Aged Care: Clinical Practice Improvement Report on Falls Prevention
VerifiedAdded on 2020/04/13
|14
|3766
|41
Report
AI Summary
This report details a Clinical Practice Improvement (CPI) project aimed at reducing fall rates in elderly residents of aged care homes through nutritional interventions. The project, focusing on Australian healthcare data and WHO reports, highlights the significance of fall prevention. It outlines clinical governance principles, including consumer value, clinical performance, risk management, and professional development, and identifies key stakeholders like beneficiaries, providers, funders, and the elderly. The report utilizes the Plan-Do-Study-Act (PDSA) cycle to implement and evaluate interventions, addressing issues like medication reminders, mobility support, and vitamin D and calcium deficiencies. The proposed intervention focuses on providing a nutritious diet to prevent falls, emphasizing vitamin D-rich foods and supplementation. Barriers to implementation, such as economical constraints and time management, are also considered. The project's evaluation includes measures and outcomes to assess the effectiveness of the implemented strategies. This report offers valuable insights into practical solutions and methodologies for improving the safety and well-being of elderly individuals in aged care settings.
0
clinical practice
improvement report
clinical practice
improvement report
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of Contents
Project Title.........................................................................................................................................1
Project Aim..........................................................................................................................................1
Project Evidence..................................................................................................................................1
Clinical Governance............................................................................................................................1
Key Stakeholder of the Aged Care.....................................................................................................3
CPI Tools..............................................................................................................................................4
Plan-Do-Study-Act (PDSA) Mechanism........................................................................................5
Plan...............................................................................................................................................5
Do..................................................................................................................................................5
Study.............................................................................................................................................6
Act.................................................................................................................................................6
Proposed Intervention.........................................................................................................................7
Barriers for the Implementation........................................................................................................8
Economical Barrier.........................................................................................................................8
Time Management...........................................................................................................................9
Evaluation of the Project....................................................................................................................9
Measures and Outcomes.................................................................................................................9
References..........................................................................................................................................10
Project Title.........................................................................................................................................1
Project Aim..........................................................................................................................................1
Project Evidence..................................................................................................................................1
Clinical Governance............................................................................................................................1
Key Stakeholder of the Aged Care.....................................................................................................3
CPI Tools..............................................................................................................................................4
Plan-Do-Study-Act (PDSA) Mechanism........................................................................................5
Plan...............................................................................................................................................5
Do..................................................................................................................................................5
Study.............................................................................................................................................6
Act.................................................................................................................................................6
Proposed Intervention.........................................................................................................................7
Barriers for the Implementation........................................................................................................8
Economical Barrier.........................................................................................................................8
Time Management...........................................................................................................................9
Evaluation of the Project....................................................................................................................9
Measures and Outcomes.................................................................................................................9
References..........................................................................................................................................10
Project Title
Nutritious Diet for Fall Prevention in elderly people
Project Aim
This project aims to decline the fall rate in the aged people who stay in the Aged care
homes by less than 30%, within 6 months by providing nutritious diet.
Project Evidence
Certain evidences that support that the problem is worth to solve includes, the
Australian Health Care reports and, the report of Health and welfare of the elderly people i.e.,
provided by the WHO (World Health Organization). Australian Health and welfare reports
has reported that, from 2011-2012 around 1, 26,000 elderly people were admitted to the
hospitals. The reason is reported as injuries caused because of falling. For every 1, 00,000
count the rate of fall in women is 4,252 and in men it is estimated as 3,235 (Right at Home
Australia, 2018). WHO’s global health report on fall prevention in old people report stated
that, in 2006 the people above 60 years of age were estimated as 688 million, throughout the
world. It was estimated that the number could further reach up to 2 billion by 2050
(Sherrington and Tiedemann, 2015).
Clinical Governance
The Australian council defines Clinical Governance as a system that helps the
government to manage the responsibilities of the mangers, staff and clinicians. It also ensures
to check their accountability in terms of quality health care, decreased risks, continuous
improvement and development in the patients (Avant.org.au, 2018) (Western Australian
Strategic Plan for Safety and Quality in Health Care 2013–2017, 2014).
1
Nutritious Diet for Fall Prevention in elderly people
Project Aim
This project aims to decline the fall rate in the aged people who stay in the Aged care
homes by less than 30%, within 6 months by providing nutritious diet.
Project Evidence
Certain evidences that support that the problem is worth to solve includes, the
Australian Health Care reports and, the report of Health and welfare of the elderly people i.e.,
provided by the WHO (World Health Organization). Australian Health and welfare reports
has reported that, from 2011-2012 around 1, 26,000 elderly people were admitted to the
hospitals. The reason is reported as injuries caused because of falling. For every 1, 00,000
count the rate of fall in women is 4,252 and in men it is estimated as 3,235 (Right at Home
Australia, 2018). WHO’s global health report on fall prevention in old people report stated
that, in 2006 the people above 60 years of age were estimated as 688 million, throughout the
world. It was estimated that the number could further reach up to 2 billion by 2050
(Sherrington and Tiedemann, 2015).
Clinical Governance
The Australian council defines Clinical Governance as a system that helps the
government to manage the responsibilities of the mangers, staff and clinicians. It also ensures
to check their accountability in terms of quality health care, decreased risks, continuous
improvement and development in the patients (Avant.org.au, 2018) (Western Australian
Strategic Plan for Safety and Quality in Health Care 2013–2017, 2014).
1
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
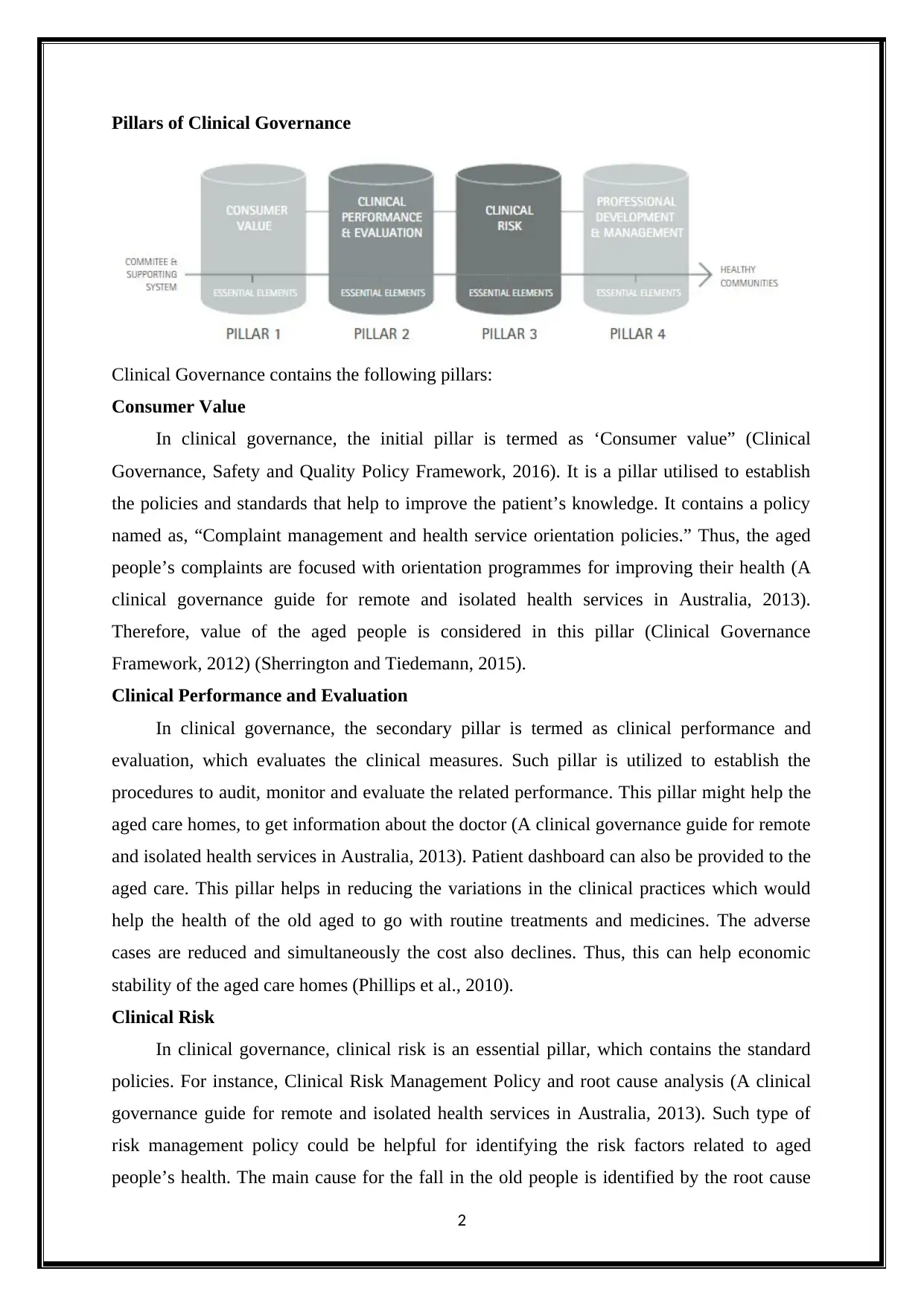
Pillars of Clinical Governance
Clinical Governance contains the following pillars:
Consumer Value
In clinical governance, the initial pillar is termed as ‘Consumer value” (Clinical
Governance, Safety and Quality Policy Framework, 2016). It is a pillar utilised to establish
the policies and standards that help to improve the patient’s knowledge. It contains a policy
named as, “Complaint management and health service orientation policies.” Thus, the aged
people’s complaints are focused with orientation programmes for improving their health (A
clinical governance guide for remote and isolated health services in Australia, 2013).
Therefore, value of the aged people is considered in this pillar (Clinical Governance
Framework, 2012) (Sherrington and Tiedemann, 2015).
Clinical Performance and Evaluation
In clinical governance, the secondary pillar is termed as clinical performance and
evaluation, which evaluates the clinical measures. Such pillar is utilized to establish the
procedures to audit, monitor and evaluate the related performance. This pillar might help the
aged care homes, to get information about the doctor (A clinical governance guide for remote
and isolated health services in Australia, 2013). Patient dashboard can also be provided to the
aged care. This pillar helps in reducing the variations in the clinical practices which would
help the health of the old aged to go with routine treatments and medicines. The adverse
cases are reduced and simultaneously the cost also declines. Thus, this can help economic
stability of the aged care homes (Phillips et al., 2010).
Clinical Risk
In clinical governance, clinical risk is an essential pillar, which contains the standard
policies. For instance, Clinical Risk Management Policy and root cause analysis (A clinical
governance guide for remote and isolated health services in Australia, 2013). Such type of
risk management policy could be helpful for identifying the risk factors related to aged
people’s health. The main cause for the fall in the old people is identified by the root cause
2
Clinical Governance contains the following pillars:
Consumer Value
In clinical governance, the initial pillar is termed as ‘Consumer value” (Clinical
Governance, Safety and Quality Policy Framework, 2016). It is a pillar utilised to establish
the policies and standards that help to improve the patient’s knowledge. It contains a policy
named as, “Complaint management and health service orientation policies.” Thus, the aged
people’s complaints are focused with orientation programmes for improving their health (A
clinical governance guide for remote and isolated health services in Australia, 2013).
Therefore, value of the aged people is considered in this pillar (Clinical Governance
Framework, 2012) (Sherrington and Tiedemann, 2015).
Clinical Performance and Evaluation
In clinical governance, the secondary pillar is termed as clinical performance and
evaluation, which evaluates the clinical measures. Such pillar is utilized to establish the
procedures to audit, monitor and evaluate the related performance. This pillar might help the
aged care homes, to get information about the doctor (A clinical governance guide for remote
and isolated health services in Australia, 2013). Patient dashboard can also be provided to the
aged care. This pillar helps in reducing the variations in the clinical practices which would
help the health of the old aged to go with routine treatments and medicines. The adverse
cases are reduced and simultaneously the cost also declines. Thus, this can help economic
stability of the aged care homes (Phillips et al., 2010).
Clinical Risk
In clinical governance, clinical risk is an essential pillar, which contains the standard
policies. For instance, Clinical Risk Management Policy and root cause analysis (A clinical
governance guide for remote and isolated health services in Australia, 2013). Such type of
risk management policy could be helpful for identifying the risk factors related to aged
people’s health. The main cause for the fall in the old people is identified by the root cause
2
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
analysis, which can be used to resolve the identified causes (Wu and Hsieh, 2013). This
results in prevention of falls (Fenn and Egan, 2012).
Professional Development and Management
In clinical governance, the final pillar is termed as, “Professional development and
management.” This pillar ensures to improve the health care services and is utilized for its
professional development (A clinical governance guide for remote and isolated health
services in Australia, 2013). This policy directs the rules of clinical practice for the staff and
helps them to take care of the elderly people living in the aged care homes (Phillips et al.,
2010).
Clinical Governance for Old Age Care Homes
Government of South Australia conducts SA Health Care programs like, “Preventing
Falls” and “Harm from falls” for the aged people. They have taken certain policy measures to
prevent falls in the elderly people. National quality and safety has 10 standards and among 10
standards, the two important standards are “Preventing Falls” and “Harm from falls”
(Sahealth.sa.gov.au, 2017). Organizations that provide health care services has certain
governance structure and system for reducing falls, which minimizes the injuries that are
caused due to falls (Church, Haas and Goodall, 2015). The Australian hospitals, communities
and the residential aged care homes got best practice guideline in 2009, for reducing the fall
in old people. They produced three different documents. One for hospitals, second one for the
Residential Aged care homes and third one for the community care. This governance was
established on January 1, 2009 (Sahealth.sa.gov.au, 2017). This governance had reported to
address various aspects like, interventions and precautionary measures for falls (Stevens et
al., 2015). They provided many possible risk factors and interventions for the falls in the aged
people (Myagedcare.gov.au, 2015).
Key Stakeholder of the Aged Care
Stakeholder can either be an individual or a group of people who can either impact or
get impacted by any activity. The aged care homes ‘primary stakeholders are as follows:
Beneficiaries
They are the owners of the aged care home and they get income from it.
Providers or helpers
They are the people who provide health care facilities for the elderly people.
3
results in prevention of falls (Fenn and Egan, 2012).
Professional Development and Management
In clinical governance, the final pillar is termed as, “Professional development and
management.” This pillar ensures to improve the health care services and is utilized for its
professional development (A clinical governance guide for remote and isolated health
services in Australia, 2013). This policy directs the rules of clinical practice for the staff and
helps them to take care of the elderly people living in the aged care homes (Phillips et al.,
2010).
Clinical Governance for Old Age Care Homes
Government of South Australia conducts SA Health Care programs like, “Preventing
Falls” and “Harm from falls” for the aged people. They have taken certain policy measures to
prevent falls in the elderly people. National quality and safety has 10 standards and among 10
standards, the two important standards are “Preventing Falls” and “Harm from falls”
(Sahealth.sa.gov.au, 2017). Organizations that provide health care services has certain
governance structure and system for reducing falls, which minimizes the injuries that are
caused due to falls (Church, Haas and Goodall, 2015). The Australian hospitals, communities
and the residential aged care homes got best practice guideline in 2009, for reducing the fall
in old people. They produced three different documents. One for hospitals, second one for the
Residential Aged care homes and third one for the community care. This governance was
established on January 1, 2009 (Sahealth.sa.gov.au, 2017). This governance had reported to
address various aspects like, interventions and precautionary measures for falls (Stevens et
al., 2015). They provided many possible risk factors and interventions for the falls in the aged
people (Myagedcare.gov.au, 2015).
Key Stakeholder of the Aged Care
Stakeholder can either be an individual or a group of people who can either impact or
get impacted by any activity. The aged care homes ‘primary stakeholders are as follows:
Beneficiaries
They are the owners of the aged care home and they get income from it.
Providers or helpers
They are the people who provide health care facilities for the elderly people.
3
Funders
They are the people who provide funds for facilitating the old people.
Old Age people
Old Age people are those who are directly involved in the Aged care homes (Winter,
Watt and Peel, 2012).
CPI Tools
Clinical Practice Improvement (CPI) improves the health care process and its results. It
is a methodology that provides multidimensional outcomes which can be directly applied in
patient’s clinical management process. CPI is a tool that, acts as an assistance to understand
and implement the feedbacks for supporting the knowledge in the clinical environment. It
mainly helps in the following processes:
i. To identify and diagnose the issue.
ii. To implement interventions.
iii. For re-measuring the results, to know whether the interventions were effective
enough or not.
Thus, CPI is referred as a tool that deals to organize the health care related issues.
The methodology of CPI is to explore the following (Qualitymatters.co, 2018):
a) What has to be achieved?
b) How to know that change can lead to improvement i.e., what must be
measured?
c) What kind of changes must be made that results as improvement?
CPI’s fundamental principles are listed below (Qualitymatters.co, 2018):
1) It is possible to analyse the health care process.
2) It is possible to measure the clinical process and its results.
3) A desire to implement change.
4) Reflective knowledge on human performance and essential care system related
to health care process is required.
5) In the health care process for effective improvements, multidisciplinary
teamwork and designing novel solutions are very much important.
4
They are the people who provide funds for facilitating the old people.
Old Age people
Old Age people are those who are directly involved in the Aged care homes (Winter,
Watt and Peel, 2012).
CPI Tools
Clinical Practice Improvement (CPI) improves the health care process and its results. It
is a methodology that provides multidimensional outcomes which can be directly applied in
patient’s clinical management process. CPI is a tool that, acts as an assistance to understand
and implement the feedbacks for supporting the knowledge in the clinical environment. It
mainly helps in the following processes:
i. To identify and diagnose the issue.
ii. To implement interventions.
iii. For re-measuring the results, to know whether the interventions were effective
enough or not.
Thus, CPI is referred as a tool that deals to organize the health care related issues.
The methodology of CPI is to explore the following (Qualitymatters.co, 2018):
a) What has to be achieved?
b) How to know that change can lead to improvement i.e., what must be
measured?
c) What kind of changes must be made that results as improvement?
CPI’s fundamental principles are listed below (Qualitymatters.co, 2018):
1) It is possible to analyse the health care process.
2) It is possible to measure the clinical process and its results.
3) A desire to implement change.
4) Reflective knowledge on human performance and essential care system related
to health care process is required.
5) In the health care process for effective improvements, multidisciplinary
teamwork and designing novel solutions are very much important.
4
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
According to various health care reports, the hospitals take actions and measures only
after the fall. But, this project demands implementing precautionary measure before the
occurrence of fall in the old people. Thus, a properly defined CPI tool is essential to
implement the precautionary measures. Various CPI tools are available to improve patient’s
safety and to improve the quality of health care services. The tools include like, Six Sigma,
Plan-Do-Study-Act (PDSA), Lean, Root cause analysis and so on.
Plan-Do-Study-Act (PDSA) Mechanism
This project considers "Plan-Do-Study-Act" mechanism as a perfect CPI tool for the
prevention of falls in the aged people. PDSA is a quality improving cycle. Its main objective
is to establish relationship between the modifications done in the process, which gives
positive impacts on the final outcomes of the process (Clinical Prevention And Population
Health Curriculum Framework, 2015).
Plan
Plan States: To provide nutritious food and medications to the aged people present in
the Aged care homes, for improving their health (NCOA, 2018) (Mucavele, 2013).
Expected Results of the Plan: The nutrients in the diet along with the medication at
the right time declines the rate of fall in the aged people, due to improved care and nutrition.
Plan’s Execution Steps:
1) Initially, the current fall rate in the elderly people will be estimated.
2) A diet plan for all the aged people will be distributed in the aged care homes.
3) The diet will be strictly followed along with the doctor prescribed
medications.
4) The providers or helpers will ensure that all the elderly people are provided
their respective diet.
5) These steps will be continued for the next six months.
6) The fall rate will be evaluated again, to check the results of the implemented
plan.
Do
What was observed?
1) It was observed that the aged people required help or assistance in reminding
to take their medications on time.
2) They faced difficulty in walking and standing, without any support.
5
after the fall. But, this project demands implementing precautionary measure before the
occurrence of fall in the old people. Thus, a properly defined CPI tool is essential to
implement the precautionary measures. Various CPI tools are available to improve patient’s
safety and to improve the quality of health care services. The tools include like, Six Sigma,
Plan-Do-Study-Act (PDSA), Lean, Root cause analysis and so on.
Plan-Do-Study-Act (PDSA) Mechanism
This project considers "Plan-Do-Study-Act" mechanism as a perfect CPI tool for the
prevention of falls in the aged people. PDSA is a quality improving cycle. Its main objective
is to establish relationship between the modifications done in the process, which gives
positive impacts on the final outcomes of the process (Clinical Prevention And Population
Health Curriculum Framework, 2015).
Plan
Plan States: To provide nutritious food and medications to the aged people present in
the Aged care homes, for improving their health (NCOA, 2018) (Mucavele, 2013).
Expected Results of the Plan: The nutrients in the diet along with the medication at
the right time declines the rate of fall in the aged people, due to improved care and nutrition.
Plan’s Execution Steps:
1) Initially, the current fall rate in the elderly people will be estimated.
2) A diet plan for all the aged people will be distributed in the aged care homes.
3) The diet will be strictly followed along with the doctor prescribed
medications.
4) The providers or helpers will ensure that all the elderly people are provided
their respective diet.
5) These steps will be continued for the next six months.
6) The fall rate will be evaluated again, to check the results of the implemented
plan.
Do
What was observed?
1) It was observed that the aged people required help or assistance in reminding
to take their medications on time.
2) They faced difficulty in walking and standing, without any support.
5
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
3) Every time young people or helpers were not around to give them the
required support to stand and walk.
4) Some hated consuming more tablets and took excuses for having their
tablets.
5) Deficiency of vitamin D and calcium was observed in the old people.
Study
What was studied?
a) It was studied that the aged people require additional supplement to strengthen
their bones.
b) The study projected that, the aged people need immediate support of
supportive objects to walk and stand all by themselves.
c) Further, it was observed from the study that, the aged people stayed at their
bed most of the time and they rarely went out to get additional vitamin D.
d) Additional calcium for strengthen their bones was missing.
Were the measured goals achieved?
The initial plan had certain flaws, which failed the plan. The encountered
flaws are listed below:
1) Lack of Vitamin D and calcium.
2) Lack of supportive objects for independently moving around.
3) Lack of knowledge about their medicines.
Act
Conclusion:
a) As elderly people felt uneasy to rely on other’s support, provide essential
support objects that help them to stand and walk by themselves. Thus, this will
help them to be independent.
b) Educate the aged people about the benefits of taking their medicines, on time.
This will help them to have their tablets without any excuses. Moreover, they
will realize the importance of their tablets and would be careful not to miss it
at any cost.
c) Thus, the elderly people can go out by themselves to intake sunlight, for
additional vitamin D.
6
required support to stand and walk.
4) Some hated consuming more tablets and took excuses for having their
tablets.
5) Deficiency of vitamin D and calcium was observed in the old people.
Study
What was studied?
a) It was studied that the aged people require additional supplement to strengthen
their bones.
b) The study projected that, the aged people need immediate support of
supportive objects to walk and stand all by themselves.
c) Further, it was observed from the study that, the aged people stayed at their
bed most of the time and they rarely went out to get additional vitamin D.
d) Additional calcium for strengthen their bones was missing.
Were the measured goals achieved?
The initial plan had certain flaws, which failed the plan. The encountered
flaws are listed below:
1) Lack of Vitamin D and calcium.
2) Lack of supportive objects for independently moving around.
3) Lack of knowledge about their medicines.
Act
Conclusion:
a) As elderly people felt uneasy to rely on other’s support, provide essential
support objects that help them to stand and walk by themselves. Thus, this will
help them to be independent.
b) Educate the aged people about the benefits of taking their medicines, on time.
This will help them to have their tablets without any excuses. Moreover, they
will realize the importance of their tablets and would be careful not to miss it
at any cost.
c) Thus, the elderly people can go out by themselves to intake sunlight, for
additional vitamin D.
6
Henceforth, the second cycle of PDSA will help to implement solutions to the flaws
observed in the first plan. Thus, solution for the flaws is adding enough supportive objects, in
the aged care homes, intake of sunlight for vitamin D and calcium supplements are
recommended in the next plan, as an improved plan.
Proposed Intervention
This section describes and explains the proposed interventions or plan.
Problem
The rate of fall in the old people has increased in the Australian aged care homes, to a
large extent.
Aim
This report aims to prevent fall in the aged people, by providing them nutritious diet.
Thus, the plan just enforces correct intake of nutritious food.
Problem Dimensions
The identified reasons for the fall are listed below:
1) Lack of nutritious diet.
2) Lack of knowledge about the benefits and value of the medications in the
patients.
3) Lack of independent support for standing and walking.
4) Lack of care and support in the aged care homes.
Proposal Justification
a) The plan just enforces on effective intake of nutritious food for the old people (more
than 65 years old) living in the Aged care homes.
b) The food rich in vitamin D are added in the diet such as, Salmon, mackerel, tuna and
beef’s liver. Soya milk, cheese and raw milk are the dairy products included in the
diet that contains vitamin D and calcium. Orange is the fruit that is added in the diet to
add Vitamin D intake in the old people. The food rich in vitamin D rich helps the old
people to recover from fractured bones that is observed in patient of Osteoporosis.
The fall in old people results in Osteoporosis.
Limitations of the Proposal
7
observed in the first plan. Thus, solution for the flaws is adding enough supportive objects, in
the aged care homes, intake of sunlight for vitamin D and calcium supplements are
recommended in the next plan, as an improved plan.
Proposed Intervention
This section describes and explains the proposed interventions or plan.
Problem
The rate of fall in the old people has increased in the Australian aged care homes, to a
large extent.
Aim
This report aims to prevent fall in the aged people, by providing them nutritious diet.
Thus, the plan just enforces correct intake of nutritious food.
Problem Dimensions
The identified reasons for the fall are listed below:
1) Lack of nutritious diet.
2) Lack of knowledge about the benefits and value of the medications in the
patients.
3) Lack of independent support for standing and walking.
4) Lack of care and support in the aged care homes.
Proposal Justification
a) The plan just enforces on effective intake of nutritious food for the old people (more
than 65 years old) living in the Aged care homes.
b) The food rich in vitamin D are added in the diet such as, Salmon, mackerel, tuna and
beef’s liver. Soya milk, cheese and raw milk are the dairy products included in the
diet that contains vitamin D and calcium. Orange is the fruit that is added in the diet to
add Vitamin D intake in the old people. The food rich in vitamin D rich helps the old
people to recover from fractured bones that is observed in patient of Osteoporosis.
The fall in old people results in Osteoporosis.
Limitations of the Proposal
7
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
a) This proposal fails to concentrate on the other essential care that the old
people require. For instance, independence through supportive objects and
knowledge about their medication. Thus, the important thing that this proposal
lacks is improving human balance.
b) Lacks additional calcium intake in the diet, as the old people have weak bones
and muscles that results in fall. Therefore, adding calcium intake in their diet
is important.
c) Though, the diet includes food is rich in vitamin D, it is not sufficient for the
old people. Because, it is also important to get sunlight exposure for providing
enough vitamin D. On the other hand, even the experts suggest the benefits of
sunlight exposure on the old people’s body parts like face and upper limbs just
for five to fifteen minutes. This is considered to save the old people from
Osteoporosis. Thus, the proposal lacks vitamin D, got through sunlight.
d) The proposal also require sponsors for providing funds to economically
support the old aged people living in the aged care homes.
Therefore, including solutions for these limitations can support this proposal to
accomplish.
Barriers for the Implementation
The barriers for fall prevention program includes, time management and economic
factors (Child et al., 2012).
Time Management
It is the primary factor that acts a as barrier for the elderly people, as the daily lifestyle
of the elderly people keeps changing due to their ailments. The elderly people require help
from other people to visit their doctors for routine check-up, to resolve their health problem.
But, their close ones might be busy with other works. Therefore, this results in time
management issue for their concerned ones, as they have to spend their time in waiting for
the taxi and the waiting time to meet the doctor (Child et al., 2012).
Economical Barrier
Various studies prove that, the cost used for resolving any proposed solution is the
biggest barrier of the project. More money is required to purchase the nutritious food
8
people require. For instance, independence through supportive objects and
knowledge about their medication. Thus, the important thing that this proposal
lacks is improving human balance.
b) Lacks additional calcium intake in the diet, as the old people have weak bones
and muscles that results in fall. Therefore, adding calcium intake in their diet
is important.
c) Though, the diet includes food is rich in vitamin D, it is not sufficient for the
old people. Because, it is also important to get sunlight exposure for providing
enough vitamin D. On the other hand, even the experts suggest the benefits of
sunlight exposure on the old people’s body parts like face and upper limbs just
for five to fifteen minutes. This is considered to save the old people from
Osteoporosis. Thus, the proposal lacks vitamin D, got through sunlight.
d) The proposal also require sponsors for providing funds to economically
support the old aged people living in the aged care homes.
Therefore, including solutions for these limitations can support this proposal to
accomplish.
Barriers for the Implementation
The barriers for fall prevention program includes, time management and economic
factors (Child et al., 2012).
Time Management
It is the primary factor that acts a as barrier for the elderly people, as the daily lifestyle
of the elderly people keeps changing due to their ailments. The elderly people require help
from other people to visit their doctors for routine check-up, to resolve their health problem.
But, their close ones might be busy with other works. Therefore, this results in time
management issue for their concerned ones, as they have to spend their time in waiting for
the taxi and the waiting time to meet the doctor (Child et al., 2012).
Economical Barrier
Various studies prove that, the cost used for resolving any proposed solution is the
biggest barrier of the project. More money is required to purchase the nutritious food
8
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
resources, for the aged care homes. Thus, appropriate medications by consulting a doctor is
also economically difficult. The elderly people often get health issues, and consulting a
doctor often for all their issues might not be possible by all. Moreover, it is not possible for
the old people to use public transport for visiting the doctor and hence a private taxi has to be
used. This becomes the economic barrier (Child et al., 2012).
Project Evaluation
This section includes evaluating the measures and results of the proposed interventions.
Evaluation Result
1. Plan’s Strategic Fit
The current fall rate in the old people is estimated and is compared after completing
the plan, for a set period of time.
2. Project Validity
The results are evaluated after a duration of six months.
3. Progress and effectiveness of the Plan
This project considers CPI tool as its foundation and it implements using effective
PDSA cycle, which helps it to identify the drawbacks of the plan and help in
improving the plan in the next cycle.
4. Resource Efficiency
This project lacks management of resources like nutritious food.
5. Effective Management
This project also lacks effective management.
6. Plan’s Sustainability
The plan will be sustainable only it is financially supported, to facilitate the aged care
homes with nutritious food, supportive objects to walk. But, this project plan doesn’t provide
details about methods that supporting funds. One of the method is promotions of aged care
homes.
References
9
also economically difficult. The elderly people often get health issues, and consulting a
doctor often for all their issues might not be possible by all. Moreover, it is not possible for
the old people to use public transport for visiting the doctor and hence a private taxi has to be
used. This becomes the economic barrier (Child et al., 2012).
Project Evaluation
This section includes evaluating the measures and results of the proposed interventions.
Evaluation Result
1. Plan’s Strategic Fit
The current fall rate in the old people is estimated and is compared after completing
the plan, for a set period of time.
2. Project Validity
The results are evaluated after a duration of six months.
3. Progress and effectiveness of the Plan
This project considers CPI tool as its foundation and it implements using effective
PDSA cycle, which helps it to identify the drawbacks of the plan and help in
improving the plan in the next cycle.
4. Resource Efficiency
This project lacks management of resources like nutritious food.
5. Effective Management
This project also lacks effective management.
6. Plan’s Sustainability
The plan will be sustainable only it is financially supported, to facilitate the aged care
homes with nutritious food, supportive objects to walk. But, this project plan doesn’t provide
details about methods that supporting funds. One of the method is promotions of aged care
homes.
References
9
A clinical governance guide for remote and isolated health services in Australia.
(2013). CRANAplus. [online] Available at: https://crana.org.au/uploads/pdfs/CRANAplus-
Clinical-Governance-Guide.pdf.
Avant.org.au. (2018). Clinical governance. [online] Available at:
http://www.avant.org.au/resources/start-a-practice/practice-planning/business-planning/
clinical-governance/ [Accessed 8 Jan. 2018].
Child, S., Goodwin, V., Garside, R., Jones-Hughes, T., Boddy, K. and Stein, K. (2012).
Factors influencing the implementation of fall-prevention programmes: a systematic review
and synthesis of qualitative studies. Implementation Science, 7(1).
Church, J., Haas, M. and Goodall, S. (2015). Cost Effectiveness of Falls and Injury
Prevention Strategies for Older Adults Living in Residential Aged Care
Facilities. PharmacoEconomics, 33(12), pp.1301-1310.
Clinical Governance Framework. (2012). HealthDirect Australia, (3).
Clinical Governance, Safety and Quality Policy Framework. (2016). Department of Health,
Western Australia. [online] Available at:
http://www.health.wa.gov.au/circularsnew/frameworks/Clinical_Governance,_Safety_and_Q
uality.pdf.
Clinical Prevention And Population Health Curriculum Framework. (2015). Association for
Prevention Teaching and Research, [online] (3). Available at:
http://c.ymcdn.com/sites/www.aptrweb.org/resource/resmgr/HPCTF_Docs/
Revised_CPPH_Framework_2.201.pdf [Accessed 8 Jan. 2018].
Fenn, P. and Egan, T. (2012). Risk management in the NHS: governance, finance and clinical
risk. Clinical Medicine, 12(1), pp.25-28.
Mucavele, P. (2013). Providing a balanced and nutritious diet. Early Years Educator, 14(10),
pp.38-44.
Myagedcare.gov.au. (2015). Preventing falls in the elderly. [online] Available at:
https://www.myagedcare.gov.au/getting-started/healthy-and-active-ageing/preventing-falls-
in-elderly [Accessed 8 Jan. 2018].
10
(2013). CRANAplus. [online] Available at: https://crana.org.au/uploads/pdfs/CRANAplus-
Clinical-Governance-Guide.pdf.
Avant.org.au. (2018). Clinical governance. [online] Available at:
http://www.avant.org.au/resources/start-a-practice/practice-planning/business-planning/
clinical-governance/ [Accessed 8 Jan. 2018].
Child, S., Goodwin, V., Garside, R., Jones-Hughes, T., Boddy, K. and Stein, K. (2012).
Factors influencing the implementation of fall-prevention programmes: a systematic review
and synthesis of qualitative studies. Implementation Science, 7(1).
Church, J., Haas, M. and Goodall, S. (2015). Cost Effectiveness of Falls and Injury
Prevention Strategies for Older Adults Living in Residential Aged Care
Facilities. PharmacoEconomics, 33(12), pp.1301-1310.
Clinical Governance Framework. (2012). HealthDirect Australia, (3).
Clinical Governance, Safety and Quality Policy Framework. (2016). Department of Health,
Western Australia. [online] Available at:
http://www.health.wa.gov.au/circularsnew/frameworks/Clinical_Governance,_Safety_and_Q
uality.pdf.
Clinical Prevention And Population Health Curriculum Framework. (2015). Association for
Prevention Teaching and Research, [online] (3). Available at:
http://c.ymcdn.com/sites/www.aptrweb.org/resource/resmgr/HPCTF_Docs/
Revised_CPPH_Framework_2.201.pdf [Accessed 8 Jan. 2018].
Fenn, P. and Egan, T. (2012). Risk management in the NHS: governance, finance and clinical
risk. Clinical Medicine, 12(1), pp.25-28.
Mucavele, P. (2013). Providing a balanced and nutritious diet. Early Years Educator, 14(10),
pp.38-44.
Myagedcare.gov.au. (2015). Preventing falls in the elderly. [online] Available at:
https://www.myagedcare.gov.au/getting-started/healthy-and-active-ageing/preventing-falls-
in-elderly [Accessed 8 Jan. 2018].
10
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.