Case Study: Mrs. Brown's Acute Exacerbation of Heart Failure Analysis
VerifiedAdded on 2021/02/20
|11
|2377
|23
Case Study
AI Summary
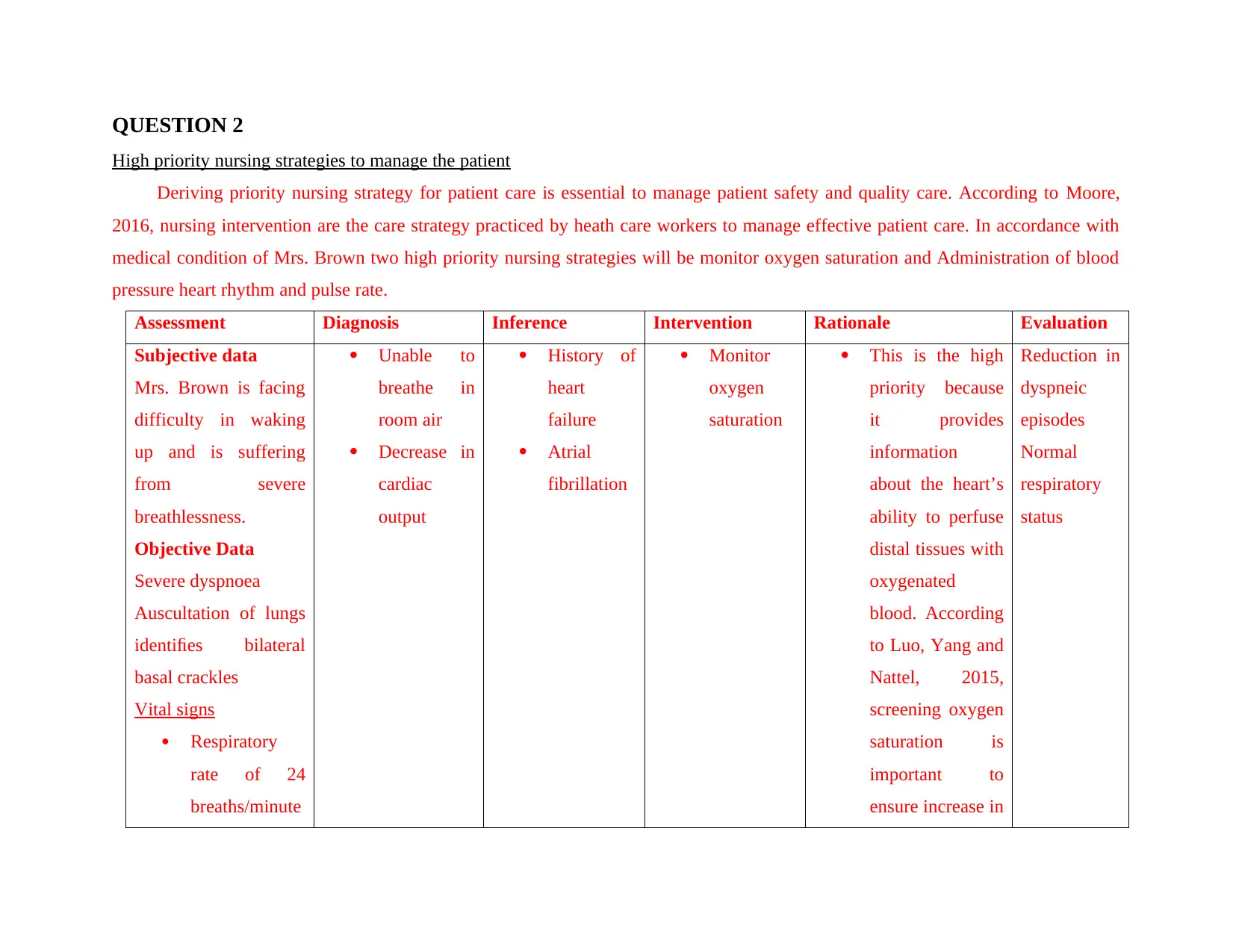
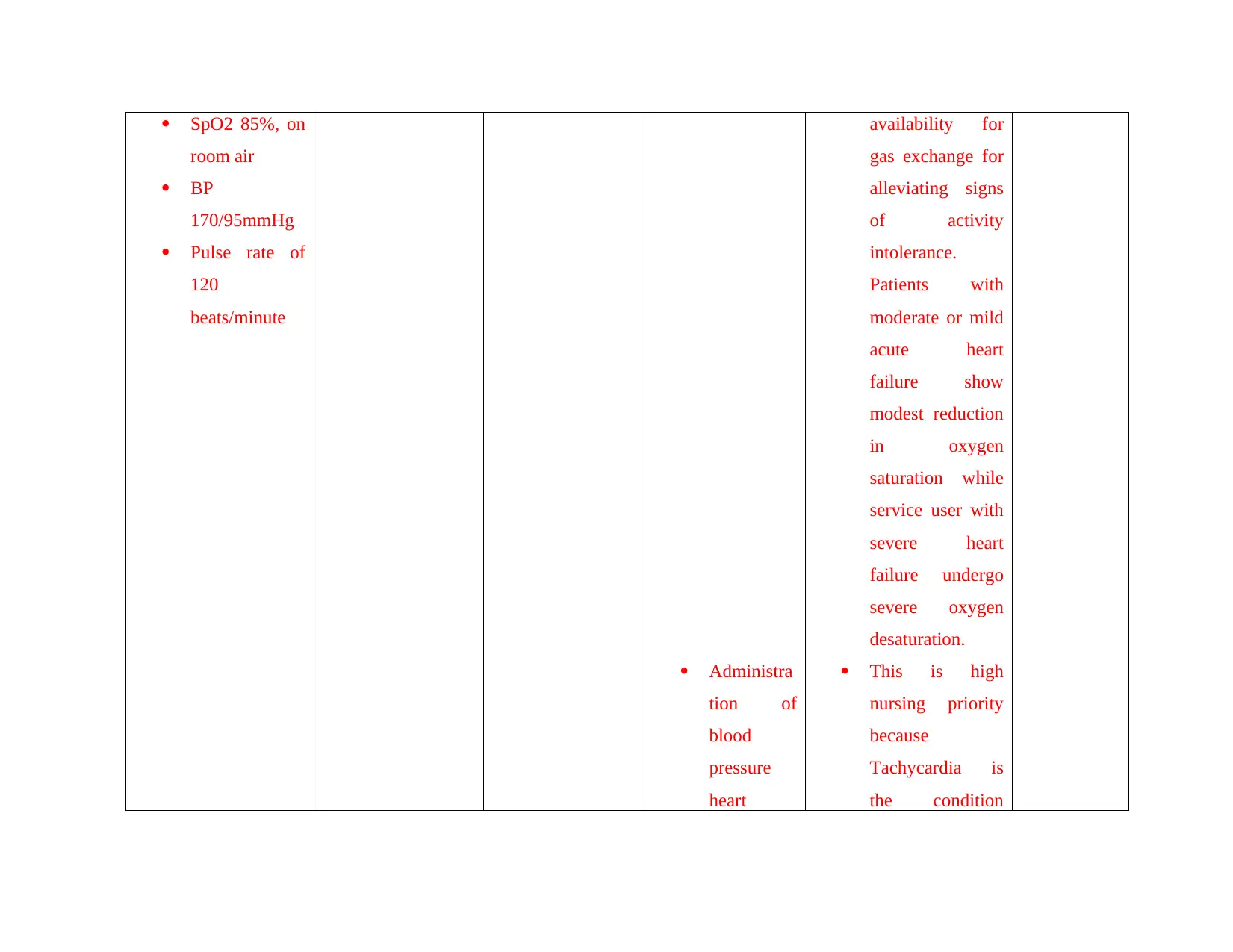
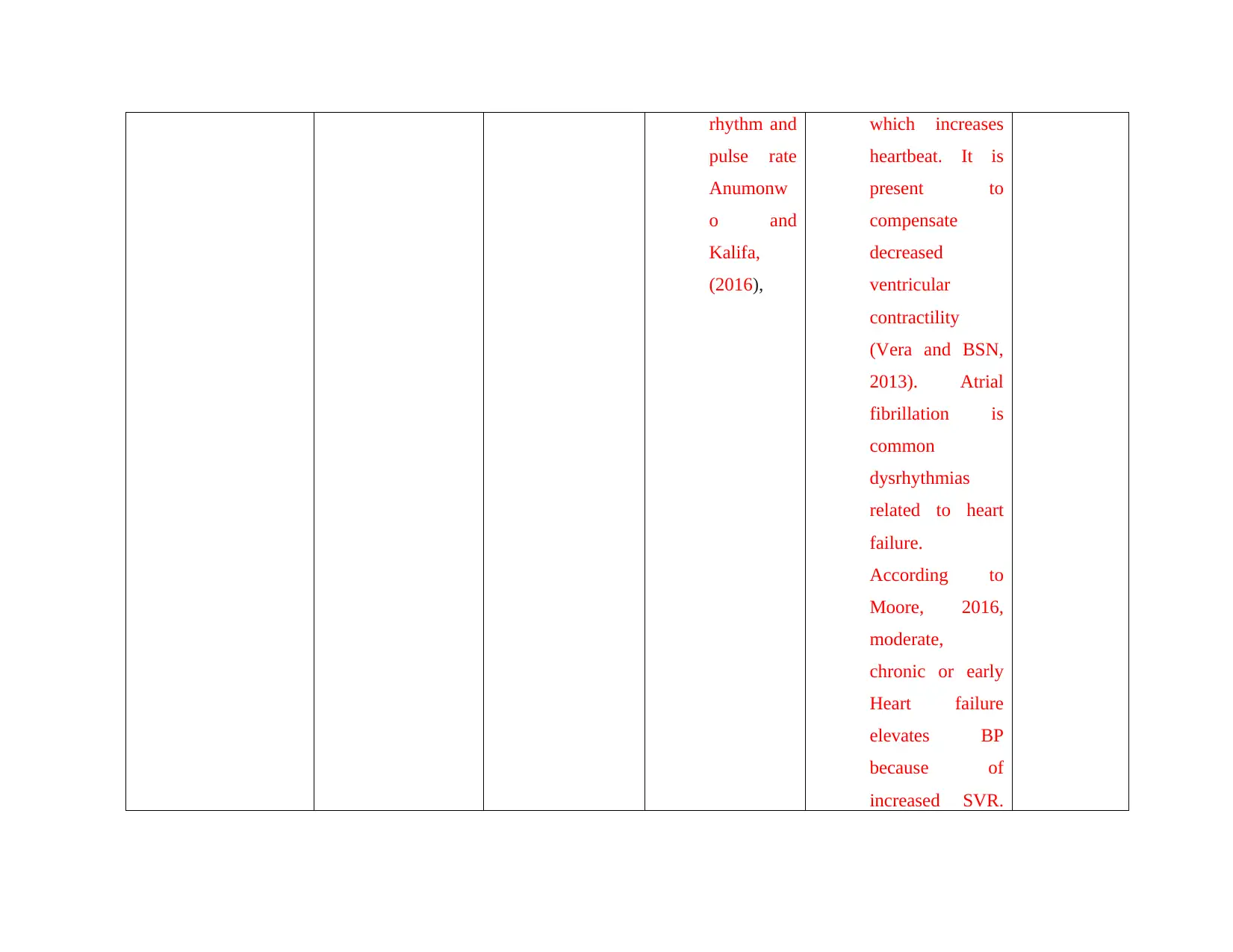
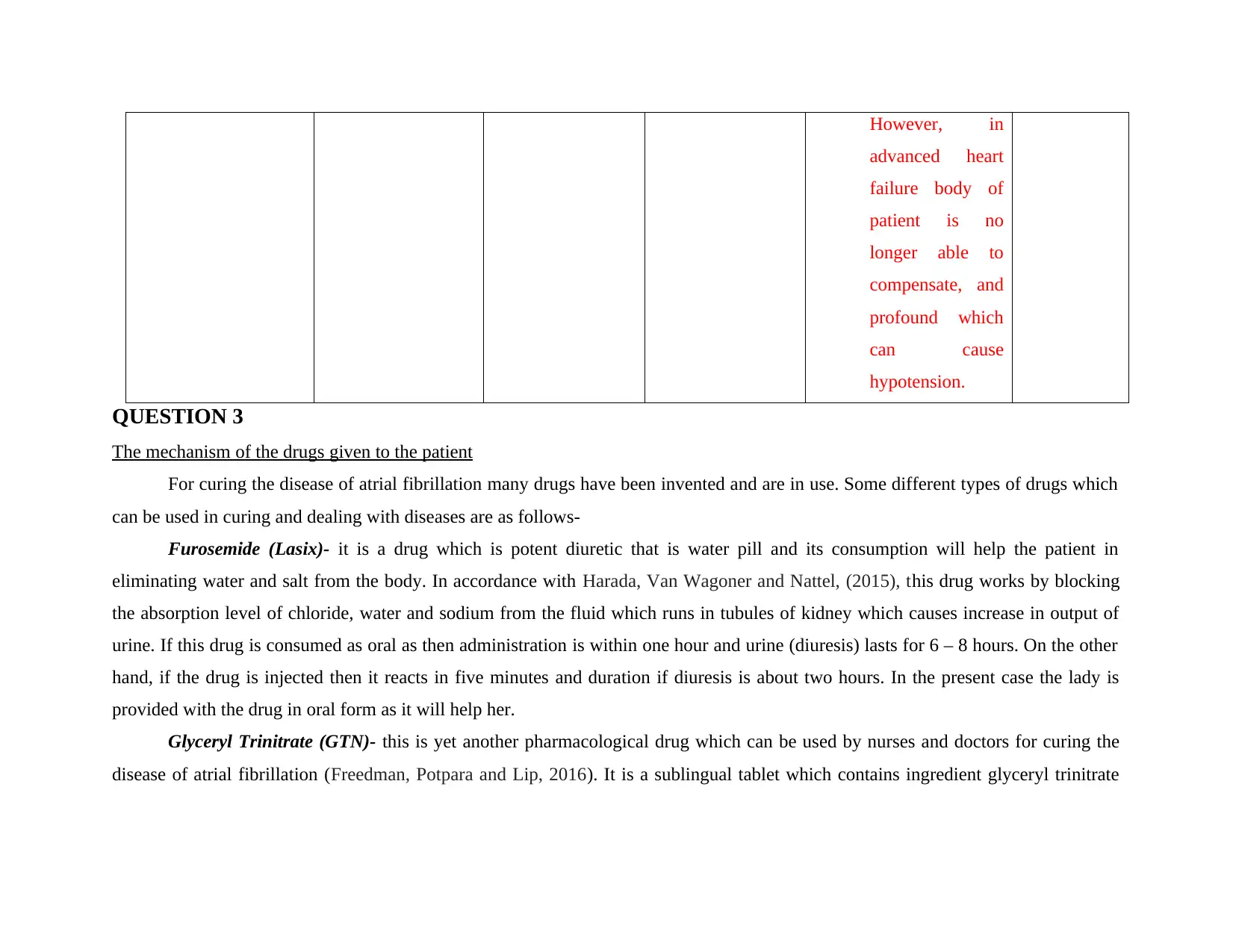
This case study examines the acute exacerbation of chronic systolic heart failure in a 78-year-old female, Mrs. Brown, who presented with severe breathlessness and atrial fibrillation. The analysis begins with an overview of the pathogenesis, detailing how disorganized electrical signals in the heart lead to clinical manifestations like dyspnea, high blood pressure, and abnormal respiratory rates, including the impact of factors such as age and pre-existing conditions like heart failure and lung diseases. The study then discusses two high-priority nursing strategies: monitoring oxygen saturation and administering blood pressure, heart rhythm, and pulse rate, providing rationales based on evidence-based practice. Finally, it explores the mechanisms of action of two drugs, Furosemide (Lasix) and Glyceryl Trinitrate (GTN), used in managing the condition, relating these mechanisms to the underlying pathophysiology of the disease. The conclusion highlights the importance of timely interventions and pharmacological support in managing atrial fibrillation and preventing complications such as systolic heart failure.
1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.