3804NRS Assignment: Community Health Nursing Essay
VerifiedAdded on 2022/08/12
|9
|2068
|34
Essay
AI Summary
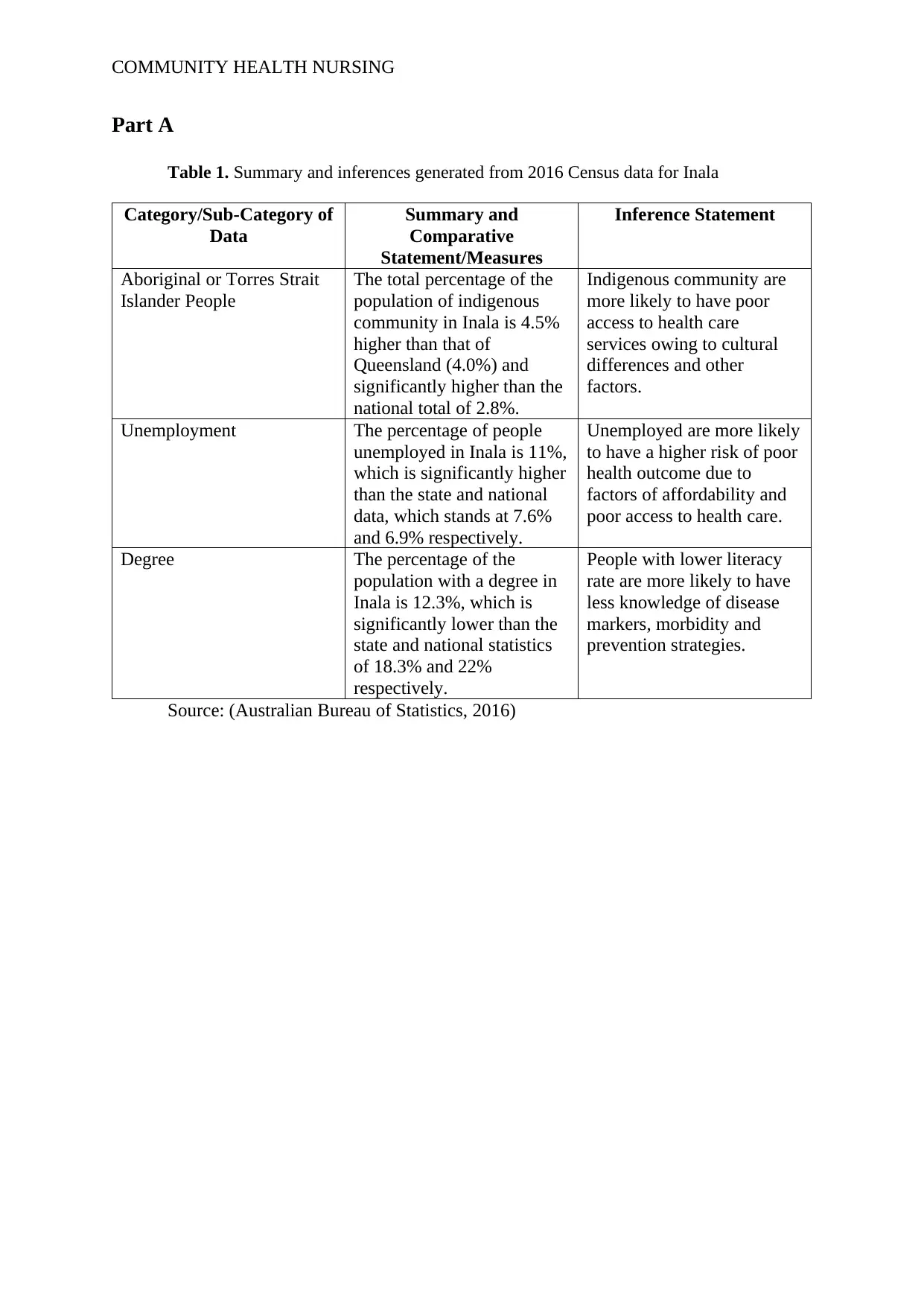
This essay, prepared for a community health nursing course, analyzes the Inala community in Brisbane, Queensland, using 2016 census data. The student identifies key social determinants of health, including indigenous status, unemployment, and lower education levels, and their impact on the community. The essay highlights the high prevalence of diabetes among the indigenous population as a critical health issue. It proposes a health promotion program based on the Medicare Benefits Scheme, focusing on health assessments, care planning, and increased access to healthcare services, including staff training and cultural awareness. The evaluation of the program is also discussed, with performance indicators such as reduced diabetes incidence and improved referral rates. The student concludes by emphasizing the importance of addressing these social determinants to improve health outcomes in the Inala community. The essay adheres to the assignment brief, providing a detailed community health nursing assessment and suggesting evidence-based interventions.


1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
© 2024 | Zucol Services PVT LTD | All rights reserved.