Analysis of policies to promote child and maternal care in India
VerifiedAdded on 2023/06/04
|43
|11762
|196
AI Summary
This research report analyzes the impact of policies on infant and maternal health in India. It evaluates the outcomes of each policy in relation to maternal health and suggests recommendations to improve healthcare systems.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
School of Public Health
Master (by coursework) Research Project Final Report – cover page for
Health Sciences Research Project (50 credits)
Master of (course)
Student ID
Given Names
Family name
Email Address
Title of Project: Analysis of the policies to promote child and maternal care in India
Human Research Ethics Approval required? YES/NO Link
Health and Safety Risk or Fieldwork assessment required? YES/NO link
Intellectual Property assessment required? YES/NO (Work funded externally)
Declaration by the student
To the best of my knowledge and belief this document contains no material previously
published by any other person except where due acknowledgment has been made.
This document contains no material which has been accepted for the award of any other
degree or diploma in any university.
Student ID:
Student Name:
Signature:
Supervisor:
Master (by coursework) Research Project Final Report – cover page for
Health Sciences Research Project (50 credits)
Master of (course)
Student ID
Given Names
Family name
Email Address
Title of Project: Analysis of the policies to promote child and maternal care in India
Human Research Ethics Approval required? YES/NO Link
Health and Safety Risk or Fieldwork assessment required? YES/NO link
Intellectual Property assessment required? YES/NO (Work funded externally)
Declaration by the student
To the best of my knowledge and belief this document contains no material previously
published by any other person except where due acknowledgment has been made.
This document contains no material which has been accepted for the award of any other
degree or diploma in any university.
Student ID:
Student Name:
Signature:
Supervisor:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Abstract:
Background: India is falling short of the MDG target despite implementation of several
maternal welfare initiatives. The main reason behind this being include poor adherence to
clinical guidelines, lack of patient centered care and inequitable delivery of care. Despite the
launch of Motherhood Scheme (Janani Suraksha Yojna program), the National Rural Health
Mission (NRHM), desired maternity health targets has not been achieved.
Methods: PRISMA guideline was used to search for articles from CINAHL, PubMed and
Medline database. Inclusion and exclusion criteria guided the search process and the
summary of the search process was provided in the form of PRISMA flowchart. Thematic
approach was used to analyse research findings.
Results: The study gave rise to four themes which included policies on MMR and
institutional delivery rate, reducing financial barrier to access, addressing inequities in
maternal care and improving access to antenatal care. It revealed the impact of program on
improving institutional delivery rate. However, quality of antenatal care was not achieved.
Discussion: From the analysis of research papers, it was found that JSY scheme did not
assess the readiness of facilities in rural areas and education and awareness aspects of health
promotion was not considered.
Conclusion: It suggests the need to remodel design of the program and increase recruitment
of skills health care professionals to improve maternal and antenatal care outcomes.
Background: India is falling short of the MDG target despite implementation of several
maternal welfare initiatives. The main reason behind this being include poor adherence to
clinical guidelines, lack of patient centered care and inequitable delivery of care. Despite the
launch of Motherhood Scheme (Janani Suraksha Yojna program), the National Rural Health
Mission (NRHM), desired maternity health targets has not been achieved.
Methods: PRISMA guideline was used to search for articles from CINAHL, PubMed and
Medline database. Inclusion and exclusion criteria guided the search process and the
summary of the search process was provided in the form of PRISMA flowchart. Thematic
approach was used to analyse research findings.
Results: The study gave rise to four themes which included policies on MMR and
institutional delivery rate, reducing financial barrier to access, addressing inequities in
maternal care and improving access to antenatal care. It revealed the impact of program on
improving institutional delivery rate. However, quality of antenatal care was not achieved.
Discussion: From the analysis of research papers, it was found that JSY scheme did not
assess the readiness of facilities in rural areas and education and awareness aspects of health
promotion was not considered.
Conclusion: It suggests the need to remodel design of the program and increase recruitment
of skills health care professionals to improve maternal and antenatal care outcomes.
Table of Contents
Introduction:...............................................................................................................................2
Literature review:.......................................................................................................................3
Aim and objectives:....................................................................................................................7
Methodology:.............................................................................................................................7
Results:.....................................................................................................................................13
Discussion:...............................................................................................................................24
Conclusion and recommendation:............................................................................................29
References:...............................................................................................................................32
Introduction:...............................................................................................................................2
Literature review:.......................................................................................................................3
Aim and objectives:....................................................................................................................7
Methodology:.............................................................................................................................7
Results:.....................................................................................................................................13
Discussion:...............................................................................................................................24
Conclusion and recommendation:............................................................................................29
References:...............................................................................................................................32
Introduction:
Pregnancy and motherhood are natural processes that bring many positive changes in
the life of a woman. However, many women end up suffering a lot during pregnancy because
of complications like preecmplasia, haeomorhage, unsafe abortion and infection. This
continues in the post-partum period and such issues occur mainly because of poor access to
quality maternal care (Mousumi, 2015). Improving maternal health and reducing maternal
deaths is one of the human rights challenges in middle and low income countries which has
attracted attention of many policy makers (Ram Jat, 2014). India is also among the middle
income countries which is struggling to deal with huge toll of maternal deaths. According to
Nair and Panda (2011), out of 5,36,000 maternal deaths worldwide every year, India
accounted for 11,700 deaths in 2005. However, with the introduction of public health
initiative in the last two to three decades, a recent report suggests a decline in maternal
mortality rate. The report by O'Neil, Naeve and Ved (2017) revealed a decline in maternal
mortality ratio from 892 maternal deaths/100, 000 live births in 1972-1976 to 178/10, 000
live births in 2010-2012. Despite this achievement, India is still short of the millennium
development goal (MDG) target of reducing maternal deaths to 109 maternal deaths/ 100, 000
live births (Travasso, 2015). In addition, due to the issue of poor maternal outcomes, the
Pregnancy and motherhood are natural processes that bring many positive changes in
the life of a woman. However, many women end up suffering a lot during pregnancy because
of complications like preecmplasia, haeomorhage, unsafe abortion and infection. This
continues in the post-partum period and such issues occur mainly because of poor access to
quality maternal care (Mousumi, 2015). Improving maternal health and reducing maternal
deaths is one of the human rights challenges in middle and low income countries which has
attracted attention of many policy makers (Ram Jat, 2014). India is also among the middle
income countries which is struggling to deal with huge toll of maternal deaths. According to
Nair and Panda (2011), out of 5,36,000 maternal deaths worldwide every year, India
accounted for 11,700 deaths in 2005. However, with the introduction of public health
initiative in the last two to three decades, a recent report suggests a decline in maternal
mortality rate. The report by O'Neil, Naeve and Ved (2017) revealed a decline in maternal
mortality ratio from 892 maternal deaths/100, 000 live births in 1972-1976 to 178/10, 000
live births in 2010-2012. Despite this achievement, India is still short of the millennium
development goal (MDG) target of reducing maternal deaths to 109 maternal deaths/ 100, 000
live births (Travasso, 2015). In addition, due to the issue of poor maternal outcomes, the
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
ultimate negative impact has been found on health of neonates and infants. Sankar et al.
(2016) explains that 0.75 million neonates dies every year in India, which is highest for any
country in the world. Although the rate of neonatal mortality rate has reduced from 52 per
1000 live births in 1990 compared to 28 per 1000 live births in 2013, rate of decline is slow
for infant and under-five children. Hence, improve figures of infant mortality rate also needs
to be prioritized.
Although many policies and initiatives have resulted in reducing the rate of maternal
maternity ratio (MMR) and improving infant development outcomes, the rate of improvement
has been very slow. Some of the issues that limit the delivery of quality maternal care in India
include poor adherence to clinical guidelines, lack of patient centered care and inequitable
delivery of care because of disproportionate distribution of facilities in urban settings (Joshi,
2013, June). Some of the policies and programs that paid attention to child and maternal
health included the Safe Motherhood Scheme (Janani Suraksha Yojna program), the National
Rural Health Mission (NRHM), immunization programs and many others. However, the
improvement in mortality rate and health of mothers has not yet achieved the desired standard
compared to other BRIC (Brazil, Russia, India and China) countries (Nair & Panda, 2011).
To understand the reason behind this trend, there is a need to analyze how policies related to
maternal and child health has fared in India. This would help to understand whether the health
care system is currently prepared to meet the key objectives of the policy or not.
The main purpose of this research is to conduct a systematic review of research
literatures to analyze the impact of policies on infant and maternal health in India. Systematic
review method will help to critically evaluate policy initiatives related to maternal and infant
health and understand their success or failures in terms of outcome achieved. Another
rationale behind conducting systematic review is that it will to critically explore all policies
implemented for maternal care in India and find out the strength and weakness of the policies
(2016) explains that 0.75 million neonates dies every year in India, which is highest for any
country in the world. Although the rate of neonatal mortality rate has reduced from 52 per
1000 live births in 1990 compared to 28 per 1000 live births in 2013, rate of decline is slow
for infant and under-five children. Hence, improve figures of infant mortality rate also needs
to be prioritized.
Although many policies and initiatives have resulted in reducing the rate of maternal
maternity ratio (MMR) and improving infant development outcomes, the rate of improvement
has been very slow. Some of the issues that limit the delivery of quality maternal care in India
include poor adherence to clinical guidelines, lack of patient centered care and inequitable
delivery of care because of disproportionate distribution of facilities in urban settings (Joshi,
2013, June). Some of the policies and programs that paid attention to child and maternal
health included the Safe Motherhood Scheme (Janani Suraksha Yojna program), the National
Rural Health Mission (NRHM), immunization programs and many others. However, the
improvement in mortality rate and health of mothers has not yet achieved the desired standard
compared to other BRIC (Brazil, Russia, India and China) countries (Nair & Panda, 2011).
To understand the reason behind this trend, there is a need to analyze how policies related to
maternal and child health has fared in India. This would help to understand whether the health
care system is currently prepared to meet the key objectives of the policy or not.
The main purpose of this research is to conduct a systematic review of research
literatures to analyze the impact of policies on infant and maternal health in India. Systematic
review method will help to critically evaluate policy initiatives related to maternal and infant
health and understand their success or failures in terms of outcome achieved. Another
rationale behind conducting systematic review is that it will to critically explore all policies
implemented for maternal care in India and find out the strength and weakness of the policies
in achieving desired maternal mortality rate target. The main objective of the systematic
review is to evaluate the outcomes of the policy initiatives and find out specific barriers or
facilitators that influenced the outcome. It also aims to recommend suggestions to improve
health care system by looking at barriers experienced while implementing policies related to
maternal health. The PRISMA framework has been applied to conduct and present the
outcomes of the selected research papers.
Literature review:
Past research papers have highlighted the challenges associated with providing quality
maternal care in India. Vora et al. (2009) gave evidence regarding the reason behind lower
maternity rate in India despite several programmatic efforts and rapid economic progress in
the country. The data related to current trends in maternal health was collected by Vora et al.
(2009) from review of literature (published and unpublished reports of government and
non-government agencies), interview with stakeholders and secondary analysis of data
from national programs. The Safe motherhood program strategies and implementation was
also analyzed to evaluate maternal health in India. The research findings revealed a decline in
MMR related to a decrease in incidence of malaria in pregnant women. In addition, most of
the maternal deaths in India occurred because of post partum haemorrhage. The report
suggested that instutional deliveries have increased in India. However, postnatal care remains
neglected as very few women visit a maternal clinic after the first week of delivery.
According to World Health Organization, postnatal period is a critical period for mothers and
babies where utmost care is needed to prevent maternal and infant deaths. However, this
remains the most neglected period for quality care provisions (World Health Organization,
2013). Hence, Vora et al. (2009) highlighted the importance of increasing postnatal care for
pregnant women. However, the gap in the research by Vora et al. (2009) is that it did not
review is to evaluate the outcomes of the policy initiatives and find out specific barriers or
facilitators that influenced the outcome. It also aims to recommend suggestions to improve
health care system by looking at barriers experienced while implementing policies related to
maternal health. The PRISMA framework has been applied to conduct and present the
outcomes of the selected research papers.
Literature review:
Past research papers have highlighted the challenges associated with providing quality
maternal care in India. Vora et al. (2009) gave evidence regarding the reason behind lower
maternity rate in India despite several programmatic efforts and rapid economic progress in
the country. The data related to current trends in maternal health was collected by Vora et al.
(2009) from review of literature (published and unpublished reports of government and
non-government agencies), interview with stakeholders and secondary analysis of data
from national programs. The Safe motherhood program strategies and implementation was
also analyzed to evaluate maternal health in India. The research findings revealed a decline in
MMR related to a decrease in incidence of malaria in pregnant women. In addition, most of
the maternal deaths in India occurred because of post partum haemorrhage. The report
suggested that instutional deliveries have increased in India. However, postnatal care remains
neglected as very few women visit a maternal clinic after the first week of delivery.
According to World Health Organization, postnatal period is a critical period for mothers and
babies where utmost care is needed to prevent maternal and infant deaths. However, this
remains the most neglected period for quality care provisions (World Health Organization,
2013). Hence, Vora et al. (2009) highlighted the importance of increasing postnatal care for
pregnant women. However, the gap in the research by Vora et al. (2009) is that it did not
mentioned whether the SAFE motherhood programme took any steps to improve the quality
of post natal care or not. This makes detailed analysis of the safe motherhood programme
necessary.
The research paper by Vora et al. (2009) also described the reason behind poor
maternal health. The study revealed the impact of education and economic status of women
as the reason behind poor access to maternal care. Considering the causal effect of education
on maternal health outcome is vital, Weitzman (2017) revealed that increasing women’s level
of education can decrease the rate of short birth intervals, unwanted pregnancy and an
increase in the use of antenatal care. Hence, finding presented by Vora et al. (2009) is
significant as it highlights areas which have remained neglected in maternal health
improvement initiative in India. It also specified limitations of the SAFE motherhood
program as giving more priority to immunization and antenatal care affected emergency
services. This occurred because fixed day scheduling of work lead to more focus on routine
preventive task and ignorance of emergency services. Overall, the analysis of the study
findings revealed that maternal care programs were implemented to strengthen the delivery of
care to nurses. Nurses can play a role in entering into partnership with medical team and
bringing changes in maternal health services (Bernstein et al., 2017). However, lack of
managerial capacity and clear overall program objectives affected the outcome of the
programme (Popescu & Predescu, 2016). As this study gave a brief idea of several initiatives,
there is a need to review those studies that evaluates single maternal care policy initiatives to
get better idea about flaws in their program planning and delivery process.
Past research evidence has also highlighted the barriers to safe motherhood in India.
Reviewing this evidence and comparing it with the activities of different maternal care
programs would help to understand whether these barriers have been considered during
program planning and implementation or not. Maternal mortality is a negative indicator of
of post natal care or not. This makes detailed analysis of the safe motherhood programme
necessary.
The research paper by Vora et al. (2009) also described the reason behind poor
maternal health. The study revealed the impact of education and economic status of women
as the reason behind poor access to maternal care. Considering the causal effect of education
on maternal health outcome is vital, Weitzman (2017) revealed that increasing women’s level
of education can decrease the rate of short birth intervals, unwanted pregnancy and an
increase in the use of antenatal care. Hence, finding presented by Vora et al. (2009) is
significant as it highlights areas which have remained neglected in maternal health
improvement initiative in India. It also specified limitations of the SAFE motherhood
program as giving more priority to immunization and antenatal care affected emergency
services. This occurred because fixed day scheduling of work lead to more focus on routine
preventive task and ignorance of emergency services. Overall, the analysis of the study
findings revealed that maternal care programs were implemented to strengthen the delivery of
care to nurses. Nurses can play a role in entering into partnership with medical team and
bringing changes in maternal health services (Bernstein et al., 2017). However, lack of
managerial capacity and clear overall program objectives affected the outcome of the
programme (Popescu & Predescu, 2016). As this study gave a brief idea of several initiatives,
there is a need to review those studies that evaluates single maternal care policy initiatives to
get better idea about flaws in their program planning and delivery process.
Past research evidence has also highlighted the barriers to safe motherhood in India.
Reviewing this evidence and comparing it with the activities of different maternal care
programs would help to understand whether these barriers have been considered during
program planning and implementation or not. Maternal mortality is a negative indicator of
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
women’s status of India and as India’s current level remains unacceptable, Singh et al. (2009)
aimed to highlight current status about maternal health in India and highlight trends related to
the gap in access to maternal health services. The study revealed the decline in fertility has
reduced risk of maternal death. However, it is far away from the Millennium Development
Goal of reducing the MMR by three-quarters in 2015 compared to 1990 (Travasso, 2015).
This was explained because of the impact of socioeconomic and cultural variations on the
access to care. This link was observed by sharp decline in maternal mortality rate in northern
and southern states of India. For example, northern states like Assam accounted for two-third
of all maternal deaths in India, whereas southern states contribute to only 10% of the maternal
death. This difference in MMR was also attributed to difference in educational attainment of
women in north and south Indian states. In addition, poverty was also found to increase the
likelihood of maternal death because of women’s inability to obtain prenatal and delivery
care. This is consistent with the research by Wickham, Barr and Taylor-Robinson (2016)
which proved that moving into poverty increase the odds of maternal psychological distress
and behavioral problems in children. Singh et al. (2009) also revealed that unplanned
childbearing and high-risk birth related to maternal age is a factor contributing to high MMR.
Hence, this evidence suggest that socio-economic variables plays a vital role in women’s
access to maternal care and utilizing maternal health programs to educate women about the
importance of prenatal care and referral to appropriate facilities during labor is important. The
effectiveness of programs like JSY (Janani Suraksha Yojana)and NRHM (National Rural
Health Mission) particularly in increasing institutional delivery particularly in states like
Uttar Pradesh and Bihar needs to be monitored.
The significance of the research by Aggarwal, Kumar and Kumar (2003) is that it
highlighted the challenges faced by pregnant women living in hilly terrains of India. This
research was done after finding high incidence of neonatal deaths compared to infant deaths
aimed to highlight current status about maternal health in India and highlight trends related to
the gap in access to maternal health services. The study revealed the decline in fertility has
reduced risk of maternal death. However, it is far away from the Millennium Development
Goal of reducing the MMR by three-quarters in 2015 compared to 1990 (Travasso, 2015).
This was explained because of the impact of socioeconomic and cultural variations on the
access to care. This link was observed by sharp decline in maternal mortality rate in northern
and southern states of India. For example, northern states like Assam accounted for two-third
of all maternal deaths in India, whereas southern states contribute to only 10% of the maternal
death. This difference in MMR was also attributed to difference in educational attainment of
women in north and south Indian states. In addition, poverty was also found to increase the
likelihood of maternal death because of women’s inability to obtain prenatal and delivery
care. This is consistent with the research by Wickham, Barr and Taylor-Robinson (2016)
which proved that moving into poverty increase the odds of maternal psychological distress
and behavioral problems in children. Singh et al. (2009) also revealed that unplanned
childbearing and high-risk birth related to maternal age is a factor contributing to high MMR.
Hence, this evidence suggest that socio-economic variables plays a vital role in women’s
access to maternal care and utilizing maternal health programs to educate women about the
importance of prenatal care and referral to appropriate facilities during labor is important. The
effectiveness of programs like JSY (Janani Suraksha Yojana)and NRHM (National Rural
Health Mission) particularly in increasing institutional delivery particularly in states like
Uttar Pradesh and Bihar needs to be monitored.
The significance of the research by Aggarwal, Kumar and Kumar (2003) is that it
highlighted the challenges faced by pregnant women living in hilly terrains of India. This
research was done after finding high incidence of neonatal deaths compared to infant deaths
in India. This also brings the question whether obstetricians in India are not skilled enough to
recognize and manage neonatal complication. By the investigation of early neonatal deaths
and cause of such deaths in four districts of Himachal Pradesh, it was found that in 84% of
infant related death cases, there was no health facility in the village and the government based
hospital was accessible at more than 2-hours in 49% cases. Another significant finding was
that about 87% of the participants had to use foot to come to travel by foot to access road and
access transport options like bus and motorized transport. Another vital finding was that in all
neonatal death cases, only 4% cases were found where health care providers warned pregnant
women regarding the possibility of complications during the delivery or the post-partum
period. This evidence indicates that rural and district areas in India lack appropriate facilities
to take care of premature babies. It also reflected lack of experience of health care
professionals in dealing with complications. This evidence provides guidance to find out
whether maternal health programmes in India have considered the issue of neonatal death and
distance issues during delivery of maternal care service or not. Hence, the gaps and
challenges found in relation to maternal delivery trends in India suggest the need to critically
evaluate individual programs and find out whether they have been effectively implemented to
address diverse concerns related to access to maternal deaths.
Aim and objectives:
The main aim of the research is to conduct a systematic review of research literature and
critically evaluate impact of policies on infant and maternal health in India. By obtaining
relevant articles related to the research aim, the main objectives of this research are as
follows:
To analyze policies implemented in India associated with improving maternal and
infant health and the promotion of maternal care
recognize and manage neonatal complication. By the investigation of early neonatal deaths
and cause of such deaths in four districts of Himachal Pradesh, it was found that in 84% of
infant related death cases, there was no health facility in the village and the government based
hospital was accessible at more than 2-hours in 49% cases. Another significant finding was
that about 87% of the participants had to use foot to come to travel by foot to access road and
access transport options like bus and motorized transport. Another vital finding was that in all
neonatal death cases, only 4% cases were found where health care providers warned pregnant
women regarding the possibility of complications during the delivery or the post-partum
period. This evidence indicates that rural and district areas in India lack appropriate facilities
to take care of premature babies. It also reflected lack of experience of health care
professionals in dealing with complications. This evidence provides guidance to find out
whether maternal health programmes in India have considered the issue of neonatal death and
distance issues during delivery of maternal care service or not. Hence, the gaps and
challenges found in relation to maternal delivery trends in India suggest the need to critically
evaluate individual programs and find out whether they have been effectively implemented to
address diverse concerns related to access to maternal deaths.
Aim and objectives:
The main aim of the research is to conduct a systematic review of research literature and
critically evaluate impact of policies on infant and maternal health in India. By obtaining
relevant articles related to the research aim, the main objectives of this research are as
follows:
To analyze policies implemented in India associated with improving maternal and
infant health and the promotion of maternal care
To evaluate outcomes of each policy in relation to maternal health parameters like
reduction in MMR, rate of institutional delivery, access of antenatal services and early
recognition of complications
To analyze the credibility of research papers in terms of methodological rigor and
consideration of biases in study
To critically reflect on the strength and weakness of the policies and the method of
implementation
To find out gaps in current policy initiative implemented to improve maternal health
To recommend future actions to fulfill unmet needs of pregnant women in India
Methodology:
Research design:
A systematic review methodology was undertaken as part of the research design which
is relevant to the purpose of research as it provides credible evidence on the effectiveness of
maternal health polices in India. A systematic review involves a rigorous process of
assessment of research studies and evaluates the effectiveness of treatment on targeted
populations. By bringing together results of separate studies related to the research question,
systematic reviews can give an insight into the overall effectiveness of the intervention
(Boland, Cherry & Dickson, 2017). Another advantage of taking systematic approach as a
method of investigation is that is the most reliable source of evidence, and can be used to
guide clinical practice and implement evidence based care (Petticrew, 2015). Hence, policy
makers and health care administrators are provided with the opportunity to identify the best
steps needed to achieve reduction in MMR and apply the evidence to enhance the maternal
health status of women in India.
reduction in MMR, rate of institutional delivery, access of antenatal services and early
recognition of complications
To analyze the credibility of research papers in terms of methodological rigor and
consideration of biases in study
To critically reflect on the strength and weakness of the policies and the method of
implementation
To find out gaps in current policy initiative implemented to improve maternal health
To recommend future actions to fulfill unmet needs of pregnant women in India
Methodology:
Research design:
A systematic review methodology was undertaken as part of the research design which
is relevant to the purpose of research as it provides credible evidence on the effectiveness of
maternal health polices in India. A systematic review involves a rigorous process of
assessment of research studies and evaluates the effectiveness of treatment on targeted
populations. By bringing together results of separate studies related to the research question,
systematic reviews can give an insight into the overall effectiveness of the intervention
(Boland, Cherry & Dickson, 2017). Another advantage of taking systematic approach as a
method of investigation is that is the most reliable source of evidence, and can be used to
guide clinical practice and implement evidence based care (Petticrew, 2015). Hence, policy
makers and health care administrators are provided with the opportunity to identify the best
steps needed to achieve reduction in MMR and apply the evidence to enhance the maternal
health status of women in India.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
To retrieve articles the evaluating the impact of different policies on maternal health
in India, the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-
Analyses) guidelines has been followed to conduct the systematic review. The PRISMA
checklist is an evidence based protocol to report about different studies and interventions.
There are 26 items contained within the PRISMA checklist which need to be included in each
section such as introduction, method, results and discussion. It is a well-described protocol
that facilitates development of a robust systematic review. Following a validated research
protocol also increases the transparency of the research process and the reliability of the data
obtained (Moher et al., 2015). For this reason, PRISMA guideline has been followed to
strengthen the methodological quality and reliability of completed systematic review.
Search strategy:
The search for article has been done by first developing eligibility criteria for the
inclusion of research papers. The advantage of framing the eligibility criteria is that it allows
for screening of research articles based on certain criteria and boundaries. The inclusion and
exclusion criteria for selecting research papers related to the research question were as
follows:
Intervention: Only those articles were included in the systematic review which investigated
policy or policies related to maternal and infant health in India. These could include maternal
health program or initiatives implemented by the Indian Government.
Population: Research papers which focused on Indian women, new born and/or infants were
included in the systematic review.
Context or setting: Articles must investigate policies that have been implemented in health
care setting or states of India.
in India, the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-
Analyses) guidelines has been followed to conduct the systematic review. The PRISMA
checklist is an evidence based protocol to report about different studies and interventions.
There are 26 items contained within the PRISMA checklist which need to be included in each
section such as introduction, method, results and discussion. It is a well-described protocol
that facilitates development of a robust systematic review. Following a validated research
protocol also increases the transparency of the research process and the reliability of the data
obtained (Moher et al., 2015). For this reason, PRISMA guideline has been followed to
strengthen the methodological quality and reliability of completed systematic review.
Search strategy:
The search for article has been done by first developing eligibility criteria for the
inclusion of research papers. The advantage of framing the eligibility criteria is that it allows
for screening of research articles based on certain criteria and boundaries. The inclusion and
exclusion criteria for selecting research papers related to the research question were as
follows:
Intervention: Only those articles were included in the systematic review which investigated
policy or policies related to maternal and infant health in India. These could include maternal
health program or initiatives implemented by the Indian Government.
Population: Research papers which focused on Indian women, new born and/or infants were
included in the systematic review.
Context or setting: Articles must investigate policies that have been implemented in health
care setting or states of India.
Publication: Only those research papers were included which has been published between the
year 2008 to 2018.
Language: Only research papers that were published in English were included in the review
Type of research design: The selection of research papers were not restricted by any
particular research design. All research papers which were associated with the impact of
policies on maternal health in India were included.
According to the PRISMA checklist, the next phase after framing the research
question is to give overview of all information sources from where articles will be retrieved.
To find research articles that can address the research question, it was decided to access those
databases that publish research in the field of health and bioscience. With this perspective,
databases such as MEDLINE, CINAHL and PubMed were used to search for relevant
articles. The main rationale for including databases is that all refer to high quality search
articles that have been published in peer reviewed journals from across the world (McCall,
2014). Hence, papers were retrieved from the above mentioned databases. The search strategy
is a comprehensive process and the success of the search process depends on use of
appropriate search terms and search strategy for individual databases (Gough, Oliver &
Thomas, 2017). The keywords that were used in the search across all three databases included
‘maternal health policy’, ‘maternal health in India’ and ‘maternity policy in India’. Apart
from these search terms and search phrases, certain search limits such as language and
publication date was applied to ensure that eligible research papers are retrieved.
As per the PRISMA protocol for reporting about systematic reviews, this section also
provided comprehensive detail regarding search strategy for conducting search in CINAHL
database. The main advantage of conducting search in CINAHL is that it has both basic and
advanced search options (Wright, Golder & Lewis-Light, 2015). Hence, when articles cannot
year 2008 to 2018.
Language: Only research papers that were published in English were included in the review
Type of research design: The selection of research papers were not restricted by any
particular research design. All research papers which were associated with the impact of
policies on maternal health in India were included.
According to the PRISMA checklist, the next phase after framing the research
question is to give overview of all information sources from where articles will be retrieved.
To find research articles that can address the research question, it was decided to access those
databases that publish research in the field of health and bioscience. With this perspective,
databases such as MEDLINE, CINAHL and PubMed were used to search for relevant
articles. The main rationale for including databases is that all refer to high quality search
articles that have been published in peer reviewed journals from across the world (McCall,
2014). Hence, papers were retrieved from the above mentioned databases. The search strategy
is a comprehensive process and the success of the search process depends on use of
appropriate search terms and search strategy for individual databases (Gough, Oliver &
Thomas, 2017). The keywords that were used in the search across all three databases included
‘maternal health policy’, ‘maternal health in India’ and ‘maternity policy in India’. Apart
from these search terms and search phrases, certain search limits such as language and
publication date was applied to ensure that eligible research papers are retrieved.
As per the PRISMA protocol for reporting about systematic reviews, this section also
provided comprehensive detail regarding search strategy for conducting search in CINAHL
database. The main advantage of conducting search in CINAHL is that it has both basic and
advanced search options (Wright, Golder & Lewis-Light, 2015). Hence, when articles cannot
be retrieved by the use of primary search terms or phrases mentioned above, the advanced
search option was used to conduct paper search. The main feature of advanced search filter in
CINAHL database is that boolean operators like ‘AND’ and ‘OR’ can be applied to make the
research process more explicit. Karimi et al. (2014) explains that the information seeking task
requires boolean search methods and it can improve the overall search performance. It also
increases the credibility of the work as oolean retrieval method divides a search space on the
basis of eligibility criteria and combining string of keywords with Boolean operators
enhanced the proficiency of the search process (McGowan et al., 2016). The key words were
developed after identification of primary search terms and using thesaurus to identify words
with similar meanings. This helped to develop many important search terms for the review.
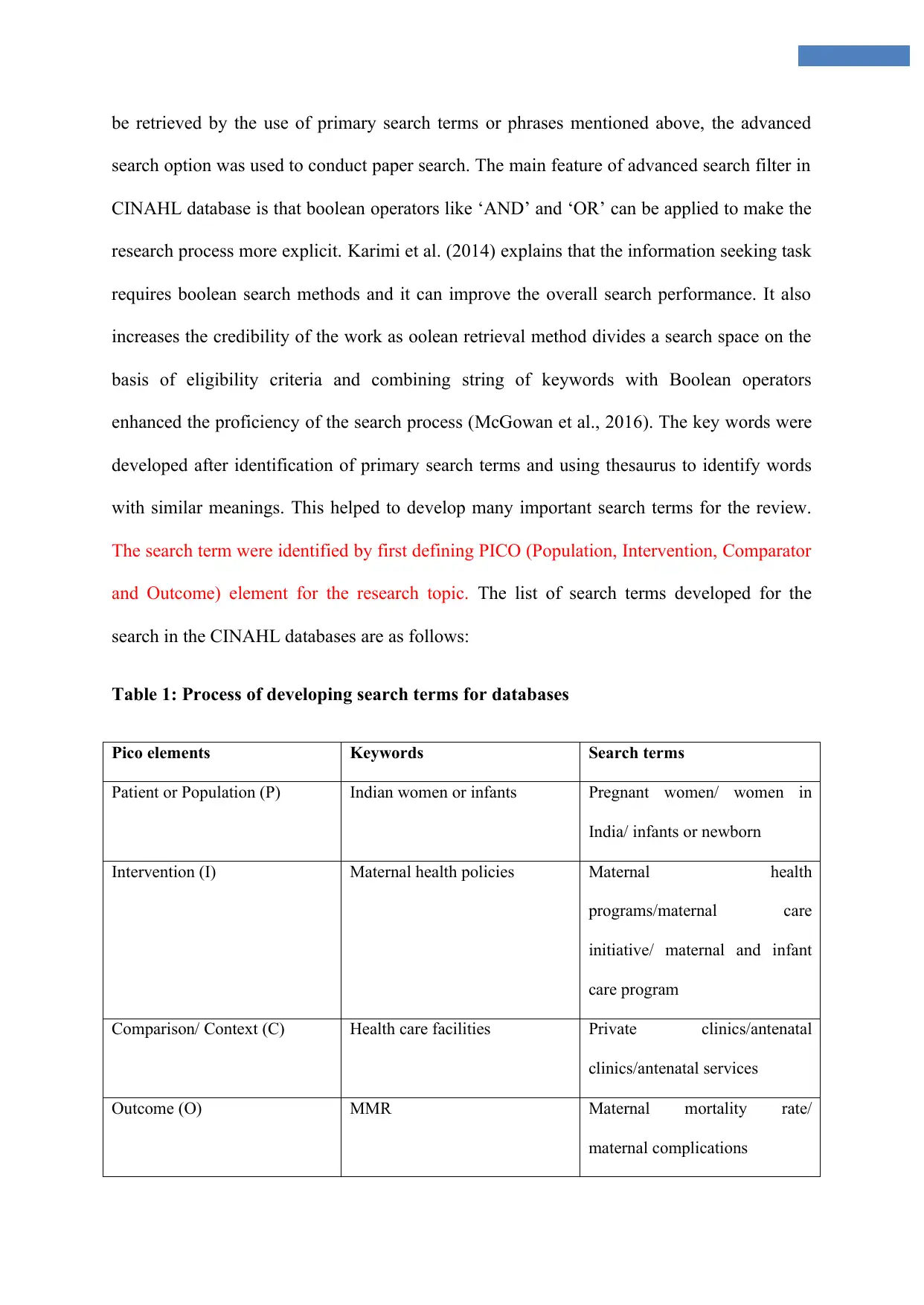
The search term were identified by first defining PICO (Population, Intervention, Comparator
and Outcome) element for the research topic. The list of search terms developed for the
search in the CINAHL databases are as follows:
Table 1: Process of developing search terms for databases
Pico elements Keywords Search terms
Patient or Population (P) Indian women or infants Pregnant women/ women in
India/ infants or newborn
Intervention (I) Maternal health policies Maternal health
programs/maternal care
initiative/ maternal and infant
care program
Comparison/ Context (C) Health care facilities Private clinics/antenatal
clinics/antenatal services
Outcome (O) MMR Maternal mortality rate/
maternal complications
search option was used to conduct paper search. The main feature of advanced search filter in
CINAHL database is that boolean operators like ‘AND’ and ‘OR’ can be applied to make the
research process more explicit. Karimi et al. (2014) explains that the information seeking task
requires boolean search methods and it can improve the overall search performance. It also
increases the credibility of the work as oolean retrieval method divides a search space on the
basis of eligibility criteria and combining string of keywords with Boolean operators
enhanced the proficiency of the search process (McGowan et al., 2016). The key words were
developed after identification of primary search terms and using thesaurus to identify words
with similar meanings. This helped to develop many important search terms for the review.
The search term were identified by first defining PICO (Population, Intervention, Comparator
and Outcome) element for the research topic. The list of search terms developed for the
search in the CINAHL databases are as follows:
Table 1: Process of developing search terms for databases
Pico elements Keywords Search terms
Patient or Population (P) Indian women or infants Pregnant women/ women in
India/ infants or newborn
Intervention (I) Maternal health policies Maternal health
programs/maternal care
initiative/ maternal and infant
care program
Comparison/ Context (C) Health care facilities Private clinics/antenatal
clinics/antenatal services
Outcome (O) MMR Maternal mortality rate/
maternal complications
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
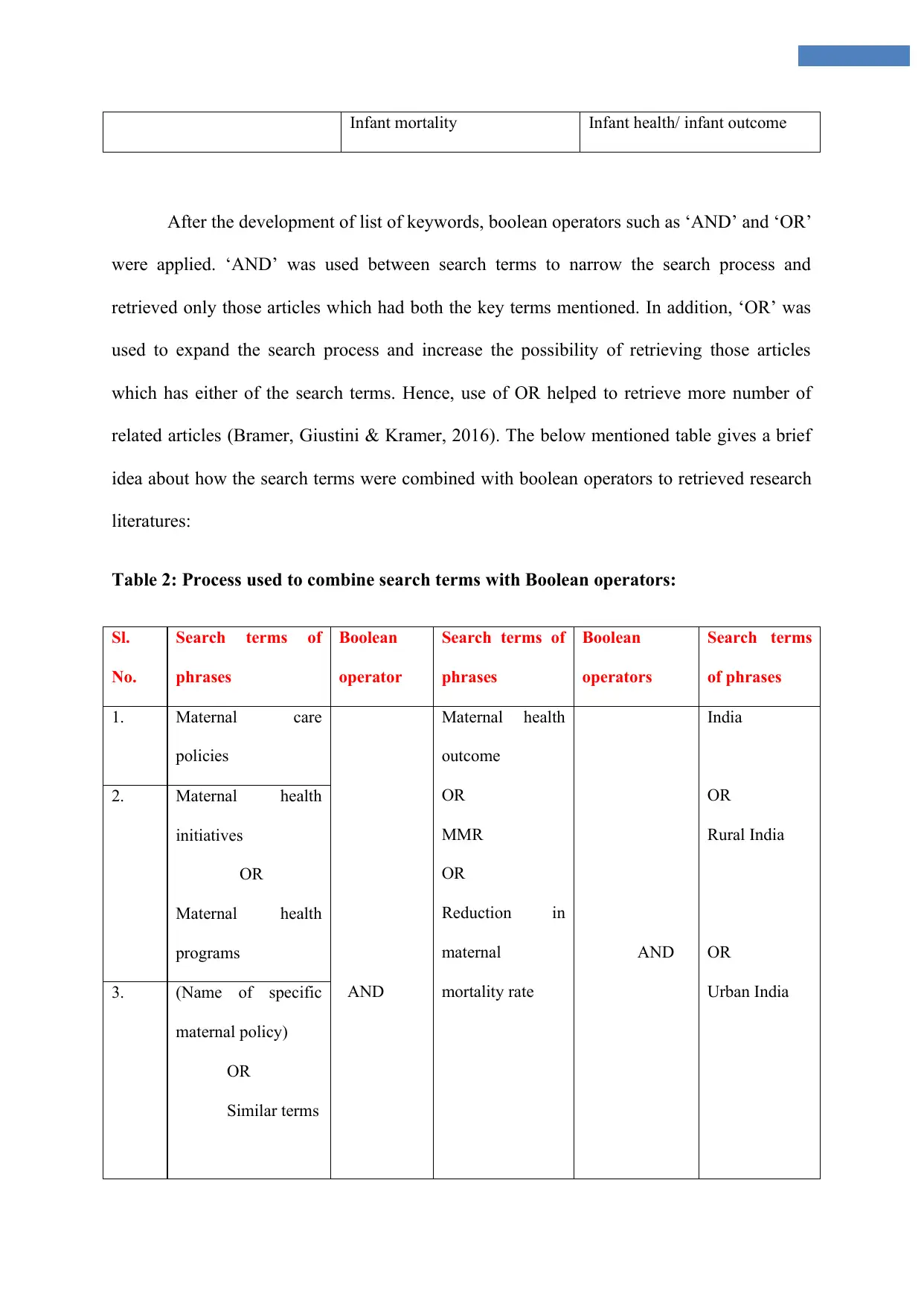
Infant mortality Infant health/ infant outcome
After the development of list of keywords, boolean operators such as ‘AND’ and ‘OR’
were applied. ‘AND’ was used between search terms to narrow the search process and
retrieved only those articles which had both the key terms mentioned. In addition, ‘OR’ was
used to expand the search process and increase the possibility of retrieving those articles
which has either of the search terms. Hence, use of OR helped to retrieve more number of
related articles (Bramer, Giustini & Kramer, 2016). The below mentioned table gives a brief
idea about how the search terms were combined with boolean operators to retrieved research
literatures:
Table 2: Process used to combine search terms with Boolean operators:
Sl.
No.
Search terms of
phrases
Boolean
operator
Search terms of
phrases
Boolean
operators
Search terms
of phrases
1. Maternal care
policies
AND
Maternal health
outcome
OR
MMR
OR
Reduction in
maternal
mortality rate
AND
India
OR
Rural India
OR
Urban India
2. Maternal health
initiatives
OR
Maternal health
programs
3. (Name of specific
maternal policy)
OR
Similar terms
After the development of list of keywords, boolean operators such as ‘AND’ and ‘OR’
were applied. ‘AND’ was used between search terms to narrow the search process and
retrieved only those articles which had both the key terms mentioned. In addition, ‘OR’ was
used to expand the search process and increase the possibility of retrieving those articles
which has either of the search terms. Hence, use of OR helped to retrieve more number of
related articles (Bramer, Giustini & Kramer, 2016). The below mentioned table gives a brief
idea about how the search terms were combined with boolean operators to retrieved research
literatures:
Table 2: Process used to combine search terms with Boolean operators:
Sl.
No.
Search terms of
phrases
Boolean
operator
Search terms of
phrases
Boolean
operators
Search terms
of phrases
1. Maternal care
policies
AND
Maternal health
outcome
OR
MMR
OR
Reduction in
maternal
mortality rate
AND
India
OR
Rural India
OR
Urban India
2. Maternal health
initiatives
OR
Maternal health
programs
3. (Name of specific
maternal policy)
OR
Similar terms
Data collection:
The final set of research papers were selected based on rigorous process of
identification, screening, eligibility and inclusion of research papers in the study. The
identification of an article was accomplished by entering search terms and screening articles
based on inclusion and exclusion criteria. The initial strategy during the eligibility phase was
to review the title and abstract of the articles (Shamseer et al., 2015). To further confirm the
relevance of the selected research papers, the full text article of the paper was analyzed to
identify the full detail of outcomes of policy outcomes are discussed or whether only
descriptive overview was provided. This process helped to confirm the final list of research
papers that would be included in the systematic review. The number of records obtained after
the database searching, the number of articles screened and number of articles assessed for
eligibility are provided in the PRISMA flow diagram (Appendix 2). The main advantage of
using a PRISMA flow diagram is that it can give a quick overview of the number of papers
which were initially identified and the number of articles finally selected for the review based
on the search process (Stewart et al., 2015). The format for the PRISMA flow diagram which
is used in the results section is given in Appendix 1.
Data extraction is also the most vital part of a systematic review and approach taken
to highlight the most important part of research paper makes the research presentation clear
and useful (Moons et al., 2014). For the purpose of this systematic review, the following
items have been summarized in the data extraction table (Appendix III):
Author and year
Research aim
Policy discussed
The final set of research papers were selected based on rigorous process of
identification, screening, eligibility and inclusion of research papers in the study. The
identification of an article was accomplished by entering search terms and screening articles
based on inclusion and exclusion criteria. The initial strategy during the eligibility phase was
to review the title and abstract of the articles (Shamseer et al., 2015). To further confirm the
relevance of the selected research papers, the full text article of the paper was analyzed to
identify the full detail of outcomes of policy outcomes are discussed or whether only
descriptive overview was provided. This process helped to confirm the final list of research
papers that would be included in the systematic review. The number of records obtained after
the database searching, the number of articles screened and number of articles assessed for
eligibility are provided in the PRISMA flow diagram (Appendix 2). The main advantage of
using a PRISMA flow diagram is that it can give a quick overview of the number of papers
which were initially identified and the number of articles finally selected for the review based
on the search process (Stewart et al., 2015). The format for the PRISMA flow diagram which
is used in the results section is given in Appendix 1.
Data extraction is also the most vital part of a systematic review and approach taken
to highlight the most important part of research paper makes the research presentation clear
and useful (Moons et al., 2014). For the purpose of this systematic review, the following
items have been summarized in the data extraction table (Appendix III):
Author and year
Research aim
Policy discussed
Outcome of the policy
Strength and weakness
Implications of the work
By going through the summary table, brief idea regarding the important elements presented in
a single study can be understood.
Data analysis:
As this research aims to identify the role of maternal policies on child and maternal
health India, it is evident that the systematic review is being done to evaluate changes found
in the maternal health care system in India post policy implementation. Hence, thematic
analysis has been undertaken as a method of analysis as this would help to identify common
themes from qualitative data and use them to identify or interpret experiences of perceptions
related to participation in a phenomenon (Braun, Clarke & Terry, 2014). As quality is also
important to confirm the credibility and reliability of the work, the critical appraisal was done
by review of considerations to reduce bias in studies, methodological rigor, sample size and
recruitment process. This process helped to categorize whether the research is of high, low or
medium quality.
Results:
Based on the use of key words to search for literatures in the three databases, a total of
105 articles were identified. Out of these research articles, the 15 articles were removed as
they were duplicates or almost similar studies. The remaining 80 articles were screened as per
the inclusion and exclusion criteria. Based on the review of full-text articles, 8 were found
suitable for inclusion in the study. The screening and reporting process has been conducted
based on PRISMA guideline and the PRISMA diagram for the screening and eligibility
Strength and weakness
Implications of the work
By going through the summary table, brief idea regarding the important elements presented in
a single study can be understood.
Data analysis:
As this research aims to identify the role of maternal policies on child and maternal
health India, it is evident that the systematic review is being done to evaluate changes found
in the maternal health care system in India post policy implementation. Hence, thematic
analysis has been undertaken as a method of analysis as this would help to identify common
themes from qualitative data and use them to identify or interpret experiences of perceptions
related to participation in a phenomenon (Braun, Clarke & Terry, 2014). As quality is also
important to confirm the credibility and reliability of the work, the critical appraisal was done
by review of considerations to reduce bias in studies, methodological rigor, sample size and
recruitment process. This process helped to categorize whether the research is of high, low or
medium quality.
Results:
Based on the use of key words to search for literatures in the three databases, a total of
105 articles were identified. Out of these research articles, the 15 articles were removed as
they were duplicates or almost similar studies. The remaining 80 articles were screened as per
the inclusion and exclusion criteria. Based on the review of full-text articles, 8 were found
suitable for inclusion in the study. The screening and reporting process has been conducted
based on PRISMA guideline and the PRISMA diagram for the screening and eligibility
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
process can be found in Appendix II.
Figure 1: PRISMA flow chart for the search process
Different research methods were used in the 8 articles selected for the research
analysis process. Two papers were descriptive observational study. Retrospective analysis by
means of mixed method study and several quantitative analysis method was also implemented
to gain idea about the impact of different policies on maternal health. The key policies or
government based initiatives that has been analyzed in the eight papers include NRHM
(National Rural Health MIssion), ICDS (Integrated Child Development Scheme) and JSY
(Janani Suraksha Yojana). A brief overview of each paper is given in appendix III.
The systematic review and analysis of research papers gave rise to fouee themes.
These themes are relevant to the research objectives and highlight the role of maternal health
policy on MMR, rate of institutional delivery, access of antenatal services and early
recognition of complications. The thematic analysis also gives an insight into the strength and
weakness of each policy in terms of impact and method of implementation.
Theme 1: Impact of maternal policies on institutional delivery rate and MMR:
Out of eight articles, there were four articles that reported on the impact of maternal
policies on institutional child delivery rate. Papers 1, 2, 3 and 8 reported on the stable
increase of institutional delivery rates post the implementation of JSY scheme in India.
Papers by (Gupta et al. 2012) Paper 1 and (Khan, Hazra and Bhatnagar 2010) paper discussed
the impact of JSY particularly in the state of Madhya Pradesh and rural Uttar Pradesh
respectively. However, paper 2 gave an insight into impact of rate of institutional delivery
and maternal maternity rate across India. Paper 3 finding is considered a high quality
Figure 1: PRISMA flow chart for the search process
Different research methods were used in the 8 articles selected for the research
analysis process. Two papers were descriptive observational study. Retrospective analysis by
means of mixed method study and several quantitative analysis method was also implemented
to gain idea about the impact of different policies on maternal health. The key policies or
government based initiatives that has been analyzed in the eight papers include NRHM
(National Rural Health MIssion), ICDS (Integrated Child Development Scheme) and JSY
(Janani Suraksha Yojana). A brief overview of each paper is given in appendix III.
The systematic review and analysis of research papers gave rise to fouee themes.
These themes are relevant to the research objectives and highlight the role of maternal health
policy on MMR, rate of institutional delivery, access of antenatal services and early
recognition of complications. The thematic analysis also gives an insight into the strength and
weakness of each policy in terms of impact and method of implementation.
Theme 1: Impact of maternal policies on institutional delivery rate and MMR:
Out of eight articles, there were four articles that reported on the impact of maternal
policies on institutional child delivery rate. Papers 1, 2, 3 and 8 reported on the stable
increase of institutional delivery rates post the implementation of JSY scheme in India.
Papers by (Gupta et al. 2012) Paper 1 and (Khan, Hazra and Bhatnagar 2010) paper discussed
the impact of JSY particularly in the state of Madhya Pradesh and rural Uttar Pradesh
respectively. However, paper 2 gave an insight into impact of rate of institutional delivery
and maternal maternity rate across India. Paper 3 finding is considered a high quality
evidence retrospective cohort based study which looked at increasing the reliability of the
program evaluation process (Campbell & Stanley, 2015). Cohort based study are more
generalizable as it give an overview of the state of maternal health in all types of region. The
common findings from the paper 1 and paper 2 is that both studies highlighted t the same
gaps in JSY scheme suggesting that the program focused too much on increasing institution
delivery. However, no steps were taken to upgrade antenatal care. It revealed lack of skills of
professional in increasing awareness about maternal health. The strength of paper 3 is that by
showing positive effect of incorporating counseling element in the JSY program, Khan, Hazra
and Bhatnagar (2010) revealed that JSY has the potential to improve other behaviors such as
early breastfeeding, post natal care, timely referral and delivery by skilled personnel. The
gives implication for upgrading infrastructural arrangements so that ASHA (Accredited
Social Health Activist) program could visit home of women and provide necessary education
to prevent infant death (Bills et al., 2018).
Theme 2: Impact of maternal policies on reducing financial stress in families:
Maternal health policies in India mainly targeted improving the rate of hospital
delivery so that pregnancy complications and poor antenatal outcomes could be avoided.
There were two papers that specifically targeted the reduction of financial barriers to maternal
health in India. Paper 4 (Angadi, Davalgi and Raghavendra 2017) highlighted about the role
of several maternity benefit schemes like Madilu Yojana, Thayi Bhagya schemes and
Prasuthi Araike Yojana schemes on improving financial and geographical access to quality
care for poor women. Working on this issue was important because Vail et al. (2018)
revealed structural barriers such as poverty and logistical barriers such as inadequate labour
facilities and human resource shortage as some of the cause behind poor maternal and infant
health outcomes. Paper 4 revealed JSY as to be the service with the highest utilization rate
and the main determinants of such high utilization rate included literacy of mothers, husband
program evaluation process (Campbell & Stanley, 2015). Cohort based study are more
generalizable as it give an overview of the state of maternal health in all types of region. The
common findings from the paper 1 and paper 2 is that both studies highlighted t the same
gaps in JSY scheme suggesting that the program focused too much on increasing institution
delivery. However, no steps were taken to upgrade antenatal care. It revealed lack of skills of
professional in increasing awareness about maternal health. The strength of paper 3 is that by
showing positive effect of incorporating counseling element in the JSY program, Khan, Hazra
and Bhatnagar (2010) revealed that JSY has the potential to improve other behaviors such as
early breastfeeding, post natal care, timely referral and delivery by skilled personnel. The
gives implication for upgrading infrastructural arrangements so that ASHA (Accredited
Social Health Activist) program could visit home of women and provide necessary education
to prevent infant death (Bills et al., 2018).
Theme 2: Impact of maternal policies on reducing financial stress in families:
Maternal health policies in India mainly targeted improving the rate of hospital
delivery so that pregnancy complications and poor antenatal outcomes could be avoided.
There were two papers that specifically targeted the reduction of financial barriers to maternal
health in India. Paper 4 (Angadi, Davalgi and Raghavendra 2017) highlighted about the role
of several maternity benefit schemes like Madilu Yojana, Thayi Bhagya schemes and
Prasuthi Araike Yojana schemes on improving financial and geographical access to quality
care for poor women. Working on this issue was important because Vail et al. (2018)
revealed structural barriers such as poverty and logistical barriers such as inadequate labour
facilities and human resource shortage as some of the cause behind poor maternal and infant
health outcomes. Paper 4 revealed JSY as to be the service with the highest utilization rate
and the main determinants of such high utilization rate included literacy of mothers, husband
and families and belonging to above poverty line. In addition, there were also groups which
did not utilized the services and major reason behind non-utilization was lack of awareness
about scheme. Hence, the paper 4 was able to highlight the gap in the cash incentive scheme
which was that the program could not reach out to desired audience. To achieve the MDG
target, it was necessary to focus on socioeconomic barriers to antenatal care and visits. Paper
5 by Sidneyet al. (2012) highlighted about the strength or weakness of the implementation
process. For example, JSY was found to provide cash benefits on a timely basis. However,
the possibility of introducing home visit to educate women was identified.
Theme 3: Impact of policies on reducing inequities in maternal care
There were two papers that reported about reducing inequities in maternal care. This
included paper 7 (Rao and Kaul 2018) and 8 (Vellakkal et al. 2017). Paper 7 indicates about
impact ICDS scheme on addressing equity issues in maternal care. The main advantage of
ICDS was that it particularly targeted the problem of malnutrition and poor learning
outcomes in children below 5 years. The study reported positive development of the ICDS
scheme on increasing supplementary food provisions in infant. However, challenges in the
implementation of the program suggested need for reforming the implementation process.
The paper 8 is significant as it particular aimed to evaluated NRHM on reducing inequities in
maternal health. Women from low socioeconomic background living in deprived Indian states
were targeted. The significance of the research methodology is that all types of index of
inequality such as maternal age, rural-urban and caste was considered. The benefit of NRHM
was seen by means of increase in uptake of institutional delivery. Hence, the study revealed
that by increasing coverage of maternal care programs, inequity related issues can be
addressed. However, some discrepancy in NRHM scheme is that inter-state variations were
found because of difference in quality of health services and skills of ASHAs in each village.
These factors need to be considered in future.
did not utilized the services and major reason behind non-utilization was lack of awareness
about scheme. Hence, the paper 4 was able to highlight the gap in the cash incentive scheme
which was that the program could not reach out to desired audience. To achieve the MDG
target, it was necessary to focus on socioeconomic barriers to antenatal care and visits. Paper
5 by Sidneyet al. (2012) highlighted about the strength or weakness of the implementation
process. For example, JSY was found to provide cash benefits on a timely basis. However,
the possibility of introducing home visit to educate women was identified.
Theme 3: Impact of policies on reducing inequities in maternal care
There were two papers that reported about reducing inequities in maternal care. This
included paper 7 (Rao and Kaul 2018) and 8 (Vellakkal et al. 2017). Paper 7 indicates about
impact ICDS scheme on addressing equity issues in maternal care. The main advantage of
ICDS was that it particularly targeted the problem of malnutrition and poor learning
outcomes in children below 5 years. The study reported positive development of the ICDS
scheme on increasing supplementary food provisions in infant. However, challenges in the
implementation of the program suggested need for reforming the implementation process.
The paper 8 is significant as it particular aimed to evaluated NRHM on reducing inequities in
maternal health. Women from low socioeconomic background living in deprived Indian states
were targeted. The significance of the research methodology is that all types of index of
inequality such as maternal age, rural-urban and caste was considered. The benefit of NRHM
was seen by means of increase in uptake of institutional delivery. Hence, the study revealed
that by increasing coverage of maternal care programs, inequity related issues can be
addressed. However, some discrepancy in NRHM scheme is that inter-state variations were
found because of difference in quality of health services and skills of ASHAs in each village.
These factors need to be considered in future.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Theme 4: Impact on access to antenatal care in India
The paper 1, 2, 3 and 8 highlighted about the role of maternal policy and initiatives on
increasing access to antenatal care. These improvements were achieved by motivating people
to join the program through cash benefit schemes and integration of services in rural areas.
This indicates the application of health belief model of changes as people’s belief and
thinking related to antenatal care was changed by means of cash incentives (Skinner, Tiro &
Champion, 2015). However, wider impact could not be achieved as vital aspects such as
increasing knowledge and awareness was ignored.
Discussion:
Upon conducting a systematic review of scholar literature, with the aim of assessing
the effects of different policies on maternal and infant health in India, four primary themes
namely, (1) Impact of maternal policies on institutional delivery rate and MMR, (2) Impact of
maternal policies on reducing financial stress in families, (3) Impact of policies on reducing
inequities in maternal care, and (4) Impact on access to antenatal care in India, were
identified. It was found that recent advancements have been made in order to improve
different quality aspects of maternal health in the public healthcare system of India. This
chapter will present a detailed discussion of the identified articles and correlate them with
other relevant findings in order to draw inferences related to the research question.
Policy implementation
The research by Gupta et al. (2012) elaborated on the fact that the implementation of
the Janani Suraksha Yojana (JSY) was effective in increasing the rates of institutional
deliveries by an estimated 42.6% among those that belong to poor socioeconomic status. The
results demonstrated the fact that pregnancy in the initial stages creates great risk to mothers.
The paper 1, 2, 3 and 8 highlighted about the role of maternal policy and initiatives on
increasing access to antenatal care. These improvements were achieved by motivating people
to join the program through cash benefit schemes and integration of services in rural areas.
This indicates the application of health belief model of changes as people’s belief and
thinking related to antenatal care was changed by means of cash incentives (Skinner, Tiro &
Champion, 2015). However, wider impact could not be achieved as vital aspects such as
increasing knowledge and awareness was ignored.
Discussion:
Upon conducting a systematic review of scholar literature, with the aim of assessing
the effects of different policies on maternal and infant health in India, four primary themes
namely, (1) Impact of maternal policies on institutional delivery rate and MMR, (2) Impact of
maternal policies on reducing financial stress in families, (3) Impact of policies on reducing
inequities in maternal care, and (4) Impact on access to antenatal care in India, were
identified. It was found that recent advancements have been made in order to improve
different quality aspects of maternal health in the public healthcare system of India. This
chapter will present a detailed discussion of the identified articles and correlate them with
other relevant findings in order to draw inferences related to the research question.
Policy implementation
The research by Gupta et al. (2012) elaborated on the fact that the implementation of
the Janani Suraksha Yojana (JSY) was effective in increasing the rates of institutional
deliveries by an estimated 42.6% among those that belong to poor socioeconomic status. The
results demonstrated the fact that pregnancy in the initial stages creates great risk to mothers.
As a result, an increase in institutional deliveries were found among the females belonging to
the particular early age group resulting in substantial reduction in the maternal mortality ratio
and accomplishment of Millennium Development Goal 5. These findings were consistent
with research conducted by Randive, San Sebastian, De Costa and Lindholm (2014) who
stated that although there exists an inequality in the access to appropriate institutional
delivery services, the JSY has the potential of reducing rates of such inequity. As per the
research objective, the research by Gupta et al. (2012) has highlighted about the potential
benefits of the JSY scheme. By increasing institutional delivery rate and hospital attendance
among women, it can be interpreted that JSY has implemented strategies to reach those
population which earlier preferred home delivery. Hence, the provision of cash incentive
through the JSY scheme is the major contributor behind improved institutional delivery rate.
Similar type of cash incentive program was implemented in Nepal too and it revealed
correlation between women’s knowledge about the program and the increased institutional
delivery rate (Pandey, 2018). However, the findings related to increase in maternal mortality
rate shows that the trend is common among lower-middle class and more number of cases
became reported as more number of such families enrolled in hospital after being aware about
the JSY scheme.
The article by Guin, Sahu, Khare and Kavishwar (2012) significant as it reveals some
flaws in the JSY scheme. The evidence revealed that JSY was able to put undue pressure on
the rates of institutional deliveries, without creating provisions for earnest effort, with the aim
of promoting the prominence of adequate antenatal care in decreasing maternal rates of
morbidity and mortality. While there was an increase in the institutional delivery, pregnant
women were brought in a dilapidated state to the hospitals, and there was an upsurge in the
maternal mortality rates. This indicates lack of recruitment of trained and motivated
personnel as some drawback of the planning process. The findings give the implication to
the particular early age group resulting in substantial reduction in the maternal mortality ratio
and accomplishment of Millennium Development Goal 5. These findings were consistent
with research conducted by Randive, San Sebastian, De Costa and Lindholm (2014) who
stated that although there exists an inequality in the access to appropriate institutional
delivery services, the JSY has the potential of reducing rates of such inequity. As per the
research objective, the research by Gupta et al. (2012) has highlighted about the potential
benefits of the JSY scheme. By increasing institutional delivery rate and hospital attendance
among women, it can be interpreted that JSY has implemented strategies to reach those
population which earlier preferred home delivery. Hence, the provision of cash incentive
through the JSY scheme is the major contributor behind improved institutional delivery rate.
Similar type of cash incentive program was implemented in Nepal too and it revealed
correlation between women’s knowledge about the program and the increased institutional
delivery rate (Pandey, 2018). However, the findings related to increase in maternal mortality
rate shows that the trend is common among lower-middle class and more number of cases
became reported as more number of such families enrolled in hospital after being aware about
the JSY scheme.
The article by Guin, Sahu, Khare and Kavishwar (2012) significant as it reveals some
flaws in the JSY scheme. The evidence revealed that JSY was able to put undue pressure on
the rates of institutional deliveries, without creating provisions for earnest effort, with the aim
of promoting the prominence of adequate antenatal care in decreasing maternal rates of
morbidity and mortality. While there was an increase in the institutional delivery, pregnant
women were brought in a dilapidated state to the hospitals, and there was an upsurge in the
maternal mortality rates. This indicates lack of recruitment of trained and motivated
personnel as some drawback of the planning process. The findings give the implication to
remodel the JSY scheme to achieve the desired maternal health outcome.
However, Ng et al. (2014) presented results that did not confirm the association
between reduction in maternal mortality and implementation of JSY. Their research instead
illustrated that a significant improvement in the proportion of institutional deliveries in the
state of Madhya Pradesh (23.9% in 2005 vs. 55.9% in 2010). Further increase were also
observed in the proportion of institutional deliveries that were supported by JSY from 14% in
the year 2005 to 80% in 2010. Nonetheless, declines in MMR during this time period ranged
from 2% to 35%. Another article by Goudar et al. (2013) elaborated on the trends related to
institutional delivery, NMR (neonatal mortality), PMR (perinatal mortality) and risk factors
in India. The results indicated that there was a significant increase in the rates of institutional
deliveries from 2005-2009 of 92.6-96.1% in Belgaum, followed by 89.5-98.6% in Nagpur
with a confidence level of (p<0.0001). Furthermore, the trends also provided evidence for an
increase in the hospital rates from 63.4-71.0% (p=0.002), and 63.1-72.0% (p<0.0001),
respectively. Owing to the fact that significant elevations in institutional deliveries were
associated with decline in PMR from 41.3-34.6 (p=0.008), and in stillbirth from 22.5-16.3 in
Belgaum and 29.3-21.1 in Nagpur (p=0.002), the researchers were able to establish
effectiveness of institutional deliveries. It can be interpreted that the decline in PMR and
stillbirth was due to an increase in neonatal resuscitation and caesarean section rates. Increase
in hospital rates can be attributed to greater awareness and knowledge among the women on
institutional deliveries and their benefits, in relation to infant and maternal health.
Khan, Hazra and Bhatnagar (2010) conducted a research that elaborated on the effects
of Janani Suraksha Yojana. The findings presented in the article indicated that the fiscal
incentives related to JSY and non-incentivized facilities, were able to bring about a successful
contact between the client and the providers. This, in addition to ASHA counseling also
increased the fraction of females who obtained institutional delivery and three ANC (ante
However, Ng et al. (2014) presented results that did not confirm the association
between reduction in maternal mortality and implementation of JSY. Their research instead
illustrated that a significant improvement in the proportion of institutional deliveries in the
state of Madhya Pradesh (23.9% in 2005 vs. 55.9% in 2010). Further increase were also
observed in the proportion of institutional deliveries that were supported by JSY from 14% in
the year 2005 to 80% in 2010. Nonetheless, declines in MMR during this time period ranged
from 2% to 35%. Another article by Goudar et al. (2013) elaborated on the trends related to
institutional delivery, NMR (neonatal mortality), PMR (perinatal mortality) and risk factors
in India. The results indicated that there was a significant increase in the rates of institutional
deliveries from 2005-2009 of 92.6-96.1% in Belgaum, followed by 89.5-98.6% in Nagpur
with a confidence level of (p<0.0001). Furthermore, the trends also provided evidence for an
increase in the hospital rates from 63.4-71.0% (p=0.002), and 63.1-72.0% (p<0.0001),
respectively. Owing to the fact that significant elevations in institutional deliveries were
associated with decline in PMR from 41.3-34.6 (p=0.008), and in stillbirth from 22.5-16.3 in
Belgaum and 29.3-21.1 in Nagpur (p=0.002), the researchers were able to establish
effectiveness of institutional deliveries. It can be interpreted that the decline in PMR and
stillbirth was due to an increase in neonatal resuscitation and caesarean section rates. Increase
in hospital rates can be attributed to greater awareness and knowledge among the women on
institutional deliveries and their benefits, in relation to infant and maternal health.
Khan, Hazra and Bhatnagar (2010) conducted a research that elaborated on the effects
of Janani Suraksha Yojana. The findings presented in the article indicated that the fiscal
incentives related to JSY and non-incentivized facilities, were able to bring about a successful
contact between the client and the providers. This, in addition to ASHA counseling also
increased the fraction of females who obtained institutional delivery and three ANC (ante
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
natal) check-ups. The JSY practices which included the delivery of maternal and prenatal
advice and counseling that in turn, generated the implementation of healthy behaviors,
resulting in the improvement of both child and maternal health. Secondary data analysis from
District Level Household Survey (DLHS-3) conducted in 2007-2008 suggested that more
than half of the deliveries of India during the time frame occurred within the home (52%).
Financial burden
The out-of-pocket-expenditure (OOPE) for females being subjected to institutional
deliveries were high, with substantial variation between the union territories and the states.
The mean OOPE of normal delivery in private and public institution were an estimated Rs.
1,624 and Rs. 4,458, respectively. Corresponding rates for caesarean-section were
approximately Rs. 5,935 and Rs. 14,276, respectively. For illiterate and poor women, the
expenditures on caesarean sections were further than their capacity to pay, and subsequently
resulted in suggestively more borrowings. Hence, the study was able to establish significant
correlation between elevated wealth and literacy with an increased likelihood of institutional
deliveries, and greater OOPE, without significant variations in JSY usage (Modugu, Kumar,
Kumar & Millett, 2012). Thus, it can be stated that the OOPE burden was high among less
educated, low wealth index, and poor social group families. Data findings from a study
conducted in Ghana suggested that there had been a marginalised upsurge in the access and
utilisation of skilled delivery, antenatal and postnatal care services, after the implementation
of appropriate policies. This illustrated the effectiveness of exemption of user fees for the
maternal healthcare services, for the improvement of access to adequate care services (Ganle,
Parker, Fitzpatrick & Otupiri, 2014).
Coffey (2014) conducted a qualitative study on the influences of conditional transfer
of cash for birth in health facilities and provided evidence for the fact that that healthcare
advice and counseling that in turn, generated the implementation of healthy behaviors,
resulting in the improvement of both child and maternal health. Secondary data analysis from
District Level Household Survey (DLHS-3) conducted in 2007-2008 suggested that more
than half of the deliveries of India during the time frame occurred within the home (52%).
Financial burden
The out-of-pocket-expenditure (OOPE) for females being subjected to institutional
deliveries were high, with substantial variation between the union territories and the states.
The mean OOPE of normal delivery in private and public institution were an estimated Rs.
1,624 and Rs. 4,458, respectively. Corresponding rates for caesarean-section were
approximately Rs. 5,935 and Rs. 14,276, respectively. For illiterate and poor women, the
expenditures on caesarean sections were further than their capacity to pay, and subsequently
resulted in suggestively more borrowings. Hence, the study was able to establish significant
correlation between elevated wealth and literacy with an increased likelihood of institutional
deliveries, and greater OOPE, without significant variations in JSY usage (Modugu, Kumar,
Kumar & Millett, 2012). Thus, it can be stated that the OOPE burden was high among less
educated, low wealth index, and poor social group families. Data findings from a study
conducted in Ghana suggested that there had been a marginalised upsurge in the access and
utilisation of skilled delivery, antenatal and postnatal care services, after the implementation
of appropriate policies. This illustrated the effectiveness of exemption of user fees for the
maternal healthcare services, for the improvement of access to adequate care services (Ganle,
Parker, Fitzpatrick & Otupiri, 2014).
Coffey (2014) conducted a qualitative study on the influences of conditional transfer
of cash for birth in health facilities and provided evidence for the fact that that healthcare
service providers primarily place an emphasis on apprehending the economic rents allied with
the program, and deliver a tremendously poor quality of care. Further, the cash transfer
program does not eventually deliver beneficiaries a great net fiscal transfer during the time of
child birth. Hence, the value of the transmission to beneficiaries was found to be less due to
the hospital birth associated costs.
These findings were supported by additional evidence presented by Carvalho,
Thacker, Gupta and Salomon (2014) who suggested that financial support from JSY had an
increase in the immunization rates ranging from fluctuating from 3.1 % polio vaccination to
to 9.1% to completely vaccinated children. The findings were also able to provide proof of
the impacts of JSY on an elevation in the rates of post-partum check-up and initial
breastfeeding practices that were in use, during the time of childbirth. However, the research
indicated that JSY failed to exert a major impact on care-seeking behaviours and exclusive
breastfeeding practices. Sidney, Diwan, El-Khatib and De Costa (2012) suggested that an
estimated 76% of all deliveries (318/418) were found to occur within the JSY program, where
approximately 81% mothers were present below the poverty line. The results further stated
that 90% women had previous knowledge about the program. Most mothers reported getting
cash incentive within two weeks of child delivery. The influence of ASHA on the decisions
taken by the mothers regarding place of delivery was low. Increased susceptibility of
infection during delivery at homes was found among women who were illiterate and did not
have previous knowledge of the JSY package.
According to Powell-Jackson, Mazumdar and Mills (2015) also elaborated that that
fiscal incentives to females were related with augmented uptake of maternity facilities.
However, the authors failed to form a correlation between JSY and the decrease in early
neonatal or neonatal mortality. The positive impacts on utilisation were found to be larger for
less cultured and subordinate women, in homes where cash payment was more impactful.
the program, and deliver a tremendously poor quality of care. Further, the cash transfer
program does not eventually deliver beneficiaries a great net fiscal transfer during the time of
child birth. Hence, the value of the transmission to beneficiaries was found to be less due to
the hospital birth associated costs.
These findings were supported by additional evidence presented by Carvalho,
Thacker, Gupta and Salomon (2014) who suggested that financial support from JSY had an
increase in the immunization rates ranging from fluctuating from 3.1 % polio vaccination to
to 9.1% to completely vaccinated children. The findings were also able to provide proof of
the impacts of JSY on an elevation in the rates of post-partum check-up and initial
breastfeeding practices that were in use, during the time of childbirth. However, the research
indicated that JSY failed to exert a major impact on care-seeking behaviours and exclusive
breastfeeding practices. Sidney, Diwan, El-Khatib and De Costa (2012) suggested that an
estimated 76% of all deliveries (318/418) were found to occur within the JSY program, where
approximately 81% mothers were present below the poverty line. The results further stated
that 90% women had previous knowledge about the program. Most mothers reported getting
cash incentive within two weeks of child delivery. The influence of ASHA on the decisions
taken by the mothers regarding place of delivery was low. Increased susceptibility of
infection during delivery at homes was found among women who were illiterate and did not
have previous knowledge of the JSY package.
According to Powell-Jackson, Mazumdar and Mills (2015) also elaborated that that
fiscal incentives to females were related with augmented uptake of maternity facilities.
However, the authors failed to form a correlation between JSY and the decrease in early
neonatal or neonatal mortality. The positive impacts on utilisation were found to be larger for
less cultured and subordinate women, in homes where cash payment was more impactful.
These results were supported by another study that indicated that maternal referral at the time
of term delivery was related with greater odds of adverse birth outcomes (OR- 2.6, 95% CI:
1.0–6.6 p = 0.04) (Chaturvedi, Randive, Diwan & De Costa, 2014). Hence, cash payments
were allied with more utilization of maternity facilities among families that belonged to poor
socioeconomic background.
Upon conducting an exploration of the child and maternal health under the scheme of
the NRHM framework (National Rural Health Mission) it was found that the program makes
the participation of PRI members through village health, sanitation, and nutrition groups
mandatory, placing an emphasis on their participation in health based intervention at the
grassroots level. However, inadequate monitoring by the committee authorities were regarded
as a major barrier in monitoring the outcomes (Dwivedi, 2015). While the ASHA programme
did not direct towards HIV/AIDS, the CHW programmes (Community health workers) have
been highlighted as an important means of targeting the shortage of health resource in under-
developed countries, especially in association to HIV/AIDS (Scott & Shanker, 2010). This
helped in establishing the fact that ASHA is a key component of the NRHM initiative and
gains support by a noteworthy growth in government disbursement on public health (0.9%
GDP to 2-3%). Thus, it can be stated that ASHA has been able to create an awareness on
health and the associated social determinants, with the aim of mobilising the community
towards better utilisation of the health services.
The paper by Vellakkal et al. (2017) mainly gave an insight into the role of different
maternal and infant health programs in reducing inequity and quality issues in infant and
maternal care. Paper 7 by Rao and Kaul (2018) mainly gave idea regarding the impact of a
scheme that particularly targeted infant health. The policy discussed in the paper was ICDS
(Integrated Child Development Scheme). The ICDS scheme followed a life cycle approach to
promote early child development. Services related to nutrition and community education was
of term delivery was related with greater odds of adverse birth outcomes (OR- 2.6, 95% CI:
1.0–6.6 p = 0.04) (Chaturvedi, Randive, Diwan & De Costa, 2014). Hence, cash payments
were allied with more utilization of maternity facilities among families that belonged to poor
socioeconomic background.
Upon conducting an exploration of the child and maternal health under the scheme of
the NRHM framework (National Rural Health Mission) it was found that the program makes
the participation of PRI members through village health, sanitation, and nutrition groups
mandatory, placing an emphasis on their participation in health based intervention at the
grassroots level. However, inadequate monitoring by the committee authorities were regarded
as a major barrier in monitoring the outcomes (Dwivedi, 2015). While the ASHA programme
did not direct towards HIV/AIDS, the CHW programmes (Community health workers) have
been highlighted as an important means of targeting the shortage of health resource in under-
developed countries, especially in association to HIV/AIDS (Scott & Shanker, 2010). This
helped in establishing the fact that ASHA is a key component of the NRHM initiative and
gains support by a noteworthy growth in government disbursement on public health (0.9%
GDP to 2-3%). Thus, it can be stated that ASHA has been able to create an awareness on
health and the associated social determinants, with the aim of mobilising the community
towards better utilisation of the health services.
The paper by Vellakkal et al. (2017) mainly gave an insight into the role of different
maternal and infant health programs in reducing inequity and quality issues in infant and
maternal care. Paper 7 by Rao and Kaul (2018) mainly gave idea regarding the impact of a
scheme that particularly targeted infant health. The policy discussed in the paper was ICDS
(Integrated Child Development Scheme). The ICDS scheme followed a life cycle approach to
promote early child development. Services related to nutrition and community education was
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
provided. Since launch of the scheme in 1975, it was found that several restructuring initiavte
to the scheme was implemented in the past 40 years. The study revealed challenges in
achieving the objectives of the program because of the lack of health professionals to support
the scheme. In addition, Vellakkal et al. (2017) highlighted about reduction in inequities
through the NRHM program. The success was achieved because deprived population were
targeted. Working in this area was significant and it is consistent with other research paper as
conducted by Handa et al. (2016), who also revealed that poverty targeted schemes have the
potential to improve maternal health. This was supported by a separate investigation
regarding the impact of Zambia’s Child Grant Program on maternal health utilization. Hence,
on the whole deprived areas and population group were targeted to improve maternal and
infant health in India. However, lack of preparation to meet the objectives of various schemes
and poor implementation of the program affected ability to meet MDG (Millennium
Development Goals) targets compared to other countries.
Conclusion and recommendation:
By conducting systematic review of research literatures, the main aim of the paper
was to evaluate the impact maternal and infant health related policies on improving maternal
and infant health outcomes and indicators like MMR, access to care, quality of care and
reduction in complication rate. By the process of screening of articles, a total of 8 papers were
found to give answer to the research question. Furthermore, the review and critical analysis of
the 8 papers gave rise to four different themes which gave clear idea regarding the impact of
different policies on maternal health indicators. The four themes included 1) impact of
maternal policies on MMR and institutional delivery rate; 2) reducing financial barrier to
access; 3) addressing inequities in maternal care; and 4) improving access to antenatal care.
From the overall analysis of the eight papers, it can be concluded that the JSY scheme was a
to the scheme was implemented in the past 40 years. The study revealed challenges in
achieving the objectives of the program because of the lack of health professionals to support
the scheme. In addition, Vellakkal et al. (2017) highlighted about reduction in inequities
through the NRHM program. The success was achieved because deprived population were
targeted. Working in this area was significant and it is consistent with other research paper as
conducted by Handa et al. (2016), who also revealed that poverty targeted schemes have the
potential to improve maternal health. This was supported by a separate investigation
regarding the impact of Zambia’s Child Grant Program on maternal health utilization. Hence,
on the whole deprived areas and population group were targeted to improve maternal and
infant health in India. However, lack of preparation to meet the objectives of various schemes
and poor implementation of the program affected ability to meet MDG (Millennium
Development Goals) targets compared to other countries.
Conclusion and recommendation:
By conducting systematic review of research literatures, the main aim of the paper
was to evaluate the impact maternal and infant health related policies on improving maternal
and infant health outcomes and indicators like MMR, access to care, quality of care and
reduction in complication rate. By the process of screening of articles, a total of 8 papers were
found to give answer to the research question. Furthermore, the review and critical analysis of
the 8 papers gave rise to four different themes which gave clear idea regarding the impact of
different policies on maternal health indicators. The four themes included 1) impact of
maternal policies on MMR and institutional delivery rate; 2) reducing financial barrier to
access; 3) addressing inequities in maternal care; and 4) improving access to antenatal care.
From the overall analysis of the eight papers, it can be concluded that the JSY scheme was a
useful scheme that aimed to reduce MMR and pregnancy complication by avoiding. Offering
cash incentives to deprived women was taken as a strategy to bring women to health care
institutions for delivery. However, the review of observation studies like that of Gupta et al.
(2012) revealed this could address behaviours like uptake of post-natal care, however it could
not address the service gap that was present before the pregnancy. Hence, instead of focusing
on structural barriers to institutional delivery, the JSY stakeholders should have worked to
focus on strategies to address cultural and geographical barriers in care. For example, the
problem highlighted by Khan, Hazra and Bhatnagar (2010) was that quality antenatal care
was not achieved because many women gained access to antenatal care in the last week of
pregnancy. However, to identify risk and complication, there was a need to implement
process to increase attendance in antenatal services from the beginning.
From the review of papers that particularly examine the impact of JSY scheme, it can
be concluded that increasing uptake of institutional deliveries alone do not determine
maternal health outcomes. The gaps and limitations in the implementation process revealed
the need to assess the readiness of facilities in rural areas to provide quality care.
Furthermore, training needs was also found as success of counseling and awareness will
depend on communication and negotiation skills of health care workers. In addition, review
of child development scheme like ICDS gave the implication that the program was not
prepared to deal with diversity of the Indian population which affected the goal of achieving
equitable provision of services. Furthermore, many initiatives implemented under NRHM
revealed improvement in outcome related to MMR. However, lot needs to be done still now
to deal with cultural challenges like family preference for antenatal care, educational
attainment of husband and attitude of women towards positive pregnancy outcomes. Hence, it
is recommended that maternal health policy should go beyond institutional delivery and it
should to address issues like malaria and tuberculosis in patient. It is also recommended to
cash incentives to deprived women was taken as a strategy to bring women to health care
institutions for delivery. However, the review of observation studies like that of Gupta et al.
(2012) revealed this could address behaviours like uptake of post-natal care, however it could
not address the service gap that was present before the pregnancy. Hence, instead of focusing
on structural barriers to institutional delivery, the JSY stakeholders should have worked to
focus on strategies to address cultural and geographical barriers in care. For example, the
problem highlighted by Khan, Hazra and Bhatnagar (2010) was that quality antenatal care
was not achieved because many women gained access to antenatal care in the last week of
pregnancy. However, to identify risk and complication, there was a need to implement
process to increase attendance in antenatal services from the beginning.
From the review of papers that particularly examine the impact of JSY scheme, it can
be concluded that increasing uptake of institutional deliveries alone do not determine
maternal health outcomes. The gaps and limitations in the implementation process revealed
the need to assess the readiness of facilities in rural areas to provide quality care.
Furthermore, training needs was also found as success of counseling and awareness will
depend on communication and negotiation skills of health care workers. In addition, review
of child development scheme like ICDS gave the implication that the program was not
prepared to deal with diversity of the Indian population which affected the goal of achieving
equitable provision of services. Furthermore, many initiatives implemented under NRHM
revealed improvement in outcome related to MMR. However, lot needs to be done still now
to deal with cultural challenges like family preference for antenatal care, educational
attainment of husband and attitude of women towards positive pregnancy outcomes. Hence, it
is recommended that maternal health policy should go beyond institutional delivery and it
should to address issues like malaria and tuberculosis in patient. It is also recommended to
develop a comprehensive maternal health package that gives women idea about signs of good
pregnancy outcome, types of services available and importance of good quality antenatal
care. Language and cultural consideration must also be addressed while planning educational
activities for at risk women population in India.
References:
Aggarwal, A. K., Kumar, R., & Kumar, P. (2003). early neonatal mortality in a hilly north
Indian state: Sociodemographic factors and treatment seeking behavior. Indian
Journal of Preventive and Social Medicine, 34(1&2), 46-52. Retrieved from:
http://medind.nic.in/ibl/t03/i1/iblt03i1p46o.pdf
Angadi, N., Davalgi, S., & Raghavendra, S. K. (2017). Determinants of utilization of
maternity benefit schemes among mothers in urban slums of Davangere city,
Karnataka, India. International Journal of Community Medicine and Public
Health, 3(3), 651-657. DOI: http://dx.doi.org/10.18203/2394-6040.ijcmph20160627
Bernstein, P. S., Martin, J. N., Barton, J. R., Shields, L. E., Druzin, M. L., Scavone, B. M., ...
& Tsigas, E. Z. (2017). National partnership for maternal safety: consensus bundle on
severe hypertension during pregnancy and the postpartum period. Anesthesia &
Analgesia, 125(2), 540-547. DOI: 10.1213/ANE.0000000000002304
Bills, C. B., Newberry, J. A., Darmstadt, G., Pirrotta, E. A., Rao, G. R., Mahadevan, S. V., &
Strehlow, M. C. (2018). Reducing early infant mortality in India: results of a
pregnancy outcome, types of services available and importance of good quality antenatal
care. Language and cultural consideration must also be addressed while planning educational
activities for at risk women population in India.
References:
Aggarwal, A. K., Kumar, R., & Kumar, P. (2003). early neonatal mortality in a hilly north
Indian state: Sociodemographic factors and treatment seeking behavior. Indian
Journal of Preventive and Social Medicine, 34(1&2), 46-52. Retrieved from:
http://medind.nic.in/ibl/t03/i1/iblt03i1p46o.pdf
Angadi, N., Davalgi, S., & Raghavendra, S. K. (2017). Determinants of utilization of
maternity benefit schemes among mothers in urban slums of Davangere city,
Karnataka, India. International Journal of Community Medicine and Public
Health, 3(3), 651-657. DOI: http://dx.doi.org/10.18203/2394-6040.ijcmph20160627
Bernstein, P. S., Martin, J. N., Barton, J. R., Shields, L. E., Druzin, M. L., Scavone, B. M., ...
& Tsigas, E. Z. (2017). National partnership for maternal safety: consensus bundle on
severe hypertension during pregnancy and the postpartum period. Anesthesia &
Analgesia, 125(2), 540-547. DOI: 10.1213/ANE.0000000000002304
Bills, C. B., Newberry, J. A., Darmstadt, G., Pirrotta, E. A., Rao, G. R., Mahadevan, S. V., &
Strehlow, M. C. (2018). Reducing early infant mortality in India: results of a
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
prospective cohort of pregnant women using emergency medical services. BMJ
open, 8(4), e019937, http://dx.doi.org/10.1136/bmjopen-2017-019937
Boland, A., Cherry, G., & Dickson, R. (Eds.). (2017). Doing a systematic review: A student's
guide. Sage. Retrieved from: https://books.google.co.in/books?
hl=en&lr=&id=Zpc3DwAAQBAJ&oi=fnd&pg=PP1&dq=Doing+a+systematic+revie
w:+A+student%27s+guide.
+&ots=KhFd3BIPz4&sig=KThiycXtk3saRSGSNz8BxoSu6-U
Bramer, W. M., Giustini, D., & Kramer, B. M. (2016). Comparing the coverage, recall, and
precision of searches for 120 systematic reviews in Embase, MEDLINE, and Google
Scholar: a prospective study. Systematic reviews, 5(1), 39.
Braun, V., Clarke, V., & Terry, G. (2014). Thematic analysis. Qual Res Clin Health
Psychol, 24, 95-114.
Campbell, D. T., & Stanley, J. C. (2015). Experimental and quasi-experimental designs for
research. Ravenio Books.
Dwivedi, P. (2015). Assessment of Maternal and Child Health under the NRHM frame work
A Study of four Districts of UP Bahraich Balrampur Varanasi and Lucknow.
Retrieved from:
http://shodhganga.inflibnet.ac.in/bitstream/10603/47000/13/summary.pdf
Goudar, S. S., Goco, N., Somannavar, M. S., Vernekar, S. S., Mallapur, A. A., Moore, J.
L., ... & Koso-Thomas, M. (2015). Institutional deliveries and perinatal and neonatal
mortality in Southern and Central India. Reproductive health, 12(2), S13.
https://doi.org/10.1186/1742-4755-12-S2-S13
Gough, D., Oliver, S., & Thomas, J. (Eds.). (2017). An introduction to systematic reviews.
open, 8(4), e019937, http://dx.doi.org/10.1136/bmjopen-2017-019937
Boland, A., Cherry, G., & Dickson, R. (Eds.). (2017). Doing a systematic review: A student's
guide. Sage. Retrieved from: https://books.google.co.in/books?
hl=en&lr=&id=Zpc3DwAAQBAJ&oi=fnd&pg=PP1&dq=Doing+a+systematic+revie
w:+A+student%27s+guide.
+&ots=KhFd3BIPz4&sig=KThiycXtk3saRSGSNz8BxoSu6-U
Bramer, W. M., Giustini, D., & Kramer, B. M. (2016). Comparing the coverage, recall, and
precision of searches for 120 systematic reviews in Embase, MEDLINE, and Google
Scholar: a prospective study. Systematic reviews, 5(1), 39.
Braun, V., Clarke, V., & Terry, G. (2014). Thematic analysis. Qual Res Clin Health
Psychol, 24, 95-114.
Campbell, D. T., & Stanley, J. C. (2015). Experimental and quasi-experimental designs for
research. Ravenio Books.
Dwivedi, P. (2015). Assessment of Maternal and Child Health under the NRHM frame work
A Study of four Districts of UP Bahraich Balrampur Varanasi and Lucknow.
Retrieved from:
http://shodhganga.inflibnet.ac.in/bitstream/10603/47000/13/summary.pdf
Goudar, S. S., Goco, N., Somannavar, M. S., Vernekar, S. S., Mallapur, A. A., Moore, J.
L., ... & Koso-Thomas, M. (2015). Institutional deliveries and perinatal and neonatal
mortality in Southern and Central India. Reproductive health, 12(2), S13.
https://doi.org/10.1186/1742-4755-12-S2-S13
Gough, D., Oliver, S., & Thomas, J. (Eds.). (2017). An introduction to systematic reviews.
Sage.
Guin, G., Sahu, B., Khare, S., & Kavishwar, A. (2012). Trends in Maternal Mortality and
Impact of Janani Suraksha Yojana (JSY) on Maternal Mortality Ratio in a Tertiary
Referral Hospital. Journal of Obstetrics and Gynaecology of India, 62(3), 307–311.
http://doi.org/10.1007/s13224-012-0221-1
Gupta, S. K., Pal, D. K., Tiwari, R., Garg, R., Shrivastava, A. K., Sarawagi, R., … Lahariya,
C. (2012). Impact of Janani Suraksha Yojana on Institutional Delivery Rate and
Maternal Morbidity and Mortality: An Observational Study in India. Journal of
Health, Population, and Nutrition, 30(4), 464–471. doi: 10.3402/gha.v7.24939.
Handa, S., Peterman, A., Seidenfeld, D., & Tembo, G. (2016). Income transfers and maternal
health: evidence from a national randomized social cash transfer program in
Zambia. Health economics, 25(2), 225-236. https://doi.org/10.1002/hec.3136
Joshi, S. (2013, June). Maternal and child health in India: what is the role of policy?.
In International Affairs Forum (Vol. 4, No. 1, pp. 40-44). Routledge.
https://doi.org/10.1080/23258020.2013.824235
Karimi, S., Pohl, S., Scholer, F., Cavedon, L., & Zobel, J. (2010). Boolean versus ranked
querying for biomedical systematic reviews. BMC Medical Informatics and Decision
Making, 10, 58. http://doi.org/10.1186/1472-6947-10-58
Khan, M. E., Hazra, A., & Bhatnagar, I. (2010). Impact of Janani Suraksha Yojana on
selected family health behaviors in rural Uttar Pradesh. J Fam Welf, 56(Special Issue),
9-22. Retrieved from: http://medind.nic.in/jah/t10/s1/jaht10s1p9.pdf
McCall, M. C. (2014). In search of yoga: Research trends in a western medical
database. International journal of yoga, 7(1), 4.
Guin, G., Sahu, B., Khare, S., & Kavishwar, A. (2012). Trends in Maternal Mortality and
Impact of Janani Suraksha Yojana (JSY) on Maternal Mortality Ratio in a Tertiary
Referral Hospital. Journal of Obstetrics and Gynaecology of India, 62(3), 307–311.
http://doi.org/10.1007/s13224-012-0221-1
Gupta, S. K., Pal, D. K., Tiwari, R., Garg, R., Shrivastava, A. K., Sarawagi, R., … Lahariya,
C. (2012). Impact of Janani Suraksha Yojana on Institutional Delivery Rate and
Maternal Morbidity and Mortality: An Observational Study in India. Journal of
Health, Population, and Nutrition, 30(4), 464–471. doi: 10.3402/gha.v7.24939.
Handa, S., Peterman, A., Seidenfeld, D., & Tembo, G. (2016). Income transfers and maternal
health: evidence from a national randomized social cash transfer program in
Zambia. Health economics, 25(2), 225-236. https://doi.org/10.1002/hec.3136
Joshi, S. (2013, June). Maternal and child health in India: what is the role of policy?.
In International Affairs Forum (Vol. 4, No. 1, pp. 40-44). Routledge.
https://doi.org/10.1080/23258020.2013.824235
Karimi, S., Pohl, S., Scholer, F., Cavedon, L., & Zobel, J. (2010). Boolean versus ranked
querying for biomedical systematic reviews. BMC Medical Informatics and Decision
Making, 10, 58. http://doi.org/10.1186/1472-6947-10-58
Khan, M. E., Hazra, A., & Bhatnagar, I. (2010). Impact of Janani Suraksha Yojana on
selected family health behaviors in rural Uttar Pradesh. J Fam Welf, 56(Special Issue),
9-22. Retrieved from: http://medind.nic.in/jah/t10/s1/jaht10s1p9.pdf
McCall, M. C. (2014). In search of yoga: Research trends in a western medical
database. International journal of yoga, 7(1), 4.
McGowan, J., Sampson, M., Salzwedel, D. M., Cogo, E., Foerster, V., & Lefebvre, C. (2016).
PRESS peer review of electronic search strategies: 2015 guideline statement. Journal
of clinical epidemiology, 75, 40-46.
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., ... & Stewart, L.
A. (2015). Preferred reporting items for systematic review and meta-analysis
protocols (PRISMA-P) 2015 statement. Systematic reviews, 4(1), 1.
https://doi.org/10.1186/2046-4053-4-1
Moons, K. G., de Groot, J. A., Bouwmeester, W., Vergouwe, Y., Mallett, S., Altman, D.
G., ... & Collins, G. S. (2014). Critical appraisal and data extraction for systematic
reviews of prediction modelling studies: the CHARMS checklist. PLoS
medicine, 11(10), e1001744.
Mousumi, G. (2015). Pregnancy complications and birth outcome: do health care services
make a difference. Int Res J Soc Sci, 4(3), 27-35. Retrieved from:
http://www.isca.in/IJSS/Archive/v4/i3/5.ISCA-IRJSS-2014-297.pdf
Nair, H., & Panda, R. (2011). Quality of maternal healthcare in India: Has the National Rural
Health Mission made a difference? Journal of Global Health, 1(1), 79–86. Retrieved
from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3484741/
O'Neil, S., Naeve, K., & Ved, R. (2017). An Examination of the Maternal Health Quality of
Care Landscape in India (No. b4ac5292bf6148798f37782c2920844e). Mathematica
Policy Research. Retrieved from:
https://www.macfound.org/media/files/50268_Landscape_Report_2017.03.02.pdf
Petticrew, M. (2015). Time to rethink the systematic review catechism? Moving from ‘what
works’ to ‘what happens’. Systematic reviews, 4(1), 36.
PRESS peer review of electronic search strategies: 2015 guideline statement. Journal
of clinical epidemiology, 75, 40-46.
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., ... & Stewart, L.
A. (2015). Preferred reporting items for systematic review and meta-analysis
protocols (PRISMA-P) 2015 statement. Systematic reviews, 4(1), 1.
https://doi.org/10.1186/2046-4053-4-1
Moons, K. G., de Groot, J. A., Bouwmeester, W., Vergouwe, Y., Mallett, S., Altman, D.
G., ... & Collins, G. S. (2014). Critical appraisal and data extraction for systematic
reviews of prediction modelling studies: the CHARMS checklist. PLoS
medicine, 11(10), e1001744.
Mousumi, G. (2015). Pregnancy complications and birth outcome: do health care services
make a difference. Int Res J Soc Sci, 4(3), 27-35. Retrieved from:
http://www.isca.in/IJSS/Archive/v4/i3/5.ISCA-IRJSS-2014-297.pdf
Nair, H., & Panda, R. (2011). Quality of maternal healthcare in India: Has the National Rural
Health Mission made a difference? Journal of Global Health, 1(1), 79–86. Retrieved
from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3484741/
O'Neil, S., Naeve, K., & Ved, R. (2017). An Examination of the Maternal Health Quality of
Care Landscape in India (No. b4ac5292bf6148798f37782c2920844e). Mathematica
Policy Research. Retrieved from:
https://www.macfound.org/media/files/50268_Landscape_Report_2017.03.02.pdf
Petticrew, M. (2015). Time to rethink the systematic review catechism? Moving from ‘what
works’ to ‘what happens’. Systematic reviews, 4(1), 36.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
https://doi.org/10.1186/s13643-015-0027-1
Popescu, G. H., & Predescu, V. (2016). The role of leadership in public health. American
Journal of Medical Research, 3(1), 273. Retrieved from:
https://www.ceeol.com/search/article-detail?id=649324
Ram Jat, T. (2014). Maternal health and health care in Madhya Pradesh state of India: an
exploration using a human rights lens (Doctoral dissertation, Umeå universitet).
Retrieved from: http://www.diva-portal.org/smash/record.jsf?
pid=diva2%3A761328&dswid=mainwindow
Rao, N., & Kaul, V. (2018). India's integrated child development services scheme: challenges
for scaling up. Child: care, health and development, 44(1), 31-40.
https://doi.org/10.1111/cch.12531
Sankar, M. J., Neogi, S. B., Sharma, J., Chauhan, M., Srivastava, R., Prabhakar, P. K., …
Paul, V. K. (2016). State of newborn health in India. Journal of
Perinatology, 36(Suppl 3), S3–S8. http://doi.org/10.1038/jp.2016.183
Shamseer, L., Moher, D., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., ... & Stewart, L.
A. (2015). Preferred reporting items for systematic review and meta-analysis
protocols (PRISMA-P) 2015: elaboration and explanation. Bmj, 349, g7647.
Sidney, K., Diwan, V., El-Khatib, Z., & De Costa, A. (2012). India's JSY cash transfer
program for maternal health: Who participates and who doesn't-a report from Ujjain
district. Reproductive health, 9(1), 2. doi: 10.1186/1742-4755-9-2
Singh, S., Remez, L., Ram, U., Moore, A. M., & Audam, S. (2009). Barriers to safe
motherhood in India. New York: Guttmacher Institute, 1-35.
Popescu, G. H., & Predescu, V. (2016). The role of leadership in public health. American
Journal of Medical Research, 3(1), 273. Retrieved from:
https://www.ceeol.com/search/article-detail?id=649324
Ram Jat, T. (2014). Maternal health and health care in Madhya Pradesh state of India: an
exploration using a human rights lens (Doctoral dissertation, Umeå universitet).
Retrieved from: http://www.diva-portal.org/smash/record.jsf?
pid=diva2%3A761328&dswid=mainwindow
Rao, N., & Kaul, V. (2018). India's integrated child development services scheme: challenges
for scaling up. Child: care, health and development, 44(1), 31-40.
https://doi.org/10.1111/cch.12531
Sankar, M. J., Neogi, S. B., Sharma, J., Chauhan, M., Srivastava, R., Prabhakar, P. K., …
Paul, V. K. (2016). State of newborn health in India. Journal of
Perinatology, 36(Suppl 3), S3–S8. http://doi.org/10.1038/jp.2016.183
Shamseer, L., Moher, D., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., ... & Stewart, L.
A. (2015). Preferred reporting items for systematic review and meta-analysis
protocols (PRISMA-P) 2015: elaboration and explanation. Bmj, 349, g7647.
Sidney, K., Diwan, V., El-Khatib, Z., & De Costa, A. (2012). India's JSY cash transfer
program for maternal health: Who participates and who doesn't-a report from Ujjain
district. Reproductive health, 9(1), 2. doi: 10.1186/1742-4755-9-2
Singh, S., Remez, L., Ram, U., Moore, A. M., & Audam, S. (2009). Barriers to safe
motherhood in India. New York: Guttmacher Institute, 1-35.
Skinner, C. S., Tiro, J., & Champion, V. L. (2015). The health belief model. Health behavior:
theory, research, and practice. 5th ed. San Francisco (US): Jossey-Bass, 75-94.
Stewart, L. A., Clarke, M., Rovers, M., Riley, R. D., Simmonds, M., Stewart, G., & Tierney,
J. F. (2015). Preferred reporting items for a systematic review and meta-analysis of
individual participant data: the PRISMA-IPD statement. Jama, 313(16), 1657-1665.
Travasso, C. (2015). India is set to meet target on reducing maternal mortality.
doi: https://doi.org/10.1136/bmj.h724
Vail, B., Morgan, M. C., Dyer, J., Christmas, A., Cohen, S. R., Joshi, M., ... & Walker, D. M.
(2018). Logistical, cultural, and structural barriers to immediate neonatal care and
neonatal resuscitation in Bihar, India. BMC pregnancy and childbirth, 18(1), 385.
https://doi.org/10.1186/s12884-018-2017-5
Vellakkal, S., Gupta, A., Khan, Z., Stuckler, D., Reeves, A., Ebrahim, S., … Doyle, P.
(2017). Has India’s national rural health mission reduced inequities in maternal health
services? A pre-post repeated cross-sectional study. Health Policy and
Planning, 32(1), 79–90. http://doi.org/10.1093/heapol/czw100
Vora, K. S., Mavalankar, D. V., Ramani, K. V., Upadhyaya, M., Sharma, B., Iyengar, S., …
Iyengar, K. (2009). Maternal Health Situation in India: A Case Study. Journal of
Health, Population, and Nutrition, 27(2), 184–201.
Weitzman, A. (2017). The effects of women's education on maternal health: Evidence from
Peru. Social Science & Medicine, 180, 1-9.
Wickham, S., Barr, B., & Taylor-Robinson, D. (2016). Impact of moving into poverty on
maternal and child mental health: longitudinal analysis of the Millennium Cohort
Study. The Lancet, 388, S4.
theory, research, and practice. 5th ed. San Francisco (US): Jossey-Bass, 75-94.
Stewart, L. A., Clarke, M., Rovers, M., Riley, R. D., Simmonds, M., Stewart, G., & Tierney,
J. F. (2015). Preferred reporting items for a systematic review and meta-analysis of
individual participant data: the PRISMA-IPD statement. Jama, 313(16), 1657-1665.
Travasso, C. (2015). India is set to meet target on reducing maternal mortality.
doi: https://doi.org/10.1136/bmj.h724
Vail, B., Morgan, M. C., Dyer, J., Christmas, A., Cohen, S. R., Joshi, M., ... & Walker, D. M.
(2018). Logistical, cultural, and structural barriers to immediate neonatal care and
neonatal resuscitation in Bihar, India. BMC pregnancy and childbirth, 18(1), 385.
https://doi.org/10.1186/s12884-018-2017-5
Vellakkal, S., Gupta, A., Khan, Z., Stuckler, D., Reeves, A., Ebrahim, S., … Doyle, P.
(2017). Has India’s national rural health mission reduced inequities in maternal health
services? A pre-post repeated cross-sectional study. Health Policy and
Planning, 32(1), 79–90. http://doi.org/10.1093/heapol/czw100
Vora, K. S., Mavalankar, D. V., Ramani, K. V., Upadhyaya, M., Sharma, B., Iyengar, S., …
Iyengar, K. (2009). Maternal Health Situation in India: A Case Study. Journal of
Health, Population, and Nutrition, 27(2), 184–201.
Weitzman, A. (2017). The effects of women's education on maternal health: Evidence from
Peru. Social Science & Medicine, 180, 1-9.
Wickham, S., Barr, B., & Taylor-Robinson, D. (2016). Impact of moving into poverty on
maternal and child mental health: longitudinal analysis of the Millennium Cohort
Study. The Lancet, 388, S4.
World Health Organization. (2013). WHO recommendations on postnatal care of the mother
and newborn. Retrieved from:
http://www.who.int/maternal_child_adolescent/documents/postnatal-care-
recommendations/en/
Wright, K., Golder, S., & Lewis-Light, K. (2015). What value is the CINAHL database when
searching for systematic reviews of qualitative studies?. Systematic reviews, 4(1), 104.
and newborn. Retrieved from:
http://www.who.int/maternal_child_adolescent/documents/postnatal-care-
recommendations/en/
Wright, K., Golder, S., & Lewis-Light, K. (2015). What value is the CINAHL database when
searching for systematic reviews of qualitative studies?. Systematic reviews, 4(1), 104.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Appendix:
I. The PRISMA flow diagram for selection of research papers:
II. PRISMA flow diagram summarizing the search results
I. The PRISMA flow diagram for selection of research papers:
II. PRISMA flow diagram summarizing the search results
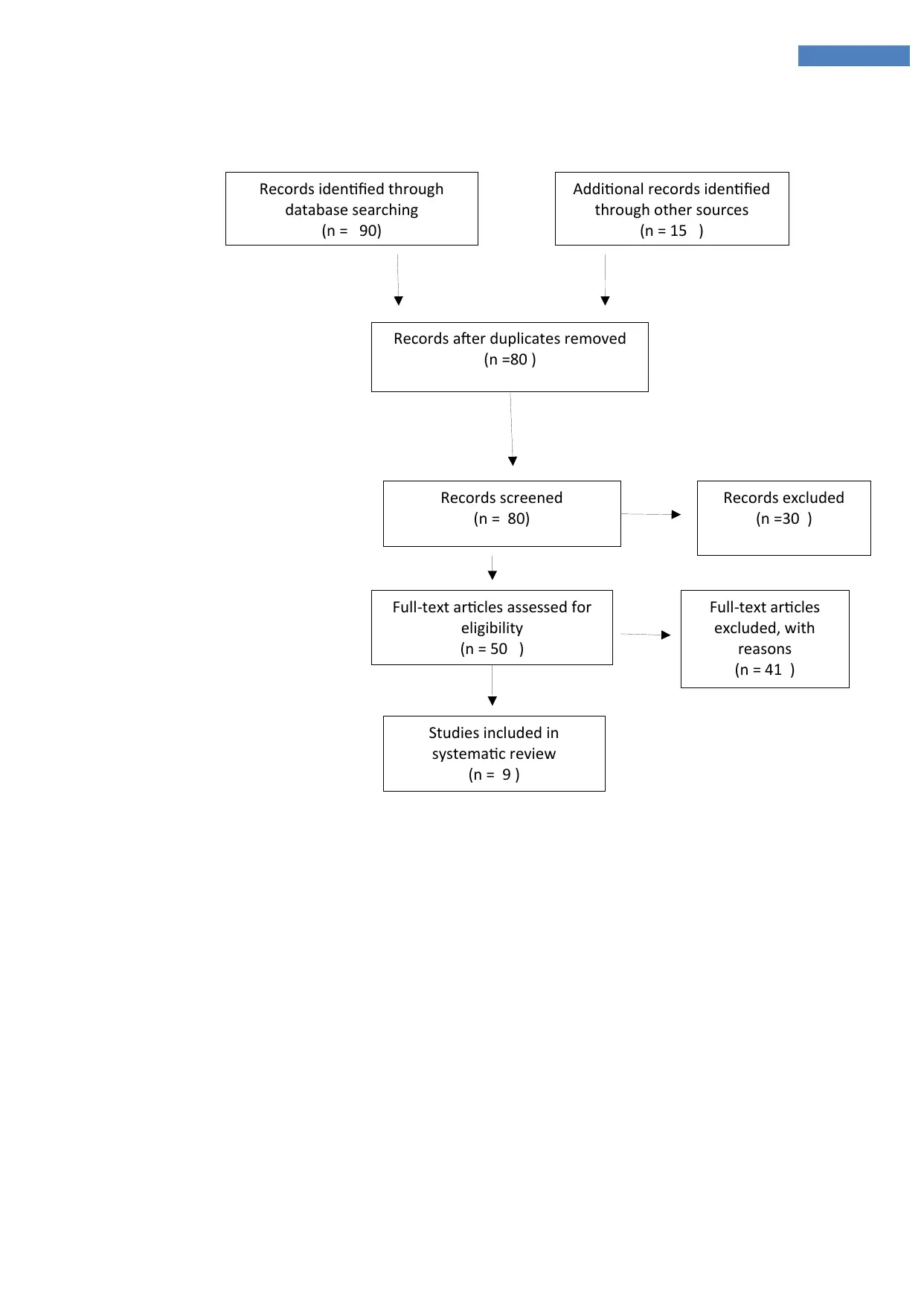
Records identified through
database searching
(n = 90)
Additional records identified
through other sources
(n = 15 )
Records after duplicates removed
(n =80 )
Records screened
(n = 80)
Records excluded
(n =30 )
Full-text articles assessed for
eligibility
(n = 50 )
Studies included in
systematic review
(n = 9 )
Full-text articles
excluded, with
reasons
(n = 41 )
database searching
(n = 90)
Additional records identified
through other sources
(n = 15 )
Records after duplicates removed
(n =80 )
Records screened
(n = 80)
Records excluded
(n =30 )
Full-text articles assessed for
eligibility
(n = 50 )
Studies included in
systematic review
(n = 9 )
Full-text articles
excluded, with
reasons
(n = 41 )
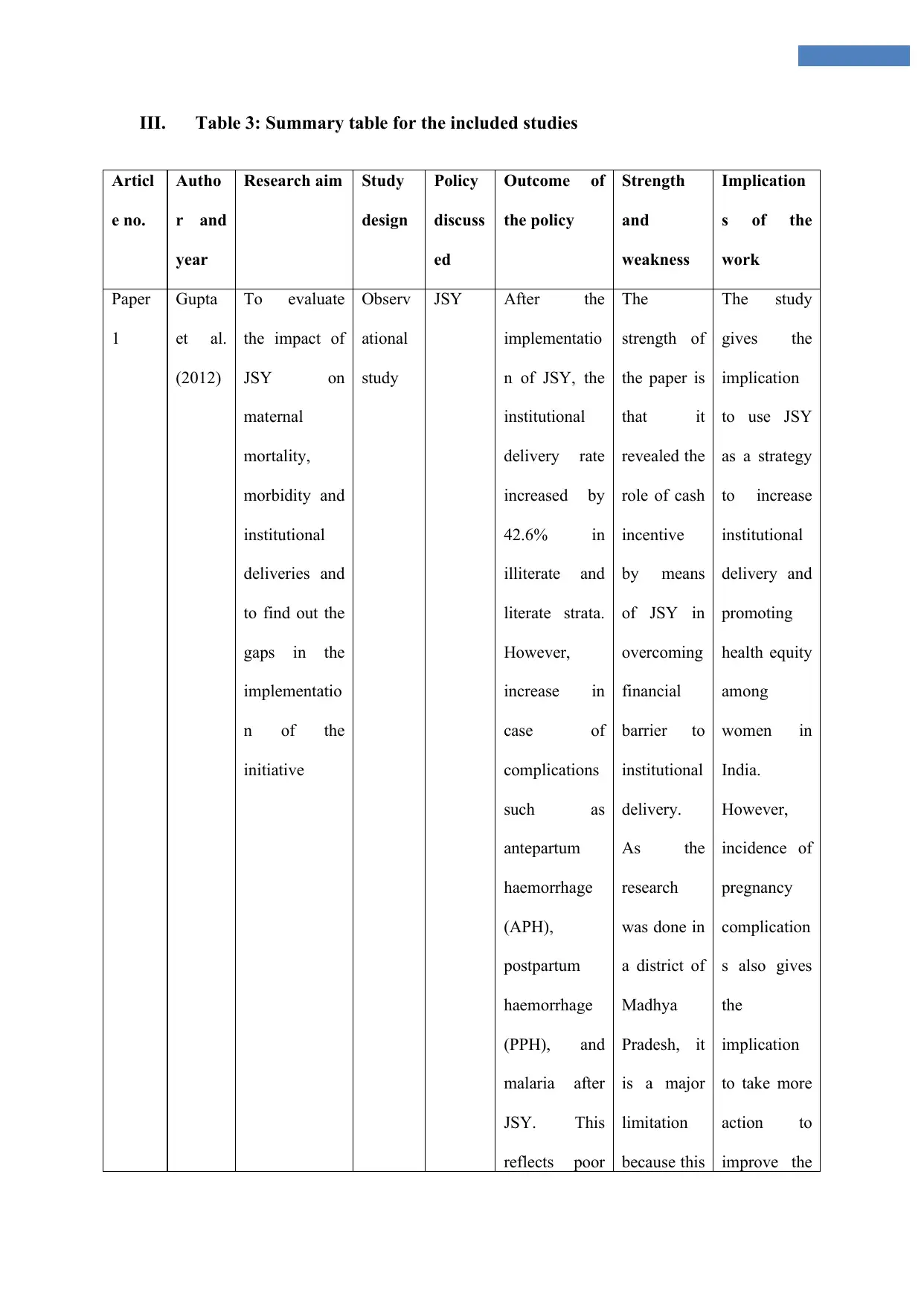
III. Table 3: Summary table for the included studies
Articl
e no.
Autho
r and
year
Research aim Study
design
Policy
discuss
ed
Outcome of
the policy
Strength
and
weakness
Implication
s of the
work
Paper
1
Gupta
et al.
(2012)
To evaluate
the impact of
JSY on
maternal
mortality,
morbidity and
institutional
deliveries and
to find out the
gaps in the
implementatio
n of the
initiative
Observ
ational
study
JSY After the
implementatio
n of JSY, the
institutional
delivery rate
increased by
42.6% in
illiterate and
literate strata.
However,
increase in
case of
complications
such as
antepartum
haemorrhage
(APH),
postpartum
haemorrhage
(PPH), and
malaria after
JSY. This
reflects poor
The
strength of
the paper is
that it
revealed the
role of cash
incentive
by means
of JSY in
overcoming
financial
barrier to
institutional
delivery.
As the
research
was done in
a district of
Madhya
Pradesh, it
is a major
limitation
because this
The study
gives the
implication
to use JSY
as a strategy
to increase
institutional
delivery and
promoting
health equity
among
women in
India.
However,
incidence of
pregnancy
complication
s also gives
the
implication
to take more
action to
improve the
Articl
e no.
Autho
r and
year
Research aim Study
design
Policy
discuss
ed
Outcome of
the policy
Strength
and
weakness
Implication
s of the
work
Paper
1
Gupta
et al.
(2012)
To evaluate
the impact of
JSY on
maternal
mortality,
morbidity and
institutional
deliveries and
to find out the
gaps in the
implementatio
n of the
initiative
Observ
ational
study
JSY After the
implementatio
n of JSY, the
institutional
delivery rate
increased by
42.6% in
illiterate and
literate strata.
However,
increase in
case of
complications
such as
antepartum
haemorrhage
(APH),
postpartum
haemorrhage
(PPH), and
malaria after
JSY. This
reflects poor
The
strength of
the paper is
that it
revealed the
role of cash
incentive
by means
of JSY in
overcoming
financial
barrier to
institutional
delivery.
As the
research
was done in
a district of
Madhya
Pradesh, it
is a major
limitation
because this
The study
gives the
implication
to use JSY
as a strategy
to increase
institutional
delivery and
promoting
health equity
among
women in
India.
However,
incidence of
pregnancy
complication
s also gives
the
implication
to take more
action to
improve the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
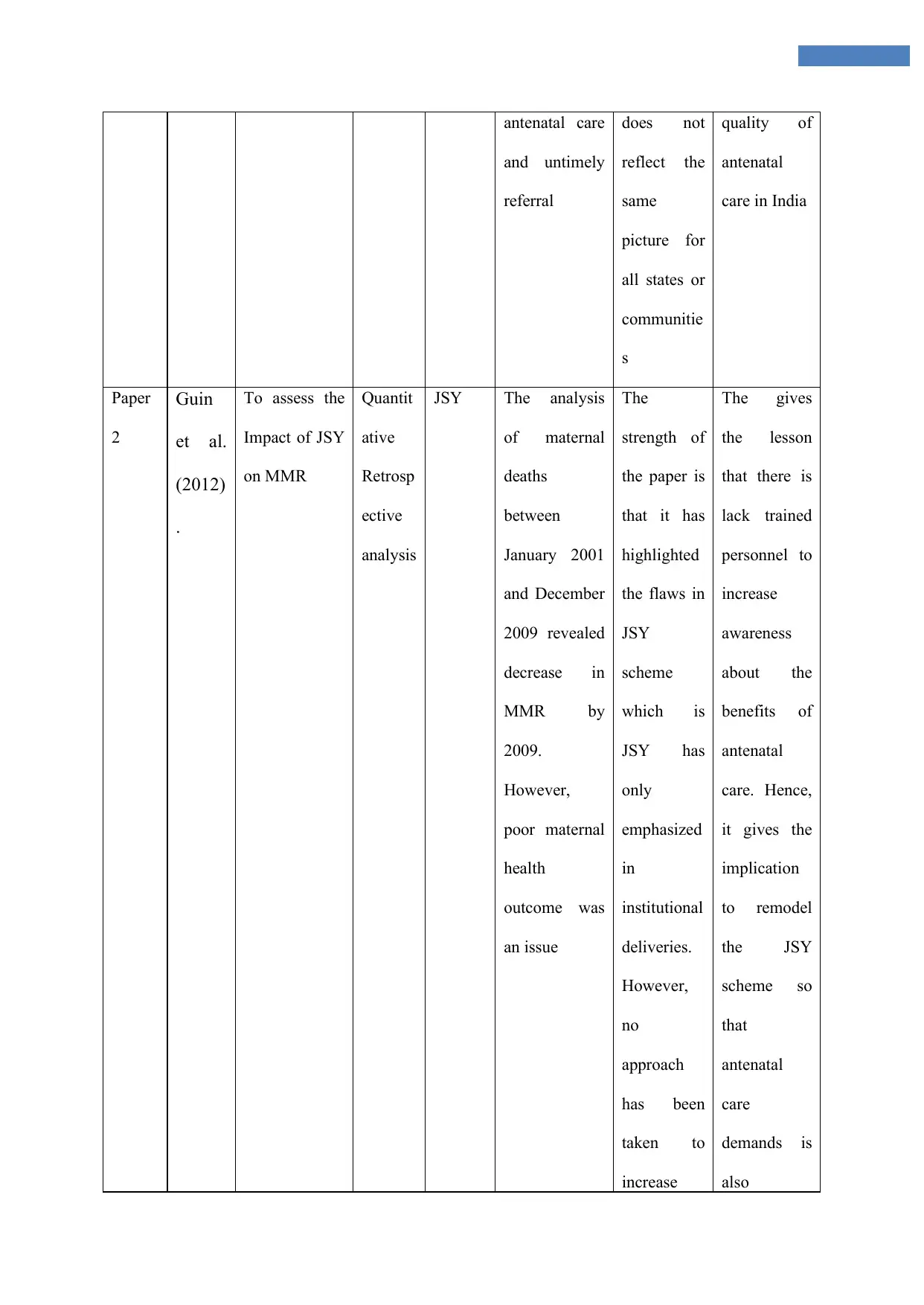
antenatal care
and untimely
referral
does not
reflect the
same
picture for
all states or
communitie
s
quality of
antenatal
care in India
Paper
2
Guin
et al.
(2012)
.
To assess the
Impact of JSY
on MMR
Quantit
ative
Retrosp
ective
analysis
JSY The analysis
of maternal
deaths
between
January 2001
and December
2009 revealed
decrease in
MMR by
2009.
However,
poor maternal
health
outcome was
an issue
The
strength of
the paper is
that it has
highlighted
the flaws in
JSY
scheme
which is
JSY has
only
emphasized
in
institutional
deliveries.
However,
no
approach
has been
taken to
increase
The gives
the lesson
that there is
lack trained
personnel to
increase
awareness
about the
benefits of
antenatal
care. Hence,
it gives the
implication
to remodel
the JSY
scheme so
that
antenatal
care
demands is
also
and untimely
referral
does not
reflect the
same
picture for
all states or
communitie
s
quality of
antenatal
care in India
Paper
2
Guin
et al.
(2012)
.
To assess the
Impact of JSY
on MMR
Quantit
ative
Retrosp
ective
analysis
JSY The analysis
of maternal
deaths
between
January 2001
and December
2009 revealed
decrease in
MMR by
2009.
However,
poor maternal
health
outcome was
an issue
The
strength of
the paper is
that it has
highlighted
the flaws in
JSY
scheme
which is
JSY has
only
emphasized
in
institutional
deliveries.
However,
no
approach
has been
taken to
increase
The gives
the lesson
that there is
lack trained
personnel to
increase
awareness
about the
benefits of
antenatal
care. Hence,
it gives the
implication
to remodel
the JSY
scheme so
that
antenatal
care
demands is
also
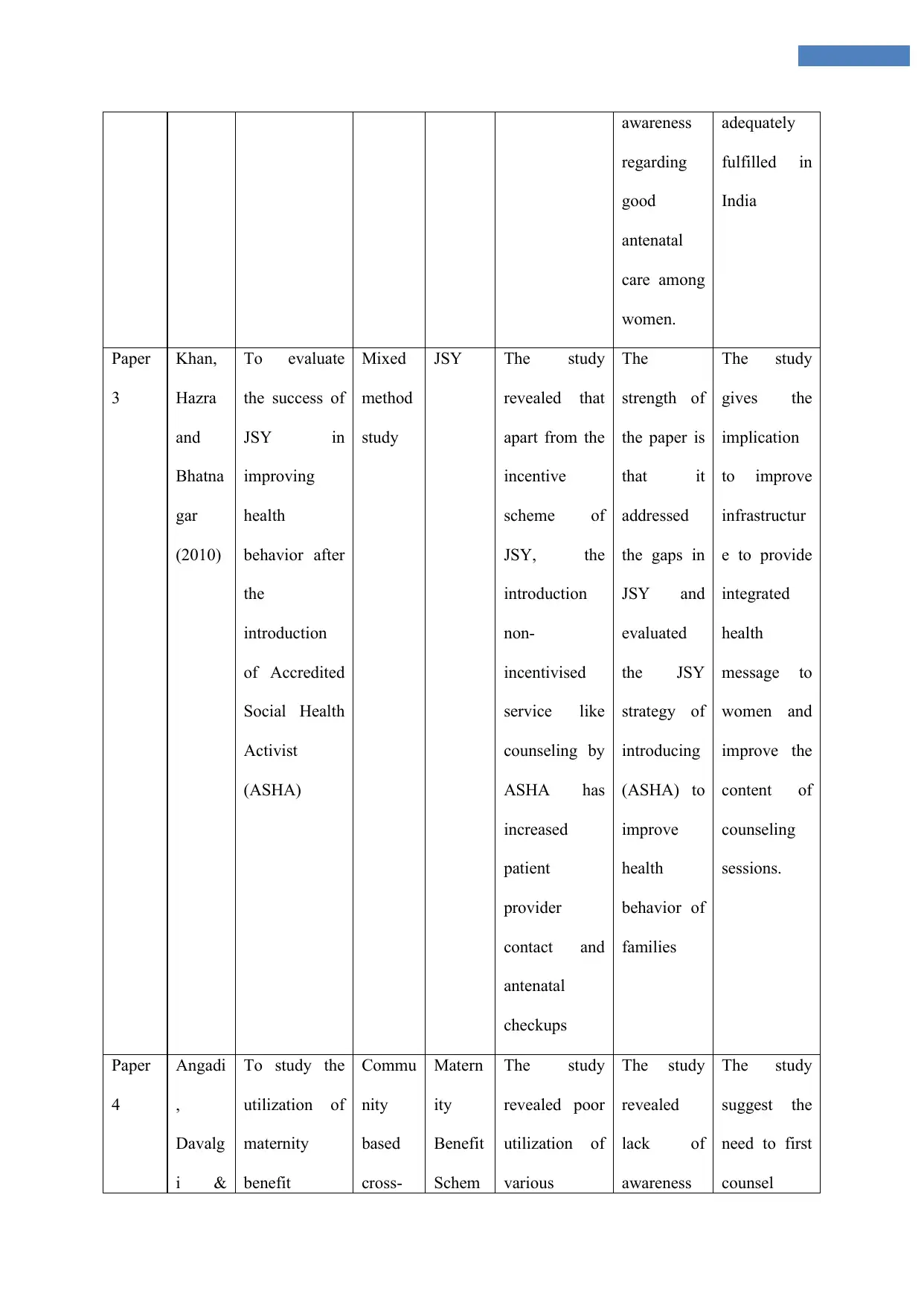
awareness
regarding
good
antenatal
care among
women.
adequately
fulfilled in
India
Paper
3
Khan,
Hazra
and
Bhatna
gar
(2010)
To evaluate
the success of
JSY in
improving
health
behavior after
the
introduction
of Accredited
Social Health
Activist
(ASHA)
Mixed
method
study
JSY The study
revealed that
apart from the
incentive
scheme of
JSY, the
introduction
non-
incentivised
service like
counseling by
ASHA has
increased
patient
provider
contact and
antenatal
checkups
The
strength of
the paper is
that it
addressed
the gaps in
JSY and
evaluated
the JSY
strategy of
introducing
(ASHA) to
improve
health
behavior of
families
The study
gives the
implication
to improve
infrastructur
e to provide
integrated
health
message to
women and
improve the
content of
counseling
sessions.
Paper
4
Angadi
,
Davalg
i &
To study the
utilization of
maternity
benefit
Commu
nity
based
cross-
Matern
ity
Benefit
Schem
The study
revealed poor
utilization of
various
The study
revealed
lack of
awareness
The study
suggest the
need to first
counsel
regarding
good
antenatal
care among
women.
adequately
fulfilled in
India
Paper
3
Khan,
Hazra
and
Bhatna
gar
(2010)
To evaluate
the success of
JSY in
improving
health
behavior after
the
introduction
of Accredited
Social Health
Activist
(ASHA)
Mixed
method
study
JSY The study
revealed that
apart from the
incentive
scheme of
JSY, the
introduction
non-
incentivised
service like
counseling by
ASHA has
increased
patient
provider
contact and
antenatal
checkups
The
strength of
the paper is
that it
addressed
the gaps in
JSY and
evaluated
the JSY
strategy of
introducing
(ASHA) to
improve
health
behavior of
families
The study
gives the
implication
to improve
infrastructur
e to provide
integrated
health
message to
women and
improve the
content of
counseling
sessions.
Paper
4
Angadi
,
Davalg
i &
To study the
utilization of
maternity
benefit
Commu
nity
based
cross-
Matern
ity
Benefit
Schem
The study
revealed poor
utilization of
various
The study
revealed
lack of
awareness
The study
suggest the
need to first
counsel
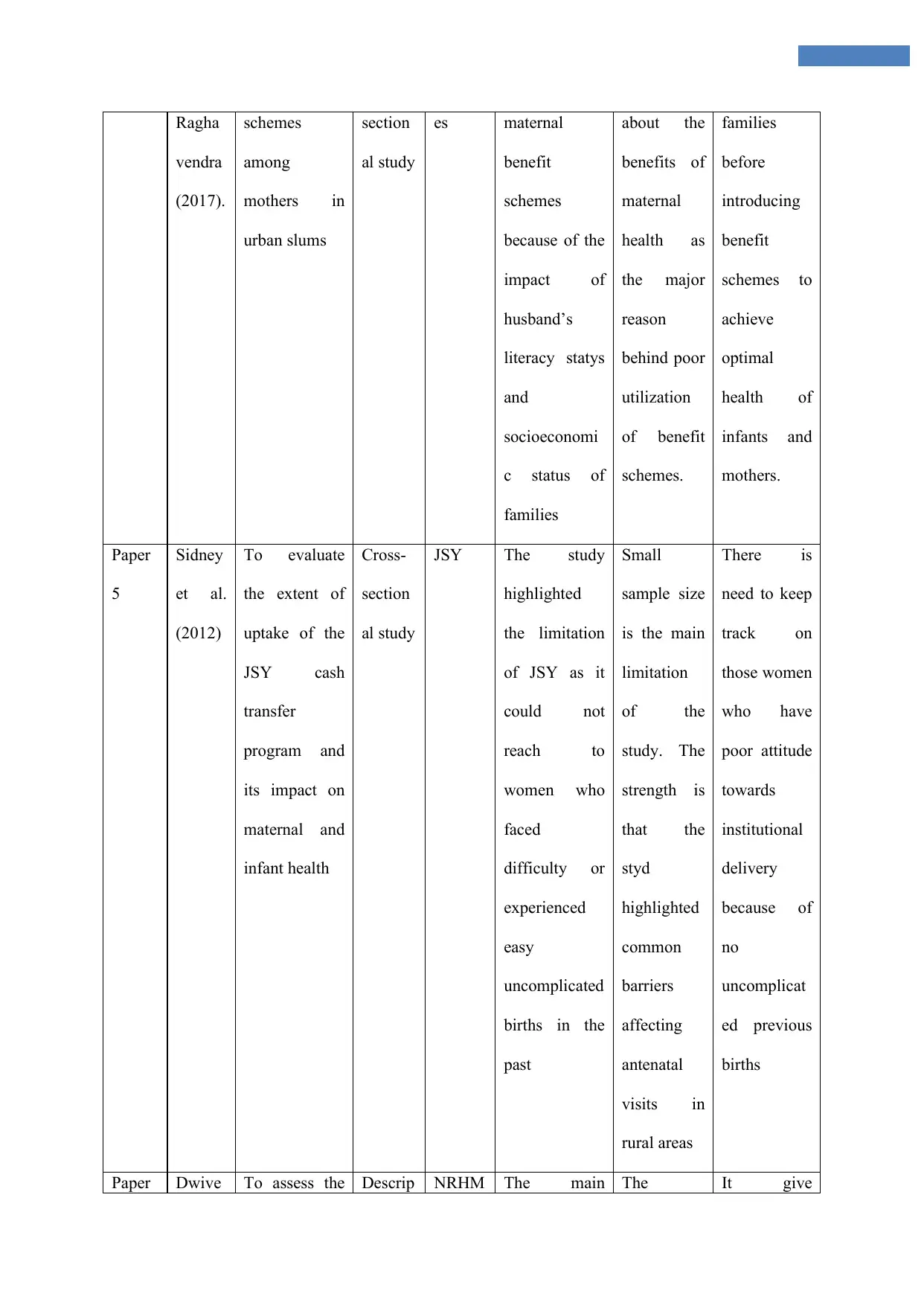
Ragha
vendra
(2017).
schemes
among
mothers in
urban slums
section
al study
es maternal
benefit
schemes
because of the
impact of
husband’s
literacy statys
and
socioeconomi
c status of
families
about the
benefits of
maternal
health as
the major
reason
behind poor
utilization
of benefit
schemes.
families
before
introducing
benefit
schemes to
achieve
optimal
health of
infants and
mothers.
Paper
5
Sidney
et al.
(2012)
To evaluate
the extent of
uptake of the
JSY cash
transfer
program and
its impact on
maternal and
infant health
Cross-
section
al study
JSY The study
highlighted
the limitation
of JSY as it
could not
reach to
women who
faced
difficulty or
experienced
easy
uncomplicated
births in the
past
Small
sample size
is the main
limitation
of the
study. The
strength is
that the
styd
highlighted
common
barriers
affecting
antenatal
visits in
rural areas
There is
need to keep
track on
those women
who have
poor attitude
towards
institutional
delivery
because of
no
uncomplicat
ed previous
births
Paper Dwive To assess the Descrip NRHM The main The It give
vendra
(2017).
schemes
among
mothers in
urban slums
section
al study
es maternal
benefit
schemes
because of the
impact of
husband’s
literacy statys
and
socioeconomi
c status of
families
about the
benefits of
maternal
health as
the major
reason
behind poor
utilization
of benefit
schemes.
families
before
introducing
benefit
schemes to
achieve
optimal
health of
infants and
mothers.
Paper
5
Sidney
et al.
(2012)
To evaluate
the extent of
uptake of the
JSY cash
transfer
program and
its impact on
maternal and
infant health
Cross-
section
al study
JSY The study
highlighted
the limitation
of JSY as it
could not
reach to
women who
faced
difficulty or
experienced
easy
uncomplicated
births in the
past
Small
sample size
is the main
limitation
of the
study. The
strength is
that the
styd
highlighted
common
barriers
affecting
antenatal
visits in
rural areas
There is
need to keep
track on
those women
who have
poor attitude
towards
institutional
delivery
because of
no
uncomplicat
ed previous
births
Paper Dwive To assess the Descrip NRHM The main The It give
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
6 di
(2015).
impact of
community
level
intervention
under NRHM
on infant and
maternal
health
tive
explora
tory
researc
h
method
findings from
the study
included lack
of receipt of
any advice
from health
personnels
and there was
minimum
interaction
between
women and
support staffs
limitation is
that no
appropriate
tool or
framework
was used to
analyzed
the data.
However,
the study
gave many
suggestions
for
improveme
nt
implication
to change
the
implementati
on approach
to make
NRHM
initiative
more
effective
Paper
7
Rao
and
Kaul
(2018).
To evaluate
the growth
and challenges
associated
with ICDS in
improving
quality of
maternal care
Review ICDS
(Integr
ated
Child
Develo
pment
Schem
e)
The results
revealed
positive
outcomes in
the area of
decreasing
malnutrition
and improving
child
development
in India
The
limitation
of the paper
is that it has
not used
rigorous
and
systematic
method for
reviewing
the scheme
It gives the
implication
to improve
the
implementati
on process
and consider
quality
standards.
Paper
8
Vellak
kal et
To evaluate
the impact of
Survey NRHM Steep decline
in inequities
The
limitation is
It gives the
implication
(2015).
impact of
community
level
intervention
under NRHM
on infant and
maternal
health
tive
explora
tory
researc
h
method
findings from
the study
included lack
of receipt of
any advice
from health
personnels
and there was
minimum
interaction
between
women and
support staffs
limitation is
that no
appropriate
tool or
framework
was used to
analyzed
the data.
However,
the study
gave many
suggestions
for
improveme
nt
implication
to change
the
implementati
on approach
to make
NRHM
initiative
more
effective
Paper
7
Rao
and
Kaul
(2018).
To evaluate
the growth
and challenges
associated
with ICDS in
improving
quality of
maternal care
Review ICDS
(Integr
ated
Child
Develo
pment
Schem
e)
The results
revealed
positive
outcomes in
the area of
decreasing
malnutrition
and improving
child
development
in India
The
limitation
of the paper
is that it has
not used
rigorous
and
systematic
method for
reviewing
the scheme
It gives the
implication
to improve
the
implementati
on process
and consider
quality
standards.
Paper
8
Vellak
kal et
To evaluate
the impact of
Survey NRHM Steep decline
in inequities
The
limitation is
It gives the
implication
al.
(2017)
NHRM on
addressing
socio-
economic
inequities in
antenatal care
method seen in lowest
and middle
wealth grouo
that impact
could not
be
evaluated
based on
control and
treatment
group.
However,
the strength
is that
focusing on
lower
socioecono
mic group
is important
to achieve
maternal
and infant
health
targets
to take steps
to increase
the outreach
of such
programs
(2017)
NHRM on
addressing
socio-
economic
inequities in
antenatal care
method seen in lowest
and middle
wealth grouo
that impact
could not
be
evaluated
based on
control and
treatment
group.
However,
the strength
is that
focusing on
lower
socioecono
mic group
is important
to achieve
maternal
and infant
health
targets
to take steps
to increase
the outreach
of such
programs
1 out of 43
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.