Clinical Judgment & Reasoning: Asthma Case Study & Care Planning
VerifiedAdded on 2023/06/12
|15
|3705
|498
Case Study
AI Summary
This case study presents a clinical reasoning exercise focused on a 32-year-old female patient, Lucy, with a history of asthma. The analysis includes the sequencing of a proposed health assessment, emphasizing the importance of gathering patient history and conducting a thorough clinical examination. Findings from the assessment, including vital signs and respiratory evaluations, are analyzed in relation to the pathophysiology of asthma, highlighting the role of environmental triggers and airway inflammation. The evaluation of assessment results leads to the development of a detailed nursing care plan, addressing ineffective breathing patterns, impaired gas exchange, and activity intolerance. The case study also reflects on the patient's adverse reaction to Salbutamol, indicating the complexity of asthma management and the need for individualized treatment approaches. The document is available on Desklib, a platform offering a range of study tools and resources for students.

Running head: CLINICAL JUDGMENT AND REASONING
Clinical judgment and reasoning
Name of the student:
Name of the University:
Author’s note
Clinical judgment and reasoning
Name of the student:
Name of the University:
Author’s note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1CLINICAL JUDGMENT AND REASONING
Table of Contents
Introduction:....................................................................................................................................2
Sequencing of proposed assessment: 300 words approx.................................................................2
Process for informing proposed assessment:...................................................................................3
Analysis of findings in relation to the health and clinical assessment:...........................................4
Evaluation of results: 300 words approx.........................................................................................6
Plan of care:.....................................................................................................................................8
Reference:......................................................................................................................................12
Table of Contents
Introduction:....................................................................................................................................2
Sequencing of proposed assessment: 300 words approx.................................................................2
Process for informing proposed assessment:...................................................................................3
Analysis of findings in relation to the health and clinical assessment:...........................................4
Evaluation of results: 300 words approx.........................................................................................6
Plan of care:.....................................................................................................................................8
Reference:......................................................................................................................................12
2CLINICAL JUDGMENT AND REASONING
Introduction:
Clinical reasoning is an important skill in nursing practice to engage in safe and effective
care. It is the process of critical thinking and decision making that supports the nurse to engage
in comprehensive health assessment of patient, identify potential problem in patient and develop
nursing care plan accordingly (Carvalho, Oliveira-Kumakura and Morais, 2017). This report
discusses the process of focused health assessment of a patient by the analysis of the case
scenario of Lucy, a 32 year old woman with symptom of asthma. The report also provides
detailed plan of care for patients based on analysis of clinical assessment findings.
Sequencing of proposed assessment: 300 words approx
Lucy is a patient who is suffering from asthma since childhood. Although her asthma is
well-controlled by the daily intake of beclomethasone, however current issues for patient is that
she has become dyspnoeic and suffering from respiratory issues. To engage in more focused
health assessment, the proposed sequence is to first consider the patient situation and her context
and then collect all vital cues that can help in assessment of client. To gain an understanding
about patient situation, the background of Lucy and people surrounding her will be assessed.
Knowing about patient’s background and the people surrounding them is important to gain idea
about risk factors of disease. It may also inform about medical history of patient, the role of
culture or social life in the diagnosis of disease and changes in factors overtime resulting in
present clinical condition (Forbes and Watt 2015).
In addition, to collect cues related to patient condition, the plan is to first collect data
related to medical history, social history, family history and medication history of patient and
Introduction:
Clinical reasoning is an important skill in nursing practice to engage in safe and effective
care. It is the process of critical thinking and decision making that supports the nurse to engage
in comprehensive health assessment of patient, identify potential problem in patient and develop
nursing care plan accordingly (Carvalho, Oliveira-Kumakura and Morais, 2017). This report
discusses the process of focused health assessment of a patient by the analysis of the case
scenario of Lucy, a 32 year old woman with symptom of asthma. The report also provides
detailed plan of care for patients based on analysis of clinical assessment findings.
Sequencing of proposed assessment: 300 words approx
Lucy is a patient who is suffering from asthma since childhood. Although her asthma is
well-controlled by the daily intake of beclomethasone, however current issues for patient is that
she has become dyspnoeic and suffering from respiratory issues. To engage in more focused
health assessment, the proposed sequence is to first consider the patient situation and her context
and then collect all vital cues that can help in assessment of client. To gain an understanding
about patient situation, the background of Lucy and people surrounding her will be assessed.
Knowing about patient’s background and the people surrounding them is important to gain idea
about risk factors of disease. It may also inform about medical history of patient, the role of
culture or social life in the diagnosis of disease and changes in factors overtime resulting in
present clinical condition (Forbes and Watt 2015).
In addition, to collect cues related to patient condition, the plan is to first collect data
related to medical history, social history, family history and medication history of patient and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CLINICAL JUDGMENT AND REASONING
then engage in clinical assessment of patient as per the signs and assessment of patient. This
would help to process the patient information and prioritize care for patient (Brown et al. 2017).
For example, as Lucy is a patient with asthma from childhood, reviewing family history is
important to understand the reason behind the cause of disease. Secondly, her social life needs to
evaluate to detect environment cause of asthma and presenting issues in patient. As Lucy was
suffering from symptom of dyspnea, wheezing cough and chest tightness, the sequence for
clinical assessment is to first conduct vital sign assessment of patient and then engage in
respiratory assessment. Vital sign assessment like monitoring of BP, pulse, heart beat and
oxygen saturation level is necessary to detect signs and severity of breathing difficulty. Vital sign
assessment is also important as all the vital signs are associated with the pathophysiology of
asthma. In addition, respiratory assessment of Lucy will be done by means of auscultation of
chest and assessment of breathing rate in patient. Hence, respiratory assessment is necessary for
Joel to monitor severity of asthma symptoms (Aaron et al. 2017). Lastly, review of patient chart
is necessary to identify medications taken by patient and the impact of medication on presenting
sign and symptoms. On the whole, the above sequence of assessment can help to process the
information and understand the severity of patient’s health condition.
Process for informing proposed assessment:
The data related to health history is an important element of patient focused health
assessment as it gives idea about past illness, surgery or any surgical complication in patient. The
data related to patient history supports nurse or other staff to gain better understanding about
patient’s problem and the complexity surrounding diseases. It helps in proper identification of
care priorities and enables the delivery of high quality care (Fawcett and Rhynas 2012). To
collect information related to patient history, having patient-centered communication skill is
then engage in clinical assessment of patient as per the signs and assessment of patient. This
would help to process the patient information and prioritize care for patient (Brown et al. 2017).
For example, as Lucy is a patient with asthma from childhood, reviewing family history is
important to understand the reason behind the cause of disease. Secondly, her social life needs to
evaluate to detect environment cause of asthma and presenting issues in patient. As Lucy was
suffering from symptom of dyspnea, wheezing cough and chest tightness, the sequence for
clinical assessment is to first conduct vital sign assessment of patient and then engage in
respiratory assessment. Vital sign assessment like monitoring of BP, pulse, heart beat and
oxygen saturation level is necessary to detect signs and severity of breathing difficulty. Vital sign
assessment is also important as all the vital signs are associated with the pathophysiology of
asthma. In addition, respiratory assessment of Lucy will be done by means of auscultation of
chest and assessment of breathing rate in patient. Hence, respiratory assessment is necessary for
Joel to monitor severity of asthma symptoms (Aaron et al. 2017). Lastly, review of patient chart
is necessary to identify medications taken by patient and the impact of medication on presenting
sign and symptoms. On the whole, the above sequence of assessment can help to process the
information and understand the severity of patient’s health condition.
Process for informing proposed assessment:
The data related to health history is an important element of patient focused health
assessment as it gives idea about past illness, surgery or any surgical complication in patient. The
data related to patient history supports nurse or other staff to gain better understanding about
patient’s problem and the complexity surrounding diseases. It helps in proper identification of
care priorities and enables the delivery of high quality care (Fawcett and Rhynas 2012). To
collect information related to patient history, having patient-centered communication skill is
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CLINICAL JUDGMENT AND REASONING
necessary. It helps in establishing rapport with patient and get detailed patient history. After
establishing rapport with patient, the question that can be asked related to patient history includes
‘Do you suffer from other illness or have you been diagnosed with any other disease in the
past?’. As Joel is a patient with asthma, information related to management of asthma in the past
can be obtained by asking question like ‘What medications you have taken in the past to treat
symptoms of asthma?’. In addition, family and social history can be obtained by question related
to nature of professional life of patient and diagnosis of asthma in other family members. The
above process related to history taking for Joel can inform the proposed assessment process as it
would help to establish link between past medical history and current symptom in patient. This
would help to develop effective care plan for patient in order of priority.
Analysis of findings in relation to the health and clinical assessment:
Based on information obtained from health history and clinical assessment of patient, this
sections provides detailed analysis of findings in related to the underlying pathophysiology of
asthma. The assessment of patient history revealed that Lucy has had asthma since she was a
child and her father was one member of the family, who died because of complications due to
asthma. This information indicates that Joel might have developed asthma related complications
like wheezing sound and chest tightness because of presence of the condition in blood relatives.
Beasley, Semprini and Mitchell (2015) explained that genetic, environmental and host factors are
some of the risk factors of asthma. Although family history of asthma is common in patient,
however environmental triggers play a major role in development of asthma in patient. By the
process of history taking for Joel, environmental risk factors for asthma were also identified.
While questioning patient on her profession and nature of work she does, it was found that Joel
works as a cleaner in private aged care facility. Hence, it is very likely that Joel might be
necessary. It helps in establishing rapport with patient and get detailed patient history. After
establishing rapport with patient, the question that can be asked related to patient history includes
‘Do you suffer from other illness or have you been diagnosed with any other disease in the
past?’. As Joel is a patient with asthma, information related to management of asthma in the past
can be obtained by asking question like ‘What medications you have taken in the past to treat
symptoms of asthma?’. In addition, family and social history can be obtained by question related
to nature of professional life of patient and diagnosis of asthma in other family members. The
above process related to history taking for Joel can inform the proposed assessment process as it
would help to establish link between past medical history and current symptom in patient. This
would help to develop effective care plan for patient in order of priority.
Analysis of findings in relation to the health and clinical assessment:
Based on information obtained from health history and clinical assessment of patient, this
sections provides detailed analysis of findings in related to the underlying pathophysiology of
asthma. The assessment of patient history revealed that Lucy has had asthma since she was a
child and her father was one member of the family, who died because of complications due to
asthma. This information indicates that Joel might have developed asthma related complications
like wheezing sound and chest tightness because of presence of the condition in blood relatives.
Beasley, Semprini and Mitchell (2015) explained that genetic, environmental and host factors are
some of the risk factors of asthma. Although family history of asthma is common in patient,
however environmental triggers play a major role in development of asthma in patient. By the
process of history taking for Joel, environmental risk factors for asthma were also identified.
While questioning patient on her profession and nature of work she does, it was found that Joel
works as a cleaner in private aged care facility. Hence, it is very likely that Joel might be
5CLINICAL JUDGMENT AND REASONING
exposed to allergens and pollutant that lead to exacerbation of her symptom. The exposure of
allergen or irritants predispose patient to immune response and the allergen acts as the stimuli
that lead to development of airway inflammation. In response to exposure to stimuli like
allergens, the bronchial muscles contracts and narrows the respiratory airways resulting in acute
exacerbation of asthma (Chung 2015).
On the basis of clinical assessment of patient as per her currently symptoms, the first
sequence was to conduct vital health assessment in patient. During vital sign assessment, her
body temperature was 38 C, pulse rate was 115, respiration rate was 32, BP was 160/90 and
SaO2 was 91%. The vital sign assessment revealed severe respiratory complication in patient as
her respiratory rate is higher than the normal value of 12-20 breaths per minutes and her pulse
rate is also above the normal range. Her BP reading also shows she is hypertensive, however her
SpO2 level is within the normal range. She would have required supplementary oxygen therapy
if her SpO2 level had fallen below 90%. However, presence respiratory problems like high
breathing rate and increases pulse rate also indicate signs of exacerbation of asthma in patient.
This assessment finding is linked to the underlying pathophysiology of asthma. The main
pathophysiological features of the disease are bronchial inflammation, shortness of breath,
wheeziness and airflow limitations (Sullivan et al. 2016). Similar symptoms were observed in
Joel too and this mainly occurred because of airway inflammation process. Respiratory rate
increases in patients with asthma because of the action of immune cells like T-lymphocytes,
macrophages, neutrophils and mast cells. They contribute to airway inflammation resulting in
narrowing of respiratory airways, airflow limitation and consequently respiratory problem in
patient. Chronic inflammation also results in permanent changes in airway structure of patient
(Fahy 2015).
exposed to allergens and pollutant that lead to exacerbation of her symptom. The exposure of
allergen or irritants predispose patient to immune response and the allergen acts as the stimuli
that lead to development of airway inflammation. In response to exposure to stimuli like
allergens, the bronchial muscles contracts and narrows the respiratory airways resulting in acute
exacerbation of asthma (Chung 2015).
On the basis of clinical assessment of patient as per her currently symptoms, the first
sequence was to conduct vital health assessment in patient. During vital sign assessment, her
body temperature was 38 C, pulse rate was 115, respiration rate was 32, BP was 160/90 and
SaO2 was 91%. The vital sign assessment revealed severe respiratory complication in patient as
her respiratory rate is higher than the normal value of 12-20 breaths per minutes and her pulse
rate is also above the normal range. Her BP reading also shows she is hypertensive, however her
SpO2 level is within the normal range. She would have required supplementary oxygen therapy
if her SpO2 level had fallen below 90%. However, presence respiratory problems like high
breathing rate and increases pulse rate also indicate signs of exacerbation of asthma in patient.
This assessment finding is linked to the underlying pathophysiology of asthma. The main
pathophysiological features of the disease are bronchial inflammation, shortness of breath,
wheeziness and airflow limitations (Sullivan et al. 2016). Similar symptoms were observed in
Joel too and this mainly occurred because of airway inflammation process. Respiratory rate
increases in patients with asthma because of the action of immune cells like T-lymphocytes,
macrophages, neutrophils and mast cells. They contribute to airway inflammation resulting in
narrowing of respiratory airways, airflow limitation and consequently respiratory problem in
patient. Chronic inflammation also results in permanent changes in airway structure of patient
(Fahy 2015).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CLINICAL JUDGMENT AND REASONING
As Joel was dysnpoeic, oxygen saturation assessment was also conducted in patient. Her
oxygen saturation rate dropped to 88% which is below the normal range of 95-100%. Hence,
from this perspective, it is clear that Joel is in need of supplemental oxygen to prevent symptom
of dyspnea. The respiratory assessment of patient also revealed that she had loud expiratory
wheeze. She was using her accessory muscles. Symptoms of wheezing are also linked to the
pathophysiology of asthma. This can be said because wheezing is produced due to inflammation
of the airways and during acute exacerbation, the exposure of allergens or irritants initiate the
process for airway inflammation in patient. Due to inflammation of the airway, airflow
obstruction and airway limitation is observed in patient. Such pathophysiological changes cause
recurrent episodes of wheezing and breathlessness in patient (Lambrecht and Hammad 2015).
Airway narrowing is the main physiological event that results in airflow obstruction and the
process of airway inflammation establishes the cause of wheezing sound during chest
auscultation for Joel.
The review of medication history of Joel revealed that earlier she used to beclomethasone
medication to control her asthma. However, after admission to hospital during acute
exacerbation, she was given Salbutamol, but her condition deteriorated after giving medication.
Hence, in response to this, it is necessary to find out the cause of such deterioration and suggest
new medication accordingly for symptom improvement.
Evaluation of results:
The first and foremost assessment that has been done for the patient includes the history
of the patient that reveals Lucy had asthma as a child and her father died due to asthma
complications. It has to be mentioned that genetic predisposition associated with asthma is a
As Joel was dysnpoeic, oxygen saturation assessment was also conducted in patient. Her
oxygen saturation rate dropped to 88% which is below the normal range of 95-100%. Hence,
from this perspective, it is clear that Joel is in need of supplemental oxygen to prevent symptom
of dyspnea. The respiratory assessment of patient also revealed that she had loud expiratory
wheeze. She was using her accessory muscles. Symptoms of wheezing are also linked to the
pathophysiology of asthma. This can be said because wheezing is produced due to inflammation
of the airways and during acute exacerbation, the exposure of allergens or irritants initiate the
process for airway inflammation in patient. Due to inflammation of the airway, airflow
obstruction and airway limitation is observed in patient. Such pathophysiological changes cause
recurrent episodes of wheezing and breathlessness in patient (Lambrecht and Hammad 2015).
Airway narrowing is the main physiological event that results in airflow obstruction and the
process of airway inflammation establishes the cause of wheezing sound during chest
auscultation for Joel.
The review of medication history of Joel revealed that earlier she used to beclomethasone
medication to control her asthma. However, after admission to hospital during acute
exacerbation, she was given Salbutamol, but her condition deteriorated after giving medication.
Hence, in response to this, it is necessary to find out the cause of such deterioration and suggest
new medication accordingly for symptom improvement.
Evaluation of results:
The first and foremost assessment that has been done for the patient includes the history
of the patient that reveals Lucy had asthma as a child and her father died due to asthma
complications. It has to be mentioned that genetic predisposition associated with asthma is a
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CLINICAL JUDGMENT AND REASONING
very common risk factor that enhances the vulnerability of a patient towards exacerbations of
asthma. Along with that assessment of the past medical history of a patient reveals crucial
clinical cues based on which the patient situational analysis and synthesis of the processed
information of the clinical reasoning cycle takes place which provides the foundation based on
which the primary and secondary diagnosis will take place (Boulet et al. 2012). Hence it can be
concluded that patient history assessment is a very important aspect associated with care
planning and it has fundamental significance in the entire procedure. It has to be mentioned that
along with genetic predisposition the impact of environmental triggers is also a cute in case of
asthma exacerbations. During subjective and objective patient data documentation it was
revealed that she had been a cleaner in a private aged care facility. Hence the chances of the
patient been exposed to various environmental trigger such as a legends and pollutants is very
high that could have been the pathophysiological reason leading to the exercise patience offer
symptoms. Hence it has acute importance in the care planning procedure as well (Black et al.
2013).
Elaborating on the vital sign assessment, results indicate that the patient had high
respiratory rate, high blood pressure, and high temperature. All of these symptoms are associated
with acute asthma exacerbations and have significant value in the diagnosis and post Diagnostic
care planning procedure. However, it has to be mentioned that the oxygen saturation of the
patient is within the normal rates hence, it does not indicate at significant results relevant to the
care scenario of the patient. However, later the oxygen saturation count of the patient declined to
88% which indicated at acute inflammation of the airways and bronchial spasms. Hence this
result also holds significance in understanding the etiology of the present condition of Joel and
planning of further care plans (Zipkin et al. 2013). It has to be mentioned in this context that the
very common risk factor that enhances the vulnerability of a patient towards exacerbations of
asthma. Along with that assessment of the past medical history of a patient reveals crucial
clinical cues based on which the patient situational analysis and synthesis of the processed
information of the clinical reasoning cycle takes place which provides the foundation based on
which the primary and secondary diagnosis will take place (Boulet et al. 2012). Hence it can be
concluded that patient history assessment is a very important aspect associated with care
planning and it has fundamental significance in the entire procedure. It has to be mentioned that
along with genetic predisposition the impact of environmental triggers is also a cute in case of
asthma exacerbations. During subjective and objective patient data documentation it was
revealed that she had been a cleaner in a private aged care facility. Hence the chances of the
patient been exposed to various environmental trigger such as a legends and pollutants is very
high that could have been the pathophysiological reason leading to the exercise patience offer
symptoms. Hence it has acute importance in the care planning procedure as well (Black et al.
2013).
Elaborating on the vital sign assessment, results indicate that the patient had high
respiratory rate, high blood pressure, and high temperature. All of these symptoms are associated
with acute asthma exacerbations and have significant value in the diagnosis and post Diagnostic
care planning procedure. However, it has to be mentioned that the oxygen saturation of the
patient is within the normal rates hence, it does not indicate at significant results relevant to the
care scenario of the patient. However, later the oxygen saturation count of the patient declined to
88% which indicated at acute inflammation of the airways and bronchial spasms. Hence this
result also holds significance in understanding the etiology of the present condition of Joel and
planning of further care plans (Zipkin et al. 2013). It has to be mentioned in this context that the
8CLINICAL JUDGMENT AND REASONING
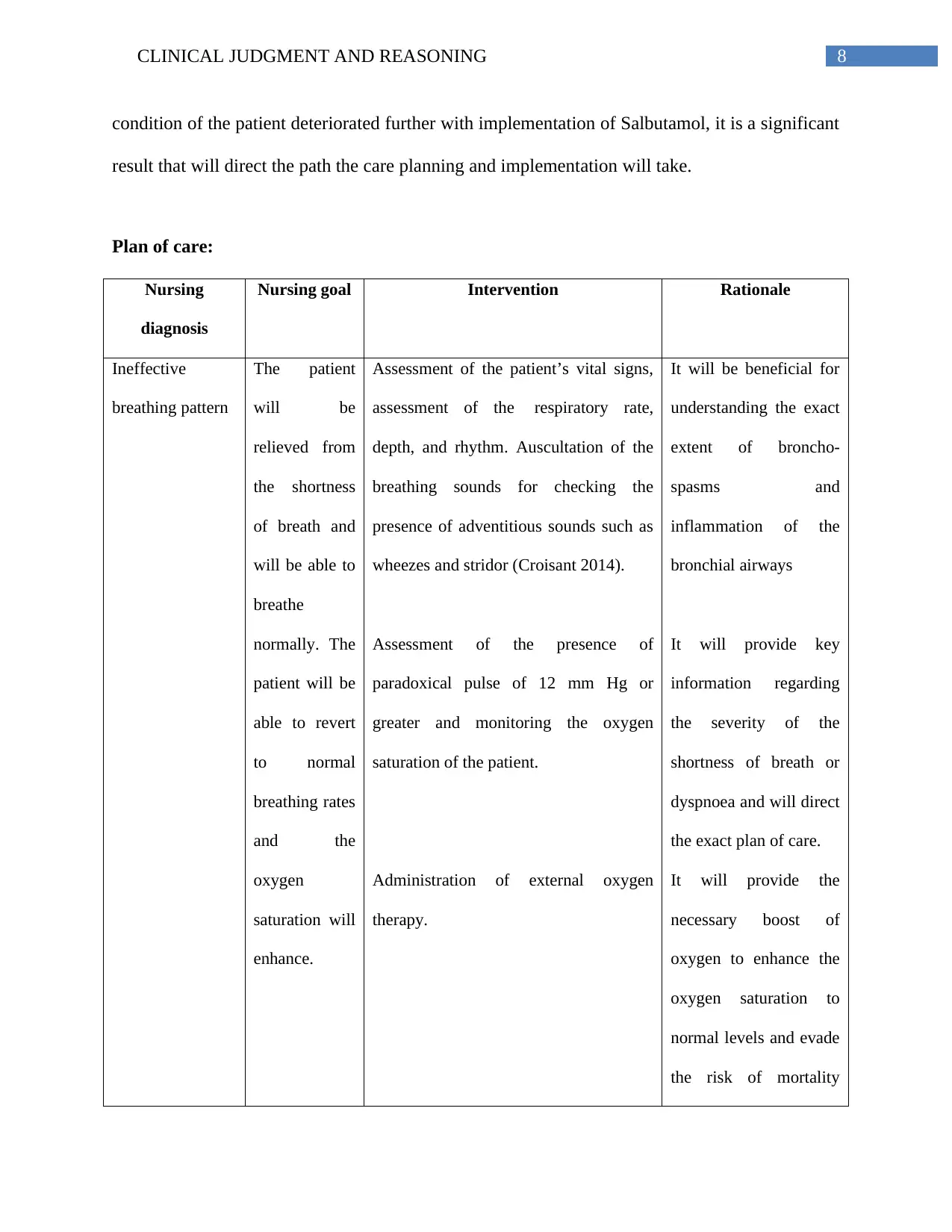
condition of the patient deteriorated further with implementation of Salbutamol, it is a significant
result that will direct the path the care planning and implementation will take.
Plan of care:
Nursing
diagnosis
Nursing goal Intervention Rationale
Ineffective
breathing pattern
The patient
will be
relieved from
the shortness
of breath and
will be able to
breathe
normally. The
patient will be
able to revert
to normal
breathing rates
and the
oxygen
saturation will
enhance.
Assessment of the patient’s vital signs,
assessment of the respiratory rate,
depth, and rhythm. Auscultation of the
breathing sounds for checking the
presence of adventitious sounds such as
wheezes and stridor (Croisant 2014).
Assessment of the presence of
paradoxical pulse of 12 mm Hg or
greater and monitoring the oxygen
saturation of the patient.
Administration of external oxygen
therapy.
It will be beneficial for
understanding the exact
extent of broncho-
spasms and
inflammation of the
bronchial airways
It will provide key
information regarding
the severity of the
shortness of breath or
dyspnoea and will direct
the exact plan of care.
It will provide the
necessary boost of
oxygen to enhance the
oxygen saturation to
normal levels and evade
the risk of mortality
condition of the patient deteriorated further with implementation of Salbutamol, it is a significant
result that will direct the path the care planning and implementation will take.
Plan of care:
Nursing
diagnosis
Nursing goal Intervention Rationale
Ineffective
breathing pattern
The patient
will be
relieved from
the shortness
of breath and
will be able to
breathe
normally. The
patient will be
able to revert
to normal
breathing rates
and the
oxygen
saturation will
enhance.
Assessment of the patient’s vital signs,
assessment of the respiratory rate,
depth, and rhythm. Auscultation of the
breathing sounds for checking the
presence of adventitious sounds such as
wheezes and stridor (Croisant 2014).
Assessment of the presence of
paradoxical pulse of 12 mm Hg or
greater and monitoring the oxygen
saturation of the patient.
Administration of external oxygen
therapy.
It will be beneficial for
understanding the exact
extent of broncho-
spasms and
inflammation of the
bronchial airways
It will provide key
information regarding
the severity of the
shortness of breath or
dyspnoea and will direct
the exact plan of care.
It will provide the
necessary boost of
oxygen to enhance the
oxygen saturation to
normal levels and evade
the risk of mortality
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9CLINICAL JUDGMENT AND REASONING
Administration of albuterol, levalbuterol
and terbutaline.
Administration of Inhaled
Corticosteroids such as Pulmicort,
Flovent, Vancenase, Asmanex
Twisthaler.
(Chunchu et al. 2012).
Administration of Short-
acting beta2-agonists
are bronchodilators will
help in relaxing the
muscles lining the
airways that carry air to
the lungs;
Corticosteroids will
help in reducing
inflammation in the
airways that carry air to
the lungs and reducing
the mucus production.
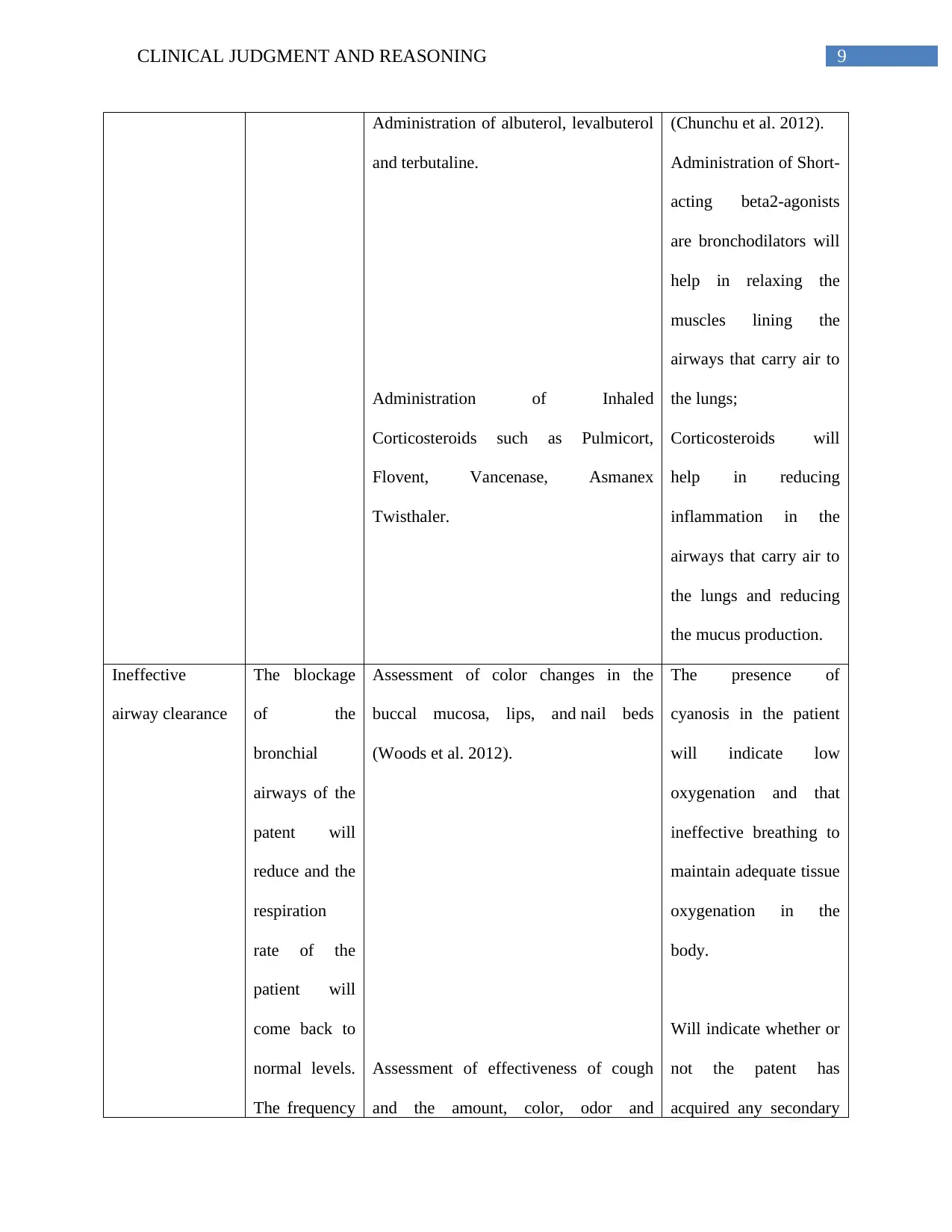
Ineffective
airway clearance
The blockage
of the
bronchial
airways of the
patent will
reduce and the
respiration
rate of the
patient will
come back to
normal levels.
The frequency
Assessment of color changes in the
buccal mucosa, lips, and nail beds
(Woods et al. 2012).
Assessment of effectiveness of cough
and the amount, color, odor and
The presence of
cyanosis in the patient
will indicate low
oxygenation and that
ineffective breathing to
maintain adequate tissue
oxygenation in the
body.
Will indicate whether or
not the patent has
acquired any secondary
Administration of albuterol, levalbuterol
and terbutaline.
Administration of Inhaled
Corticosteroids such as Pulmicort,
Flovent, Vancenase, Asmanex
Twisthaler.
(Chunchu et al. 2012).
Administration of Short-
acting beta2-agonists
are bronchodilators will
help in relaxing the
muscles lining the
airways that carry air to
the lungs;
Corticosteroids will
help in reducing
inflammation in the
airways that carry air to
the lungs and reducing
the mucus production.
Ineffective
airway clearance
The blockage
of the
bronchial
airways of the
patent will
reduce and the
respiration
rate of the
patient will
come back to
normal levels.
The frequency
Assessment of color changes in the
buccal mucosa, lips, and nail beds
(Woods et al. 2012).
Assessment of effectiveness of cough
and the amount, color, odor and
The presence of
cyanosis in the patient
will indicate low
oxygenation and that
ineffective breathing to
maintain adequate tissue
oxygenation in the
body.
Will indicate whether or
not the patent has
acquired any secondary
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
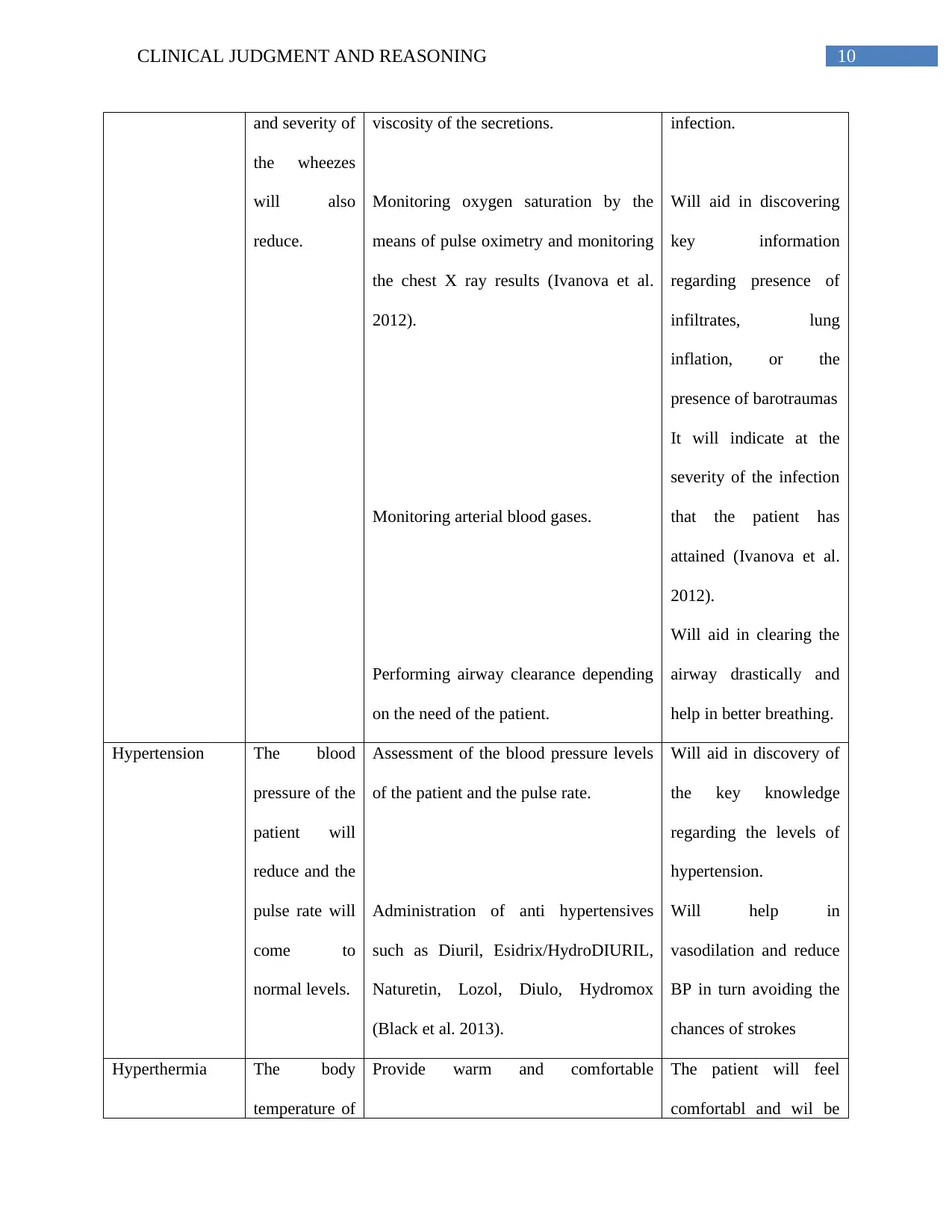
10CLINICAL JUDGMENT AND REASONING
and severity of
the wheezes
will also
reduce.
viscosity of the secretions.
Monitoring oxygen saturation by the
means of pulse oximetry and monitoring
the chest X ray results (Ivanova et al.
2012).
Monitoring arterial blood gases.
Performing airway clearance depending
on the need of the patient.
infection.
Will aid in discovering
key information
regarding presence of
infiltrates, lung
inflation, or the
presence of barotraumas
It will indicate at the
severity of the infection
that the patient has
attained (Ivanova et al.
2012).
Will aid in clearing the
airway drastically and
help in better breathing.
Hypertension The blood
pressure of the
patient will
reduce and the
pulse rate will
come to
normal levels.
Assessment of the blood pressure levels
of the patient and the pulse rate.
Administration of anti hypertensives
such as Diuril, Esidrix/HydroDIURIL,
Naturetin, Lozol, Diulo, Hydromox
(Black et al. 2013).
Will aid in discovery of
the key knowledge
regarding the levels of
hypertension.
Will help in
vasodilation and reduce
BP in turn avoiding the
chances of strokes
Hyperthermia The body
temperature of
Provide warm and comfortable The patient will feel
comfortabl and wil be
and severity of
the wheezes
will also
reduce.
viscosity of the secretions.
Monitoring oxygen saturation by the
means of pulse oximetry and monitoring
the chest X ray results (Ivanova et al.
2012).
Monitoring arterial blood gases.
Performing airway clearance depending
on the need of the patient.
infection.
Will aid in discovering
key information
regarding presence of
infiltrates, lung
inflation, or the
presence of barotraumas
It will indicate at the
severity of the infection
that the patient has
attained (Ivanova et al.
2012).
Will aid in clearing the
airway drastically and
help in better breathing.
Hypertension The blood
pressure of the
patient will
reduce and the
pulse rate will
come to
normal levels.
Assessment of the blood pressure levels
of the patient and the pulse rate.
Administration of anti hypertensives
such as Diuril, Esidrix/HydroDIURIL,
Naturetin, Lozol, Diulo, Hydromox
(Black et al. 2013).
Will aid in discovery of
the key knowledge
regarding the levels of
hypertension.
Will help in
vasodilation and reduce
BP in turn avoiding the
chances of strokes
Hyperthermia The body
temperature of
Provide warm and comfortable The patient will feel
comfortabl and wil be
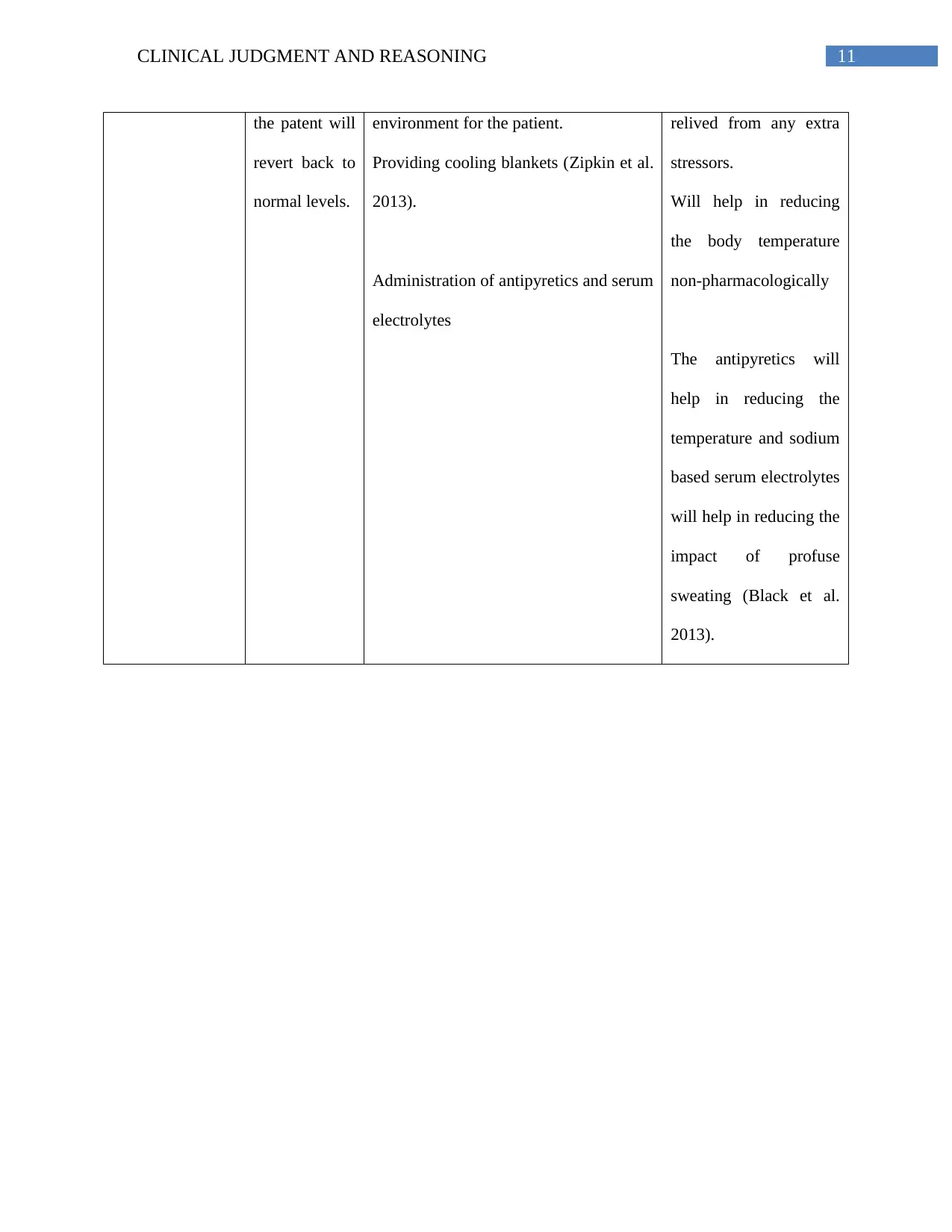
11CLINICAL JUDGMENT AND REASONING
the patent will
revert back to
normal levels.
environment for the patient.
Providing cooling blankets (Zipkin et al.
2013).
Administration of antipyretics and serum
electrolytes
relived from any extra
stressors.
Will help in reducing
the body temperature
non-pharmacologically
The antipyretics will
help in reducing the
temperature and sodium
based serum electrolytes
will help in reducing the
impact of profuse
sweating (Black et al.
2013).
the patent will
revert back to
normal levels.
environment for the patient.
Providing cooling blankets (Zipkin et al.
2013).
Administration of antipyretics and serum
electrolytes
relived from any extra
stressors.
Will help in reducing
the body temperature
non-pharmacologically
The antipyretics will
help in reducing the
temperature and sodium
based serum electrolytes
will help in reducing the
impact of profuse
sweating (Black et al.
2013).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.