CNA255: University Nursing Case Study: Ms. Nancy Huang's Diabetes
VerifiedAdded on 2021/06/17
|7
|2543
|52
Case Study
AI Summary
This case study presents Ms. Nancy Huang, a 29-year-old university student with type 1 diabetes, admitted to the emergency bay due to hyperglycemia and other complications. The assessment reveals vital signs, including a high BGL, confusion, and frequent urination. The analysis explores the relationship between her stress, lifestyle changes, and the exacerbation of her diabetes. The nursing problems are identified as unstable blood glucose levels, disturbed sensory perception, and impaired skin integrity. The assignment details goals and interventions, such as monitoring blood glucose levels and mental status, and provides rationales for each action. It also includes a reflection on how this encounter informs future nursing practice, emphasizing the importance of critical thinking and evidence-based practice in patient care. The document references several sources to support the analysis and recommendations.
CNA255: Scenario 1- Ms Nancy Huang
Consider the patient
situation
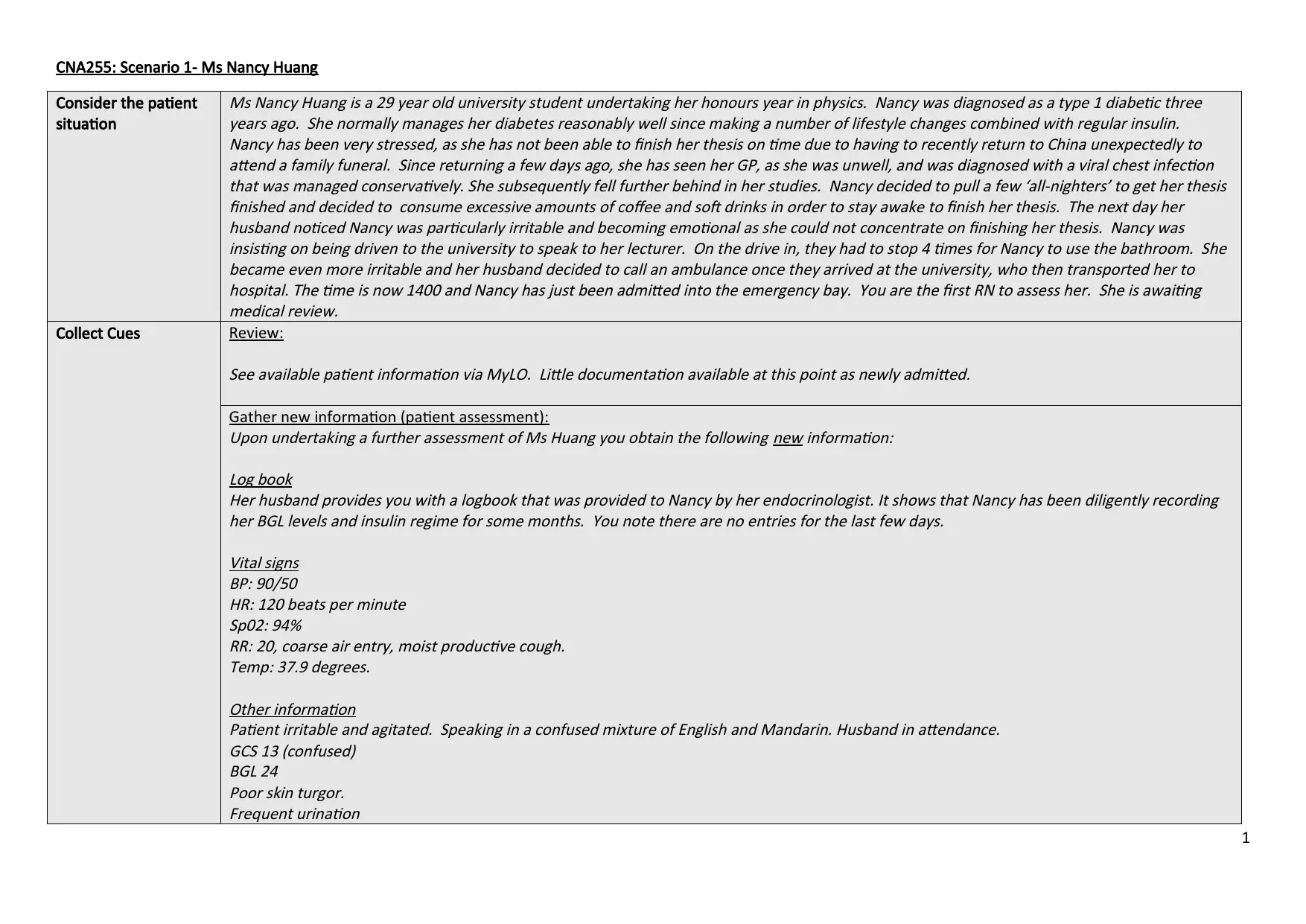
Ms Nancy Huang is a 29 year old university student undertaking her honours year in physics. Nancy was diagnosed as a type 1 diabetic three
years ago. She normally manages her diabetes reasonably well since making a number of lifestyle changes combined with regular insulin.
Nancy has been very stressed, as she has not been able to finish her thesis on time due to having to recently return to China unexpectedly to
attend a family funeral. Since returning a few days ago, she has seen her GP, as she was unwell, and was diagnosed with a viral chest infection
that was managed conservatively. She subsequently fell further behind in her studies. Nancy decided to pull a few ‘all-nighters’ to get her thesis
finished and decided to consume excessive amounts of coffee and soft drinks in order to stay awake to finish her thesis. The next day her
husband noticed Nancy was particularly irritable and becoming emotional as she could not concentrate on finishing her thesis. Nancy was
insisting on being driven to the university to speak to her lecturer. On the drive in, they had to stop 4 times for Nancy to use the bathroom. She
became even more irritable and her husband decided to call an ambulance once they arrived at the university, who then transported her to
hospital. The time is now 1400 and Nancy has just been admitted into the emergency bay. You are the first RN to assess her. She is awaiting
medical review.
Collect Cues Review:
See available patient information via MyLO. Little documentation available at this point as newly admitted.
Gather new information (patient assessment):
Upon undertaking a further assessment of Ms Huang you obtain the following new information:
Log book
Her husband provides you with a logbook that was provided to Nancy by her endocrinologist. It shows that Nancy has been diligently recording
her BGL levels and insulin regime for some months. You note there are no entries for the last few days.
Vital signs
BP: 90/50
HR: 120 beats per minute
Sp02: 94%
RR: 20, coarse air entry, moist productive cough.
Temp: 37.9 degrees.
Other information
Patient irritable and agitated. Speaking in a confused mixture of English and Mandarin. Husband in attendance.
GCS 13 (confused)
BGL 24
Poor skin turgor.
Frequent urination
1
Consider the patient
situation
Ms Nancy Huang is a 29 year old university student undertaking her honours year in physics. Nancy was diagnosed as a type 1 diabetic three
years ago. She normally manages her diabetes reasonably well since making a number of lifestyle changes combined with regular insulin.
Nancy has been very stressed, as she has not been able to finish her thesis on time due to having to recently return to China unexpectedly to
attend a family funeral. Since returning a few days ago, she has seen her GP, as she was unwell, and was diagnosed with a viral chest infection
that was managed conservatively. She subsequently fell further behind in her studies. Nancy decided to pull a few ‘all-nighters’ to get her thesis
finished and decided to consume excessive amounts of coffee and soft drinks in order to stay awake to finish her thesis. The next day her
husband noticed Nancy was particularly irritable and becoming emotional as she could not concentrate on finishing her thesis. Nancy was
insisting on being driven to the university to speak to her lecturer. On the drive in, they had to stop 4 times for Nancy to use the bathroom. She
became even more irritable and her husband decided to call an ambulance once they arrived at the university, who then transported her to
hospital. The time is now 1400 and Nancy has just been admitted into the emergency bay. You are the first RN to assess her. She is awaiting
medical review.
Collect Cues Review:
See available patient information via MyLO. Little documentation available at this point as newly admitted.
Gather new information (patient assessment):
Upon undertaking a further assessment of Ms Huang you obtain the following new information:
Log book
Her husband provides you with a logbook that was provided to Nancy by her endocrinologist. It shows that Nancy has been diligently recording
her BGL levels and insulin regime for some months. You note there are no entries for the last few days.
Vital signs
BP: 90/50
HR: 120 beats per minute
Sp02: 94%
RR: 20, coarse air entry, moist productive cough.
Temp: 37.9 degrees.
Other information
Patient irritable and agitated. Speaking in a confused mixture of English and Mandarin. Husband in attendance.
GCS 13 (confused)
BGL 24
Poor skin turgor.
Frequent urination
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
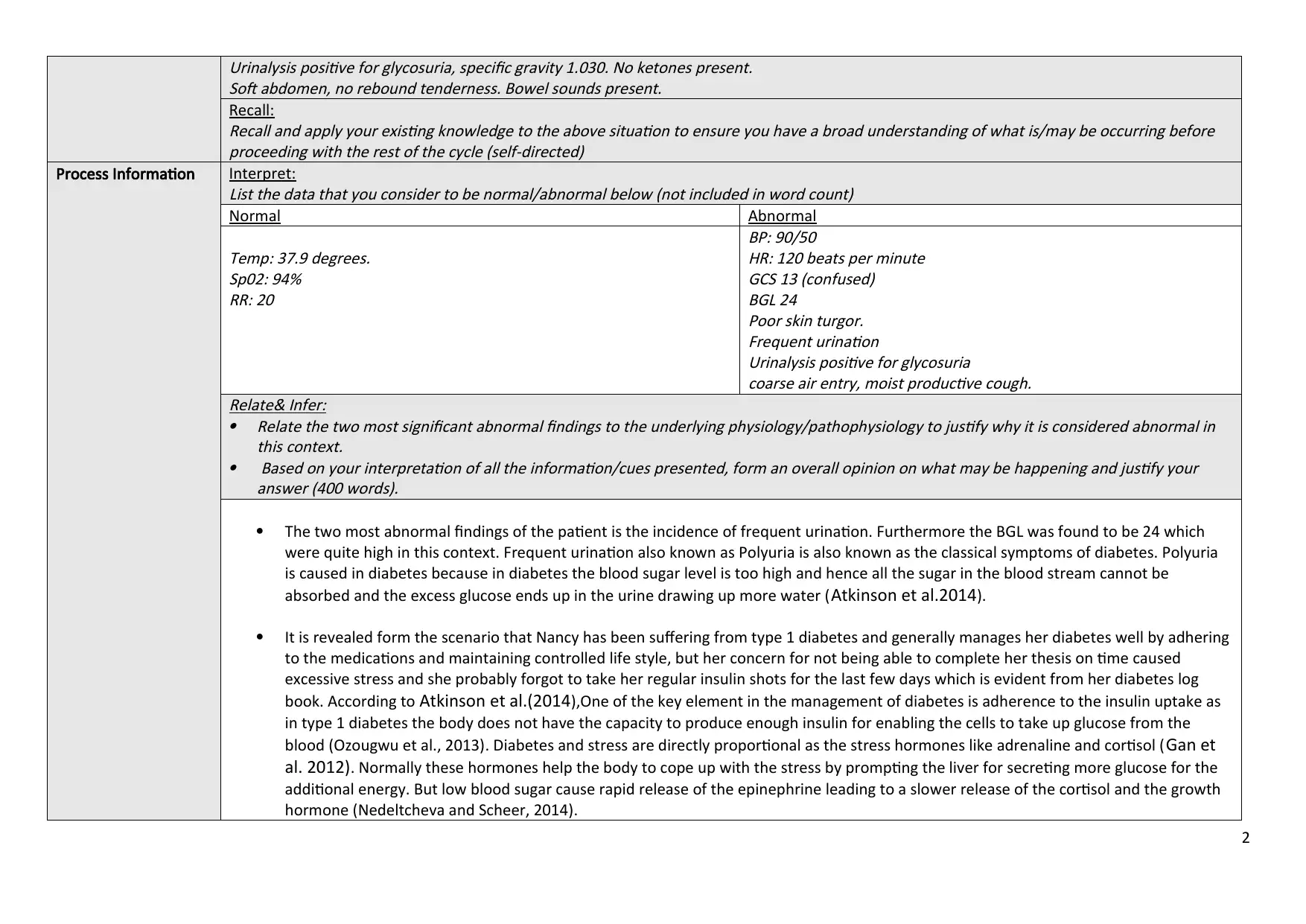
Urinalysis positive for glycosuria, specific gravity 1.030. No ketones present.
Soft abdomen, no rebound tenderness. Bowel sounds present.
Recall:
Recall and apply your existing knowledge to the above situation to ensure you have a broad understanding of what is/may be occurring before
proceeding with the rest of the cycle (self-directed)
Process Information Interpret:
List the data that you consider to be normal/abnormal below (not included in word count)
Normal Abnormal
Temp: 37.9 degrees.
Sp02: 94%
RR: 20
BP: 90/50
HR: 120 beats per minute
GCS 13 (confused)
BGL 24
Poor skin turgor.
Frequent urination
Urinalysis positive for glycosuria
coarse air entry, moist productive cough.
Relate& Infer:
Relate the two most significant abnormal findings to the underlying physiology/pathophysiology to justify why it is considered abnormal in
this context.
Based on your interpretation of all the information/cues presented, form an overall opinion on what may be happening and justify your
answer (400 words).
The two most abnormal findings of the patient is the incidence of frequent urination. Furthermore the BGL was found to be 24 which
were quite high in this context. Frequent urination also known as Polyuria is also known as the classical symptoms of diabetes. Polyuria
is caused in diabetes because in diabetes the blood sugar level is too high and hence all the sugar in the blood stream cannot be
absorbed and the excess glucose ends up in the urine drawing up more water (Atkinson et al.2014).
It is revealed form the scenario that Nancy has been suffering from type 1 diabetes and generally manages her diabetes well by adhering
to the medications and maintaining controlled life style, but her concern for not being able to complete her thesis on time caused
excessive stress and she probably forgot to take her regular insulin shots for the last few days which is evident from her diabetes log
book. According to Atkinson et al.(2014),One of the key element in the management of diabetes is adherence to the insulin uptake as
in type 1 diabetes the body does not have the capacity to produce enough insulin for enabling the cells to take up glucose from the
blood (Ozougwu et al., 2013). Diabetes and stress are directly proportional as the stress hormones like adrenaline and cortisol (Gan et
al. 2012). Normally these hormones help the body to cope up with the stress by prompting the liver for secreting more glucose for the
additional energy. But low blood sugar cause rapid release of the epinephrine leading to a slower release of the cortisol and the growth
hormone (Nedeltcheva and Scheer, 2014).
2
Soft abdomen, no rebound tenderness. Bowel sounds present.
Recall:
Recall and apply your existing knowledge to the above situation to ensure you have a broad understanding of what is/may be occurring before
proceeding with the rest of the cycle (self-directed)
Process Information Interpret:
List the data that you consider to be normal/abnormal below (not included in word count)
Normal Abnormal
Temp: 37.9 degrees.
Sp02: 94%
RR: 20
BP: 90/50
HR: 120 beats per minute
GCS 13 (confused)
BGL 24
Poor skin turgor.
Frequent urination
Urinalysis positive for glycosuria
coarse air entry, moist productive cough.
Relate& Infer:
Relate the two most significant abnormal findings to the underlying physiology/pathophysiology to justify why it is considered abnormal in
this context.
Based on your interpretation of all the information/cues presented, form an overall opinion on what may be happening and justify your
answer (400 words).
The two most abnormal findings of the patient is the incidence of frequent urination. Furthermore the BGL was found to be 24 which
were quite high in this context. Frequent urination also known as Polyuria is also known as the classical symptoms of diabetes. Polyuria
is caused in diabetes because in diabetes the blood sugar level is too high and hence all the sugar in the blood stream cannot be
absorbed and the excess glucose ends up in the urine drawing up more water (Atkinson et al.2014).
It is revealed form the scenario that Nancy has been suffering from type 1 diabetes and generally manages her diabetes well by adhering
to the medications and maintaining controlled life style, but her concern for not being able to complete her thesis on time caused
excessive stress and she probably forgot to take her regular insulin shots for the last few days which is evident from her diabetes log
book. According to Atkinson et al.(2014),One of the key element in the management of diabetes is adherence to the insulin uptake as
in type 1 diabetes the body does not have the capacity to produce enough insulin for enabling the cells to take up glucose from the
blood (Ozougwu et al., 2013). Diabetes and stress are directly proportional as the stress hormones like adrenaline and cortisol (Gan et
al. 2012). Normally these hormones help the body to cope up with the stress by prompting the liver for secreting more glucose for the
additional energy. But low blood sugar cause rapid release of the epinephrine leading to a slower release of the cortisol and the growth
hormone (Nedeltcheva and Scheer, 2014).
2
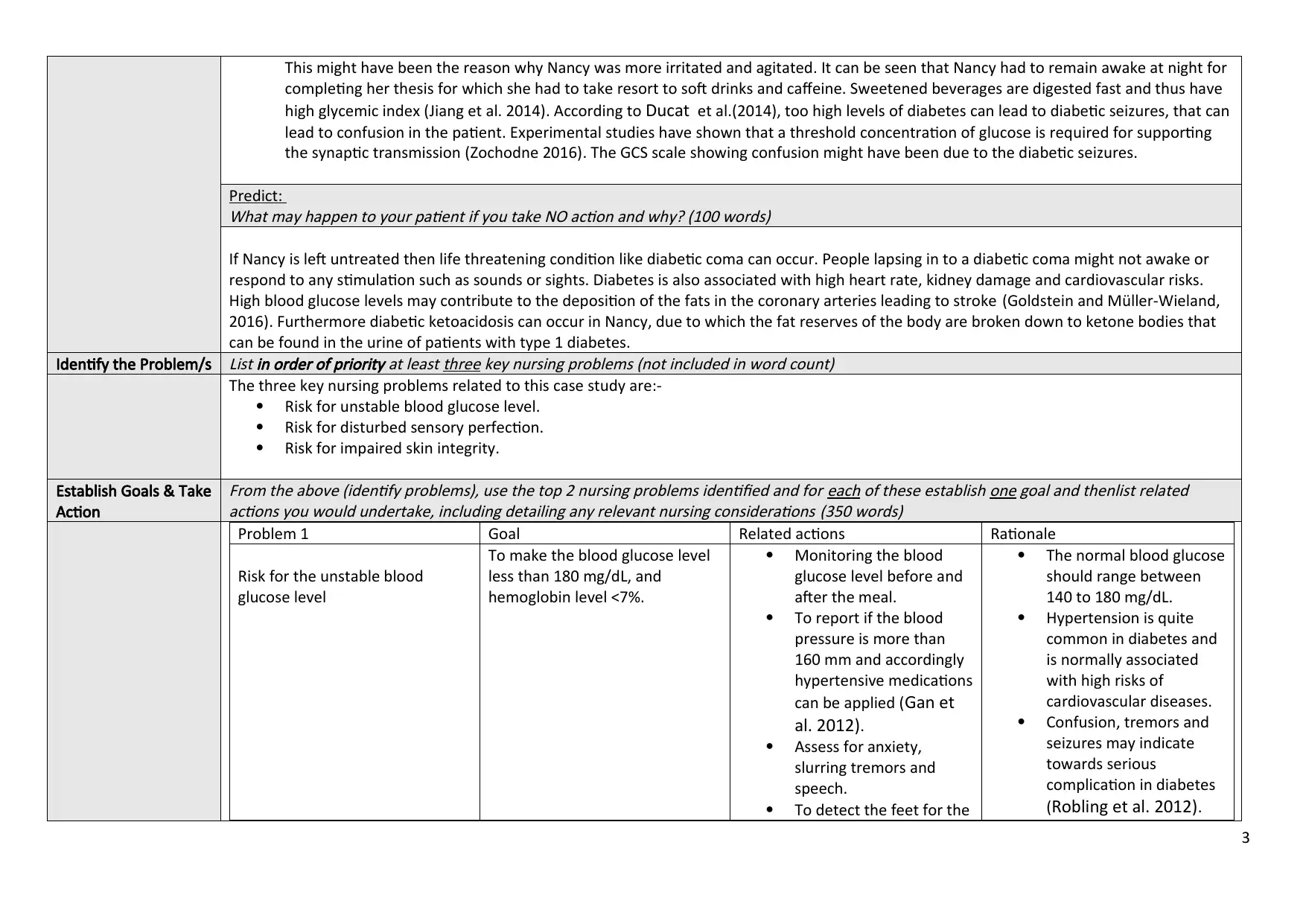
This might have been the reason why Nancy was more irritated and agitated. It can be seen that Nancy had to remain awake at night for
completing her thesis for which she had to take resort to soft drinks and caffeine. Sweetened beverages are digested fast and thus have
high glycemic index (Jiang et al. 2014). According to Ducat et al.(2014), too high levels of diabetes can lead to diabetic seizures, that can
lead to confusion in the patient. Experimental studies have shown that a threshold concentration of glucose is required for supporting
the synaptic transmission (Zochodne 2016). The GCS scale showing confusion might have been due to the diabetic seizures.
Predict:
What may happen to your patient if you take NO action and why? (100 words)
If Nancy is left untreated then life threatening condition like diabetic coma can occur. People lapsing in to a diabetic coma might not awake or
respond to any stimulation such as sounds or sights. Diabetes is also associated with high heart rate, kidney damage and cardiovascular risks.
High blood glucose levels may contribute to the deposition of the fats in the coronary arteries leading to stroke (Goldstein and Müller-Wieland,
2016). Furthermore diabetic ketoacidosis can occur in Nancy, due to which the fat reserves of the body are broken down to ketone bodies that
can be found in the urine of patients with type 1 diabetes.
Identify the Problem/s
List in order of priority at least three key nursing problems (not included in word count)
The three key nursing problems related to this case study are:-
Risk for unstable blood glucose level.
Risk for disturbed sensory perfection.
Risk for impaired skin integrity.
Establish Goals & Take
Action
From the above (identify problems), use the top 2 nursing problems identified and for each of these establish one goal and thenlist related
actions you would undertake, including detailing any relevant nursing considerations (350 words)
Problem 1 Goal Related actions Rationale
Risk for the unstable blood
glucose level
To make the blood glucose level
less than 180 mg/dL, and
hemoglobin level <7%.
Monitoring the blood
glucose level before and
after the meal.
To report if the blood
pressure is more than
160 mm and accordingly
hypertensive medications
can be applied (Gan et
al. 2012).
Assess for anxiety,
slurring tremors and
speech.
To detect the feet for the
The normal blood glucose
should range between
140 to 180 mg/dL.
Hypertension is quite
common in diabetes and
is normally associated
with high risks of
cardiovascular diseases.
Confusion, tremors and
seizures may indicate
towards serious
complication in diabetes
(Robling et al. 2012).
3
completing her thesis for which she had to take resort to soft drinks and caffeine. Sweetened beverages are digested fast and thus have
high glycemic index (Jiang et al. 2014). According to Ducat et al.(2014), too high levels of diabetes can lead to diabetic seizures, that can
lead to confusion in the patient. Experimental studies have shown that a threshold concentration of glucose is required for supporting
the synaptic transmission (Zochodne 2016). The GCS scale showing confusion might have been due to the diabetic seizures.
Predict:
What may happen to your patient if you take NO action and why? (100 words)
If Nancy is left untreated then life threatening condition like diabetic coma can occur. People lapsing in to a diabetic coma might not awake or
respond to any stimulation such as sounds or sights. Diabetes is also associated with high heart rate, kidney damage and cardiovascular risks.
High blood glucose levels may contribute to the deposition of the fats in the coronary arteries leading to stroke (Goldstein and Müller-Wieland,
2016). Furthermore diabetic ketoacidosis can occur in Nancy, due to which the fat reserves of the body are broken down to ketone bodies that
can be found in the urine of patients with type 1 diabetes.
Identify the Problem/s
List in order of priority at least three key nursing problems (not included in word count)
The three key nursing problems related to this case study are:-
Risk for unstable blood glucose level.
Risk for disturbed sensory perfection.
Risk for impaired skin integrity.
Establish Goals & Take
Action
From the above (identify problems), use the top 2 nursing problems identified and for each of these establish one goal and thenlist related
actions you would undertake, including detailing any relevant nursing considerations (350 words)
Problem 1 Goal Related actions Rationale
Risk for the unstable blood
glucose level
To make the blood glucose level
less than 180 mg/dL, and
hemoglobin level <7%.
Monitoring the blood
glucose level before and
after the meal.
To report if the blood
pressure is more than
160 mm and accordingly
hypertensive medications
can be applied (Gan et
al. 2012).
Assess for anxiety,
slurring tremors and
speech.
To detect the feet for the
The normal blood glucose
should range between
140 to 180 mg/dL.
Hypertension is quite
common in diabetes and
is normally associated
with high risks of
cardiovascular diseases.
Confusion, tremors and
seizures may indicate
towards serious
complication in diabetes
(Robling et al. 2012).
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
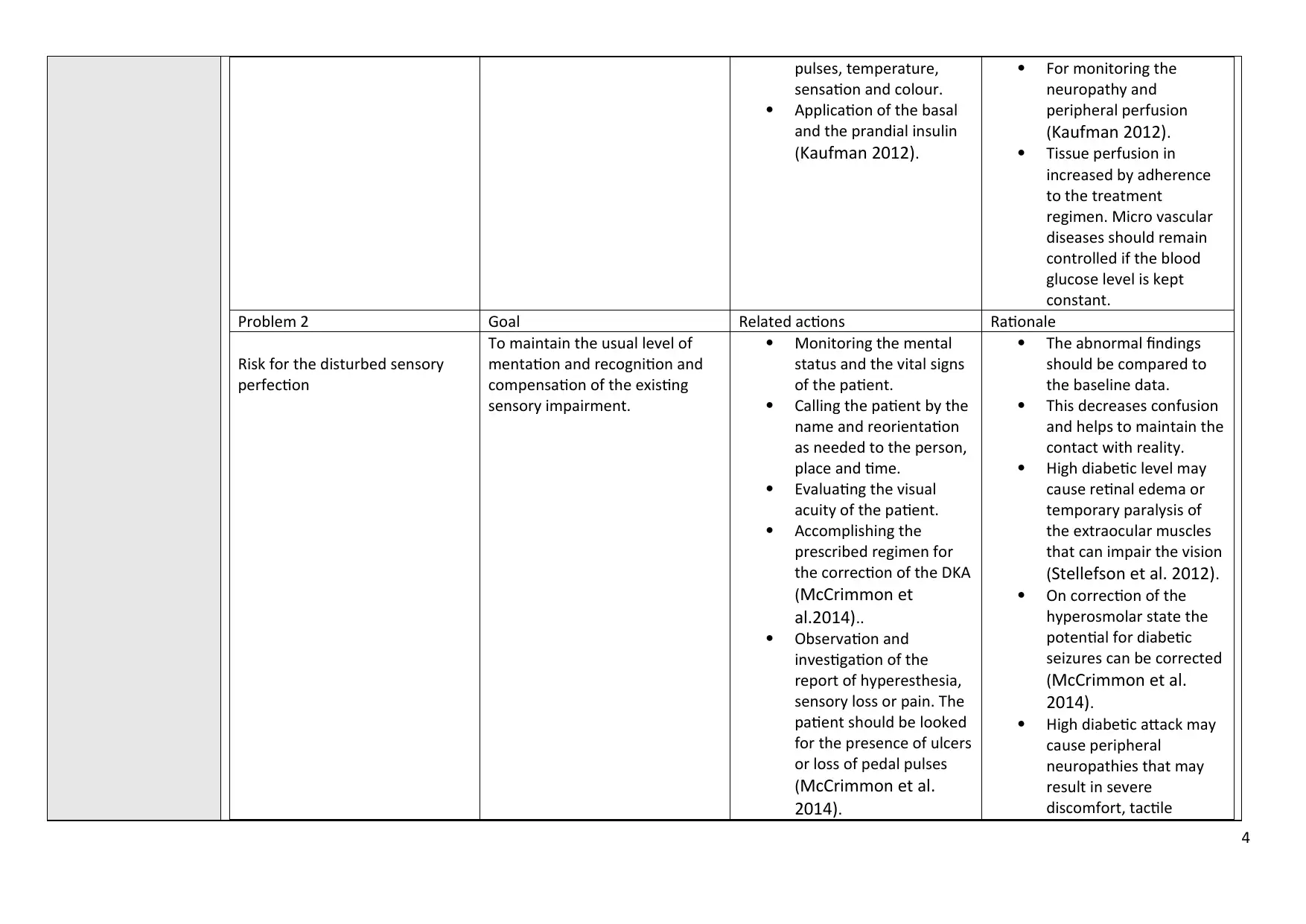
pulses, temperature,
sensation and colour.
Application of the basal
and the prandial insulin
(Kaufman 2012).
For monitoring the
neuropathy and
peripheral perfusion
(Kaufman 2012).
Tissue perfusion in
increased by adherence
to the treatment
regimen. Micro vascular
diseases should remain
controlled if the blood
glucose level is kept
constant.
Problem 2 Goal Related actions Rationale
Risk for the disturbed sensory
perfection
To maintain the usual level of
mentation and recognition and
compensation of the existing
sensory impairment.
Monitoring the mental
status and the vital signs
of the patient.
Calling the patient by the
name and reorientation
as needed to the person,
place and time.
Evaluating the visual
acuity of the patient.
Accomplishing the
prescribed regimen for
the correction of the DKA
(McCrimmon et
al.2014)..
Observation and
investigation of the
report of hyperesthesia,
sensory loss or pain. The
patient should be looked
for the presence of ulcers
or loss of pedal pulses
(McCrimmon et al.
2014).
The abnormal findings
should be compared to
the baseline data.
This decreases confusion
and helps to maintain the
contact with reality.
High diabetic level may
cause retinal edema or
temporary paralysis of
the extraocular muscles
that can impair the vision
(Stellefson et al. 2012).
On correction of the
hyperosmolar state the
potential for diabetic
seizures can be corrected
(McCrimmon et al.
2014).
High diabetic attack may
cause peripheral
neuropathies that may
result in severe
discomfort, tactile
4
sensation and colour.
Application of the basal
and the prandial insulin
(Kaufman 2012).
For monitoring the
neuropathy and
peripheral perfusion
(Kaufman 2012).
Tissue perfusion in
increased by adherence
to the treatment
regimen. Micro vascular
diseases should remain
controlled if the blood
glucose level is kept
constant.
Problem 2 Goal Related actions Rationale
Risk for the disturbed sensory
perfection
To maintain the usual level of
mentation and recognition and
compensation of the existing
sensory impairment.
Monitoring the mental
status and the vital signs
of the patient.
Calling the patient by the
name and reorientation
as needed to the person,
place and time.
Evaluating the visual
acuity of the patient.
Accomplishing the
prescribed regimen for
the correction of the DKA
(McCrimmon et
al.2014)..
Observation and
investigation of the
report of hyperesthesia,
sensory loss or pain. The
patient should be looked
for the presence of ulcers
or loss of pedal pulses
(McCrimmon et al.
2014).
The abnormal findings
should be compared to
the baseline data.
This decreases confusion
and helps to maintain the
contact with reality.
High diabetic level may
cause retinal edema or
temporary paralysis of
the extraocular muscles
that can impair the vision
(Stellefson et al. 2012).
On correction of the
hyperosmolar state the
potential for diabetic
seizures can be corrected
(McCrimmon et al.
2014).
High diabetic attack may
cause peripheral
neuropathies that may
result in severe
discomfort, tactile
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
sensation and risk of
dermal injury or
impairment of balance
(McCrimmon et al.
2014).
Evaluate outcomes&
Reflect on new
learning
Briefly describe how you would evaluate the effectiveness of the care provided (i.e. what do you want to happen?) and reflect on how this
encounter has informed your nursing practice if you were to encounter a similar situation in the future (150 words).
Evaluation of the nursing care would be evident from the nursing outcomes and the feedback shared by the Nancy and her husband. The better
outcomes should include the glucose level less than 180 mg/dL, the patient would display a normal cognitive status. The stress level will be
decreased with no signs of irritation or confusion. The nursing interventions should also contain the self management strategies for diabetes,
regarding the insulin uptake and maintenance of proper records (Haas et al. 2012).
My encounter with this patient would be helpful in my future practice as I believe that it has helped me to enhance my decision making skills by
applying my critical thinking skills. My eagerness for understanding the underlying pathophysiology has helped me to apply evidence based
practice in my nursing research, as I have brainstormed through several nursing articles to understand the pathophysiology and is connected to
the symptoms. I have been successful in evaluating the patient outcome, which I feel is an integral part of the nursing professional standards.
5
dermal injury or
impairment of balance
(McCrimmon et al.
2014).
Evaluate outcomes&
Reflect on new
learning
Briefly describe how you would evaluate the effectiveness of the care provided (i.e. what do you want to happen?) and reflect on how this
encounter has informed your nursing practice if you were to encounter a similar situation in the future (150 words).
Evaluation of the nursing care would be evident from the nursing outcomes and the feedback shared by the Nancy and her husband. The better
outcomes should include the glucose level less than 180 mg/dL, the patient would display a normal cognitive status. The stress level will be
decreased with no signs of irritation or confusion. The nursing interventions should also contain the self management strategies for diabetes,
regarding the insulin uptake and maintenance of proper records (Haas et al. 2012).
My encounter with this patient would be helpful in my future practice as I believe that it has helped me to enhance my decision making skills by
applying my critical thinking skills. My eagerness for understanding the underlying pathophysiology has helped me to apply evidence based
practice in my nursing research, as I have brainstormed through several nursing articles to understand the pathophysiology and is connected to
the symptoms. I have been successful in evaluating the patient outcome, which I feel is an integral part of the nursing professional standards.
5
References
American Diabetes Association, 2013. Standards of medical care in diabetes—2013.
Diabetes care,
36(Suppl 1), p.S11.
Atkinson, M.A., Eisenbarth, G.S. and Michels, A.W., 2014. Type 1 diabetes.
The Lancet,
383(9911), pp.69-82.
Ducat, L., Philipson, L.H. and Anderson, B.J., 2014. The mental health comorbidities of diabetes.
Jama,
312(7), pp.691-692.
Gan, M.J., Albanese-O’Neill, A. and Haller, M.J., 2012. Type 1 diabetes: current concepts in epidemiology, pathophysiology, clinical care, and research.
Current
problems in pediatric and adolescent health care,
42(10), pp.269-291.
Goldstein, B.J. and Müller-Wieland, D. eds., 2016.
Type 1 diabetes: principles and practice. CRC Press.
Haas, L., Maryniuk, M., Beck, J., Cox, C.E., Duker, P., Edwards, L., Fisher, E., Hanson, L., Kent, D., Kolb, L. and McLaughlin, S., 2012. National standards for
diabetes self-management education and support.
The Diabetes Educator,
38(5), pp.619-629.
Jiang, X., Zhang, D. and Jiang, W., 2014. Coffee and caffeine intake and incidence of type 1 diabetes mellitus: a meta-analysis of prospective studies.
European journal of
nutrition,
53(1), pp.25-38.
Kaufman, F. R. (Ed.). (2012).
Medical management of type 1 diabetes. American Diabetes Association.
McCrimmon, R.J., Ryan, C.M. and Frier, B.M., 2012. Diabetes and cognitive dysfunction.
The Lancet,
379(9833), pp.2291-2299.
Mixcoatl-Zecuatl, T. and Calcutt, N.A., 2013. Biology and pathophysiology of painful diabetic neuropathy. In
Painful Diabetic Polyneuropathy (pp. 13-26). Springer, New York,
NY.
Nedeltcheva, A.V. and Scheer, F.A., 2014. Metabolic effects of sleep disruption, links to obesity and diabetes.
Current opinion in endocrinology, diabetes, and obesity,
21(4),
p.293.
Ozougwu, J.C., Obimba, K.C., Belonwu, C.D. and Unakalamba, C.B., 2013. The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus.
Journal of
Physiology and Pathophysiology,
4(4), pp.46-57.
6
American Diabetes Association, 2013. Standards of medical care in diabetes—2013.
Diabetes care,
36(Suppl 1), p.S11.
Atkinson, M.A., Eisenbarth, G.S. and Michels, A.W., 2014. Type 1 diabetes.
The Lancet,
383(9911), pp.69-82.
Ducat, L., Philipson, L.H. and Anderson, B.J., 2014. The mental health comorbidities of diabetes.
Jama,
312(7), pp.691-692.
Gan, M.J., Albanese-O’Neill, A. and Haller, M.J., 2012. Type 1 diabetes: current concepts in epidemiology, pathophysiology, clinical care, and research.
Current
problems in pediatric and adolescent health care,
42(10), pp.269-291.
Goldstein, B.J. and Müller-Wieland, D. eds., 2016.
Type 1 diabetes: principles and practice. CRC Press.
Haas, L., Maryniuk, M., Beck, J., Cox, C.E., Duker, P., Edwards, L., Fisher, E., Hanson, L., Kent, D., Kolb, L. and McLaughlin, S., 2012. National standards for
diabetes self-management education and support.
The Diabetes Educator,
38(5), pp.619-629.
Jiang, X., Zhang, D. and Jiang, W., 2014. Coffee and caffeine intake and incidence of type 1 diabetes mellitus: a meta-analysis of prospective studies.
European journal of
nutrition,
53(1), pp.25-38.
Kaufman, F. R. (Ed.). (2012).
Medical management of type 1 diabetes. American Diabetes Association.
McCrimmon, R.J., Ryan, C.M. and Frier, B.M., 2012. Diabetes and cognitive dysfunction.
The Lancet,
379(9833), pp.2291-2299.
Mixcoatl-Zecuatl, T. and Calcutt, N.A., 2013. Biology and pathophysiology of painful diabetic neuropathy. In
Painful Diabetic Polyneuropathy (pp. 13-26). Springer, New York,
NY.
Nedeltcheva, A.V. and Scheer, F.A., 2014. Metabolic effects of sleep disruption, links to obesity and diabetes.
Current opinion in endocrinology, diabetes, and obesity,
21(4),
p.293.
Ozougwu, J.C., Obimba, K.C., Belonwu, C.D. and Unakalamba, C.B., 2013. The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus.
Journal of
Physiology and Pathophysiology,
4(4), pp.46-57.
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Robling, M., McNamara, R., Bennert, K., Butler, C.C., Channon, S., Cohen, D., Crowne, E., Hambly, H., Hawthorne, K., Hood, K. and Longo, M., 2012. The effect
of the Talking Diabetes consulting skills intervention on glycaemic control and quality of life in children with type 1 diabetes: cluster randomised controlled
trial (DEPICTED study).
Bmj,
344, p.e2359.
Stellefson, M., Dipnarine, K. and Stopka, C., 2013. Peer reviewed: The chronic care model and diabetes management in US primary care settings: A systematic
review.
Preventing chronic disease,
10.
Zochodne, D.W., 2016. Sensory neurodegeneration in diabetes: beyond glucotoxicity. In
International review of neurobiology (Vol. 127, pp. 151-180). Academic Press.
7
of the Talking Diabetes consulting skills intervention on glycaemic control and quality of life in children with type 1 diabetes: cluster randomised controlled
trial (DEPICTED study).
Bmj,
344, p.e2359.
Stellefson, M., Dipnarine, K. and Stopka, C., 2013. Peer reviewed: The chronic care model and diabetes management in US primary care settings: A systematic
review.
Preventing chronic disease,
10.
Zochodne, D.W., 2016. Sensory neurodegeneration in diabetes: beyond glucotoxicity. In
International review of neurobiology (Vol. 127, pp. 151-180). Academic Press.
7
1 out of 7



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.