Case Study Analysis: Post-Operative Care of Mr. Jankovic, NSB335
VerifiedAdded on 2023/03/20
|16
|3995
|60
Case Study
AI Summary
This case study analyzes the post-operative care of Mr. Ivan Jankovic, a 78-year-old patient who underwent a left total hip replacement. The assignment addresses various aspects of his care, including the causes of obesity and its impact on health, communication errors in pre-operative assessments, and the importance of pre-operative checklists. It identifies risks associated with obesity and anesthesia, such as intubation problems, high-dose risk factors, and hypoventilation. The case study also explores the nursing responsibilities in addressing medication errors, managing post-operative delirium, and dealing with issues like severe pain, immobility, and post-operative delirium. It outlines nursing interventions, including pain management strategies, creating a safe environment, and providing physiotherapy. The evaluation of these interventions involves regular pain assessments, behavioral chart reviews, and mobility assessments. The study also highlights the importance of monitoring fluid intake and output and discusses potential causes and assessments for behavioral changes. The assignment is designed to demonstrate critical thinking and decision-making skills in complex healthcare situations.

Running head: CASE STUDY REVIEW.
CASE STUDY REVIEW
Name of Student:
Name of University:
Author’s Note:
CASE STUDY REVIEW
Name of Student:
Name of University:
Author’s Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1CASE STUDY REVIEW
Answer no 1.
Person who is obese have BMI of more than 26 and this outcome in the situation of low-
grade inflammation (Nuttall, 2015). The functioning and metabolism of the body are affected.
The cause of obesity is numerous; it is mostly instigated by the triacylglycerol which is stored in
the adipose tissue of the organs. The storage of such fats results because of high intake of
calories (Garvey, Hurley& Kushner, 2016). The fatty acid gets released due to Lipogenesis
which causes lipotoxicity inside the body. With copious secretion of lipids, it causes high blood
glucose level which in turn causes more storage of the fats. This cause release of adipokines like
visfatin where it gets accumulated in the joint ends, resulting in arthritis (Gul et al., 2015).
Adipocytes get aggregated in the bones joint which deteriorates the cartilage tissue of the bone
(Kulkarni et al., 2016). The primary reason for causing the occurrence of osteoarthritis is obesity.
Due to this, the bone becomes weak and dis-shaped. Obesity increases the pressure of the whole
body on the joint which causes in worse condition.
Answer no 2.
Numerous communication error has been noticed in the per-operative video of the patient
and nurse. While assessing the patient, the care provider did not communicate with the patient
and his family verbally. He neither introduced himself to the patient nor asked name, date of
birth and other essential details from the patients. It was seen that when the care provider came to
the patient to administer medicine, no full and relevant information was given by them. Instead,
the patient was forced to take medicine to complete their work fast. As per the standard of
NHSQH, the nurse and staffs must give detail information about the drug. From point of view of
Answer no 1.
Person who is obese have BMI of more than 26 and this outcome in the situation of low-
grade inflammation (Nuttall, 2015). The functioning and metabolism of the body are affected.
The cause of obesity is numerous; it is mostly instigated by the triacylglycerol which is stored in
the adipose tissue of the organs. The storage of such fats results because of high intake of
calories (Garvey, Hurley& Kushner, 2016). The fatty acid gets released due to Lipogenesis
which causes lipotoxicity inside the body. With copious secretion of lipids, it causes high blood
glucose level which in turn causes more storage of the fats. This cause release of adipokines like
visfatin where it gets accumulated in the joint ends, resulting in arthritis (Gul et al., 2015).
Adipocytes get aggregated in the bones joint which deteriorates the cartilage tissue of the bone
(Kulkarni et al., 2016). The primary reason for causing the occurrence of osteoarthritis is obesity.
Due to this, the bone becomes weak and dis-shaped. Obesity increases the pressure of the whole
body on the joint which causes in worse condition.
Answer no 2.
Numerous communication error has been noticed in the per-operative video of the patient
and nurse. While assessing the patient, the care provider did not communicate with the patient
and his family verbally. He neither introduced himself to the patient nor asked name, date of
birth and other essential details from the patients. It was seen that when the care provider came to
the patient to administer medicine, no full and relevant information was given by them. Instead,
the patient was forced to take medicine to complete their work fast. As per the standard of
NHSQH, the nurse and staffs must give detail information about the drug. From point of view of
2CASE STUDY REVIEW
the patient, they need to know about the treatment given to him with all pertinent information.
Communication issue.was also noticed during checklist assessment. The care provider was using
unprofessional language and asking all irrelevant questions. Patient felt that the care provider is
only overviewing the checklist and least pondered in knowing the situation of the patients. The
body language of the care provider was not professional; rather it depicted disinterest and apathy
towards the patient's treatment and diagnosis.
Answer no 3.
The essentiality of the pre-operative checklist as tool in health sector is used to recognize
and document the complaint of the patients. If there is any risk related to health of the patients,
the issue is communicated to the concern doctors. The checklist highlights the critical
information about the objective and subjective data taken by the nurse, and this helps to evaluate
the vital sign at average level better. Additionally, it ensures that right patient is getting correct
medications and assessment (Molina et al., 2016). The pre-operative checklist also provides
possible concern of anaesthesia, and possible complication patient might have in a surgical
procedure (Haugen et al., 2015). Thus, it can be said that pre-operative checklist aims towards
safety of the patients which is related to the National Safety and Quality Health Service
(NSQHS) Standards (Australian Commission on Safety and Quality in Health Care, 2016). The
standard of comprehensive care is related to minimization of the harm of patients by ensuring
quality care plan developed by the care provider. The pre-operative checklist is the part of such
safety plan of the patient, by gathering and monitoring all the necessary health data. NSQHS 5
which focus on identification of the patient and matching procedure relates with the checklist
system as patient is investigated about their name and type of care given to them.
the patient, they need to know about the treatment given to him with all pertinent information.
Communication issue.was also noticed during checklist assessment. The care provider was using
unprofessional language and asking all irrelevant questions. Patient felt that the care provider is
only overviewing the checklist and least pondered in knowing the situation of the patients. The
body language of the care provider was not professional; rather it depicted disinterest and apathy
towards the patient's treatment and diagnosis.
Answer no 3.
The essentiality of the pre-operative checklist as tool in health sector is used to recognize
and document the complaint of the patients. If there is any risk related to health of the patients,
the issue is communicated to the concern doctors. The checklist highlights the critical
information about the objective and subjective data taken by the nurse, and this helps to evaluate
the vital sign at average level better. Additionally, it ensures that right patient is getting correct
medications and assessment (Molina et al., 2016). The pre-operative checklist also provides
possible concern of anaesthesia, and possible complication patient might have in a surgical
procedure (Haugen et al., 2015). Thus, it can be said that pre-operative checklist aims towards
safety of the patients which is related to the National Safety and Quality Health Service
(NSQHS) Standards (Australian Commission on Safety and Quality in Health Care, 2016). The
standard of comprehensive care is related to minimization of the harm of patients by ensuring
quality care plan developed by the care provider. The pre-operative checklist is the part of such
safety plan of the patient, by gathering and monitoring all the necessary health data. NSQHS 5
which focus on identification of the patient and matching procedure relates with the checklist
system as patient is investigated about their name and type of care given to them.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CASE STUDY REVIEW
Answer no 4.
The three crucial risks related to the health of Mr Jankovic concerning obesity and
anaesthesia are as follows:
1. Problem in intubation- In obese person, it is difficult to manage the airways passage
especially in elderly person. Obesity is the main challenge risk for occurrence in
problematic intubation (Kido et al., 2015). While administration of anaesthesia, the most
challenging part is to maintain the safe apnoea period. The morbid obese person tends to
have short apnoea period as it results in low saturation level of oxygen (Dohrn et
al.,2016)
2. High dose risk factor- From the study of Tjeertes et al. (2015), it is known that
administering correct dose is most crucial step in anaesthesia. In old adult, it is more
difficult phase, as any fault will result in lethal condition of the patient. The dose given is
calculated in accordance with the weight of the patients. Older people given large dose or
less dose might cause poorer result and loss of stimulator response or even death
respectively which is hard to get it reverse (Nightingale et al., 2015)
3. Hypoventilation- Study of Surve et al. (2015) tells that obese and old people breathe
slowly when given anaesthesia, as they may face the situation of hypoventilation which is
associated with issue of hypoxia, hypercapnia and heart stroke.
Answer no 5.
In the situation of wrong medication given to the patients, it is the responsibility of the
nurse to communicate the issue to the concerned doctor as soon as possible. Before this, the
Answer no 4.
The three crucial risks related to the health of Mr Jankovic concerning obesity and
anaesthesia are as follows:
1. Problem in intubation- In obese person, it is difficult to manage the airways passage
especially in elderly person. Obesity is the main challenge risk for occurrence in
problematic intubation (Kido et al., 2015). While administration of anaesthesia, the most
challenging part is to maintain the safe apnoea period. The morbid obese person tends to
have short apnoea period as it results in low saturation level of oxygen (Dohrn et
al.,2016)
2. High dose risk factor- From the study of Tjeertes et al. (2015), it is known that
administering correct dose is most crucial step in anaesthesia. In old adult, it is more
difficult phase, as any fault will result in lethal condition of the patient. The dose given is
calculated in accordance with the weight of the patients. Older people given large dose or
less dose might cause poorer result and loss of stimulator response or even death
respectively which is hard to get it reverse (Nightingale et al., 2015)
3. Hypoventilation- Study of Surve et al. (2015) tells that obese and old people breathe
slowly when given anaesthesia, as they may face the situation of hypoventilation which is
associated with issue of hypoxia, hypercapnia and heart stroke.
Answer no 5.
In the situation of wrong medication given to the patients, it is the responsibility of the
nurse to communicate the issue to the concerned doctor as soon as possible. Before this, the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CASE STUDY REVIEW
treating team and team leader of the nurse need to get information for proper evaluation and
quick action. The family of the patient is required to get information about the right plan of care
given to solve the issue (Smolowitze et al., 2015). The blood glucose level of the patient should
be immediately checked as because the medicine Metformin and Gliclazide are diabetic specific
tablets, which lowers the level of glucose in the blood (Hassan & Abd-Allah, 2015). Aspirin is
also known to reduce the blood platelets; the site of the wound should be assessed by the nursing
team for treatment. To overcome the problem, correct medication should be provided.
Responsibility of registered nurse in regard to the administration of the medicine and NSQHS
standard are;
1. Registered nurse need to help the health care professional in administering proper
medication and treatment plan to the patients.
2. To provide detail information about the type of medication, its side effects and procedure
for intake to the patient and their family members.
The nurse staff mainly provides NHQHS standard of medication safety and comprehensive care
by giving correct medicine in time. The registered nurse is the responsible body to provide
complete care by ensuring skilled clinical safety practice. If patient has any side effect of the
medicine, they need to communicate this to doctors and should take necessary step to provide
care to the patients. The nurse should ensure that correct medicine is given to the patient by
rechecking the medication and health checklist (Australian Commission on Safety and Quality in
Health Care, 2016).
treating team and team leader of the nurse need to get information for proper evaluation and
quick action. The family of the patient is required to get information about the right plan of care
given to solve the issue (Smolowitze et al., 2015). The blood glucose level of the patient should
be immediately checked as because the medicine Metformin and Gliclazide are diabetic specific
tablets, which lowers the level of glucose in the blood (Hassan & Abd-Allah, 2015). Aspirin is
also known to reduce the blood platelets; the site of the wound should be assessed by the nursing
team for treatment. To overcome the problem, correct medication should be provided.
Responsibility of registered nurse in regard to the administration of the medicine and NSQHS
standard are;
1. Registered nurse need to help the health care professional in administering proper
medication and treatment plan to the patients.
2. To provide detail information about the type of medication, its side effects and procedure
for intake to the patient and their family members.
The nurse staff mainly provides NHQHS standard of medication safety and comprehensive care
by giving correct medicine in time. The registered nurse is the responsible body to provide
complete care by ensuring skilled clinical safety practice. If patient has any side effect of the
medicine, they need to communicate this to doctors and should take necessary step to provide
care to the patients. The nurse should ensure that correct medicine is given to the patient by
rechecking the medication and health checklist (Australian Commission on Safety and Quality in
Health Care, 2016).
5CASE STUDY REVIEW
Answer no 6.
Ivan seems to be in a confused state of mind with aggressive behaviour post-operation
which can be related to occurrence of delirium and age factor. The neurological functioning of
the patient is adversely affected. Delirium is the prevailing situation in older patients which
might happen because of long hospitalization period (Marcantonio, 2017). With age, the neuron
starts to get degenerated resulting in cognitive impairment and aggressive behaviour (Shoair et
al., 2015).
The vital area of nursing management related to problem of cognitive dysfunction are as follows:
1. To give safety to the patient- In situation of behavioural change, safety of patient is of
high priority. The nurse must ensure the patient is not harming himself or others. There is
the need to take a step to make the patient relax by employing either correct medication
or by lowering the environmental stimulus (Björk et al., 2016).
2. To provide effective communication- Nurse needs to communicate detail information
about the possible side effect of the anaesthesia to the patient as well as to their family.
All the treatment care plan is shared by the nurse regarding the occurrence of behavioural
change (Hasemann et al., 2016).
Answer no 7.
The problem related to the cause of post-surgical phase of left hip replacement are:
1. Issue of severe pain- Hip replacement causes severe pain; hence nurse priority problem
is to manage the pain of the patient by administering pain reliever.
Answer no 6.
Ivan seems to be in a confused state of mind with aggressive behaviour post-operation
which can be related to occurrence of delirium and age factor. The neurological functioning of
the patient is adversely affected. Delirium is the prevailing situation in older patients which
might happen because of long hospitalization period (Marcantonio, 2017). With age, the neuron
starts to get degenerated resulting in cognitive impairment and aggressive behaviour (Shoair et
al., 2015).
The vital area of nursing management related to problem of cognitive dysfunction are as follows:
1. To give safety to the patient- In situation of behavioural change, safety of patient is of
high priority. The nurse must ensure the patient is not harming himself or others. There is
the need to take a step to make the patient relax by employing either correct medication
or by lowering the environmental stimulus (Björk et al., 2016).
2. To provide effective communication- Nurse needs to communicate detail information
about the possible side effect of the anaesthesia to the patient as well as to their family.
All the treatment care plan is shared by the nurse regarding the occurrence of behavioural
change (Hasemann et al., 2016).
Answer no 7.
The problem related to the cause of post-surgical phase of left hip replacement are:
1. Issue of severe pain- Hip replacement causes severe pain; hence nurse priority problem
is to manage the pain of the patient by administering pain reliever.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CASE STUDY REVIEW
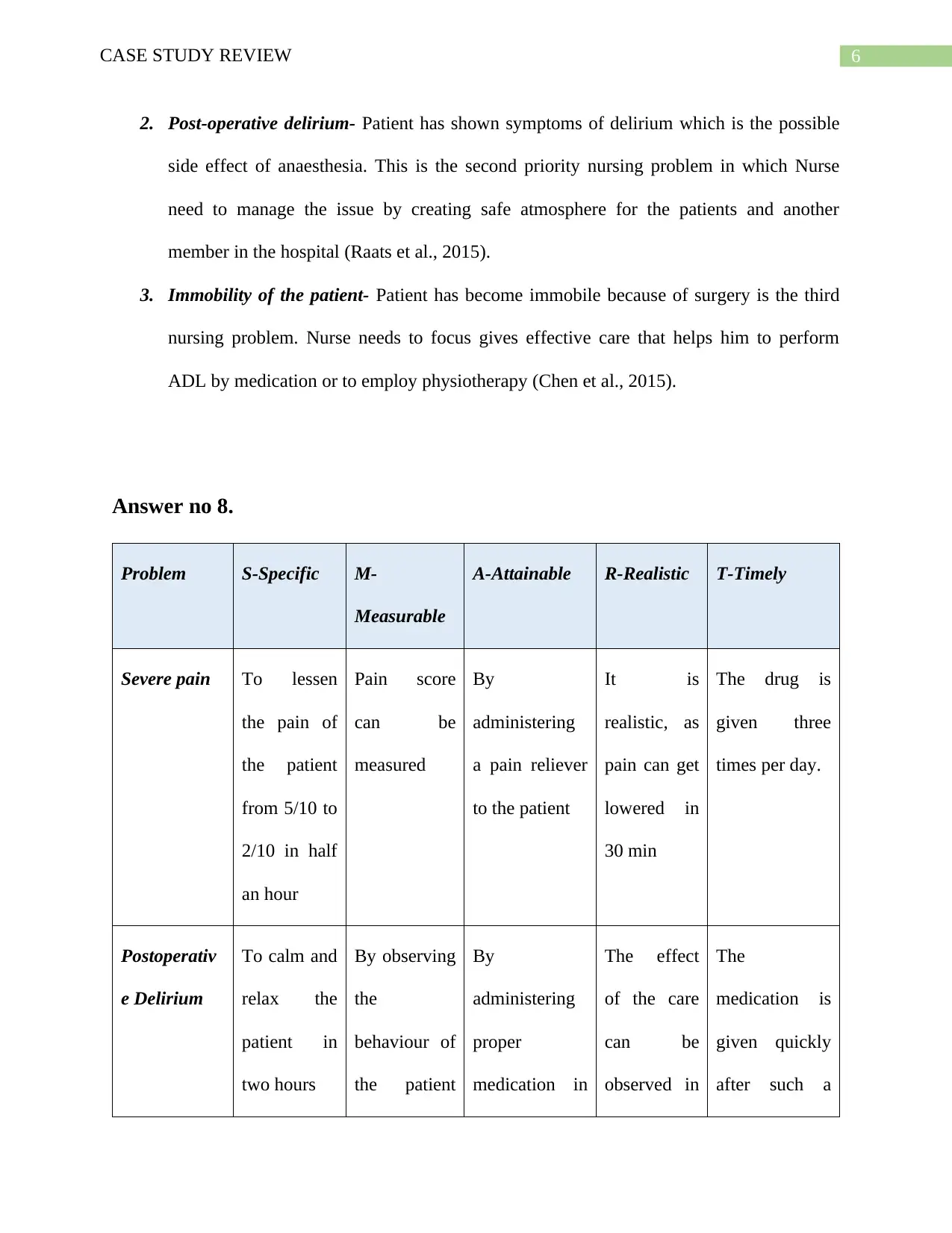
2. Post-operative delirium- Patient has shown symptoms of delirium which is the possible
side effect of anaesthesia. This is the second priority nursing problem in which Nurse
need to manage the issue by creating safe atmosphere for the patients and another
member in the hospital (Raats et al., 2015).
3. Immobility of the patient- Patient has become immobile because of surgery is the third
nursing problem. Nurse needs to focus gives effective care that helps him to perform
ADL by medication or to employ physiotherapy (Chen et al., 2015).
Answer no 8.
Problem S-Specific M-
Measurable
A-Attainable R-Realistic T-Timely
Severe pain To lessen
the pain of
the patient
from 5/10 to
2/10 in half
an hour
Pain score
can be
measured
By
administering
a pain reliever
to the patient
It is
realistic, as
pain can get
lowered in
30 min
The drug is
given three
times per day.
Postoperativ
e Delirium
To calm and
relax the
patient in
two hours
By observing
the
behaviour of
the patient
By
administering
proper
medication in
The effect
of the care
can be
observed in
The
medication is
given quickly
after such a
2. Post-operative delirium- Patient has shown symptoms of delirium which is the possible
side effect of anaesthesia. This is the second priority nursing problem in which Nurse
need to manage the issue by creating safe atmosphere for the patients and another
member in the hospital (Raats et al., 2015).
3. Immobility of the patient- Patient has become immobile because of surgery is the third
nursing problem. Nurse needs to focus gives effective care that helps him to perform
ADL by medication or to employ physiotherapy (Chen et al., 2015).
Answer no 8.
Problem S-Specific M-
Measurable
A-Attainable R-Realistic T-Timely
Severe pain To lessen
the pain of
the patient
from 5/10 to
2/10 in half
an hour
Pain score
can be
measured
By
administering
a pain reliever
to the patient
It is
realistic, as
pain can get
lowered in
30 min
The drug is
given three
times per day.
Postoperativ
e Delirium
To calm and
relax the
patient in
two hours
By observing
the
behaviour of
the patient
By
administering
proper
medication in
The effect
of the care
can be
observed in
The
medication is
given quickly
after such a
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CASE STUDY REVIEW
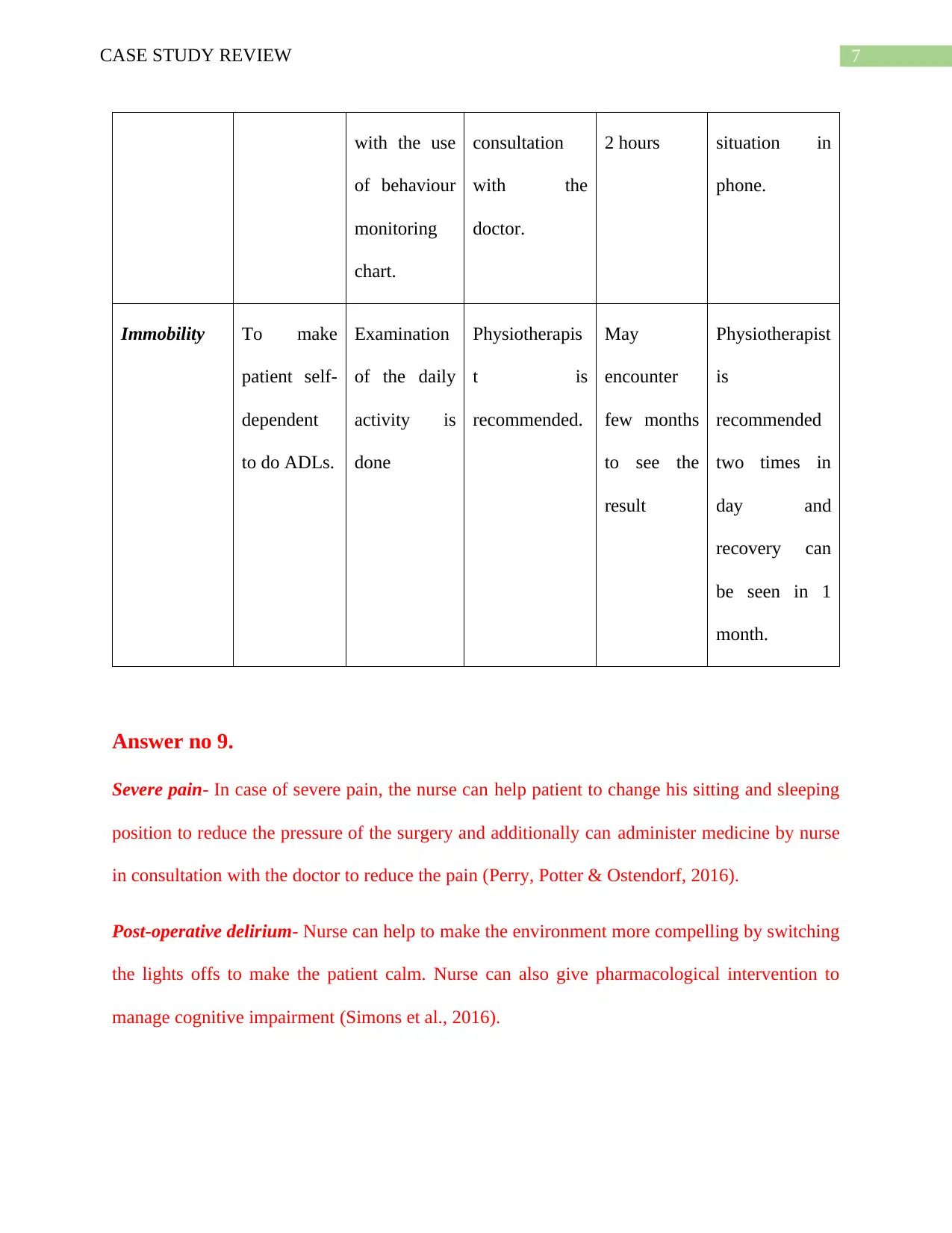
with the use
of behaviour
monitoring
chart.
consultation
with the
doctor.
2 hours situation in
phone.
Immobility To make
patient self-
dependent
to do ADLs.
Examination
of the daily
activity is
done
Physiotherapis
t is
recommended.
May
encounter
few months
to see the
result
Physiotherapist
is
recommended
two times in
day and
recovery can
be seen in 1
month.
Answer no 9.
Severe pain- In case of severe pain, the nurse can help patient to change his sitting and sleeping
position to reduce the pressure of the surgery and additionally can administer medicine by nurse
in consultation with the doctor to reduce the pain (Perry, Potter & Ostendorf, 2016).
Post-operative delirium- Nurse can help to make the environment more compelling by switching
the lights offs to make the patient calm. Nurse can also give pharmacological intervention to
manage cognitive impairment (Simons et al., 2016).
with the use
of behaviour
monitoring
chart.
consultation
with the
doctor.
2 hours situation in
phone.
Immobility To make
patient self-
dependent
to do ADLs.
Examination
of the daily
activity is
done
Physiotherapis
t is
recommended.
May
encounter
few months
to see the
result
Physiotherapist
is
recommended
two times in
day and
recovery can
be seen in 1
month.
Answer no 9.
Severe pain- In case of severe pain, the nurse can help patient to change his sitting and sleeping
position to reduce the pressure of the surgery and additionally can administer medicine by nurse
in consultation with the doctor to reduce the pain (Perry, Potter & Ostendorf, 2016).
Post-operative delirium- Nurse can help to make the environment more compelling by switching
the lights offs to make the patient calm. Nurse can also give pharmacological intervention to
manage cognitive impairment (Simons et al., 2016).
8CASE STUDY REVIEW
Immobility- To make the person able to stand on his own feet, nurse can arrange physiotherapy
that will help in proper circulation of blood and faster healing. Nurse can also administer relevant
medicine to make quick recovery of the patient (Devlin et al., 2018).
Answer no 10.
To evaluate the intervention made for severe pain of the patient, nurse can regularly investigate
the status of pain and pain score can be measured every day (Song et al., 2015).
To evaluate the post-operative delirium, the score in the behaviour chart prepared by the nurse is
checked every day. If there is reduction of score, it indicate better health of the patient. Nurse
also make observation of less confusion and aggression state of the patient (Todd et al., 2015).
To evaluate the mobility, ease in movement is assessed during each handover shift and the
investigation regarding the ease in movement is done, and score of range of motion is given by
the nurse (Richards et al., 2018).
Answer no 11.
The nursing assessment can be made to check the daily fluid intake of the patient and to monitor
the daily urinal output. For this nurse, motivate and encourage patient to increase the oral fluid
and they may also ask the patient for using bottle or commode chair as he is having problem in
moving.
Answer no 12.
One important reason for behaviour change in patient can be the side effect of
anaesthesia.
The three assessment are:
Immobility- To make the person able to stand on his own feet, nurse can arrange physiotherapy
that will help in proper circulation of blood and faster healing. Nurse can also administer relevant
medicine to make quick recovery of the patient (Devlin et al., 2018).
Answer no 10.
To evaluate the intervention made for severe pain of the patient, nurse can regularly investigate
the status of pain and pain score can be measured every day (Song et al., 2015).
To evaluate the post-operative delirium, the score in the behaviour chart prepared by the nurse is
checked every day. If there is reduction of score, it indicate better health of the patient. Nurse
also make observation of less confusion and aggression state of the patient (Todd et al., 2015).
To evaluate the mobility, ease in movement is assessed during each handover shift and the
investigation regarding the ease in movement is done, and score of range of motion is given by
the nurse (Richards et al., 2018).
Answer no 11.
The nursing assessment can be made to check the daily fluid intake of the patient and to monitor
the daily urinal output. For this nurse, motivate and encourage patient to increase the oral fluid
and they may also ask the patient for using bottle or commode chair as he is having problem in
moving.
Answer no 12.
One important reason for behaviour change in patient can be the side effect of
anaesthesia.
The three assessment are:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9CASE STUDY REVIEW
1. Assessment for stroke- He was drowsy and having slurred speech, so CT scan is done to
checks signs of stroke.
2. To check any medication error- Behavioural change in patient can be side effect of
wrong medicine. Hence, assessment of medication error is done.
3. Evaluating the pain reliever drugs- Pain reliever has side effect of cognitive
dysfunctional. Hence, nurse needs to properly assess the dose of medicine given.
Answer no 13.
Discharge planning is vital as it provides relevant and detail information about the status
of health of patient. It tells about the quality care given and association of hospital and
community. The discharge planning focus to reduce the stay of patient in hospital and assist in
managing the unplanned readmission in the hospital (Gonçalves‐Bradley et al., 2016).
The three realistic strategies are:
1. Recommending community nurse- Will help patient with medical care and support
in better recovery (McTiernan & McDonald, 2015).
2. Recommending community service – Domestic help patient to do his daily living
activities. Assistance in getting taxi voucher will help in travelling to hospital when
required (Grossman et al., 2018).
3. Recommending community physiotherapist- Will help patient to do exercise in time
and increase the mobility of the patient. Suggestion is also given like including a
nonslip mat in home and rails in the bed will help the patient from future falling
(Lewis, Peiris & Shields, 2017).
1. Assessment for stroke- He was drowsy and having slurred speech, so CT scan is done to
checks signs of stroke.
2. To check any medication error- Behavioural change in patient can be side effect of
wrong medicine. Hence, assessment of medication error is done.
3. Evaluating the pain reliever drugs- Pain reliever has side effect of cognitive
dysfunctional. Hence, nurse needs to properly assess the dose of medicine given.
Answer no 13.
Discharge planning is vital as it provides relevant and detail information about the status
of health of patient. It tells about the quality care given and association of hospital and
community. The discharge planning focus to reduce the stay of patient in hospital and assist in
managing the unplanned readmission in the hospital (Gonçalves‐Bradley et al., 2016).
The three realistic strategies are:
1. Recommending community nurse- Will help patient with medical care and support
in better recovery (McTiernan & McDonald, 2015).
2. Recommending community service – Domestic help patient to do his daily living
activities. Assistance in getting taxi voucher will help in travelling to hospital when
required (Grossman et al., 2018).
3. Recommending community physiotherapist- Will help patient to do exercise in time
and increase the mobility of the patient. Suggestion is also given like including a
nonslip mat in home and rails in the bed will help the patient from future falling
(Lewis, Peiris & Shields, 2017).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

10CASE STUDY REVIEW
11CASE STUDY REVIEW
Reference
Australian Commission on Safety and Quality in Health Care. (2016). Retrieved from
https://www.safetyandquality.gov.au/wp-content/uploads/2017/11/National-Safety-and-
Quality-Health-Service-Standards-second-edition.pdf
Chen, H., Gao, J., Su, S., Zhang, X., & Wang, Z. (2015). A visual-aided wireless monitoring
system design for total hip replacement surgery. IEEE transactions on biomedical
circuits and systems, 9(2), 227-236.
Devlin, J. W., Skrobik, Y., Gélinas, C., Needham, D. M., Slooter, A. J., Pandharipande, P. P., ...
& Balas, M. C. (2018). Clinical practice guidelines for the prevention and management of
pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the
ICU. Critical care medicine, 46(9), e825-e873.
Dohrn, N., Sommer, T., Bisgaard, J., Rønholm, E., & Larsen, J. F. (2016). Difficult tracheal
intubation in obese gastric bypass patients. Obesity surgery, 26(11), 2640-2647.
Garvey, W. T., Hurley, D. L., & Kushner, R. F. (2016). Patient-centered care of the patient with
obesity. Endocrine Practice, 22, 9.
Gonçalves‐Bradley, D. C., Lannin, N. A., Clemson, L. M., Cameron, I. D., & Shepperd, S.
(2016). Discharge planning from hospital. Cochrane database of systematic reviews, (1).
Grossman, D. C., Curry, S. J., Owens, D. K., Barry, M. J., Caughey, A. B., Davidson, K. W., ...
& Kubik, M. (2018). Interventions to prevent falls in community-dwelling older adults:
US Preventive Services Task Force recommendation statement. Jama, 319(16), 1696-
1704.
Reference
Australian Commission on Safety and Quality in Health Care. (2016). Retrieved from
https://www.safetyandquality.gov.au/wp-content/uploads/2017/11/National-Safety-and-
Quality-Health-Service-Standards-second-edition.pdf
Chen, H., Gao, J., Su, S., Zhang, X., & Wang, Z. (2015). A visual-aided wireless monitoring
system design for total hip replacement surgery. IEEE transactions on biomedical
circuits and systems, 9(2), 227-236.
Devlin, J. W., Skrobik, Y., Gélinas, C., Needham, D. M., Slooter, A. J., Pandharipande, P. P., ...
& Balas, M. C. (2018). Clinical practice guidelines for the prevention and management of
pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the
ICU. Critical care medicine, 46(9), e825-e873.
Dohrn, N., Sommer, T., Bisgaard, J., Rønholm, E., & Larsen, J. F. (2016). Difficult tracheal
intubation in obese gastric bypass patients. Obesity surgery, 26(11), 2640-2647.
Garvey, W. T., Hurley, D. L., & Kushner, R. F. (2016). Patient-centered care of the patient with
obesity. Endocrine Practice, 22, 9.
Gonçalves‐Bradley, D. C., Lannin, N. A., Clemson, L. M., Cameron, I. D., & Shepperd, S.
(2016). Discharge planning from hospital. Cochrane database of systematic reviews, (1).
Grossman, D. C., Curry, S. J., Owens, D. K., Barry, M. J., Caughey, A. B., Davidson, K. W., ...
& Kubik, M. (2018). Interventions to prevent falls in community-dwelling older adults:
US Preventive Services Task Force recommendation statement. Jama, 319(16), 1696-
1704.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 16
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.