Gold Coast University: 2804NRS Spinal Cord Compression Case Study
VerifiedAdded on 2022/09/15
|7
|1528
|18
Case Study
AI Summary
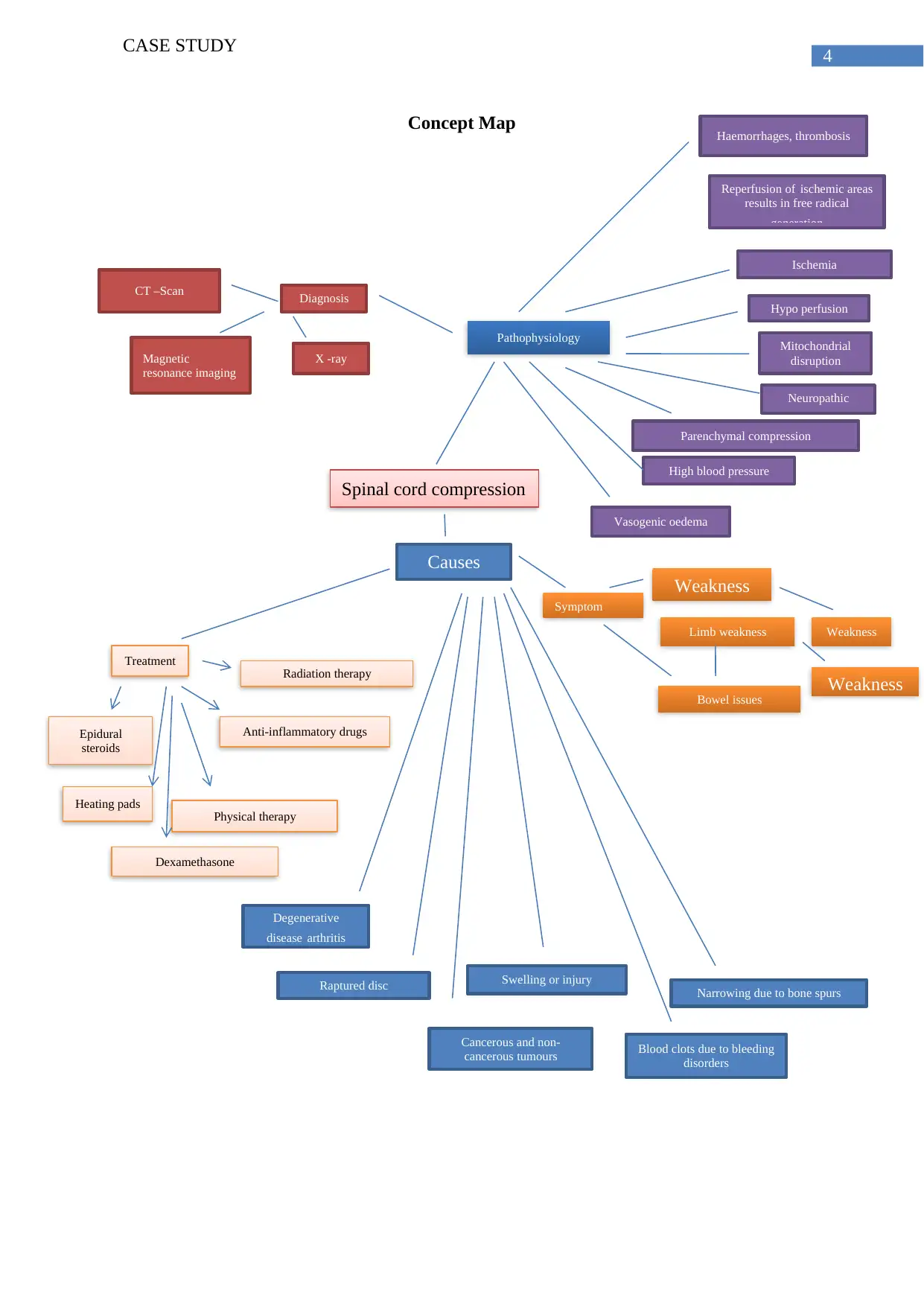
This case study examines a 65-year-old woman, Susan Kennedy, presenting with spinal cord compression due to osteoporotic vertebral fractures. The assignment details the patient's symptoms including back pain, numbness, and high blood pressure, along with hyperreflexia. It explores the aetiology, pathophysiology, diagnostic methods such as MRI and CT scans, and treatment options including medication, physical therapy, and epidural steroids. The analysis covers risk factors like osteoporosis and trauma, the step-by-step sequence of the links between the aetiology and the pathophysiology of the diagnosed disease, and the clinical manifestations. A concept map is included that visually represents the connections between risk factors, aetiology, pathophysiology, clinical manifestations, diagnostic tests, and treatment modalities. The assignment aims to demonstrate clinical reasoning skills and the ability to differentiate normal from abnormal presentations in a nursing context. The document also includes a concept map that visually represents the connections between risk factors, aetiology, pathophysiology, clinical manifestations, diagnostic tests, and treatment modalities, and a references list.

1 out of 7


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.