Mental Health Nursing Case Study: Rehabilitation and Recovery Project
VerifiedAdded on 2022/11/13
|15
|4002
|7
Case Study
AI Summary
This case study presents a detailed analysis of a 23-year-old Somali woman's experience with mental health issues, specifically post-traumatic stress disorder (PTSD), stemming from female genital mutilation (FGM), forced marriage, domestic violence and immigration. The paper outlines the nursing interventions undertaken, including the process of engagement and relationship building, identification of specific needs and strengths, and the application of rehabilitation and recovery principles. The study highlights the cultural factors that influenced the patient's condition and the barriers to effective engagement. The interventions recommended include physical exercises and trauma-focused counseling, with cognitive processing therapy as the specific trauma-focused treatment. The case underscores the importance of cultural sensitivity, therapeutic listening, and patient-centered care in mental health nursing, particularly when dealing with immigrant populations who have experienced trauma.

Running head: CASE STUDY 1
Case Study: Mental Health Nursing
Name
Institutional Affiliation
Case Study: Mental Health Nursing
Name
Institutional Affiliation
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CASE STUDY 2
Case Study: Mental Health Nursing
In this paper I focused on a mental health nursing in unique scenarios that I have
experienced in my clinical practice. In this case, I describe my encounter with an immigrant
woman who had undergone various cultural practices including gender based violence and
female genital mutilation (FGM). The purpose is to describe the rehabilitation and recovery
process of the woman with a focus on nursing roles and interventions I undertook. The
sections included in the study include a presentation of the case, the process of engagement
and relationship building, identification of specific needs/problems and strengths,
application of principles of rehabilitation and recovery, the interventions implemented on
the patient and the assessment tools/rating scales used.
A Case History
I was on morning shift when a 23-year-old Somali woman comes to the hospital
accompanied by an elderly woman. She complained of sleeplessness, and attention deficit.
The elderly woman who was identified as her friend stated that she had been having
inconsistent thoughts, was easily irritated, had lost interest in activities such as knitting,
which she was previously engaged in and she often seemed anxious. The young woman was
unwilling to share finer details regarding her condition, but insisted she had not been
sleeping adequately. The friend asserted that she had been spending much time alone and
was often scared by noises and motions.
I requested the friend to leave the room. Upon leaving, the woman explained that she
had been in Australia for the last 6 months. She left Somalia through a refugee program to
seek asylum in Australia. She has one child who she got from a forced marriage in her
teenage years. She also underwent female circumcision which was a traumatizing experience
at the age of 12 years, before being forcefully married off to an older man. She went on to
narrate that since the birth of her first child, she had been experiencing severe pain in her
Case Study: Mental Health Nursing
In this paper I focused on a mental health nursing in unique scenarios that I have
experienced in my clinical practice. In this case, I describe my encounter with an immigrant
woman who had undergone various cultural practices including gender based violence and
female genital mutilation (FGM). The purpose is to describe the rehabilitation and recovery
process of the woman with a focus on nursing roles and interventions I undertook. The
sections included in the study include a presentation of the case, the process of engagement
and relationship building, identification of specific needs/problems and strengths,
application of principles of rehabilitation and recovery, the interventions implemented on
the patient and the assessment tools/rating scales used.
A Case History
I was on morning shift when a 23-year-old Somali woman comes to the hospital
accompanied by an elderly woman. She complained of sleeplessness, and attention deficit.
The elderly woman who was identified as her friend stated that she had been having
inconsistent thoughts, was easily irritated, had lost interest in activities such as knitting,
which she was previously engaged in and she often seemed anxious. The young woman was
unwilling to share finer details regarding her condition, but insisted she had not been
sleeping adequately. The friend asserted that she had been spending much time alone and
was often scared by noises and motions.
I requested the friend to leave the room. Upon leaving, the woman explained that she
had been in Australia for the last 6 months. She left Somalia through a refugee program to
seek asylum in Australia. She has one child who she got from a forced marriage in her
teenage years. She also underwent female circumcision which was a traumatizing experience
at the age of 12 years, before being forcefully married off to an older man. She went on to
narrate that since the birth of her first child, she had been experiencing severe pain in her
CASE STUDY 3
genitalia, which was a major challenge in her marriage. She suffered domestic violence and
severe beating from her husband. The memories of the horrific FGM experience and severe
violence inflicted on her kept haunting her. She could not share the experiences with fellow
Somali women due to influences of stigma, cultural viewpoints and fear of victimization.
Following her case history, she is diagnosed with posttraumatic stress disorder (PTSD).
The Process of Engagement and Relationship Building
In my interaction with the patient, I observed that the effectiveness of healthcare
engagements and relationships was influenced by the cultural, environmental and individual
factors of the patient. Cultural factors were a major barrier to effective engagement and
relationship building among victims of FGM. The woman still perceived FGM to be a
justifiable and appropriate procedure due to her cultural orientation. Klein, Helzner,
Shayowitz, Kohlhoff, and Smith-Norowitz (2018) explained that female circumcision
involves the manipulation or alteration of external genitalia for women and girls. In
developing countries, it is often regarded as a societal norm is a requirement for families to
be accepted in the community. In the cultural perspective, FGM is upheld due to the
perceptions that it is preserves fertility, improves chastity among girls, and enhances sexual
pleasure for men and promoted hygiene. Failure to undergo FGM is regarded as bringing
shame to the family (Klein et al., 2018).
I also realised that the woman had suffered stigma from the community regarding
reporting of FGM incidences was another barrier to effective interactions. Knipscheer et al.
(2015) explained that circumcised immigrant women are at risk of emotional instability,
PTSD, depression and anxiety. Specifically, the victims of FGM in the Somali community
often fear reporting the incidences due to different cultural perceptions and taboos that make
them ashamed to discuss their problems and feel a sense of stigma. Further, they my fear
genitalia, which was a major challenge in her marriage. She suffered domestic violence and
severe beating from her husband. The memories of the horrific FGM experience and severe
violence inflicted on her kept haunting her. She could not share the experiences with fellow
Somali women due to influences of stigma, cultural viewpoints and fear of victimization.
Following her case history, she is diagnosed with posttraumatic stress disorder (PTSD).
The Process of Engagement and Relationship Building
In my interaction with the patient, I observed that the effectiveness of healthcare
engagements and relationships was influenced by the cultural, environmental and individual
factors of the patient. Cultural factors were a major barrier to effective engagement and
relationship building among victims of FGM. The woman still perceived FGM to be a
justifiable and appropriate procedure due to her cultural orientation. Klein, Helzner,
Shayowitz, Kohlhoff, and Smith-Norowitz (2018) explained that female circumcision
involves the manipulation or alteration of external genitalia for women and girls. In
developing countries, it is often regarded as a societal norm is a requirement for families to
be accepted in the community. In the cultural perspective, FGM is upheld due to the
perceptions that it is preserves fertility, improves chastity among girls, and enhances sexual
pleasure for men and promoted hygiene. Failure to undergo FGM is regarded as bringing
shame to the family (Klein et al., 2018).
I also realised that the woman had suffered stigma from the community regarding
reporting of FGM incidences was another barrier to effective interactions. Knipscheer et al.
(2015) explained that circumcised immigrant women are at risk of emotional instability,
PTSD, depression and anxiety. Specifically, the victims of FGM in the Somali community
often fear reporting the incidences due to different cultural perceptions and taboos that make
them ashamed to discuss their problems and feel a sense of stigma. Further, they my fear
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
CASE STUDY 4
sharing their stories as it may be a reminder of the pain and trauma they experienced during
the mutilation (Knipscheer et al., 2015).
Societal factors also played a critical role in determining the nature of clinical
interactions. Speaking openly about trauma is an essential part of healing and recovery.
However, it is only applicable in a culture that recognizes the trauma and the psychological
consequences it causes on the individuals (Knipscheer et al., 2015). Unfortunately, in the
Somali community where the woman comes from, it is difficult to discuss the traumatic
consequences of FGM within their culture as most of the fellow women view the event less
negatively as compared to women from other cultures. Further, most Somali women are
Muslims who regard FGM as a cultural right referring to the Islamic teachers which regard
sunna (female circumcision) as acceptable).
Additionally, I realised the financial challenges of the woman that prevented her
from seeking health services. According to Suphanchaimat, Kantamaturapoj, Putthasri, and
Prakongsai (2015), there are various challenges that influence the attitudes, practices and
perceptions of healthcare providers in the delivery of healthcare services to immigrants.
Some essential factors include inadequate institutional capacity as a result of resource of
time constraints, fear resulting for perceived racism, and their legal status. Therefore, it is
essential for healthcare practitioners to ignore discussions regarding the legal status of
immigrants to enhance professionalism and functionality of the clinical practice.
Due to the cultural orientation of the patient, it was challenging to establish
therapeutic interactions. The patient approached the interactions cautiously in fear of ridicule
by fellow women. Additional, the woman did not perceive FGM as a cause of psychological
problems as she still regarded it highly due to the cultural orientation.
Identification of Specific Needs/Problems and Strengths
sharing their stories as it may be a reminder of the pain and trauma they experienced during
the mutilation (Knipscheer et al., 2015).
Societal factors also played a critical role in determining the nature of clinical
interactions. Speaking openly about trauma is an essential part of healing and recovery.
However, it is only applicable in a culture that recognizes the trauma and the psychological
consequences it causes on the individuals (Knipscheer et al., 2015). Unfortunately, in the
Somali community where the woman comes from, it is difficult to discuss the traumatic
consequences of FGM within their culture as most of the fellow women view the event less
negatively as compared to women from other cultures. Further, most Somali women are
Muslims who regard FGM as a cultural right referring to the Islamic teachers which regard
sunna (female circumcision) as acceptable).
Additionally, I realised the financial challenges of the woman that prevented her
from seeking health services. According to Suphanchaimat, Kantamaturapoj, Putthasri, and
Prakongsai (2015), there are various challenges that influence the attitudes, practices and
perceptions of healthcare providers in the delivery of healthcare services to immigrants.
Some essential factors include inadequate institutional capacity as a result of resource of
time constraints, fear resulting for perceived racism, and their legal status. Therefore, it is
essential for healthcare practitioners to ignore discussions regarding the legal status of
immigrants to enhance professionalism and functionality of the clinical practice.
Due to the cultural orientation of the patient, it was challenging to establish
therapeutic interactions. The patient approached the interactions cautiously in fear of ridicule
by fellow women. Additional, the woman did not perceive FGM as a cause of psychological
problems as she still regarded it highly due to the cultural orientation.
Identification of Specific Needs/Problems and Strengths
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CASE STUDY 5
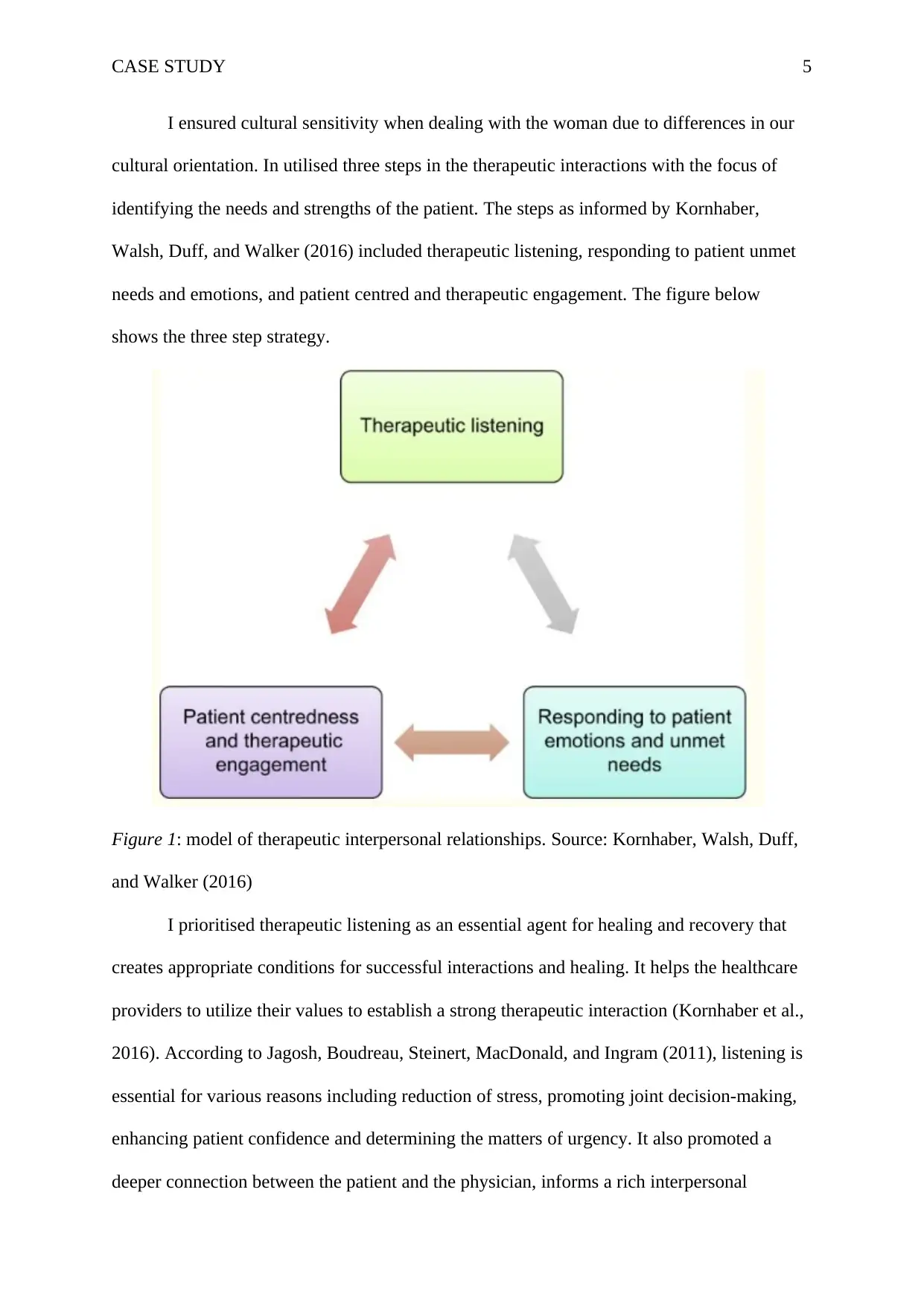
I ensured cultural sensitivity when dealing with the woman due to differences in our
cultural orientation. In utilised three steps in the therapeutic interactions with the focus of
identifying the needs and strengths of the patient. The steps as informed by Kornhaber,
Walsh, Duff, and Walker (2016) included therapeutic listening, responding to patient unmet
needs and emotions, and patient centred and therapeutic engagement. The figure below
shows the three step strategy.
Figure 1: model of therapeutic interpersonal relationships. Source: Kornhaber, Walsh, Duff,
and Walker (2016)
I prioritised therapeutic listening as an essential agent for healing and recovery that
creates appropriate conditions for successful interactions and healing. It helps the healthcare
providers to utilize their values to establish a strong therapeutic interaction (Kornhaber et al.,
2016). According to Jagosh, Boudreau, Steinert, MacDonald, and Ingram (2011), listening is
essential for various reasons including reduction of stress, promoting joint decision-making,
enhancing patient confidence and determining the matters of urgency. It also promoted a
deeper connection between the patient and the physician, informs a rich interpersonal
I ensured cultural sensitivity when dealing with the woman due to differences in our
cultural orientation. In utilised three steps in the therapeutic interactions with the focus of
identifying the needs and strengths of the patient. The steps as informed by Kornhaber,
Walsh, Duff, and Walker (2016) included therapeutic listening, responding to patient unmet
needs and emotions, and patient centred and therapeutic engagement. The figure below
shows the three step strategy.
Figure 1: model of therapeutic interpersonal relationships. Source: Kornhaber, Walsh, Duff,
and Walker (2016)
I prioritised therapeutic listening as an essential agent for healing and recovery that
creates appropriate conditions for successful interactions and healing. It helps the healthcare
providers to utilize their values to establish a strong therapeutic interaction (Kornhaber et al.,
2016). According to Jagosh, Boudreau, Steinert, MacDonald, and Ingram (2011), listening is
essential for various reasons including reduction of stress, promoting joint decision-making,
enhancing patient confidence and determining the matters of urgency. It also promoted a
deeper connection between the patient and the physician, informs a rich interpersonal
CASE STUDY 6
dialogue and promoted awareness of self-bias and preconceptions, particularly in situations
that are emotionally charged.
I also focused on responding to patients unmet needs and emotions as essential part
of a therapeutic interaction in mental health. It involves the nurses’ responses to various
verbal expressions provided by the patient. The nurses should be empathetic of the patients’
expressions and negative emotions by fostering good patient-nurse communication
(Kornhaber et al., 2016). Adams, Cimino, Arnold, and Anderson (2012) explained that
neutral responses from healthcare professionals contributed to the willingness of a patient to
disclose information regarding social issues, goals of care and concerns. Disclosure is
critical in guiding further communication and determining the treatment plans. Sympathetic
and empathetic responses from nurses contribute an agreement regarding treatment plans,
toward and neutral responses help to build rapport with the patient
Finally, I practiced therapeutic engagement and patient centeredness asessential
aspects in the relationship between patients and their healthcare providers. The engagements
ensure uphold respect for individuality and uniqueness (Kornhaber et al., 2016). Cultural
competence is essential at this step of nurse-patient interactions in this case. Healthcare
professionals in countries that receive immigrants need to develop services and interventions
that cater for women or girls who have undergone FGM in a manner that is culturally
sensitive. They should also be tactful in addressing legal, socioeconomic, cultural and
language barriers that may affect immigrants in their search for healthcare (Degni,
Suominen, Essén, El Ansari, & Vehviläinen-Julkunen, 2012; Evans et al., 2017).
Application of Principles of Rehabilitation and Recovery
The consumer in this case had PTSD associated with trauma as a result of
immigration experiences, the consequences of FGM, early marriage, and intimate partner
violence. Therefore, I needed a unique rehabilitation and recovery process. Victims may
dialogue and promoted awareness of self-bias and preconceptions, particularly in situations
that are emotionally charged.
I also focused on responding to patients unmet needs and emotions as essential part
of a therapeutic interaction in mental health. It involves the nurses’ responses to various
verbal expressions provided by the patient. The nurses should be empathetic of the patients’
expressions and negative emotions by fostering good patient-nurse communication
(Kornhaber et al., 2016). Adams, Cimino, Arnold, and Anderson (2012) explained that
neutral responses from healthcare professionals contributed to the willingness of a patient to
disclose information regarding social issues, goals of care and concerns. Disclosure is
critical in guiding further communication and determining the treatment plans. Sympathetic
and empathetic responses from nurses contribute an agreement regarding treatment plans,
toward and neutral responses help to build rapport with the patient
Finally, I practiced therapeutic engagement and patient centeredness asessential
aspects in the relationship between patients and their healthcare providers. The engagements
ensure uphold respect for individuality and uniqueness (Kornhaber et al., 2016). Cultural
competence is essential at this step of nurse-patient interactions in this case. Healthcare
professionals in countries that receive immigrants need to develop services and interventions
that cater for women or girls who have undergone FGM in a manner that is culturally
sensitive. They should also be tactful in addressing legal, socioeconomic, cultural and
language barriers that may affect immigrants in their search for healthcare (Degni,
Suominen, Essén, El Ansari, & Vehviläinen-Julkunen, 2012; Evans et al., 2017).
Application of Principles of Rehabilitation and Recovery
The consumer in this case had PTSD associated with trauma as a result of
immigration experiences, the consequences of FGM, early marriage, and intimate partner
violence. Therefore, I needed a unique rehabilitation and recovery process. Victims may
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
CASE STUDY 7
result in avoidance in the efforts to stress and distress symptoms that may result from FGM
or to relieve themselves from the negative and intense emotions that may result from FGM
(Knipscheer et al., 2015). According to Drake and Whitley (2014), successful recovery
interventions in mental health contexts should focus on empowering people to make
informed decisions regarding their treatments and life goals. The patients should also be
encouraged to practice self-management of their lives and disorders. Additionally, the
interventions need to focus on residential, financial and personal independence. Knipscheer
et al. (2015) explained that interventions associated with the clinical treatment of immigrant
women who have undergone circumcision should focus on equipping them with coping
mechanisms that enable them to deal with their experiences. Additionally, they should be
aware of the various types of FGM and the related symptoms. Also the interventions need to
be applicable to the patient’s context with an awareness of the potential that women may be
hesitant to seek psychological help (Knipscheer et al., 2015).
The Interventions
To address the current case, I recommended two interventions. The first intervention
was physical exercises. Various researchers have upheld physical exercise as an essential
intervention for treating PTSD and other psychological disorders such as depression and
anxiety among a wide range of populations (Asmundson, Fetzner, DeBoer, Powers, Otto, &
Smits, 2013; Hegberg, Hayes, & Hayes, 2019; Herring, Jacob, Suveg, Dishman, &
O’Connor, 2012; Suphanchaimat, Kantamaturapoj, Putthasri, & Prakongsai, 2015; Schuch et
al., 2016). Budde, Akko, Ainamani, Murillo-Rodríguez, and Weierstall (2018) confirmed
that exercise training is a simple intervention that can be implemented in a cost-effective and
low-threshold manner that is implementable in a resource-poor setting. The aerobic and
exercise programs are cheap and can be done with no cost at all. Oppizzi and Umberger
result in avoidance in the efforts to stress and distress symptoms that may result from FGM
or to relieve themselves from the negative and intense emotions that may result from FGM
(Knipscheer et al., 2015). According to Drake and Whitley (2014), successful recovery
interventions in mental health contexts should focus on empowering people to make
informed decisions regarding their treatments and life goals. The patients should also be
encouraged to practice self-management of their lives and disorders. Additionally, the
interventions need to focus on residential, financial and personal independence. Knipscheer
et al. (2015) explained that interventions associated with the clinical treatment of immigrant
women who have undergone circumcision should focus on equipping them with coping
mechanisms that enable them to deal with their experiences. Additionally, they should be
aware of the various types of FGM and the related symptoms. Also the interventions need to
be applicable to the patient’s context with an awareness of the potential that women may be
hesitant to seek psychological help (Knipscheer et al., 2015).
The Interventions
To address the current case, I recommended two interventions. The first intervention
was physical exercises. Various researchers have upheld physical exercise as an essential
intervention for treating PTSD and other psychological disorders such as depression and
anxiety among a wide range of populations (Asmundson, Fetzner, DeBoer, Powers, Otto, &
Smits, 2013; Hegberg, Hayes, & Hayes, 2019; Herring, Jacob, Suveg, Dishman, &
O’Connor, 2012; Suphanchaimat, Kantamaturapoj, Putthasri, & Prakongsai, 2015; Schuch et
al., 2016). Budde, Akko, Ainamani, Murillo-Rodríguez, and Weierstall (2018) confirmed
that exercise training is a simple intervention that can be implemented in a cost-effective and
low-threshold manner that is implementable in a resource-poor setting. The aerobic and
exercise programs are cheap and can be done with no cost at all. Oppizzi and Umberger
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CASE STUDY 8
(2018) added that physical activity is an effective strategy for reducing the severely of PTSD
symptoms. Therefore, there are appropriate for the woman in her current situation.
The second intervention was trauma-focused counselling. Trauma-focused
interventions are effective for addressing memories of traumatic events of the feelings and
thoughts that result from a traumatic event. (Watkins, Sprang, & Rothbaum, 2018).
According to van Vliet, Huntjens, van Dijk, and de Jongh (2018), there is a link between
PTSD and physical or sexual abuse during childhood. The experience of traumatisation may
result in the development of symptoms such as negative self-concept, interpersonal
problems and regulation which s associated with complex PTSD. van Vliet et l. (2018) cited
that a trauma-focused treatment should be preceded by a stabilization phase to minimize the
rate of drop-out from the program. On the other hand, the stabilization phase is often
criticised by arguments that it may restrict and delay access to the trauma-focused
treatments; hence hindering the immediate positive impact of the treatment son he target
patients (De Jongh et al., 2016). In this case, stabilization may be ignored due to lack of
adequate evidence to assert its importance.
Cognitive processing therapy was an appropriate trauma-focused treatment in the
treatment of the woman in this case study. The intervention is upheld by the American
Psychological Association (APA) and the Veterans Health Administration and Department
of Defense (VA/DoD) for the treatment of PTSD. Cognitive processing therapy is founded
in the informed emotional processing theory and the social cognitive theory. The
intervention is based on the argument that individuals who have undergone traumatic events
often tray to make sense out of their previous experiences and events. Consequently, there
persons develop a distorted perception of themselves, other people, and the world.
Therefore, the role of cognitive processing therapy is to alter the distorted beliefs to adapt to
new learning and conform to previous beliefs. The cognitive processing therapy may be
(2018) added that physical activity is an effective strategy for reducing the severely of PTSD
symptoms. Therefore, there are appropriate for the woman in her current situation.
The second intervention was trauma-focused counselling. Trauma-focused
interventions are effective for addressing memories of traumatic events of the feelings and
thoughts that result from a traumatic event. (Watkins, Sprang, & Rothbaum, 2018).
According to van Vliet, Huntjens, van Dijk, and de Jongh (2018), there is a link between
PTSD and physical or sexual abuse during childhood. The experience of traumatisation may
result in the development of symptoms such as negative self-concept, interpersonal
problems and regulation which s associated with complex PTSD. van Vliet et l. (2018) cited
that a trauma-focused treatment should be preceded by a stabilization phase to minimize the
rate of drop-out from the program. On the other hand, the stabilization phase is often
criticised by arguments that it may restrict and delay access to the trauma-focused
treatments; hence hindering the immediate positive impact of the treatment son he target
patients (De Jongh et al., 2016). In this case, stabilization may be ignored due to lack of
adequate evidence to assert its importance.
Cognitive processing therapy was an appropriate trauma-focused treatment in the
treatment of the woman in this case study. The intervention is upheld by the American
Psychological Association (APA) and the Veterans Health Administration and Department
of Defense (VA/DoD) for the treatment of PTSD. Cognitive processing therapy is founded
in the informed emotional processing theory and the social cognitive theory. The
intervention is based on the argument that individuals who have undergone traumatic events
often tray to make sense out of their previous experiences and events. Consequently, there
persons develop a distorted perception of themselves, other people, and the world.
Therefore, the role of cognitive processing therapy is to alter the distorted beliefs to adapt to
new learning and conform to previous beliefs. The cognitive processing therapy may be
CASE STUDY 9
achieved using 12 weekly sessions that are attended individually that are focused on psycho
education and counselling (Watkins, Sprang, & Rothbaum, 2018).
Assessment Tools/Rating Scales Used
I utilised the Primary Care-Posttraumatic Stress Disorder (PC-PTSD) tool and
nurses’ critical intuition as essential tools for assessing improvement and the severity of
PTSD symptoms in the case study. Nurses play a critical role in utilizing critical thinking to
assess the psychological issues reported by patients. Consequently, the nurses are able to
inform and advocate for appropriate patient treatments. Additionally, the use of a
standardised tool such as PC-PTSD is important in heightening the awareness of nurses
while assessing the patients’ psychological issues (Frank, Schroeter, & Shaw, 2017).
Based on the PC-PTSD tool, a score of less than 3 was an indicator of poor
intervention outcomes, while a score above 3 indicated that the intervention goals have been
achieved. The PC-PTSD assessment was conducted at intervals of 2 weeks to assess the
effectiveness of treatment interventions. The nurses’ critical assessments by nurses involved
clinical appointments that occurred after two weeks. The communication, behaviour and
expression of the patient were essential in informing the nurse of any possible recovery
progress resulting from the interventions. The key resource personnel that were necessary in
the realization of the interventions and assessment included a mental health nurse, a physical
therapist, the patient and close friends who provide an appropriate support system for
recovery and rehabilitation. The physical therapist was involved in actively guiding the
patient through a schedule of simple aerobics and physical exercises that can aid her
recovery.
Final Outcomes in Terms of the Individual’s Responses
After going through the intervention, the woman demonstrated better coping
strategies and self-awareness. The expected outcomes of the interventions included an
achieved using 12 weekly sessions that are attended individually that are focused on psycho
education and counselling (Watkins, Sprang, & Rothbaum, 2018).
Assessment Tools/Rating Scales Used
I utilised the Primary Care-Posttraumatic Stress Disorder (PC-PTSD) tool and
nurses’ critical intuition as essential tools for assessing improvement and the severity of
PTSD symptoms in the case study. Nurses play a critical role in utilizing critical thinking to
assess the psychological issues reported by patients. Consequently, the nurses are able to
inform and advocate for appropriate patient treatments. Additionally, the use of a
standardised tool such as PC-PTSD is important in heightening the awareness of nurses
while assessing the patients’ psychological issues (Frank, Schroeter, & Shaw, 2017).
Based on the PC-PTSD tool, a score of less than 3 was an indicator of poor
intervention outcomes, while a score above 3 indicated that the intervention goals have been
achieved. The PC-PTSD assessment was conducted at intervals of 2 weeks to assess the
effectiveness of treatment interventions. The nurses’ critical assessments by nurses involved
clinical appointments that occurred after two weeks. The communication, behaviour and
expression of the patient were essential in informing the nurse of any possible recovery
progress resulting from the interventions. The key resource personnel that were necessary in
the realization of the interventions and assessment included a mental health nurse, a physical
therapist, the patient and close friends who provide an appropriate support system for
recovery and rehabilitation. The physical therapist was involved in actively guiding the
patient through a schedule of simple aerobics and physical exercises that can aid her
recovery.
Final Outcomes in Terms of the Individual’s Responses
After going through the intervention, the woman demonstrated better coping
strategies and self-awareness. The expected outcomes of the interventions included an
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
CASE STUDY 10
increased capacity of the individual to interact with their environment and utilize available
resources. They demonstrated positive personal attributes including adopting positive self-
concepts and having a bright facial appearance. Additionally, the individual had managed to
develop strong bonds with at least one family member of community member, and to solicit
support from the community, develop social attachments, get involved in community
activities, achieve normalization of their daily life, demonstrate hardiness and develop
coping strategies (Ajdukovic et al., 2013).
Conclusion and Recommendations
From the case study, it is evident that immigrant’s from developing countries have
unique healthcare needs. Some of the needs may be difficult to due to culture shock and
cultural differences. Coping in such situations within the healthcare system requires culture
competence of the healthcare provider. The nurses and other professionals should be aware
on how to hance unique situations such as women and girls who live in trauma as a result if
FGM, domestic violence or early marriage, as demonstrated in the case. Physical exercises
and therapeutic counselling are effective interventions for addressing PTSD. At the end of
the intervention, the woman demonstrated better self-esteem, increased involvement in
community activities, better stress coping mechanism, and willingness to report any mental
health problems. Additionally, the woman was aware of how to manage past traumatizing
memories and feelings. Therefore, it is essential that nurses equip themselves with adequate
knowledge regarding cultural competence, and various cultural beliefs, values and
viewpoints, taboos and norms from different parts of the world, and particularly asylums and
refugees.
increased capacity of the individual to interact with their environment and utilize available
resources. They demonstrated positive personal attributes including adopting positive self-
concepts and having a bright facial appearance. Additionally, the individual had managed to
develop strong bonds with at least one family member of community member, and to solicit
support from the community, develop social attachments, get involved in community
activities, achieve normalization of their daily life, demonstrate hardiness and develop
coping strategies (Ajdukovic et al., 2013).
Conclusion and Recommendations
From the case study, it is evident that immigrant’s from developing countries have
unique healthcare needs. Some of the needs may be difficult to due to culture shock and
cultural differences. Coping in such situations within the healthcare system requires culture
competence of the healthcare provider. The nurses and other professionals should be aware
on how to hance unique situations such as women and girls who live in trauma as a result if
FGM, domestic violence or early marriage, as demonstrated in the case. Physical exercises
and therapeutic counselling are effective interventions for addressing PTSD. At the end of
the intervention, the woman demonstrated better self-esteem, increased involvement in
community activities, better stress coping mechanism, and willingness to report any mental
health problems. Additionally, the woman was aware of how to manage past traumatizing
memories and feelings. Therefore, it is essential that nurses equip themselves with adequate
knowledge regarding cultural competence, and various cultural beliefs, values and
viewpoints, taboos and norms from different parts of the world, and particularly asylums and
refugees.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

CASE STUDY 11
CASE STUDY 12
References
Adams, K., Cimino, J. E., Arnold, R. M., & Anderson, W. G. (2012). Why should I talk
about emotion? Communication patterns associated with physician discussion of
patient expressions of negative emotion in hospital admission encounters. Patient
education and counseling, 89(1), 44–50. doi:10.1016/j.pec.2012.04.005
Ajdukovic, D., Ajdukovic, D., Bogic, M., Franciskovic, T., Galeazzi, G. M., Kucukalic,
A., ... & Priebe, S. (2013). Recovery from posttraumatic stress symptoms: A
qualitative study of attributions in survivors of war. PloS one, 8(8).
doi:10.1371/journal.pone.0070579
Asmundson, G. J., Fetzner, M. G., DeBoer, L. B., Powers, M. B., Otto, M. W., & Smits, J.
A. (2013). Let's get physical: a contemporary review of the anxiolytic effects of
exercise for anxiety and its disorders. Depression and anxiety, 30(4), 362-373.
Budde, H., Akko, D. P., Ainamani, H. E., Murillo-Rodríguez, E., & Weierstall, R. (2018).
The impact of an exercise training intervention on cortisol levels and post-
traumatic stress disorder in juveniles from an Ugandan refugee settlement: study
protocol for a randomized control trial. Trials, 19(1), 364. doi:10.1186/s13063-
018-2753-x
De Jongh, A., Resick, P. A., Zoellner, L. A., Van Minnen, A., Lee, C. W., Monson, C. M.,
... & Rauch, S. A. (2016). Critical analysis of the current treatment guidelines for
complex PTSD in adults. Depression and Anxiety, 33(5), 359-369.
Degni, F., Suominen, S., Essén, B., El Ansari, W., & Vehviläinen-Julkunen, K. (2012).
Communication and cultural issues in providing reproductive health care to
immigrant women: health care providers’ experiences in meeting Somali women
living in Finland. Journal of immigrant and minority health, 14(2), 330-343.
References
Adams, K., Cimino, J. E., Arnold, R. M., & Anderson, W. G. (2012). Why should I talk
about emotion? Communication patterns associated with physician discussion of
patient expressions of negative emotion in hospital admission encounters. Patient
education and counseling, 89(1), 44–50. doi:10.1016/j.pec.2012.04.005
Ajdukovic, D., Ajdukovic, D., Bogic, M., Franciskovic, T., Galeazzi, G. M., Kucukalic,
A., ... & Priebe, S. (2013). Recovery from posttraumatic stress symptoms: A
qualitative study of attributions in survivors of war. PloS one, 8(8).
doi:10.1371/journal.pone.0070579
Asmundson, G. J., Fetzner, M. G., DeBoer, L. B., Powers, M. B., Otto, M. W., & Smits, J.
A. (2013). Let's get physical: a contemporary review of the anxiolytic effects of
exercise for anxiety and its disorders. Depression and anxiety, 30(4), 362-373.
Budde, H., Akko, D. P., Ainamani, H. E., Murillo-Rodríguez, E., & Weierstall, R. (2018).
The impact of an exercise training intervention on cortisol levels and post-
traumatic stress disorder in juveniles from an Ugandan refugee settlement: study
protocol for a randomized control trial. Trials, 19(1), 364. doi:10.1186/s13063-
018-2753-x
De Jongh, A., Resick, P. A., Zoellner, L. A., Van Minnen, A., Lee, C. W., Monson, C. M.,
... & Rauch, S. A. (2016). Critical analysis of the current treatment guidelines for
complex PTSD in adults. Depression and Anxiety, 33(5), 359-369.
Degni, F., Suominen, S., Essén, B., El Ansari, W., & Vehviläinen-Julkunen, K. (2012).
Communication and cultural issues in providing reproductive health care to
immigrant women: health care providers’ experiences in meeting Somali women
living in Finland. Journal of immigrant and minority health, 14(2), 330-343.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.