Policy Critique Assessment 2022
VerifiedAdded on 2022/10/01
|17
|3674
|17
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Assessment Task 2
Policy Critique
Student’s Name:
University:
1
Policy Critique
Student’s Name:
University:
1
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Table of Contents
Introduction 3
Health Policy 4
Consultation with consumers and colleagues 5
New policy 6
Implementation in practice 7
Community setting 7
Hospital setting 7
Residential care setting 8
Action Plan: Implementing a policy 8
Recommendations on the measurement of implementation 9
Conclusion 10
Appendix A- 11
1. POLICY STATEMENT 12
2. AIMS 12
3. TARGET AUDIENCE 13
4. RESPONSIBILITIES 13
5. DEFINITIONS 13
6. DOCUMENTATION 13
REFERENCES 13
REVISION & APPROVAL HISTORY 13
Appendix B 14
2
Introduction 3
Health Policy 4
Consultation with consumers and colleagues 5
New policy 6
Implementation in practice 7
Community setting 7
Hospital setting 7
Residential care setting 8
Action Plan: Implementing a policy 8
Recommendations on the measurement of implementation 9
Conclusion 10
Appendix A- 11
1. POLICY STATEMENT 12
2. AIMS 12
3. TARGET AUDIENCE 13
4. RESPONSIBILITIES 13
5. DEFINITIONS 13
6. DOCUMENTATION 13
REFERENCES 13
REVISION & APPROVAL HISTORY 13
Appendix B 14
2
Introduction
The complicated, as well as multifactorial nature of the risk of fall within a quickly aging
population, requests a pro activated a deliberate way to prevent falls. The policy's role in
preventing falls prevention among older individuals is to give the framework and support
fundamental to integrate falls prevention within a practice. The new policies tend to replace the
existing policies or gets amended with new every new research. Hence, it is essential that the
policies should be amended or designed followed by reviewing so as to give evidence-based
consideration to the older people in terms of fall prevention. Despite the fact that due to the
utilization of policies there are several pieces of evidence that support that the risk of falls in
Australia has diminished, but both the numbers and rate for all falls-related medical clinic
admission among older individuals have been increasing (Dapp, Anders, Suijker & Bjorkman,
2014). This demonstrates that a new or amended policy is required if the anticipated wellbeing
framework burden because of falls is to be directed (Day et al., 2010). Falls are a huge danger to
the safety, wellbeing, and freedom of Australia's older residents, representing 62 percent of
coincidental passings for individuals over 75 years (Martins, Andrade & Santos, 2015). Falls are
generally normal, among the older individuals accounting for about 28 to 39 percent above 65
years encountering one fall every year, and up to half encountering numerous falls (Taylor-
Piliae, Peterson & Mohler, 2017). The aging population in Australia which is above 65 years is
anticipated to increment from 1 percent in 2008 for up to 25 percent by the year 2056, with the
number of individuals above 80 growing generally significantly (Warner Frieson, 2016).
The main objective of the present report is to update an existing policy to be implemented for
preventing falls and its management among older individuals of age above 65 years while
supporting the present policy using evidence-based research. An action plan is also discussed to
implement the policy with evaluation tools.
Health Policy
3
The complicated, as well as multifactorial nature of the risk of fall within a quickly aging
population, requests a pro activated a deliberate way to prevent falls. The policy's role in
preventing falls prevention among older individuals is to give the framework and support
fundamental to integrate falls prevention within a practice. The new policies tend to replace the
existing policies or gets amended with new every new research. Hence, it is essential that the
policies should be amended or designed followed by reviewing so as to give evidence-based
consideration to the older people in terms of fall prevention. Despite the fact that due to the
utilization of policies there are several pieces of evidence that support that the risk of falls in
Australia has diminished, but both the numbers and rate for all falls-related medical clinic
admission among older individuals have been increasing (Dapp, Anders, Suijker & Bjorkman,
2014). This demonstrates that a new or amended policy is required if the anticipated wellbeing
framework burden because of falls is to be directed (Day et al., 2010). Falls are a huge danger to
the safety, wellbeing, and freedom of Australia's older residents, representing 62 percent of
coincidental passings for individuals over 75 years (Martins, Andrade & Santos, 2015). Falls are
generally normal, among the older individuals accounting for about 28 to 39 percent above 65
years encountering one fall every year, and up to half encountering numerous falls (Taylor-
Piliae, Peterson & Mohler, 2017). The aging population in Australia which is above 65 years is
anticipated to increment from 1 percent in 2008 for up to 25 percent by the year 2056, with the
number of individuals above 80 growing generally significantly (Warner Frieson, 2016).
The main objective of the present report is to update an existing policy to be implemented for
preventing falls and its management among older individuals of age above 65 years while
supporting the present policy using evidence-based research. An action plan is also discussed to
implement the policy with evaluation tools.
Health Policy
3
The policy selected for the present assessment is the “Fall and Fall Injury Prevention and
Management Policy” which is an amended and updated form of an existing policy that is
proposed by the “National Safety and Quality Health Service Standards Australian Commission
for Safety” as well as the “Quality in Health Care” (System Performance and Service Delivery,
2016). The major goal of the policy is to enhance life quality while maximizing the
independence of older individuals. It also helps in the establishment of the principles of best
practice required for a hospital, residential homes, as well as several community settings. The
policy tends to target the people while they are present in the mentioned care settings (İyigün et
al., 2016).
The overview of the policy provides an explanation that the policy makes use of 6 major toolkits
to prevent falls among older people. They are as follows (System Performance and Service
Delivery, 2016):
Tool 1 - It consists of TOR i.e., Terms of Reference which helps to illustrate a committee about
the leading activities which are required for improving care while reducing risk and meeting
health safety and standard needs.
Tool 2 - This tool is helpful in providing recommendations on how to screen a fall risk and
when, planning of care to be provided, care assessment as well as planning od discharge of older
individuals with careful input and consultation from consumers and colleagues.
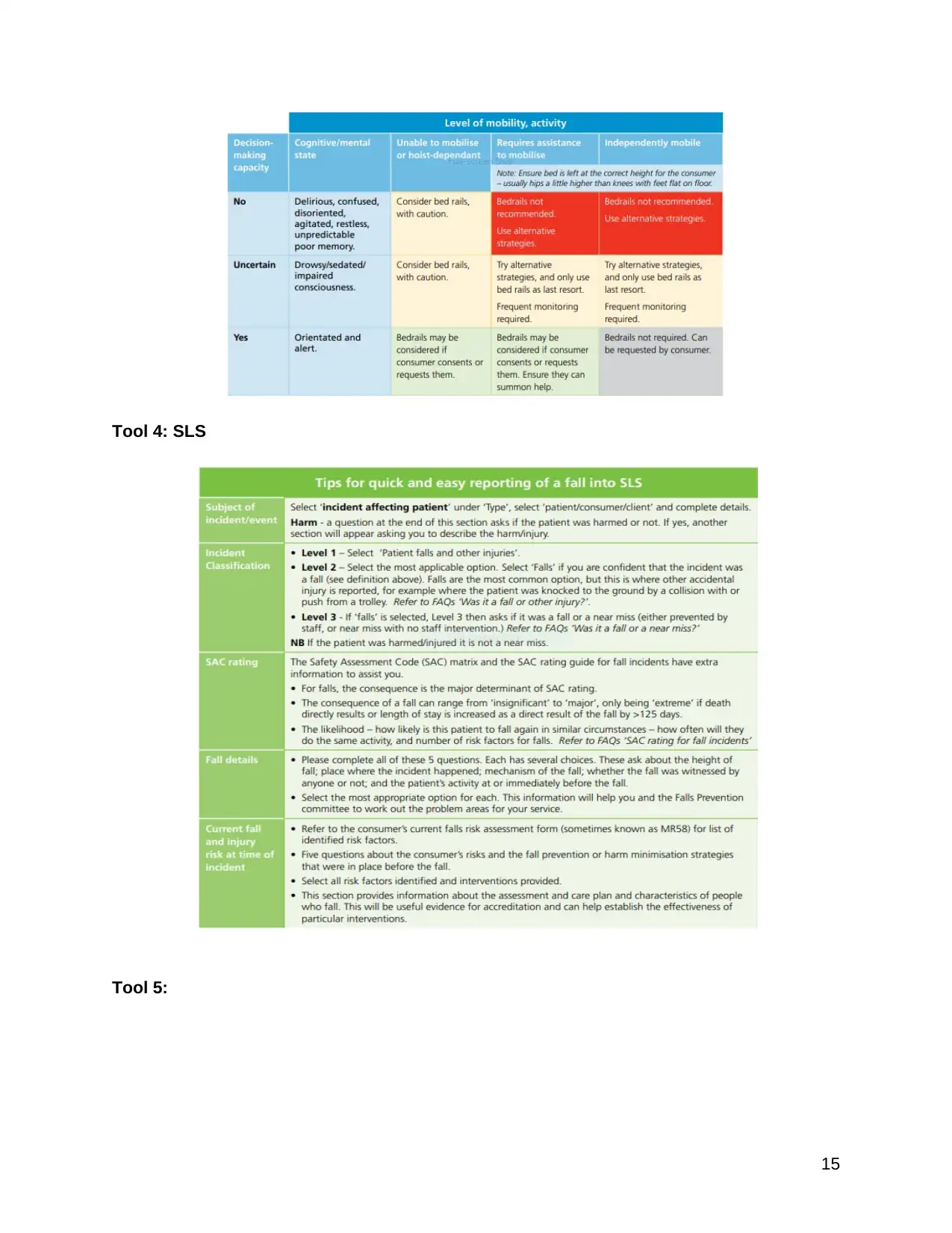
Tool 3 - This tool helps to design safe utilization of bed rails by minimizing is utilization through
alternate approaches, risk of capable harm due to unsafe utilization, identification of restraint
while using bed rails, and the requirement of SLS (i.e., Safety Learning System).
Tool 4 - to report about an incident of an older individual fall in SLS containing the important
details to notify the incidents.
Tool 5 - To report about the incident using FAQs (i.e., frequently asked questions) by providing
scenarios and examples in the form of illustrations for clarifying about the report of a fall.
4
Management Policy” which is an amended and updated form of an existing policy that is
proposed by the “National Safety and Quality Health Service Standards Australian Commission
for Safety” as well as the “Quality in Health Care” (System Performance and Service Delivery,
2016). The major goal of the policy is to enhance life quality while maximizing the
independence of older individuals. It also helps in the establishment of the principles of best
practice required for a hospital, residential homes, as well as several community settings. The
policy tends to target the people while they are present in the mentioned care settings (İyigün et
al., 2016).
The overview of the policy provides an explanation that the policy makes use of 6 major toolkits
to prevent falls among older people. They are as follows (System Performance and Service
Delivery, 2016):
Tool 1 - It consists of TOR i.e., Terms of Reference which helps to illustrate a committee about
the leading activities which are required for improving care while reducing risk and meeting
health safety and standard needs.
Tool 2 - This tool is helpful in providing recommendations on how to screen a fall risk and
when, planning of care to be provided, care assessment as well as planning od discharge of older
individuals with careful input and consultation from consumers and colleagues.
Tool 3 - This tool helps to design safe utilization of bed rails by minimizing is utilization through
alternate approaches, risk of capable harm due to unsafe utilization, identification of restraint
while using bed rails, and the requirement of SLS (i.e., Safety Learning System).
Tool 4 - to report about an incident of an older individual fall in SLS containing the important
details to notify the incidents.
Tool 5 - To report about the incident using FAQs (i.e., frequently asked questions) by providing
scenarios and examples in the form of illustrations for clarifying about the report of a fall.
4
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Tool 6 - It is a review that is utilized as a guide for investigating and reviewing post-fall. It
explains the procedure of the review during 2 days of a severe or repetitive fall. Hence, enabling
reviewing of several fall incidents along with enhancement in consumer safety in a timely
manner with decreased repetitive falls.
Consultation with consumers and colleagues
The consumer and the colleagues are made clear of the result of the appraisal and show their
participation when required in the arrangement and development of interventions, as per
prerequisites of the National Safety and Quality Health Service Standards. It consists of the
following steps (Clemson et al., 2017):
● The consumers should join forces with the staff in the improvement of the falls
prevention plan of care and furthermore the plan of the discharge.
● The colleagues will offer help while coordinating care to the consumers to encourage
their commitment and consideration, with the thought of wellbeing proficiency and social
and language prerequisites.
● Composed and verbal data could help, however not substitute this procedure.
● Present learning of the risk factors of consumers related to falls and related damage in
case of a fall is basic in actualizing a viable consideration plan, and for discussing that
with other colleagues.
● Screening, appraisal, survey, and reassessment to recognize the older person's fall and fall
damage hazard variables is directed Guidelines.
● Suggested screening, evaluation and audit or reassessment for an assortment of healthcare
settings.
New policy
5
explains the procedure of the review during 2 days of a severe or repetitive fall. Hence, enabling
reviewing of several fall incidents along with enhancement in consumer safety in a timely
manner with decreased repetitive falls.
Consultation with consumers and colleagues
The consumer and the colleagues are made clear of the result of the appraisal and show their
participation when required in the arrangement and development of interventions, as per
prerequisites of the National Safety and Quality Health Service Standards. It consists of the
following steps (Clemson et al., 2017):
● The consumers should join forces with the staff in the improvement of the falls
prevention plan of care and furthermore the plan of the discharge.
● The colleagues will offer help while coordinating care to the consumers to encourage
their commitment and consideration, with the thought of wellbeing proficiency and social
and language prerequisites.
● Composed and verbal data could help, however not substitute this procedure.
● Present learning of the risk factors of consumers related to falls and related damage in
case of a fall is basic in actualizing a viable consideration plan, and for discussing that
with other colleagues.
● Screening, appraisal, survey, and reassessment to recognize the older person's fall and fall
damage hazard variables is directed Guidelines.
● Suggested screening, evaluation and audit or reassessment for an assortment of healthcare
settings.
New policy
5
The literature review was carried out on the prevention and management of falls among older
people in Australia. Delirium with the help of online guides and search engines such as
CINAHL, Google Scholar, etc. The criteria for the search was kept limited to interventions and
current policies in Australia on falls prevention among older individuals. The current policy
provides guided actions to prevent and manage the risk of falls and related damage. The
guidelines of the policy have been amended as some of the guidelines was unable to fulfill the
needs to prevent fall among older individuals hence, the appropriate tools that were added are
(System Performance and Service Delivery, 2016):
1. In the policy, the new included principle is that the care should be provided in a way that
it reduces the utilization of restrictive practices along with effective management of risk
towards the consumers as reflected in Tool 3.
2. Tool 1 was amended with little changes while recommendations were provided in Tool 2
in terms of screening and evaluation of a consumer’s risk of falls in several healthcare
settings while the previous policy was only based on specific settings. The new policy
also involves the input of consumers and colleagues after consultation.
3. The new policy assists Tool 3 for the identification of the avoidance of bed rails when
required while ensuring the safety of the consumer and the implementation of risk control
measures for minimizing capable harm.
4. In Tool 4 the addition of SLS and FAQs in Tool 5 helps in providing clear guidance on
how to report the incidents of falls.
5. The flowchart used in Tool 6 has been amended with smaller changes for guiding the
process of review post-fall.
Implementation in practice
Followed by the consultation with consumers and colleagues there is a requirement of an action
plan to be implemented. The method used to implement a proper structure and planning of new
policies is in the form of a table which consists of several activities. However, several settings
6
people in Australia. Delirium with the help of online guides and search engines such as
CINAHL, Google Scholar, etc. The criteria for the search was kept limited to interventions and
current policies in Australia on falls prevention among older individuals. The current policy
provides guided actions to prevent and manage the risk of falls and related damage. The
guidelines of the policy have been amended as some of the guidelines was unable to fulfill the
needs to prevent fall among older individuals hence, the appropriate tools that were added are
(System Performance and Service Delivery, 2016):
1. In the policy, the new included principle is that the care should be provided in a way that
it reduces the utilization of restrictive practices along with effective management of risk
towards the consumers as reflected in Tool 3.
2. Tool 1 was amended with little changes while recommendations were provided in Tool 2
in terms of screening and evaluation of a consumer’s risk of falls in several healthcare
settings while the previous policy was only based on specific settings. The new policy
also involves the input of consumers and colleagues after consultation.
3. The new policy assists Tool 3 for the identification of the avoidance of bed rails when
required while ensuring the safety of the consumer and the implementation of risk control
measures for minimizing capable harm.
4. In Tool 4 the addition of SLS and FAQs in Tool 5 helps in providing clear guidance on
how to report the incidents of falls.
5. The flowchart used in Tool 6 has been amended with smaller changes for guiding the
process of review post-fall.
Implementation in practice
Followed by the consultation with consumers and colleagues there is a requirement of an action
plan to be implemented. The method used to implement a proper structure and planning of new
policies is in the form of a table which consists of several activities. However, several settings
6
are considered as the issue of falls is not uniformly distributed. Hence, it is essential to
reconsider the recent and basic living conditions of an older individual requiring fall preventative
approaches. It has been recognized that when older people change places it requires evidence-
based fall prevention which could be applied with the help of evidence applied within a setting
(System Performance and Service Delivery, 2016).
Community setting
Almost all the falls are due to the interaction of several risk factors such as intrinsic/extrinsic.
The early trials to prevent falls consider the identification of several risk factors followed by
their interventions. Such type of approach is efficient for older individuals at higher risk
including, the one recognized through screening questions or specific clinical factors. Another
approach is targeting one risk factor such as physical activity for balance deficit.
Hospital setting
Older individuals in the hospital are more prone to falls due to the fact that they are adjusting for
being not well, the experience of unfamiliar surroundings, reduction in self-control with more
dependency on staff. Hence, there is a requirement for the colleagues and older individuals to
adjust according to different behaviors as suggested in several randomized clinical trials (Lau et
al., 2015).
Residential care setting
The rate of falls in residential care accounts for about a case or two within six months hence
increasing the overall rate of cognitive problems, impairments, etc (Laflamme, Monárrez-Espino,
Johnell, Elling & Möller, 2015). Many evidence has been studied, however, they consist of
substantial gaps within the important areas such as recent caution around exercise in terms of an
intervention. Moreover, for particular patients, the exercise suggested by the trained
professionals is effective which is supported in a review revealing the limitation in terms of
compliance as well as acceptability which impacts the effectiveness (Finnegan, Seers & Bruce,
2019).
7
reconsider the recent and basic living conditions of an older individual requiring fall preventative
approaches. It has been recognized that when older people change places it requires evidence-
based fall prevention which could be applied with the help of evidence applied within a setting
(System Performance and Service Delivery, 2016).
Community setting
Almost all the falls are due to the interaction of several risk factors such as intrinsic/extrinsic.
The early trials to prevent falls consider the identification of several risk factors followed by
their interventions. Such type of approach is efficient for older individuals at higher risk
including, the one recognized through screening questions or specific clinical factors. Another
approach is targeting one risk factor such as physical activity for balance deficit.
Hospital setting
Older individuals in the hospital are more prone to falls due to the fact that they are adjusting for
being not well, the experience of unfamiliar surroundings, reduction in self-control with more
dependency on staff. Hence, there is a requirement for the colleagues and older individuals to
adjust according to different behaviors as suggested in several randomized clinical trials (Lau et
al., 2015).
Residential care setting
The rate of falls in residential care accounts for about a case or two within six months hence
increasing the overall rate of cognitive problems, impairments, etc (Laflamme, Monárrez-Espino,
Johnell, Elling & Möller, 2015). Many evidence has been studied, however, they consist of
substantial gaps within the important areas such as recent caution around exercise in terms of an
intervention. Moreover, for particular patients, the exercise suggested by the trained
professionals is effective which is supported in a review revealing the limitation in terms of
compliance as well as acceptability which impacts the effectiveness (Finnegan, Seers & Bruce,
2019).
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
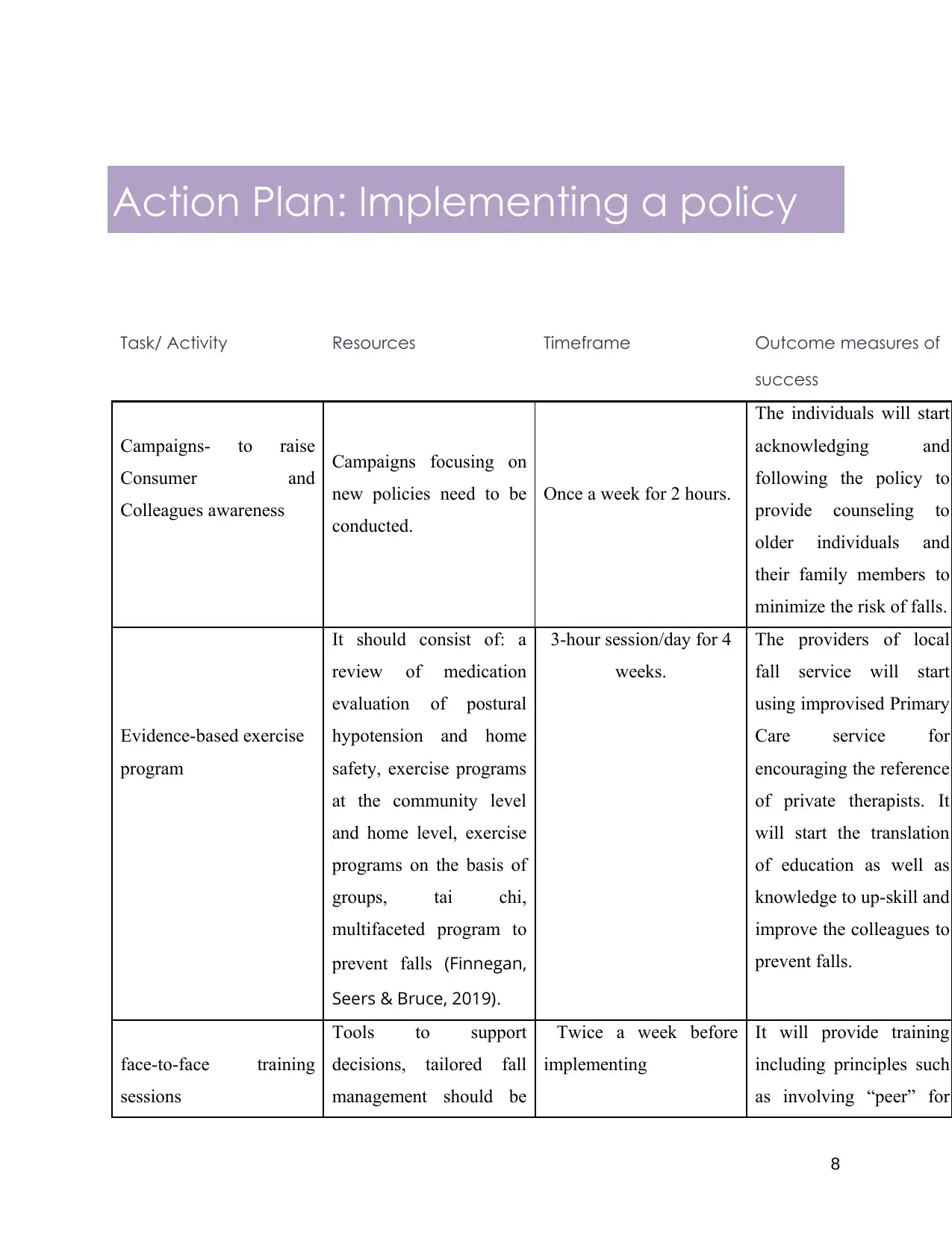
Action Plan: Implementing a policy
Task/ Activity Resources Timeframe Outcome measures of
success
Campaigns- to raise
Consumer and
Colleagues awareness
Campaigns focusing on
new policies need to be
conducted.
Once a week for 2 hours.
The individuals will start
acknowledging and
following the policy to
provide counseling to
older individuals and
their family members to
minimize the risk of falls.
Evidence-based exercise
program
It should consist of: a
review of medication
evaluation of postural
hypotension and home
safety, exercise programs
at the community level
and home level, exercise
programs on the basis of
groups, tai chi,
multifaceted program to
prevent falls (Finnegan,
Seers & Bruce, 2019).
3-hour session/day for 4
weeks.
The providers of local
fall service will start
using improvised Primary
Care service for
encouraging the reference
of private therapists. It
will start the translation
of education as well as
knowledge to up-skill and
improve the colleagues to
prevent falls.
face-to-face training
sessions
Tools to support
decisions, tailored fall
management should be
Twice a week before
implementing
It will provide training
including principles such
as involving “peer” for
8
Task/ Activity Resources Timeframe Outcome measures of
success
Campaigns- to raise
Consumer and
Colleagues awareness
Campaigns focusing on
new policies need to be
conducted.
Once a week for 2 hours.
The individuals will start
acknowledging and
following the policy to
provide counseling to
older individuals and
their family members to
minimize the risk of falls.
Evidence-based exercise
program
It should consist of: a
review of medication
evaluation of postural
hypotension and home
safety, exercise programs
at the community level
and home level, exercise
programs on the basis of
groups, tai chi,
multifaceted program to
prevent falls (Finnegan,
Seers & Bruce, 2019).
3-hour session/day for 4
weeks.
The providers of local
fall service will start
using improvised Primary
Care service for
encouraging the reference
of private therapists. It
will start the translation
of education as well as
knowledge to up-skill and
improve the colleagues to
prevent falls.
face-to-face training
sessions
Tools to support
decisions, tailored fall
management should be
Twice a week before
implementing
It will provide training
including principles such
as involving “peer” for
8
included. enabling rapport as well
as credibility for the
facilitation of behavior
change (Barker, Talevski
& Bird, 2015).
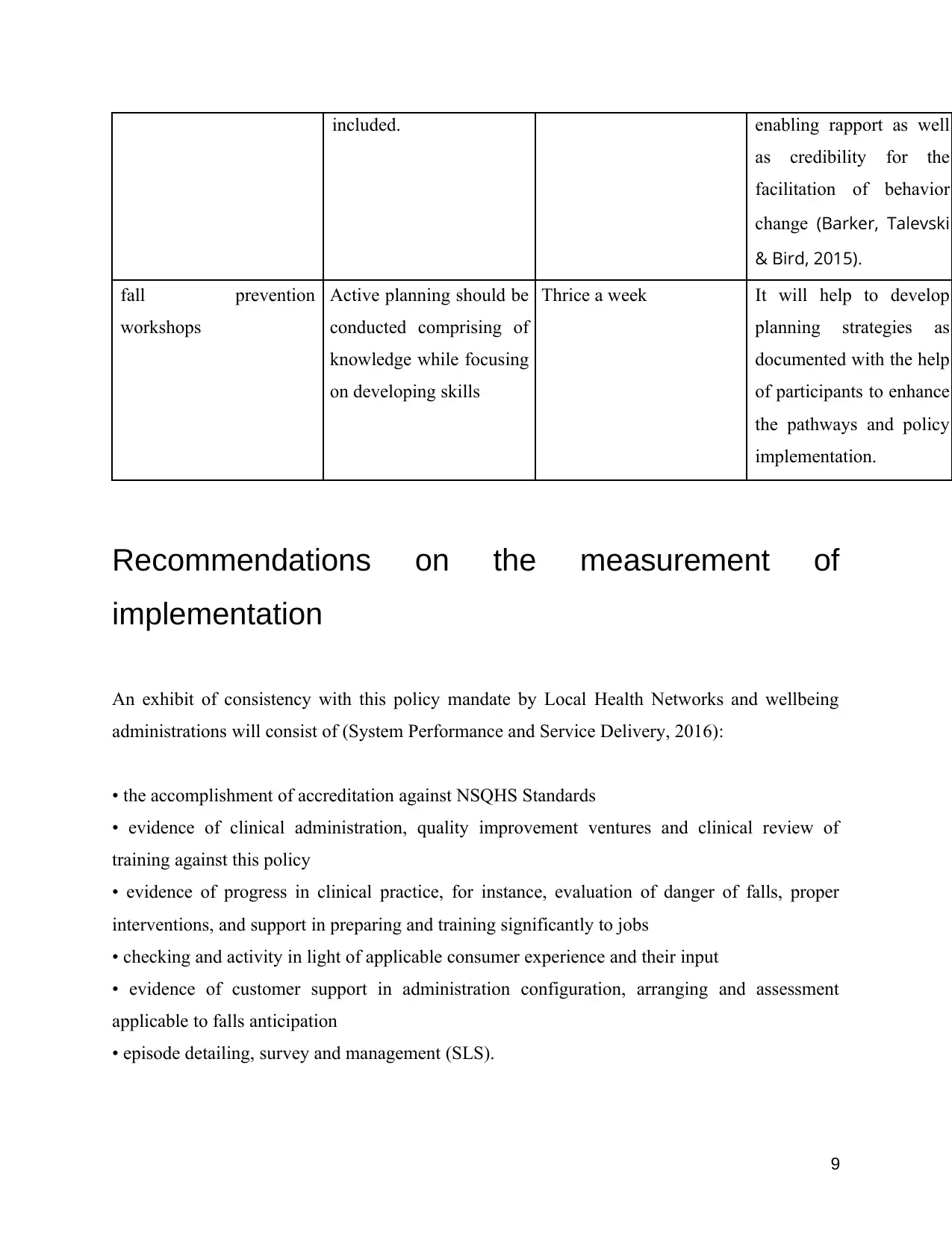
fall prevention
workshops
Active planning should be
conducted comprising of
knowledge while focusing
on developing skills
Thrice a week It will help to develop
planning strategies as
documented with the help
of participants to enhance
the pathways and policy
implementation.
Recommendations on the measurement of
implementation
An exhibit of consistency with this policy mandate by Local Health Networks and wellbeing
administrations will consist of (System Performance and Service Delivery, 2016):
• the accomplishment of accreditation against NSQHS Standards
• evidence of clinical administration, quality improvement ventures and clinical review of
training against this policy
• evidence of progress in clinical practice, for instance, evaluation of danger of falls, proper
interventions, and support in preparing and training significantly to jobs
• checking and activity in light of applicable consumer experience and their input
• evidence of customer support in administration configuration, arranging and assessment
applicable to falls anticipation
• episode detailing, survey and management (SLS).
9
as credibility for the
facilitation of behavior
change (Barker, Talevski
& Bird, 2015).
fall prevention
workshops
Active planning should be
conducted comprising of
knowledge while focusing
on developing skills
Thrice a week It will help to develop
planning strategies as
documented with the help
of participants to enhance
the pathways and policy
implementation.
Recommendations on the measurement of
implementation
An exhibit of consistency with this policy mandate by Local Health Networks and wellbeing
administrations will consist of (System Performance and Service Delivery, 2016):
• the accomplishment of accreditation against NSQHS Standards
• evidence of clinical administration, quality improvement ventures and clinical review of
training against this policy
• evidence of progress in clinical practice, for instance, evaluation of danger of falls, proper
interventions, and support in preparing and training significantly to jobs
• checking and activity in light of applicable consumer experience and their input
• evidence of customer support in administration configuration, arranging and assessment
applicable to falls anticipation
• episode detailing, survey and management (SLS).
9
Conclusion
The new policy has opened entryways for a few creative thoughts in regard to falls prevention.
The examination given by the investigation has featured the significance of help and advising for
falls prevention and its further outcomes. The paper thinks about the dynamic cooperation of the
relatives and carers of older people at risk of falls for giving help and directing to them. This new
arrangement has been very helpful in improving the physical and mental condition of older
individuals. Another methodology examined in the paper for falls avoidance is intently checking
the customer and limiting further dangers. The further dangers and results to the patients at risk
of falls are limited by evaluating their degree of torment, limiting their likelihood to fall by
utilizing the physical restrictions such as bed rails, giving help to the old having visual and
hearing weakness and by giving a safe condition. The definition of such a policy has prompted a
discourse among the healthcare staff. This new approach is anything but difficult to actualize. So
further research ought to be finished with respect to the arrangement of psychosocial support to
the patients at risk of falls to prevent falls.
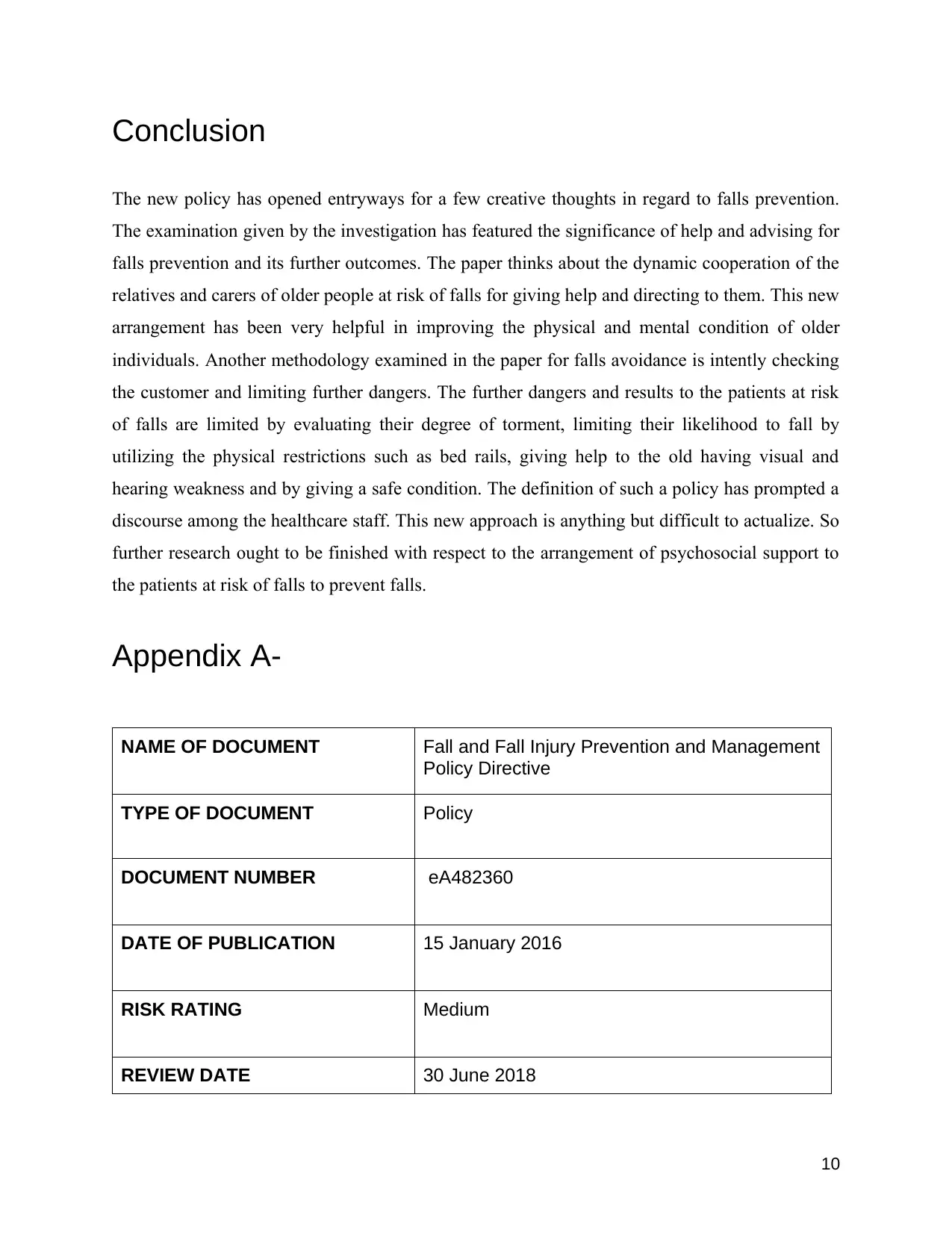
Appendix A-
NAME OF DOCUMENT Fall and Fall Injury Prevention and Management
Policy Directive
TYPE OF DOCUMENT Policy
DOCUMENT NUMBER eA482360
DATE OF PUBLICATION 15 January 2016
RISK RATING Medium
REVIEW DATE 30 June 2018
10
The new policy has opened entryways for a few creative thoughts in regard to falls prevention.
The examination given by the investigation has featured the significance of help and advising for
falls prevention and its further outcomes. The paper thinks about the dynamic cooperation of the
relatives and carers of older people at risk of falls for giving help and directing to them. This new
arrangement has been very helpful in improving the physical and mental condition of older
individuals. Another methodology examined in the paper for falls avoidance is intently checking
the customer and limiting further dangers. The further dangers and results to the patients at risk
of falls are limited by evaluating their degree of torment, limiting their likelihood to fall by
utilizing the physical restrictions such as bed rails, giving help to the old having visual and
hearing weakness and by giving a safe condition. The definition of such a policy has prompted a
discourse among the healthcare staff. This new approach is anything but difficult to actualize. So
further research ought to be finished with respect to the arrangement of psychosocial support to
the patients at risk of falls to prevent falls.
Appendix A-
NAME OF DOCUMENT Fall and Fall Injury Prevention and Management
Policy Directive
TYPE OF DOCUMENT Policy
DOCUMENT NUMBER eA482360
DATE OF PUBLICATION 15 January 2016
RISK RATING Medium
REVIEW DATE 30 June 2018
10
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
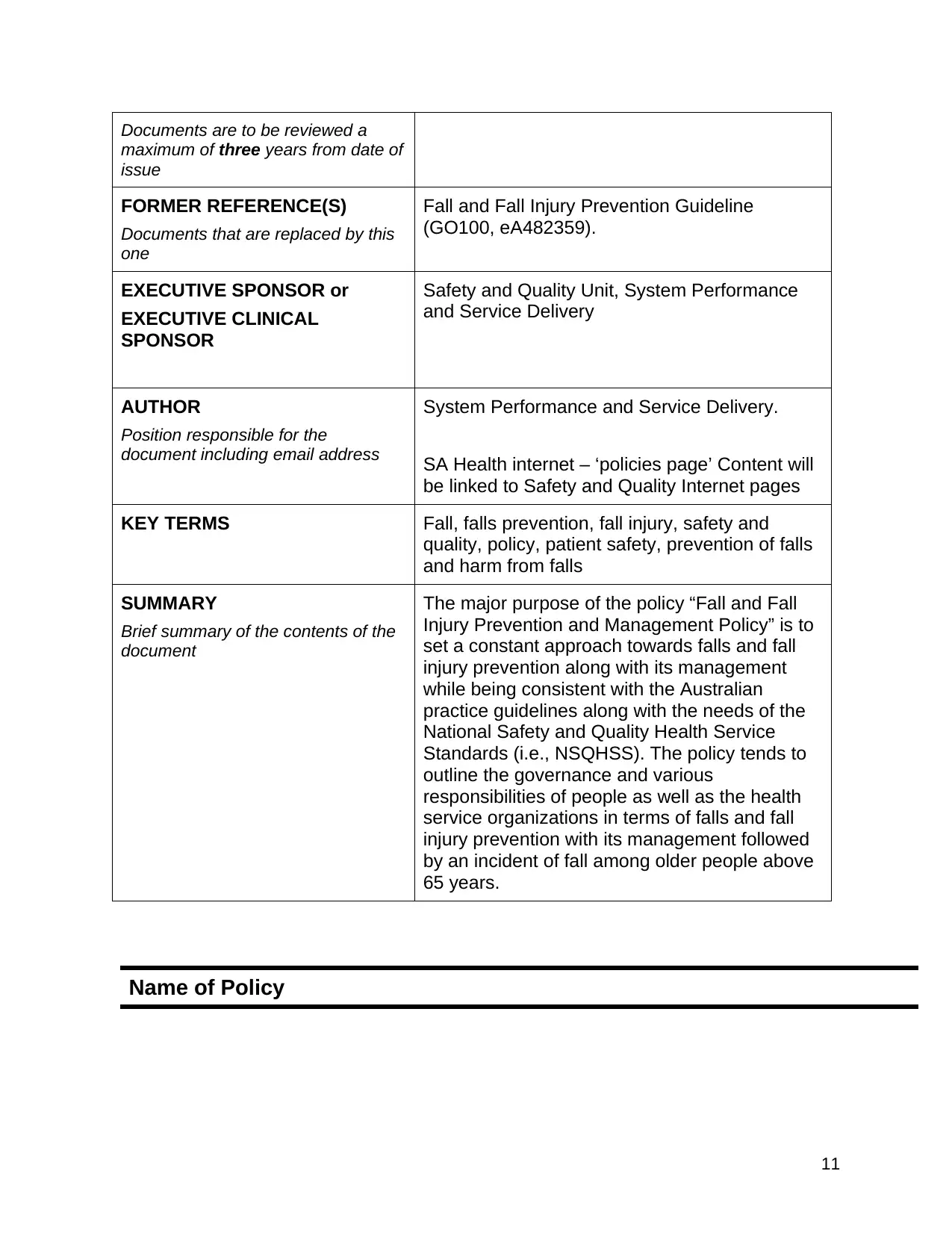
Documents are to be reviewed a
maximum of three years from date of
issue
FORMER REFERENCE(S)
Documents that are replaced by this
one
Fall and Fall Injury Prevention Guideline
(GO100, eA482359).
EXECUTIVE SPONSOR or
EXECUTIVE CLINICAL
SPONSOR
Safety and Quality Unit, System Performance
and Service Delivery
AUTHOR
Position responsible for the
document including email address
System Performance and Service Delivery.
SA Health internet – ‘policies page’ Content will
be linked to Safety and Quality Internet pages
KEY TERMS Fall, falls prevention, fall injury, safety and
quality, policy, patient safety, prevention of falls
and harm from falls
SUMMARY
Brief summary of the contents of the
document
The major purpose of the policy “Fall and Fall
Injury Prevention and Management Policy” is to
set a constant approach towards falls and fall
injury prevention along with its management
while being consistent with the Australian
practice guidelines along with the needs of the
National Safety and Quality Health Service
Standards (i.e., NSQHSS). The policy tends to
outline the governance and various
responsibilities of people as well as the health
service organizations in terms of falls and fall
injury prevention with its management followed
by an incident of fall among older people above
65 years.
Name of Policy
11
maximum of three years from date of
issue
FORMER REFERENCE(S)
Documents that are replaced by this
one
Fall and Fall Injury Prevention Guideline
(GO100, eA482359).
EXECUTIVE SPONSOR or
EXECUTIVE CLINICAL
SPONSOR
Safety and Quality Unit, System Performance
and Service Delivery
AUTHOR
Position responsible for the
document including email address
System Performance and Service Delivery.
SA Health internet – ‘policies page’ Content will
be linked to Safety and Quality Internet pages
KEY TERMS Fall, falls prevention, fall injury, safety and
quality, policy, patient safety, prevention of falls
and harm from falls
SUMMARY
Brief summary of the contents of the
document
The major purpose of the policy “Fall and Fall
Injury Prevention and Management Policy” is to
set a constant approach towards falls and fall
injury prevention along with its management
while being consistent with the Australian
practice guidelines along with the needs of the
National Safety and Quality Health Service
Standards (i.e., NSQHSS). The policy tends to
outline the governance and various
responsibilities of people as well as the health
service organizations in terms of falls and fall
injury prevention with its management followed
by an incident of fall among older people above
65 years.
Name of Policy
11
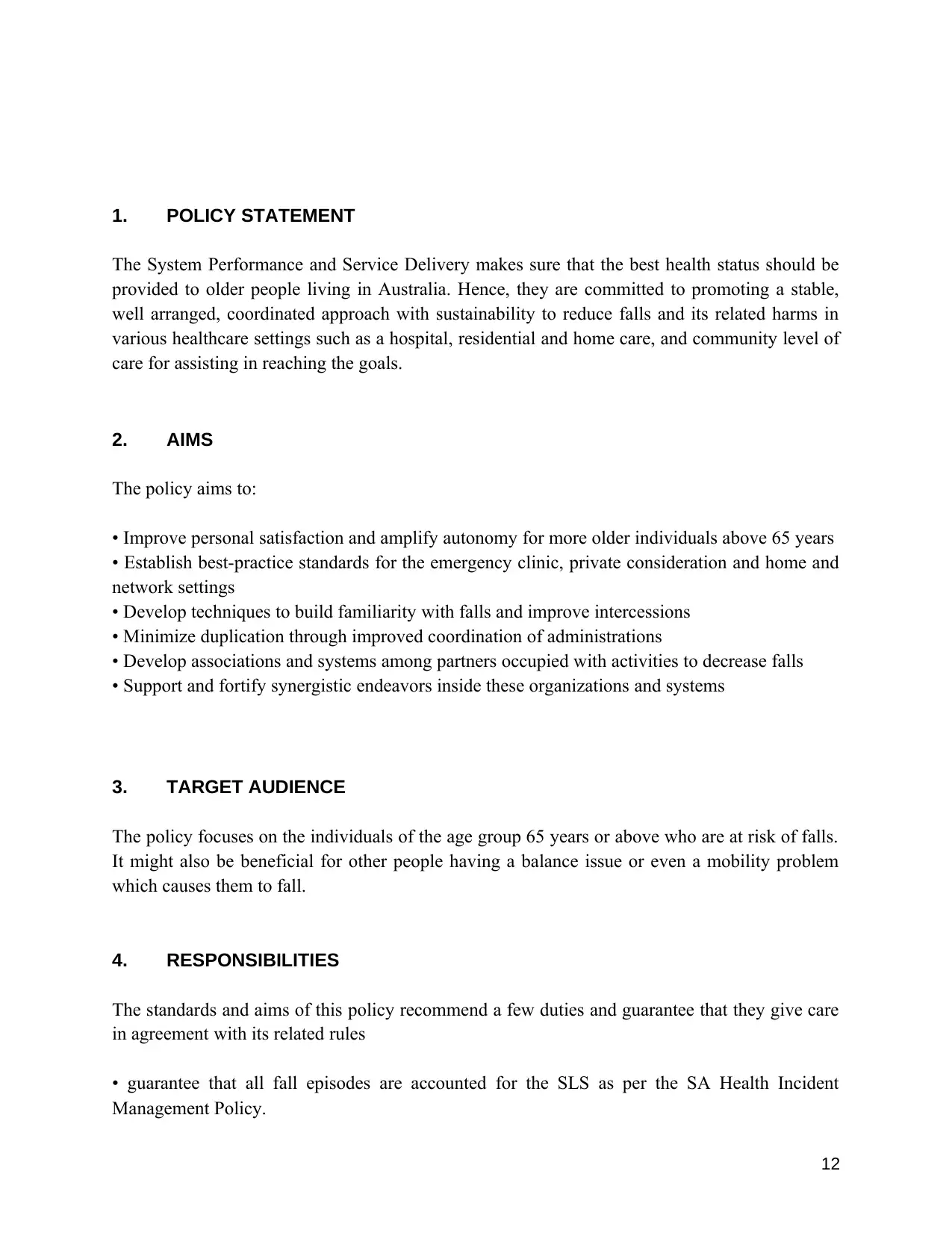
1. POLICY STATEMENT
The System Performance and Service Delivery makes sure that the best health status should be
provided to older people living in Australia. Hence, they are committed to promoting a stable,
well arranged, coordinated approach with sustainability to reduce falls and its related harms in
various healthcare settings such as a hospital, residential and home care, and community level of
care for assisting in reaching the goals.
2. AIMS
The policy aims to:
• Improve personal satisfaction and amplify autonomy for more older individuals above 65 years
• Establish best-practice standards for the emergency clinic, private consideration and home and
network settings
• Develop techniques to build familiarity with falls and improve intercessions
• Minimize duplication through improved coordination of administrations
• Develop associations and systems among partners occupied with activities to decrease falls
• Support and fortify synergistic endeavors inside these organizations and systems
3. TARGET AUDIENCE
The policy focuses on the individuals of the age group 65 years or above who are at risk of falls.
It might also be beneficial for other people having a balance issue or even a mobility problem
which causes them to fall.
4. RESPONSIBILITIES
The standards and aims of this policy recommend a few duties and guarantee that they give care
in agreement with its related rules
• guarantee that all fall episodes are accounted for the SLS as per the SA Health Incident
Management Policy.
12
The System Performance and Service Delivery makes sure that the best health status should be
provided to older people living in Australia. Hence, they are committed to promoting a stable,
well arranged, coordinated approach with sustainability to reduce falls and its related harms in
various healthcare settings such as a hospital, residential and home care, and community level of
care for assisting in reaching the goals.
2. AIMS
The policy aims to:
• Improve personal satisfaction and amplify autonomy for more older individuals above 65 years
• Establish best-practice standards for the emergency clinic, private consideration and home and
network settings
• Develop techniques to build familiarity with falls and improve intercessions
• Minimize duplication through improved coordination of administrations
• Develop associations and systems among partners occupied with activities to decrease falls
• Support and fortify synergistic endeavors inside these organizations and systems
3. TARGET AUDIENCE
The policy focuses on the individuals of the age group 65 years or above who are at risk of falls.
It might also be beneficial for other people having a balance issue or even a mobility problem
which causes them to fall.
4. RESPONSIBILITIES
The standards and aims of this policy recommend a few duties and guarantee that they give care
in agreement with its related rules
• guarantee that all fall episodes are accounted for the SLS as per the SA Health Incident
Management Policy.
12
• take an interest in education or training or preparing to guarantee that they have learning and
aptitudes pertinent to their job in keeping falls and damage from falls.
5. DEFINITIONS
fall: an occasion which results in an individual stopping coincidentally on the ground or floor or
other lower level.
6. DOCUMENTATION
Tool 3-6 (Appendix- B)
7. REFERENCES
Barker, A., Talevski, J., & Bird, M. (2015). Effect of pilates exercise for improving balance
and decreasing falls risk in older adults: a systematic review with meta-analysis.
Physiotherapy, 101, e111-e112. doi: 10.1016/j.physio.2015.03.249
Clemson, L., Mackenzie, L., Roberts, C., Poulos, R., Tan, A., & Lovarini, M. et al. (2017).
Integrated solutions for sustainable fall prevention in primary care, the iSOLVE
project: a type 2 hybrid effectiveness-implementation design. Implementation Science,
12(1). doi: 10.1186/s13012-016-0529-9
Dapp, U., Anders, J., Suijker, J., & Bjorkman, M. (2014). SS3.04: Various aspects of
interventions on physical functioning in community dwelling older persons. European
Geriatric Medicine, 5, S26-S27. doi: 10.1016/s1878-7649(14)70060-9
Day, L., Finch, C., Hill, K., Haines, T., Clemson, L., Thomas, M., & Thompson, C. (2010).
A protocol for evidence-based targeting and evaluation of statewide strategies for
preventing falls among community-dwelling older people in Victoria, Australia. Injury
Prevention, 17(2), e3-e3. doi: 10.1136/ip.2010.030775
Finnegan, S., Seers, K., & Bruce, J. (2019). Long-term follow-up of exercise interventions
for preventing falls in older people living in the community: a systematic review and
meta-analysis. Physiotherapy, 105, e132-e133. doi: 10.1016/j.physio.2018.11.123
İyigün, G., Can, F., Kırmızıgil, B., Angın, E., Öksüz, S., & Malkoç, M. (2016). The
comparison of different level of cognitive impairment on falls and fall risks in
community dwelling older adults. Physiotherapy, 102, e171-e172. doi:
10.1016/j.physio.2016.10.203
Laflamme, L., Monárrez-Espino, J., Johnell, K., Elling, B., & Möller, J. (2015). Type,
Number or Both? A Population-Based Matched Case-Control Study on the Risk of Fall
13
aptitudes pertinent to their job in keeping falls and damage from falls.
5. DEFINITIONS
fall: an occasion which results in an individual stopping coincidentally on the ground or floor or
other lower level.
6. DOCUMENTATION
Tool 3-6 (Appendix- B)
7. REFERENCES
Barker, A., Talevski, J., & Bird, M. (2015). Effect of pilates exercise for improving balance
and decreasing falls risk in older adults: a systematic review with meta-analysis.
Physiotherapy, 101, e111-e112. doi: 10.1016/j.physio.2015.03.249
Clemson, L., Mackenzie, L., Roberts, C., Poulos, R., Tan, A., & Lovarini, M. et al. (2017).
Integrated solutions for sustainable fall prevention in primary care, the iSOLVE
project: a type 2 hybrid effectiveness-implementation design. Implementation Science,
12(1). doi: 10.1186/s13012-016-0529-9
Dapp, U., Anders, J., Suijker, J., & Bjorkman, M. (2014). SS3.04: Various aspects of
interventions on physical functioning in community dwelling older persons. European
Geriatric Medicine, 5, S26-S27. doi: 10.1016/s1878-7649(14)70060-9
Day, L., Finch, C., Hill, K., Haines, T., Clemson, L., Thomas, M., & Thompson, C. (2010).
A protocol for evidence-based targeting and evaluation of statewide strategies for
preventing falls among community-dwelling older people in Victoria, Australia. Injury
Prevention, 17(2), e3-e3. doi: 10.1136/ip.2010.030775
Finnegan, S., Seers, K., & Bruce, J. (2019). Long-term follow-up of exercise interventions
for preventing falls in older people living in the community: a systematic review and
meta-analysis. Physiotherapy, 105, e132-e133. doi: 10.1016/j.physio.2018.11.123
İyigün, G., Can, F., Kırmızıgil, B., Angın, E., Öksüz, S., & Malkoç, M. (2016). The
comparison of different level of cognitive impairment on falls and fall risks in
community dwelling older adults. Physiotherapy, 102, e171-e172. doi:
10.1016/j.physio.2016.10.203
Laflamme, L., Monárrez-Espino, J., Johnell, K., Elling, B., & Möller, J. (2015). Type,
Number or Both? A Population-Based Matched Case-Control Study on the Risk of Fall
13
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Injuries among Older People and Number of Medications beyond Fall-Inducing Drugs.
PLOS ONE, 10(3), e0123390. doi: 10.1371/journal.pone.0123390
Lau, R., Stevenson, F., Ong, B., Dziedzic, K., Treweek, S., & Eldridge, S. et al. (2015).
Achieving change in primary care—effectiveness of strategies for improving
implementation of complex interventions: systematic review of reviews. BMJ Open,
5(12), e009993. doi: 10.1136/bmjopen-2015-009993
Martins, A., Andrade, S., & Santos, D. (2015). Screening and assessment of the risk of fall
—an initiative to prevent falls in community dwelling older adults. Physiotherapy, 101,
e958. doi: 10.1016/j.physio.2015.03.1811
System Performance and Service Delivery. (2016). Policy Directive: compliance is
mandatory Fall and Fall Injury Prevention and Management Policy Directive [Ebook].
South Australia: Department for Health and Ageing. Retrieved from
https://www.sahealth.sa.gov.au/wps/wcm/connect/8acea4004654c05ab1a9fb2e504170d
4/Directive_Fall+%26+Fall+Injury+Prevention+%26+Management+PD+
%26+Toolkit_Dec2015.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-
8acea4004654c05ab1a9fb2e504170d4-mMz0WJ6
Taylor-Piliae, R., Peterson, R., & Mohler, M. (2017). Clinical and Community Strategies to
Prevent Falls and Fall-Related Injuries Among Community-Dwelling Older Adults.
Nursing Clinics Of North America, 52(3), 489-497. doi: 10.1016/j.cnur.2017.04.004
Warner Frieson, C. (2016). Predictors of Recurrent Falls in Community-Dwelling Older
Adults after Fall- Related Hip Fracture. Journal Of Perioperative & Critical Intensive
Care Nursing, 2(2). doi: 10.4172/2471-9870.1000e107
8. REVISION & APPROVAL HISTORY
Date Revision No. Author and Approval
15/01/2016 V3 Portfolio Executive
Appendix B
Tool 3:
14
PLOS ONE, 10(3), e0123390. doi: 10.1371/journal.pone.0123390
Lau, R., Stevenson, F., Ong, B., Dziedzic, K., Treweek, S., & Eldridge, S. et al. (2015).
Achieving change in primary care—effectiveness of strategies for improving
implementation of complex interventions: systematic review of reviews. BMJ Open,
5(12), e009993. doi: 10.1136/bmjopen-2015-009993
Martins, A., Andrade, S., & Santos, D. (2015). Screening and assessment of the risk of fall
—an initiative to prevent falls in community dwelling older adults. Physiotherapy, 101,
e958. doi: 10.1016/j.physio.2015.03.1811
System Performance and Service Delivery. (2016). Policy Directive: compliance is
mandatory Fall and Fall Injury Prevention and Management Policy Directive [Ebook].
South Australia: Department for Health and Ageing. Retrieved from
https://www.sahealth.sa.gov.au/wps/wcm/connect/8acea4004654c05ab1a9fb2e504170d
4/Directive_Fall+%26+Fall+Injury+Prevention+%26+Management+PD+
%26+Toolkit_Dec2015.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-
8acea4004654c05ab1a9fb2e504170d4-mMz0WJ6
Taylor-Piliae, R., Peterson, R., & Mohler, M. (2017). Clinical and Community Strategies to
Prevent Falls and Fall-Related Injuries Among Community-Dwelling Older Adults.
Nursing Clinics Of North America, 52(3), 489-497. doi: 10.1016/j.cnur.2017.04.004
Warner Frieson, C. (2016). Predictors of Recurrent Falls in Community-Dwelling Older
Adults after Fall- Related Hip Fracture. Journal Of Perioperative & Critical Intensive
Care Nursing, 2(2). doi: 10.4172/2471-9870.1000e107
8. REVISION & APPROVAL HISTORY
Date Revision No. Author and Approval
15/01/2016 V3 Portfolio Executive
Appendix B
Tool 3:
14
Tool 4: SLS
Tool 5:
15
Tool 5:
15
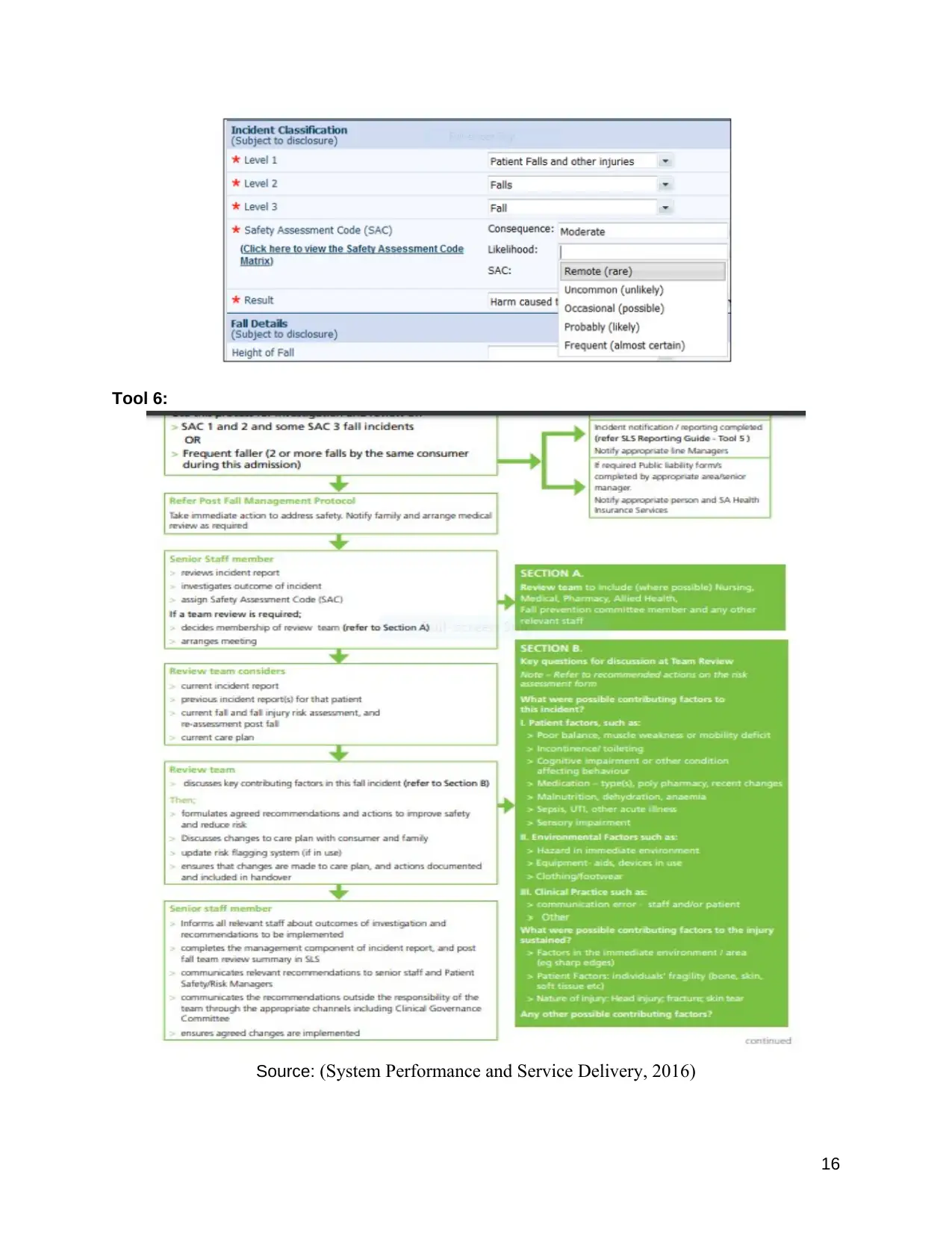
Tool 6:
Source: (System Performance and Service Delivery, 2016)
16
Source: (System Performance and Service Delivery, 2016)
16
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.

17
1 out of 17
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.