University Complex Nursing Care: Medical Surgical Report Analysis
VerifiedAdded on 2023/01/20
|12
|2940
|63
Report
AI Summary
This report presents a comprehensive analysis of a complex nursing care scenario involving a 54-year-old male, Christopher Collins, who underwent a left high tibia knee osteotomy and presented with post-operative complications. The report details the patient's medical history, including osteoarthritis and asthma, and outlines the assessment findings, including vital signs, lab results, and subjective complaints. The report identifies key nursing problems such as wound infection and impaired gas exchange, providing a thorough discussion of the pathophysiology, assessment, and interventions for each problem. The nursing interventions include pharmacological and non-pharmacological approaches, with a focus on achieving optimal patient outcomes. The plan of care is based on the nursing process, including patient assessment data, problem identification, and optimal patient outcomes or goals. The interventions include both independent and collaborative approaches, with a strong emphasis on patient safety and effective communication. The report also addresses the patient's risk of venous thrombosis and restricted physical mobility. The report incorporates relevant research and evidence-based practice to support the nursing interventions and patient outcomes. The report also includes a plan of care as an appendix.

1COMPLEX NURSING CARE: MEDICAL SURGICAL
COMPLEX NURSING CARE: MEDICAL SURGICAL
Name of the Student
University Name
Author’s note
COMPLEX NURSING CARE: MEDICAL SURGICAL
Name of the Student
University Name
Author’s note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1COMPLEX NURSING CARE: MEDICAL SURGICAL
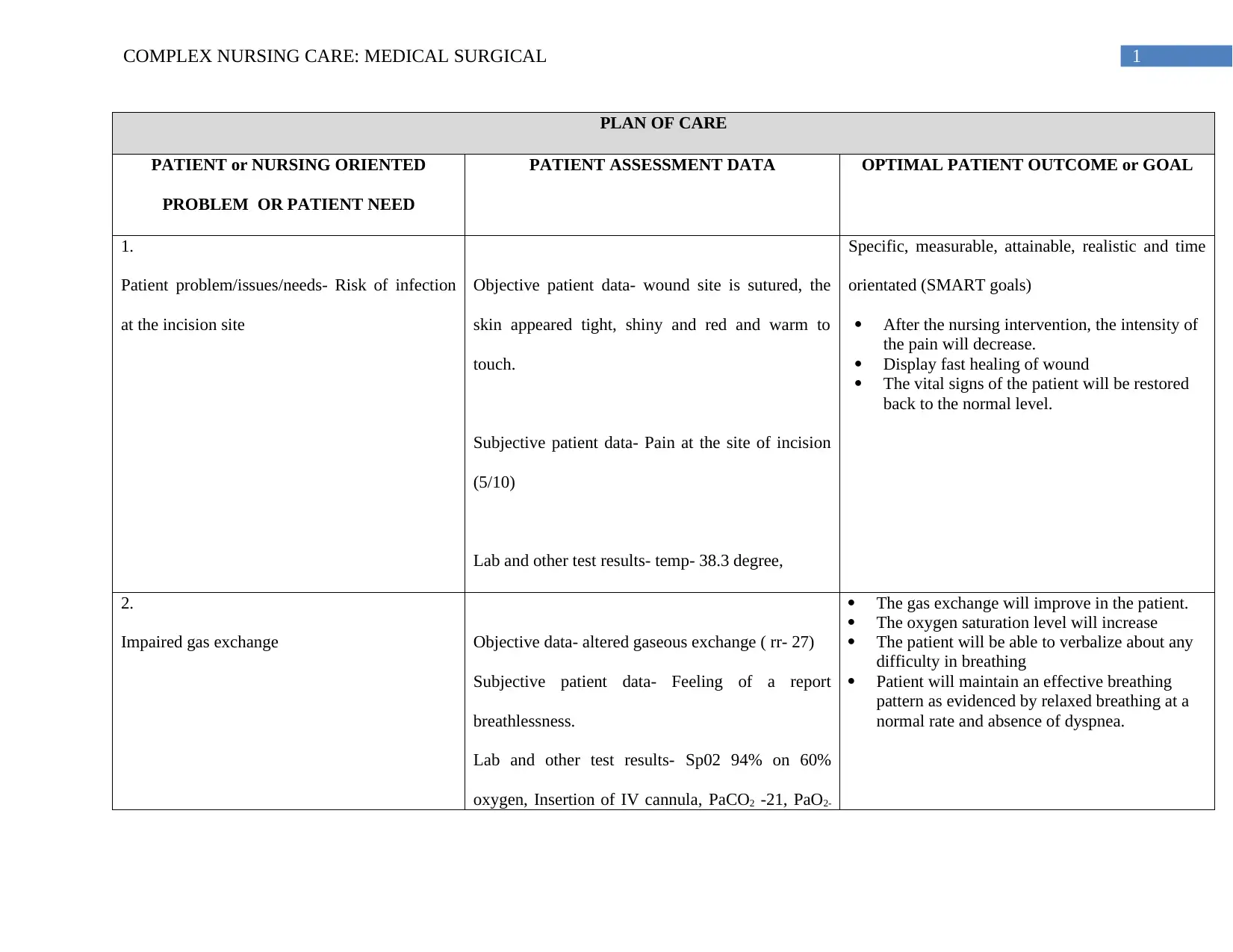
PLAN OF CARE
PATIENT or NURSING ORIENTED
PROBLEM OR PATIENT NEED
PATIENT ASSESSMENT DATA OPTIMAL PATIENT OUTCOME or GOAL
1.
Patient problem/issues/needs- Risk of infection
at the incision site
Objective patient data- wound site is sutured, the
skin appeared tight, shiny and red and warm to
touch.
Subjective patient data- Pain at the site of incision
(5/10)
Lab and other test results- temp- 38.3 degree,
Specific, measurable, attainable, realistic and time
orientated (SMART goals)
After the nursing intervention, the intensity of
the pain will decrease.
Display fast healing of wound
The vital signs of the patient will be restored
back to the normal level.
2.
Impaired gas exchange Objective data- altered gaseous exchange ( rr- 27)
Subjective patient data- Feeling of a report
breathlessness.
Lab and other test results- Sp02 94% on 60%
oxygen, Insertion of IV cannula, PaCO2 -21, PaO2-
The gas exchange will improve in the patient.
The oxygen saturation level will increase
The patient will be able to verbalize about any
difficulty in breathing
Patient will maintain an effective breathing
pattern as evidenced by relaxed breathing at a
normal rate and absence of dyspnea.
PLAN OF CARE
PATIENT or NURSING ORIENTED
PROBLEM OR PATIENT NEED
PATIENT ASSESSMENT DATA OPTIMAL PATIENT OUTCOME or GOAL
1.
Patient problem/issues/needs- Risk of infection
at the incision site
Objective patient data- wound site is sutured, the
skin appeared tight, shiny and red and warm to
touch.
Subjective patient data- Pain at the site of incision
(5/10)
Lab and other test results- temp- 38.3 degree,
Specific, measurable, attainable, realistic and time
orientated (SMART goals)
After the nursing intervention, the intensity of
the pain will decrease.
Display fast healing of wound
The vital signs of the patient will be restored
back to the normal level.
2.
Impaired gas exchange Objective data- altered gaseous exchange ( rr- 27)
Subjective patient data- Feeling of a report
breathlessness.
Lab and other test results- Sp02 94% on 60%
oxygen, Insertion of IV cannula, PaCO2 -21, PaO2-
The gas exchange will improve in the patient.
The oxygen saturation level will increase
The patient will be able to verbalize about any
difficulty in breathing
Patient will maintain an effective breathing
pattern as evidenced by relaxed breathing at a
normal rate and absence of dyspnea.
2COMPLEX NURSING CARE: MEDICAL SURGICAL
80.
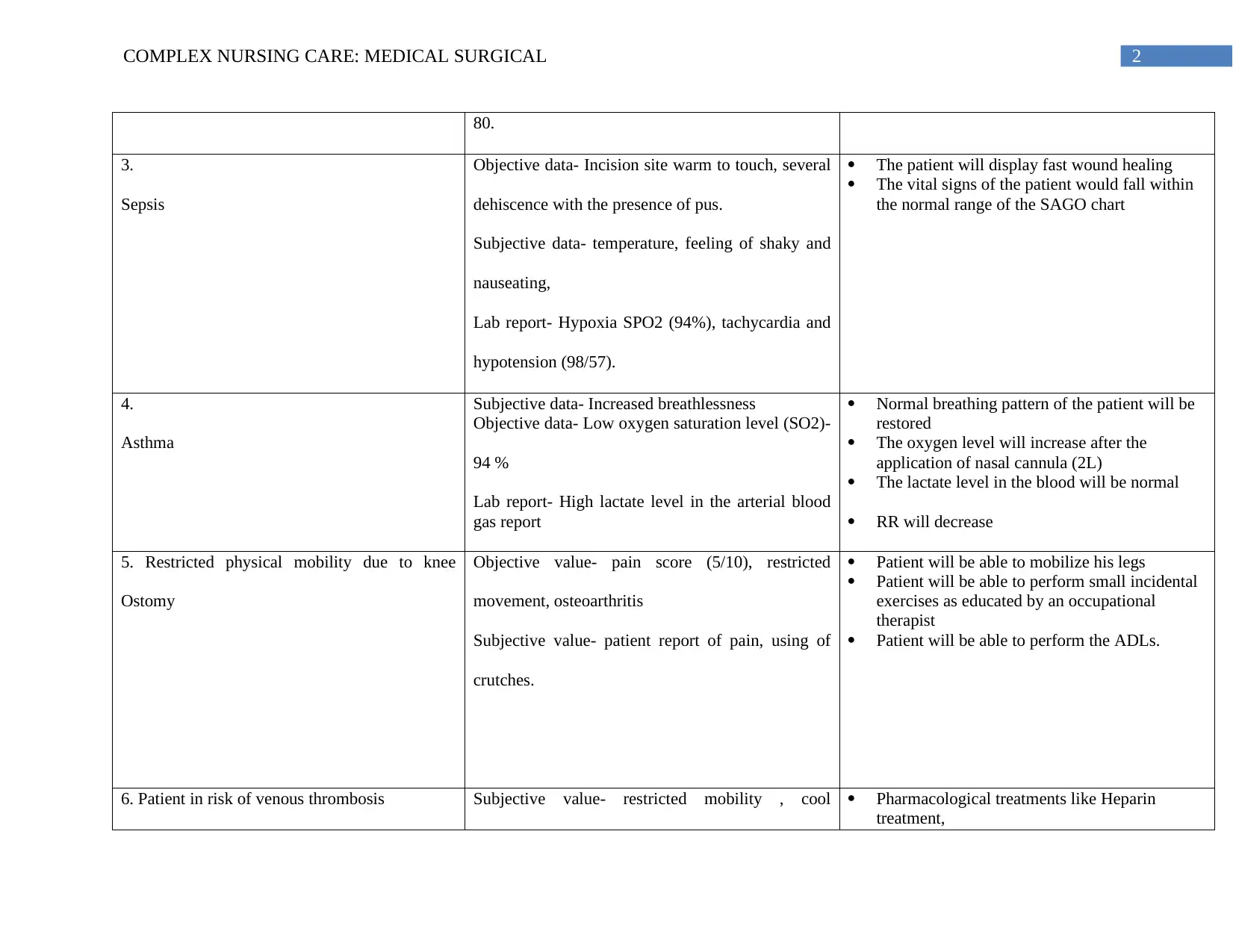
3.
Sepsis
Objective data- Incision site warm to touch, several
dehiscence with the presence of pus.
Subjective data- temperature, feeling of shaky and
nauseating,
Lab report- Hypoxia SPO2 (94%), tachycardia and
hypotension (98/57).
The patient will display fast wound healing
The vital signs of the patient would fall within
the normal range of the SAGO chart
4.
Asthma
Subjective data- Increased breathlessness
Objective data- Low oxygen saturation level (SO2)-
94 %
Lab report- High lactate level in the arterial blood
gas report
Normal breathing pattern of the patient will be
restored
The oxygen level will increase after the
application of nasal cannula (2L)
The lactate level in the blood will be normal
RR will decrease
5. Restricted physical mobility due to knee
Ostomy
Objective value- pain score (5/10), restricted
movement, osteoarthritis
Subjective value- patient report of pain, using of
crutches.
Patient will be able to mobilize his legs
Patient will be able to perform small incidental
exercises as educated by an occupational
therapist
Patient will be able to perform the ADLs.
6. Patient in risk of venous thrombosis Subjective value- restricted mobility , cool Pharmacological treatments like Heparin
treatment,
80.
3.
Sepsis
Objective data- Incision site warm to touch, several
dehiscence with the presence of pus.
Subjective data- temperature, feeling of shaky and
nauseating,
Lab report- Hypoxia SPO2 (94%), tachycardia and
hypotension (98/57).
The patient will display fast wound healing
The vital signs of the patient would fall within
the normal range of the SAGO chart
4.
Asthma
Subjective data- Increased breathlessness
Objective data- Low oxygen saturation level (SO2)-
94 %
Lab report- High lactate level in the arterial blood
gas report
Normal breathing pattern of the patient will be
restored
The oxygen level will increase after the
application of nasal cannula (2L)
The lactate level in the blood will be normal
RR will decrease
5. Restricted physical mobility due to knee
Ostomy
Objective value- pain score (5/10), restricted
movement, osteoarthritis
Subjective value- patient report of pain, using of
crutches.
Patient will be able to mobilize his legs
Patient will be able to perform small incidental
exercises as educated by an occupational
therapist
Patient will be able to perform the ADLs.
6. Patient in risk of venous thrombosis Subjective value- restricted mobility , cool Pharmacological treatments like Heparin
treatment,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3COMPLEX NURSING CARE: MEDICAL SURGICAL
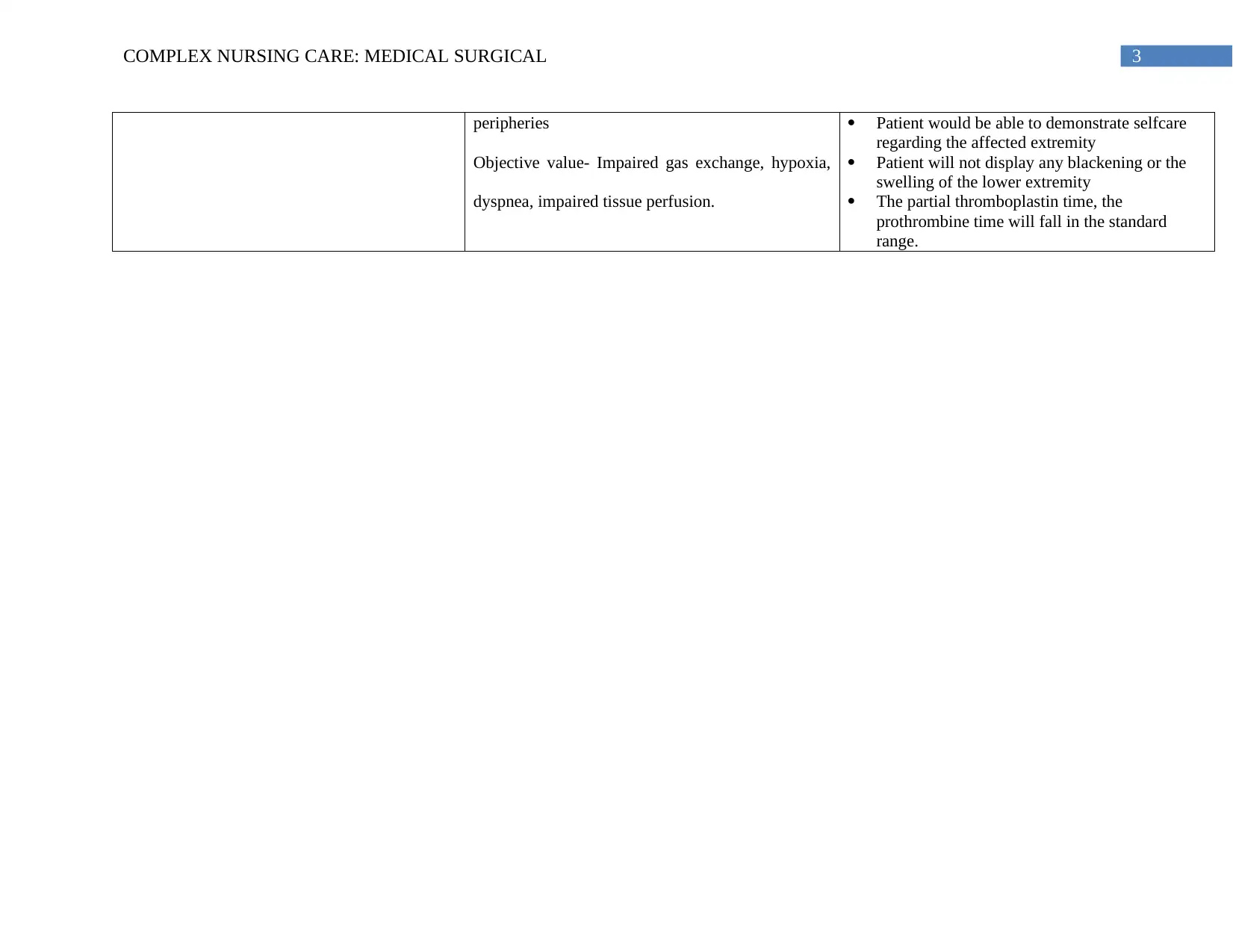
peripheries
Objective value- Impaired gas exchange, hypoxia,
dyspnea, impaired tissue perfusion.
Patient would be able to demonstrate selfcare
regarding the affected extremity
Patient will not display any blackening or the
swelling of the lower extremity
The partial thromboplastin time, the
prothrombine time will fall in the standard
range.
peripheries
Objective value- Impaired gas exchange, hypoxia,
dyspnea, impaired tissue perfusion.
Patient would be able to demonstrate selfcare
regarding the affected extremity
Patient will not display any blackening or the
swelling of the lower extremity
The partial thromboplastin time, the
prothrombine time will fall in the standard
range.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1COMPLEX NURSING CARE: MEDICAL SURGICAL
Background
The report is based Cristopher Collins, a 54 years male, who had been diagnosed with an
early stage osteoarthritis in the left knee, causing pan in the left knee and affecting the mobility
of the patient. After the osteotomy has been performed 5 days ago and an uneventful post-
operative period, the patient was discharged. Mr. Collins had been discharged with non-steroidal
anti-inflammatory medication as pain reliever. For improving the mobility he was recommended
with crutches and was fitted with a supportive knee brace.
After this, the patient was admitted in the emergency department with pain at the site of
incision, nauseating and shivering feeling. The wound site in the left knee was sutured with
several areas of dehiscence with en evidence of pus present. The client also reported to have
been suffering from breathlessness.
Mr. Collins ad past history of osteoarthritis and asthma since childhood. He does not have any
history of allergies and is non-smoker and regular swimmer.
Assessment
An A-G assessment was performed in the patient, which suggested that airway of the
patient is patent and clear. Respiratory is 27 which is a bit higher than that of the standard value,
which can be due to the occurrence of respiratory distress. The oxygen saturation level is 94 %
that is higher than the normal value. The vital signs of the patient had displayed tachycardia with
a heart rate of 125. According to the arterial blood gas values, the patient had been hypotensive.
The patient is febrile (38.3 degree) and is feeling shaky. The patient had reported pain in the left
knee with a pain score of 5/10. Objective date the displays low HB 112, WBC 18.4 and the level
Background
The report is based Cristopher Collins, a 54 years male, who had been diagnosed with an
early stage osteoarthritis in the left knee, causing pan in the left knee and affecting the mobility
of the patient. After the osteotomy has been performed 5 days ago and an uneventful post-
operative period, the patient was discharged. Mr. Collins had been discharged with non-steroidal
anti-inflammatory medication as pain reliever. For improving the mobility he was recommended
with crutches and was fitted with a supportive knee brace.
After this, the patient was admitted in the emergency department with pain at the site of
incision, nauseating and shivering feeling. The wound site in the left knee was sutured with
several areas of dehiscence with en evidence of pus present. The client also reported to have
been suffering from breathlessness.
Mr. Collins ad past history of osteoarthritis and asthma since childhood. He does not have any
history of allergies and is non-smoker and regular swimmer.
Assessment
An A-G assessment was performed in the patient, which suggested that airway of the
patient is patent and clear. Respiratory is 27 which is a bit higher than that of the standard value,
which can be due to the occurrence of respiratory distress. The oxygen saturation level is 94 %
that is higher than the normal value. The vital signs of the patient had displayed tachycardia with
a heart rate of 125. According to the arterial blood gas values, the patient had been hypotensive.
The patient is febrile (38.3 degree) and is feeling shaky. The patient had reported pain in the left
knee with a pain score of 5/10. Objective date the displays low HB 112, WBC 18.4 and the level
2COMPLEX NURSING CARE: MEDICAL SURGICAL
of platelets 276. The arterial blood gas displays a pH 7.3, with PaO2- 21 and PaO2- 80 and
HCO3-18 and BE- 4.The lactate of the patient is 2.8mmol/ L).
As evidences by the assessment levels, two clinical priorities that has been observed in
the patient is management of the wound infection and restoration of breathing pattern in the
patient.
Wound infection
Surgery involves incision in the skin that can cause wound infection after the surgical
procedure. Surgical site infection is one of the common health care problems that occurs in 8 5 of
the patients being admitted in a hospital. The development of SSI is dependent upon the
contamination of the site at the end of the surgical procedure (Fang et al., 2013). It relates to the
pathogenicity and the inoculum of the pathogens present, balanced against the immune system of
the host. The microorganisms causing infections are usually derived from the patient itself.
Surgical site infections might lead to the development of sepsis, which is a fatal condition and
can cause hypovolemic shock. Sepsis and hypovolemic shock can be detrimental causing multi-
organ failure and mortality (Bertesteanu et al., 2013).
Pathophysiology of surgical site infection
With the creation of an incision site, some initiators of the human inflammatory
responses are initiated generally. As a part of the homeostatic mechanism, the coagulation of the
platelets and the proteins are initiated. The complement proteins and the mast cells are also
activated and Bradykinin is secreted from the ubiquitous protein receptor. This causes
inflammation and restricted blood flow at the incision site. Local vasodilation and an increase
vascular permeability causes the formation of the edema (Fang et al., 2013). Therefore, the
of platelets 276. The arterial blood gas displays a pH 7.3, with PaO2- 21 and PaO2- 80 and
HCO3-18 and BE- 4.The lactate of the patient is 2.8mmol/ L).
As evidences by the assessment levels, two clinical priorities that has been observed in
the patient is management of the wound infection and restoration of breathing pattern in the
patient.
Wound infection
Surgery involves incision in the skin that can cause wound infection after the surgical
procedure. Surgical site infection is one of the common health care problems that occurs in 8 5 of
the patients being admitted in a hospital. The development of SSI is dependent upon the
contamination of the site at the end of the surgical procedure (Fang et al., 2013). It relates to the
pathogenicity and the inoculum of the pathogens present, balanced against the immune system of
the host. The microorganisms causing infections are usually derived from the patient itself.
Surgical site infections might lead to the development of sepsis, which is a fatal condition and
can cause hypovolemic shock. Sepsis and hypovolemic shock can be detrimental causing multi-
organ failure and mortality (Bertesteanu et al., 2013).
Pathophysiology of surgical site infection
With the creation of an incision site, some initiators of the human inflammatory
responses are initiated generally. As a part of the homeostatic mechanism, the coagulation of the
platelets and the proteins are initiated. The complement proteins and the mast cells are also
activated and Bradykinin is secreted from the ubiquitous protein receptor. This causes
inflammation and restricted blood flow at the incision site. Local vasodilation and an increase
vascular permeability causes the formation of the edema (Fang et al., 2013). Therefore, the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3COMPLEX NURSING CARE: MEDICAL SURGICAL
wound site in the patients appears swollen and painful. With the increased vascular activity, the
phagocytic cells gets access to the injured soft tissues. However, proinflammatory cytokines,
products of tissue injury orchestrates the movements of the phagocytes in the wound (Makris,
Abrams, Gurland & Reid, 2014). The lipid peroxidation leads to more tissue injury and activates
the signals of the initiators. Finally the wound space is filled bacteria, necrotic tissue and
proteinacious fluids that forms the puss.
Intervention
Interventions would include setting of long term and short term goals to facilitate proper
and fast healing of wound and to prevent wound infection. The patient had reported pain in the
incision site, which can be managed by the application of pharmacological and non
pharmacologal interventions (Sørensen 2012). Pharmacological interventions, like the
administration of paracetamol, Ibuprofen can be administered to the patient as per the medication
chart. In case the pain increases (7-10), opioid can be given as per his age and body weight
(Bartels et al., 2016). The PQRST pain assessment scale should be used to assess the intensity of
the pain, as it gives important information about the quality of pain, radiation, temporal factors,
and the severity of the pain. Other alternative therapies might include the application of cold
compression therapy, massage (McCartney and Nelligan 2014).
Normally infections occurs within 30 days of the surgery with varied symptoms. Some of
the common clinical manifestation of the surgical site infection is that, the incision site is red,
swollen with the presence of some puss around the wound. Again, it is evident that Mr Collins
was febrile, which indicates towards the incidence of an infection. Fever is generally, one of the
ways in which, the immune system tries to combat and infection (Sørensen 2012).
wound site in the patients appears swollen and painful. With the increased vascular activity, the
phagocytic cells gets access to the injured soft tissues. However, proinflammatory cytokines,
products of tissue injury orchestrates the movements of the phagocytes in the wound (Makris,
Abrams, Gurland & Reid, 2014). The lipid peroxidation leads to more tissue injury and activates
the signals of the initiators. Finally the wound space is filled bacteria, necrotic tissue and
proteinacious fluids that forms the puss.
Intervention
Interventions would include setting of long term and short term goals to facilitate proper
and fast healing of wound and to prevent wound infection. The patient had reported pain in the
incision site, which can be managed by the application of pharmacological and non
pharmacologal interventions (Sørensen 2012). Pharmacological interventions, like the
administration of paracetamol, Ibuprofen can be administered to the patient as per the medication
chart. In case the pain increases (7-10), opioid can be given as per his age and body weight
(Bartels et al., 2016). The PQRST pain assessment scale should be used to assess the intensity of
the pain, as it gives important information about the quality of pain, radiation, temporal factors,
and the severity of the pain. Other alternative therapies might include the application of cold
compression therapy, massage (McCartney and Nelligan 2014).
Normally infections occurs within 30 days of the surgery with varied symptoms. Some of
the common clinical manifestation of the surgical site infection is that, the incision site is red,
swollen with the presence of some puss around the wound. Again, it is evident that Mr Collins
was febrile, which indicates towards the incidence of an infection. Fever is generally, one of the
ways in which, the immune system tries to combat and infection (Sørensen 2012).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4COMPLEX NURSING CARE: MEDICAL SURGICAL
Furthermore, it can be seen that the assessment of the patient lies in the SAGO chart.
Yellow zone in the SAGO chart represents early deterioration of the patient and requires for an
urgent review and a rapid response. In order to ensure that, it is necessary to have an excellent
communication between allied health care professionals. This calls for the use of an ISBAR tool
for a proper clinical handover. Again, it is evident, that the patient has the risk of developing
sepsis, which can be managed by the intravenous application of the IV fluids (Bloos & Reinhart
2014). Since, Mr. Collin is suspected to be having an infection, proper hand hygiene techniques
has to be maintained, while handling or dressing the wound. Proper wound management would
include a proper wound debriment, cleansing and appropriate dressings (Sørensen 2012).
Outcome
Patient will be able to report less pain
The vital observation of the patient would fall within the normal range of the SAGO chart
The patient would display low risks of developing sepsis
Patient and the family would be able to verbalise all the preventive measures that can be
taken to prevent infections.
Impaired gas exchange
The gaseous exchange between the alveoli and the pulmonary capillaries occur due to
diffusion. The difference in the concentration is maintained by the continuous flow of blood in
the alveoli and the pulmonary capillaries (Petersson & Glenny 2014). Any changes in the alveoli
and the pulmonary pressure might lead to a blockage of the airways. In case of high alveoli
pressure, the capillaries gets narrowed and squeezed causing impaired ventilation. This disrupts
the perfusion of the lungs causing an impaired gas exchange. The common clinical manifestation
Furthermore, it can be seen that the assessment of the patient lies in the SAGO chart.
Yellow zone in the SAGO chart represents early deterioration of the patient and requires for an
urgent review and a rapid response. In order to ensure that, it is necessary to have an excellent
communication between allied health care professionals. This calls for the use of an ISBAR tool
for a proper clinical handover. Again, it is evident, that the patient has the risk of developing
sepsis, which can be managed by the intravenous application of the IV fluids (Bloos & Reinhart
2014). Since, Mr. Collin is suspected to be having an infection, proper hand hygiene techniques
has to be maintained, while handling or dressing the wound. Proper wound management would
include a proper wound debriment, cleansing and appropriate dressings (Sørensen 2012).
Outcome
Patient will be able to report less pain
The vital observation of the patient would fall within the normal range of the SAGO chart
The patient would display low risks of developing sepsis
Patient and the family would be able to verbalise all the preventive measures that can be
taken to prevent infections.
Impaired gas exchange
The gaseous exchange between the alveoli and the pulmonary capillaries occur due to
diffusion. The difference in the concentration is maintained by the continuous flow of blood in
the alveoli and the pulmonary capillaries (Petersson & Glenny 2014). Any changes in the alveoli
and the pulmonary pressure might lead to a blockage of the airways. In case of high alveoli
pressure, the capillaries gets narrowed and squeezed causing impaired ventilation. This disrupts
the perfusion of the lungs causing an impaired gas exchange. The common clinical manifestation
5COMPLEX NURSING CARE: MEDICAL SURGICAL
of impaired gas exchange is abnormal arterial gas level, abnormal arterial pH level, high lactose
level, hypoxemia, tachycardia and dyspnea (Pascoal et al., 2014). Low PO2 level signifies that
the amount of the oxygen gas dissolved in the blood is low. High lactate level in the blood of the
patient signifies that the oxygen level is low in the blood. When the oxygen level is low, the
carbohydrate breaks down for the generation of energy making the lactate acid levels in the
blood. Again, the high lactate level in blood can be linked with conditions like sepsis or shock
that reduces the flow of oxygen and blood throughout the body (Sola et al., 2014). The oxygen
saturation level of the patients is 94 %, which is less than the standard value, indicating towards
the occurrence of hypoxia. Again the haemoglobin level of the patient indicates towards the
occurrence of anaemia.
Intervention
Intervention for an impaired gas exchange would involve a continuous assessment and
recording of the respiratory rate, assessment of the BGL levels, noting the pH, PaCO2, HCO3.
Again, it is again necessary to measure, if there is an unusual breathing pattern. It is necessary to
assess the rate and the depth of respiration. It is necessary to assess the patient for conditions like
apnoea, Biot’s respiration as they also clearly displays cessation of breathing. As per the lab
reports of the patient, the oxygen saturation level and the lactate level of the patient has to be
restored. A continuous pulse oximetry testing has to be done to detect any changes in the oxygen
saturation level (Sola et al., 2016). The patient should also be assessed for hypoxia, that can lead
to cyanosis to the inside of a mouth is an emergency situation. Some useful techniques like
pursed lip- breathing, abdominal breathing and relaxation techniques can be used for improving
the ventilation (Gläser et al.,2013). Depending upon the comfort level of the patient, the head of
the bed should be placed at an angle of 45°.
of impaired gas exchange is abnormal arterial gas level, abnormal arterial pH level, high lactose
level, hypoxemia, tachycardia and dyspnea (Pascoal et al., 2014). Low PO2 level signifies that
the amount of the oxygen gas dissolved in the blood is low. High lactate level in the blood of the
patient signifies that the oxygen level is low in the blood. When the oxygen level is low, the
carbohydrate breaks down for the generation of energy making the lactate acid levels in the
blood. Again, the high lactate level in blood can be linked with conditions like sepsis or shock
that reduces the flow of oxygen and blood throughout the body (Sola et al., 2014). The oxygen
saturation level of the patients is 94 %, which is less than the standard value, indicating towards
the occurrence of hypoxia. Again the haemoglobin level of the patient indicates towards the
occurrence of anaemia.
Intervention
Intervention for an impaired gas exchange would involve a continuous assessment and
recording of the respiratory rate, assessment of the BGL levels, noting the pH, PaCO2, HCO3.
Again, it is again necessary to measure, if there is an unusual breathing pattern. It is necessary to
assess the rate and the depth of respiration. It is necessary to assess the patient for conditions like
apnoea, Biot’s respiration as they also clearly displays cessation of breathing. As per the lab
reports of the patient, the oxygen saturation level and the lactate level of the patient has to be
restored. A continuous pulse oximetry testing has to be done to detect any changes in the oxygen
saturation level (Sola et al., 2016). The patient should also be assessed for hypoxia, that can lead
to cyanosis to the inside of a mouth is an emergency situation. Some useful techniques like
pursed lip- breathing, abdominal breathing and relaxation techniques can be used for improving
the ventilation (Gläser et al.,2013). Depending upon the comfort level of the patient, the head of
the bed should be placed at an angle of 45°.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6COMPLEX NURSING CARE: MEDICAL SURGICAL
Outcome
The patient will be able to maintain an effective breathing pattern and relaxed breathing
at a normal rate and depth with an RR of 12-22 and HR- 65-100.
The respiratory levels of the patient will remain within the normal limits
The ABG levels will be restored back to the normal limits.
The oxygen saturation level of the patient will increase
The patient will be able to demonstrate maximum expansion of the lungs with adequate
ventilation.
Outcome
The patient will be able to maintain an effective breathing pattern and relaxed breathing
at a normal rate and depth with an RR of 12-22 and HR- 65-100.
The respiratory levels of the patient will remain within the normal limits
The ABG levels will be restored back to the normal limits.
The oxygen saturation level of the patient will increase
The patient will be able to demonstrate maximum expansion of the lungs with adequate
ventilation.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7COMPLEX NURSING CARE: MEDICAL SURGICAL
References
Bartels, K., Mayes, L.M., Dingmann, C., Bullard, K.J., Hopfer, C.J. and Binswanger, I.A., 2016.
‘Opioid use and storage patterns by patients after hospital discharge following
surgery’. PloS one, vol. 11, no. 1, p.e0147972.
Bertesteanu, S., Triaridis, S., Stankovic, M., Lazar, V., Chifiriuc, M.C., Vlad, M. & Grigore, R.,
2014. ‘Polymicrobial wound infections: pathophysiology and current therapeutic
approaches’. International journal of pharmaceutics, vol. 463, no.2, pp.119-126.
Bloos, F., & Reinhart, K. 2014. Rapid diagnosis of sepsis. Virulence, 5(1), pp. 154-160.
Fang, C., Wong, T.M., Lau, T.W., To, K.K., Wong, S.S. & Leung, F., 2017. ‘Infection after
fracture osteosynthesis–Part I: Pathogenesis, diagnosis and classification’. Journal of
Orthopaedic Surgery, vol. 25, no. (1), p.2309499017692712.
Gläser, S., Obst, A., Koch, B., Henkel, B., Grieger, A., Felix, S.B., Halank, M., Bruch, L.,
Bollmann, T., Warnke, C. & Schäper, C., 2013. ‘Pulmonary hypertension in patients with
idiopathic pulmonary fibrosis–the predictive value of exercise capacity and gas exchange
efficiency’. PLoS One,vol. 8 ,no. 6, p.e65643.
Makris, U. E., Abrams, R. C., Gurland, B., & Reid, M. C. 2014. ‘Management of persistent pain
in the older patient: a clinical review’. JAMA, vol. 312, no.8,pp. 825–836.
References
Bartels, K., Mayes, L.M., Dingmann, C., Bullard, K.J., Hopfer, C.J. and Binswanger, I.A., 2016.
‘Opioid use and storage patterns by patients after hospital discharge following
surgery’. PloS one, vol. 11, no. 1, p.e0147972.
Bertesteanu, S., Triaridis, S., Stankovic, M., Lazar, V., Chifiriuc, M.C., Vlad, M. & Grigore, R.,
2014. ‘Polymicrobial wound infections: pathophysiology and current therapeutic
approaches’. International journal of pharmaceutics, vol. 463, no.2, pp.119-126.
Bloos, F., & Reinhart, K. 2014. Rapid diagnosis of sepsis. Virulence, 5(1), pp. 154-160.
Fang, C., Wong, T.M., Lau, T.W., To, K.K., Wong, S.S. & Leung, F., 2017. ‘Infection after
fracture osteosynthesis–Part I: Pathogenesis, diagnosis and classification’. Journal of
Orthopaedic Surgery, vol. 25, no. (1), p.2309499017692712.
Gläser, S., Obst, A., Koch, B., Henkel, B., Grieger, A., Felix, S.B., Halank, M., Bruch, L.,
Bollmann, T., Warnke, C. & Schäper, C., 2013. ‘Pulmonary hypertension in patients with
idiopathic pulmonary fibrosis–the predictive value of exercise capacity and gas exchange
efficiency’. PLoS One,vol. 8 ,no. 6, p.e65643.
Makris, U. E., Abrams, R. C., Gurland, B., & Reid, M. C. 2014. ‘Management of persistent pain
in the older patient: a clinical review’. JAMA, vol. 312, no.8,pp. 825–836.
8COMPLEX NURSING CARE: MEDICAL SURGICAL
McCartney, C.J. & Nelligan, K., 2014. ‘Postoperative pain management after total knee
arthroplasty in elderly patients: treatment options’. Drugs & aging, vol. 31, no. 2, pp.83-
91.
Pascoal, L. M., Lopes, M. V., Chaves, D. B., Beltrão, B. A., da Silva, V. M., & Monteiro, F. P.
2015. ‘Impaired gas exchange: accuracy of defining characteristics in children with acute
respiratory infection’. Revista latino-americana de enfermagem, vol. 23, no. 3,pp. 491–
499.
Petersson, J. & Glenny, R.W., 2014. ‘Gas exchange and ventilation–perfusion relationships in
the lung’. Archives of surgery, vol. 140 , no. 4, pp.200-254
Sola, A., Golombek, S.G., Montes Bueno, M.T., Lemus‐Varela, L., Zuluaga, C., Domínguez, F.,
Baquero, H., Young Sarmiento, A.E., Natta, D., Rodriguez Perez, J.M. & Deulofeut, R.,
2014. ‘Safe oxygen saturation targeting and monitoring in preterm infants: can we avoid
hypoxia and hyperoxia?’. Acta paediatrica, vol.103 , no. 10), pp.1009-1018.
Sørensen, L.T., 2012. ‘Wound healing and infection in surgery: the clinical impact of smoking
and smoking cessation: a systematic review and meta-analysis’. Archives of surgery, vol.
147 , no. 4, pp.373-383.
McCartney, C.J. & Nelligan, K., 2014. ‘Postoperative pain management after total knee
arthroplasty in elderly patients: treatment options’. Drugs & aging, vol. 31, no. 2, pp.83-
91.
Pascoal, L. M., Lopes, M. V., Chaves, D. B., Beltrão, B. A., da Silva, V. M., & Monteiro, F. P.
2015. ‘Impaired gas exchange: accuracy of defining characteristics in children with acute
respiratory infection’. Revista latino-americana de enfermagem, vol. 23, no. 3,pp. 491–
499.
Petersson, J. & Glenny, R.W., 2014. ‘Gas exchange and ventilation–perfusion relationships in
the lung’. Archives of surgery, vol. 140 , no. 4, pp.200-254
Sola, A., Golombek, S.G., Montes Bueno, M.T., Lemus‐Varela, L., Zuluaga, C., Domínguez, F.,
Baquero, H., Young Sarmiento, A.E., Natta, D., Rodriguez Perez, J.M. & Deulofeut, R.,
2014. ‘Safe oxygen saturation targeting and monitoring in preterm infants: can we avoid
hypoxia and hyperoxia?’. Acta paediatrica, vol.103 , no. 10), pp.1009-1018.
Sørensen, L.T., 2012. ‘Wound healing and infection in surgery: the clinical impact of smoking
and smoking cessation: a systematic review and meta-analysis’. Archives of surgery, vol.
147 , no. 4, pp.373-383.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.