Public Health Leadership and Cardiovascular Disease Prevention
VerifiedAdded on 2021/04/21
|16
|4734
|164
AI Summary
This assignment provides a comprehensive review of public health leadership and its role in preventing cardiovascular disease. It examines the impact of salt reduction initiatives, minimum unit pricing policies, and other interventions on cardiovascular health outcomes. The assignment draws on research from various countries, including England, Australia, and Scotland, to highlight best practices and strategies for effective public health leadership.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
Contemporary themes in health care level 6
Name of the student:
Name of the University:
Author’s note
Contemporary themes in health care level 6
Name of the student:
Name of the University:
Author’s note
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
Identify the six articles for the essay:
Journal References:
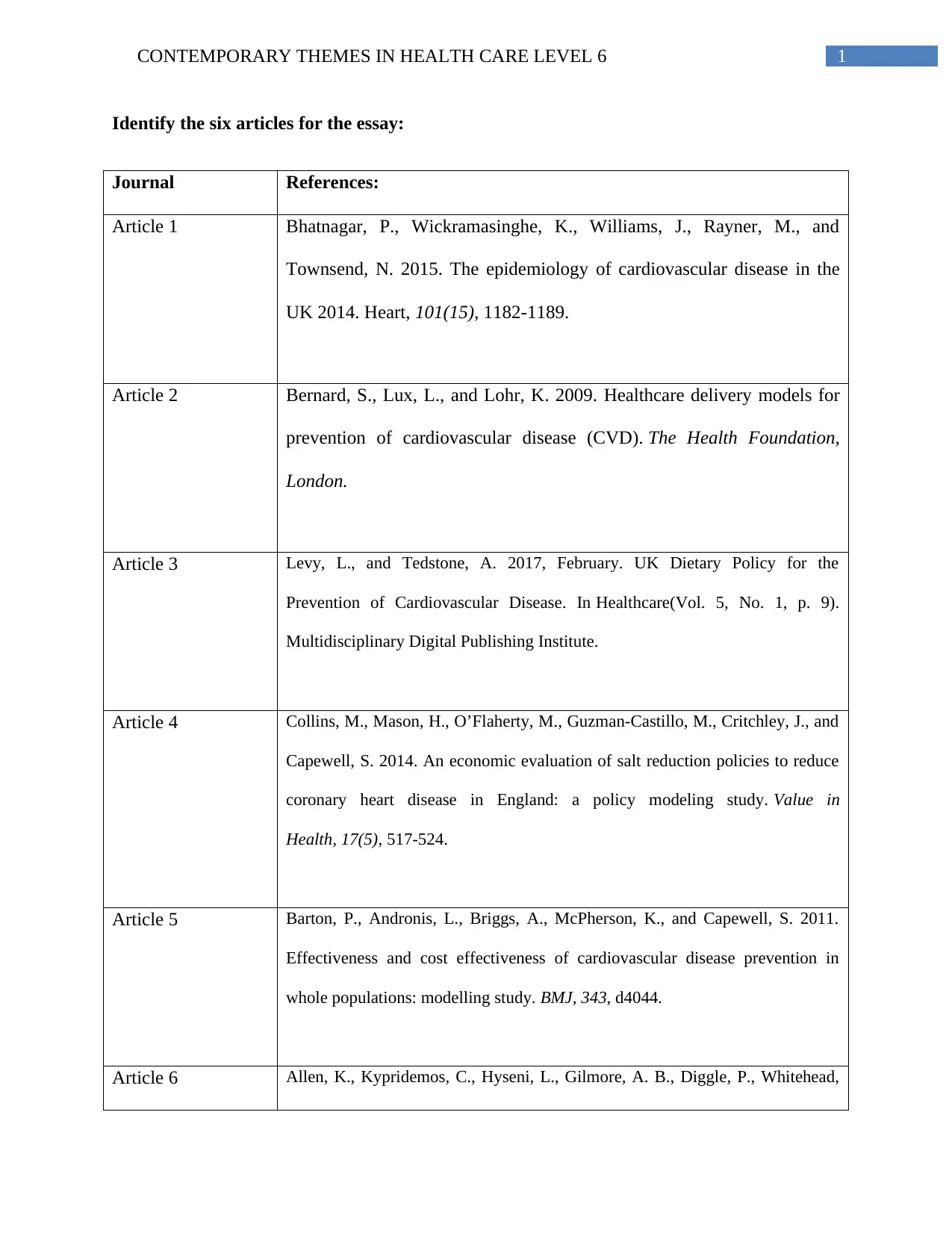
Article 1 Bhatnagar, P., Wickramasinghe, K., Williams, J., Rayner, M., and
Townsend, N. 2015. The epidemiology of cardiovascular disease in the
UK 2014. Heart, 101(15), 1182-1189.
Article 2 Bernard, S., Lux, L., and Lohr, K. 2009. Healthcare delivery models for
prevention of cardiovascular disease (CVD). The Health Foundation,
London.
Article 3 Levy, L., and Tedstone, A. 2017, February. UK Dietary Policy for the
Prevention of Cardiovascular Disease. In Healthcare(Vol. 5, No. 1, p. 9).
Multidisciplinary Digital Publishing Institute.
Article 4 Collins, M., Mason, H., O’Flaherty, M., Guzman-Castillo, M., Critchley, J., and
Capewell, S. 2014. An economic evaluation of salt reduction policies to reduce
coronary heart disease in England: a policy modeling study. Value in
Health, 17(5), 517-524.
Article 5 Barton, P., Andronis, L., Briggs, A., McPherson, K., and Capewell, S. 2011.
Effectiveness and cost effectiveness of cardiovascular disease prevention in
whole populations: modelling study. BMJ, 343, d4044.
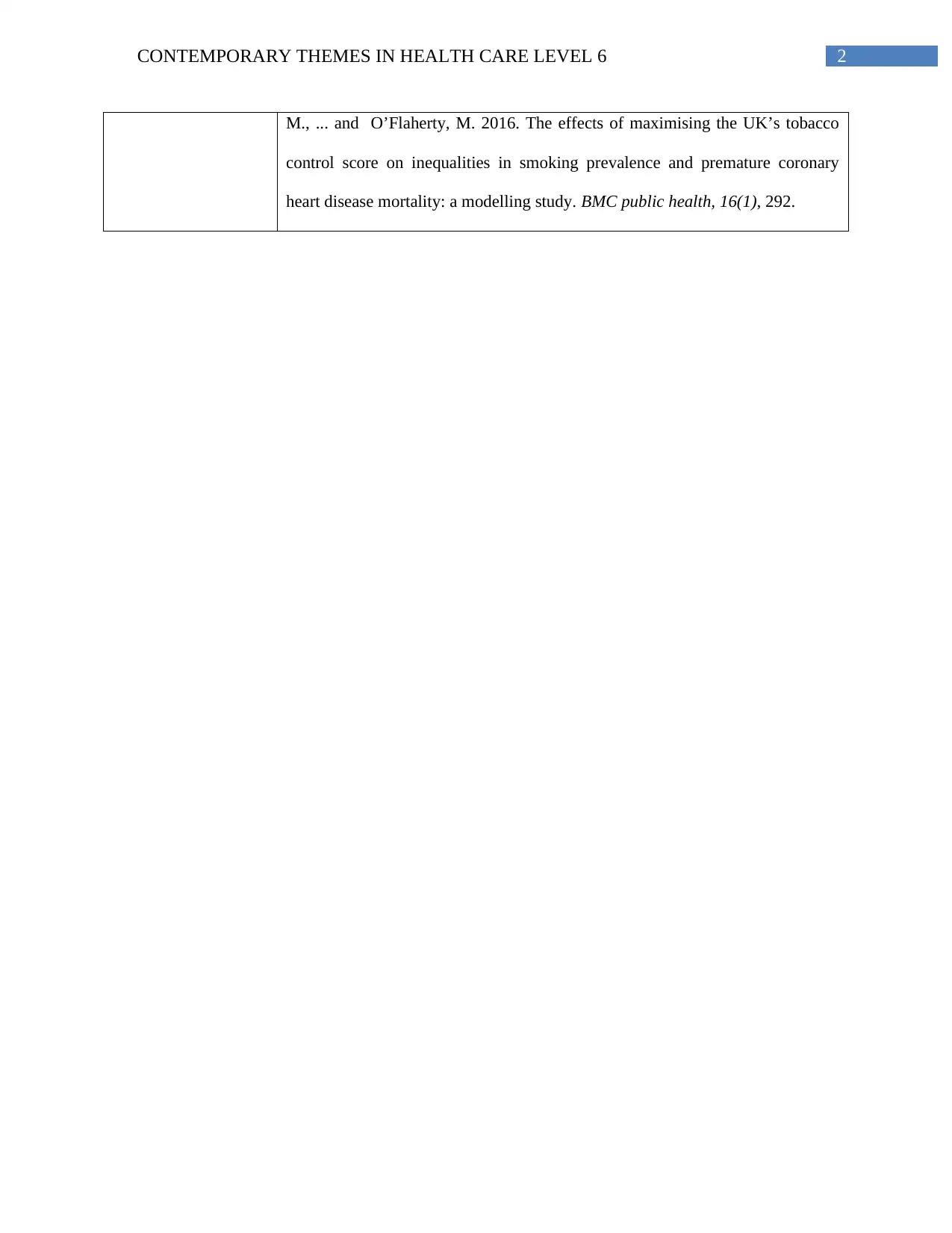
Article 6 Allen, K., Kypridemos, C., Hyseni, L., Gilmore, A. B., Diggle, P., Whitehead,
Identify the six articles for the essay:
Journal References:
Article 1 Bhatnagar, P., Wickramasinghe, K., Williams, J., Rayner, M., and
Townsend, N. 2015. The epidemiology of cardiovascular disease in the
UK 2014. Heart, 101(15), 1182-1189.
Article 2 Bernard, S., Lux, L., and Lohr, K. 2009. Healthcare delivery models for
prevention of cardiovascular disease (CVD). The Health Foundation,
London.
Article 3 Levy, L., and Tedstone, A. 2017, February. UK Dietary Policy for the
Prevention of Cardiovascular Disease. In Healthcare(Vol. 5, No. 1, p. 9).
Multidisciplinary Digital Publishing Institute.
Article 4 Collins, M., Mason, H., O’Flaherty, M., Guzman-Castillo, M., Critchley, J., and
Capewell, S. 2014. An economic evaluation of salt reduction policies to reduce
coronary heart disease in England: a policy modeling study. Value in
Health, 17(5), 517-524.
Article 5 Barton, P., Andronis, L., Briggs, A., McPherson, K., and Capewell, S. 2011.
Effectiveness and cost effectiveness of cardiovascular disease prevention in
whole populations: modelling study. BMJ, 343, d4044.
Article 6 Allen, K., Kypridemos, C., Hyseni, L., Gilmore, A. B., Diggle, P., Whitehead,
2CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
M., ... and O’Flaherty, M. 2016. The effects of maximising the UK’s tobacco
control score on inequalities in smoking prevalence and premature coronary
heart disease mortality: a modelling study. BMC public health, 16(1), 292.
M., ... and O’Flaherty, M. 2016. The effects of maximising the UK’s tobacco
control score on inequalities in smoking prevalence and premature coronary
heart disease mortality: a modelling study. BMC public health, 16(1), 292.
3CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
Introduction
The mortality and mortality associated with cardiovascular disease (CVD) is increasing
globally. CVD is regarded as the number 1 cause of death globally. The review of latest 2015
global CVD death statistics suggest about 17.7 million death caused due to CVD. This means
that CVD was the reason for about 31% of global death. CVD is an umbrella term for different
types of heart disease and coronary heart disease is one of the major type of CVD, which has
caused about 7.4 million deaths in 2015 (World Health Organization 2015). Hence, from this
statistics, it is understood that coronary heart disease (CHD) significantly contributes to total
deaths globally. The CVD related deaths caused in UK is also alarming as latest reports have
shown that CVD causes more than 25% of all deaths in UK and about 7 million people are living
with the disease in UK. Among CVDs, CHD has been found to be the leading cause of death in
UK (Bhf.org.uk. 2016). Considering such prevalence of coronary heart disease in UK, the main
purpose of this essay is to identify six articles related to the incidence and management of
CHD in UK and explore in depth about the ways in which the disease was managed. The
paper also explores range of framework, policy approach and intervention that can be effective in
reducing the risk of CHD in UK. After the evaluation of the articles, the paper also proposes a
recommendation for the health care system of UK to reduce the incidence of CHD in UK.
Argument/main body:
To get an understanding about different management strategies and models or
frameworks implemented in UK for the management of CHD in UK, six academic articles have
been chosen for analysis. The summary of the six articles has been presented in this section.
The first article by Bhatnagar et al. (2015) gives an insight about the prevalence rate of coronary
Introduction
The mortality and mortality associated with cardiovascular disease (CVD) is increasing
globally. CVD is regarded as the number 1 cause of death globally. The review of latest 2015
global CVD death statistics suggest about 17.7 million death caused due to CVD. This means
that CVD was the reason for about 31% of global death. CVD is an umbrella term for different
types of heart disease and coronary heart disease is one of the major type of CVD, which has
caused about 7.4 million deaths in 2015 (World Health Organization 2015). Hence, from this
statistics, it is understood that coronary heart disease (CHD) significantly contributes to total
deaths globally. The CVD related deaths caused in UK is also alarming as latest reports have
shown that CVD causes more than 25% of all deaths in UK and about 7 million people are living
with the disease in UK. Among CVDs, CHD has been found to be the leading cause of death in
UK (Bhf.org.uk. 2016). Considering such prevalence of coronary heart disease in UK, the main
purpose of this essay is to identify six articles related to the incidence and management of
CHD in UK and explore in depth about the ways in which the disease was managed. The
paper also explores range of framework, policy approach and intervention that can be effective in
reducing the risk of CHD in UK. After the evaluation of the articles, the paper also proposes a
recommendation for the health care system of UK to reduce the incidence of CHD in UK.
Argument/main body:
To get an understanding about different management strategies and models or
frameworks implemented in UK for the management of CHD in UK, six academic articles have
been chosen for analysis. The summary of the six articles has been presented in this section.
The first article by Bhatnagar et al. (2015) gives an insight about the prevalence rate of coronary
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
heart disease in UK. The article mainly provides up to date statistics on mortality, prevalence and
cost associated with CVD in UK. The prevalence of coronary heart disease is found the highest
in North of England and Scotland. The articles also cover regional variations in mortality,
prevalence and inpatient episodes related to CVD. The second article by Bernard, Lux and Lohr
(2009) mainly covers the theme of different health care delivery models available in UK for the
management heart diseases like CHD. The article mainly summarizes about CVD care delivery
models starting from prevention work to palliative care and more detailed insight about care for
CVD in prevention and primary care setting in UK. This article can be useful in understanding
the preventive and primary care practices that helped to identify unknown case of CHD in UK.
In relation to government policies for the management of risk factors related to CHD, two
articles has been found to cover in details about policies related to heart disease prevention. The
third article by Levy and Tedstone (2017, February) covers the theme of UK dietary policies for
prevention of heart disease. From the review of this article, the UK government recommendation
in relation to energy intake, salt intake, fruits and vegetable consumption, saturated fat
consumption and level of oily fish and fiber needed for citizens is covered. The dietary advice
has been integrated with Eatwell guide to support people to understand proper diet needed to
improve health and cardiovascular health. In addition, the fourth article by Collins et al. (2014)
provides detail insight related to implication of salt reduction policies in reducing the prevalence
of coronary heart disease in England. The review of this evidence strengthens the idea about the
way in which heart disease policy are modeled in UK and policy is analyzes by means of cost
effectiveness analysis, uncertainty analysis and sensitivity analysis.
The details related to cost effectiveness of population wide risk factor reduction
programme targeting heart disease like CHD in England has been covered by Barton et al.
heart disease in UK. The article mainly provides up to date statistics on mortality, prevalence and
cost associated with CVD in UK. The prevalence of coronary heart disease is found the highest
in North of England and Scotland. The articles also cover regional variations in mortality,
prevalence and inpatient episodes related to CVD. The second article by Bernard, Lux and Lohr
(2009) mainly covers the theme of different health care delivery models available in UK for the
management heart diseases like CHD. The article mainly summarizes about CVD care delivery
models starting from prevention work to palliative care and more detailed insight about care for
CVD in prevention and primary care setting in UK. This article can be useful in understanding
the preventive and primary care practices that helped to identify unknown case of CHD in UK.
In relation to government policies for the management of risk factors related to CHD, two
articles has been found to cover in details about policies related to heart disease prevention. The
third article by Levy and Tedstone (2017, February) covers the theme of UK dietary policies for
prevention of heart disease. From the review of this article, the UK government recommendation
in relation to energy intake, salt intake, fruits and vegetable consumption, saturated fat
consumption and level of oily fish and fiber needed for citizens is covered. The dietary advice
has been integrated with Eatwell guide to support people to understand proper diet needed to
improve health and cardiovascular health. In addition, the fourth article by Collins et al. (2014)
provides detail insight related to implication of salt reduction policies in reducing the prevalence
of coronary heart disease in England. The review of this evidence strengthens the idea about the
way in which heart disease policy are modeled in UK and policy is analyzes by means of cost
effectiveness analysis, uncertainty analysis and sensitivity analysis.
The details related to cost effectiveness of population wide risk factor reduction
programme targeting heart disease like CHD in England has been covered by Barton et al.
5CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
(2011). The generic economic model is the main theoretical framework that determines the way
in which specific risk factor reduction programs decreases the trends related to incidence of
heart disease. Smoking has been found to be a major risk factor of coronary heart disease and
the sixth article by Allen et al. (2016) focused on evaluating the impact of tobacco control
strategies on reducing inequalities related to smoking prevalence and premature mortality due to
CHD. The strength of tobacco control policies in reducing one of the major risk factor of CHD is
understood from this academic article.
It is necessary to evaluate theories and management practices presented in the
article selected for the paper. The first article provides an insight into the 19th edition of the
Cardiovascular Disease Statistics 2014 report. The burden of CVD, CHD and stroke in UK was
presented by means of detail on mortality, treatment cost and morbidity. The mortality data
suggested that improvement in mortality rate was achieved in 2012 as it became the second
leading cause of death compared to being the first leading cause of death previously (Bhatnagar
et al. 2015). However, gender based disparities in CVD outcome was seen as the report showed
that CVD remained the leading cause for death for women. In addition, regional variations in
mortality were also found as higher mortality was found in North England compared to South
England. Hence, the article highlighted the issue of health inequality, however how leadership
can play a role in advancing health equity and eliminating health disparities was not covered.
The article by Graci and Ruffin, (2014) emphasized that certain agencies drive leadership
and coordination process for eliminating health disparities. Hence, effective public health
leadership can be one source to address inequalities related to incidence of CHD. From this
perspective, the transformational leadership can address problem related to CHD in UK. This is
said informed by the theoretical aspects of transformational leadership. The theory suggests that
(2011). The generic economic model is the main theoretical framework that determines the way
in which specific risk factor reduction programs decreases the trends related to incidence of
heart disease. Smoking has been found to be a major risk factor of coronary heart disease and
the sixth article by Allen et al. (2016) focused on evaluating the impact of tobacco control
strategies on reducing inequalities related to smoking prevalence and premature mortality due to
CHD. The strength of tobacco control policies in reducing one of the major risk factor of CHD is
understood from this academic article.
It is necessary to evaluate theories and management practices presented in the
article selected for the paper. The first article provides an insight into the 19th edition of the
Cardiovascular Disease Statistics 2014 report. The burden of CVD, CHD and stroke in UK was
presented by means of detail on mortality, treatment cost and morbidity. The mortality data
suggested that improvement in mortality rate was achieved in 2012 as it became the second
leading cause of death compared to being the first leading cause of death previously (Bhatnagar
et al. 2015). However, gender based disparities in CVD outcome was seen as the report showed
that CVD remained the leading cause for death for women. In addition, regional variations in
mortality were also found as higher mortality was found in North England compared to South
England. Hence, the article highlighted the issue of health inequality, however how leadership
can play a role in advancing health equity and eliminating health disparities was not covered.
The article by Graci and Ruffin, (2014) emphasized that certain agencies drive leadership
and coordination process for eliminating health disparities. Hence, effective public health
leadership can be one source to address inequalities related to incidence of CHD. From this
perspective, the transformational leadership can address problem related to CHD in UK. This is
said informed by the theoretical aspects of transformational leadership. The theory suggests that
6CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
transformational leaders are inspiring and visionary and they can take the approach to change
individuals as well as the social system (Banks et al. 2016). Koh and Nowinski (2010) also
suggest that public health leader can translate health equity goals at community level. The
presence of transformational leadership trait can help them to address social determinant factors
affecting development of CHD and promote health equality in this area. When gender is the
reason for difference in prevalence rate, then leaders involved in the management of CHD should
focus on developing gender responsive health programmes (World Health Organization 2015).
Based on this information, it can be said that working to address social determinants of health
and health disparities should also be a part of preventive strategy for CVD in UK.
The second article by Bernard, Lux and Lohr (2009) focused on investigating about care
for CVD in prevention and primary care setting. In contrast to the first article, the second article
reviewed about the health delivery model for CVD. The first article gave idea about gender
inequality issues in disease prevalence, whereas the second articles highlighted about limitations
in health screening process for CVD. The article gave a comprehensive overview for each type
of health delivery model implemented for CVD. However, the limitation found in the article was
that it did not provided good evidence to translate diet and exercise intervention into the delivery
system of UK. It also showed that general physicians are the excellent sources for risk screening,
time constraints issues indicates training of other allied health staffs in the area of CVD risk
assessment. According to Ryley and Middleton (2016), empowering allied health professional is
necessary as they can become the leader of change and serve to improve screening process in
underserved areas.
In UK, health delivery model has mainly adopted medical model, however
biopsychosocial model should also become a necessary part of preventive work to maximize
transformational leaders are inspiring and visionary and they can take the approach to change
individuals as well as the social system (Banks et al. 2016). Koh and Nowinski (2010) also
suggest that public health leader can translate health equity goals at community level. The
presence of transformational leadership trait can help them to address social determinant factors
affecting development of CHD and promote health equality in this area. When gender is the
reason for difference in prevalence rate, then leaders involved in the management of CHD should
focus on developing gender responsive health programmes (World Health Organization 2015).
Based on this information, it can be said that working to address social determinants of health
and health disparities should also be a part of preventive strategy for CVD in UK.
The second article by Bernard, Lux and Lohr (2009) focused on investigating about care
for CVD in prevention and primary care setting. In contrast to the first article, the second article
reviewed about the health delivery model for CVD. The first article gave idea about gender
inequality issues in disease prevalence, whereas the second articles highlighted about limitations
in health screening process for CVD. The article gave a comprehensive overview for each type
of health delivery model implemented for CVD. However, the limitation found in the article was
that it did not provided good evidence to translate diet and exercise intervention into the delivery
system of UK. It also showed that general physicians are the excellent sources for risk screening,
time constraints issues indicates training of other allied health staffs in the area of CVD risk
assessment. According to Ryley and Middleton (2016), empowering allied health professional is
necessary as they can become the leader of change and serve to improve screening process in
underserved areas.
In UK, health delivery model has mainly adopted medical model, however
biopsychosocial model should also become a necessary part of preventive work to maximize
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
inclusiveness in preventive work and empower vulnerable group to improve their health. This
would mean taking actions according to the Marmot Review policy as it proposed developing
sustainable places and ensuring healthy standards of living for all. This means the focus should
not only be one illness prevention, but also enabling people to take right control over their lives
(Goldblatt 2016). Hence, consideration about the limitation of medical model to CHD and the
advantage of social model to CHD may help to effectively integrate social model in preventive
programs. This action will also in relevance with the Ottawa Charter as creating supportive
environment and reorienting health services are important elements of the Ottawa Charter
(Gagné and Lapalme 2017). Therefore, efforts like implementing healthy food programs in
schools and inculcating values of health lifestyle in children may pave the way for creating
supportive environment for people in UK in the near future. In addition, inclusion of counselors
or dieticians in school health promotion program or programs for women may help to reorient
health services.
The third article by Levy and Tedstone (2017) gave an insight about UK dietary policy
for the prevention of CVD. The dietary policy mainly focused on controlling intake of sugar and
fibre. The UK government recommendation was to take actions regarding the amount of sugar
sweetened beverages and sugar intake among children and young people. It also proposed action
to increase total dietary fibre intake as this is strongly associated with lower risk of
cardiometabolic abnormalities in people. Hence, it provides useful implications to make changes
in dietary guideline for UK population. However, encouraging people to eat as per dietary
recommendation is a challenging task for the government. In this situation, food industry
stakeholders should also be targeted so that they provided good nutritionals information and
inclusiveness in preventive work and empower vulnerable group to improve their health. This
would mean taking actions according to the Marmot Review policy as it proposed developing
sustainable places and ensuring healthy standards of living for all. This means the focus should
not only be one illness prevention, but also enabling people to take right control over their lives
(Goldblatt 2016). Hence, consideration about the limitation of medical model to CHD and the
advantage of social model to CHD may help to effectively integrate social model in preventive
programs. This action will also in relevance with the Ottawa Charter as creating supportive
environment and reorienting health services are important elements of the Ottawa Charter
(Gagné and Lapalme 2017). Therefore, efforts like implementing healthy food programs in
schools and inculcating values of health lifestyle in children may pave the way for creating
supportive environment for people in UK in the near future. In addition, inclusion of counselors
or dieticians in school health promotion program or programs for women may help to reorient
health services.
The third article by Levy and Tedstone (2017) gave an insight about UK dietary policy
for the prevention of CVD. The dietary policy mainly focused on controlling intake of sugar and
fibre. The UK government recommendation was to take actions regarding the amount of sugar
sweetened beverages and sugar intake among children and young people. It also proposed action
to increase total dietary fibre intake as this is strongly associated with lower risk of
cardiometabolic abnormalities in people. Hence, it provides useful implications to make changes
in dietary guideline for UK population. However, encouraging people to eat as per dietary
recommendation is a challenging task for the government. In this situation, food industry
stakeholders should also be targeted so that they provided good nutritionals information and
8CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
control salt and sugar level in food items to improve health of the population (Christoforou et al.
2016).
The article also gave the idea that reduction of salt intake by 1g can prevent 4147,
premature deaths and lead to total cost savings for NHS in UK. Hence, this showed implies that
dietary modifications and lifestyle intervention should be intensified in high risk individual as
dietary salt and high blood pressure are two important CVD risk factors (Klaus, Hoyer and
Middeke 2010). The UK government has collaborated with food manufacturing companies and
implemented salt awareness campaign to control salt intake and reduce risk of CHD. This
preventive strategy gives the lesson that analysis and engagement of all key stakeholders is
necessary to achieve the goals of CHD prevention. As food industry played a major role in
changing dietary habit of people, identifying and managing key stakeholder’s action can prove to
be a successful strategy towards change (Christoforou 016).
The fourth article by Collins et al. (2014) mainly focused on economical evaluation of
salt reduction policies for reducing CHD in England. CHD is the most prevalence type of CVD
in UK and high level of dietary salt intake is one factor that increases blood pressure and creates
the condition for the diagnosis of CHD (Ettehad et al., 2016). The study used modeling
techniques to identify the effect of reducing dietary salt intake on cardiovascular health outcome
for English population. The main trigger for such salt reduction intervention was the
implementation of health promotion policies like Change4Life and Health Weight, Healthy Lives
Strategy for England. These campaigns utilized media and advertising tools to encourage people
to make healthy food choices. The review of the study revealed that such media campaigns are
control salt and sugar level in food items to improve health of the population (Christoforou et al.
2016).
The article also gave the idea that reduction of salt intake by 1g can prevent 4147,
premature deaths and lead to total cost savings for NHS in UK. Hence, this showed implies that
dietary modifications and lifestyle intervention should be intensified in high risk individual as
dietary salt and high blood pressure are two important CVD risk factors (Klaus, Hoyer and
Middeke 2010). The UK government has collaborated with food manufacturing companies and
implemented salt awareness campaign to control salt intake and reduce risk of CHD. This
preventive strategy gives the lesson that analysis and engagement of all key stakeholders is
necessary to achieve the goals of CHD prevention. As food industry played a major role in
changing dietary habit of people, identifying and managing key stakeholder’s action can prove to
be a successful strategy towards change (Christoforou 016).
The fourth article by Collins et al. (2014) mainly focused on economical evaluation of
salt reduction policies for reducing CHD in England. CHD is the most prevalence type of CVD
in UK and high level of dietary salt intake is one factor that increases blood pressure and creates
the condition for the diagnosis of CHD (Ettehad et al., 2016). The study used modeling
techniques to identify the effect of reducing dietary salt intake on cardiovascular health outcome
for English population. The main trigger for such salt reduction intervention was the
implementation of health promotion policies like Change4Life and Health Weight, Healthy Lives
Strategy for England. These campaigns utilized media and advertising tools to encourage people
to make healthy food choices. The review of the study revealed that such media campaigns are
9CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
effective in changing health related behavior of patient as well as supporting UK food
manufacturers and retailers to make changes in food packaging and labeling so that people easily
understand nutritional intake in the food they consume. This kind of policies has been found
feasible to reduce the major risk factor of CHD in UK. Hence, research article by Collins et al.
(2014) mainly depicted the role of modeling technique in evaluating government policies related
to changes in food labeling and manufacturing. The study used IMPACT CHT model which was
relevant for the study objective. Creation of such simple models that are supported both
theoretically and empirically can be effective in understanding preventive work in the area of
CHD prevention.
Government’s action to implement salt reduction is a necessary management strategy for
heart disease because due to changes in lifestyle preference and availability of different packaged
food items, adults are consuming more salt than required (Trieu et al. 2015). Hence, when there
is comprehensive evidence regarding the effectiveness of reducing dietary intake of health
outcome, then UK government can implement multiple interventions like reformulation of food
items, food labeling and media campaigns to reduce salt consumption and make people aware
about harmful effect of high salt intake on future risk of CHD (Hyseni et al. 2017). Salt
reduction strategy is likely to be effective because this kind of interventions restrict the dietary
intake of sodium chloride and act to reduce the risk factor of CHD like high blood pressure.
However, rapid success cannot be achieved and it will require patience to get the desired result.
The fifth article utilized the economic modeling approach to assess the cost-
effectiveness of risk factor reduction programme targeting CVD in England and Wales. A
generic economic model was created to two scenarios- one consisting of decrease in blood
pressure at population and other related to legislative interventions aimed at reducing intakes of
effective in changing health related behavior of patient as well as supporting UK food
manufacturers and retailers to make changes in food packaging and labeling so that people easily
understand nutritional intake in the food they consume. This kind of policies has been found
feasible to reduce the major risk factor of CHD in UK. Hence, research article by Collins et al.
(2014) mainly depicted the role of modeling technique in evaluating government policies related
to changes in food labeling and manufacturing. The study used IMPACT CHT model which was
relevant for the study objective. Creation of such simple models that are supported both
theoretically and empirically can be effective in understanding preventive work in the area of
CHD prevention.
Government’s action to implement salt reduction is a necessary management strategy for
heart disease because due to changes in lifestyle preference and availability of different packaged
food items, adults are consuming more salt than required (Trieu et al. 2015). Hence, when there
is comprehensive evidence regarding the effectiveness of reducing dietary intake of health
outcome, then UK government can implement multiple interventions like reformulation of food
items, food labeling and media campaigns to reduce salt consumption and make people aware
about harmful effect of high salt intake on future risk of CHD (Hyseni et al. 2017). Salt
reduction strategy is likely to be effective because this kind of interventions restrict the dietary
intake of sodium chloride and act to reduce the risk factor of CHD like high blood pressure.
However, rapid success cannot be achieved and it will require patience to get the desired result.
The fifth article utilized the economic modeling approach to assess the cost-
effectiveness of risk factor reduction programme targeting CVD in England and Wales. A
generic economic model was created to two scenarios- one consisting of decrease in blood
pressure at population and other related to legislative interventions aimed at reducing intakes of
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
salt and trans fats (Barton et al., 2011). The advantage of the generic model was that it was
created in a way to identify cases of CVDs that were prevented or postponed. The model also
helped to estimate cost savings to the NHS and gain in life years and quality adjusted life years
(QALYs). Individual benefits as well as total accumulated benefits were calculated. The cost
analysis was done by the use of Sheffield prevention model. The uniqueness of the Sheffield
model is that it is a deterministic causal model that analyzed econometric component and the
epidemiological component (Katikireddi, Hilton and Bond 2016). Use of this modeling
technique in the study showed that reducing CVD risk by 1% can prevent 25000 new cases of
CVD and prevent 3500 deaths. This meant a cost saving of about £265m. Barton et al. (2011)
also emphasized on the extent of cost saving by stating that this would means annual savings of
about £30m for 10 years of the programme.
In case of specific intervention, Barton et al. (2011) showed that when salt intake
legislation reduces salt intake by 3g/day, then it would mean a reduction in population systolic
blood pressure by 2.5 mm Hg. In case of legislations related to ban of industrial fats, it showed
that reduction in energy intake by 0.5% can reduce risk of death by 5%. Hence, the review of this
study indicated that when policy intervention acts to even achieve 1% reduction in risk of VD,
then it can leads to substantial cost savings for the NHS (Barton et al. 2011). It can be said that
the spreadsheet model is the main highlight of this study as it proved that development of a
transparent model for cost estimation can help the UK government to track progress in CHD
outcomes when interventions are implemented at local levels. Inclusion of this model in
preventive programs can assist in making modifications in the right area and understanding the
crucial impact of intervention on population health. This would also create the pathway for a
responsive regulation that strengthens the effectiveness of health programs aiming to reduce
salt and trans fats (Barton et al., 2011). The advantage of the generic model was that it was
created in a way to identify cases of CVDs that were prevented or postponed. The model also
helped to estimate cost savings to the NHS and gain in life years and quality adjusted life years
(QALYs). Individual benefits as well as total accumulated benefits were calculated. The cost
analysis was done by the use of Sheffield prevention model. The uniqueness of the Sheffield
model is that it is a deterministic causal model that analyzed econometric component and the
epidemiological component (Katikireddi, Hilton and Bond 2016). Use of this modeling
technique in the study showed that reducing CVD risk by 1% can prevent 25000 new cases of
CVD and prevent 3500 deaths. This meant a cost saving of about £265m. Barton et al. (2011)
also emphasized on the extent of cost saving by stating that this would means annual savings of
about £30m for 10 years of the programme.
In case of specific intervention, Barton et al. (2011) showed that when salt intake
legislation reduces salt intake by 3g/day, then it would mean a reduction in population systolic
blood pressure by 2.5 mm Hg. In case of legislations related to ban of industrial fats, it showed
that reduction in energy intake by 0.5% can reduce risk of death by 5%. Hence, the review of this
study indicated that when policy intervention acts to even achieve 1% reduction in risk of VD,
then it can leads to substantial cost savings for the NHS (Barton et al. 2011). It can be said that
the spreadsheet model is the main highlight of this study as it proved that development of a
transparent model for cost estimation can help the UK government to track progress in CHD
outcomes when interventions are implemented at local levels. Inclusion of this model in
preventive programs can assist in making modifications in the right area and understanding the
crucial impact of intervention on population health. This would also create the pathway for a
responsive regulation that strengthens the effectiveness of health programs aiming to reduce
11CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
prevalence of CHD in UK. This approach is also an example of creative regulatory strategies that
supports government to fulfill key obligations related to public health and improve food industry
action towards population health (Magnusson and Reeve 2015).
The sixth articles provide an insight into management practices that are necessary for
prevention of chronic disease. It focused on analyzing the affect of Tobacco control score on
smoking prevalence and premature CHD mortality. The policy model was responsible for
feasible improvement in tobacco control policy and paved the way for reducing health
inequalities in England (Allen et al. 2016 ). Focusing on this area was important because tobacco
smoking is regarded as major causal link for diagnosis of CHD. The analysis of other cohort
based study also proves that smoking highly contributes to CVD deaths. The seriousness of
smoking is also understood from the fact it increases the mortality risk by two fold. However,
interventions aimed at addressing the dose of smoking were found to reduce the risk of CVD
mortality with time (Mons et al. 2015). Hence, preventive work in this area will lead to reduction
in risk for oldest age groups too. This intervention is in relevance with the theory of reasoned
action as the theory states that person’s health behavior is affected by their attitude towards the
behavior and smoking cessation programs focus on changing people’s attitude towards smoking
after knowing about its risk for cardiovascular health (Montano and Kasprzyk 2015.)
As the analysis of six articles revealed several shortcomings in the management and
prevention of CHD in UK, the UK government is recommended to prioritize the following
action in the future. Firstly, to mitigate gender based differences in CVD hospitalization and
mortality, they should focus on developing responsive CVD risk factor management program
among women. Secondly, in the area of implementing policies in the area of CHD prevention,
there is a need to go beyond patients who are diagnosed with disease and focus more on
prevalence of CHD in UK. This approach is also an example of creative regulatory strategies that
supports government to fulfill key obligations related to public health and improve food industry
action towards population health (Magnusson and Reeve 2015).
The sixth articles provide an insight into management practices that are necessary for
prevention of chronic disease. It focused on analyzing the affect of Tobacco control score on
smoking prevalence and premature CHD mortality. The policy model was responsible for
feasible improvement in tobacco control policy and paved the way for reducing health
inequalities in England (Allen et al. 2016 ). Focusing on this area was important because tobacco
smoking is regarded as major causal link for diagnosis of CHD. The analysis of other cohort
based study also proves that smoking highly contributes to CVD deaths. The seriousness of
smoking is also understood from the fact it increases the mortality risk by two fold. However,
interventions aimed at addressing the dose of smoking were found to reduce the risk of CVD
mortality with time (Mons et al. 2015). Hence, preventive work in this area will lead to reduction
in risk for oldest age groups too. This intervention is in relevance with the theory of reasoned
action as the theory states that person’s health behavior is affected by their attitude towards the
behavior and smoking cessation programs focus on changing people’s attitude towards smoking
after knowing about its risk for cardiovascular health (Montano and Kasprzyk 2015.)
As the analysis of six articles revealed several shortcomings in the management and
prevention of CHD in UK, the UK government is recommended to prioritize the following
action in the future. Firstly, to mitigate gender based differences in CVD hospitalization and
mortality, they should focus on developing responsive CVD risk factor management program
among women. Secondly, in the area of implementing policies in the area of CHD prevention,
there is a need to go beyond patients who are diagnosed with disease and focus more on
12CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
population at risk of developing the disease in the future. Health policies should also aim at
evaluating the effectiveness of program by the use of evidence based models that favor cost
analysis as evaluating effectiveness in terms of cost associated with care.
Conclusion:
The essay provided an insight into the evaluation of management practices for CHD in
UK by the analysis of six articles related to prevention of the disease. The six articles covered
important areas like prevalence rate, risk reduction policy, dietary policy, health model and salt
intake policies. It enlightened issues related to health inequality, lack of vision for program and
lack of evidence regarding effectiveness of certain intervention. However, the articles gave
important insight into the use of different models and framework to guide preventive programs.
Appropriate lessons can be taken from such programs to take constructive step towards reducing
the burden of CVD in UK in the future.
population at risk of developing the disease in the future. Health policies should also aim at
evaluating the effectiveness of program by the use of evidence based models that favor cost
analysis as evaluating effectiveness in terms of cost associated with care.
Conclusion:
The essay provided an insight into the evaluation of management practices for CHD in
UK by the analysis of six articles related to prevention of the disease. The six articles covered
important areas like prevalence rate, risk reduction policy, dietary policy, health model and salt
intake policies. It enlightened issues related to health inequality, lack of vision for program and
lack of evidence regarding effectiveness of certain intervention. However, the articles gave
important insight into the use of different models and framework to guide preventive programs.
Appropriate lessons can be taken from such programs to take constructive step towards reducing
the burden of CVD in UK in the future.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
References:
Allen, K., Kypridemos, C., Hyseni, L., Gilmore, A. B., Diggle, P., Whitehead, M., ... and
O’Flaherty, M. 2016. The effects of maximising the UK’s tobacco control score on inequalities
in smoking prevalence and premature coronary heart disease mortality: a modelling study. BMC
public health, 16(1), 292.
Banks, G.C., McCauley, K.D., Gardner, W.L. and Guler, C.E., 2016. A meta-analytic review of
authentic and transformational leadership: A test for redundancy. The Leadership
Quarterly, 27(4), pp.634-652.
Barton, P., Andronis, L., Briggs, A., McPherson, K., and Capewell, S. 2011. Effectiveness and
cost effectiveness of cardiovascular disease prevention in whole populations: modelling
study. BMJ, 343, d4044.
Bernard, S., Lux, L., and Lohr, K. 2009. Healthcare delivery models for prevention of
cardiovascular disease (CVD). The Health Foundation, London.
Bhatnagar, P., Wickramasinghe, K., Williams, J., Rayner, M., and Townsend, N. 2015. The
epidemiology of cardiovascular disease in the UK 2014. Heart, 101(15), 1182-1189.
Bhf.org.uk. 2016 Heart statistics. Retrieved 3 March 2018, from
https://www.bhf.org.uk/research/heart-statistics
Christoforou, A., Trieu, K., Land, M.A., Bolam, B. and Webster, J., 2016. State-level and
community-level salt reduction initiatives: a systematic review of global programmes and their
impact. J Epidemiol Community Health, 70(11), pp.1140-1150.
References:
Allen, K., Kypridemos, C., Hyseni, L., Gilmore, A. B., Diggle, P., Whitehead, M., ... and
O’Flaherty, M. 2016. The effects of maximising the UK’s tobacco control score on inequalities
in smoking prevalence and premature coronary heart disease mortality: a modelling study. BMC
public health, 16(1), 292.
Banks, G.C., McCauley, K.D., Gardner, W.L. and Guler, C.E., 2016. A meta-analytic review of
authentic and transformational leadership: A test for redundancy. The Leadership
Quarterly, 27(4), pp.634-652.
Barton, P., Andronis, L., Briggs, A., McPherson, K., and Capewell, S. 2011. Effectiveness and
cost effectiveness of cardiovascular disease prevention in whole populations: modelling
study. BMJ, 343, d4044.
Bernard, S., Lux, L., and Lohr, K. 2009. Healthcare delivery models for prevention of
cardiovascular disease (CVD). The Health Foundation, London.
Bhatnagar, P., Wickramasinghe, K., Williams, J., Rayner, M., and Townsend, N. 2015. The
epidemiology of cardiovascular disease in the UK 2014. Heart, 101(15), 1182-1189.
Bhf.org.uk. 2016 Heart statistics. Retrieved 3 March 2018, from
https://www.bhf.org.uk/research/heart-statistics
Christoforou, A., Trieu, K., Land, M.A., Bolam, B. and Webster, J., 2016. State-level and
community-level salt reduction initiatives: a systematic review of global programmes and their
impact. J Epidemiol Community Health, 70(11), pp.1140-1150.
14CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
Collins, M., Mason, H., O’Flaherty, M., Guzman-Castillo, M., Critchley, J., and Capewell, S.
2014. An economic evaluation of salt reduction policies to reduce coronary heart disease in
England: a policy modeling study. Value in Health, 17(5), 517-524.
Ettehad, D., Emdin, C.A., Kiran, A., Anderson, S.G., Callender, T., Emberson, J., Chalmers, J.,
Rodgers, A. and Rahimi, K., 2016. Blood pressure lowering for prevention of cardiovascular
disease and death: a systematic review and meta-analysis. The Lancet, 387(10022), pp.957-967.
Gagné, T. and Lapalme, J., 2017. 1986: Ottawa and onwards. The Lancet Public Health, 2(2),
p.e71.
Goldblatt, P.O., 2016. Moving forward monitoring of the social determinants of health in a
country: lessons from England 5 years after the Marmot Review. Global health action, 9(1),
p.29627.
Gracia, J.N. and Ruffin, J., 2014. Partnership, research, and leadership to advance health equity
and eliminate health disparities.
Hyseni, L., Elliot-Green, A., Lloyd-Williams, F., Kypridemos, C., O’Flaherty, M., McGill, R.,
Orton, L., Bromley, H., Cappuccio, F.P. and Capewell, S., 2017. Systematic review of dietary
salt reduction policies: Evidence for an effectiveness hierarchy?. PloS one, 12(5), p.e0177535.
Katikireddi, S.V., Hilton, S. and Bond, L., 2016. The role of the Sheffield model on the
minimum unit pricing of alcohol debate: the importance of a rhetorical perspective. Evidence &
policy: a journal of research, debate and practice, 12(4), pp.521-539.
Klaus, D., Hoyer, J. and Middeke, M., 2010. Salt restriction for the prevention of cardiovascular
disease. Deutsches Aerzteblatt International, 107(26), p.457.
Collins, M., Mason, H., O’Flaherty, M., Guzman-Castillo, M., Critchley, J., and Capewell, S.
2014. An economic evaluation of salt reduction policies to reduce coronary heart disease in
England: a policy modeling study. Value in Health, 17(5), 517-524.
Ettehad, D., Emdin, C.A., Kiran, A., Anderson, S.G., Callender, T., Emberson, J., Chalmers, J.,
Rodgers, A. and Rahimi, K., 2016. Blood pressure lowering for prevention of cardiovascular
disease and death: a systematic review and meta-analysis. The Lancet, 387(10022), pp.957-967.
Gagné, T. and Lapalme, J., 2017. 1986: Ottawa and onwards. The Lancet Public Health, 2(2),
p.e71.
Goldblatt, P.O., 2016. Moving forward monitoring of the social determinants of health in a
country: lessons from England 5 years after the Marmot Review. Global health action, 9(1),
p.29627.
Gracia, J.N. and Ruffin, J., 2014. Partnership, research, and leadership to advance health equity
and eliminate health disparities.
Hyseni, L., Elliot-Green, A., Lloyd-Williams, F., Kypridemos, C., O’Flaherty, M., McGill, R.,
Orton, L., Bromley, H., Cappuccio, F.P. and Capewell, S., 2017. Systematic review of dietary
salt reduction policies: Evidence for an effectiveness hierarchy?. PloS one, 12(5), p.e0177535.
Katikireddi, S.V., Hilton, S. and Bond, L., 2016. The role of the Sheffield model on the
minimum unit pricing of alcohol debate: the importance of a rhetorical perspective. Evidence &
policy: a journal of research, debate and practice, 12(4), pp.521-539.
Klaus, D., Hoyer, J. and Middeke, M., 2010. Salt restriction for the prevention of cardiovascular
disease. Deutsches Aerzteblatt International, 107(26), p.457.
15CONTEMPORARY THEMES IN HEALTH CARE LEVEL 6
Koh, H.K. and Nowinski, J.M., 2010. Health equity and public health leadership, Retrieved
from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2837440/
Levy, L., and Tedstone, A. 2017, February. UK Dietary Policy for the Prevention of
Cardiovascular Disease. In Healthcare(Vol. 5, No. 1, p. 9). Multidisciplinary Digital Publishing
Institute.
Magnusson, R. and Reeve, B., 2015. Food reformulation, responsive regulation, and “regulatory
scaffolding”: Strengthening performance of salt reduction programs in Australia and the United
Kingdom. Nutrients, 7(7), pp.5281-5308.
Mons, U., Müezzinler, A., Gellert, C., Schöttker, B., Abnet, C.C., Bobak, M., de Groot, L.,
Freedman, N.D., Jansen, E., Kee, F. and Kromhout, D., 2015. Impact of smoking and smoking
cessation on cardiovascular events and mortality among older adults: meta-analysis of individual
participant data from prospective cohort studies of the CHANCES consortium. bmj, 350,
p.h1551.
Montano, D.E. and Kasprzyk, D., 2015. Theory of reasoned action, theory of planned behavior,
and the integrated behavioral model. Health behavior: Theory, research and practice, pp.95-124.
Ryley, N. and Middleton, C., 2016. Framework for advanced nursing, midwifery and allied
health professional practice in Wales: the implementation process. Journal of nursing
management, 24(1).
Trieu, K., Neal, B., Hawkes, C., Dunford, E., Campbell, N., Rodriguez-Fernandez, R., Legetic,
B., McLaren, L., Barberio, A. and Webster, J., 2015. Salt reduction initiatives around the world–
a systematic review of progress towards the global target. PloS one, 10(7), p.e0130247.
Koh, H.K. and Nowinski, J.M., 2010. Health equity and public health leadership, Retrieved
from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2837440/
Levy, L., and Tedstone, A. 2017, February. UK Dietary Policy for the Prevention of
Cardiovascular Disease. In Healthcare(Vol. 5, No. 1, p. 9). Multidisciplinary Digital Publishing
Institute.
Magnusson, R. and Reeve, B., 2015. Food reformulation, responsive regulation, and “regulatory
scaffolding”: Strengthening performance of salt reduction programs in Australia and the United
Kingdom. Nutrients, 7(7), pp.5281-5308.
Mons, U., Müezzinler, A., Gellert, C., Schöttker, B., Abnet, C.C., Bobak, M., de Groot, L.,
Freedman, N.D., Jansen, E., Kee, F. and Kromhout, D., 2015. Impact of smoking and smoking
cessation on cardiovascular events and mortality among older adults: meta-analysis of individual
participant data from prospective cohort studies of the CHANCES consortium. bmj, 350,
p.h1551.
Montano, D.E. and Kasprzyk, D., 2015. Theory of reasoned action, theory of planned behavior,
and the integrated behavioral model. Health behavior: Theory, research and practice, pp.95-124.
Ryley, N. and Middleton, C., 2016. Framework for advanced nursing, midwifery and allied
health professional practice in Wales: the implementation process. Journal of nursing
management, 24(1).
Trieu, K., Neal, B., Hawkes, C., Dunford, E., Campbell, N., Rodriguez-Fernandez, R., Legetic,
B., McLaren, L., Barberio, A. and Webster, J., 2015. Salt reduction initiatives around the world–
a systematic review of progress towards the global target. PloS one, 10(7), p.e0130247.
1 out of 16
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.