
considered to be effective with little or no disagreement in this ground. Traditional knee
replacement surgery has been used for years and is associated with low risks of
complications. In recent years orthopaedic surgeons have recommended innovative
approach for knee replacement and that is MIKRS (Broekman, Carrière & Bredenoord,
2016). This helps to reduce the severity of wound incurred, decreased time of the hospital
stay and decrease in the level of post-operative time. There are ample evidences suggesting
that MIKRS is an effective approach for surgical replacement of the knee bone with
prosthetics. However, few evidences also suggest that this new technique might be
associated with other potential risk factors also demands superior expertise of the surgeon.
This uncertainty of the potential risk factors creates uncertainty in maintaining the ethical
BUSINESS CASE
asked to recommend for the patients in the conduction of the knee replacement surgery in
order to improve the activities of daily living, reduce pain and improving other functional
limitations. Both the characteristics of the patient and physicians (orthopaedic surgeons and
rheumatologists) influence the recommendations of the surgical procedures. Difference in
the line of the decision making among the surgeons and the rheumatologists create
regulatory problems in proposing for proper yet best fit surgery for the patient’s recovery
on time. Moreover, difference in the opinion of the surgeons and the rheumatologists
hamper the overall patients’ decision making process (Smieliauskas, 2016).
Recommendations
In order reduce the difference opinion group discussion must be held among the
doctors (orthopaedic surgeons) and rheumatologist. Mosadeghrad (2014) are of the opinion
that effective group discussion among the multidisciplinary teams helps in the proper
exchange of the information and thereby helping to avoid the conflict of interest and at the
same time helps to increase the patients’ safety. Facilitation of the proper interaction
between the stakeholders (multidisciplinary team + hospital authority) is highlighted in the
communication planning below.
Ethical complications
There are significant ethical issues inherent towards the introduction of surgical
innovation in a health care organisation in the field of the orthopaedics. For the treatment
of the decaying bones in osteo-arthritis, traditional knee replacement approach is
considered to be effective with little or no disagreement in this ground. Traditional knee
replacement surgery has been used for years and is associated with low risks of
complications. In recent years orthopaedic surgeons have recommended innovative
approach for knee replacement and that is MIKRS (Broekman, Carrière & Bredenoord,
2016). This helps to reduce the severity of wound incurred, decreased time of the hospital
stay and decrease in the level of post-operative time. There are ample evidences suggesting
that MIKRS is an effective approach for surgical replacement of the knee bone with
prosthetics. However, few evidences also suggest that this new technique might be
associated with other potential risk factors also demands superior expertise of the surgeon.
This uncertainty of the potential risk factors creates uncertainty in maintaining the ethical
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
BUSINESS CASE
guidelines of beneficence and non-maleficence. Beneficence deals with balancing the
benefits associated with the treatment against the risks and subsequent costs of the
treatments. Non-maleficence implies that total harm must not outnumber the sum of total
benefits associated with the treatment. Since the all the potential risk factors of MIKRS are
not known, the overall effect of beneficence and non-malficence cannot be measured
(Broekman, Carrière & Bredenoord, 2016).
Recommendations
Thus in order to overcome the ethical complications of the beneficence and non-
malefinece, all the potential risks that are associated with the surgery (the risks that are
known or are elucidated till now) must be discussed in detail with the patients. The call for
the final surgery must be done based on the consent of the patients under proper
understanding of the impending risks and benefits. This provision of patients’ decision-
making process will help to uphold the ethical concept of autonomy (Teman et al., 2014).
Human Resource (HR) issues
The case study highlights that comprehensive application of the MIKRS requires
proper installation of the new equipment in the operation theatres along with training of
the healthcare professionals (both the physicians and the nurses) in handling those new
equipment. Thus the main HR issues will be set up a proper training sessions for the existing
orthopaedic surgeons and the surgical nurses in order to get accustomed with the new set-
up of the MIKRS (Stone et al., 2015). Moreover, Gallardo-Gallardo and Thunnissen (2016)
are of the opinion that the newly graduate orthopaedic surgeons are more likely to take
inherit the new training procedure in comparison to the existing doctors this is because,
newly graduate doctors are more exposed to the technological advancements in the
healthcare like the use of robotics in the surgical systems. This in order to decrease the
manual error during the surgical procedures, use of robotics is important and thus
increasing the needs of the fresh technologically advanced graduates. The role of the HR will
be set new recruitment requisition for fresh graduates trained in robotics. The experienced
yet veterans doctors are also important in MIKRS this is because, significant experience is
required in order to locate the area of incision, depth of incision and to judge whether the
BUSINESS CASE
guidelines of beneficence and non-maleficence. Beneficence deals with balancing the
benefits associated with the treatment against the risks and subsequent costs of the
treatments. Non-maleficence implies that total harm must not outnumber the sum of total
benefits associated with the treatment. Since the all the potential risk factors of MIKRS are
not known, the overall effect of beneficence and non-malficence cannot be measured
(Broekman, Carrière & Bredenoord, 2016).
Recommendations
Thus in order to overcome the ethical complications of the beneficence and non-
malefinece, all the potential risks that are associated with the surgery (the risks that are
known or are elucidated till now) must be discussed in detail with the patients. The call for
the final surgery must be done based on the consent of the patients under proper
understanding of the impending risks and benefits. This provision of patients’ decision-
making process will help to uphold the ethical concept of autonomy (Teman et al., 2014).
Human Resource (HR) issues
The case study highlights that comprehensive application of the MIKRS requires
proper installation of the new equipment in the operation theatres along with training of
the healthcare professionals (both the physicians and the nurses) in handling those new
equipment. Thus the main HR issues will be set up a proper training sessions for the existing
orthopaedic surgeons and the surgical nurses in order to get accustomed with the new set-
up of the MIKRS (Stone et al., 2015). Moreover, Gallardo-Gallardo and Thunnissen (2016)
are of the opinion that the newly graduate orthopaedic surgeons are more likely to take
inherit the new training procedure in comparison to the existing doctors this is because,
newly graduate doctors are more exposed to the technological advancements in the
healthcare like the use of robotics in the surgical systems. This in order to decrease the
manual error during the surgical procedures, use of robotics is important and thus
increasing the needs of the fresh technologically advanced graduates. The role of the HR will
be set new recruitment requisition for fresh graduates trained in robotics. The experienced
yet veterans doctors are also important in MIKRS this is because, significant experience is
required in order to locate the area of incision, depth of incision and to judge whether the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
BUSINESS CASE
patients’ physiological parameter is suitable enough to withstand the trauma of the surgery.
Thus the role of the HR will include proper human resource planning (Stone et al., 2015).
Recommendations
Gallardo-Gallardo and Thunnissen (2016) are of the opinion that the empirical talent
management research will be important in order to make proper human resource planning.
The human resource planning must encompass a proper balance between the veterans and
newly recruited doctors. The planning of the HR must be done under the supervision of
hospital administrative authority in order to make the recruitment planning based on the
patients’ strength of the healthcare organization, funding and the estimated healthcare
costs per surgery.
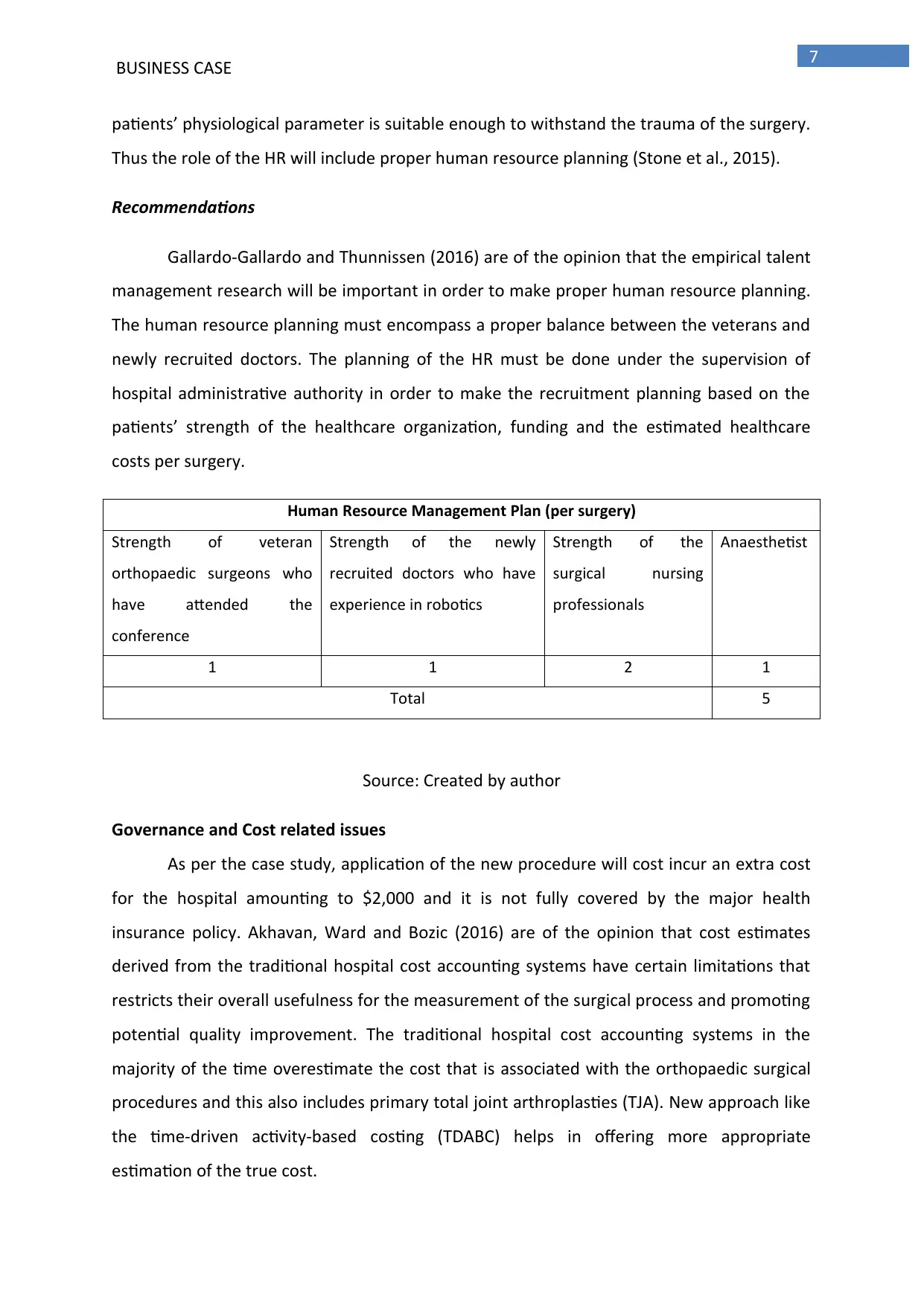
Human Resource Management Plan (per surgery)
Strength of veteran
orthopaedic surgeons who
have attended the
conference
Strength of the newly
recruited doctors who have
experience in robotics
Strength of the
surgical nursing
professionals
Anaesthetist
1 1 2 1
Total 5
Source: Created by author
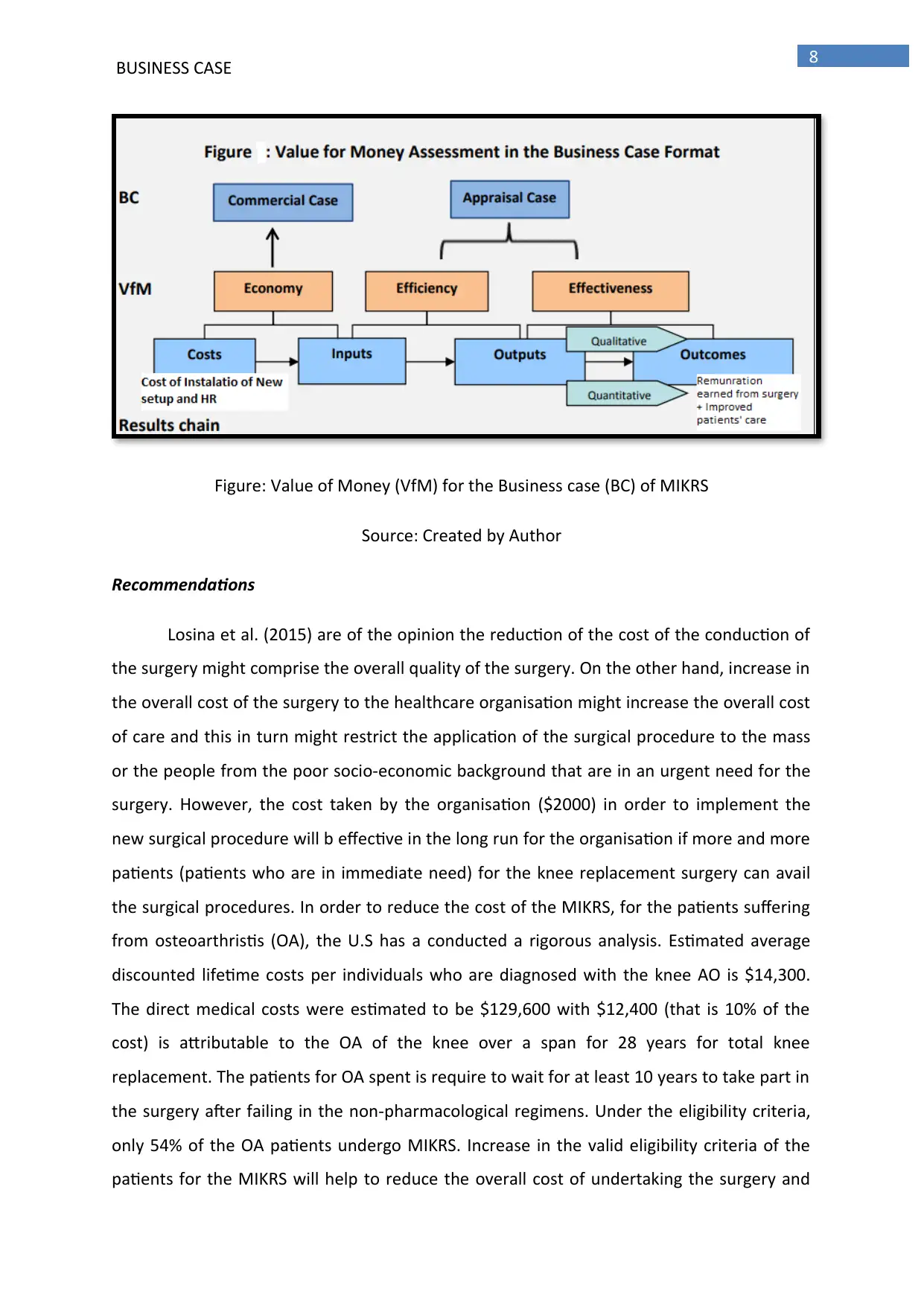
Governance and Cost related issues
As per the case study, application of the new procedure will cost incur an extra cost
for the hospital amounting to $2,000 and it is not fully covered by the major health
insurance policy. Akhavan, Ward and Bozic (2016) are of the opinion that cost estimates
derived from the traditional hospital cost accounting systems have certain limitations that
restricts their overall usefulness for the measurement of the surgical process and promoting
potential quality improvement. The traditional hospital cost accounting systems in the
majority of the time overestimate the cost that is associated with the orthopaedic surgical
procedures and this also includes primary total joint arthroplasties (TJA). New approach like
the time-driven activity-based costing (TDABC) helps in offering more appropriate
estimation of the true cost.
BUSINESS CASE
patients’ physiological parameter is suitable enough to withstand the trauma of the surgery.
Thus the role of the HR will include proper human resource planning (Stone et al., 2015).
Recommendations
Gallardo-Gallardo and Thunnissen (2016) are of the opinion that the empirical talent
management research will be important in order to make proper human resource planning.
The human resource planning must encompass a proper balance between the veterans and
newly recruited doctors. The planning of the HR must be done under the supervision of
hospital administrative authority in order to make the recruitment planning based on the
patients’ strength of the healthcare organization, funding and the estimated healthcare
costs per surgery.
Human Resource Management Plan (per surgery)
Strength of veteran
orthopaedic surgeons who
have attended the
conference
Strength of the newly
recruited doctors who have
experience in robotics
Strength of the
surgical nursing
professionals
Anaesthetist
1 1 2 1
Total 5
Source: Created by author
Governance and Cost related issues
As per the case study, application of the new procedure will cost incur an extra cost
for the hospital amounting to $2,000 and it is not fully covered by the major health
insurance policy. Akhavan, Ward and Bozic (2016) are of the opinion that cost estimates
derived from the traditional hospital cost accounting systems have certain limitations that
restricts their overall usefulness for the measurement of the surgical process and promoting
potential quality improvement. The traditional hospital cost accounting systems in the
majority of the time overestimate the cost that is associated with the orthopaedic surgical
procedures and this also includes primary total joint arthroplasties (TJA). New approach like
the time-driven activity-based costing (TDABC) helps in offering more appropriate
estimation of the true cost.
8
BUSINESS CASE
Figure: Value of Money (VfM) for the Business case (BC) of MIKRS
Source: Created by Author
Recommendations
Losina et al. (2015) are of the opinion the reduction of the cost of the conduction of
the surgery might comprise the overall quality of the surgery. On the other hand, increase in
the overall cost of the surgery to the healthcare organisation might increase the overall cost
of care and this in turn might restrict the application of the surgical procedure to the mass
or the people from the poor socio-economic background that are in an urgent need for the
surgery. However, the cost taken by the organisation ($2000) in order to implement the
new surgical procedure will b effective in the long run for the organisation if more and more
patients (patients who are in immediate need) for the knee replacement surgery can avail
the surgical procedures. In order to reduce the cost of the MIKRS, for the patients suffering
from osteoarthristis (OA), the U.S has a conducted a rigorous analysis. Estimated average
discounted lifetime costs per individuals who are diagnosed with the knee AO is $14,300.
The direct medical costs were estimated to be $129,600 with $12,400 (that is 10% of the
cost) is attributable to the OA of the knee over a span for 28 years for total knee
replacement. The patients for OA spent is require to wait for at least 10 years to take part in
the surgery after failing in the non-pharmacological regimens. Under the eligibility criteria,
only 54% of the OA patients undergo MIKRS. Increase in the valid eligibility criteria of the
patients for the MIKRS will help to reduce the overall cost of undertaking the surgery and
BUSINESS CASE
Figure: Value of Money (VfM) for the Business case (BC) of MIKRS
Source: Created by Author
Recommendations
Losina et al. (2015) are of the opinion the reduction of the cost of the conduction of
the surgery might comprise the overall quality of the surgery. On the other hand, increase in
the overall cost of the surgery to the healthcare organisation might increase the overall cost
of care and this in turn might restrict the application of the surgical procedure to the mass
or the people from the poor socio-economic background that are in an urgent need for the
surgery. However, the cost taken by the organisation ($2000) in order to implement the
new surgical procedure will b effective in the long run for the organisation if more and more
patients (patients who are in immediate need) for the knee replacement surgery can avail
the surgical procedures. In order to reduce the cost of the MIKRS, for the patients suffering
from osteoarthristis (OA), the U.S has a conducted a rigorous analysis. Estimated average
discounted lifetime costs per individuals who are diagnosed with the knee AO is $14,300.
The direct medical costs were estimated to be $129,600 with $12,400 (that is 10% of the
cost) is attributable to the OA of the knee over a span for 28 years for total knee
replacement. The patients for OA spent is require to wait for at least 10 years to take part in
the surgery after failing in the non-pharmacological regimens. Under the eligibility criteria,
only 54% of the OA patients undergo MIKRS. Increase in the valid eligibility criteria of the
patients for the MIKRS will help to reduce the overall cost of undertaking the surgery and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
BUSINESS CASE
this will in turn help the hospital to pay-back for the total investments made in the process
of installation of the surgical setup (Losina et al., 2015; Kapadia et al., 2014).
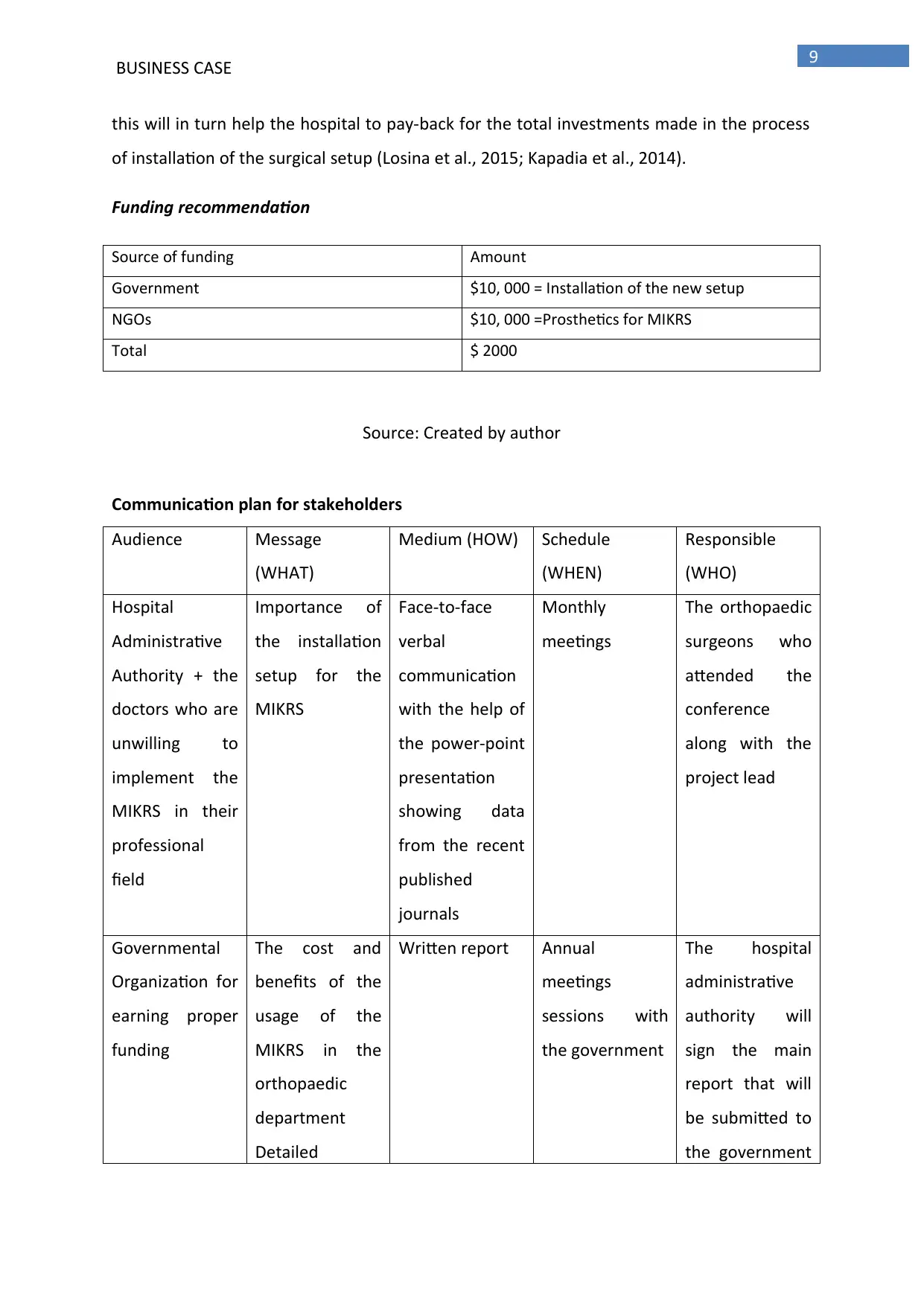
Funding recommendation
Source of funding Amount
Government $10, 000 = Installation of the new setup
NGOs $10, 000 =Prosthetics for MIKRS
Total $ 2000
Source: Created by author
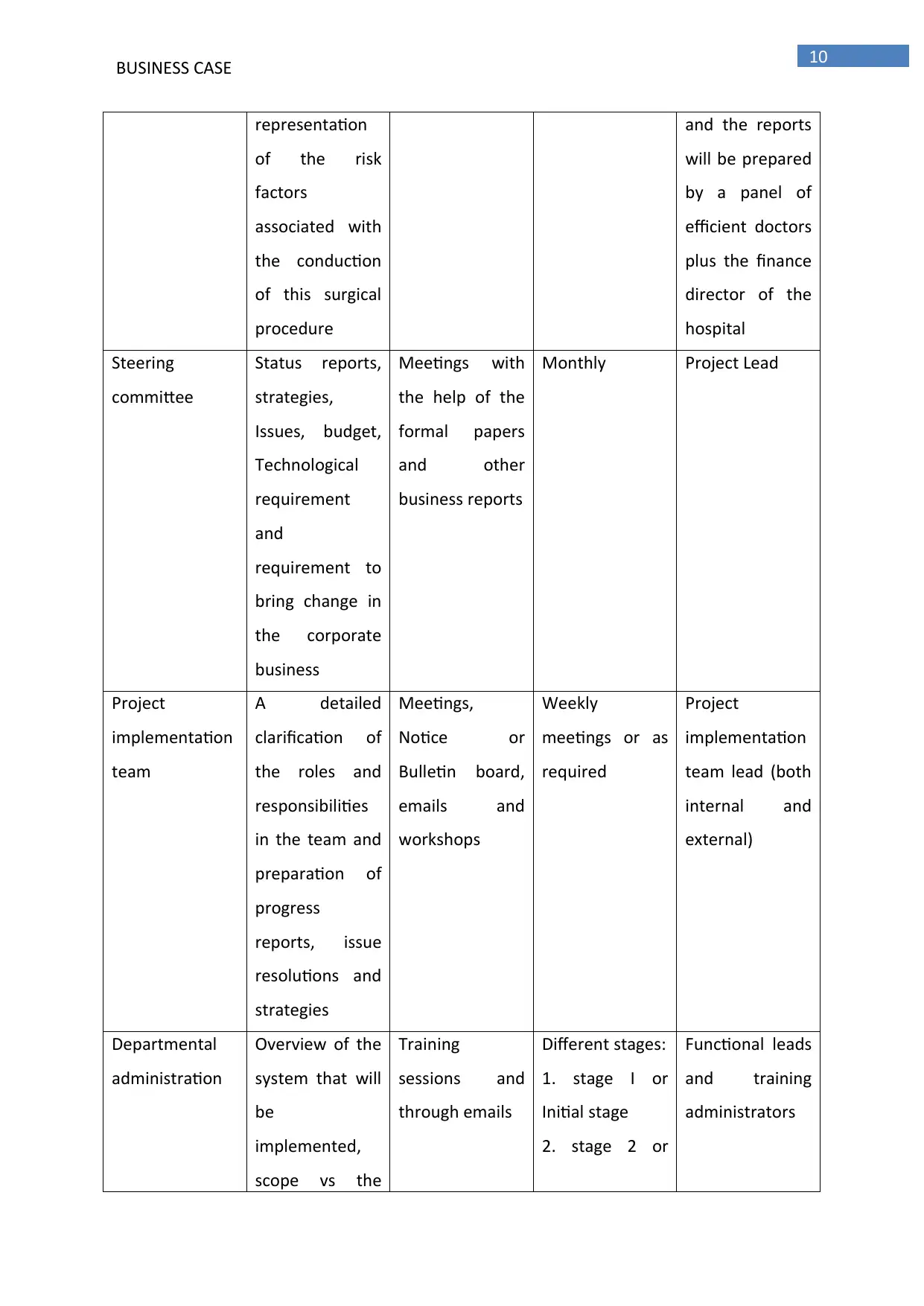
Communication plan for stakeholders
Audience Message
(WHAT)
Medium (HOW) Schedule
(WHEN)
Responsible
(WHO)
Hospital
Administrative
Authority + the
doctors who are
unwilling to
implement the
MIKRS in their
professional
field
Importance of
the installation
setup for the
MIKRS
Face-to-face
verbal
communication
with the help of
the power-point
presentation
showing data
from the recent
published
journals
Monthly
meetings
The orthopaedic
surgeons who
attended the
conference
along with the
project lead
Governmental
Organization for
earning proper
funding
The cost and
benefits of the
usage of the
MIKRS in the
orthopaedic
department
Detailed
Written report Annual
meetings
sessions with
the government
The hospital
administrative
authority will
sign the main
report that will
be submitted to
the government
BUSINESS CASE
this will in turn help the hospital to pay-back for the total investments made in the process
of installation of the surgical setup (Losina et al., 2015; Kapadia et al., 2014).
Funding recommendation
Source of funding Amount
Government $10, 000 = Installation of the new setup
NGOs $10, 000 =Prosthetics for MIKRS
Total $ 2000
Source: Created by author
Communication plan for stakeholders
Audience Message
(WHAT)
Medium (HOW) Schedule
(WHEN)
Responsible
(WHO)
Hospital
Administrative
Authority + the
doctors who are
unwilling to
implement the
MIKRS in their
professional
field
Importance of
the installation
setup for the
MIKRS
Face-to-face
verbal
communication
with the help of
the power-point
presentation
showing data
from the recent
published
journals
Monthly
meetings
The orthopaedic
surgeons who
attended the
conference
along with the
project lead
Governmental
Organization for
earning proper
funding
The cost and
benefits of the
usage of the
MIKRS in the
orthopaedic
department
Detailed
Written report Annual
meetings
sessions with
the government
The hospital
administrative
authority will
sign the main
report that will
be submitted to
the government
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
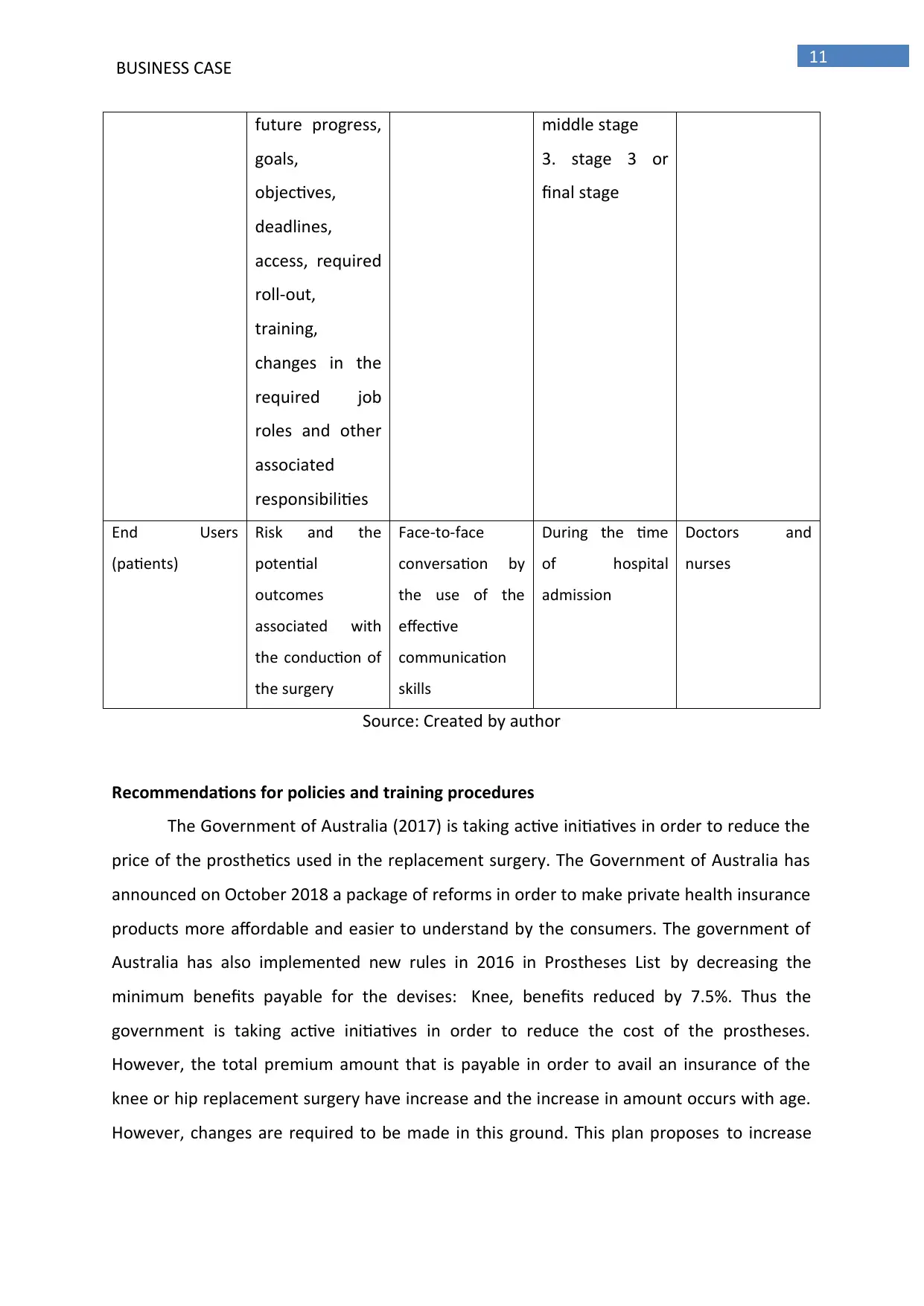
BUSINESS CASE
representation
of the risk
factors
associated with
the conduction
of this surgical
procedure
and the reports
will be prepared
by a panel of
efficient doctors
plus the finance
director of the
hospital
Steering
committee
Status reports,
strategies,
Issues, budget,
Technological
requirement
and
requirement to
bring change in
the corporate
business
Meetings with
the help of the
formal papers
and other
business reports
Monthly Project Lead
Project
implementation
team
A detailed
clarification of
the roles and
responsibilities
in the team and
preparation of
progress
reports, issue
resolutions and
strategies
Meetings,
Notice or
Bulletin board,
emails and
workshops
Weekly
meetings or as
required
Project
implementation
team lead (both
internal and
external)
Departmental
administration
Overview of the
system that will
be
implemented,
scope vs the
Training
sessions and
through emails
Different stages:
1. stage I or
Initial stage
2. stage 2 or
Functional leads
and training
administrators
BUSINESS CASE
representation
of the risk
factors
associated with
the conduction
of this surgical
procedure
and the reports
will be prepared
by a panel of
efficient doctors
plus the finance
director of the
hospital
Steering
committee
Status reports,
strategies,
Issues, budget,
Technological
requirement
and
requirement to
bring change in
the corporate
business
Meetings with
the help of the
formal papers
and other
business reports
Monthly Project Lead
Project
implementation
team
A detailed
clarification of
the roles and
responsibilities
in the team and
preparation of
progress
reports, issue
resolutions and
strategies
Meetings,
Notice or
Bulletin board,
emails and
workshops
Weekly
meetings or as
required
Project
implementation
team lead (both
internal and
external)
Departmental
administration
Overview of the
system that will
be
implemented,
scope vs the
Training
sessions and
through emails
Different stages:
1. stage I or
Initial stage
2. stage 2 or
Functional leads
and training
administrators
11
BUSINESS CASE
future progress,
goals,
objectives,
deadlines,
access, required
roll-out,
training,
changes in the
required job
roles and other
associated
responsibilities
middle stage
3. stage 3 or
final stage
End Users
(patients)
Risk and the
potential
outcomes
associated with
the conduction of
the surgery
Face-to-face
conversation by
the use of the
effective
communication
skills
During the time
of hospital
admission
Doctors and
nurses
Source: Created by author
Recommendations for policies and training procedures
The Government of Australia (2017) is taking active initiatives in order to reduce the
price of the prosthetics used in the replacement surgery. The Government of Australia has
announced on October 2018 a package of reforms in order to make private health insurance
products more affordable and easier to understand by the consumers. The government of
Australia has also implemented new rules in 2016 in Prostheses List by decreasing the
minimum benefits payable for the devises: Knee, benefits reduced by 7.5%. Thus the
government is taking active initiatives in order to reduce the cost of the prostheses.
However, the total premium amount that is payable in order to avail an insurance of the
knee or hip replacement surgery have increase and the increase in amount occurs with age.
However, changes are required to be made in this ground. This plan proposes to increase
BUSINESS CASE
future progress,
goals,
objectives,
deadlines,
access, required
roll-out,
training,
changes in the
required job
roles and other
associated
responsibilities
middle stage
3. stage 3 or
final stage
End Users
(patients)
Risk and the
potential
outcomes
associated with
the conduction of
the surgery
Face-to-face
conversation by
the use of the
effective
communication
skills
During the time
of hospital
admission
Doctors and
nurses
Source: Created by author
Recommendations for policies and training procedures
The Government of Australia (2017) is taking active initiatives in order to reduce the
price of the prosthetics used in the replacement surgery. The Government of Australia has
announced on October 2018 a package of reforms in order to make private health insurance
products more affordable and easier to understand by the consumers. The government of
Australia has also implemented new rules in 2016 in Prostheses List by decreasing the
minimum benefits payable for the devises: Knee, benefits reduced by 7.5%. Thus the
government is taking active initiatives in order to reduce the cost of the prostheses.
However, the total premium amount that is payable in order to avail an insurance of the
knee or hip replacement surgery have increase and the increase in amount occurs with age.
However, changes are required to be made in this ground. This plan proposes to increase
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 16


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.