Cohort & Case-Control Studies: Detailed Research Article Analysis
VerifiedAdded on 2023/06/04
|8
|1975
|461
Homework Assignment
AI Summary
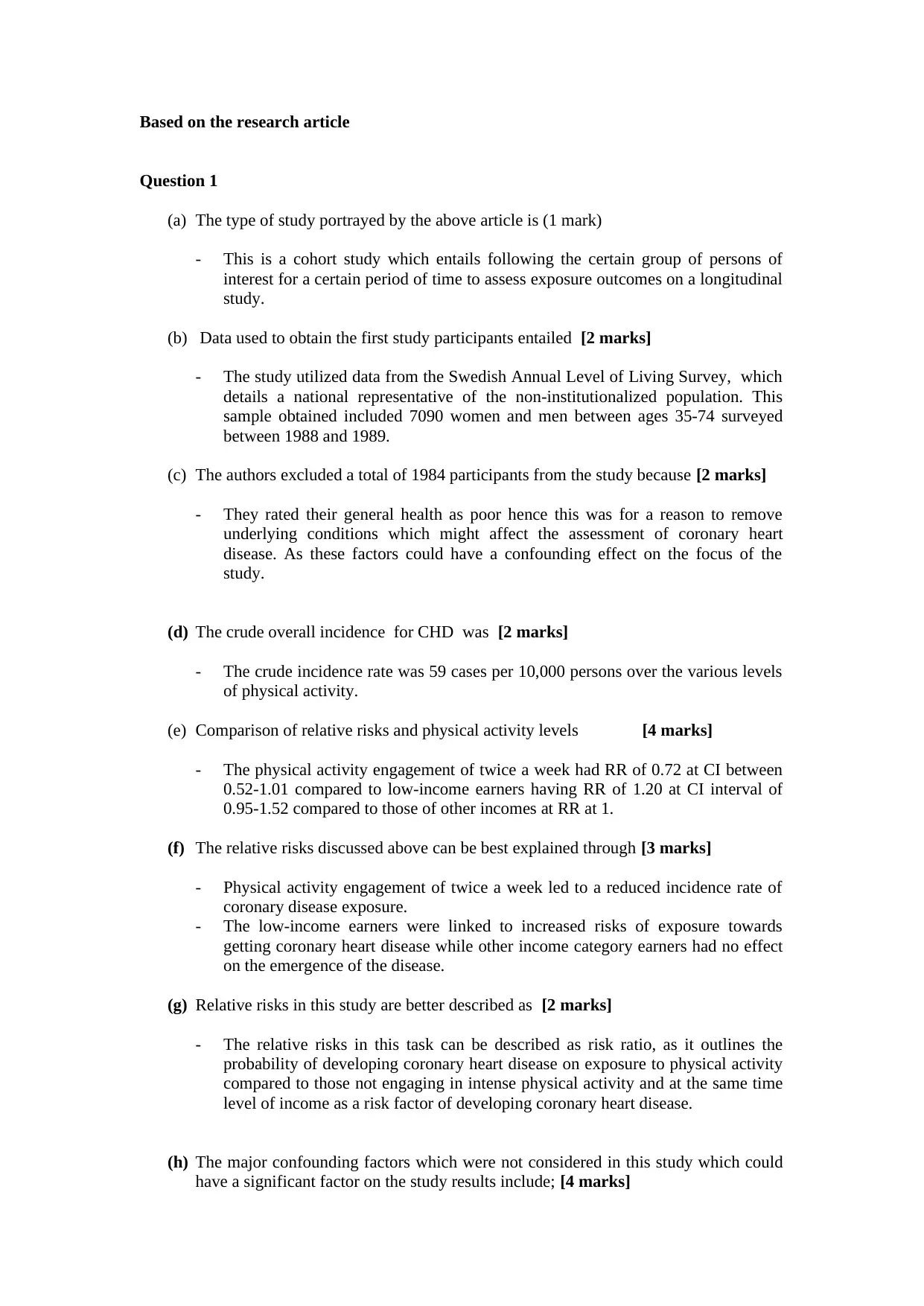
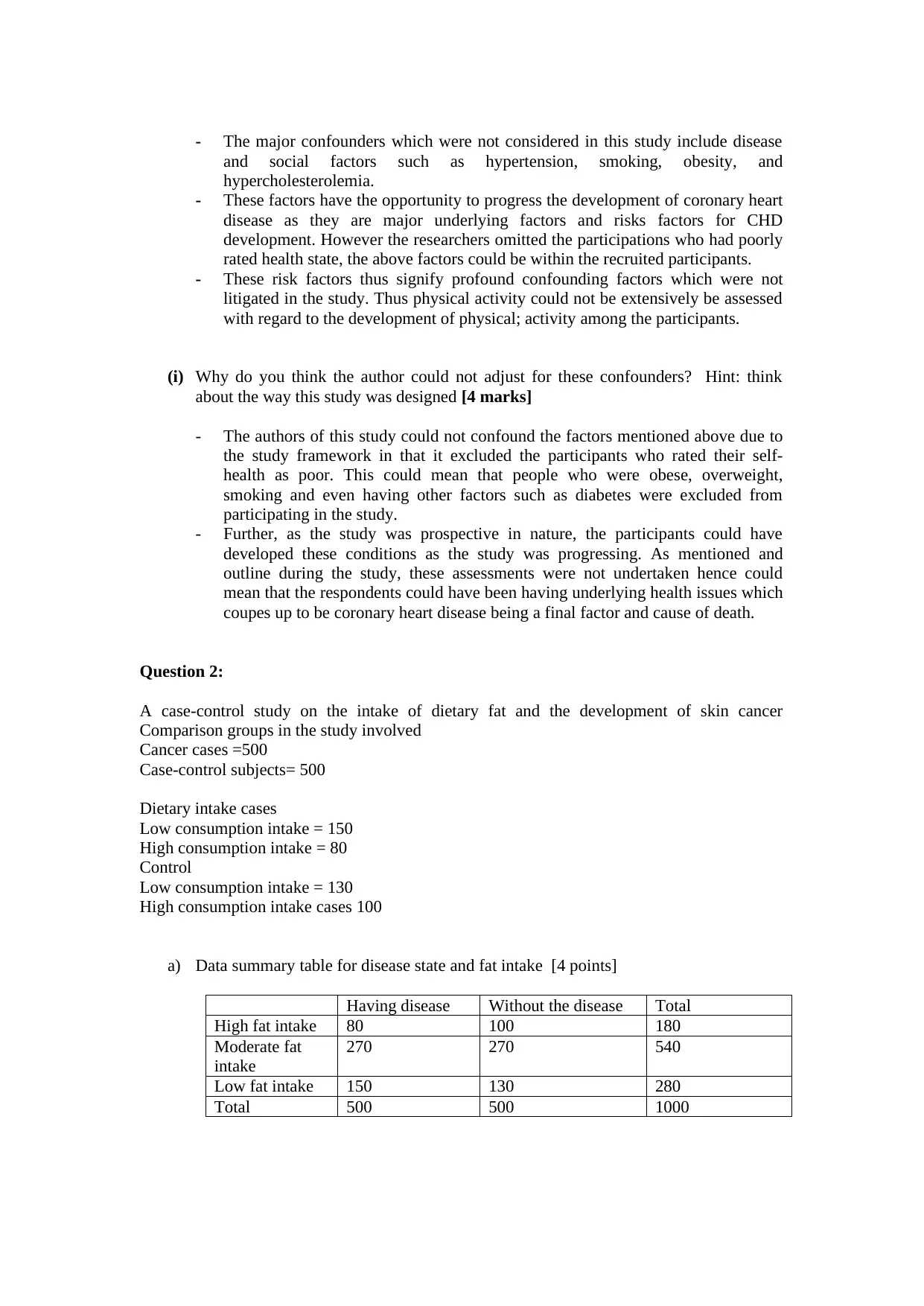
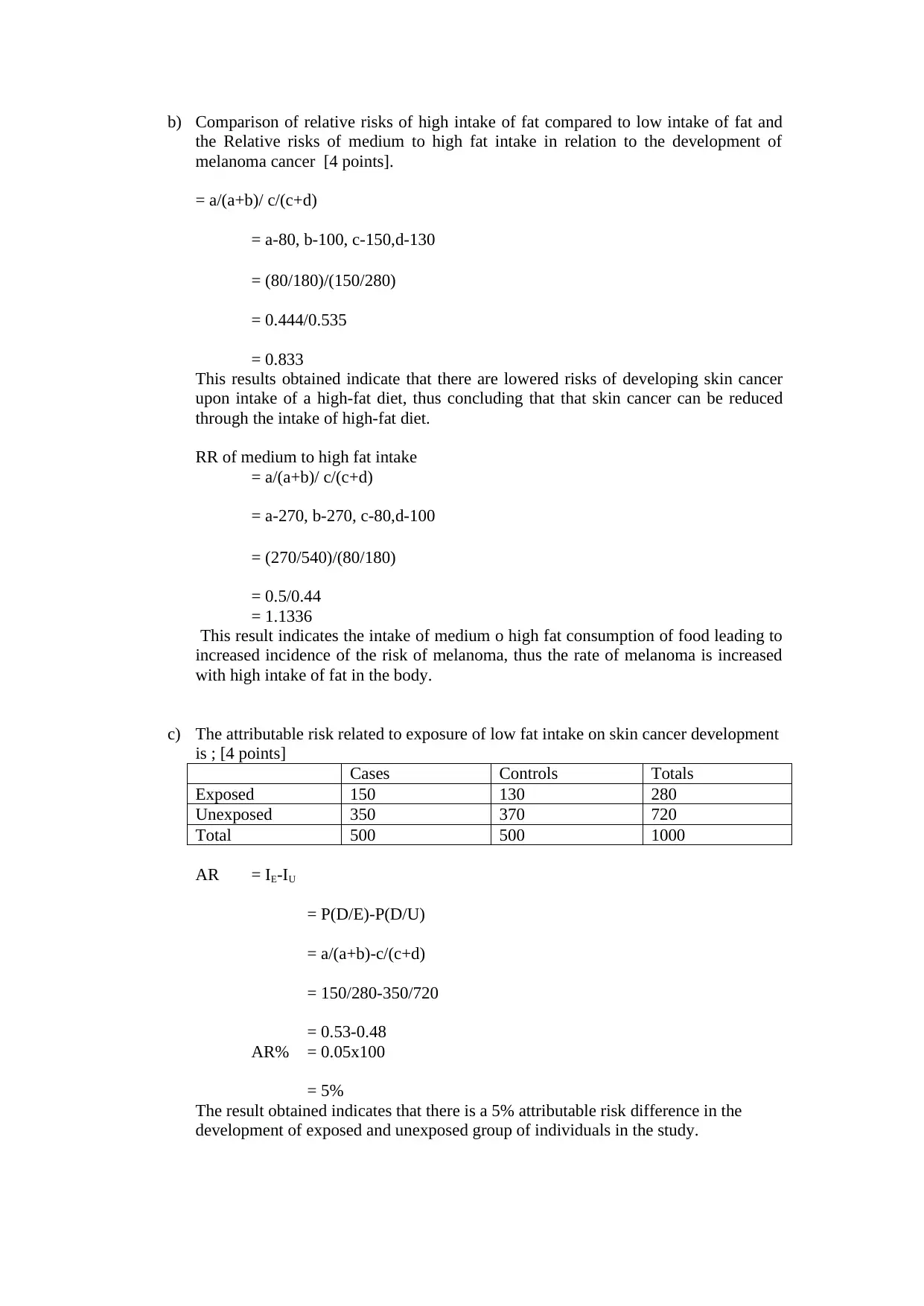
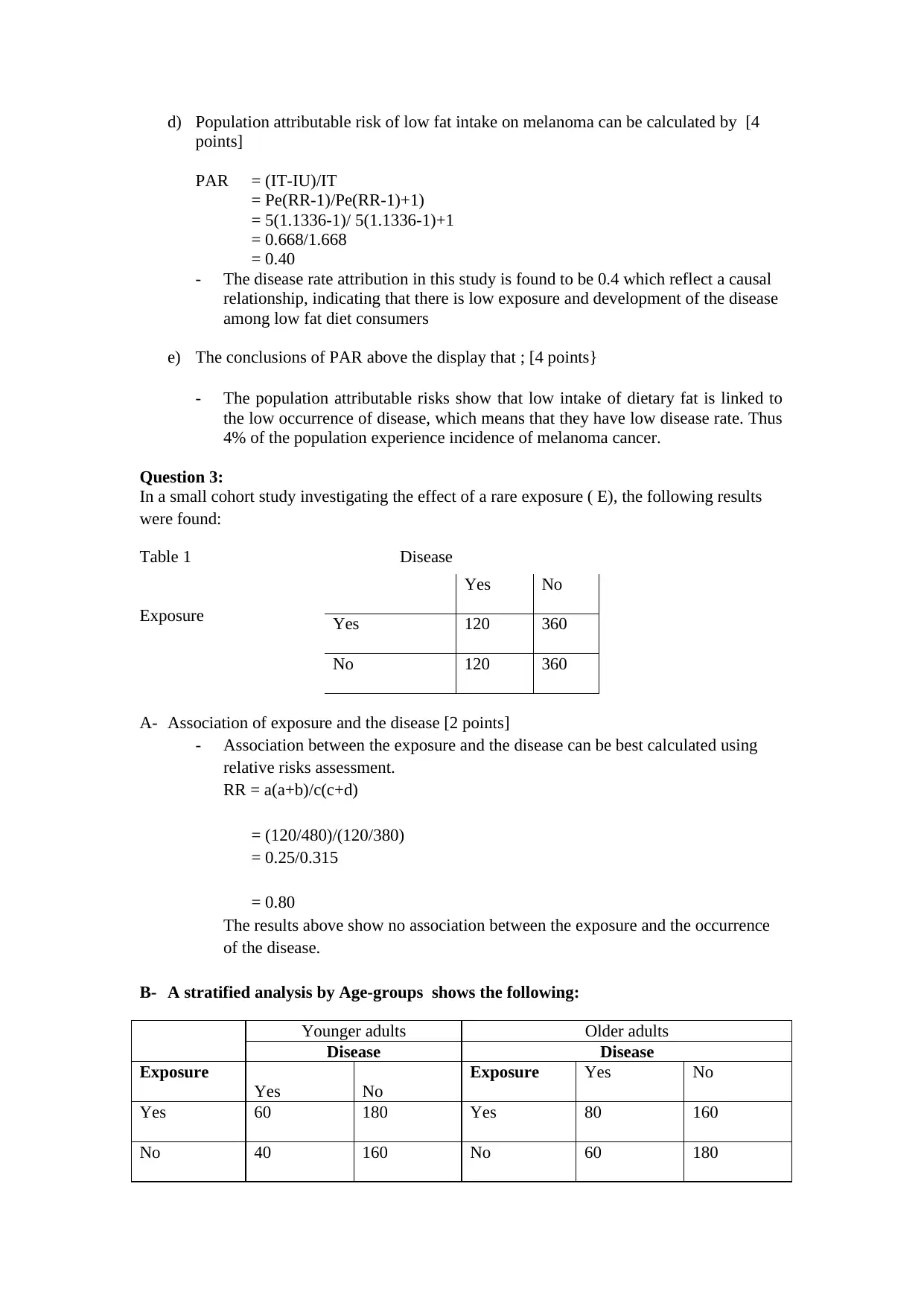
This assignment provides a detailed analysis of research articles focusing on cohort and case-control study designs. It addresses questions related to identifying the type of study, data usage, reasons for participant exclusion, crude incidence rates, comparison of relative risks and physical activity levels, and the explanation of relative risks. The analysis further delves into major confounding factors not considered in the study and the reasons for their omission. Additionally, the assignment includes a case-control study on dietary fat intake and skin cancer development, covering data summarization, comparison of relative risks, attributable risk calculation, population attributable risk, and interpretation of results. Finally, it examines a cohort study investigating the effect of rare exposure and discusses potential biases in both cohort and case-control studies, along with methods for addressing confounding factors and the effect of participant loss. Desklib offers a wealth of similar solved assignments and study resources for students.


1 out of 8
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.