Complex Nursing Care 92442: Medical Surgical Case Study of Ben Casey
VerifiedAdded on 2023/06/13
|11
|2748
|189
Case Study
AI Summary
This assignment presents a comprehensive case study of Mr. Ben Casey, a 38-year-old male admitted to the Emergency Department following a motor vehicle accident (MVA). The case details Ben's background, assessment data including vital signs and injuries (oblique fracture of the left femur and an open displaced tibia), and the subsequent surgical interventions. The assignment identifies key nursing problems such as acute pain, impaired skin integrity, and risk for infection, and outlines appropriate nursing interventions including immobilization, pain management, wound care, and patient education. The goal is to ensure Ben remains infection-free, manages his pain effectively, and regains normal physiological function through collaborative and patient-centered care. The document also includes potential problems like risk of trauma and falls, diminished physical immobility, and risk for impaired neuromuscular function, with corresponding nursing interventions and monitoring strategies.

Running head: COMPLEX NURSING CARE.
Complex Nursing Care
Name of student
Institutional affiliation
Complex Nursing Care
Name of student
Institutional affiliation
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
COMPLEX NURSING CARE.
2
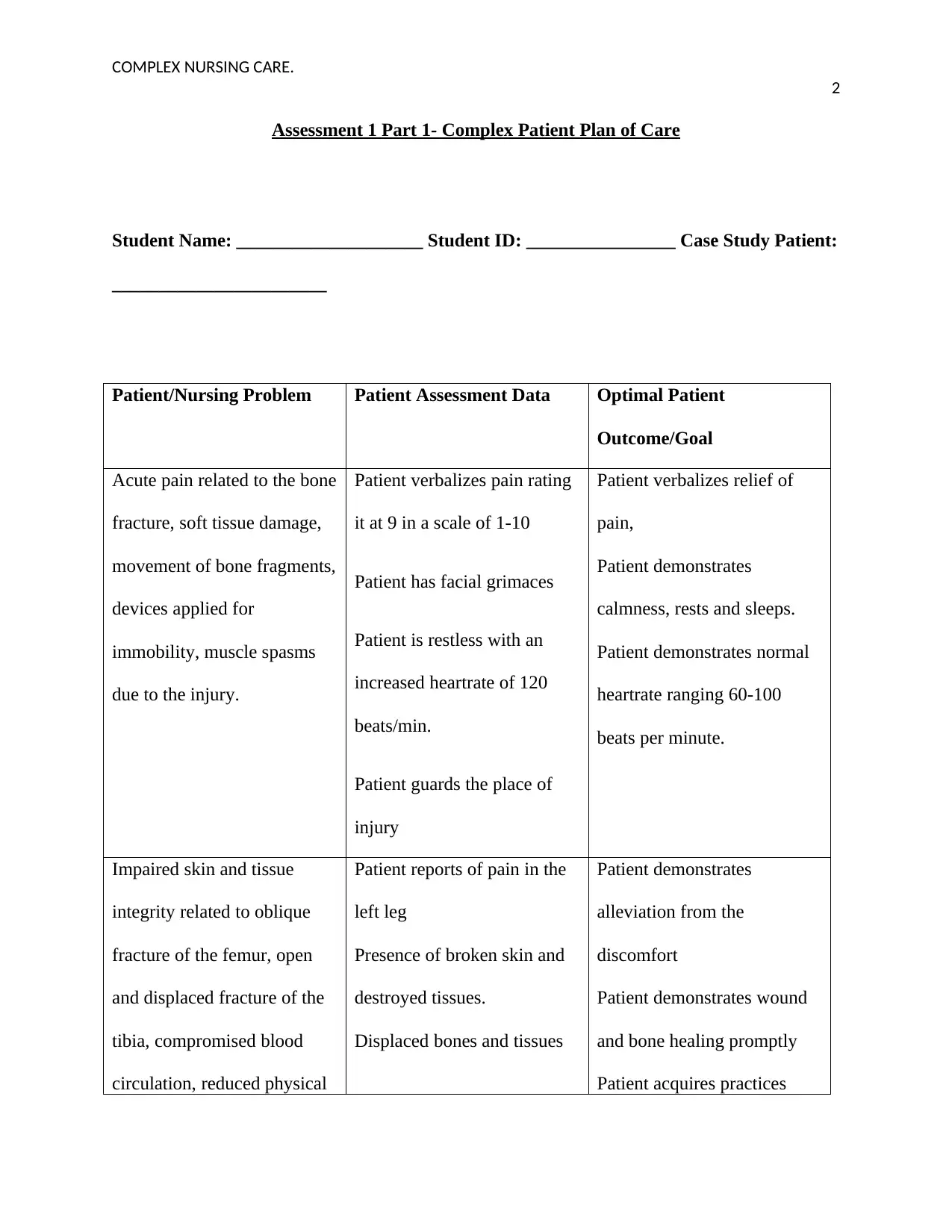
Assessment 1 Part 1- Complex Patient Plan of Care
Student Name: ____________________ Student ID: ________________ Case Study Patient:
_______________________
Patient/Nursing Problem Patient Assessment Data Optimal Patient
Outcome/Goal
Acute pain related to the bone
fracture, soft tissue damage,
movement of bone fragments,
devices applied for
immobility, muscle spasms
due to the injury.
Patient verbalizes pain rating
it at 9 in a scale of 1-10
Patient has facial grimaces
Patient is restless with an
increased heartrate of 120
beats/min.
Patient guards the place of
injury
Patient verbalizes relief of
pain,
Patient demonstrates
calmness, rests and sleeps.
Patient demonstrates normal
heartrate ranging 60-100
beats per minute.
Impaired skin and tissue
integrity related to oblique
fracture of the femur, open
and displaced fracture of the
tibia, compromised blood
circulation, reduced physical
Patient reports of pain in the
left leg
Presence of broken skin and
destroyed tissues.
Displaced bones and tissues
Patient demonstrates
alleviation from the
discomfort
Patient demonstrates wound
and bone healing promptly
Patient acquires practices
2
Assessment 1 Part 1- Complex Patient Plan of Care
Student Name: ____________________ Student ID: ________________ Case Study Patient:
_______________________
Patient/Nursing Problem Patient Assessment Data Optimal Patient
Outcome/Goal
Acute pain related to the bone
fracture, soft tissue damage,
movement of bone fragments,
devices applied for
immobility, muscle spasms
due to the injury.
Patient verbalizes pain rating
it at 9 in a scale of 1-10
Patient has facial grimaces
Patient is restless with an
increased heartrate of 120
beats/min.
Patient guards the place of
injury
Patient verbalizes relief of
pain,
Patient demonstrates
calmness, rests and sleeps.
Patient demonstrates normal
heartrate ranging 60-100
beats per minute.
Impaired skin and tissue
integrity related to oblique
fracture of the femur, open
and displaced fracture of the
tibia, compromised blood
circulation, reduced physical
Patient reports of pain in the
left leg
Presence of broken skin and
destroyed tissues.
Displaced bones and tissues
Patient demonstrates
alleviation from the
discomfort
Patient demonstrates wound
and bone healing promptly
Patient acquires practices
COMPLEX NURSING CARE.
3
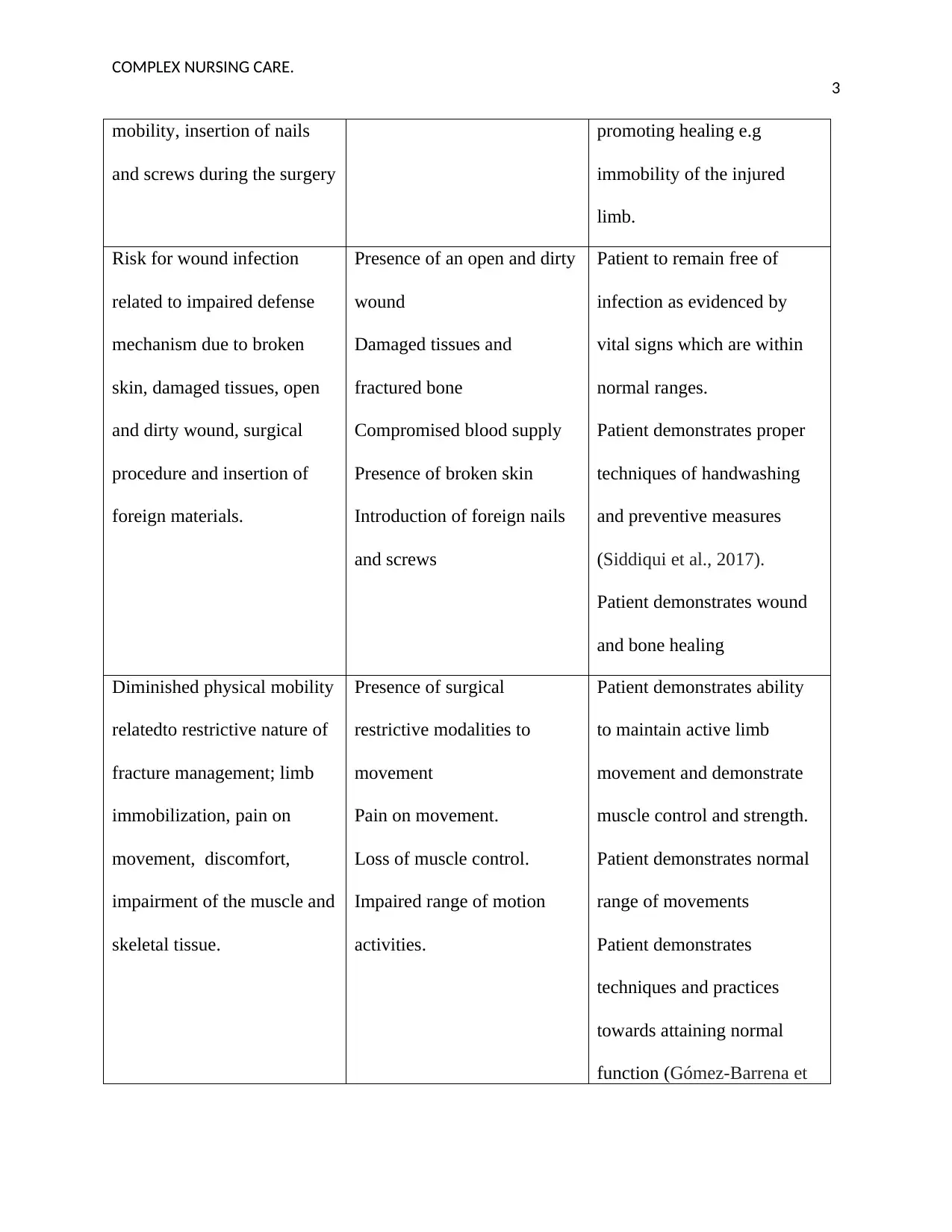
mobility, insertion of nails
and screws during the surgery
promoting healing e.g
immobility of the injured
limb.
Risk for wound infection
related to impaired defense
mechanism due to broken
skin, damaged tissues, open
and dirty wound, surgical
procedure and insertion of
foreign materials.
Presence of an open and dirty
wound
Damaged tissues and
fractured bone
Compromised blood supply
Presence of broken skin
Introduction of foreign nails
and screws
Patient to remain free of
infection as evidenced by
vital signs which are within
normal ranges.
Patient demonstrates proper
techniques of handwashing
and preventive measures
(Siddiqui et al., 2017).
Patient demonstrates wound
and bone healing
Diminished physical mobility
relatedto restrictive nature of
fracture management; limb
immobilization, pain on
movement, discomfort,
impairment of the muscle and
skeletal tissue.
Presence of surgical
restrictive modalities to
movement
Pain on movement.
Loss of muscle control.
Impaired range of motion
activities.
Patient demonstrates ability
to maintain active limb
movement and demonstrate
muscle control and strength.
Patient demonstrates normal
range of movements
Patient demonstrates
techniques and practices
towards attaining normal
function (Gómez-Barrena et
3
mobility, insertion of nails
and screws during the surgery
promoting healing e.g
immobility of the injured
limb.
Risk for wound infection
related to impaired defense
mechanism due to broken
skin, damaged tissues, open
and dirty wound, surgical
procedure and insertion of
foreign materials.
Presence of an open and dirty
wound
Damaged tissues and
fractured bone
Compromised blood supply
Presence of broken skin
Introduction of foreign nails
and screws
Patient to remain free of
infection as evidenced by
vital signs which are within
normal ranges.
Patient demonstrates proper
techniques of handwashing
and preventive measures
(Siddiqui et al., 2017).
Patient demonstrates wound
and bone healing
Diminished physical mobility
relatedto restrictive nature of
fracture management; limb
immobilization, pain on
movement, discomfort,
impairment of the muscle and
skeletal tissue.
Presence of surgical
restrictive modalities to
movement
Pain on movement.
Loss of muscle control.
Impaired range of motion
activities.
Patient demonstrates ability
to maintain active limb
movement and demonstrate
muscle control and strength.
Patient demonstrates normal
range of movements
Patient demonstrates
techniques and practices
towards attaining normal
function (Gómez-Barrena et
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
COMPLEX NURSING CARE.
4
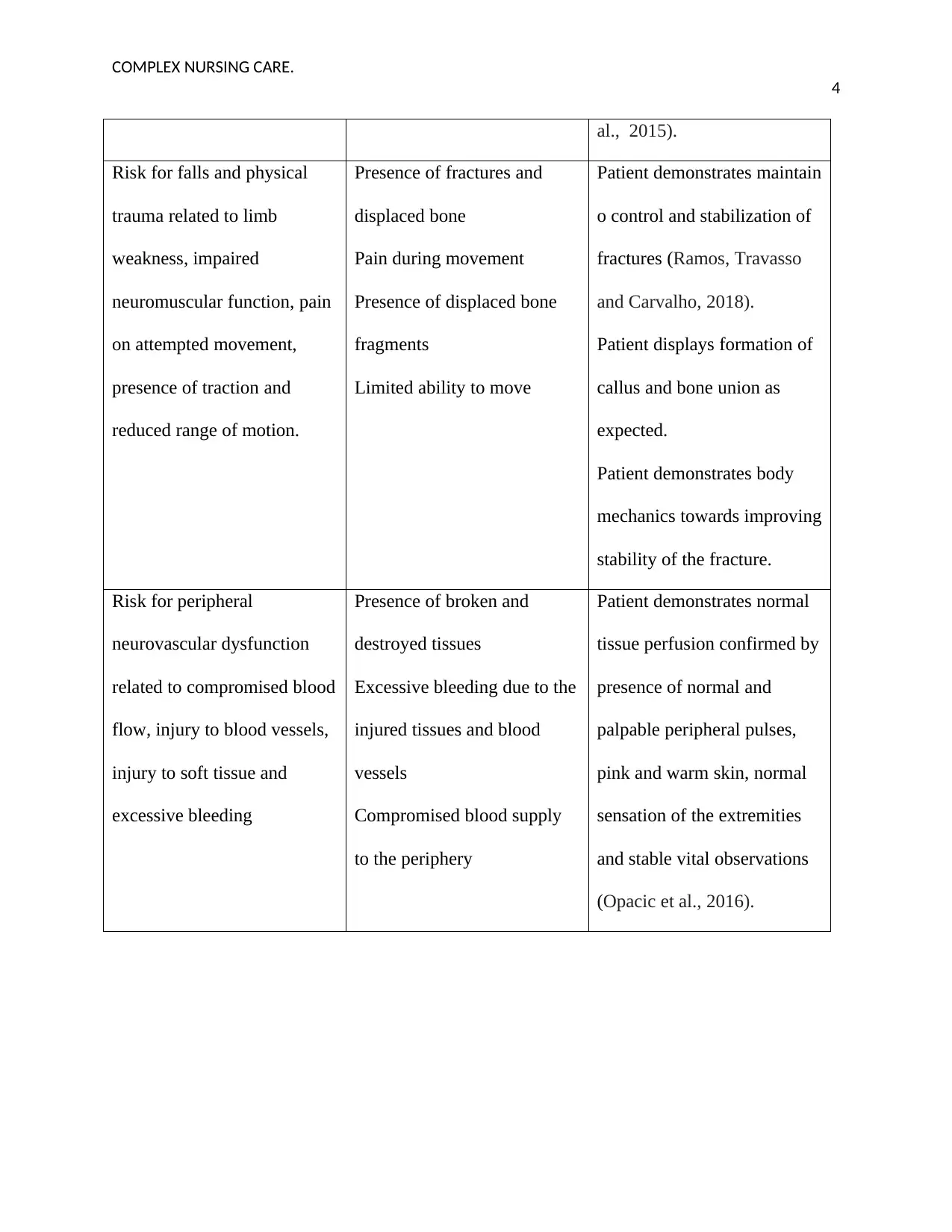
al., 2015).
Risk for falls and physical
trauma related to limb
weakness, impaired
neuromuscular function, pain
on attempted movement,
presence of traction and
reduced range of motion.
Presence of fractures and
displaced bone
Pain during movement
Presence of displaced bone
fragments
Limited ability to move
Patient demonstrates maintain
o control and stabilization of
fractures (Ramos, Travasso
and Carvalho, 2018).
Patient displays formation of
callus and bone union as
expected.
Patient demonstrates body
mechanics towards improving
stability of the fracture.
Risk for peripheral
neurovascular dysfunction
related to compromised blood
flow, injury to blood vessels,
injury to soft tissue and
excessive bleeding
Presence of broken and
destroyed tissues
Excessive bleeding due to the
injured tissues and blood
vessels
Compromised blood supply
to the periphery
Patient demonstrates normal
tissue perfusion confirmed by
presence of normal and
palpable peripheral pulses,
pink and warm skin, normal
sensation of the extremities
and stable vital observations
(Opacic et al., 2016).
4
al., 2015).
Risk for falls and physical
trauma related to limb
weakness, impaired
neuromuscular function, pain
on attempted movement,
presence of traction and
reduced range of motion.
Presence of fractures and
displaced bone
Pain during movement
Presence of displaced bone
fragments
Limited ability to move
Patient demonstrates maintain
o control and stabilization of
fractures (Ramos, Travasso
and Carvalho, 2018).
Patient displays formation of
callus and bone union as
expected.
Patient demonstrates body
mechanics towards improving
stability of the fracture.
Risk for peripheral
neurovascular dysfunction
related to compromised blood
flow, injury to blood vessels,
injury to soft tissue and
excessive bleeding
Presence of broken and
destroyed tissues
Excessive bleeding due to the
injured tissues and blood
vessels
Compromised blood supply
to the periphery
Patient demonstrates normal
tissue perfusion confirmed by
presence of normal and
palpable peripheral pulses,
pink and warm skin, normal
sensation of the extremities
and stable vital observations
(Opacic et al., 2016).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
COMPLEX NURSING CARE.
5
ASSESSMENT 1 PART 2 – INDIVIDUAL WRITTEN REPORT
Ben’s Background Information
Mr.Ben Casey, with 38 years and male, was rushed into the UTS Emergency Department today
morning by an ambulance reporting injuries as a result of MVA. Bens major complaint was pain
and his admission vital observation were as follows; heart rate of 120 beats/min, BP of 130/78,
respiration rate of 24 breaths/min, and an oxygen saturation of 96% on room air. The X-raysat
the ED presented an oblique fracture of the left femur and an open displaced tibia affecting flow
of blood to the limbthe wound had a lot of dirt and gravel from the accident scene. He has a
fractured rib and a small hemo-pneumothorax. Estimated blood loss at the scene was 750-
1000mls. An ICC was inserted. He was immediately scheduled for an urgent surgery for
reduction and internal fixation of the femur and the tibia. The procedure lasted for three hours
and was noneventful with a blood loss of 750mls. Ben has been given 25mg of morphine and
reports pain to be at 4/10. He has a drain in the right thigh that is active. Has a dressing on the
thigh and shin that are intact with a small ooze. The pedal pulses are strong and palpaple. He is
on oxygen via nasal cannula at 2L. He is resting and rates pain at 6/10. He is alert with a GCS of
15/15.
Assessment Data
Assessment of the patient was performed by the A-G approach. Subjective data was patient
verbalization of pain of level 6/10 on his left leg. The objective data was the patient appeared
disturbed, anxious and presence of facial grimaces and guarding of the left thigh. The vital
observations were: pulse-120beats/min, respirations of 24 breaths/minute, BP of 130/78, and an
oxygen saturation of 96% on room air. The patient reported injuries on his left limb which was a
5
ASSESSMENT 1 PART 2 – INDIVIDUAL WRITTEN REPORT
Ben’s Background Information
Mr.Ben Casey, with 38 years and male, was rushed into the UTS Emergency Department today
morning by an ambulance reporting injuries as a result of MVA. Bens major complaint was pain
and his admission vital observation were as follows; heart rate of 120 beats/min, BP of 130/78,
respiration rate of 24 breaths/min, and an oxygen saturation of 96% on room air. The X-raysat
the ED presented an oblique fracture of the left femur and an open displaced tibia affecting flow
of blood to the limbthe wound had a lot of dirt and gravel from the accident scene. He has a
fractured rib and a small hemo-pneumothorax. Estimated blood loss at the scene was 750-
1000mls. An ICC was inserted. He was immediately scheduled for an urgent surgery for
reduction and internal fixation of the femur and the tibia. The procedure lasted for three hours
and was noneventful with a blood loss of 750mls. Ben has been given 25mg of morphine and
reports pain to be at 4/10. He has a drain in the right thigh that is active. Has a dressing on the
thigh and shin that are intact with a small ooze. The pedal pulses are strong and palpaple. He is
on oxygen via nasal cannula at 2L. He is resting and rates pain at 6/10. He is alert with a GCS of
15/15.
Assessment Data
Assessment of the patient was performed by the A-G approach. Subjective data was patient
verbalization of pain of level 6/10 on his left leg. The objective data was the patient appeared
disturbed, anxious and presence of facial grimaces and guarding of the left thigh. The vital
observations were: pulse-120beats/min, respirations of 24 breaths/minute, BP of 130/78, and an
oxygen saturation of 96% on room air. The patient reported injuries on his left limb which was a
COMPLEX NURSING CARE.
6
possible risk of infection. The objective data was that the patient had an open wound on the left
shin of the tibial bone and the wound was filled with gravel together with sand from the scene
where he incurred the accident, there was compromised blood flow and the sugical procedure
increased the risk for infection.
Actual problem is; acute pain related to the bone fracture, soft tissue damage, movement of
bone fragments, devices applied for immobility, muscle spasms due to the injury.
Pain is what the patient says it is. It is subjective, and it’s an emotional, physical and sensory
feeling of ailment of injury to the bone and tissues. The cluster of cues for the finding was
Patient verbalizing the unpleasant feeling rating it at 9 in a scale of 1 to 10, Patient has facial
grimaces demonstrating perception of pain, Patient is restless and anxious with an increased
heart rate of 120 beats/min and Patient guards the place of injury (Kua et al., 2016).The data was
both subjective and objective in nature. The assessment data was arrived at by collaboration and
teamwork from a team of nurses and other physicians. The expected outcome was that patient
verbalizes relief of pain and demonstrates calmness, rests and sleeps. Patient will demonstrate
normal heart rate ranging 60-100 beats per minute (Chaudhuri et al., 2015).
Nursing interventions
Injured limbs were immobilized using a cast, skeletal tractions and patient was advised to rest so
as to alleviate pain and ensure stability of the fracture for alignment hence promoting fast and
prompt healing. The broken areas were carefully raised to facilitate return of blood to the heart
hence reduce accumulation of fluid at the extremity and ensure the integrity of the nerves and
foot in general. Frequent assessment and recording of pin was done in reference to the pain scale
(Lavin, Harper and Barr, 2015). Documentation ensures ease and prompt monitoring as it
6
possible risk of infection. The objective data was that the patient had an open wound on the left
shin of the tibial bone and the wound was filled with gravel together with sand from the scene
where he incurred the accident, there was compromised blood flow and the sugical procedure
increased the risk for infection.
Actual problem is; acute pain related to the bone fracture, soft tissue damage, movement of
bone fragments, devices applied for immobility, muscle spasms due to the injury.
Pain is what the patient says it is. It is subjective, and it’s an emotional, physical and sensory
feeling of ailment of injury to the bone and tissues. The cluster of cues for the finding was
Patient verbalizing the unpleasant feeling rating it at 9 in a scale of 1 to 10, Patient has facial
grimaces demonstrating perception of pain, Patient is restless and anxious with an increased
heart rate of 120 beats/min and Patient guards the place of injury (Kua et al., 2016).The data was
both subjective and objective in nature. The assessment data was arrived at by collaboration and
teamwork from a team of nurses and other physicians. The expected outcome was that patient
verbalizes relief of pain and demonstrates calmness, rests and sleeps. Patient will demonstrate
normal heart rate ranging 60-100 beats per minute (Chaudhuri et al., 2015).
Nursing interventions
Injured limbs were immobilized using a cast, skeletal tractions and patient was advised to rest so
as to alleviate pain and ensure stability of the fracture for alignment hence promoting fast and
prompt healing. The broken areas were carefully raised to facilitate return of blood to the heart
hence reduce accumulation of fluid at the extremity and ensure the integrity of the nerves and
foot in general. Frequent assessment and recording of pin was done in reference to the pain scale
(Lavin, Harper and Barr, 2015). Documentation ensures ease and prompt monitoring as it
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
COMPLEX NURSING CARE.
7
provides the shift in presentations. Objective data for pain; patient mood, facial grimace and vital
observations majorly the heart rate were observed. This was to perform the evaluation aspect of
all the interventions applied by the health care workers. Direct actions were applied to ensure
gaining of physiological function and ensure client centered care.
Health education
Nurses established trust by reassuring him of client confidentiality. They educated ben on
reporting any signs of changes to the wound, such as increased pain or feeling of itchiness.
(Banaszkiewicz, 2014). Before performing any procedure, the process was explained and its
importance to alley anxiety and prepare him. Consent as also obtained before each procedure.
They explained on how he should participate positively towards quality care promoting
collaborative care (Gordon, 2014).
Patient monitoring
Close monitoring was done to check the fluctuation of pain with the analgesics. Monitoring was
by assessing the wound and taking vital signs against the normal ranges. Patient was given
emotional care by being educated on use of ways of managing anxiety such as gaseous exchange
exercises and was reassured on the prognosis of his condition. Pain was assessed often in
reference to the scale of 1-10 to ensure relief from pain and comfort (Lamego et al., 2017). Left
limb was assessed for presence of sensation to monitor the function of the nerve and limb. The
doctor was consulted to reassess him for severity of pain and give a medical prescription to the
patient. Patient was encouraged and supervised on exercises on active and passive Range of
motion to promote strength and activity of the joint and muscle to promote relief of swelling and
in damaged soft tissues to ensure normal physiology.
7
provides the shift in presentations. Objective data for pain; patient mood, facial grimace and vital
observations majorly the heart rate were observed. This was to perform the evaluation aspect of
all the interventions applied by the health care workers. Direct actions were applied to ensure
gaining of physiological function and ensure client centered care.
Health education
Nurses established trust by reassuring him of client confidentiality. They educated ben on
reporting any signs of changes to the wound, such as increased pain or feeling of itchiness.
(Banaszkiewicz, 2014). Before performing any procedure, the process was explained and its
importance to alley anxiety and prepare him. Consent as also obtained before each procedure.
They explained on how he should participate positively towards quality care promoting
collaborative care (Gordon, 2014).
Patient monitoring
Close monitoring was done to check the fluctuation of pain with the analgesics. Monitoring was
by assessing the wound and taking vital signs against the normal ranges. Patient was given
emotional care by being educated on use of ways of managing anxiety such as gaseous exchange
exercises and was reassured on the prognosis of his condition. Pain was assessed often in
reference to the scale of 1-10 to ensure relief from pain and comfort (Lamego et al., 2017). Left
limb was assessed for presence of sensation to monitor the function of the nerve and limb. The
doctor was consulted to reassess him for severity of pain and give a medical prescription to the
patient. Patient was encouraged and supervised on exercises on active and passive Range of
motion to promote strength and activity of the joint and muscle to promote relief of swelling and
in damaged soft tissues to ensure normal physiology.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
COMPLEX NURSING CARE.
8
Patient was assessed for pain using a scale of 0-10 to assess comfort and healing. To check the
prognosis of the interventions of the nurse and other clinicians implemented, repeat assessment
was done. Patient confirmed relief of unpleasant feeling and demonstrated calmness and rest.
Ben was at ease of resting and sleeping without the unpleasant feeling. The patient outcomes
were concluded based on the patient’s report of decreased perception of pain and the face
appeared brighter.
Potential Problem: Risk of Infection related to impaired defense mechanism due to broken
skin, damaged tissues, open and dirty wound, surgical procedure and insertion of foreign
materials.
Ben has a risk for infection due to impaired defense mechanism in relation to presence of broken
skin, destroyed tissues that have weakened the body’s immunity, he suffered an open wound that
is dirty and full of gravel from the scene (Mohania et al., 2017). The dirt is a source of infection
from the environment. Ben underwent a surgical procedure, reduction and internal reduction. In
the surgery, he was fixed with interlocking nails and screws which are foreign objects and make
him susceptible to infection. The procedure itself places him at a risk for infection.
The main objective in this case is to ensure Ben remains infection free and the wound heals well
and he regains normal physiological function. The interventions also centered at educating Ben
on the proper ways of keeping his wound clean and out of reach of microorganisms. He was also
warned about contacting the wound. Aseptic technique use awareness was created on change of
dressings and cubital intravenous line care. This breaks microorganism’s chain of transmission
and renders Ben infection free through the period of hospital stay.
8
Patient was assessed for pain using a scale of 0-10 to assess comfort and healing. To check the
prognosis of the interventions of the nurse and other clinicians implemented, repeat assessment
was done. Patient confirmed relief of unpleasant feeling and demonstrated calmness and rest.
Ben was at ease of resting and sleeping without the unpleasant feeling. The patient outcomes
were concluded based on the patient’s report of decreased perception of pain and the face
appeared brighter.
Potential Problem: Risk of Infection related to impaired defense mechanism due to broken
skin, damaged tissues, open and dirty wound, surgical procedure and insertion of foreign
materials.
Ben has a risk for infection due to impaired defense mechanism in relation to presence of broken
skin, destroyed tissues that have weakened the body’s immunity, he suffered an open wound that
is dirty and full of gravel from the scene (Mohania et al., 2017). The dirt is a source of infection
from the environment. Ben underwent a surgical procedure, reduction and internal reduction. In
the surgery, he was fixed with interlocking nails and screws which are foreign objects and make
him susceptible to infection. The procedure itself places him at a risk for infection.
The main objective in this case is to ensure Ben remains infection free and the wound heals well
and he regains normal physiological function. The interventions also centered at educating Ben
on the proper ways of keeping his wound clean and out of reach of microorganisms. He was also
warned about contacting the wound. Aseptic technique use awareness was created on change of
dressings and cubital intravenous line care. This breaks microorganism’s chain of transmission
and renders Ben infection free through the period of hospital stay.
COMPLEX NURSING CARE.
9
The interventions included assessing the wound for presence of increased pain and edema. Use
of aseptic technique during dressing and cleaning of the wound (Kamoun, Kenawy, and Chen,
2017). The wound should be assessed for changes in color and any smell. This will identify early
signs of infection that will call for prompt management. Vital observations should be observed
for fluctuation, especially temperature monitoring to pick out infection.
Health Education
All clinicians were enlightened on the advantages of proper hand washing before any procedure
to Ben (Siddiqui et al., 2017). Use of clean running water and rubbing hands eliminated some of
the pathogens from one patient to another. Clinicians maintained the hand washing protocol.
Mr. Ben, his family and friends were educated on the importance of hand washing before
entering the ward and after visiting the patient.
Conclusion
Ben’s case was handled with professional care and collaboratively from the clinicians. Careful
assessment was done to arrive at priority nursing diagnoses; acute pain, impaired skin integrity,
risk for infection, risk for trauma and falls, diminished physical immobility and risk for impaired
neuromuscular function. Appropriate nursing interventions were implemented towards
management. Patient education was given appropriately and the patient participated positively
towards management.
9
The interventions included assessing the wound for presence of increased pain and edema. Use
of aseptic technique during dressing and cleaning of the wound (Kamoun, Kenawy, and Chen,
2017). The wound should be assessed for changes in color and any smell. This will identify early
signs of infection that will call for prompt management. Vital observations should be observed
for fluctuation, especially temperature monitoring to pick out infection.
Health Education
All clinicians were enlightened on the advantages of proper hand washing before any procedure
to Ben (Siddiqui et al., 2017). Use of clean running water and rubbing hands eliminated some of
the pathogens from one patient to another. Clinicians maintained the hand washing protocol.
Mr. Ben, his family and friends were educated on the importance of hand washing before
entering the ward and after visiting the patient.
Conclusion
Ben’s case was handled with professional care and collaboratively from the clinicians. Careful
assessment was done to arrive at priority nursing diagnoses; acute pain, impaired skin integrity,
risk for infection, risk for trauma and falls, diminished physical immobility and risk for impaired
neuromuscular function. Appropriate nursing interventions were implemented towards
management. Patient education was given appropriately and the patient participated positively
towards management.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
COMPLEX NURSING CARE.
10
References
Banaszkiewicz, P. (2014). Traumatic arthritis of the hip after dislocation and acetabular fractures:
treatment by mold arthroplasty: an end-result study using a new method of result evaluation. In
Classic Papers in Orthopaedics, pp. 13-17.
Chaudhuri, K., Rizos, A., Trenkwalder, C., Rascul, O., Pal, S., Martino, D., Carroll, C., Paviour, D.,
Falup-pecurariu, C., Kessel, B. and Silverdale, M. (2015). King's Parkinson's disease pain scale,
the first scale for pain in PD: an international validation. Movement disorders, 3 (12), pp.1623-
1631.
Gomez-barrena, E., Rosset, P., Lozano, D., Stanovici, J., Ermthallar, C. and Gerbhard, F. (2015). Bone
fracture healing: cell therapy in delayed unions and nonunions. Bone, 70, pp.93-101.
Gordon, M., 2014. Manual of nursing diagnosis. Jones & Bartlett Publishers.
Kamuun, E., Kenawy, E. and Chen, X. (2017). . A review on polymeric hydrogel membranes for wound
dressing applications: PVA-based hydrogel dressings. Journal of advanced research, 8(3),
pp.217-233.
Kua, J., Ramason, R., Rajamoney, G. and Chung, M. (2016). Which frailty measure is a good predictor
of early post-operative complications in elderly hip fracture patients? Archives of orthopaedic
and trauma surgery,, 136(5), pp.639-647.
Lamego, M., Kiani, M., Lam, K., Dalvi, C., Vo, H. and Masimo, C. (2017). . Patient monitoring
system., 9, pp.532-722.
10
References
Banaszkiewicz, P. (2014). Traumatic arthritis of the hip after dislocation and acetabular fractures:
treatment by mold arthroplasty: an end-result study using a new method of result evaluation. In
Classic Papers in Orthopaedics, pp. 13-17.
Chaudhuri, K., Rizos, A., Trenkwalder, C., Rascul, O., Pal, S., Martino, D., Carroll, C., Paviour, D.,
Falup-pecurariu, C., Kessel, B. and Silverdale, M. (2015). King's Parkinson's disease pain scale,
the first scale for pain in PD: an international validation. Movement disorders, 3 (12), pp.1623-
1631.
Gomez-barrena, E., Rosset, P., Lozano, D., Stanovici, J., Ermthallar, C. and Gerbhard, F. (2015). Bone
fracture healing: cell therapy in delayed unions and nonunions. Bone, 70, pp.93-101.
Gordon, M., 2014. Manual of nursing diagnosis. Jones & Bartlett Publishers.
Kamuun, E., Kenawy, E. and Chen, X. (2017). . A review on polymeric hydrogel membranes for wound
dressing applications: PVA-based hydrogel dressings. Journal of advanced research, 8(3),
pp.217-233.
Kua, J., Ramason, R., Rajamoney, G. and Chung, M. (2016). Which frailty measure is a good predictor
of early post-operative complications in elderly hip fracture patients? Archives of orthopaedic
and trauma surgery,, 136(5), pp.639-647.
Lamego, M., Kiani, M., Lam, K., Dalvi, C., Vo, H. and Masimo, C. (2017). . Patient monitoring
system., 9, pp.532-722.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
COMPLEX NURSING CARE.
11
Lavin, M., Harper, E. and Barr, N. (2015). . Health information technology, patient safety, and
professional nursing care documentation in acute care settings. Online J Issues Nurs, 20(6).
Mohania, D., Chandel, S., Kumar, P., Verma, V., Digvijay, K., Tripathi, D., Choudhury, K., Mitten, S.
and Shah, D. (2017). Ultraviolet radiations: Skin defense-damage mechanism. In Ultraviolet
Light in Human Health, Diseases and Environment, pp.71-87.
Opacic, D., Bragt, K., Nasrallah, H., Schottenq, U. and Verheule, S. (2016). . Atrial metabolism and
tissue perfusion as determinants of electrical and structural remodelling in atrial fibrillation.
Cardiovascular research, 109(4), pp.527-541.
Ramos, J., Travasso, R. and Carvalho, J. (2018). . Capillary network formation from dispersed
endothelial cells: Influence of cell traction, cell adhesion, and extracellular matrix rigidity.
Physical Review, 97(1), p.012408.
Siddiqui, N., Friedman, Z., Macgeer, A., Yousefzadeh, A., Carvalho, J. and Davies, S. (2017). Optimal
hand washing technique to minimize bacterial contamination before neuraxial anesthesia: a
randomized control trial. International journal of obstetric anesthesia, 29, pp.39-44.
.
.
11
Lavin, M., Harper, E. and Barr, N. (2015). . Health information technology, patient safety, and
professional nursing care documentation in acute care settings. Online J Issues Nurs, 20(6).
Mohania, D., Chandel, S., Kumar, P., Verma, V., Digvijay, K., Tripathi, D., Choudhury, K., Mitten, S.
and Shah, D. (2017). Ultraviolet radiations: Skin defense-damage mechanism. In Ultraviolet
Light in Human Health, Diseases and Environment, pp.71-87.
Opacic, D., Bragt, K., Nasrallah, H., Schottenq, U. and Verheule, S. (2016). . Atrial metabolism and
tissue perfusion as determinants of electrical and structural remodelling in atrial fibrillation.
Cardiovascular research, 109(4), pp.527-541.
Ramos, J., Travasso, R. and Carvalho, J. (2018). . Capillary network formation from dispersed
endothelial cells: Influence of cell traction, cell adhesion, and extracellular matrix rigidity.
Physical Review, 97(1), p.012408.
Siddiqui, N., Friedman, Z., Macgeer, A., Yousefzadeh, A., Carvalho, J. and Davies, S. (2017). Optimal
hand washing technique to minimize bacterial contamination before neuraxial anesthesia: a
randomized control trial. International journal of obstetric anesthesia, 29, pp.39-44.
.
.
1 out of 11
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.