University of Newcastle: Childhood Motor Skills & Fitness Analysis
VerifiedAdded on 2023/05/29
|8
|8018
|136
Case Study
AI Summary
This case study investigates whether fundamental motor skill proficiency in childhood predicts subsequent adolescent cardiorespiratory fitness. The study followed participants from an elementary school-based intervention in 2000 to assess their motor skills (object control and locomotor skills) and then followed up in 2006/2007 to measure cardiorespiratory fitness using the Multistage Fitness Test. The results indicated that object control proficiency in childhood was significantly associated with adolescent cardiorespiratory fitness, accounting for 26% of the fitness variation. The study concludes that children with good object control skills are more likely to become fit adolescents, suggesting that fundamental motor skill development in childhood is an important component of interventions aimed at promoting long-term fitness. The research was conducted with ethics approval from relevant institutions and involved statistical analysis using linear regression to control for gender and other variables.
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
PhysicalFitness and Performance
Does Childhood Motor SkillProficiency
Predict Adolescent Fitness?
LISA M. BARNETT1, ERIC VAN BEURDEN2,3
, PHILIP J. MORGAN4, LYNDON O. BROOKS3, and JOHN R. BEARD1,3,5
1Department of Rural Health (Northern Rivers),University of Sydney,Lismore,New South Wales,AUSTRALIA;2Health
Promotion, North Coast Area Health Service, Lismore, New South Wales, AUSTRALIA;3Southern Cross University, Lismore,
New South Wales,AUSTRALIA;4Faculty of Education and Arts,University of Newcastle,Newcastle,New South Wales,
AUSTRALIA; and5New York Academy of Medicine,New York,NY
ABSTRACT
BARNETT, L. M, E. VAN BEURDEN, P. J. MORGAN, L. O. BROOKS, and J. R. BEARD. Does Childhood Motor Skill Proficiency
Predict Adolescent Fitness? Med. Sci. Sports Exerc., Vol. 40, No. 12, pp. 2137–2144, 2008. Purpose: To determine whether childho
fundamental motor skill proficiency predicts subsequent adolescent cardiorespiratory fitness. Methods: In 2000, children_s proficie
in a battery of skills was assessed as part of an elementary school-based intervention. Participants were followed up during 2006/2
as part of the Physical Activity and Skills Study, and cardiorespiratory fitness was measured using the Multistage Fitness Test. Line
regressionwas used to examinethe relationshipbetweenchildhoodfundamentalmotor skill proficiencyand adolescent
cardiorespiratory fitness controlling for gender.Composite objectcontrol(kick,catch,throw) and locomotor skill(hop,side gallop,
verticaljump)wereconstructed foranalysis.A separatelinearregression examined theability of the sprintrun to predict
cardiorespiratory fitness.Results: Of the 928 originalintervention participants,481 were in 28 schools,276 (57%) of whom were
assessed.Two hundred and forty-fourstudents (88.4%)completed the fitness test.One hundred and twenty-seven were females
(52.1%), 60.1% of whom were in grade 10 and 39.0% were in grade 11. As children, almost all 244 completed each motor assessm
except for the sprint run (n = 154, 55.8%). The mean composite skill score in 2000 was 17.7 (SD 5.1). In 2006/2007, the mean num
of laps on the Multistage Fitness Test was 50.5 (SD 24.4). Object control proficiency in childhood, adjusting for gender (P = 0.000)
was associated with adolescentcardiorespiratory fitness (P = 0.012),accounting for 26% of fitness variation.Conclusion: Children
with good object control skills are more likely to become fit adolescents. Fundamental motor skill development in childhood may b
importantcomponentof interventionsaiming to promote long-term fitness.Key Words: FUNDAMENTAL MOTOR SKILL,
CARDIORESPIRATORY ENDURANCE, CHILD, LONGITUDINAL
The increasing prevalence of obesity in many devel-
oped countries has led to a growing interestin the
determinantsof physicalactivity in thegeneral
population.Because physicalactivity hasa strong dose
relationship to fitness(7), the natureand the relative
importanceof fitnessdeterminantsmay also becritical
(29). A recent review suggests that cardiorespiratory fitness
or endurance is associated with both obesity and cardiovas-
culardisease factors (29),and there is also a significant
relationship between adolescentcardiorespiratory fitness
and later body fatness (2,12).
In fact,cardiorespiratory fitness is emerging as a factor
even more deserving ofattention than physicalactivity.
Fitnesshas been found to bea strongerpredictorof
mortality in adultmen than activity patterns(23), and
cardiovascular risk factors seem to relate more strongly to
cardiorespiratoryfitnessthan componentsof physical
activity in children and adolescents (16).Yet despite the
importanceof physicalfitness,cardiorespiratory fitness
among youth is declining (11).As fitness in adolescence
is closely related to fitness in adult years (33,36), improvin
the cardiorespiratoryfitness of adolescentsthrough
increasesin time spentin vigorousactivity and high-
intensity training should bean importantpublichealth
priority (29).
One possible determinantof adolescentfitness is motor
skill proficiency. Motor development models propose many
levels through which a child must progress to achieve mot
proficiency.Fundamentalmotorskills, eitherlocomotor
(involving movement,e.g., hopping)or objectcontrol
Addressfor correspondence:Lisa M. Barnett,MPH, Bch, Soc Sci,
Departmentof Rural Health (Northern Rivers),University ofSydney,
PO Box 3074, Lismore,NSW 2480, Australia;Email: lisa.barnett@
ncahs.health.nsw.gov.au.
Submitted for publication March 2008.
Accepted for publication May 2008.
0195-9131/08/4012-2137/0
MEDICINE & SCIENCE IN SPORTS & EXERCISEÒ
Copyright Ó 2008 by the American College of Sports Medicine
DOI: 10.1249/MSS.0b013e31818160d3
2137
APPLIED SCIENCES
PhysicalFitness and Performance
Does Childhood Motor SkillProficiency
Predict Adolescent Fitness?
LISA M. BARNETT1, ERIC VAN BEURDEN2,3
, PHILIP J. MORGAN4, LYNDON O. BROOKS3, and JOHN R. BEARD1,3,5
1Department of Rural Health (Northern Rivers),University of Sydney,Lismore,New South Wales,AUSTRALIA;2Health
Promotion, North Coast Area Health Service, Lismore, New South Wales, AUSTRALIA;3Southern Cross University, Lismore,
New South Wales,AUSTRALIA;4Faculty of Education and Arts,University of Newcastle,Newcastle,New South Wales,
AUSTRALIA; and5New York Academy of Medicine,New York,NY
ABSTRACT
BARNETT, L. M, E. VAN BEURDEN, P. J. MORGAN, L. O. BROOKS, and J. R. BEARD. Does Childhood Motor Skill Proficiency
Predict Adolescent Fitness? Med. Sci. Sports Exerc., Vol. 40, No. 12, pp. 2137–2144, 2008. Purpose: To determine whether childho
fundamental motor skill proficiency predicts subsequent adolescent cardiorespiratory fitness. Methods: In 2000, children_s proficie
in a battery of skills was assessed as part of an elementary school-based intervention. Participants were followed up during 2006/2
as part of the Physical Activity and Skills Study, and cardiorespiratory fitness was measured using the Multistage Fitness Test. Line
regressionwas used to examinethe relationshipbetweenchildhoodfundamentalmotor skill proficiencyand adolescent
cardiorespiratory fitness controlling for gender.Composite objectcontrol(kick,catch,throw) and locomotor skill(hop,side gallop,
verticaljump)wereconstructed foranalysis.A separatelinearregression examined theability of the sprintrun to predict
cardiorespiratory fitness.Results: Of the 928 originalintervention participants,481 were in 28 schools,276 (57%) of whom were
assessed.Two hundred and forty-fourstudents (88.4%)completed the fitness test.One hundred and twenty-seven were females
(52.1%), 60.1% of whom were in grade 10 and 39.0% were in grade 11. As children, almost all 244 completed each motor assessm
except for the sprint run (n = 154, 55.8%). The mean composite skill score in 2000 was 17.7 (SD 5.1). In 2006/2007, the mean num
of laps on the Multistage Fitness Test was 50.5 (SD 24.4). Object control proficiency in childhood, adjusting for gender (P = 0.000)
was associated with adolescentcardiorespiratory fitness (P = 0.012),accounting for 26% of fitness variation.Conclusion: Children
with good object control skills are more likely to become fit adolescents. Fundamental motor skill development in childhood may b
importantcomponentof interventionsaiming to promote long-term fitness.Key Words: FUNDAMENTAL MOTOR SKILL,
CARDIORESPIRATORY ENDURANCE, CHILD, LONGITUDINAL
The increasing prevalence of obesity in many devel-
oped countries has led to a growing interestin the
determinantsof physicalactivity in thegeneral
population.Because physicalactivity hasa strong dose
relationship to fitness(7), the natureand the relative
importanceof fitnessdeterminantsmay also becritical
(29). A recent review suggests that cardiorespiratory fitness
or endurance is associated with both obesity and cardiovas-
culardisease factors (29),and there is also a significant
relationship between adolescentcardiorespiratory fitness
and later body fatness (2,12).
In fact,cardiorespiratory fitness is emerging as a factor
even more deserving ofattention than physicalactivity.
Fitnesshas been found to bea strongerpredictorof
mortality in adultmen than activity patterns(23), and
cardiovascular risk factors seem to relate more strongly to
cardiorespiratoryfitnessthan componentsof physical
activity in children and adolescents (16).Yet despite the
importanceof physicalfitness,cardiorespiratory fitness
among youth is declining (11).As fitness in adolescence
is closely related to fitness in adult years (33,36), improvin
the cardiorespiratoryfitness of adolescentsthrough
increasesin time spentin vigorousactivity and high-
intensity training should bean importantpublichealth
priority (29).
One possible determinantof adolescentfitness is motor
skill proficiency. Motor development models propose many
levels through which a child must progress to achieve mot
proficiency.Fundamentalmotorskills, eitherlocomotor
(involving movement,e.g., hopping)or objectcontrol
Addressfor correspondence:Lisa M. Barnett,MPH, Bch, Soc Sci,
Departmentof Rural Health (Northern Rivers),University ofSydney,
PO Box 3074, Lismore,NSW 2480, Australia;Email: lisa.barnett@
ncahs.health.nsw.gov.au.
Submitted for publication March 2008.
Accepted for publication May 2008.
0195-9131/08/4012-2137/0
MEDICINE & SCIENCE IN SPORTS & EXERCISEÒ
Copyright Ó 2008 by the American College of Sports Medicine
DOI: 10.1249/MSS.0b013e31818160d3
2137
APPLIED SCIENCES
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
(involving manipulation ofan object,e.g.,kicking),are
usually perceived as occurring after a stage (or stages) that
involves birth reflexes. Mastery of fundamental motor skills
provides the foundation for the development of more sports-
specificskills (15). Cross-sectionalstudiessuggestthat
fundamentalmotorskill proficiency is related to physical
activity participation in children and youth (4,15,24,37),
and there is evidence thatyouth with poorerfundamental
motor skill proficiency have lower cardiorespiratory endur-
ance (4,15,24,32,37). Because motor skill proficiency tracks
through childhood (6,21),it is plausible thatchildren with
poorermotorskills may become lessactive adolescents
with associated poorerfitness levels.However,no longi-
tudinalresearch hasinvestigatedwhetherfundamental
motorskill proficiency in childhood predictsadolescent
fitness.This articleexaminesthe relationship between
childhood motorskill proficiency and subsequentadoles-
cent cardiorespiratory fitness as part of a longitudinal cohort
study known asthe PhysicalActivity and SkillsStudy
(PASS).
SUBJECTS AND METHODS
In 2000,1045 children from 18 randomly selected and
stratified primary (elementary)schoolsin a study area
comprising24555km2 in New South Wales (NSW),
Australia,had theirproficiency in a battery ofmotorskills
assessed for a school-based physical activity intervention (34).
Mean age of the sample was 10.1 yr (range = 7.9–11.9 yr).
In 2006/2007, the list of original study participants (1021
had initials on records and 929 records (91.0%) matched by
gender and name to class roll) was sentto 41 consenting
high schoolsin the originalstudy districtto identify
adolescentstudentsfor follow-up aspartof the PASS.
One schoolin the study area did notconsentto partic-
ipation.When students_ names were identified on the high
school register, students were given a letter inviting them to
participate in the PASS, an information sheet, and a consent
form. Students who returned a consent form signed by their
parents/guardian and themselves were included in the PASS
sample.Ethics approval was gained from the University of
Sydney (07-2006/9243), the NSW Department of Education
and Training (06.296),and the local Catholic Diocese.
Slightly more than half of the 928 original(one student
died before consent) participants (51.8%, n = 481/928) were
in 28 schools.Each ofthese students was approached to
participate in the study,with a consentrate of 61.7% (n =
297/481) and 57.4% (n = 276/481) ultimately assessed as
partof the PASS.The overallfollow-up rate was 29.7%
(276/928). The followed-up sample of 276 did not differ by
gender (W2 = 2.403, P = 0.121) but was more likely to have
been originally tested in grade 4 (61.5%) than in grade 5
(38.5%;W2 = 22.666,P G 0.0001).This may reflectthe
greater difficulty of finding older participants atfollow-up
because they are more likely to have left the school system.
Participants not lost to follow-up also had a slightly higher
(17.5 compared with 16.5)mean compositechildhood
fundamental motor skill score (t = j2.60,P = 0.009).The
childhood fundamentalmotorskill proficiency of the 244
studentswith fitnesstestresultswas also higher(17.7
compared with 16.7)than thosewho did not consent
(t = j2.18,P = 0.030).
Data collection. Datawere collected by thestudy
coordinatorand threeresearch assistants.The assistants
completed3 d of training facilitatedby the study
coordinatorand a trainerwho had trained teachersin
fundamentalmotor skillassessmentand assessed children
as partof a separatestudy (17).The majority ofdata
(994%)werecollected overterm 4 in 2006,with the
remainder early in term 1 in 2007 (both over summer).
Motor skill measurement. Theinitial intervention
had used the Australian resource, ‘‘Get Skilled Get Active,’
(New South Wales Departmentof Education and Training
2000:DET ProductNumber10614/DVD)to assessthe
eight (kick, catch, overhand throw, hop, side gallop, vertic
jump,sprintrun, and static balance)motorskills. This
resource specifiesa battery offundamentalmotorskills
tests,eightof which were validated in an originalmanual
(catch,overhand throw,kick, forehand strike,sprintrun,
leap,dodge,and verticaljump)(9), returning reliability
estimates (alpha coefficient method) of r = 0.70 (P G 0.01
or greater for all skills except the leap and run (r = 0.13 an
r = 0.17, respectively; not significant). Four additional skil
(hop, static balance, skip, and side gallop) were validated
partof the subsequenttestbattery and were found to have
good test–retest reliability for young children (28).
Seven skills,threeobjectcontrol(kick, catch,and
overhand throw)and fourlocomotor(hop,side gallop,
verticaljump,and sprintrun), assessed in 2000 were
reported on in this study.This battery includes skills that
both malesand femaleshave demonstrated performance
mastery (22,24,35).Each skillis made up offive or six
features considered integral to the proficient performance
the skill. For example, the catch consists of six features: 1
eyes focused on the object throughout; 2) feet move to pla
body in line with object; 3) hands move to meet the object
4) hands and fingers relaxed and slightly cupped; 5) catch
controlobjectwith hands only,well-timed closure;and 6)
elbows bend to absorb force of object.
The testing procedureallowed studentsto observea
fundamentalmotor skilldemonstration before being asked
to perform the skill.For the catch,kick,overhand throw,
and vertical jump, the skill was performed five times with a
featuredeemed aspresentif the studentperformed it
consistently overfive occasions(9). If therewas any
uncertainty about whether a feature was consistently pres
or not,the assistantwas instructed to check the feature as
absent.For the hop and side gallop,the skill was observed
as students traveled back and forth once between two poi
15 m apart. The sprint run was observed as students ran a
fastas possible between two points 20 m apart.Interrater
reliability was reported previously as kappa = 0.61 (34).
http://www.acsm-msse.org2138 OfficialJournal of the American College of Sports Medicine
APPLIED SCIENCES
(involving manipulation ofan object,e.g.,kicking),are
usually perceived as occurring after a stage (or stages) that
involves birth reflexes. Mastery of fundamental motor skills
provides the foundation for the development of more sports-
specificskills (15). Cross-sectionalstudiessuggestthat
fundamentalmotorskill proficiency is related to physical
activity participation in children and youth (4,15,24,37),
and there is evidence thatyouth with poorerfundamental
motor skill proficiency have lower cardiorespiratory endur-
ance (4,15,24,32,37). Because motor skill proficiency tracks
through childhood (6,21),it is plausible thatchildren with
poorermotorskills may become lessactive adolescents
with associated poorerfitness levels.However,no longi-
tudinalresearch hasinvestigatedwhetherfundamental
motorskill proficiency in childhood predictsadolescent
fitness.This articleexaminesthe relationship between
childhood motorskill proficiency and subsequentadoles-
cent cardiorespiratory fitness as part of a longitudinal cohort
study known asthe PhysicalActivity and SkillsStudy
(PASS).
SUBJECTS AND METHODS
In 2000,1045 children from 18 randomly selected and
stratified primary (elementary)schoolsin a study area
comprising24555km2 in New South Wales (NSW),
Australia,had theirproficiency in a battery ofmotorskills
assessed for a school-based physical activity intervention (34).
Mean age of the sample was 10.1 yr (range = 7.9–11.9 yr).
In 2006/2007, the list of original study participants (1021
had initials on records and 929 records (91.0%) matched by
gender and name to class roll) was sentto 41 consenting
high schoolsin the originalstudy districtto identify
adolescentstudentsfor follow-up aspartof the PASS.
One schoolin the study area did notconsentto partic-
ipation.When students_ names were identified on the high
school register, students were given a letter inviting them to
participate in the PASS, an information sheet, and a consent
form. Students who returned a consent form signed by their
parents/guardian and themselves were included in the PASS
sample.Ethics approval was gained from the University of
Sydney (07-2006/9243), the NSW Department of Education
and Training (06.296),and the local Catholic Diocese.
Slightly more than half of the 928 original(one student
died before consent) participants (51.8%, n = 481/928) were
in 28 schools.Each ofthese students was approached to
participate in the study,with a consentrate of 61.7% (n =
297/481) and 57.4% (n = 276/481) ultimately assessed as
partof the PASS.The overallfollow-up rate was 29.7%
(276/928). The followed-up sample of 276 did not differ by
gender (W2 = 2.403, P = 0.121) but was more likely to have
been originally tested in grade 4 (61.5%) than in grade 5
(38.5%;W2 = 22.666,P G 0.0001).This may reflectthe
greater difficulty of finding older participants atfollow-up
because they are more likely to have left the school system.
Participants not lost to follow-up also had a slightly higher
(17.5 compared with 16.5)mean compositechildhood
fundamental motor skill score (t = j2.60,P = 0.009).The
childhood fundamentalmotorskill proficiency of the 244
studentswith fitnesstestresultswas also higher(17.7
compared with 16.7)than thosewho did not consent
(t = j2.18,P = 0.030).
Data collection. Datawere collected by thestudy
coordinatorand threeresearch assistants.The assistants
completed3 d of training facilitatedby the study
coordinatorand a trainerwho had trained teachersin
fundamentalmotor skillassessmentand assessed children
as partof a separatestudy (17).The majority ofdata
(994%)werecollected overterm 4 in 2006,with the
remainder early in term 1 in 2007 (both over summer).
Motor skill measurement. Theinitial intervention
had used the Australian resource, ‘‘Get Skilled Get Active,’
(New South Wales Departmentof Education and Training
2000:DET ProductNumber10614/DVD)to assessthe
eight (kick, catch, overhand throw, hop, side gallop, vertic
jump,sprintrun, and static balance)motorskills. This
resource specifiesa battery offundamentalmotorskills
tests,eightof which were validated in an originalmanual
(catch,overhand throw,kick, forehand strike,sprintrun,
leap,dodge,and verticaljump)(9), returning reliability
estimates (alpha coefficient method) of r = 0.70 (P G 0.01
or greater for all skills except the leap and run (r = 0.13 an
r = 0.17, respectively; not significant). Four additional skil
(hop, static balance, skip, and side gallop) were validated
partof the subsequenttestbattery and were found to have
good test–retest reliability for young children (28).
Seven skills,threeobjectcontrol(kick, catch,and
overhand throw)and fourlocomotor(hop,side gallop,
verticaljump,and sprintrun), assessed in 2000 were
reported on in this study.This battery includes skills that
both malesand femaleshave demonstrated performance
mastery (22,24,35).Each skillis made up offive or six
features considered integral to the proficient performance
the skill. For example, the catch consists of six features: 1
eyes focused on the object throughout; 2) feet move to pla
body in line with object; 3) hands move to meet the object
4) hands and fingers relaxed and slightly cupped; 5) catch
controlobjectwith hands only,well-timed closure;and 6)
elbows bend to absorb force of object.
The testing procedureallowed studentsto observea
fundamentalmotor skilldemonstration before being asked
to perform the skill.For the catch,kick,overhand throw,
and vertical jump, the skill was performed five times with a
featuredeemed aspresentif the studentperformed it
consistently overfive occasions(9). If therewas any
uncertainty about whether a feature was consistently pres
or not,the assistantwas instructed to check the feature as
absent.For the hop and side gallop,the skill was observed
as students traveled back and forth once between two poi
15 m apart. The sprint run was observed as students ran a
fastas possible between two points 20 m apart.Interrater
reliability was reported previously as kappa = 0.61 (34).
http://www.acsm-msse.org2138 OfficialJournal of the American College of Sports Medicine
APPLIED SCIENCES
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
Cardiorespiratory fitness measure. Cardiorespi-
ratory ‘‘fitness’’or ‘‘endurance’’was estimated indirectly
in 2006/2007 from the numberof laps completed on the
Multistage Fitness Test(also known as the 20-m Shuttle
Run Test,Beep Test,or PACER) (20). This testwas
selected overotherfield measuresof cardiorespiratory
endurance such as timed and distance runs because ithas
been shown to be more motivationaland appropriate for
indoortesting and isless influenced by pacing among
children and adolescents (10). It is also considered to be an
appropriate and time-efficienttestof aerobic fitnessfor
large groups of students (10).Students are required to run
between two lines 20 m apart(one ‘‘lap’’)starting at8.5
kmIhj1 (level 1) and increasing by 0.5 kmIhj1 every 2 min,
in time with a recorded beep signal,with each increase
correspondingto a changein level. The numberof
‘‘acceptable’’ laps completed is determined by the student
not keeping pace with the signalfrom the tape fortwo
consecutive laps (whereupon they are withdrawn from the
test) or the student withdraws themselves (10).
Students were played the initialtaped introduction that
describes the test protocol. Students were advised they must
keep in time with the ‘‘beep’’ sound and mustplace their
footon or over the line each time.The 20-m distance was
markedout using a tapemeasureand witches_hats.
Students were run in groups of no more than 15 to ensure
adequate spacing.On termination,each studenthad their
finalleveland shuttle scores written on their hand by the
study coordinator,and scoreswere recorded when all
students finished.
Students were also asked to specify date of birth, gender,
and language spoken athome and allorganized physical
activities (activities involving regularclasses,training,or
competition thatwere somewhatstructured orformaland
had a coach,instructor,or teacher)in which they partici-
pated in a usualweek,in both summerand winter.The
validated AdolescentPhysicalActivity RecallQuestion-
naire was used for this assessment (3).
Data and analysis. Forthe fundamentalmotorskill
measures, the number of features rated as present or correct
was summed for each subject. For the descriptive reporting
by skill,all features correctwas considered as ‘‘mastery,’’
all butone feature correctas ‘‘nearmastery,’’and more
than one featureincorrectas ‘‘poor.’’ Categoriesof
‘‘mastery’’ and ‘‘near mastery’’ were combined and termed
‘‘advanced skillproficiency’’(5). Each skill(exceptthe
sprint run) was then standardized to a score of 5, and scores
for the six skills were summed to create scores out of 15 for
the three objectcontrol(kick,catch,and overhand throw)
and three locomotorskills (hop,side gallop,and vertical
jump) (27).
Scores for the Multistage Fitness Test were based on the
lastleveland shuttle completed by a student.This result
was converted to the number of laps achieved to create a
continuousvariablefor analysis.We reportcardiorespi-
ratory fitness firstin terms of the number of laps achieved
and secondly afteradjusting forage and gender.We
adjusted levelsusing theCooperInstitutefor Aerobics
Research standards,constructed to ascertain the levelof
cardiorespiratory fitness needed to decrease risk of all-cau
mortality (above 20th percentile formalesand 40th for
females)(8). Each physicalactivity was assigned a MET
value (1 MET = 3.5 mL oxygenIkgj1 body weightj1 Iminj1 )
from a comprehensive list of physical activities (1).As per
the SPANS,activities G10 min in duration,with a MET
value of G3.0, or less than once per week were excluded (
To gain a listof highly reported voluntary out-of-school–
organized sporting activities, ‘‘physical education,’’ ‘‘sport
science,’’ and ‘‘school sport’’ were excluded.
A general linear model in SPSS (SPSS, Inc, Chicago, IL;
http://www.spss.com/)was fitted to examine the relation-
ship between fundamental motor skill proficiency in child-
hood and cardiorespiratory fitness (number of laps achieve
on the MultistageFitnessTest) in adolescence.The
dependentvariable (cardiorespiratory fitness)was square
root-transformed before analysis to normalize its distribu-
tion.The relationship between school grade,gender,child-
hood objectcontrolproficiency and childhood locomotor
proficiency,and fitness in adolescencewas initially
assessed univariately for significance.
Significant variables were included as main effects in the
model.Interactions between significantmotorskill profi-
ciency variablesand genderwereincluded to examine
whetherthe relationships between motorskill proficiency
and fitnessdiffered between maleand femalestudents.
Interaction terms were only retained in the finalmodelif
found significant.Predicted valuesof cardiorespiratory
fitness, on the basis of the model parameter estimates, we
back-transformed from their square root values and plotte
againstthe observed range ofobjectcontrolvariables by
gender (Fig.1).
Because there was only data forhalf the sample (n =
154),a separate linearregression examined the ability of
advanced performance ofthe sprintrun in childhood to
predictcardiorespiratory fitness in adolescence.The rela-
tionship between gender,advanced performanceof the
sprint run,and fitness in adolescence was initially assessed
univariately for significance. School grade was not include
because the sprint run was primarily only assessed for one
grade (grade 4, n = 140; grade 5, n = 14). Univariately, th
sprintrun wasfound notto be a significantpredictor.
However,the sprintrun was stilltested in a modelwith
gender and the interaction term between gender and sprin
run to see ifthe relationship between childhood perform-
anceof the sprintrun and adolescentcardiorespiratory
fitness differed according to gender.
RESULTS
Sample. Of 276 students followed up for the PASS, 234
(84.8%)completed theMultistageFitnessTest. Of 42
nonparticipants, 31 were unwilling to do some aspect of th
CHILDHOOD MOTOR SKILL AND ADOLESCENT FITNESS Medicine & Science in Sports & Exercised 2139
APPLIED SCIENCES
Cardiorespiratory fitness measure. Cardiorespi-
ratory ‘‘fitness’’or ‘‘endurance’’was estimated indirectly
in 2006/2007 from the numberof laps completed on the
Multistage Fitness Test(also known as the 20-m Shuttle
Run Test,Beep Test,or PACER) (20). This testwas
selected overotherfield measuresof cardiorespiratory
endurance such as timed and distance runs because ithas
been shown to be more motivationaland appropriate for
indoortesting and isless influenced by pacing among
children and adolescents (10). It is also considered to be an
appropriate and time-efficienttestof aerobic fitnessfor
large groups of students (10).Students are required to run
between two lines 20 m apart(one ‘‘lap’’)starting at8.5
kmIhj1 (level 1) and increasing by 0.5 kmIhj1 every 2 min,
in time with a recorded beep signal,with each increase
correspondingto a changein level. The numberof
‘‘acceptable’’ laps completed is determined by the student
not keeping pace with the signalfrom the tape fortwo
consecutive laps (whereupon they are withdrawn from the
test) or the student withdraws themselves (10).
Students were played the initialtaped introduction that
describes the test protocol. Students were advised they must
keep in time with the ‘‘beep’’ sound and mustplace their
footon or over the line each time.The 20-m distance was
markedout using a tapemeasureand witches_hats.
Students were run in groups of no more than 15 to ensure
adequate spacing.On termination,each studenthad their
finalleveland shuttle scores written on their hand by the
study coordinator,and scoreswere recorded when all
students finished.
Students were also asked to specify date of birth, gender,
and language spoken athome and allorganized physical
activities (activities involving regularclasses,training,or
competition thatwere somewhatstructured orformaland
had a coach,instructor,or teacher)in which they partici-
pated in a usualweek,in both summerand winter.The
validated AdolescentPhysicalActivity RecallQuestion-
naire was used for this assessment (3).
Data and analysis. Forthe fundamentalmotorskill
measures, the number of features rated as present or correct
was summed for each subject. For the descriptive reporting
by skill,all features correctwas considered as ‘‘mastery,’’
all butone feature correctas ‘‘nearmastery,’’and more
than one featureincorrectas ‘‘poor.’’ Categoriesof
‘‘mastery’’ and ‘‘near mastery’’ were combined and termed
‘‘advanced skillproficiency’’(5). Each skill(exceptthe
sprint run) was then standardized to a score of 5, and scores
for the six skills were summed to create scores out of 15 for
the three objectcontrol(kick,catch,and overhand throw)
and three locomotorskills (hop,side gallop,and vertical
jump) (27).
Scores for the Multistage Fitness Test were based on the
lastleveland shuttle completed by a student.This result
was converted to the number of laps achieved to create a
continuousvariablefor analysis.We reportcardiorespi-
ratory fitness firstin terms of the number of laps achieved
and secondly afteradjusting forage and gender.We
adjusted levelsusing theCooperInstitutefor Aerobics
Research standards,constructed to ascertain the levelof
cardiorespiratory fitness needed to decrease risk of all-cau
mortality (above 20th percentile formalesand 40th for
females)(8). Each physicalactivity was assigned a MET
value (1 MET = 3.5 mL oxygenIkgj1 body weightj1 Iminj1 )
from a comprehensive list of physical activities (1).As per
the SPANS,activities G10 min in duration,with a MET
value of G3.0, or less than once per week were excluded (
To gain a listof highly reported voluntary out-of-school–
organized sporting activities, ‘‘physical education,’’ ‘‘sport
science,’’ and ‘‘school sport’’ were excluded.
A general linear model in SPSS (SPSS, Inc, Chicago, IL;
http://www.spss.com/)was fitted to examine the relation-
ship between fundamental motor skill proficiency in child-
hood and cardiorespiratory fitness (number of laps achieve
on the MultistageFitnessTest) in adolescence.The
dependentvariable (cardiorespiratory fitness)was square
root-transformed before analysis to normalize its distribu-
tion.The relationship between school grade,gender,child-
hood objectcontrolproficiency and childhood locomotor
proficiency,and fitness in adolescencewas initially
assessed univariately for significance.
Significant variables were included as main effects in the
model.Interactions between significantmotorskill profi-
ciency variablesand genderwereincluded to examine
whetherthe relationships between motorskill proficiency
and fitnessdiffered between maleand femalestudents.
Interaction terms were only retained in the finalmodelif
found significant.Predicted valuesof cardiorespiratory
fitness, on the basis of the model parameter estimates, we
back-transformed from their square root values and plotte
againstthe observed range ofobjectcontrolvariables by
gender (Fig.1).
Because there was only data forhalf the sample (n =
154),a separate linearregression examined the ability of
advanced performance ofthe sprintrun in childhood to
predictcardiorespiratory fitness in adolescence.The rela-
tionship between gender,advanced performanceof the
sprint run,and fitness in adolescence was initially assessed
univariately for significance. School grade was not include
because the sprint run was primarily only assessed for one
grade (grade 4, n = 140; grade 5, n = 14). Univariately, th
sprintrun wasfound notto be a significantpredictor.
However,the sprintrun was stilltested in a modelwith
gender and the interaction term between gender and sprin
run to see ifthe relationship between childhood perform-
anceof the sprintrun and adolescentcardiorespiratory
fitness differed according to gender.
RESULTS
Sample. Of 276 students followed up for the PASS, 234
(84.8%)completed theMultistageFitnessTest. Of 42
nonparticipants, 31 were unwilling to do some aspect of th
CHILDHOOD MOTOR SKILL AND ADOLESCENT FITNESS Medicine & Science in Sports & Exercised 2139
APPLIED SCIENCES
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
testing/surveying.Of 42 nonparticipants,10 provided a
Multistage Fitness Testresultundertaken during physical
education atschoolin the previous 3-month period.These
results were included bringing the total number of students
with fitness results to 244 (88.4%). Slightly more than half
of this sample were females (52.1%,n = 127),with 60.1%
(n = 146) in grade 10 and 39.0% (n = 97) in grade 11.All
but one spoke English at home.
Childhood motor skillproficiency. Nearly all of the
244 students followed up were assessed in the catch,kick,
overhand throw,verticaljump,side gallop,and hop.The
sprint run was only assessed for students in one of the two
schoolgrades (Table 1).Mean composite childhood motor
skill score was 17.7 (SD 5.1).Overall,males were more
proficientwith a mean of19.3 (CI18.4–20.2)compared
with females with a mean of16.4 (CI15.5–17.3).There
were no differences between those originally tested in grade
4 and thosetested in grade5 in terms of childhood
locomotorskill proficiency (t= j0.42, P = 0.677) or
object control skill proficiency (t = j1.36,P = 0.174).
Males were more proficient at performing object control
skills, 11.5 (CI 11.0–12.0), compared with females, 7.9 (CI
7.5–8.4).More malespossessed advanced skillsin the
catch, overhand throw, and kick. More males also possess
advanced skills in the sprint run, which is a locomotor skill
For the otherlocomotorskills, although femalesscored
slightly higherin skill proficiency,this did not reach
significance(8.5 compared with 7.8;t = j1.86, P =
0.064). This pattern was repeated for the vertical jump, sid
gallop,and hop (Table 1).
Cardiorespiratory fitness and sporting partici-
pation in adolescence. The meannumberof laps
completed was50.5 (SD 24.39).Malesachieved higher
cardiorespiratory fitness scores,with a mean of63.4 laps
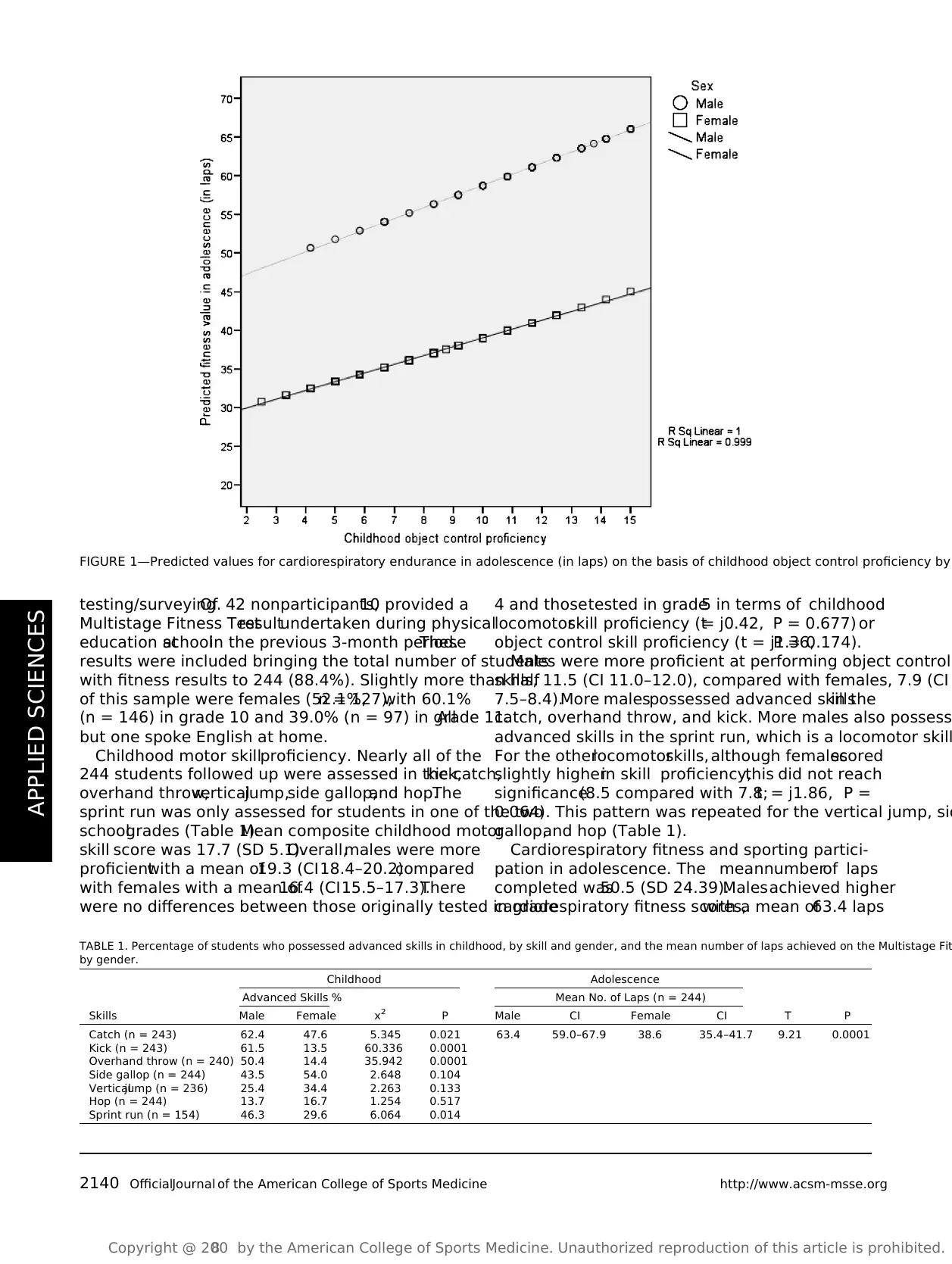
FIGURE 1—Predicted values for cardiorespiratory endurance in adolescence (in laps) on the basis of childhood object control proficiency by
TABLE 1. Percentage of students who possessed advanced skills in childhood, by skill and gender, and the mean number of laps achieved on the Multistage Fit
by gender.
Childhood Adolescence
Advanced Skills % Mean No. of Laps (n = 244)
Skills Male Female x 2 P Male CI Female CI T P
Catch (n = 243) 62.4 47.6 5.345 0.021 63.4 59.0–67.9 38.6 35.4–41.7 9.21 0.0001
Kick (n = 243) 61.5 13.5 60.336 0.0001
Overhand throw (n = 240) 50.4 14.4 35.942 0.0001
Side gallop (n = 244) 43.5 54.0 2.648 0.104
Verticaljump (n = 236) 25.4 34.4 2.263 0.133
Hop (n = 244) 13.7 16.7 1.254 0.517
Sprint run (n = 154) 46.3 29.6 6.064 0.014
http://www.acsm-msse.org2140 OfficialJournal of the American College of Sports Medicine
APPLIED SCIENCES
testing/surveying.Of 42 nonparticipants,10 provided a
Multistage Fitness Testresultundertaken during physical
education atschoolin the previous 3-month period.These
results were included bringing the total number of students
with fitness results to 244 (88.4%). Slightly more than half
of this sample were females (52.1%,n = 127),with 60.1%
(n = 146) in grade 10 and 39.0% (n = 97) in grade 11.All
but one spoke English at home.
Childhood motor skillproficiency. Nearly all of the
244 students followed up were assessed in the catch,kick,
overhand throw,verticaljump,side gallop,and hop.The
sprint run was only assessed for students in one of the two
schoolgrades (Table 1).Mean composite childhood motor
skill score was 17.7 (SD 5.1).Overall,males were more
proficientwith a mean of19.3 (CI18.4–20.2)compared
with females with a mean of16.4 (CI15.5–17.3).There
were no differences between those originally tested in grade
4 and thosetested in grade5 in terms of childhood
locomotorskill proficiency (t= j0.42, P = 0.677) or
object control skill proficiency (t = j1.36,P = 0.174).
Males were more proficient at performing object control
skills, 11.5 (CI 11.0–12.0), compared with females, 7.9 (CI
7.5–8.4).More malespossessed advanced skillsin the
catch, overhand throw, and kick. More males also possess
advanced skills in the sprint run, which is a locomotor skill
For the otherlocomotorskills, although femalesscored
slightly higherin skill proficiency,this did not reach
significance(8.5 compared with 7.8;t = j1.86, P =
0.064). This pattern was repeated for the vertical jump, sid
gallop,and hop (Table 1).
Cardiorespiratory fitness and sporting partici-
pation in adolescence. The meannumberof laps
completed was50.5 (SD 24.39).Malesachieved higher
cardiorespiratory fitness scores,with a mean of63.4 laps
FIGURE 1—Predicted values for cardiorespiratory endurance in adolescence (in laps) on the basis of childhood object control proficiency by
TABLE 1. Percentage of students who possessed advanced skills in childhood, by skill and gender, and the mean number of laps achieved on the Multistage Fit
by gender.
Childhood Adolescence
Advanced Skills % Mean No. of Laps (n = 244)
Skills Male Female x 2 P Male CI Female CI T P
Catch (n = 243) 62.4 47.6 5.345 0.021 63.4 59.0–67.9 38.6 35.4–41.7 9.21 0.0001
Kick (n = 243) 61.5 13.5 60.336 0.0001
Overhand throw (n = 240) 50.4 14.4 35.942 0.0001
Side gallop (n = 244) 43.5 54.0 2.648 0.104
Verticaljump (n = 236) 25.4 34.4 2.263 0.133
Hop (n = 244) 13.7 16.7 1.254 0.517
Sprint run (n = 154) 46.3 29.6 6.064 0.014
http://www.acsm-msse.org2140 OfficialJournal of the American College of Sports Medicine
APPLIED SCIENCES
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
compared with 38.6 laps for females, see Table 1. However,
after adjusting according to the Cooper Institute for Aerobics
Research standards for males and females and different ages
(8),there was no significantdifference between males and
females, with 59.8% of males and 63.0% of females reaching
the specified standard (W2 = 0.260, P = 0.610). There was no
relationship between cardiorespiratory fitnessand school
grade. Students from grade 10 recorded a mean of 49.9 laps
(CI 45.1–53.7)compared with 51.0 (CI45.9–56.1)for
students from grade 11.
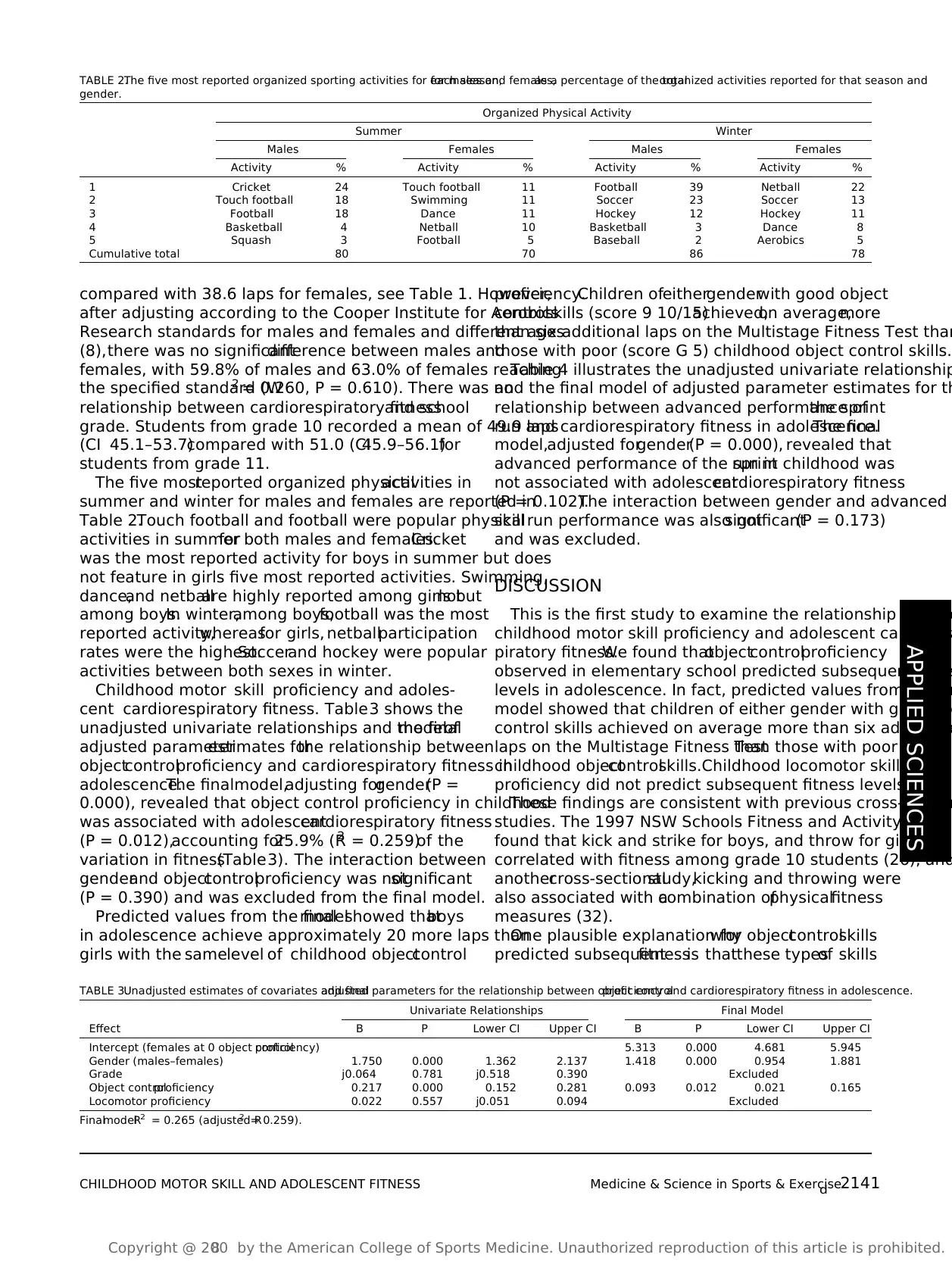
The five mostreported organized physicalactivities in
summer and winter for males and females are reported in
Table 2.Touch football and football were popular physical
activities in summerfor both males and females.Cricket
was the most reported activity for boys in summer but does
not feature in girls five most reported activities. Swimming,
dance,and netballare highly reported among girls butnot
among boys.In winter,among boys,football was the most
reported activity,whereasfor girls, netballparticipation
rates were the highest.Soccerand hockey were popular
activities between both sexes in winter.
Childhood motor skill proficiency and adoles-
cent cardiorespiratory fitness. Table3 shows the
unadjusted univariate relationships and the finalmodelof
adjusted parameterestimates forthe relationship between
objectcontrolproficiency and cardiorespiratory fitness in
adolescence.The finalmodel,adjusting forgender(P =
0.000), revealed that object control proficiency in childhood
was associated with adolescentcardiorespiratory fitness
(P = 0.012),accounting for25.9% (R2 = 0.259)of the
variation in fitness(Table3). The interaction between
genderand objectcontrolproficiency was notsignificant
(P = 0.390) and was excluded from the final model.
Predicted values from the finalmodelshowed thatboys
in adolescence achieve approximately 20 more laps than
girls with the samelevel of childhood objectcontrol
proficiency.Children ofeithergenderwith good object
controlskills (score 9 10/15)achieved,on average,more
than six additional laps on the Multistage Fitness Test than
those with poor (score G 5) childhood object control skills.
Table 4 illustrates the unadjusted univariate relationship
and the final model of adjusted parameter estimates for th
relationship between advanced performance ofthe sprint
run and cardiorespiratory fitness in adolescence.The final
model,adjusted forgender(P = 0.000), revealed that
advanced performance of the sprintrun in childhood was
not associated with adolescentcardiorespiratory fitness
(P = 0.102).The interaction between gender and advanced
skill run performance was also notsignificant(P = 0.173)
and was excluded.
DISCUSSION
This is the first study to examine the relationship betwee
childhood motor skill proficiency and adolescent cardiores
piratory fitness.We found thatobjectcontrolproficiency
observed in elementary school predicted subsequent fitne
levels in adolescence. In fact, predicted values from the fin
model showed that children of either gender with good ob
control skills achieved on average more than six additiona
laps on the Multistage Fitness Testthan those with poor
childhood objectcontrolskills.Childhood locomotor skill
proficiency did not predict subsequent fitness levels.
These findings are consistent with previous cross-section
studies. The 1997 NSW Schools Fitness and Activity Surve
found that kick and strike for boys, and throw for girls, wer
correlated with fitness among grade 10 students (26), and
anothercross-sectionalstudy,kicking and throwing were
also associated with acombination ofphysicalfitness
measures (32).
One plausible explanation forwhy objectcontrolskills
predicted subsequentfitnessis thatthese typesof skills
TABLE 2.The five most reported organized sporting activities for each season,for males and females,as a percentage of the totalorganized activities reported for that season and
gender.
Organized Physical Activity
Summer Winter
Males Females Males Females
Activity % Activity % Activity % Activity %
1 Cricket 24 Touch football 11 Football 39 Netball 22
2 Touch football 18 Swimming 11 Soccer 23 Soccer 13
3 Football 18 Dance 11 Hockey 12 Hockey 11
4 Basketball 4 Netball 10 Basketball 3 Dance 8
5 Squash 3 Football 5 Baseball 2 Aerobics 5
Cumulative total 80 70 86 78
TABLE 3.Unadjusted estimates of covariates and finaladjusted parameters for the relationship between object controlproficiency and cardiorespiratory fitness in adolescence.
Univariate Relationships Final Model
Effect B P Lower CI Upper CI B P Lower CI Upper CI
Intercept (females at 0 object controlproficiency) 5.313 0.000 4.681 5.945
Gender (males–females) 1.750 0.000 1.362 2.137 1.418 0.000 0.954 1.881
Grade j0.064 0.781 j0.518 0.390 Excluded
Object controlproficiency 0.217 0.000 0.152 0.281 0.093 0.012 0.021 0.165
Locomotor proficiency 0.022 0.557 j0.051 0.094 Excluded
FinalmodelR2 = 0.265 (adjusted R2 = 0.259).
CHILDHOOD MOTOR SKILL AND ADOLESCENT FITNESS Medicine & Science in Sports & Exercised 2141
APPLIED SCIENCES
compared with 38.6 laps for females, see Table 1. However,
after adjusting according to the Cooper Institute for Aerobics
Research standards for males and females and different ages
(8),there was no significantdifference between males and
females, with 59.8% of males and 63.0% of females reaching
the specified standard (W2 = 0.260, P = 0.610). There was no
relationship between cardiorespiratory fitnessand school
grade. Students from grade 10 recorded a mean of 49.9 laps
(CI 45.1–53.7)compared with 51.0 (CI45.9–56.1)for
students from grade 11.
The five mostreported organized physicalactivities in
summer and winter for males and females are reported in
Table 2.Touch football and football were popular physical
activities in summerfor both males and females.Cricket
was the most reported activity for boys in summer but does
not feature in girls five most reported activities. Swimming,
dance,and netballare highly reported among girls butnot
among boys.In winter,among boys,football was the most
reported activity,whereasfor girls, netballparticipation
rates were the highest.Soccerand hockey were popular
activities between both sexes in winter.
Childhood motor skill proficiency and adoles-
cent cardiorespiratory fitness. Table3 shows the
unadjusted univariate relationships and the finalmodelof
adjusted parameterestimates forthe relationship between
objectcontrolproficiency and cardiorespiratory fitness in
adolescence.The finalmodel,adjusting forgender(P =
0.000), revealed that object control proficiency in childhood
was associated with adolescentcardiorespiratory fitness
(P = 0.012),accounting for25.9% (R2 = 0.259)of the
variation in fitness(Table3). The interaction between
genderand objectcontrolproficiency was notsignificant
(P = 0.390) and was excluded from the final model.
Predicted values from the finalmodelshowed thatboys
in adolescence achieve approximately 20 more laps than
girls with the samelevel of childhood objectcontrol
proficiency.Children ofeithergenderwith good object
controlskills (score 9 10/15)achieved,on average,more
than six additional laps on the Multistage Fitness Test than
those with poor (score G 5) childhood object control skills.
Table 4 illustrates the unadjusted univariate relationship
and the final model of adjusted parameter estimates for th
relationship between advanced performance ofthe sprint
run and cardiorespiratory fitness in adolescence.The final
model,adjusted forgender(P = 0.000), revealed that
advanced performance of the sprintrun in childhood was
not associated with adolescentcardiorespiratory fitness
(P = 0.102).The interaction between gender and advanced
skill run performance was also notsignificant(P = 0.173)
and was excluded.
DISCUSSION
This is the first study to examine the relationship betwee
childhood motor skill proficiency and adolescent cardiores
piratory fitness.We found thatobjectcontrolproficiency
observed in elementary school predicted subsequent fitne
levels in adolescence. In fact, predicted values from the fin
model showed that children of either gender with good ob
control skills achieved on average more than six additiona
laps on the Multistage Fitness Testthan those with poor
childhood objectcontrolskills.Childhood locomotor skill
proficiency did not predict subsequent fitness levels.
These findings are consistent with previous cross-section
studies. The 1997 NSW Schools Fitness and Activity Surve
found that kick and strike for boys, and throw for girls, wer
correlated with fitness among grade 10 students (26), and
anothercross-sectionalstudy,kicking and throwing were
also associated with acombination ofphysicalfitness
measures (32).
One plausible explanation forwhy objectcontrolskills
predicted subsequentfitnessis thatthese typesof skills
TABLE 2.The five most reported organized sporting activities for each season,for males and females,as a percentage of the totalorganized activities reported for that season and
gender.
Organized Physical Activity
Summer Winter
Males Females Males Females
Activity % Activity % Activity % Activity %
1 Cricket 24 Touch football 11 Football 39 Netball 22
2 Touch football 18 Swimming 11 Soccer 23 Soccer 13
3 Football 18 Dance 11 Hockey 12 Hockey 11
4 Basketball 4 Netball 10 Basketball 3 Dance 8
5 Squash 3 Football 5 Baseball 2 Aerobics 5
Cumulative total 80 70 86 78
TABLE 3.Unadjusted estimates of covariates and finaladjusted parameters for the relationship between object controlproficiency and cardiorespiratory fitness in adolescence.
Univariate Relationships Final Model
Effect B P Lower CI Upper CI B P Lower CI Upper CI
Intercept (females at 0 object controlproficiency) 5.313 0.000 4.681 5.945
Gender (males–females) 1.750 0.000 1.362 2.137 1.418 0.000 0.954 1.881
Grade j0.064 0.781 j0.518 0.390 Excluded
Object controlproficiency 0.217 0.000 0.152 0.281 0.093 0.012 0.021 0.165
Locomotor proficiency 0.022 0.557 j0.051 0.094 Excluded
FinalmodelR2 = 0.265 (adjusted R2 = 0.259).
CHILDHOOD MOTOR SKILL AND ADOLESCENT FITNESS Medicine & Science in Sports & Exercised 2141
APPLIED SCIENCES

Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
(kicking,throwing,and catching) are often associated with
physical activity experiences of a moderate and/or vigorous
intensity (such as recreationalor organized sports training
and competition) (30).Thus,students who are proficient at
performing these skills may participate more in the type of
activities likely to increase fitness levels.This is supported
by the type of organized sporting activities most reported in
the currentstudy.Of the sports reported by males in both
summer and winter, all centered on object control skill ability
(cricket,football,basketball,squash,soccer,hockey,and
baseball). For girls, highly reported activities also benefit from
object control skill proficiency (football, netball, soccer, and
hockey). Dance and aerobics, which primarily use locomotor
skills, were also reported by girls but only constituted 13% of
the organized activities in winter.Physical activity opportu-
nitiesof adolescentsmay thusbe increased ifthey are
competent at performing many prerequisite sports skills that
may be associated with training and competition that develop
cardiorespiratory fitness.
Our findingsdid not supportpreviouscross-sectional
research thathas found an association between locomotor
skill proficiency and fitness.The 1997 NSW Schools
Fitness and PhysicalActivity Survey found thatthe sprint
run and the jump were associated with fitness (26),and a
study tracking a smallgroup ofchildren overtime found
thatchildren with low locomotor competence (in the run,
broad jump,and balance)performed less welleach year
than children with high motor competence on both fitness
and motor skill competency measures (14). The same skills
were measured with the same instrument in the PASS study
as in the NSW SchoolsFitnessand PhysicalActivity
Survey,so it is surprising thatthe sprintrun wasnot
predictive offitness in ourstudy.Because the Multistage
Fitness Test is a cardiorespiratory test involving running, it
mightbe expected thatthis skill would relate to fitness
measured in thisway (26). However,process-oriented
motor skill assessments which assess technique (as opposed
to speed or endurance) may not relate as expected to fitness
as measured by theMultistageFitnessTest.It is also
possible thatbecause we had a reduced sample forthis
analysis,a largersample would have provided different
results.Lastly,the run is reported to have a low reliability
estimate (alpha coefficientmethod,r = 0.17) (9),possibly
indicating thatassessmentfor the sprintrun is not as
accurate with this instrument.
An importantfinding ofour study wasthat26% of
variancein adolescentcardiorespiratoryfitness was
explained by childhood objectcontrolproficiency.By
comparison,the 1997 NSW Schools Fitness and Physical
Activity Survey found thatthe battery ofsix skills (four
being objectcontrol) assessed in grade 10 girls explained
28% of variance in fitness,whereas for boys,this measure
only accounted for18% (26).Even by adolescence,very
few girls have reached proficiency in objectcontrolskills
(only 20% of girls in grade 10 have advanced skills in the
kick and overhand throw (4)). These findings suggest that
a girl possesses these skills in adolescence,the influence
may be stronger on physical activity and subsequent fitne
than for a boy. However, this study was cross-sectional, an
our findingsprovide additionalinsightinto the potential
long-term influence offundamentalmotorskill develop-
ment in childhood on health-related behaviors later in life.
Consistentwith otherstudies (19),we also found that
boys completed more lapsthan girlson the Multistage
FitnessTest. We also found thatboys in adolescence
achieved approximately 20 more lapson the Multistage
Fitness Testthan girls with the same levelof childhood
object controlproficiency.However,the relationship
between childhood objectcontrolproficiency and adoles-
centcardiorespiratory fitness did notdifferby gender.In
otherwords,higherskill in childhood predicted higher
fitness in adolescent for both males and females. Also, afte
adjusting according to standards proposed by the Cooper
Institute for Aerobics Research,there were no differences
between the proportion of males and females thatreached
the required standard offitness(girls according to this
standard are not expected to reach the same level of fitne
of boys).The proportion of boys (60%) and girls (63%) in
the PASS who reached criterion standards ofcardiorespi-
ratory fitness associated with health benefits was compara
ble to that found in representative studies in the Australia
population (67% for boys and 63% for girls in the Schools
Physical Activity and Nutrition Study (4)).
Our study hasindicated thata skill-oriented focusin
childhood may help to address health-related concerns in
later life through the promotion of cardiorespiratory fitnes
in adolescence.Assisting children to become competent
and confident performers of object control or sports-relate
skills may lead to a greaterwillingness to participate in
competitiveand noncompetitivesporting activitiesthat
provide opportunities to improve fitness levels.In partic-
ular,our findings suggestthatobjectcontrolskills should
be targeted through school and community interventions a
a key strategy in promoting subsequentcardiorespiratory
fitness. It is important that such skills are taught during th
primary orelementary schoolyears as children are atan
TABLE 4.Unadjusted estimates ofcovariates and finaladjusted parameters for the relationship between advanced performance ofthe sprintrun and cardiorespiratory fitness in
adolescence.
Univariate Relationships Final Model
Effect B P Lower CI Upper CI B P Lower CI Upper CI
Intercept (females at 0 proficiency) 6.569 0.000 5.926 7.212
Gender (males–females) 1.750 0.000 1.362 2.137 1.568 0.000 1.073 2.063
Advanced performance of sprint run 0.639 0.084 j0.088 1.365 0.542 0.102 j0.108 1.191
FinalmodelR2 = 0.221 (adjusted R2 = 0.211).
http://www.acsm-msse.org2142 OfficialJournal of the American College of Sports Medicine
APPLIED SCIENCES
(kicking,throwing,and catching) are often associated with
physical activity experiences of a moderate and/or vigorous
intensity (such as recreationalor organized sports training
and competition) (30).Thus,students who are proficient at
performing these skills may participate more in the type of
activities likely to increase fitness levels.This is supported
by the type of organized sporting activities most reported in
the currentstudy.Of the sports reported by males in both
summer and winter, all centered on object control skill ability
(cricket,football,basketball,squash,soccer,hockey,and
baseball). For girls, highly reported activities also benefit from
object control skill proficiency (football, netball, soccer, and
hockey). Dance and aerobics, which primarily use locomotor
skills, were also reported by girls but only constituted 13% of
the organized activities in winter.Physical activity opportu-
nitiesof adolescentsmay thusbe increased ifthey are
competent at performing many prerequisite sports skills that
may be associated with training and competition that develop
cardiorespiratory fitness.
Our findingsdid not supportpreviouscross-sectional
research thathas found an association between locomotor
skill proficiency and fitness.The 1997 NSW Schools
Fitness and PhysicalActivity Survey found thatthe sprint
run and the jump were associated with fitness (26),and a
study tracking a smallgroup ofchildren overtime found
thatchildren with low locomotor competence (in the run,
broad jump,and balance)performed less welleach year
than children with high motor competence on both fitness
and motor skill competency measures (14). The same skills
were measured with the same instrument in the PASS study
as in the NSW SchoolsFitnessand PhysicalActivity
Survey,so it is surprising thatthe sprintrun wasnot
predictive offitness in ourstudy.Because the Multistage
Fitness Test is a cardiorespiratory test involving running, it
mightbe expected thatthis skill would relate to fitness
measured in thisway (26). However,process-oriented
motor skill assessments which assess technique (as opposed
to speed or endurance) may not relate as expected to fitness
as measured by theMultistageFitnessTest.It is also
possible thatbecause we had a reduced sample forthis
analysis,a largersample would have provided different
results.Lastly,the run is reported to have a low reliability
estimate (alpha coefficientmethod,r = 0.17) (9),possibly
indicating thatassessmentfor the sprintrun is not as
accurate with this instrument.
An importantfinding ofour study wasthat26% of
variancein adolescentcardiorespiratoryfitness was
explained by childhood objectcontrolproficiency.By
comparison,the 1997 NSW Schools Fitness and Physical
Activity Survey found thatthe battery ofsix skills (four
being objectcontrol) assessed in grade 10 girls explained
28% of variance in fitness,whereas for boys,this measure
only accounted for18% (26).Even by adolescence,very
few girls have reached proficiency in objectcontrolskills
(only 20% of girls in grade 10 have advanced skills in the
kick and overhand throw (4)). These findings suggest that
a girl possesses these skills in adolescence,the influence
may be stronger on physical activity and subsequent fitne
than for a boy. However, this study was cross-sectional, an
our findingsprovide additionalinsightinto the potential
long-term influence offundamentalmotorskill develop-
ment in childhood on health-related behaviors later in life.
Consistentwith otherstudies (19),we also found that
boys completed more lapsthan girlson the Multistage
FitnessTest. We also found thatboys in adolescence
achieved approximately 20 more lapson the Multistage
Fitness Testthan girls with the same levelof childhood
object controlproficiency.However,the relationship
between childhood objectcontrolproficiency and adoles-
centcardiorespiratory fitness did notdifferby gender.In
otherwords,higherskill in childhood predicted higher
fitness in adolescent for both males and females. Also, afte
adjusting according to standards proposed by the Cooper
Institute for Aerobics Research,there were no differences
between the proportion of males and females thatreached
the required standard offitness(girls according to this
standard are not expected to reach the same level of fitne
of boys).The proportion of boys (60%) and girls (63%) in
the PASS who reached criterion standards ofcardiorespi-
ratory fitness associated with health benefits was compara
ble to that found in representative studies in the Australia
population (67% for boys and 63% for girls in the Schools
Physical Activity and Nutrition Study (4)).
Our study hasindicated thata skill-oriented focusin
childhood may help to address health-related concerns in
later life through the promotion of cardiorespiratory fitnes
in adolescence.Assisting children to become competent
and confident performers of object control or sports-relate
skills may lead to a greaterwillingness to participate in
competitiveand noncompetitivesporting activitiesthat
provide opportunities to improve fitness levels.In partic-
ular,our findings suggestthatobjectcontrolskills should
be targeted through school and community interventions a
a key strategy in promoting subsequentcardiorespiratory
fitness. It is important that such skills are taught during th
primary orelementary schoolyears as children are atan
TABLE 4.Unadjusted estimates ofcovariates and finaladjusted parameters for the relationship between advanced performance ofthe sprintrun and cardiorespiratory fitness in
adolescence.
Univariate Relationships Final Model
Effect B P Lower CI Upper CI B P Lower CI Upper CI
Intercept (females at 0 proficiency) 6.569 0.000 5.926 7.212
Gender (males–females) 1.750 0.000 1.362 2.137 1.568 0.000 1.073 2.063
Advanced performance of sprint run 0.639 0.084 j0.088 1.365 0.542 0.102 j0.108 1.191
FinalmodelR2 = 0.221 (adjusted R2 = 0.211).
http://www.acsm-msse.org2142 OfficialJournal of the American College of Sports Medicine
APPLIED SCIENCES
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
optimalage in terms of motorskill learning (13).In
addition,improving the object control skills of girls should
be a priority because many girls lack proficiency in these
skills (4), even by late adolescence.Existing school
physical educationand sport programsmay not be
sufficiently catering forgirls who arenot proficientat
performing sports-related skills.
In the currentclimate of childhood obesity concerns,it
has been suggested thatschoolphysicaleducation classes
are an effective forum to increase physicalactivity and
fitnesslevels (18).Our findings suggestthata balanced
approach forteaching (and developing)both skill and
health-related fitness components is important.The Move
It Groove Itintervention managed to increase fundamental
skill proficiency in physicaleducation lessonswithout
sacrificing physicalactivity (34),and the SPARK inter-
ventionreported substantialimprovementsin physical
activity levelswith a physicaleducation curriculum that
targeted both thedevelopmentof motorskills and the
improvementsin health-related fitness(31).A continued
challenge forphysicaleducatorsis not only to increase
object skill proficiency levels, particularly for girls, but also
to increase health-related fitnesscomponentsamong stu-
dents in physical education lessons.
LIMITATIONS
Although there was little evidence of bias,our findings
should be considered in the lightof a follow-up rate of
one third.This was unavoidable due to the length ofthe
follow-up period and the difficulties locating students who
had moved between regionsor schools.However,the
consentrate in PASS was higherthan forsimilarstudies
(4). Although there were some differences in grade between
consenters and nonconsenters, the reason for lower consent
in grade 11 wasdue to lessstudentsof this age being
located (students of this age in Australia can legally leave
school). There was also no differential loss to follow-up by
gender; however, there was a difference in mean composi
childhood skillscore,suggesting thatfollowed-up students
may have been potentially more skilled.However,because
the difference was only 1 point on a 30-point scale,loss to
follow-up is unlikely to have biased ourfindings in any
substantialway.In addition,maturation (13)and weight
status (25)were notcontrolled for,both factors thatcan
effectmotorskill performance.Moreover,it would have
been preferable to have had a complete data setfor the
sprint run to further explore whether locomotor skills can b
predictive of fitness.
CONCLUSION
This study has shown that object control skill proficiency
developed in primary school years has a strong influence o
subsequentfitness in adolescence.Its strengths include a
longitudinalcohortdesign,a valid and reliable measure of
cardiorespiratory fitness, a good sample size, and the use
a comprehensive battery ofmotorskills,divided between
locomotorand objectcontrol.Our findingssuggestthat
community and school-based interventions should conside
motorskill developmentas a key strategy in promoting
cardiorespiratory fitness.Promoting theachievementof
cardiorespiratory fitness among youth,notsimply physical
activity participation,has tangible health benefits for later
adultlife. Programsthatbalanceskill acquisition with
health-related physical activity are important. Object cont
skills should be a key skill focus,particularly for girls,be-
cause these skills are predictive of cardiorespiratory fitnes
The authors thank Dr.MichaelBooth for inputinto the original
study design, the research assistants, and importantly, the students,
teachers,and schools forparticipating.The study was funded by
the NSW Health Australia and Sydney University (Departmentof
RuralHealth—Northern Rivers). The results of the present study do
not constitute endorsement by ACSM.
REFERENCES
1. Ainsworth BE,Jacobs DR,Leon AS.Compendium ofphysical
activities:classificationof energycosts of humanphysical
activities.Med Sci Sports Exerc.1993;25(1):71–80.
2. Ara I, Vicente-Rodriguez G,Perez-Gomez J,et al. Influence of
extracurricular sportactivities on body composition and physical
fitness in boys: a 3-year longitudinal study.Int J Obes.2006;30:
1062–71.
3. Booth M, Okely AD, Chey T, Bauman A.The reliability and
validity of the Adolescent Physical Activity Recall Questionnaire.
Med Sci Sports Exerc.2002;34(12):1986–95.
4. Booth M, Okely AD, Denney-Wilson E,Hardy L, Yang B,
Dobbins T.NSW Schools PhysicalActivity and Nutrition Survey
(SPANS).Sydney (Australia): NSW Department of Health; 2006.
p. 253–4.
5. Booth M, Denney-Wilson LE, Okely AD, Hardy LL. Methods of
the NSW Schools PhysicalActivity and Nutrition Survey.J Sci
Med Sport.2005;8:284–93.
6. Branta C,HaubenstrickerJ, SeefeldtV. Age changes in motor
skills during childhood and adolescence.Exerc SportSci Rev.
1984;12:467–520.
7. Church TS, Earnest CP, Skinner JS, Blair SN. Effects of different
dosesof physicalactivity on cardiorespiratory fitnessamong
sedentary,overweightor obesepostmenopausalwomen with
elevated blood pressure:a randomized controlled trial.JAMA.
2007;297:2081–91.
8. CooperInstitutefor AerobicsResearch.FITNESSGRAM Test
AdministrationManual. 2nd ed. Champaign(IL): Human
Kinetics; 1999.p. 33–9.
9. Departmentof Education Victoria.FundamentalMotor Skills: A
Manualfor Classroom Teachers.Melbourne (Australia):Depart-
ment of Education; 1996.p. Appendix C 45.
10. Docherty D.Field testand testbatteries.In: Docherty D,editor.
Measurementin Pediatric ExerciseScience.Champaign (IL):
Human Kinetics; 1996.p. 285–334.
CHILDHOOD MOTOR SKILL AND ADOLESCENT FITNESS Medicine & Science in Sports & Exercised 2143
APPLIED SCIENCES
optimalage in terms of motorskill learning (13).In
addition,improving the object control skills of girls should
be a priority because many girls lack proficiency in these
skills (4), even by late adolescence.Existing school
physical educationand sport programsmay not be
sufficiently catering forgirls who arenot proficientat
performing sports-related skills.
In the currentclimate of childhood obesity concerns,it
has been suggested thatschoolphysicaleducation classes
are an effective forum to increase physicalactivity and
fitnesslevels (18).Our findings suggestthata balanced
approach forteaching (and developing)both skill and
health-related fitness components is important.The Move
It Groove Itintervention managed to increase fundamental
skill proficiency in physicaleducation lessonswithout
sacrificing physicalactivity (34),and the SPARK inter-
ventionreported substantialimprovementsin physical
activity levelswith a physicaleducation curriculum that
targeted both thedevelopmentof motorskills and the
improvementsin health-related fitness(31).A continued
challenge forphysicaleducatorsis not only to increase
object skill proficiency levels, particularly for girls, but also
to increase health-related fitnesscomponentsamong stu-
dents in physical education lessons.
LIMITATIONS
Although there was little evidence of bias,our findings
should be considered in the lightof a follow-up rate of
one third.This was unavoidable due to the length ofthe
follow-up period and the difficulties locating students who
had moved between regionsor schools.However,the
consentrate in PASS was higherthan forsimilarstudies
(4). Although there were some differences in grade between
consenters and nonconsenters, the reason for lower consent
in grade 11 wasdue to lessstudentsof this age being
located (students of this age in Australia can legally leave
school). There was also no differential loss to follow-up by
gender; however, there was a difference in mean composi
childhood skillscore,suggesting thatfollowed-up students
may have been potentially more skilled.However,because
the difference was only 1 point on a 30-point scale,loss to
follow-up is unlikely to have biased ourfindings in any
substantialway.In addition,maturation (13)and weight
status (25)were notcontrolled for,both factors thatcan
effectmotorskill performance.Moreover,it would have
been preferable to have had a complete data setfor the
sprint run to further explore whether locomotor skills can b
predictive of fitness.
CONCLUSION
This study has shown that object control skill proficiency
developed in primary school years has a strong influence o
subsequentfitness in adolescence.Its strengths include a
longitudinalcohortdesign,a valid and reliable measure of
cardiorespiratory fitness, a good sample size, and the use
a comprehensive battery ofmotorskills,divided between
locomotorand objectcontrol.Our findingssuggestthat
community and school-based interventions should conside
motorskill developmentas a key strategy in promoting
cardiorespiratory fitness.Promoting theachievementof
cardiorespiratory fitness among youth,notsimply physical
activity participation,has tangible health benefits for later
adultlife. Programsthatbalanceskill acquisition with
health-related physical activity are important. Object cont
skills should be a key skill focus,particularly for girls,be-
cause these skills are predictive of cardiorespiratory fitnes
The authors thank Dr.MichaelBooth for inputinto the original
study design, the research assistants, and importantly, the students,
teachers,and schools forparticipating.The study was funded by
the NSW Health Australia and Sydney University (Departmentof
RuralHealth—Northern Rivers). The results of the present study do
not constitute endorsement by ACSM.
REFERENCES
1. Ainsworth BE,Jacobs DR,Leon AS.Compendium ofphysical
activities:classificationof energycosts of humanphysical
activities.Med Sci Sports Exerc.1993;25(1):71–80.
2. Ara I, Vicente-Rodriguez G,Perez-Gomez J,et al. Influence of
extracurricular sportactivities on body composition and physical
fitness in boys: a 3-year longitudinal study.Int J Obes.2006;30:
1062–71.
3. Booth M, Okely AD, Chey T, Bauman A.The reliability and
validity of the Adolescent Physical Activity Recall Questionnaire.
Med Sci Sports Exerc.2002;34(12):1986–95.
4. Booth M, Okely AD, Denney-Wilson E,Hardy L, Yang B,
Dobbins T.NSW Schools PhysicalActivity and Nutrition Survey
(SPANS).Sydney (Australia): NSW Department of Health; 2006.
p. 253–4.
5. Booth M, Denney-Wilson LE, Okely AD, Hardy LL. Methods of
the NSW Schools PhysicalActivity and Nutrition Survey.J Sci
Med Sport.2005;8:284–93.
6. Branta C,HaubenstrickerJ, SeefeldtV. Age changes in motor
skills during childhood and adolescence.Exerc SportSci Rev.
1984;12:467–520.
7. Church TS, Earnest CP, Skinner JS, Blair SN. Effects of different
dosesof physicalactivity on cardiorespiratory fitnessamong
sedentary,overweightor obesepostmenopausalwomen with
elevated blood pressure:a randomized controlled trial.JAMA.
2007;297:2081–91.
8. CooperInstitutefor AerobicsResearch.FITNESSGRAM Test
AdministrationManual. 2nd ed. Champaign(IL): Human
Kinetics; 1999.p. 33–9.
9. Departmentof Education Victoria.FundamentalMotor Skills: A
Manualfor Classroom Teachers.Melbourne (Australia):Depart-
ment of Education; 1996.p. Appendix C 45.
10. Docherty D.Field testand testbatteries.In: Docherty D,editor.
Measurementin Pediatric ExerciseScience.Champaign (IL):
Human Kinetics; 1996.p. 285–334.
CHILDHOOD MOTOR SKILL AND ADOLESCENT FITNESS Medicine & Science in Sports & Exercised 2143
APPLIED SCIENCES
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Copyright @ 200 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.8
11. Dollman J,Olds T.Distributionalchanges in the performance of
Australian children on tests ofcardiorespiratory endurance.In:
Tomkinson GR,Olds TS, editors.PediatricFitness,Secular
Trends and Geographic Variability. Med Sport Sci. Basel, Karger,
2007; Vol.50,p. 210–25.
12. Eisenmann JC,Wickel EE, Welk GJ, Blair SN. Relationship
between adolescent fitness and fatness and cardiovascular disease
risk factors in adulthood: the Aerobics Center Longitudinal Study
(ACLS). Am Heart J.2005;149:46–53.
13. Gabbard C.Lifelong Motor Development.Dubuque (IA): Brown,
W.C.; 1992.p. 312.
14. Hands B.Changes in motorskill and fitness measures among
children with high and low motorcompetence:a five-year
longitudinal study.J Sci Med Sport.2008;11:155–62.
15. Haubenstricker J,SeefeldtV. Acquisition of motor skills during
childhood. In: Reston V, editor. Physical Activity and Well-Being.
Reston (VA): AAHPERD; 1986.p. 41–92.
16. Hurtig-Wennlof A,Ruiz JR, Harro M,Sjostrom M.Cardiorespi-
ratory fitnessrelatesmorestrongly than physicalactivity to
cardiovasculardiseaserisk factorsin healthychildrenand
adolescents: the European Youth Health Study. Eur J Cardiovasc
Prev Rehabil.2007;14:575–81.
17. Jones RA,Okely AD,Collins CE,et al. The HIKCUPS trial:a
multi-siterandomized controlled trialof a combined physical
activity skill–developmentand dietary modification program in
overweightand obesechildren.BMC Public Health.2007;7:
1471–2458.
18. Kahn EB,Ramsey LT,Brownson RC,et al.The effectiveness of
interventions to increase physicalactivity.A systematic review.
Am J Prev Med.2002;22:73–107.
19. Keller BA. State ofthe artreviews:developmentof fitness in
children:the influence ofgenderand physicalactivity.Am J
Lifestyle Med.2008;2:58–74.
20. Leger LA, Lambert J. A maximal multistage 20-m shuttle run test
to predict V˙O2 max.Eur J Appl Physiol.1982;49:1–12.
21. Malina RM.Tracking of physical fitness and performance during
growth. In: Buenen G, Hesquiere JG, Reybrouck T, Claessens AL,
editors.Children and Exercise.Stuttgart(Germany):Ferdinand
Enke; 1990.p. 1–10.
22. McKenzieTL, Sallis JF, BroylesSL, Zive MM, NaderPR.
Childhood movementskills: predictorsof physicalactivity in
Anglo American and Mexican American adolescents?Res Q
Exerc Sport.2002;73:238–44.
23. Myers J, Kaykha A, George S,et al. Fitnessversusphysical
activity patternsin predicting mortality in men.Am J Med.
2004;117:912–8.
24. Okely AD, Booth M.Mastery offundamentalmovementskills
among children in New South Wales: prevalence and sociodemo-
graphic distribution.J Sci Med Sport.2004;7:358–72.
25. Okely AD, Booth M, Chey T. Relationshipbetweenbody
composition and fundamentalmovementskills among children
and adolescents.Res Q Exerc Sport.2004;75:238–47.
26. Okely AD, Booth M, Patterson J.Relationship ofcardiorespi-
ratory enduranceto fundamentalmovementskill proficiency
among adolescents.Pediatr Exerc Sci.2001;13:380–391.
27. Okely AD, Booth M, Patterson JW.Relationship ofphysical
activity to fundamental movement skills among adolescents.Med
Sci Sports Exerc.2001;33:1899–904.
28. Okely AD, Booth ML. The developmentand validation ofan
instrumentto assesschildren_sfundamentalmovementskill
ability.In: Pre-OlympicCongress:InternationalCongresson
Sport Science, Sports Medicine and Physical Education; 2000 Sep
7–12:Brisbane (Australia).Queensland University ofTechnol-
ogy; 2000.p. 245.
29. Ortega FB, Ruiz JR, Castillo MJ, Sjostrom M. Physical fitness in
childhood and adolescence: a powerful marker of health.Pediatr
Rev.2008;32:1–11.
30. Raudsepp L, Pall P. The relationship between fundamental motor
skills and outside-schoolphysicalactivity ofelementary school
children.Pediatr Exerc Sci.2006;18:426–35.
31. Sallis JF, McKenzie TL, Alcaraz JE, Kolody B, Faucett N, Hovell
MF. The effects of a 2-year physical education program (SPARK)
on physicalactivity and fitness in elementary schoolstudents.
Sports,play and active recreation for kids.Am J Public Health.
1997;87:1328–34.
32. StoddenDF, LangendorferSJ, RobertonMA, Kelbley L.
Association between motorskill competence and health-related
physical fitness.J Sport Exerc Psychol.2007;29:S45.
33. Twisk J, KemperHCG, SnelJ. Tracking ofcardiovascularrisk
factors in relation to lifestyle. In: Kemper K, editor. The Amsterdam
Growth Study:A LongitudinalAnalysisof Health Fitness,and
Lifestyle. Champaign (IL): Human Kinetics; 1995. p. 203–24.
34. van Beurden E,BarnettLM, Zask A,Dietrich UC,Brooks LO,
Beard J. Can we skill and activatechildren through primary
schoolphysicaleducation lessons?‘‘Move it GrooveIt’’—a
collaborative health promotion intervention.Prev Med.2003;36:
493–501.
35. van Beurden E,Zask A,BarnettLM, Dietrich UC.Fundamental
movement skills—how do primary school children perform? The
FMove It Groove It_ program in rural Australia.J Sci Med Sport.
2002;5:244–52.
36. Van Mechelen W,Kemper HCG.Body growth,body composi-
tion,and physicalfitness.In: Kemper K,editor.The Amsterdam
Growth Study:A LongitudinalAnalysis ofHealth,Fitness,and
Lifestyle.Champaign (IL): Human Kinetics; 1995.p. 52–85.
37. Wrotniak B, Epstein HLH, Dorn JM, Jones KE, Kondilis VA. The
relationship between motorproficiency and physicalactivity in
children.Pediatrics.2006;118:1758–65.
http://www.acsm-msse.org2144 OfficialJournal of the American College of Sports Medicine
APPLIED SCIENCES
11. Dollman J,Olds T.Distributionalchanges in the performance of
Australian children on tests ofcardiorespiratory endurance.In:
Tomkinson GR,Olds TS, editors.PediatricFitness,Secular
Trends and Geographic Variability. Med Sport Sci. Basel, Karger,
2007; Vol.50,p. 210–25.
12. Eisenmann JC,Wickel EE, Welk GJ, Blair SN. Relationship
between adolescent fitness and fatness and cardiovascular disease
risk factors in adulthood: the Aerobics Center Longitudinal Study
(ACLS). Am Heart J.2005;149:46–53.
13. Gabbard C.Lifelong Motor Development.Dubuque (IA): Brown,
W.C.; 1992.p. 312.
14. Hands B.Changes in motorskill and fitness measures among
children with high and low motorcompetence:a five-year
longitudinal study.J Sci Med Sport.2008;11:155–62.
15. Haubenstricker J,SeefeldtV. Acquisition of motor skills during
childhood. In: Reston V, editor. Physical Activity and Well-Being.
Reston (VA): AAHPERD; 1986.p. 41–92.
16. Hurtig-Wennlof A,Ruiz JR, Harro M,Sjostrom M.Cardiorespi-
ratory fitnessrelatesmorestrongly than physicalactivity to
cardiovasculardiseaserisk factorsin healthychildrenand
adolescents: the European Youth Health Study. Eur J Cardiovasc
Prev Rehabil.2007;14:575–81.
17. Jones RA,Okely AD,Collins CE,et al. The HIKCUPS trial:a
multi-siterandomized controlled trialof a combined physical
activity skill–developmentand dietary modification program in
overweightand obesechildren.BMC Public Health.2007;7:
1471–2458.
18. Kahn EB,Ramsey LT,Brownson RC,et al.The effectiveness of
interventions to increase physicalactivity.A systematic review.
Am J Prev Med.2002;22:73–107.
19. Keller BA. State ofthe artreviews:developmentof fitness in
children:the influence ofgenderand physicalactivity.Am J
Lifestyle Med.2008;2:58–74.
20. Leger LA, Lambert J. A maximal multistage 20-m shuttle run test
to predict V˙O2 max.Eur J Appl Physiol.1982;49:1–12.
21. Malina RM.Tracking of physical fitness and performance during
growth. In: Buenen G, Hesquiere JG, Reybrouck T, Claessens AL,
editors.Children and Exercise.Stuttgart(Germany):Ferdinand
Enke; 1990.p. 1–10.
22. McKenzieTL, Sallis JF, BroylesSL, Zive MM, NaderPR.
Childhood movementskills: predictorsof physicalactivity in
Anglo American and Mexican American adolescents?Res Q
Exerc Sport.2002;73:238–44.
23. Myers J, Kaykha A, George S,et al. Fitnessversusphysical
activity patternsin predicting mortality in men.Am J Med.
2004;117:912–8.
24. Okely AD, Booth M.Mastery offundamentalmovementskills
among children in New South Wales: prevalence and sociodemo-
graphic distribution.J Sci Med Sport.2004;7:358–72.
25. Okely AD, Booth M, Chey T. Relationshipbetweenbody
composition and fundamentalmovementskills among children
and adolescents.Res Q Exerc Sport.2004;75:238–47.
26. Okely AD, Booth M, Patterson J.Relationship ofcardiorespi-
ratory enduranceto fundamentalmovementskill proficiency
among adolescents.Pediatr Exerc Sci.2001;13:380–391.
27. Okely AD, Booth M, Patterson JW.Relationship ofphysical
activity to fundamental movement skills among adolescents.Med
Sci Sports Exerc.2001;33:1899–904.
28. Okely AD, Booth ML. The developmentand validation ofan
instrumentto assesschildren_sfundamentalmovementskill
ability.In: Pre-OlympicCongress:InternationalCongresson
Sport Science, Sports Medicine and Physical Education; 2000 Sep
7–12:Brisbane (Australia).Queensland University ofTechnol-
ogy; 2000.p. 245.
29. Ortega FB, Ruiz JR, Castillo MJ, Sjostrom M. Physical fitness in
childhood and adolescence: a powerful marker of health.Pediatr
Rev.2008;32:1–11.
30. Raudsepp L, Pall P. The relationship between fundamental motor
skills and outside-schoolphysicalactivity ofelementary school
children.Pediatr Exerc Sci.2006;18:426–35.
31. Sallis JF, McKenzie TL, Alcaraz JE, Kolody B, Faucett N, Hovell
MF. The effects of a 2-year physical education program (SPARK)
on physicalactivity and fitness in elementary schoolstudents.
Sports,play and active recreation for kids.Am J Public Health.
1997;87:1328–34.
32. StoddenDF, LangendorferSJ, RobertonMA, Kelbley L.
Association between motorskill competence and health-related
physical fitness.J Sport Exerc Psychol.2007;29:S45.
33. Twisk J, KemperHCG, SnelJ. Tracking ofcardiovascularrisk
factors in relation to lifestyle. In: Kemper K, editor. The Amsterdam
Growth Study:A LongitudinalAnalysisof Health Fitness,and
Lifestyle. Champaign (IL): Human Kinetics; 1995. p. 203–24.
34. van Beurden E,BarnettLM, Zask A,Dietrich UC,Brooks LO,
Beard J. Can we skill and activatechildren through primary
schoolphysicaleducation lessons?‘‘Move it GrooveIt’’—a
collaborative health promotion intervention.Prev Med.2003;36:
493–501.
35. van Beurden E,Zask A,BarnettLM, Dietrich UC.Fundamental
movement skills—how do primary school children perform? The
FMove It Groove It_ program in rural Australia.J Sci Med Sport.
2002;5:244–52.
36. Van Mechelen W,Kemper HCG.Body growth,body composi-
tion,and physicalfitness.In: Kemper K,editor.The Amsterdam
Growth Study:A LongitudinalAnalysis ofHealth,Fitness,and
Lifestyle.Champaign (IL): Human Kinetics; 1995.p. 52–85.
37. Wrotniak B, Epstein HLH, Dorn JM, Jones KE, Kondilis VA. The
relationship between motorproficiency and physicalactivity in
children.Pediatrics.2006;118:1758–65.
http://www.acsm-msse.org2144 OfficialJournal of the American College of Sports Medicine
APPLIED SCIENCES
1 out of 8
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.