Analyzing Cannabis Legalization Proposals: A Canadian Critique
VerifiedAdded on 2023/06/14
|6
|8397
|500
Literature Review
AI Summary
This paper presents a critical review of cannabis legalization proposals in Canada, focusing on an editorial that advocates for legalization with strict controls. It challenges claims made in favor of legalization, particularly regarding the elimination of prohibition-related harms and the effectiveness of regulatory controls. The critique argues that evidence supporting these claims is weak and that early experiences in other jurisdictions suggest increased cannabis use among adolescents. It questions the suitability of alcohol regulation as a model for cannabis control and emphasizes the need for comprehensive knowledge about the individual and social consequences of both drug use and control measures. The review suggests decriminalization as a more appropriate initial step until sufficient knowledge is acquired to make informed decisions about legalization.

Commentary
A critique of cannabis legalization proposals in Canada
[3_TD$DIFF]Harold [6_TD$DIFF]Kalant
Department of Pharmacology & Toxicology,University of Toronto Medical Sciences Building,1 King’s College Circle Toronto,ON, Canada M5S 1A8
Introduction
The editorial by Cre´pault, Rehm & Fischer (p.1 of this issue)
provides a detailed description of the origins and rationale of a
CAMH document entitled Cannabis Policy Framework (Cre´pault,
2014),referred to below as the CPF.As described in the editorial,
the CPF concluded with a recommendation for legalization of non-
medical use of cannabis,with reliance on strict application of
regulations to prevent access to cannabis by underage users who
are most vulnerable to its adverse effects on health and social
functioning. As the editorial explains, the CPF grew out of an earlier
document from the Addiction Research Foundation (ARF)that
called for a public health approach to cannabis policy and for
decriminalization of possession for personal use (Addiction
Research Foundation, 1997). This recommendation was also made
in the LeDain Commission Report (Canadian Government,1972),
and was maintained in CAMH statements that preceded the CPF. It
is therefore useful to examine the reasons that led to the changed
recommendation in the CPF and other recent similar publications
(Haden & Emerson,2014; Spithoff,Emerson,& Spithoff,2015).
Among the important considerations mentioned in the editorial
are the following:
social harms caused by prohibition, and by its inequitable
application,
the relative modesty of the health harms attributable to cannabis
use in the majority of users,
costliness and ineffectiveness of prohibition,combined with its
deterrence of public health measures aimed at prevention and
treatment of drug-induced harm,
superior ability of legalization to prevent harm to vulnerable
groups by the use of regulatory controls that cannot be
implemented under decriminalization,
the risk that decriminalization could actually encourage the
production and distribution of cannabis.
International Journal of Drug Policy 34 (2016) 5–10
A R T I C L E I N F O
Article history:
Received 11 November 2015
Received in revised form 27 April 2016
Accepted 9 May 2016
Keywords:
Cannabis policy
Legalization
Decriminalization
Harms caused by prohibition
Harms to adolescent users
Cost-benefit assessment
A B S T R A C T
An editorial in this issue describes a cannabis policy framework document issued by a major Canadian
research centre,calling for legalization of non-medical use under strict controls to prevent increase in
use, especially by adolescents and young adults who are most vulnerable to adverse effects of cannabis
claims that such a system would eliminate the severe personal, social and monetary costs of prohibition
diminish the illicit market, and provide more humane management of cannabis use disorders. It claims
that experience with regulation of alcohol and tobacco will enable a system based on public health
principles to control access of youth to cannabis without the harm caused by prohibition.
The present critique argues that the claims made against decriminalization and for legalization are
unsupported,or even contradicted,by solid evidence.Early experience in other jurisdictions suggests
that legalization increases use by adolescents and its attendant harms. Regulation of alcohol use does n
provide a good model for cannabis controls because there is widespread alcohol use and harm among
adolescents and young adults.Government monopolies of alcoholsale have been used primarily as
sources of revenue rather than for guarding public health, and no reason has been offered to believe the
would act differently with respect to cannabis.
Good policy decisions require extensive unbiased information about the individual and social benefits
and costs of both drug use and proposed control measures, and value judgments about the benefit/harm
balance of each option. Important parts of the necessary knowledge about cannabis are not yet availabl
so that the value judgments are not yet possible. Therefore,a better case can be made for eliminating
some of the harms of prohibition by decriminalization of cannabis possession and deferring decision
about legalization until the necessary knowledge has been acquired.
ß 2016 Elsevier B.V.All rights reserved.
E-mail address: harold.kalant@utoronto.ca.
Contents lists available at ScienceDirect
International Journal of Drug Policy
j o u r n a lh o m e p a g e :w w w . e l s e v i e r . c o m / l o c a t e / d r u g p o
http://dx.doi.org/10.1016/j.drugpo.2016.05.002
0955-3959/ß 2016 Elsevier B.V.All rights reserved.
A critique of cannabis legalization proposals in Canada
[3_TD$DIFF]Harold [6_TD$DIFF]Kalant
Department of Pharmacology & Toxicology,University of Toronto Medical Sciences Building,1 King’s College Circle Toronto,ON, Canada M5S 1A8
Introduction
The editorial by Cre´pault, Rehm & Fischer (p.1 of this issue)
provides a detailed description of the origins and rationale of a
CAMH document entitled Cannabis Policy Framework (Cre´pault,
2014),referred to below as the CPF.As described in the editorial,
the CPF concluded with a recommendation for legalization of non-
medical use of cannabis,with reliance on strict application of
regulations to prevent access to cannabis by underage users who
are most vulnerable to its adverse effects on health and social
functioning. As the editorial explains, the CPF grew out of an earlier
document from the Addiction Research Foundation (ARF)that
called for a public health approach to cannabis policy and for
decriminalization of possession for personal use (Addiction
Research Foundation, 1997). This recommendation was also made
in the LeDain Commission Report (Canadian Government,1972),
and was maintained in CAMH statements that preceded the CPF. It
is therefore useful to examine the reasons that led to the changed
recommendation in the CPF and other recent similar publications
(Haden & Emerson,2014; Spithoff,Emerson,& Spithoff,2015).
Among the important considerations mentioned in the editorial
are the following:
social harms caused by prohibition, and by its inequitable
application,
the relative modesty of the health harms attributable to cannabis
use in the majority of users,
costliness and ineffectiveness of prohibition,combined with its
deterrence of public health measures aimed at prevention and
treatment of drug-induced harm,
superior ability of legalization to prevent harm to vulnerable
groups by the use of regulatory controls that cannot be
implemented under decriminalization,
the risk that decriminalization could actually encourage the
production and distribution of cannabis.
International Journal of Drug Policy 34 (2016) 5–10
A R T I C L E I N F O
Article history:
Received 11 November 2015
Received in revised form 27 April 2016
Accepted 9 May 2016
Keywords:
Cannabis policy
Legalization
Decriminalization
Harms caused by prohibition
Harms to adolescent users
Cost-benefit assessment
A B S T R A C T
An editorial in this issue describes a cannabis policy framework document issued by a major Canadian
research centre,calling for legalization of non-medical use under strict controls to prevent increase in
use, especially by adolescents and young adults who are most vulnerable to adverse effects of cannabis
claims that such a system would eliminate the severe personal, social and monetary costs of prohibition
diminish the illicit market, and provide more humane management of cannabis use disorders. It claims
that experience with regulation of alcohol and tobacco will enable a system based on public health
principles to control access of youth to cannabis without the harm caused by prohibition.
The present critique argues that the claims made against decriminalization and for legalization are
unsupported,or even contradicted,by solid evidence.Early experience in other jurisdictions suggests
that legalization increases use by adolescents and its attendant harms. Regulation of alcohol use does n
provide a good model for cannabis controls because there is widespread alcohol use and harm among
adolescents and young adults.Government monopolies of alcoholsale have been used primarily as
sources of revenue rather than for guarding public health, and no reason has been offered to believe the
would act differently with respect to cannabis.
Good policy decisions require extensive unbiased information about the individual and social benefits
and costs of both drug use and proposed control measures, and value judgments about the benefit/harm
balance of each option. Important parts of the necessary knowledge about cannabis are not yet availabl
so that the value judgments are not yet possible. Therefore,a better case can be made for eliminating
some of the harms of prohibition by decriminalization of cannabis possession and deferring decision
about legalization until the necessary knowledge has been acquired.
ß 2016 Elsevier B.V.All rights reserved.
E-mail address: harold.kalant@utoronto.ca.
Contents lists available at ScienceDirect
International Journal of Drug Policy
j o u r n a lh o m e p a g e :w w w . e l s e v i e r . c o m / l o c a t e / d r u g p o
http://dx.doi.org/10.1016/j.drugpo.2016.05.002
0955-3959/ß 2016 Elsevier B.V.All rights reserved.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
The validity of the model proposed in the CPF and reproduced
verbatim in the editorial can be assessed by examining the
available evidence concerning these and some related issues.
Is prohibition ineffective or a failure?
Prohibition has indeed failed to prevent all use of the drug, but
this is not a reasonable expectation.No prohibition, whether of
something as minor as smoking too close to a hospital entrance, as
common as exceeding speed limits,or as grave as murder, is
expected to be 100% effective. All one can reasonably expect from
prohibition of any undesirable behavior is that it asserts society’s
disapproval,and makes the disapproved behavior substantially
less frequent than it would otherwise be.
Prohibition of alcohol in North America in the 1920s and early
1930s did markedly reduce consumption and public intoxication
(Dills, Jacobson,& Miron, 2005) as well as the death rate from
alcoholic cirrhosis (Dills & Miron, 2004). However, it also had
various socially harmful consequences such as the growth of
bootlegging and organized crime,corruption of police forces,loss
of employment in alcohol-related industries and loss of important
tax revenues (Blocker,2006). It deprived millions of moderate
drinkers of what was for most of them a harmless pleasure,and
possibly of alleged health benefits of moderate consumption
(Kalant & Poikolainen, 1999). Therefore, prohibition did work, but
at the cost of important social harms. One must make a value
judgment as to whether the costs to society outweighed the
benefits,but that is not the same as saying that prohibition was
ineffective.
Neither can one say that cannabis prohibition is ineffective if
use is significantly less than it would be under legalization.The
percentage ofpast-year users ofcannabis among the Canadian
general population in 2012 was only 10% while that of the legal
drug alcohol was 78% (Health Canada, 2014). A recent study found
that 10% of US high school students who had not yet used
marijuana intended to use it if it became legal,and 18% of those
who had already used it declared intention to use more frequently
(Palamar, Ompad, & Petkova, 2014). These probably represent
minimum increases, because when the more decisive users
increase consumption,their attitudes and behaviors affect other
members of their peer groups to act similarly (Keyes et al.,2011;
Salvy,Pedersen,Miles, Tucker,& D’Amico,2014).
Greater permissiveness in the United States has been accom-
panied by a doubling of rates of use and of use disorders from
2002 to 2012 (Hasin et al.,2015).American states that adopted
very poorly controlled medical marijuana laws (MML) tantamount
to legalization had higher rates of marijuana use, abuse and
dependence than states without such laws,even among adoles-
cents who were not eligible for medical permits (Cerda`, Wall,
Keyes, Galea, & Hasin, 2012; Wall et al., 2011). ‘‘Medical’’
marijuana was deviated to illicit use in non-MML states
(Thurstone, Lieberman, & Schmiege, 2011), a risk that also applies
to legalization in Colorado (RMHIDTA,2015). In contrast, Choo
et al. (2014) did not find increased use by adolescents in states
adopting MML, and Masten and Guenzburger (2014) found that
some MML states experienced a significant increase in cannabis-
related traffic fatalities while other MML states did not.Until the
difference between the results of these studies can be explained, it
is unwarranted to argue that we know how to prevent increased
use after legalization.
Preliminary evidence to date indicates that in Colorado
cannabis use among 12 17, 18 25, and over-26 age groups
increased by between 17% and 63% in the 2 years after legalization
compared to the 2 years before,while national averages for the
same groups were either unchanged or lower (RMHIDTA,2016).
We will not know for some years yet whether the increases were
temporary or permanent, nor the resulting social costs in terms of
school and work performance, physical and mental health,
automobile accidents and deaths,etc. Without such knowledge,
there is no factual basis for saying that legalization is a better policy
for society than prohibition or decriminalization. Legalization is in
harmony with the democratic ideal of restricting individual liberty
of action only when necessary for the common good,but judging
what constitutes the common good requires comprehensive
knowledge of the consequences of each policy option,which we
do not yet have.
Does cannabis prohibition impose serious personal harms on
society that would be removed by legalization?
The editorial refers only briefly to the social harms caused by
prohibition of cannabis,but the CPF states that ‘‘Around 60,000
Canadians are arrested for simple possession ofcannabis every
year’’. The figure is based on data from Statistics Canada
(2014).This statement,combined with the CPF reference to only
the maximum possible sentences provided for in the law, gives the
impression that large numbers of Canadians suffer severe penalties
every year for simple possession of cannabis under the present
prohibition. However, Statistics Canada records all cannabis
incident reports by the police in each province, regardless of
whether cannabis possession is the principal object of the incident
or only a minor accompaniment to other more serious charges, and
the statistics give no indication of the outcomes.
In contrast,Pauls, Plecas,Cohen,& Haarhoff (2012),with the
help of the RCMP, had access to the complete files (names
removed) of all case reports in British Columbia over a 3-year
period and were able to separate them into subgroups according to
the nature of the charges and the outcomes. The results present a
dramatically different picture from that implied by the CPF.In
2011, of 22,561 files coded for marijuana possession in British
Columbia, 4,355 were dropped because of insufficient evidence. Of
the 18,206 cases in which possession was demonstrated, the great
majority were let off without being charged, e.g. with a warning or
simply a decision not to proceed. In 4,257 cases charges were laid,
but in most cases the possession charge was a minor addition to
charges of more serious crimes such as trafficking, violence,
impaired driving or others.Of the 249 charged only with simple
possession, one-third had the charges dropped and did not come to
trial. Of those that came to trial, only 42 were convicted, the others
being acquitted, discharged, or directed to treatment. Finally, only
seven of those convicted were sentenced to jail for 114 days, and
these were all repeat offenders with long criminal histories. Very
similar proportions of outcomes were found in each of 2009,
2010 and 2011. It is clear, therefore, that in British Columbia very
few people accused only of simple possession of marijuana actually
come to trial, and extremely few are convicted and fined or jailed.
Correspondingly detailed figures forOntario and for all of
Canada are not available. However, in Ontario in 2013 there were
17,641 reported incidents of cannabis possession; of these 8,045
were cleared without charges, 8,706 led to charges, and 890 were
not yet cleared (CANSIM, 2013). Among detained youth,1,281
were charged whereas 3,804 youths were released without
charges.Generally,similar figures were found for Canada as a
whole (Boyce, 2013). These figures are proportionally very
different from those prevalent in the United States, though federal
law in both countries prohibits non-medical use of cannabis.The
difference demonstrates that the manner of enforcement,rather
than prohibition per se,determines the magnitude of the social
cost. The foregoing discussion does not in any way deny the
seriousness of arrests and criminal records for simple possession of
cannabis,but in the weighing of costs and benefits of different
policy options,the size of the problem matters.There is a clear
H. Kalant / International Journal of Drug Policy 34 (2016) 5–106
verbatim in the editorial can be assessed by examining the
available evidence concerning these and some related issues.
Is prohibition ineffective or a failure?
Prohibition has indeed failed to prevent all use of the drug, but
this is not a reasonable expectation.No prohibition, whether of
something as minor as smoking too close to a hospital entrance, as
common as exceeding speed limits,or as grave as murder, is
expected to be 100% effective. All one can reasonably expect from
prohibition of any undesirable behavior is that it asserts society’s
disapproval,and makes the disapproved behavior substantially
less frequent than it would otherwise be.
Prohibition of alcohol in North America in the 1920s and early
1930s did markedly reduce consumption and public intoxication
(Dills, Jacobson,& Miron, 2005) as well as the death rate from
alcoholic cirrhosis (Dills & Miron, 2004). However, it also had
various socially harmful consequences such as the growth of
bootlegging and organized crime,corruption of police forces,loss
of employment in alcohol-related industries and loss of important
tax revenues (Blocker,2006). It deprived millions of moderate
drinkers of what was for most of them a harmless pleasure,and
possibly of alleged health benefits of moderate consumption
(Kalant & Poikolainen, 1999). Therefore, prohibition did work, but
at the cost of important social harms. One must make a value
judgment as to whether the costs to society outweighed the
benefits,but that is not the same as saying that prohibition was
ineffective.
Neither can one say that cannabis prohibition is ineffective if
use is significantly less than it would be under legalization.The
percentage ofpast-year users ofcannabis among the Canadian
general population in 2012 was only 10% while that of the legal
drug alcohol was 78% (Health Canada, 2014). A recent study found
that 10% of US high school students who had not yet used
marijuana intended to use it if it became legal,and 18% of those
who had already used it declared intention to use more frequently
(Palamar, Ompad, & Petkova, 2014). These probably represent
minimum increases, because when the more decisive users
increase consumption,their attitudes and behaviors affect other
members of their peer groups to act similarly (Keyes et al.,2011;
Salvy,Pedersen,Miles, Tucker,& D’Amico,2014).
Greater permissiveness in the United States has been accom-
panied by a doubling of rates of use and of use disorders from
2002 to 2012 (Hasin et al.,2015).American states that adopted
very poorly controlled medical marijuana laws (MML) tantamount
to legalization had higher rates of marijuana use, abuse and
dependence than states without such laws,even among adoles-
cents who were not eligible for medical permits (Cerda`, Wall,
Keyes, Galea, & Hasin, 2012; Wall et al., 2011). ‘‘Medical’’
marijuana was deviated to illicit use in non-MML states
(Thurstone, Lieberman, & Schmiege, 2011), a risk that also applies
to legalization in Colorado (RMHIDTA,2015). In contrast, Choo
et al. (2014) did not find increased use by adolescents in states
adopting MML, and Masten and Guenzburger (2014) found that
some MML states experienced a significant increase in cannabis-
related traffic fatalities while other MML states did not.Until the
difference between the results of these studies can be explained, it
is unwarranted to argue that we know how to prevent increased
use after legalization.
Preliminary evidence to date indicates that in Colorado
cannabis use among 12 17, 18 25, and over-26 age groups
increased by between 17% and 63% in the 2 years after legalization
compared to the 2 years before,while national averages for the
same groups were either unchanged or lower (RMHIDTA,2016).
We will not know for some years yet whether the increases were
temporary or permanent, nor the resulting social costs in terms of
school and work performance, physical and mental health,
automobile accidents and deaths,etc. Without such knowledge,
there is no factual basis for saying that legalization is a better policy
for society than prohibition or decriminalization. Legalization is in
harmony with the democratic ideal of restricting individual liberty
of action only when necessary for the common good,but judging
what constitutes the common good requires comprehensive
knowledge of the consequences of each policy option,which we
do not yet have.
Does cannabis prohibition impose serious personal harms on
society that would be removed by legalization?
The editorial refers only briefly to the social harms caused by
prohibition of cannabis,but the CPF states that ‘‘Around 60,000
Canadians are arrested for simple possession ofcannabis every
year’’. The figure is based on data from Statistics Canada
(2014).This statement,combined with the CPF reference to only
the maximum possible sentences provided for in the law, gives the
impression that large numbers of Canadians suffer severe penalties
every year for simple possession of cannabis under the present
prohibition. However, Statistics Canada records all cannabis
incident reports by the police in each province, regardless of
whether cannabis possession is the principal object of the incident
or only a minor accompaniment to other more serious charges, and
the statistics give no indication of the outcomes.
In contrast,Pauls, Plecas,Cohen,& Haarhoff (2012),with the
help of the RCMP, had access to the complete files (names
removed) of all case reports in British Columbia over a 3-year
period and were able to separate them into subgroups according to
the nature of the charges and the outcomes. The results present a
dramatically different picture from that implied by the CPF.In
2011, of 22,561 files coded for marijuana possession in British
Columbia, 4,355 were dropped because of insufficient evidence. Of
the 18,206 cases in which possession was demonstrated, the great
majority were let off without being charged, e.g. with a warning or
simply a decision not to proceed. In 4,257 cases charges were laid,
but in most cases the possession charge was a minor addition to
charges of more serious crimes such as trafficking, violence,
impaired driving or others.Of the 249 charged only with simple
possession, one-third had the charges dropped and did not come to
trial. Of those that came to trial, only 42 were convicted, the others
being acquitted, discharged, or directed to treatment. Finally, only
seven of those convicted were sentenced to jail for 114 days, and
these were all repeat offenders with long criminal histories. Very
similar proportions of outcomes were found in each of 2009,
2010 and 2011. It is clear, therefore, that in British Columbia very
few people accused only of simple possession of marijuana actually
come to trial, and extremely few are convicted and fined or jailed.
Correspondingly detailed figures forOntario and for all of
Canada are not available. However, in Ontario in 2013 there were
17,641 reported incidents of cannabis possession; of these 8,045
were cleared without charges, 8,706 led to charges, and 890 were
not yet cleared (CANSIM, 2013). Among detained youth,1,281
were charged whereas 3,804 youths were released without
charges.Generally,similar figures were found for Canada as a
whole (Boyce, 2013). These figures are proportionally very
different from those prevalent in the United States, though federal
law in both countries prohibits non-medical use of cannabis.The
difference demonstrates that the manner of enforcement,rather
than prohibition per se,determines the magnitude of the social
cost. The foregoing discussion does not in any way deny the
seriousness of arrests and criminal records for simple possession of
cannabis,but in the weighing of costs and benefits of different
policy options,the size of the problem matters.There is a clear
H. Kalant / International Journal of Drug Policy 34 (2016) 5–106
need for full and accurate nationwide information,which we do
not yet have.
Statistics Canada does indicate that over 699,000 Canadians
have criminal records as a result of convictions on charges of
cannabis possession, many of which occurred decades ago during
their adolescence before the Youth Criminal Justice Act came into
effect. This is certainly an important harmful effect of prohibition
of cannabis possession, and either legalization or decriminalization
would prevent it from happening in the future.However,neither
would undo the harm to those who already have criminal records.
A legislated amnesty would be required, but this could be done in
connection with decriminalization or even with continued
prohibition,and is not necessarily linked to legalization.
As in the United States, some Canadian provinces show greater
severity of application of cannabis prohibition than others.That
could just as logically call for federal government action to impose
uniform moderate sentencing rules across the country as for
legalization of cannabis use.
Does prohibition of cannabis impede the application of
measures to reduce drug-related harm to health?
The editorial’s statement to this effect is more cautious than the
CPF statement that ‘‘The law enforcement focus ofprohibition
drives cannabis users away from prevention,risk reduction and
treatment services’’,for which it cites no supporting literature. In
fact, prohibition of cannabis possession is not necessarily in
conflict with treatment of dependent persons.Diversion of cases
from the justice to the health care system has been occurring with
increasing frequency in Australia (Feeney, Connor, Young, Tucker,
& McPherson,2005),Portugal (Hughes & Stevens,2010),Canada
(Pauls et al[7_TD$DIFF]., 2012) and the UK and elsewhere in Europe (Hamilton,
Lloyd,Monaghan,& Paton,2014) where possession is still illegal.
Are adolescents and young adults especially vulnerable to the
adverse effects of cannabis on health and wellbeing?
The editorial asserts that harms caused to most users by
cannabis are relatively modest,significantly less than those for
tobacco or alcohol. It does say ‘‘at the levels and patterns of use by
most adult cannabis users’’, and this is an important qualification,
because the use of cannabis in Canada, as noted earlier, is much less
than that of alcohol. It has long been recognized that the extent of
harm caused by a drug is proportional to its use (CANYS,2009;
Hughes et al.,2014).If cannabis legalization should prove to be
followed by an important increase in its use, as discussed
elsewhere in this commentary, the difference between the extent
of harms caused by alcohol and by cannabis would almost certainly
be considerably reduced.
A more important reservation even now relates to harms
caused to young users. Both the editorial and the CPF do discuss
the potentially serious effects of cannabis use by adolescents on
mental health and maturation of cognitive functions (Hall &
Degenhardt, 2007). The importance of this topic for policy
considerations warrants a more detailed consideration. The
Dunedin study in New Zealand followed a birth cohort of over
1400 newborns through childhood, adolescence,young adult-
hood and into early middle age. Histories and mental and
physical examinations were repeated at intervals throughout
the study, measuring among many other things the effects of
early acquisition of drug-taking behavior and its maintenance or
cessation (Milne et al., 2009). A thorough analysis of the
Dunedin results (Meier et al.,2012) demonstrated that children
who did not acquire cannabis-taking behavior had a smallbut
significant increase in age-adjusted intelligence score from age
13 to age 38. Those who began cannabis use during adolescence
had a decrease in IQ at age 38, which was more marked the
earlier they had begun use, and the more intensively and
persistently they used.Similar findings were obtained in other
cohort studies (Silins, Horwood, Patton, Fergusson,& Olsson,
2014).
All tested domains of cognitive functioning were affected, and
the effect was recognizable in everyday living,including poor
school performance, higher drop-out rates, and subsequent
restriction of career possibilities.It could not be explained by
decreased years ofschooling, persistent drug presence in the
body, socioeconomic status, or other potential confounders.
Cessation of use was followed by recovery of cognitive functions
in those who began use as young adults,but not in those who
began early in adolescence. The findings are consistent with
experimental studies showing that cannabinoids prevent mature
synapse formation in maturing brain pathways involved in
‘‘executive functioning’’ (Kalant, 2014), and that the same chronic
cannabis regimen (with dosage adjusted for body mass) that
caused permanent impairment of learning and memory in
adolescent rats did not do so in mature adult rats (Stiglick &
Kalant, 1985).
A clinical diagnosis of cannabis dependency by DSM-IV criteria
was found in about 8 10% ofadult users,but in about 16% of
adolescent users (Anthony,2006).A prospective 3-year study of
young adult frequent users, aged 18 to 30 years at baseline, found a
37% cumulative incidence of dependence (van der Pol et al., 2012).
The risk of future lung cancer in heavy cannabis users of military
conscription age represents another type ofvulnerability (Call-
aghan,Allebeck,& Sidorchuk,2013).
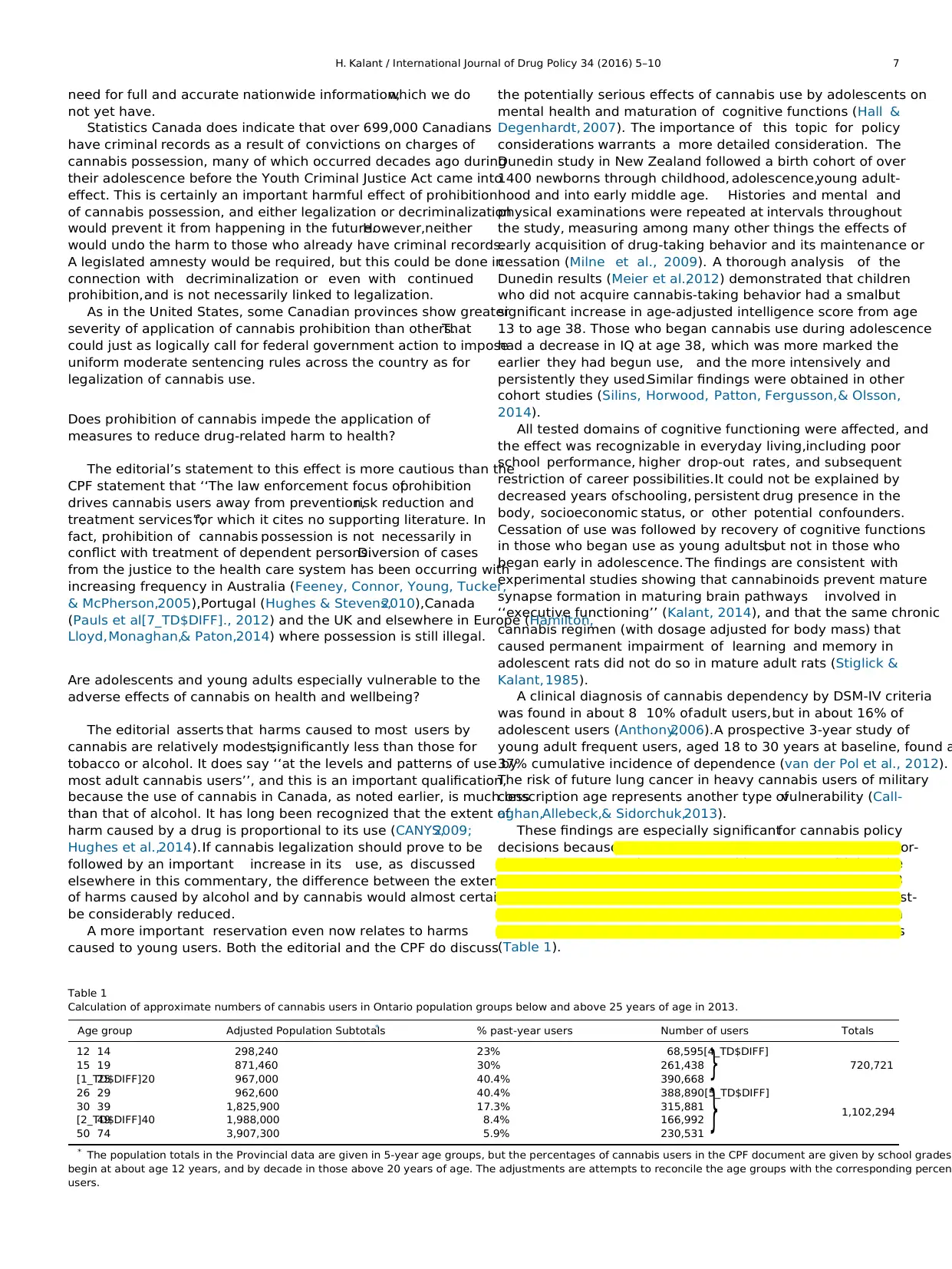
These findings are especially significantfor cannabis policy
decisions because adolescents and young adults are dispropor-
tionately represented among cannabis users.By combining the
provincial statistics of the population age distribution in 2013
(Ontario Ministry of Finance,2014) with the percentages of past-
year users in different age groups as shown in the CPF,one can
estimate that 43% of users are adolescents and young adults
(Table 1).
}
}
Table 1
Calculation of approximate numbers of cannabis users in Ontario population groups below and above 25 years of age in 2013.
Age group Adjusted Population Subtotals* % past-year users Number of users Totals
12 14 298,240 23% 68,595[4_TD$DIFF]
720,72115 19 871,460 30% 261,438
[1_TD$DIFF]2025 967,000 40.4% 390,668
26 29 962,600 40.4% 388,890[5_TD$DIFF]
1,102,294
30 39 1,825,900 17.3% 315,881
[2_TD$DIFF]4049 1,988,000 8.4% 166,992
50 74 3,907,300 5.9% 230,531
* The population totals in the Provincial data are given in 5-year age groups, but the percentages of cannabis users in the CPF document are given by school grades
begin at about age 12 years, and by decade in those above 20 years of age. The adjustments are attempts to reconcile the age groups with the corresponding percen
users.
H. Kalant / International Journal of Drug Policy 34 (2016) 5–10 7
not yet have.
Statistics Canada does indicate that over 699,000 Canadians
have criminal records as a result of convictions on charges of
cannabis possession, many of which occurred decades ago during
their adolescence before the Youth Criminal Justice Act came into
effect. This is certainly an important harmful effect of prohibition
of cannabis possession, and either legalization or decriminalization
would prevent it from happening in the future.However,neither
would undo the harm to those who already have criminal records.
A legislated amnesty would be required, but this could be done in
connection with decriminalization or even with continued
prohibition,and is not necessarily linked to legalization.
As in the United States, some Canadian provinces show greater
severity of application of cannabis prohibition than others.That
could just as logically call for federal government action to impose
uniform moderate sentencing rules across the country as for
legalization of cannabis use.
Does prohibition of cannabis impede the application of
measures to reduce drug-related harm to health?
The editorial’s statement to this effect is more cautious than the
CPF statement that ‘‘The law enforcement focus ofprohibition
drives cannabis users away from prevention,risk reduction and
treatment services’’,for which it cites no supporting literature. In
fact, prohibition of cannabis possession is not necessarily in
conflict with treatment of dependent persons.Diversion of cases
from the justice to the health care system has been occurring with
increasing frequency in Australia (Feeney, Connor, Young, Tucker,
& McPherson,2005),Portugal (Hughes & Stevens,2010),Canada
(Pauls et al[7_TD$DIFF]., 2012) and the UK and elsewhere in Europe (Hamilton,
Lloyd,Monaghan,& Paton,2014) where possession is still illegal.
Are adolescents and young adults especially vulnerable to the
adverse effects of cannabis on health and wellbeing?
The editorial asserts that harms caused to most users by
cannabis are relatively modest,significantly less than those for
tobacco or alcohol. It does say ‘‘at the levels and patterns of use by
most adult cannabis users’’, and this is an important qualification,
because the use of cannabis in Canada, as noted earlier, is much less
than that of alcohol. It has long been recognized that the extent of
harm caused by a drug is proportional to its use (CANYS,2009;
Hughes et al.,2014).If cannabis legalization should prove to be
followed by an important increase in its use, as discussed
elsewhere in this commentary, the difference between the extent
of harms caused by alcohol and by cannabis would almost certainly
be considerably reduced.
A more important reservation even now relates to harms
caused to young users. Both the editorial and the CPF do discuss
the potentially serious effects of cannabis use by adolescents on
mental health and maturation of cognitive functions (Hall &
Degenhardt, 2007). The importance of this topic for policy
considerations warrants a more detailed consideration. The
Dunedin study in New Zealand followed a birth cohort of over
1400 newborns through childhood, adolescence,young adult-
hood and into early middle age. Histories and mental and
physical examinations were repeated at intervals throughout
the study, measuring among many other things the effects of
early acquisition of drug-taking behavior and its maintenance or
cessation (Milne et al., 2009). A thorough analysis of the
Dunedin results (Meier et al.,2012) demonstrated that children
who did not acquire cannabis-taking behavior had a smallbut
significant increase in age-adjusted intelligence score from age
13 to age 38. Those who began cannabis use during adolescence
had a decrease in IQ at age 38, which was more marked the
earlier they had begun use, and the more intensively and
persistently they used.Similar findings were obtained in other
cohort studies (Silins, Horwood, Patton, Fergusson,& Olsson,
2014).
All tested domains of cognitive functioning were affected, and
the effect was recognizable in everyday living,including poor
school performance, higher drop-out rates, and subsequent
restriction of career possibilities.It could not be explained by
decreased years ofschooling, persistent drug presence in the
body, socioeconomic status, or other potential confounders.
Cessation of use was followed by recovery of cognitive functions
in those who began use as young adults,but not in those who
began early in adolescence. The findings are consistent with
experimental studies showing that cannabinoids prevent mature
synapse formation in maturing brain pathways involved in
‘‘executive functioning’’ (Kalant, 2014), and that the same chronic
cannabis regimen (with dosage adjusted for body mass) that
caused permanent impairment of learning and memory in
adolescent rats did not do so in mature adult rats (Stiglick &
Kalant, 1985).
A clinical diagnosis of cannabis dependency by DSM-IV criteria
was found in about 8 10% ofadult users,but in about 16% of
adolescent users (Anthony,2006).A prospective 3-year study of
young adult frequent users, aged 18 to 30 years at baseline, found a
37% cumulative incidence of dependence (van der Pol et al., 2012).
The risk of future lung cancer in heavy cannabis users of military
conscription age represents another type ofvulnerability (Call-
aghan,Allebeck,& Sidorchuk,2013).
These findings are especially significantfor cannabis policy
decisions because adolescents and young adults are dispropor-
tionately represented among cannabis users.By combining the
provincial statistics of the population age distribution in 2013
(Ontario Ministry of Finance,2014) with the percentages of past-
year users in different age groups as shown in the CPF,one can
estimate that 43% of users are adolescents and young adults
(Table 1).
}
}
Table 1
Calculation of approximate numbers of cannabis users in Ontario population groups below and above 25 years of age in 2013.
Age group Adjusted Population Subtotals* % past-year users Number of users Totals
12 14 298,240 23% 68,595[4_TD$DIFF]
720,72115 19 871,460 30% 261,438
[1_TD$DIFF]2025 967,000 40.4% 390,668
26 29 962,600 40.4% 388,890[5_TD$DIFF]
1,102,294
30 39 1,825,900 17.3% 315,881
[2_TD$DIFF]4049 1,988,000 8.4% 166,992
50 74 3,907,300 5.9% 230,531
* The population totals in the Provincial data are given in 5-year age groups, but the percentages of cannabis users in the CPF document are given by school grades
begin at about age 12 years, and by decade in those above 20 years of age. The adjustments are attempts to reconcile the age groups with the corresponding percen
users.
H. Kalant / International Journal of Drug Policy 34 (2016) 5–10 7
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Would legalization plus strict regulation effectively prevent
access to cannabis by underage users?
The claim that alcohol and tobacco control measures provide a
good model for controlling youth access to cannabis after
legalization (Pacula,Kilmer, Wagenaar,Chaloupka,& Caulkins,
2014; Room, 2014) is also contrary to experience. Alcohol
continues to be widely used by Ontario students at all age levels
examined (Boak, Hamilton, Adlaf, & Mann, 2013), despite
regulations against its sale or distribution to minors.Past-year
use was reported by almost 10% of Grade 7 students (1213 years
old), increasing to 74% of Grade 12 students. About 67% reported
drinking at least once a week, 20% reported binge-drinking within
the past month and 18% reported getting intoxicated in the same
period.
Among fatally injured drivers in Canada in the period 2000 to
2007, 17.4% ofthose aged 19 years or less tested positive for
alcohol,18.6% for drugs (predominantly cannabis) and about 14%
for both alcohol and drugs (Beasley,Beirness,& Porath-Waller,
2011). Similarly high and growing percentages report driving
under the influence of alcohol or cannabis,and even more report
being passengers in vehicles operated by alcohol- or cannabis-
impaired drivers (Adlaf, Mann, & Paglia, 2003). These figures
become more disturbing when viewed againstthe increase in
cannabis-related driverfatalities seen in Colorado after broad
commercialization of ‘‘medicalmarijuana’’(Salomonsen-Sautel,
Min, Sakai,Thurstone,& Hopfer,2014).Such statistics of alcohol
use,binge drinking and driving while intoxicated among under-
age users in Ontario can hardly be considered evidence for the
efficacy of current alcohol regulations in preventing access to
alcohol by those considered to be at too great a risk to be allowed to
use it. It is therefore puzzling that the CPF, as cited in the editorial,
without presenting any supporting evidence assumes that
regulation would be successfulin preventing access of under-
age users to cannabis after legalization.
Would legalization of cannabis, combined with regulation,
significantly reduce the illicit market and its associated
dangers?
As the CPF states,experience with alcoholand tobacco has
shown that price is an important determinant of per capita
consumption and of the numbers of those who suffer serious harm
from excessive consumption (Guindon,2014; Her, Giesbrecht,
Room,& Rehm,1999; Wakefield & Chaloupka,2000).Most adult
users would probably prefer to buy legal cannabis even if the price
is somewhat higher than the street price,but if the regulations
prevent sales to underage users,they would have no incentive to
stop purchasing from their accustomed illicit sources. Moreover, if
the price for legal cannabis is made significantly lower to undercut
the black market, the levels of use, especially by young people with
more limited financial resources, are likely to increase even further
rather than decrease (Anderson, 2007; Caulkins, Kilmer, MacCoun,
Pacula,& Reuter,2012; Osterberg,2011).
Tobacco presents a better model than alcohol for comparison
with legalized cannabis, because the reduction of use by the
population at large has been achieved without use ofcriminal
sanctions,by a sustained campaign of public education on health
consequences of smoking (Wakefield & Chaloupka, 2000), compa-
rable to that which led to a marked decrease of alcoholuse in
France.But we do not yet appear to have developed an effective
approach with respect to cannabis comparable to that with
tobacco, especially for adolescents. A study of high school students
in the United States ongoing since 1976 has shown that likelihood
of marijuana use was inversely related to the percentages of
students in specific birth cohorts who disapproved of use and who
believed the information about its perceived dangers. Use among
the student population as a whole has gone through two cycles of
rising and falling, but the determinants of attitude in different birth
cohorts are not yet understood (Keyes et al.,2011).Use among
Canadian youth is currently decreasing,but until we know how
their attitudes are determined,and how to direct these so as to
build a health-conscious approach to cannabis use among them,
we cannot count on continued decrease of use.
The editorial and the CPF set out some very good recommenda-
tions for controlling the levelof use of legal cannabis: prohibit
marketing and advertising, limit density of sales outlets and hours
of sale, set maximum permissible concentration of THC, and some
would add setting maximum amount per sale. But other
recommendations lack substance, such as the proposal that pricing
policy should limit demand while minimizing the opportunity for
continuation of lucrative black markets. Limiting demand calls for
higher prices, yet higher prices encourage competition from lower-
priced black markets. The authors offer no way of dealing with this
incompatibility,or of selecting an optimal target price.
Does the possibility of deriving additional government
resources through taxation of legalized cannabis represent a
significant gain for society?
A major reason advanced by politicians who favor legalization
of cannabis is the possibility ofgaining a major new source of
revenue,comparable to that from the sale of alcohol,to support
increasingly expensive public health, education and social
programs.However, alcohol consumption generates very high
social and economic costs, possibly greater than the revenue
derived from the production and sale of alcohol (Rehm et al., 2007).
The CPF advances no reason why this would not also be true of
legal cannabis sale by a government monopoly.A very limited
analysis of some of the costs attributable to cannabis under the
present legal prohibition (Fischer, Imtiaz, Rudzinski, & Rehm,
2016) shows the need for much more extensive investigation of
this question. The CPF speaks of a need to avoid a financial
incentive for a government monopoly to increase cannabis sales.
This is idealistic but surely rather naive. Experience with the
Canadian provincial government monopolies of sales of spirits and
imported wines, with their sophisticated marketing activities and
maximized opportunities for access, does not offer any reason for
believing that sales practices with cannabis would be different.
Would legalization of cannabis reduce greatly the costs of
police and court work caused by the current policy of
prohibition?
The CPF states (p.11) that legalization ‘‘would eliminate the
more than $1 billion Canada spends annually to enforce cannabis
possession laws’’.However, other estimates are substantially
lower. One article quotes a Department of Justice budget for the
drug control strategy for all of Canada as $528 million for the
period 2012 2017, or about $106 million a year, and a Simon
Fraser University estimate of $10.5 to $18.5 million as the annual
cost for British Columbia (MacQueen,2013).
More importantly, if the British Columbia findings on the
disposition of cannabis possession incidents are representative of
Canada as a whole (which remains to be determined), there would
appear to be very little police or court time devoted to enforcing
the law against possession alone. The great majority of possession
charges were add-ons in cases in which the accused were detained
for other offences. If cannabis had been legal, the police would still
have had to expend the same effort in detaining and charging them
for the principal offences,and the courts would still have had to
deal with those principal charges. Under legalization, illicit
H. Kalant / International Journal of Drug Policy 34 (2016) 5–108
access to cannabis by underage users?
The claim that alcohol and tobacco control measures provide a
good model for controlling youth access to cannabis after
legalization (Pacula,Kilmer, Wagenaar,Chaloupka,& Caulkins,
2014; Room, 2014) is also contrary to experience. Alcohol
continues to be widely used by Ontario students at all age levels
examined (Boak, Hamilton, Adlaf, & Mann, 2013), despite
regulations against its sale or distribution to minors.Past-year
use was reported by almost 10% of Grade 7 students (1213 years
old), increasing to 74% of Grade 12 students. About 67% reported
drinking at least once a week, 20% reported binge-drinking within
the past month and 18% reported getting intoxicated in the same
period.
Among fatally injured drivers in Canada in the period 2000 to
2007, 17.4% ofthose aged 19 years or less tested positive for
alcohol,18.6% for drugs (predominantly cannabis) and about 14%
for both alcohol and drugs (Beasley,Beirness,& Porath-Waller,
2011). Similarly high and growing percentages report driving
under the influence of alcohol or cannabis,and even more report
being passengers in vehicles operated by alcohol- or cannabis-
impaired drivers (Adlaf, Mann, & Paglia, 2003). These figures
become more disturbing when viewed againstthe increase in
cannabis-related driverfatalities seen in Colorado after broad
commercialization of ‘‘medicalmarijuana’’(Salomonsen-Sautel,
Min, Sakai,Thurstone,& Hopfer,2014).Such statistics of alcohol
use,binge drinking and driving while intoxicated among under-
age users in Ontario can hardly be considered evidence for the
efficacy of current alcohol regulations in preventing access to
alcohol by those considered to be at too great a risk to be allowed to
use it. It is therefore puzzling that the CPF, as cited in the editorial,
without presenting any supporting evidence assumes that
regulation would be successfulin preventing access of under-
age users to cannabis after legalization.
Would legalization of cannabis, combined with regulation,
significantly reduce the illicit market and its associated
dangers?
As the CPF states,experience with alcoholand tobacco has
shown that price is an important determinant of per capita
consumption and of the numbers of those who suffer serious harm
from excessive consumption (Guindon,2014; Her, Giesbrecht,
Room,& Rehm,1999; Wakefield & Chaloupka,2000).Most adult
users would probably prefer to buy legal cannabis even if the price
is somewhat higher than the street price,but if the regulations
prevent sales to underage users,they would have no incentive to
stop purchasing from their accustomed illicit sources. Moreover, if
the price for legal cannabis is made significantly lower to undercut
the black market, the levels of use, especially by young people with
more limited financial resources, are likely to increase even further
rather than decrease (Anderson, 2007; Caulkins, Kilmer, MacCoun,
Pacula,& Reuter,2012; Osterberg,2011).
Tobacco presents a better model than alcohol for comparison
with legalized cannabis, because the reduction of use by the
population at large has been achieved without use ofcriminal
sanctions,by a sustained campaign of public education on health
consequences of smoking (Wakefield & Chaloupka, 2000), compa-
rable to that which led to a marked decrease of alcoholuse in
France.But we do not yet appear to have developed an effective
approach with respect to cannabis comparable to that with
tobacco, especially for adolescents. A study of high school students
in the United States ongoing since 1976 has shown that likelihood
of marijuana use was inversely related to the percentages of
students in specific birth cohorts who disapproved of use and who
believed the information about its perceived dangers. Use among
the student population as a whole has gone through two cycles of
rising and falling, but the determinants of attitude in different birth
cohorts are not yet understood (Keyes et al.,2011).Use among
Canadian youth is currently decreasing,but until we know how
their attitudes are determined,and how to direct these so as to
build a health-conscious approach to cannabis use among them,
we cannot count on continued decrease of use.
The editorial and the CPF set out some very good recommenda-
tions for controlling the levelof use of legal cannabis: prohibit
marketing and advertising, limit density of sales outlets and hours
of sale, set maximum permissible concentration of THC, and some
would add setting maximum amount per sale. But other
recommendations lack substance, such as the proposal that pricing
policy should limit demand while minimizing the opportunity for
continuation of lucrative black markets. Limiting demand calls for
higher prices, yet higher prices encourage competition from lower-
priced black markets. The authors offer no way of dealing with this
incompatibility,or of selecting an optimal target price.
Does the possibility of deriving additional government
resources through taxation of legalized cannabis represent a
significant gain for society?
A major reason advanced by politicians who favor legalization
of cannabis is the possibility ofgaining a major new source of
revenue,comparable to that from the sale of alcohol,to support
increasingly expensive public health, education and social
programs.However, alcohol consumption generates very high
social and economic costs, possibly greater than the revenue
derived from the production and sale of alcohol (Rehm et al., 2007).
The CPF advances no reason why this would not also be true of
legal cannabis sale by a government monopoly.A very limited
analysis of some of the costs attributable to cannabis under the
present legal prohibition (Fischer, Imtiaz, Rudzinski, & Rehm,
2016) shows the need for much more extensive investigation of
this question. The CPF speaks of a need to avoid a financial
incentive for a government monopoly to increase cannabis sales.
This is idealistic but surely rather naive. Experience with the
Canadian provincial government monopolies of sales of spirits and
imported wines, with their sophisticated marketing activities and
maximized opportunities for access, does not offer any reason for
believing that sales practices with cannabis would be different.
Would legalization of cannabis reduce greatly the costs of
police and court work caused by the current policy of
prohibition?
The CPF states (p.11) that legalization ‘‘would eliminate the
more than $1 billion Canada spends annually to enforce cannabis
possession laws’’.However, other estimates are substantially
lower. One article quotes a Department of Justice budget for the
drug control strategy for all of Canada as $528 million for the
period 2012 2017, or about $106 million a year, and a Simon
Fraser University estimate of $10.5 to $18.5 million as the annual
cost for British Columbia (MacQueen,2013).
More importantly, if the British Columbia findings on the
disposition of cannabis possession incidents are representative of
Canada as a whole (which remains to be determined), there would
appear to be very little police or court time devoted to enforcing
the law against possession alone. The great majority of possession
charges were add-ons in cases in which the accused were detained
for other offences. If cannabis had been legal, the police would still
have had to expend the same effort in detaining and charging them
for the principal offences,and the courts would still have had to
deal with those principal charges. Under legalization, illicit
H. Kalant / International Journal of Drug Policy 34 (2016) 5–108
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
production and trafficking would stillbe criminal offences,and
would still consume police and court time.It is therefore unclear
that very large economies to the justice system would be produced
by legalization of cannabis.
Is decriminalization a half measure, subject to manipulation by
police bias?
The editorial,like the CPF,refers to decriminalization as a half
measure because of three alleged flaws.The first is that ‘‘it may
encourage the production and distribution of cannabis’’,but no
evidence is offered to support this conjecture. Indeed the
decriminalization systems adopted in Portugal, Australia and
some American states did not increase use and may even have
reduced use and drug-related harms (Hughes & Stevens,2010;
Hughes & Stevens, 2012; Single, Christie, & Ali, 2000). The second
‘‘flaw’’ is that decriminalization ‘‘does not address the health
harms of cannabis use’’.The authors themselves have correctly
stated that legalization also does not address these harms, and that
specific regulatory mechanisms must be adopted for that purpose.
The Portuguese decriminalization system has adopted other
mechanisms to address these harms,including education,admo-
nition, and referral to treatment.
The third ‘‘flaw’’ is police bias in enforcement of the law under
decriminalization and inequality of imposition of penalties against
different subgroups of the population.This concern may well be
legitimate. However, the document does not discuss the possibility
that police bias could also persist after legalization,in relation to
prosecution for illicit production and trafficking.It also does not
examine alternative methods of dealing with this problem, such as
educational and administrative approaches to altering the police
culture, nor does it compare alternatives with respect to their costs
and benefits.
Discussion
Legalization of nonmedical use of cannabis and strict regulation
of its potency,price and accessibility represents an idealthat a
democratic society might well aim at, because it proposes the least
restriction of personal freedom compatible with the protection of
those most vulnerable to the adverse effects of cannabis use. Over a
15 year period Canadian public support of legalization gradually
rose to 37% in 2014 (Ipsos Reid, 2014). In 2015, it rose more rapidly,
in tandem with the popularity of Liberal Party leader Justin
Trudeau, as stated in the editorial. After his endorsementof
legalization a 2015 Ipsos-Reid poll found 65% in favour of
decriminalization, but the wording of the question was compatible
with legalization rather than decriminalization.It is difficult to
judge whether this shift of public opinion represents a ‘‘celebrity
effect’’,uncertainty of the meanings of the terms,a progressive
movement away from laws considered oppressive, or ‘‘normaliza-
tion’’ of cannabis use (Parker, Williams, & Aldridge, 2002), as a large
majority in that poll did not consider marijuana laws to be a high
priority matter.
Sound policy decisions require at least two essential elements:
(1) complete, objective, unbiased presentation of the facts
concerning the policy matter under review,including both what
we know and what we do not yet know,and scientifically based
predictions about the most probable consequences of the various
policy options; (2) value judgments that classify the various facts
and projections as good or bad,beneficialor harmful, useful or
useless,for society as a whole. It is also necessary to assign
quantitative weights – how good or bad, how beneficial or harmful
– so that the various policy options can be compared with respect to
their overall contribution to harm reduction and society’s wellbeing
(Kalant & Kalant,1971; Shanahan,Gerard,& Ritter,2014).
As set out in the preceding sections, we lack major portions of
the necessary evidence for making such a rational choice.
Therefore, any decision to legalize cannabis in Canada now cannot
really be ‘‘evidence-based’’and must rest primarily on broader
social values,ideals and hopes rather than on a thorough cost-
benefit accounting.A strong argument can be made for decrimi-
nalizing possession of cannabis for personal use, while monitoring
closely the effects of legalization,both beneficial and harmful,in
other states or countries that have already adopted it. A system of
legalization and strict controls could possibly work to the benefit of
society, but only if we find effective solutions to the problems set
out above before making changes that may cost society more than
it gains.
References
Addiction Research Foundation (1997).Cannabis.Health and Public Policy Retrieved
April 21, 2016,from http://www.camh.ca/en/hospital/about_camh/influencing_-
public_policy/Documents/Cannabis%20HealthPublicPolicy1997.pdf.
Adlaf, E. M., Mann, R. E., & Paglia, A. (2003). Drinking, cannabis use and driving among
Ontario students.CMAJ Canadian Medical Association Journal,168,565–566.
Anderson, P. (2007). A safe, sensible and social AHRSE: new Labour and alcohol policy.
Addiction,102,1515–1521.
Anthony, J. C. (2006). The epidemiology of cannabis dependence. In R. A. Roffman & R. S
Stephens (Eds.),Cannabis dependence: its nature,consequences treatment (pp.58–
195).Cambridge: Cambridge University Press.
Beasley,E. E., Beirness,D. J., & Porath-Waller,A. J. (2011).A comparison of drug- and
alcohol-involved motor vehicle driver fatalities.Ottawa: Canadian Centre on Sub-
stance Abuse.
Blocker,J. S.,Jr. (2006).Did Prohibition really work? Alcohol prohibition as a public
health innovation.American Journal of Public Health,96,233–243.
Boak,A., Hamilton,H. A., Adlaf,E. N., & Mann,R. E. (2013).Drug Use Among Ontario
Students 19772013. CAMH Research Document Series No. 36 ISBN: 978-1-77114-
167-3.
Boyce, J. (2013). Adult criminal court statistics in Canada 2011/2012, Table 5 and Chart 1
Ottawa: Canadian Centre for Justice Statistics.ISSN 1209-6393.(Juristat).
Callaghan,R. C., Allebeck,P., & Sidorchuk,A. (2013).Marijuana use and risk of lung
cancer: a 40-year cohort study.Cancer Causes & Control,24,1811–1820.
Canadian Government Commission of Inquiry into the Non-Medical Use of Drugs (1972).
Ottawa: Information Canada.
CANSIM (2013).Table 252-0051.Incident-based crime statistics,by detailed violations,
Ontario. Retrieved 2 November 2014 from http://www5.statcan.gc.ca/cansim/
a01?lang=eng.
CANYS – Council on Addictions of New York State (2009).Alcoholconsumption and
alcohol-related problems.Retrieved 29 October 2014 from http://www.canys.net/
images/ConsumptionBrief%20-%20Final%20-%206.29.09.pdf.
Caulkins,J. P., Kilmer, B., MacCoun,R. J., Pacula,R. L., & Reuter,P. (2012). Design
considerations for legalizing cannabis: lessons inspired by analysis of California’s
Proposition 19.Addiction,107,865–871.
Cerda`, M., Wall, M., Keyes, K. M., Galea, S., & Hasin, D. (2012). Medical marijuana laws in
50 states: investigating the relationship between state legalization ofmedical
marijuana and marijuana use,abuse and dependence.Drug and AlcoholDepen-
dence,120,22–27.
Choo, E. K., Benz, M., Zaller, N., Warren, O., Rising, K. L., & McConnell, K. J. (2014). The
impact of state medical marijuana legislation on adolescent marijuana use. Journal
of Adolescent Health,55,160–166.
Cre´pault,J.-F. (2014).Cannabis Policy Framework.CAMH Research Document Series No.
40,October 2014.Toronto: Centre for Addiction and Mental Health.
Dills, A. K., Jacobson,M., & Miron, J. A. (2005).The effect of alcoholprohibition on
alcohol consumption: evidence from drunkenness arrests.Economics Letters,86,
279–284.
Dills, A. K.,& Miron, J. A. (2004).Alcohol prohibition and cirrhosis.American Law and
Economics Reviews,6(2),2185–2318.http://dx.doi.org/10.1093/aler/ahh003
Feeney, G. F. X., Connor, J. P., Young, R. M., Tucker, J., & McPherson, A. (2005). Cannabis
dependence and mental health perception amongst people diverted by police after
arrest for cannabis-related offending behaviour in Australia. Criminal Behaviour &
Mental Health,15,249–260.
Fischer,B., Imtiaz, S.,Rudzinski,K., & Rehm,J. ([36_TD$DIFF]2016).Crude estimates of cannabis-
attributable mortality and morbidity in Canada -implications for public health
focused intervention priorities. Journal of Public Health, [37_TD$DIFF]38(January (28)
http://dx.doi.org/10.1093/pubmed/fdv005
Guindon, G. E. (2014). The impact of tobacco prices on smoking onset: a methodologi-
cal review.Tobacco Control,23(2),e5.
Haden,M., & Emerson,B. (2014).A vision for cannabis regulation: a public health
approach based on lessons learned from the regulation of alcoholand tobacco.
Open Medicine,8(2),1–16.
Hall, W., & Degenhardt,L. (2007). Prevalence and correlates ofcannabis use in
developed and developing countries.Current Opinion in Psychiatry,20,393–397.
Hamilton, I., Lloyd, C., Monaghan,M. P., & Paton,K. (2014).The emerging cannabis
treatment population.Drugs and Alcohol Today,14.159-153.Retrieved at http://
eprints.whiterose.ac.uk/82720/17/Cannabis%20Treatment.pdf.
H. Kalant / International Journal of Drug Policy 34 (2016) 5–10 9
would still consume police and court time.It is therefore unclear
that very large economies to the justice system would be produced
by legalization of cannabis.
Is decriminalization a half measure, subject to manipulation by
police bias?
The editorial,like the CPF,refers to decriminalization as a half
measure because of three alleged flaws.The first is that ‘‘it may
encourage the production and distribution of cannabis’’,but no
evidence is offered to support this conjecture. Indeed the
decriminalization systems adopted in Portugal, Australia and
some American states did not increase use and may even have
reduced use and drug-related harms (Hughes & Stevens,2010;
Hughes & Stevens, 2012; Single, Christie, & Ali, 2000). The second
‘‘flaw’’ is that decriminalization ‘‘does not address the health
harms of cannabis use’’.The authors themselves have correctly
stated that legalization also does not address these harms, and that
specific regulatory mechanisms must be adopted for that purpose.
The Portuguese decriminalization system has adopted other
mechanisms to address these harms,including education,admo-
nition, and referral to treatment.
The third ‘‘flaw’’ is police bias in enforcement of the law under
decriminalization and inequality of imposition of penalties against
different subgroups of the population.This concern may well be
legitimate. However, the document does not discuss the possibility
that police bias could also persist after legalization,in relation to
prosecution for illicit production and trafficking.It also does not
examine alternative methods of dealing with this problem, such as
educational and administrative approaches to altering the police
culture, nor does it compare alternatives with respect to their costs
and benefits.
Discussion
Legalization of nonmedical use of cannabis and strict regulation
of its potency,price and accessibility represents an idealthat a
democratic society might well aim at, because it proposes the least
restriction of personal freedom compatible with the protection of
those most vulnerable to the adverse effects of cannabis use. Over a
15 year period Canadian public support of legalization gradually
rose to 37% in 2014 (Ipsos Reid, 2014). In 2015, it rose more rapidly,
in tandem with the popularity of Liberal Party leader Justin
Trudeau, as stated in the editorial. After his endorsementof
legalization a 2015 Ipsos-Reid poll found 65% in favour of
decriminalization, but the wording of the question was compatible
with legalization rather than decriminalization.It is difficult to
judge whether this shift of public opinion represents a ‘‘celebrity
effect’’,uncertainty of the meanings of the terms,a progressive
movement away from laws considered oppressive, or ‘‘normaliza-
tion’’ of cannabis use (Parker, Williams, & Aldridge, 2002), as a large
majority in that poll did not consider marijuana laws to be a high
priority matter.
Sound policy decisions require at least two essential elements:
(1) complete, objective, unbiased presentation of the facts
concerning the policy matter under review,including both what
we know and what we do not yet know,and scientifically based
predictions about the most probable consequences of the various
policy options; (2) value judgments that classify the various facts
and projections as good or bad,beneficialor harmful, useful or
useless,for society as a whole. It is also necessary to assign
quantitative weights – how good or bad, how beneficial or harmful
– so that the various policy options can be compared with respect to
their overall contribution to harm reduction and society’s wellbeing
(Kalant & Kalant,1971; Shanahan,Gerard,& Ritter,2014).
As set out in the preceding sections, we lack major portions of
the necessary evidence for making such a rational choice.
Therefore, any decision to legalize cannabis in Canada now cannot
really be ‘‘evidence-based’’and must rest primarily on broader
social values,ideals and hopes rather than on a thorough cost-
benefit accounting.A strong argument can be made for decrimi-
nalizing possession of cannabis for personal use, while monitoring
closely the effects of legalization,both beneficial and harmful,in
other states or countries that have already adopted it. A system of
legalization and strict controls could possibly work to the benefit of
society, but only if we find effective solutions to the problems set
out above before making changes that may cost society more than
it gains.
References
Addiction Research Foundation (1997).Cannabis.Health and Public Policy Retrieved
April 21, 2016,from http://www.camh.ca/en/hospital/about_camh/influencing_-
public_policy/Documents/Cannabis%20HealthPublicPolicy1997.pdf.
Adlaf, E. M., Mann, R. E., & Paglia, A. (2003). Drinking, cannabis use and driving among
Ontario students.CMAJ Canadian Medical Association Journal,168,565–566.
Anderson, P. (2007). A safe, sensible and social AHRSE: new Labour and alcohol policy.
Addiction,102,1515–1521.
Anthony, J. C. (2006). The epidemiology of cannabis dependence. In R. A. Roffman & R. S
Stephens (Eds.),Cannabis dependence: its nature,consequences treatment (pp.58–
195).Cambridge: Cambridge University Press.
Beasley,E. E., Beirness,D. J., & Porath-Waller,A. J. (2011).A comparison of drug- and
alcohol-involved motor vehicle driver fatalities.Ottawa: Canadian Centre on Sub-
stance Abuse.
Blocker,J. S.,Jr. (2006).Did Prohibition really work? Alcohol prohibition as a public
health innovation.American Journal of Public Health,96,233–243.
Boak,A., Hamilton,H. A., Adlaf,E. N., & Mann,R. E. (2013).Drug Use Among Ontario
Students 19772013. CAMH Research Document Series No. 36 ISBN: 978-1-77114-
167-3.
Boyce, J. (2013). Adult criminal court statistics in Canada 2011/2012, Table 5 and Chart 1
Ottawa: Canadian Centre for Justice Statistics.ISSN 1209-6393.(Juristat).
Callaghan,R. C., Allebeck,P., & Sidorchuk,A. (2013).Marijuana use and risk of lung
cancer: a 40-year cohort study.Cancer Causes & Control,24,1811–1820.
Canadian Government Commission of Inquiry into the Non-Medical Use of Drugs (1972).
Ottawa: Information Canada.
CANSIM (2013).Table 252-0051.Incident-based crime statistics,by detailed violations,
Ontario. Retrieved 2 November 2014 from http://www5.statcan.gc.ca/cansim/
a01?lang=eng.
CANYS – Council on Addictions of New York State (2009).Alcoholconsumption and
alcohol-related problems.Retrieved 29 October 2014 from http://www.canys.net/
images/ConsumptionBrief%20-%20Final%20-%206.29.09.pdf.
Caulkins,J. P., Kilmer, B., MacCoun,R. J., Pacula,R. L., & Reuter,P. (2012). Design
considerations for legalizing cannabis: lessons inspired by analysis of California’s
Proposition 19.Addiction,107,865–871.
Cerda`, M., Wall, M., Keyes, K. M., Galea, S., & Hasin, D. (2012). Medical marijuana laws in
50 states: investigating the relationship between state legalization ofmedical
marijuana and marijuana use,abuse and dependence.Drug and AlcoholDepen-
dence,120,22–27.
Choo, E. K., Benz, M., Zaller, N., Warren, O., Rising, K. L., & McConnell, K. J. (2014). The
impact of state medical marijuana legislation on adolescent marijuana use. Journal
of Adolescent Health,55,160–166.
Cre´pault,J.-F. (2014).Cannabis Policy Framework.CAMH Research Document Series No.
40,October 2014.Toronto: Centre for Addiction and Mental Health.
Dills, A. K., Jacobson,M., & Miron, J. A. (2005).The effect of alcoholprohibition on
alcohol consumption: evidence from drunkenness arrests.Economics Letters,86,
279–284.
Dills, A. K.,& Miron, J. A. (2004).Alcohol prohibition and cirrhosis.American Law and
Economics Reviews,6(2),2185–2318.http://dx.doi.org/10.1093/aler/ahh003
Feeney, G. F. X., Connor, J. P., Young, R. M., Tucker, J., & McPherson, A. (2005). Cannabis
dependence and mental health perception amongst people diverted by police after
arrest for cannabis-related offending behaviour in Australia. Criminal Behaviour &
Mental Health,15,249–260.
Fischer,B., Imtiaz, S.,Rudzinski,K., & Rehm,J. ([36_TD$DIFF]2016).Crude estimates of cannabis-
attributable mortality and morbidity in Canada -implications for public health
focused intervention priorities. Journal of Public Health, [37_TD$DIFF]38(January (28)
http://dx.doi.org/10.1093/pubmed/fdv005
Guindon, G. E. (2014). The impact of tobacco prices on smoking onset: a methodologi-
cal review.Tobacco Control,23(2),e5.
Haden,M., & Emerson,B. (2014).A vision for cannabis regulation: a public health
approach based on lessons learned from the regulation of alcoholand tobacco.
Open Medicine,8(2),1–16.
Hall, W., & Degenhardt,L. (2007). Prevalence and correlates ofcannabis use in
developed and developing countries.Current Opinion in Psychiatry,20,393–397.
Hamilton, I., Lloyd, C., Monaghan,M. P., & Paton,K. (2014).The emerging cannabis
treatment population.Drugs and Alcohol Today,14.159-153.Retrieved at http://
eprints.whiterose.ac.uk/82720/17/Cannabis%20Treatment.pdf.
H. Kalant / International Journal of Drug Policy 34 (2016) 5–10 9
Hasin,D. S.,Saha,T. D., Kerridge,B. T., Goldstein,R. B.,Chou,S. P., Zhang,H., Jung,J.,
Pickering, R. P., Ruan, J., Smith, S. M., Huang, B., & Grant, B. F. (2015). Prevalence of
marijuana use disorders in the United States between 20012002 and 20122013
http://dx.doi.org/10.1001/jamapsychiatry.2015.1858 Retrieved from JAMA Psy-
chiatry published online,21 October 2015,pp. E1-E8..
Health Canada (2014).Canadian alcoholand drug use monitoring survey.Summary of
results for 2012.Retrieved 27 October 2015 from http://www.hc-sc.gc.ca/hc-ps/
drugs-drogues/stat/_2012/summary-sommaire-eng.php#tphp.
Her, M., Giesbrecht, N., Room, R., & Rehm, J. (1999). Privatizing alcohol sales and alcohol
consumption: evidence and implications.Addiction,94,1125–1139.
Hughes,C. E.,& Stevens,A. (2010).What can we learn from the Portuguese decrimi-
nalization of illicit drugs? British Journal of Criminology,50,999–1022.
Hughes,C. E., & Stevens,A. (2012).A resounding success or a disastrous failure: re-
examining the interpretation of evidence on the Portuguese decriminalization of
illicit drugs.Drug and Alcohol Review,31,101–113.
Hughes,J. R.,Fingar,J. R., Budney,A. J., Naud, S.,Helzer,J. E., & Callas,P. W. (2014).
Marijuana use and intoxication among daily users: an intensive longitudinal study.
Addictive Behaviors,39,1464–1470.
Ipsos Reid report: Justice Canada Contract#19040-140006/001/CY 2014 National
Justice Survey.Retrieved 1 November 2014 from http://epe.lac-bac.gc.ca/100/
200/301/pwgsc-tpsgc/por-ef/justice_canada/2014/060-13-e/Report
Kalant, H. (2014). Effects of cannabis and cannabinoids in the human nervous system.
In B. Madras & M.J. Kuhar (Eds.),The effects of drug abuse on the human nervous
system,revised and updated print edition (pp.387-422).Waltham,MA: Academic
Press (Elsevier).
Kalant, H., & Kalant, O. J. (1971). Drugs, society and personal choice, chapters 7 & 9. Don
Mills. Ontario: General Publishing Co.
Kalant, H., & Poikolainen,K. (1999). Moderate drinking:concepts,definitions,and
public health significance.In I. Macdonald (Ed.),Health issues related to alcohol
consumption (2nd ed,pp. 1–25). Brussels,Belgium: ILSI Europe.
Keyes, K. M., Schulenberg, J. E., O’Malley, P. M., Johnston, L. D., Bachman, J. G., Li, G., &
Hasin, D. (2011). The social norms of birth cohorts and adolescent marijuana use in
the United States,1976 2007.Addiction,106,1790–1800.
MacQueen,K. (2013).Why it’s time to legalize marijuana.Maclean’s,Toronto,10 June
2013.Retrieved on 9 November 2015 at http://www.macleans.ca/news/canada/
why-its-time-to-legalize-marijuana/.
Masten, S. V., & Guenzburger, G. V. (2014). Changes in driver cannabinoid prevalence in
12 U.S. states after implementing medicalmarijuana laws. Journal of Safety
Research,50,35–52.
Meier, M. H., Caspi, A., Ambler, A., Harrington, H., Houts, R., Keefe, R. S. E., McDonald, K.,
Ward, A., Poulton, R., & Moffitt, T. E. (2012). Persistentcannabis users show
neuropsychological decline from childhood to midlife. Proceedings of the National
Academy of Sciences of the United States of America,109,E2657–E2664.
Milne, B. J., Caspi,A., Harrington,H., Poulton, R., Rutter,M., & Moffitt, T. E. (2009).
Predictive value of family history on severity of illness: the case for depression,
anxiety, alcohol dependence, and drug dependence. Archives of General Psychiatry,
66,738–747.
Ontario Ministry of Finance: Ontario population by five-year age group and gender,
selected years.Retrieved on 2 November 2014 at http://www.fin.gov.on.ca/en/
economy/demographics/projections.
Osterberg,E. L. (2011).Alcohol tax changes and the use of alcohol in Europe.Drug &
Alcohol Review,30,124–129.
Pacula,R. L., Kilmer, B., Wagenaar,A. C., Chaloupka,F. J., & Caulkins, J. P. (2014).
Developing public health regulations for marijuana:lessons from alcoholand
tobacco.American Jounal of Public Health,104,1021–1028.
Palamar, J. J., Ompad, D. C., & Petkova, E. (2014). Correlates of intentions to use cannabis
among US high school seniors in the case of cannabis legalization.International
Journal of Drug Policy,25,424–435.
Parker,H., Williams, L., & Aldridge,J. (2002).The normalization of ‘‘sensible’’recrea-
tional drug use. Further evidence from the north west England longitudinal study.
Sociology,36,941–964.
Pauls, K., Plecas,D., Cohen, I. M., & Haarhoff, T. (2012). The nature and extentof
Marihuana possession in British Columbia.Retrieved on 22 October 2014 at
https://www.ufv.ca/media/assets/criminal-justice-research/The-Nature-and-Ex-
tent-of-Marijuana-Possession-in-BC.pdf.Abbotsford,BC: University of the Fraser
Valley.
Rehm, J., Gnam, W., Popova, S., Baliunas, D., Brochu, S., Fischer, B., Patra, J., Sarnocinska-
Hart, A., & Taylor, B. (2007).The costs of alcohol,illegal drugs,and tobacco in
Canada,2002.Journal of Studies on Alcohol & Drugs,68,886–895.
RMHIDTA (2015).The legalization of Marijuana in Colorado: the impact.Volume 3.
Preview 2015.Retrieved on 20 November 2015 at www.rmhidta.org/Reports.
RMHIDTA (2016). The Legalization of Marijuana in Colorado: The Impact - Latest Results
for Colorado.Youth and Adult Marijuana Use.Retrieved on 11 January 2016 at
www.rmhidta.org/Reports.
Room, R. (2014). Legalizing a market for cannabis for pleasure: Colorado, Washington,
Uruguay and beyond.Addiction,109,345–351.
Salomonsen-Sautel, S., Min, S.-J., Sakai, J. T., Thurstone, C., & Hopfer, C. (2014). Trends in
fatal motor vehicle crashes before and aftermarijuana commercialization in
Colorado.Drug and Alcohol Dependence,140,137–144.
Salvy, S.-J., Pedersen, E. R., Miles, J. N. V., Tucker, J. S., & D’Amico, E. J. (2014). Proximal
and distal social influence on alcoholconsumption and marijuana use among
middle school adolescents.Drug and Alcohol Dependence,144,93–101.
Shanahan, M., Gerard, K., & Ritter, A. (2014). Preferences for policy options for cannabis
in an Australian generalpopulation: a discrete choice experiment.International
Journal of Drug Policy,25,682–690.
Silins, E., Horwood, L. J., Patton, G. C., Fergusson, D. M.,Olsson, D. A., et al. (2014). Young
adult sequelae of adolescent cannabis use: an integrative analysis. Lancet Psychia-
try, 1, 286–293.
Single,E., Christie,P., & Ali, R. (2000).The impact of cannabis decriminalisation in
Australia and the United States.Journal of Public Health Policy,21,157–186.
Spithoff, S., Emerson, B., & Spithoff, A. (2015). Cannabis legalization: adhering to public
health best practice.CMAJ early release articles,(September)http://dx.doi.org/
10.1503/cmaj.150657
Statistics Canada (2014). Incident-based crime statistics by detailed violations. Annual
2009-2013.CANSIM Table 252-0051.Retrieved 2 November 2014 at http://
www.statcan.gc.ca/cansim/a26.
Stiglick,A., & Kalant, H. (1985).Residualeffects of chronic cannabis treatment on
behavior in mature rats.Psychopharmacology,85,436–439.
Thurstone, C., Lieberman, S. A., & Schmiege, S. A. (2011). Medical marijuana diversion
and associated problems in adolescent substance treatment.Drug and Alcohol
Dependence,118,489–492.
van der Pol,P., Liebregts,N., de Graaf,R., Korf,D. J., van den Brink,W., & van Laar,M.
(2012).Predicting the transition from frequent cannabis use to cannabis depen-
dence: a three-year prospective study. Drug and Alcohol Dependence, 133, 352–359.
Wakefield, M., & Chaloupka, F. (2000). Effectiveness of comprehensive tobacco control
programmes in reducing teenage smoking in the USA. Tobacco Control, 9, 177–186.
Wall, M., Poh, E., Cerda`, M., Keyes,K. M., Galea,S., & Hasin, D. (2011).Adolescent
marijuana use from 2002 to 2008: higher in states with medical marijuana laws,
cause still unclear.Annals of Epidemiology,21,714–716.
H. Kalant / International Journal of Drug Policy 34 (2016) 5–1010
Pickering, R. P., Ruan, J., Smith, S. M., Huang, B., & Grant, B. F. (2015). Prevalence of
marijuana use disorders in the United States between 20012002 and 20122013
http://dx.doi.org/10.1001/jamapsychiatry.2015.1858 Retrieved from JAMA Psy-
chiatry published online,21 October 2015,pp. E1-E8..
Health Canada (2014).Canadian alcoholand drug use monitoring survey.Summary of
results for 2012.Retrieved 27 October 2015 from http://www.hc-sc.gc.ca/hc-ps/
drugs-drogues/stat/_2012/summary-sommaire-eng.php#tphp.
Her, M., Giesbrecht, N., Room, R., & Rehm, J. (1999). Privatizing alcohol sales and alcohol
consumption: evidence and implications.Addiction,94,1125–1139.
Hughes,C. E.,& Stevens,A. (2010).What can we learn from the Portuguese decrimi-
nalization of illicit drugs? British Journal of Criminology,50,999–1022.
Hughes,C. E., & Stevens,A. (2012).A resounding success or a disastrous failure: re-
examining the interpretation of evidence on the Portuguese decriminalization of
illicit drugs.Drug and Alcohol Review,31,101–113.
Hughes,J. R.,Fingar,J. R., Budney,A. J., Naud, S.,Helzer,J. E., & Callas,P. W. (2014).
Marijuana use and intoxication among daily users: an intensive longitudinal study.
Addictive Behaviors,39,1464–1470.
Ipsos Reid report: Justice Canada Contract#19040-140006/001/CY 2014 National
Justice Survey.Retrieved 1 November 2014 from http://epe.lac-bac.gc.ca/100/
200/301/pwgsc-tpsgc/por-ef/justice_canada/2014/060-13-e/Report
Kalant, H. (2014). Effects of cannabis and cannabinoids in the human nervous system.
In B. Madras & M.J. Kuhar (Eds.),The effects of drug abuse on the human nervous
system,revised and updated print edition (pp.387-422).Waltham,MA: Academic
Press (Elsevier).
Kalant, H., & Kalant, O. J. (1971). Drugs, society and personal choice, chapters 7 & 9. Don
Mills. Ontario: General Publishing Co.
Kalant, H., & Poikolainen,K. (1999). Moderate drinking:concepts,definitions,and
public health significance.In I. Macdonald (Ed.),Health issues related to alcohol
consumption (2nd ed,pp. 1–25). Brussels,Belgium: ILSI Europe.
Keyes, K. M., Schulenberg, J. E., O’Malley, P. M., Johnston, L. D., Bachman, J. G., Li, G., &
Hasin, D. (2011). The social norms of birth cohorts and adolescent marijuana use in
the United States,1976 2007.Addiction,106,1790–1800.
MacQueen,K. (2013).Why it’s time to legalize marijuana.Maclean’s,Toronto,10 June
2013.Retrieved on 9 November 2015 at http://www.macleans.ca/news/canada/
why-its-time-to-legalize-marijuana/.
Masten, S. V., & Guenzburger, G. V. (2014). Changes in driver cannabinoid prevalence in
12 U.S. states after implementing medicalmarijuana laws. Journal of Safety
Research,50,35–52.
Meier, M. H., Caspi, A., Ambler, A., Harrington, H., Houts, R., Keefe, R. S. E., McDonald, K.,
Ward, A., Poulton, R., & Moffitt, T. E. (2012). Persistentcannabis users show
neuropsychological decline from childhood to midlife. Proceedings of the National
Academy of Sciences of the United States of America,109,E2657–E2664.
Milne, B. J., Caspi,A., Harrington,H., Poulton, R., Rutter,M., & Moffitt, T. E. (2009).
Predictive value of family history on severity of illness: the case for depression,
anxiety, alcohol dependence, and drug dependence. Archives of General Psychiatry,
66,738–747.
Ontario Ministry of Finance: Ontario population by five-year age group and gender,
selected years.Retrieved on 2 November 2014 at http://www.fin.gov.on.ca/en/
economy/demographics/projections.
Osterberg,E. L. (2011).Alcohol tax changes and the use of alcohol in Europe.Drug &
Alcohol Review,30,124–129.
Pacula,R. L., Kilmer, B., Wagenaar,A. C., Chaloupka,F. J., & Caulkins, J. P. (2014).
Developing public health regulations for marijuana:lessons from alcoholand
tobacco.American Jounal of Public Health,104,1021–1028.
Palamar, J. J., Ompad, D. C., & Petkova, E. (2014). Correlates of intentions to use cannabis
among US high school seniors in the case of cannabis legalization.International
Journal of Drug Policy,25,424–435.
Parker,H., Williams, L., & Aldridge,J. (2002).The normalization of ‘‘sensible’’recrea-
tional drug use. Further evidence from the north west England longitudinal study.
Sociology,36,941–964.
Pauls, K., Plecas,D., Cohen, I. M., & Haarhoff, T. (2012). The nature and extentof
Marihuana possession in British Columbia.Retrieved on 22 October 2014 at
https://www.ufv.ca/media/assets/criminal-justice-research/The-Nature-and-Ex-
tent-of-Marijuana-Possession-in-BC.pdf.Abbotsford,BC: University of the Fraser
Valley.
Rehm, J., Gnam, W., Popova, S., Baliunas, D., Brochu, S., Fischer, B., Patra, J., Sarnocinska-
Hart, A., & Taylor, B. (2007).The costs of alcohol,illegal drugs,and tobacco in
Canada,2002.Journal of Studies on Alcohol & Drugs,68,886–895.
RMHIDTA (2015).The legalization of Marijuana in Colorado: the impact.Volume 3.
Preview 2015.Retrieved on 20 November 2015 at www.rmhidta.org/Reports.
RMHIDTA (2016). The Legalization of Marijuana in Colorado: The Impact - Latest Results
for Colorado.Youth and Adult Marijuana Use.Retrieved on 11 January 2016 at
www.rmhidta.org/Reports.
Room, R. (2014). Legalizing a market for cannabis for pleasure: Colorado, Washington,
Uruguay and beyond.Addiction,109,345–351.
Salomonsen-Sautel, S., Min, S.-J., Sakai, J. T., Thurstone, C., & Hopfer, C. (2014). Trends in
fatal motor vehicle crashes before and aftermarijuana commercialization in
Colorado.Drug and Alcohol Dependence,140,137–144.
Salvy, S.-J., Pedersen, E. R., Miles, J. N. V., Tucker, J. S., & D’Amico, E. J. (2014). Proximal
and distal social influence on alcoholconsumption and marijuana use among
middle school adolescents.Drug and Alcohol Dependence,144,93–101.
Shanahan, M., Gerard, K., & Ritter, A. (2014). Preferences for policy options for cannabis
in an Australian generalpopulation: a discrete choice experiment.International
Journal of Drug Policy,25,682–690.
Silins, E., Horwood, L. J., Patton, G. C., Fergusson, D. M.,Olsson, D. A., et al. (2014). Young
adult sequelae of adolescent cannabis use: an integrative analysis. Lancet Psychia-
try, 1, 286–293.
Single,E., Christie,P., & Ali, R. (2000).The impact of cannabis decriminalisation in
Australia and the United States.Journal of Public Health Policy,21,157–186.
Spithoff, S., Emerson, B., & Spithoff, A. (2015). Cannabis legalization: adhering to public
health best practice.CMAJ early release articles,(September)http://dx.doi.org/
10.1503/cmaj.150657
Statistics Canada (2014). Incident-based crime statistics by detailed violations. Annual
2009-2013.CANSIM Table 252-0051.Retrieved 2 November 2014 at http://
www.statcan.gc.ca/cansim/a26.
Stiglick,A., & Kalant, H. (1985).Residualeffects of chronic cannabis treatment on
behavior in mature rats.Psychopharmacology,85,436–439.
Thurstone, C., Lieberman, S. A., & Schmiege, S. A. (2011). Medical marijuana diversion
and associated problems in adolescent substance treatment.Drug and Alcohol
Dependence,118,489–492.
van der Pol,P., Liebregts,N., de Graaf,R., Korf,D. J., van den Brink,W., & van Laar,M.
(2012).Predicting the transition from frequent cannabis use to cannabis depen-
dence: a three-year prospective study. Drug and Alcohol Dependence, 133, 352–359.
Wakefield, M., & Chaloupka, F. (2000). Effectiveness of comprehensive tobacco control
programmes in reducing teenage smoking in the USA. Tobacco Control, 9, 177–186.
Wall, M., Poh, E., Cerda`, M., Keyes,K. M., Galea,S., & Hasin, D. (2011).Adolescent
marijuana use from 2002 to 2008: higher in states with medical marijuana laws,
cause still unclear.Annals of Epidemiology,21,714–716.
H. Kalant / International Journal of Drug Policy 34 (2016) 5–1010
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 6