Analysis of Congestive Heart Failure: A Comprehensive Case Study
VerifiedAdded on 2021/04/16
|11
|2475
|41
Case Study
AI Summary
This case study delves into the complexities of Congestive Heart Failure (CHF) through the analysis of Mrs. McKenzie's condition. It meticulously outlines the significant risk factors associated with CHF, encompassing older age, hypertension, high cholesterol, diabetes, and lifestyle choices like smoking, lack of exercise, and alcohol consumption. The study further examines the pathophysiology of CHF, explaining symptoms such as dyspnea, swollen ankles, dizziness, tachycardia, and appetite loss. It provides detailed insights into the mechanisms behind these symptoms, linking them to reduced cardiac output and fluid accumulation. The assignment also covers therapeutic interventions, highlighting the use of ACE inhibitors and beta-blockers, explaining their mechanisms and benefits in managing CHF. Finally, it outlines crucial cardiovascular and respiratory nursing interventions, emphasizing the importance of monitoring vital signs, assessing respiratory patterns, and providing patient education for effective CHF management, referencing relevant medical literature.
Case Study
1
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Q.1.
Most important risk factors of congestive heart failure include older age, high levels of
cholesterol, diabetes mellitus, high blood pressure and active smoking. Other risk factors
include lack of physical activity, family history, obesity and alcohol consumption.
Hypertensive female are four times more prone to congestive heart failure as compared to the
non-hypertensive female. Hypertension is responsible for the occurrence of congestive heart
failure in approximately 60 % female and 40 % male. However, it is evident that
hypertension is more evident in males as compared to females in all age groups. High levels
of low-density lipoproteins and low levels of high density lipoproteins are also responsible
for the occurrence of congestive heart failure. It is evident that smoking is responsible for
approximately 36 % cases and obesity is responsible for the approximately 20 % cases of the
congestive heart failure. Consumption of high amount of saturated fat is also responsible for
the occurrence of congestive heart failure. Increased levels of B-type natriuretic peptides are
also responsible for the occurrence of congestive heart failure (Mahmood and Wang, 2013).
Other cardiovascular conditions like coronary artery disease and heart attack, faulty heart
valves, cardiomyopathy, myocarditis, congenital heart defects and heart arrhythmias are the
cause of congestive heart failure. Other cardiovascular risk factors responsible for the
occurrence of congestive heart failure include coronary artery disease, heart attack,
congenital heart defects, irregular heartbeats and valvular heart disease. Sleep apnoea and
viral infection are also responsible for congestive heart failure. Consumption of medications
like antidiabetic medications (rosiglitazone and pioglitazone), nonsteroidal anti-inflammatory
drugs (NSAIDs), certain anaesthetics, anti-arrhythmic medications, antihypertensive and
anticancer are responsible for the occurrence of congestive heart failure. Approximately 2 %
and 5 % of persons in the age group 40 to 59 years and 60 to 69 years experiences congestive
heart failure respectively. Approximately 50 % of the patients diagnosed with congestive
heart failure die within five years after diagnosis. Approximately 6 to 9 times more sudden
death can occur in congestive heart failure patients as compared to the normal patients.
Family members of Mrs McKenzie should take responsibility to avoid exposure of risk
factors to her. Family members should monitor eating and medication consumption in her.
Family members should maintain positive communication with her because it is evident that
it can be helpful in maintaining adoption and maintenance of health behaviours. Family
members should focus on care of Mrs McKenzie rather than worrying about her diseased
2
Most important risk factors of congestive heart failure include older age, high levels of
cholesterol, diabetes mellitus, high blood pressure and active smoking. Other risk factors
include lack of physical activity, family history, obesity and alcohol consumption.
Hypertensive female are four times more prone to congestive heart failure as compared to the
non-hypertensive female. Hypertension is responsible for the occurrence of congestive heart
failure in approximately 60 % female and 40 % male. However, it is evident that
hypertension is more evident in males as compared to females in all age groups. High levels
of low-density lipoproteins and low levels of high density lipoproteins are also responsible
for the occurrence of congestive heart failure. It is evident that smoking is responsible for
approximately 36 % cases and obesity is responsible for the approximately 20 % cases of the
congestive heart failure. Consumption of high amount of saturated fat is also responsible for
the occurrence of congestive heart failure. Increased levels of B-type natriuretic peptides are
also responsible for the occurrence of congestive heart failure (Mahmood and Wang, 2013).
Other cardiovascular conditions like coronary artery disease and heart attack, faulty heart
valves, cardiomyopathy, myocarditis, congenital heart defects and heart arrhythmias are the
cause of congestive heart failure. Other cardiovascular risk factors responsible for the
occurrence of congestive heart failure include coronary artery disease, heart attack,
congenital heart defects, irregular heartbeats and valvular heart disease. Sleep apnoea and
viral infection are also responsible for congestive heart failure. Consumption of medications
like antidiabetic medications (rosiglitazone and pioglitazone), nonsteroidal anti-inflammatory
drugs (NSAIDs), certain anaesthetics, anti-arrhythmic medications, antihypertensive and
anticancer are responsible for the occurrence of congestive heart failure. Approximately 2 %
and 5 % of persons in the age group 40 to 59 years and 60 to 69 years experiences congestive
heart failure respectively. Approximately 50 % of the patients diagnosed with congestive
heart failure die within five years after diagnosis. Approximately 6 to 9 times more sudden
death can occur in congestive heart failure patients as compared to the normal patients.
Family members of Mrs McKenzie should take responsibility to avoid exposure of risk
factors to her. Family members should monitor eating and medication consumption in her.
Family members should maintain positive communication with her because it is evident that
it can be helpful in maintaining adoption and maintenance of health behaviours. Family
members should focus on care of Mrs McKenzie rather than worrying about her diseased
2
condition because worrying about patient condition can lead to inaction in care of patient
(Dhingra et al., 2014; Raman, 2016).
Q2. :
Symptom Pathophysiology
Dyspnea Reduced cardiac can lead to
impaired supply of blood to
the skeletal muscle. It leads
to the augmented left
ventricular filling pressure
to maintain optimum cardiac
output. It can lead to
reduced pulmonary diffusion
and consequently interstitial
edema which results in the
breathlessness. Raised
diastolic pressure results in
the increased expenditure of
myocardial energy. It leads
to ventricle remodelling,
raised myocardial oxygen
demand and myocardial
ischemia. Mrs McKenzie
is also experiencing
breathlessness (Güder et al.,
2014).
Swollen ankle Swollen ankle indicates
increased swelling in the leg
or ankle. It mainly occurs
due to the increased fluid
accumulation in the body.
This build-up of fluid occurs
3
(Dhingra et al., 2014; Raman, 2016).
Q2. :
Symptom Pathophysiology
Dyspnea Reduced cardiac can lead to
impaired supply of blood to
the skeletal muscle. It leads
to the augmented left
ventricular filling pressure
to maintain optimum cardiac
output. It can lead to
reduced pulmonary diffusion
and consequently interstitial
edema which results in the
breathlessness. Raised
diastolic pressure results in
the increased expenditure of
myocardial energy. It leads
to ventricle remodelling,
raised myocardial oxygen
demand and myocardial
ischemia. Mrs McKenzie
is also experiencing
breathlessness (Güder et al.,
2014).
Swollen ankle Swollen ankle indicates
increased swelling in the leg
or ankle. It mainly occurs
due to the increased fluid
accumulation in the body.
This build-up of fluid occurs
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
in the body due to decreased
blood flow out of the heart.
Release of atrial natriuretic
peptide and B-type
natriuretic peptide can lead
to the vasodilation and
reduced ventricular felling
pressure which reduces
cardiac preload and
afterload. It leads to the back
flow of blood to the heart
through the veins. Mrs
McKenzie also exhibited
signs of swollen ankle (Moe,
2013).
Dizziness Dizziness can occur in
patients of congestive heart
failure mainly due to
reduced supply of blood to
the brain. Reduction in the
blood supply to brain can
occur when there is heart
rate or rhythm is abnormal.
In such case, heart would be
unable to pump adequate
amount of blood due to
block in the blood flow
which can occur due to
narrowing of the valve. In
Mrs McKenzie also, mild
dizziness was observed
(Kovács et al., 2014).
Tachycardia Life-threatening ventricular
arrhythmias can occur in
4
blood flow out of the heart.
Release of atrial natriuretic
peptide and B-type
natriuretic peptide can lead
to the vasodilation and
reduced ventricular felling
pressure which reduces
cardiac preload and
afterload. It leads to the back
flow of blood to the heart
through the veins. Mrs
McKenzie also exhibited
signs of swollen ankle (Moe,
2013).
Dizziness Dizziness can occur in
patients of congestive heart
failure mainly due to
reduced supply of blood to
the brain. Reduction in the
blood supply to brain can
occur when there is heart
rate or rhythm is abnormal.
In such case, heart would be
unable to pump adequate
amount of blood due to
block in the blood flow
which can occur due to
narrowing of the valve. In
Mrs McKenzie also, mild
dizziness was observed
(Kovács et al., 2014).
Tachycardia Life-threatening ventricular
arrhythmias can occur in
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
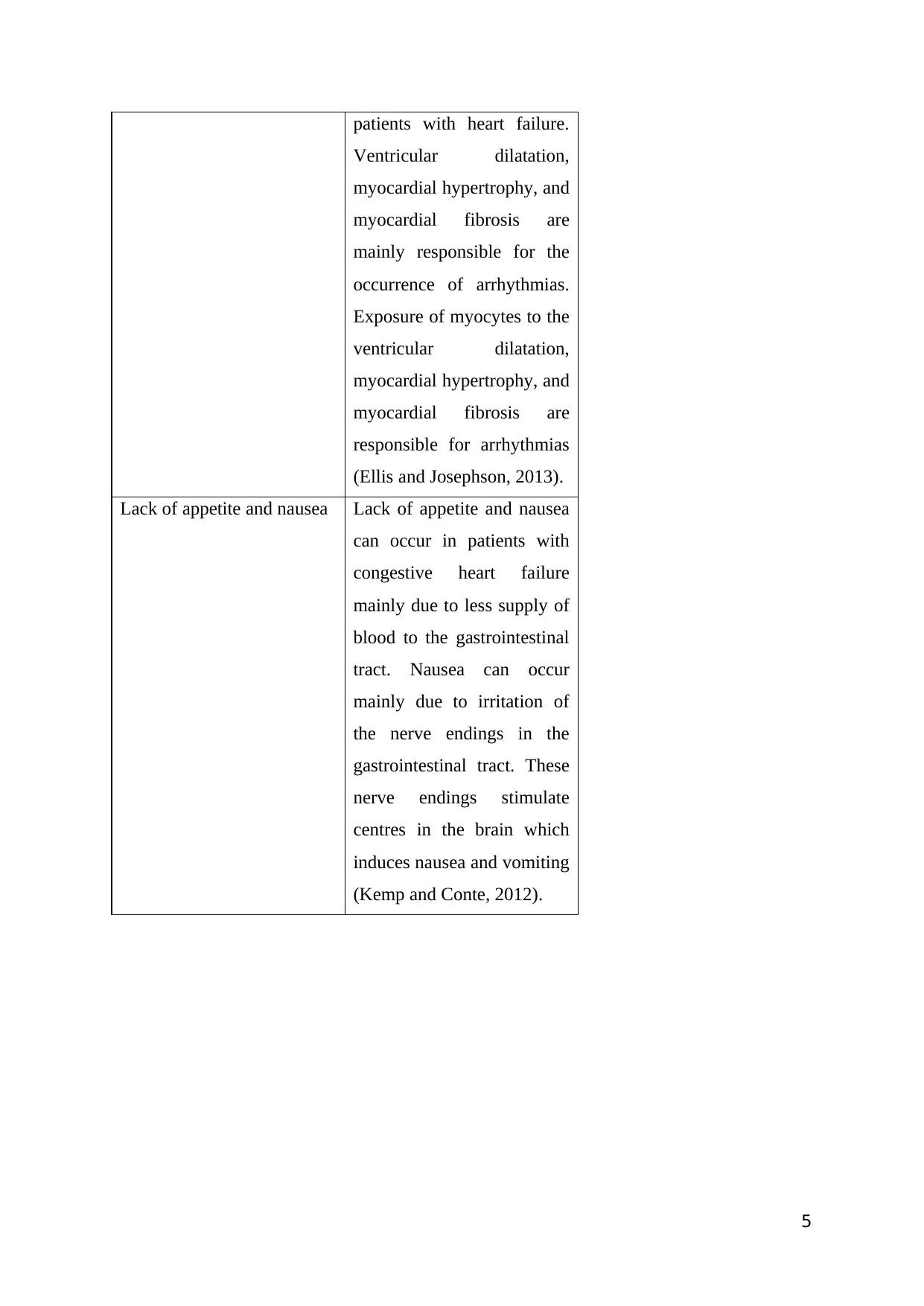
patients with heart failure.
Ventricular dilatation,
myocardial hypertrophy, and
myocardial fibrosis are
mainly responsible for the
occurrence of arrhythmias.
Exposure of myocytes to the
ventricular dilatation,
myocardial hypertrophy, and
myocardial fibrosis are
responsible for arrhythmias
(Ellis and Josephson, 2013).
Lack of appetite and nausea Lack of appetite and nausea
can occur in patients with
congestive heart failure
mainly due to less supply of
blood to the gastrointestinal
tract. Nausea can occur
mainly due to irritation of
the nerve endings in the
gastrointestinal tract. These
nerve endings stimulate
centres in the brain which
induces nausea and vomiting
(Kemp and Conte, 2012).
5
Ventricular dilatation,
myocardial hypertrophy, and
myocardial fibrosis are
mainly responsible for the
occurrence of arrhythmias.
Exposure of myocytes to the
ventricular dilatation,
myocardial hypertrophy, and
myocardial fibrosis are
responsible for arrhythmias
(Ellis and Josephson, 2013).
Lack of appetite and nausea Lack of appetite and nausea
can occur in patients with
congestive heart failure
mainly due to less supply of
blood to the gastrointestinal
tract. Nausea can occur
mainly due to irritation of
the nerve endings in the
gastrointestinal tract. These
nerve endings stimulate
centres in the brain which
induces nausea and vomiting
(Kemp and Conte, 2012).
5
Q.3.
Angiotensin-converting-enzyme inhibitor:
Angiotensin-converting-enzyme inhibitor (ACE inhibitor) can be used as the first line therapy
for the congestive heart failure. ACE inhibitors exhibits its effect by inhibiting angiotensin-
converting enzyme which is a prominent component of renin–angiotensin- aldosterone
(RAAS) system. RAAS system is responsible for the hypertension. ACE inhibitors halt
conversion of Angiotensin I (ATI) to Angiotensin II (ATII) . It leads to lowered arteriolar
resistance, augmented venous capacity, reduced cardiac output and volume, lowered
resistance in blood vessels and increased excretion of sodium in the urine. Benazepril,
zofenopril, perindopril, trandolapril, captopril, enalapril, lisinopril, and ramipril are the
examples of the ACE inhibitors. ACE inhibitors can relax blood vessels and reduce blood
volume which can be helpful in lowering blood pressure and reducing oxygen demand from
the heart (Sayer and Bhat, 2014; Valika and Gheorghiade, 2013).
Beta blockers :
Beta blockers can be useful in managing heart arrhythmias which can be helpful in reducing
second chance of heart attack. Beta blockers are competitive antagonists which acts on
receptor sites of endogenous catecholamines like epinephrine (adrenaline) and
norepinephrine (noradrenaline). Beta blockers block action of catecholamine of the
sympathetic nervous system. Few of the beta blockers act on all the β-adrenergic receptors
while others act on the specific β-adrenergic receptors like β1, β2 and β3 receptors. Beta
blockers useful in the congestive heart failure specifically act on the β1 receptors because β1-
adrenergic receptors specifically present in the heart. Bisoprolol, carvedilol, and sustained-
release metoprolol are the examples of beta blockers useful in the congestive heart failure.
Beta blockers reduce heart rate. Beta blockers also exhibit its action on renin–angiotensin
system by reducing secretion of renin. By reducing renin secretion, beta blockers lower
extracellular volume and consequently reduces heart oxygen demand. In hear failure , there is
increased sympathetic activity due to increased catecholamines which lead to the increased
oxygen demand, secretion of inflammatory mediators and inappropriate myocyte
remodelling. It leads to the reduced efficiency of cardiac contraction and reduced ejection
fraction. Beta blockers restores normal physiological functions by countering augmented
sympathetic activity (Bavishi et al., 2015; Buchhorn and McConnell, 2014).
6
Angiotensin-converting-enzyme inhibitor:
Angiotensin-converting-enzyme inhibitor (ACE inhibitor) can be used as the first line therapy
for the congestive heart failure. ACE inhibitors exhibits its effect by inhibiting angiotensin-
converting enzyme which is a prominent component of renin–angiotensin- aldosterone
(RAAS) system. RAAS system is responsible for the hypertension. ACE inhibitors halt
conversion of Angiotensin I (ATI) to Angiotensin II (ATII) . It leads to lowered arteriolar
resistance, augmented venous capacity, reduced cardiac output and volume, lowered
resistance in blood vessels and increased excretion of sodium in the urine. Benazepril,
zofenopril, perindopril, trandolapril, captopril, enalapril, lisinopril, and ramipril are the
examples of the ACE inhibitors. ACE inhibitors can relax blood vessels and reduce blood
volume which can be helpful in lowering blood pressure and reducing oxygen demand from
the heart (Sayer and Bhat, 2014; Valika and Gheorghiade, 2013).
Beta blockers :
Beta blockers can be useful in managing heart arrhythmias which can be helpful in reducing
second chance of heart attack. Beta blockers are competitive antagonists which acts on
receptor sites of endogenous catecholamines like epinephrine (adrenaline) and
norepinephrine (noradrenaline). Beta blockers block action of catecholamine of the
sympathetic nervous system. Few of the beta blockers act on all the β-adrenergic receptors
while others act on the specific β-adrenergic receptors like β1, β2 and β3 receptors. Beta
blockers useful in the congestive heart failure specifically act on the β1 receptors because β1-
adrenergic receptors specifically present in the heart. Bisoprolol, carvedilol, and sustained-
release metoprolol are the examples of beta blockers useful in the congestive heart failure.
Beta blockers reduce heart rate. Beta blockers also exhibit its action on renin–angiotensin
system by reducing secretion of renin. By reducing renin secretion, beta blockers lower
extracellular volume and consequently reduces heart oxygen demand. In hear failure , there is
increased sympathetic activity due to increased catecholamines which lead to the increased
oxygen demand, secretion of inflammatory mediators and inappropriate myocyte
remodelling. It leads to the reduced efficiency of cardiac contraction and reduced ejection
fraction. Beta blockers restores normal physiological functions by countering augmented
sympathetic activity (Bavishi et al., 2015; Buchhorn and McConnell, 2014).
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Q.4.
Intervention Rationale
Cardiovascular intervention Auscultate apical pulse,
monitor heart rate and heart
beat rhythm.
Heart sound should be
noted.
Peripheral pulses should be
palpated.
Blood pressure should be
monitored.
Amount of urine output and
Patient is associated with
bradycardia. Patients with
congestive heart failure are
associated with
dysrhythmias like premature
atrial contractions (PACs),
paroxysmal atrial
tachycardia (PAT), PVCs,
multifocal atrial tachycardia
(MAT), and atrial
fibrillation (AF).
Due to impaired pumping
action, S1 and S2 sounds
might be weak. Murmurs
might be evident due to
valvular incompetence.
Reduced cardiac output can
be evident in the abnormal
pulses like radial, popliteal,
dorsalis pedis, and post
tibial pulses.
In the initial period, there
might be occurrence of
hypertension due to
increased systemic vascular
resistance (SVR).
Due to reduced cardiac
output, there might be
7
Intervention Rationale
Cardiovascular intervention Auscultate apical pulse,
monitor heart rate and heart
beat rhythm.
Heart sound should be
noted.
Peripheral pulses should be
palpated.
Blood pressure should be
monitored.
Amount of urine output and
Patient is associated with
bradycardia. Patients with
congestive heart failure are
associated with
dysrhythmias like premature
atrial contractions (PACs),
paroxysmal atrial
tachycardia (PAT), PVCs,
multifocal atrial tachycardia
(MAT), and atrial
fibrillation (AF).
Due to impaired pumping
action, S1 and S2 sounds
might be weak. Murmurs
might be evident due to
valvular incompetence.
Reduced cardiac output can
be evident in the abnormal
pulses like radial, popliteal,
dorsalis pedis, and post
tibial pulses.
In the initial period, there
might be occurrence of
hypertension due to
increased systemic vascular
resistance (SVR).
Due to reduced cardiac
output, there might be
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
concentration of urine
should be noted.
Make sure that patient is
continuing with the
consumption of medications
like furosemide and enalpril.
reduced urine output due to
retention of sodium and
water.
Diuretics can be helpful in
improving condition of
patient by reducing preload,
maintaining normal cardiac
output and reducing
congestive symptoms.
ACE inhibitors can be useful
in congestive heart failure
patients by reducing
ventricular filling pressure
and increasing cardiac
output (Paul and Hice, 2014;
Currie, et al., 2015).
Respiratory intervention Assess respiratory rate every
four hour.
ABG levels should be
assessed.
Breathing pattern should be
observed.
Average respiratory rate for
adults is 10 – 20 bpm. If
deviation from it can be
detected as abnormal.
Detection of breathing
pattern can be helpful in
identifying abnormal
respiratory system.
It would helpful in
monitoring oxygenation and
ventilation pattern. ABG
analysis comprise of pH,
PaCO2, HCO3 and PaO2. It
would be helpful in
determining hypoxia and
acidosis.
It would be helpful in
understanding underlying
8
should be noted.
Make sure that patient is
continuing with the
consumption of medications
like furosemide and enalpril.
reduced urine output due to
retention of sodium and
water.
Diuretics can be helpful in
improving condition of
patient by reducing preload,
maintaining normal cardiac
output and reducing
congestive symptoms.
ACE inhibitors can be useful
in congestive heart failure
patients by reducing
ventricular filling pressure
and increasing cardiac
output (Paul and Hice, 2014;
Currie, et al., 2015).
Respiratory intervention Assess respiratory rate every
four hour.
ABG levels should be
assessed.
Breathing pattern should be
observed.
Average respiratory rate for
adults is 10 – 20 bpm. If
deviation from it can be
detected as abnormal.
Detection of breathing
pattern can be helpful in
identifying abnormal
respiratory system.
It would helpful in
monitoring oxygenation and
ventilation pattern. ABG
analysis comprise of pH,
PaCO2, HCO3 and PaO2. It
would be helpful in
determining hypoxia and
acidosis.
It would be helpful in
understanding underlying
8
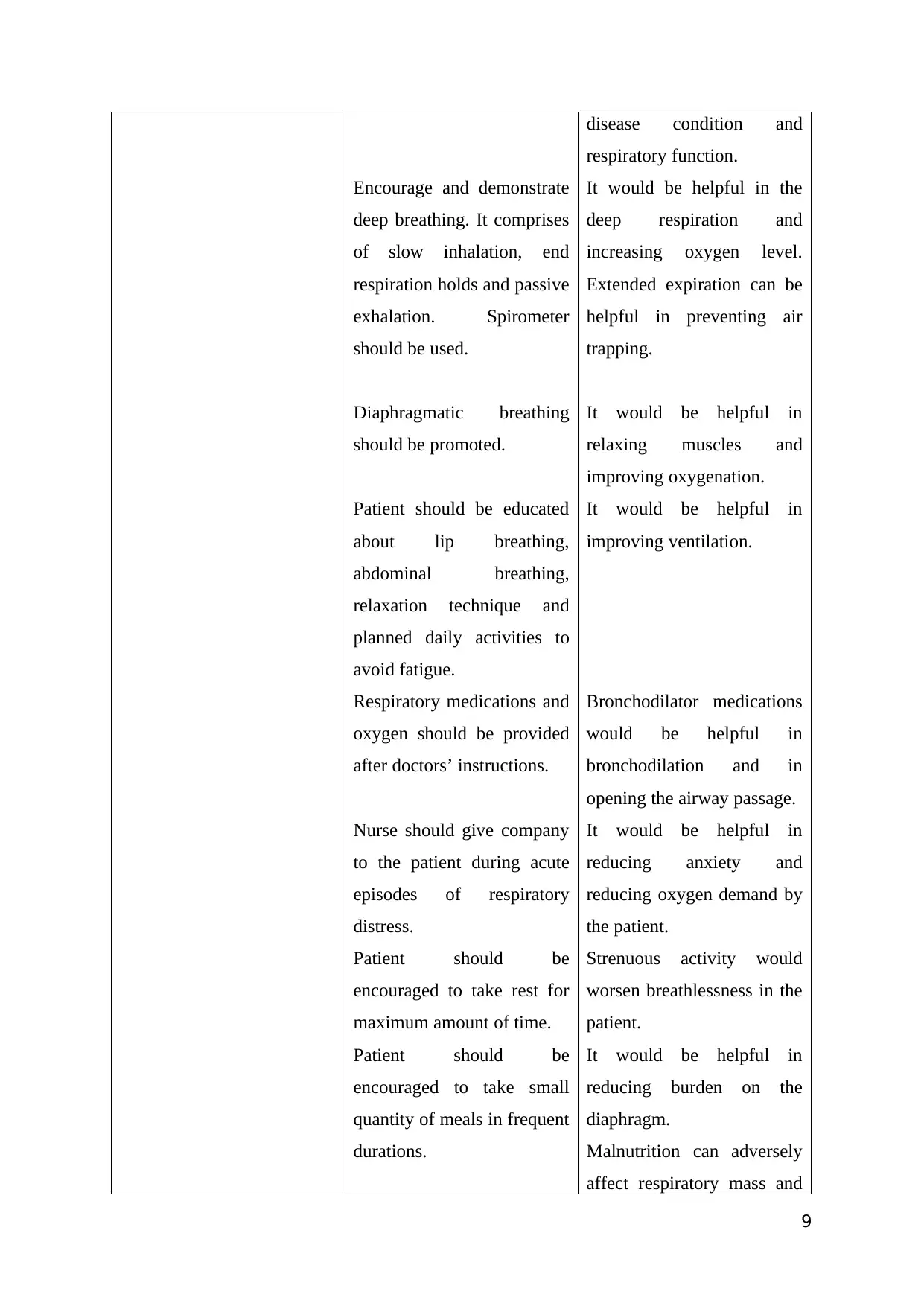
Encourage and demonstrate
deep breathing. It comprises
of slow inhalation, end
respiration holds and passive
exhalation. Spirometer
should be used.
Diaphragmatic breathing
should be promoted.
Patient should be educated
about lip breathing,
abdominal breathing,
relaxation technique and
planned daily activities to
avoid fatigue.
Respiratory medications and
oxygen should be provided
after doctors’ instructions.
Nurse should give company
to the patient during acute
episodes of respiratory
distress.
Patient should be
encouraged to take rest for
maximum amount of time.
Patient should be
encouraged to take small
quantity of meals in frequent
durations.
disease condition and
respiratory function.
It would be helpful in the
deep respiration and
increasing oxygen level.
Extended expiration can be
helpful in preventing air
trapping.
It would be helpful in
relaxing muscles and
improving oxygenation.
It would be helpful in
improving ventilation.
Bronchodilator medications
would be helpful in
bronchodilation and in
opening the airway passage.
It would be helpful in
reducing anxiety and
reducing oxygen demand by
the patient.
Strenuous activity would
worsen breathlessness in the
patient.
It would be helpful in
reducing burden on the
diaphragm.
Malnutrition can adversely
affect respiratory mass and
9
deep breathing. It comprises
of slow inhalation, end
respiration holds and passive
exhalation. Spirometer
should be used.
Diaphragmatic breathing
should be promoted.
Patient should be educated
about lip breathing,
abdominal breathing,
relaxation technique and
planned daily activities to
avoid fatigue.
Respiratory medications and
oxygen should be provided
after doctors’ instructions.
Nurse should give company
to the patient during acute
episodes of respiratory
distress.
Patient should be
encouraged to take rest for
maximum amount of time.
Patient should be
encouraged to take small
quantity of meals in frequent
durations.
disease condition and
respiratory function.
It would be helpful in the
deep respiration and
increasing oxygen level.
Extended expiration can be
helpful in preventing air
trapping.
It would be helpful in
relaxing muscles and
improving oxygenation.
It would be helpful in
improving ventilation.
Bronchodilator medications
would be helpful in
bronchodilation and in
opening the airway passage.
It would be helpful in
reducing anxiety and
reducing oxygen demand by
the patient.
Strenuous activity would
worsen breathlessness in the
patient.
It would be helpful in
reducing burden on the
diaphragm.
Malnutrition can adversely
affect respiratory mass and
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
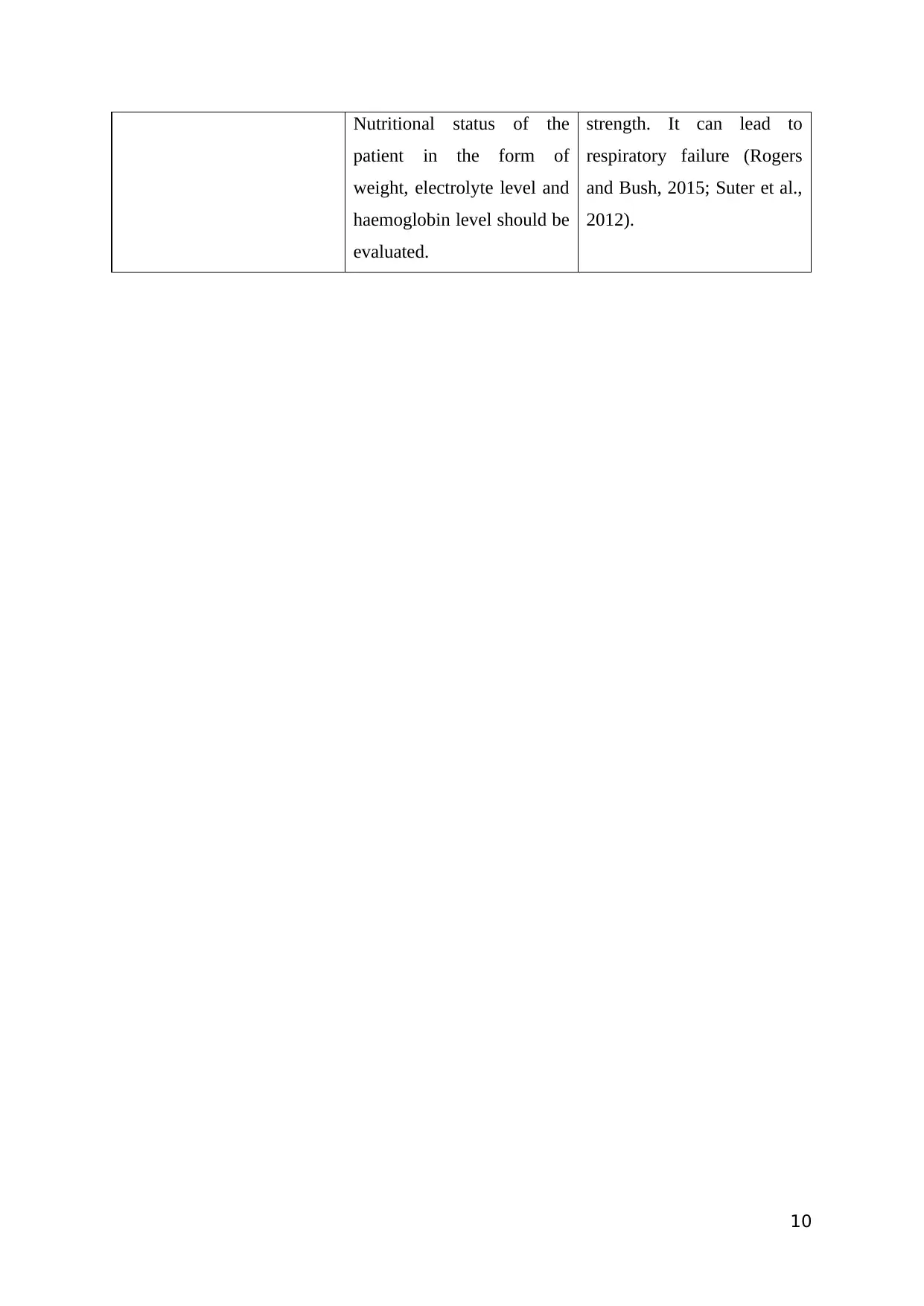
Nutritional status of the
patient in the form of
weight, electrolyte level and
haemoglobin level should be
evaluated.
strength. It can lead to
respiratory failure (Rogers
and Bush, 2015; Suter et al.,
2012).
10
patient in the form of
weight, electrolyte level and
haemoglobin level should be
evaluated.
strength. It can lead to
respiratory failure (Rogers
and Bush, 2015; Suter et al.,
2012).
10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
References:
Bavishi, C., Chatterjee, S., Ather, S., et al. (2015). Beta-blockers in heart failure with
preserved ejection fraction: a meta-analysis. Heart Failure Reviews, 20(2), 193-201.
Buchhorn, R., and McConnell, M.E. (2014). Beta blockers in childhood heart failure - why
not? International Journal of Cardiology, 175(1), 211-2.
Currie, K., Strachan, P.H., Spaling, M., et al. (2015). The importance of interactions between
patients and healthcare professionals for heart failure self-care: A systematic review
of qualitative research into patient perspectives. European Journal of Cardiovascular
Nursing, 14(6), 525-35.
Dhingra, A., Garg, A., Kaur, S., Chopra, S., et al. (2014). Epidemiology of heart failure with
preserved ejection fraction. Current Heart Failure Reports, 11(4), 354-65.
Ellis, E.R., and Josephson, M.E. (2013). Heart failure and tachycardia-induced
cardiomyopathy. Current Heart Failure Reports, 10(4), 296-306.
Güde, G., Brenner, S., Störk, S., Hoes, A., and Rutten, H. Chronic obstructive pulmonary
disease in heart failure: accurate diagnosis and treatment. European Journal of Heart
Failure, 16(12), 1273-82.
Kemp, C.D., and Conte, J.V. (2012). The pathophysiology of heart failure. Cardiovascular
Pathology, 21(5), 365-71.
Kovács, Á., Papp, Z., and Nagy, L. (2014). Causes and pathophysiology of heart failure with
preserved ejection fraction. Heart Failure Clinics, 10(3), 389-98.
Mahmood, S. S., and Wang, T. J. (2013). The epidemiology of congestive heart failure: the
Framingham Heart Study perspective. Global Heart, 8(1), 77–82.
Moe, G. (2016). Heart failure with multiple comorbidities. Current Opinion in Cardiology,
31(2), 209-16.
Paul, S., and Hice, A. (2014). Role of the acute care nurse in managing patients with heart
failure using evidence-based care. Critical Care Nursing Q, 37(4), 357-76.
Raman, J. (2016). Management of Heart Failure. Springer.
Rogers, C., and Bush, N. (2015). Heart Failure: Pathophysiology, Diagnosis, Medical
Treatment Guidelines, and Nursing Management. Nursing Clinics of North America,
50(4), 787-99.
Sayer, G., and Bhat, G. (2014). The renin-angiotensin-aldosterone system and heart failure.
Cardiology Clinics, 32(1), 21-32.
Suter, P.M., Gorski, L.A., Hennessey, B., and Suter, W.N. (2012). Best practices for heart
failure: a focused review. Home Healthcare Nurse, 30(7), 394-405.
Valika, A.A., and Gheorghiade, M. (2013). Ace inhibitor therapy for heart failure in patients
with impaired renal function: a review of the literature. Heart Failure Reviews, 18(2),
135-40.
11
Bavishi, C., Chatterjee, S., Ather, S., et al. (2015). Beta-blockers in heart failure with
preserved ejection fraction: a meta-analysis. Heart Failure Reviews, 20(2), 193-201.
Buchhorn, R., and McConnell, M.E. (2014). Beta blockers in childhood heart failure - why
not? International Journal of Cardiology, 175(1), 211-2.
Currie, K., Strachan, P.H., Spaling, M., et al. (2015). The importance of interactions between
patients and healthcare professionals for heart failure self-care: A systematic review
of qualitative research into patient perspectives. European Journal of Cardiovascular
Nursing, 14(6), 525-35.
Dhingra, A., Garg, A., Kaur, S., Chopra, S., et al. (2014). Epidemiology of heart failure with
preserved ejection fraction. Current Heart Failure Reports, 11(4), 354-65.
Ellis, E.R., and Josephson, M.E. (2013). Heart failure and tachycardia-induced
cardiomyopathy. Current Heart Failure Reports, 10(4), 296-306.
Güde, G., Brenner, S., Störk, S., Hoes, A., and Rutten, H. Chronic obstructive pulmonary
disease in heart failure: accurate diagnosis and treatment. European Journal of Heart
Failure, 16(12), 1273-82.
Kemp, C.D., and Conte, J.V. (2012). The pathophysiology of heart failure. Cardiovascular
Pathology, 21(5), 365-71.
Kovács, Á., Papp, Z., and Nagy, L. (2014). Causes and pathophysiology of heart failure with
preserved ejection fraction. Heart Failure Clinics, 10(3), 389-98.
Mahmood, S. S., and Wang, T. J. (2013). The epidemiology of congestive heart failure: the
Framingham Heart Study perspective. Global Heart, 8(1), 77–82.
Moe, G. (2016). Heart failure with multiple comorbidities. Current Opinion in Cardiology,
31(2), 209-16.
Paul, S., and Hice, A. (2014). Role of the acute care nurse in managing patients with heart
failure using evidence-based care. Critical Care Nursing Q, 37(4), 357-76.
Raman, J. (2016). Management of Heart Failure. Springer.
Rogers, C., and Bush, N. (2015). Heart Failure: Pathophysiology, Diagnosis, Medical
Treatment Guidelines, and Nursing Management. Nursing Clinics of North America,
50(4), 787-99.
Sayer, G., and Bhat, G. (2014). The renin-angiotensin-aldosterone system and heart failure.
Cardiology Clinics, 32(1), 21-32.
Suter, P.M., Gorski, L.A., Hennessey, B., and Suter, W.N. (2012). Best practices for heart
failure: a focused review. Home Healthcare Nurse, 30(7), 394-405.
Valika, A.A., and Gheorghiade, M. (2013). Ace inhibitor therapy for heart failure in patients
with impaired renal function: a review of the literature. Heart Failure Reviews, 18(2),
135-40.
11
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.