NSB 204 Mental Health: Assessment Task 2 - Holistic Assessment Report
VerifiedAdded on 2023/06/08
|19
|3790
|138
Report
AI Summary
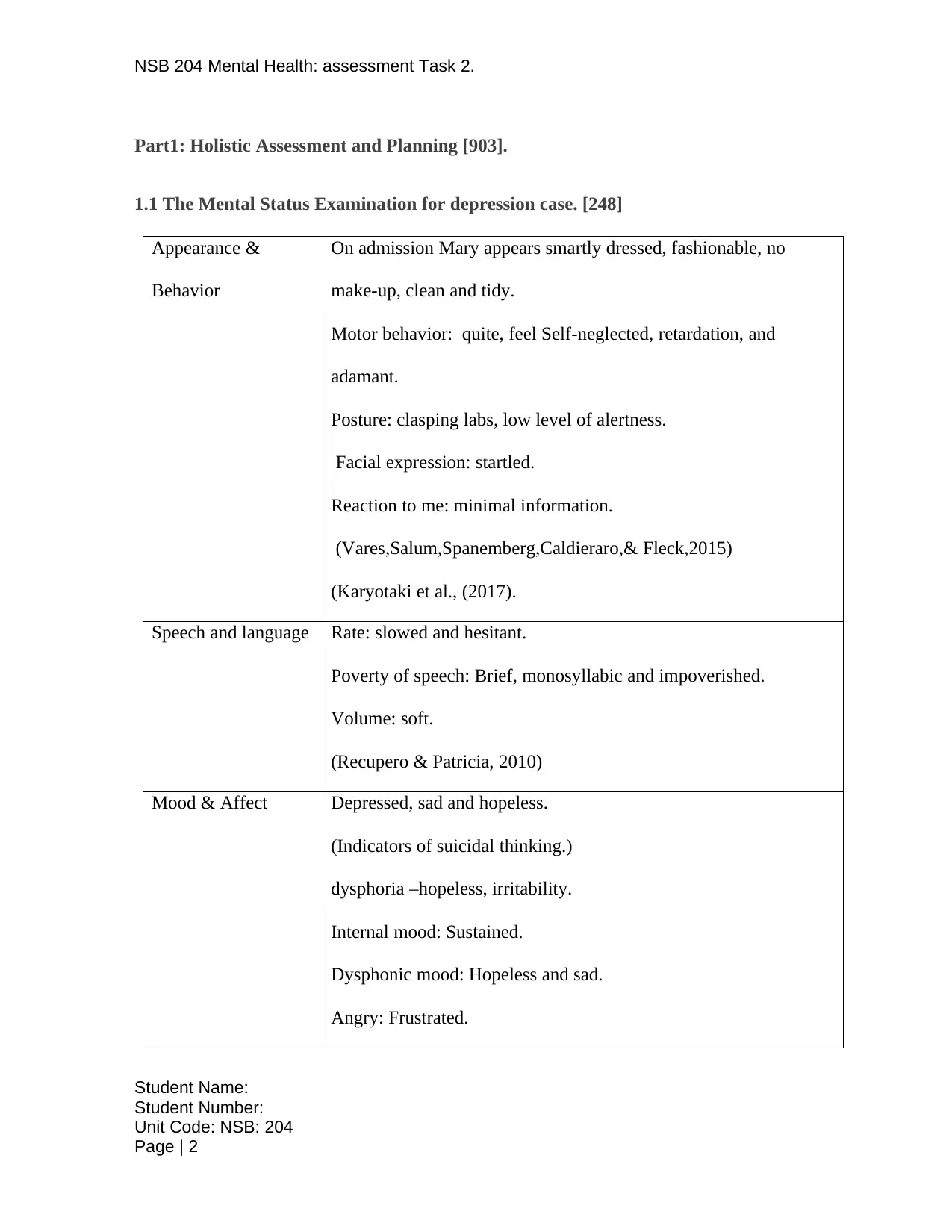
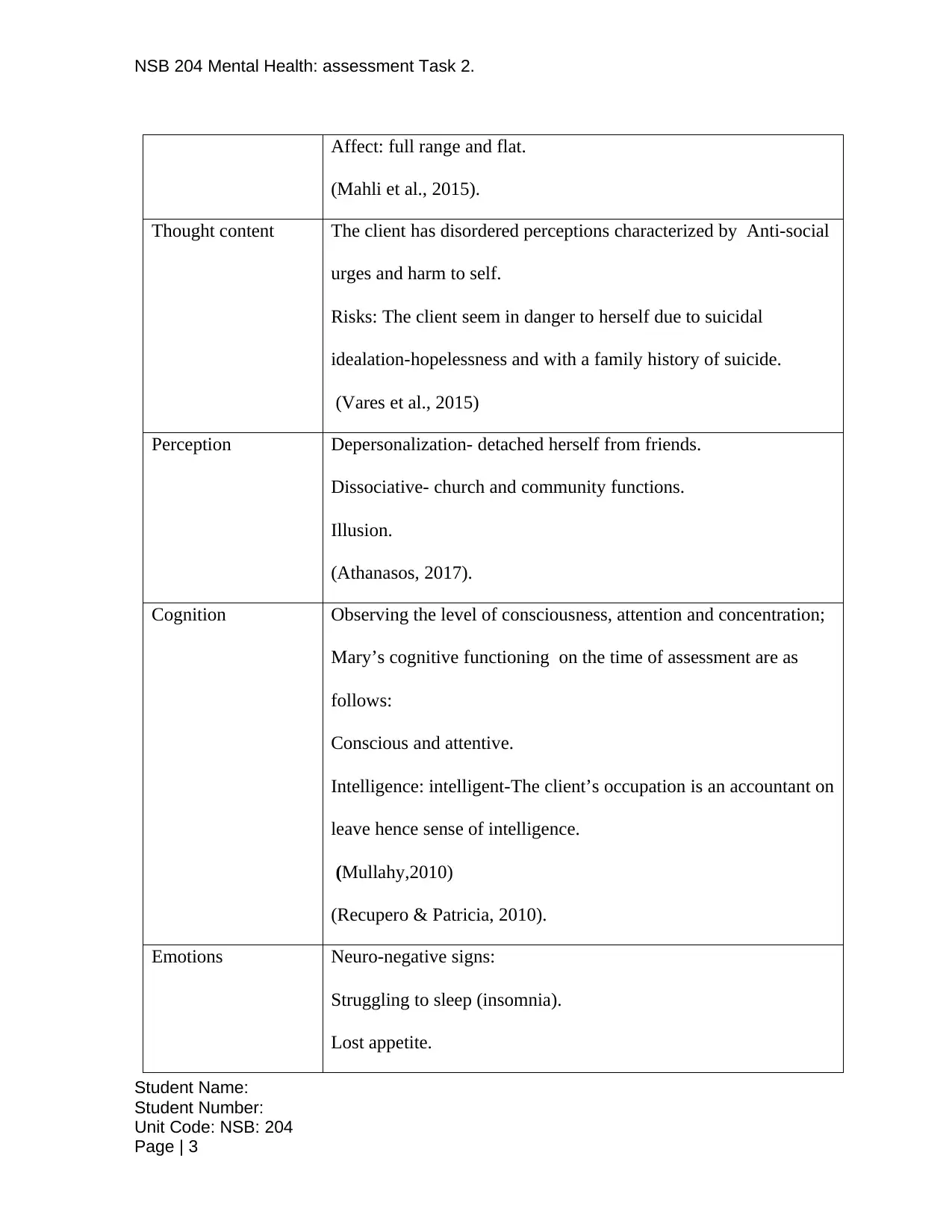
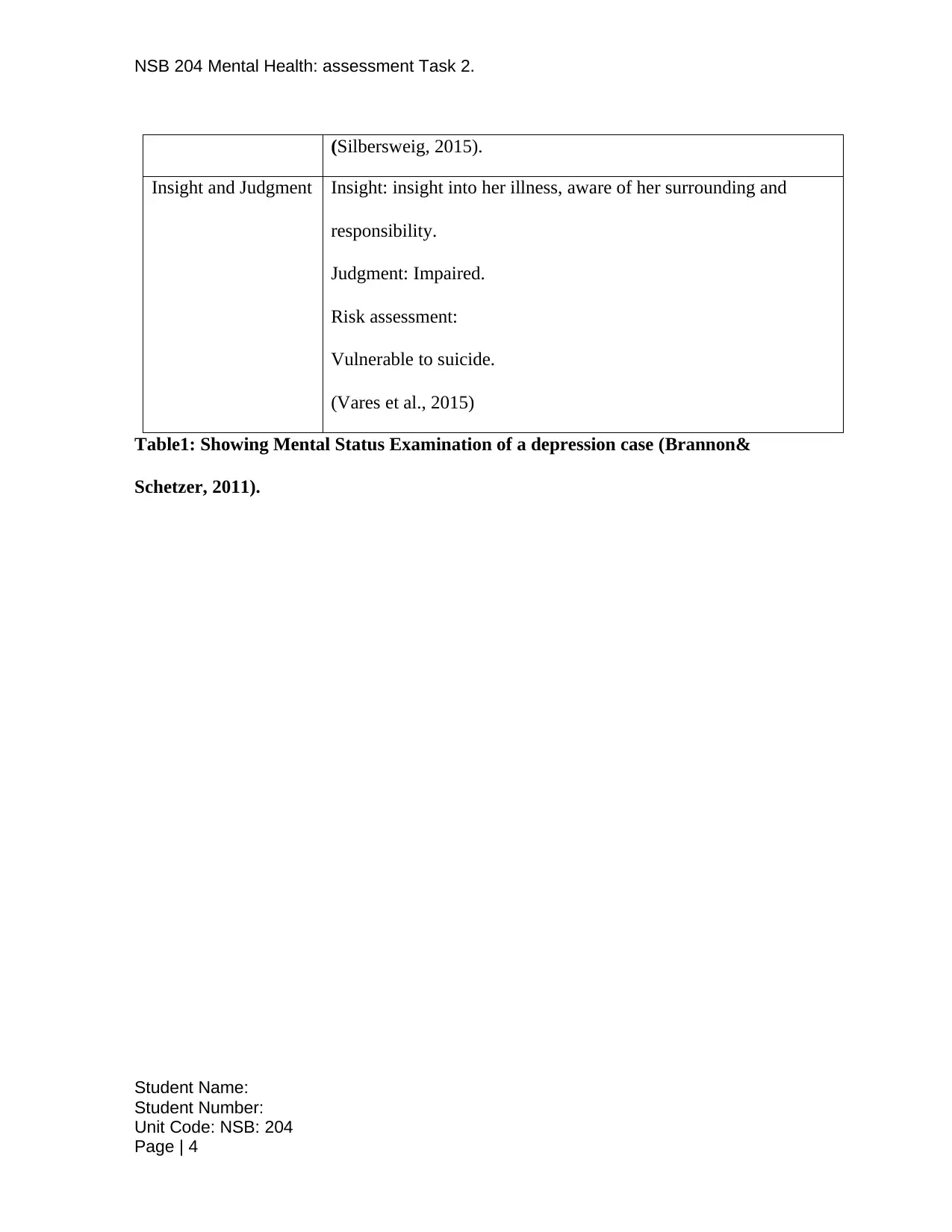
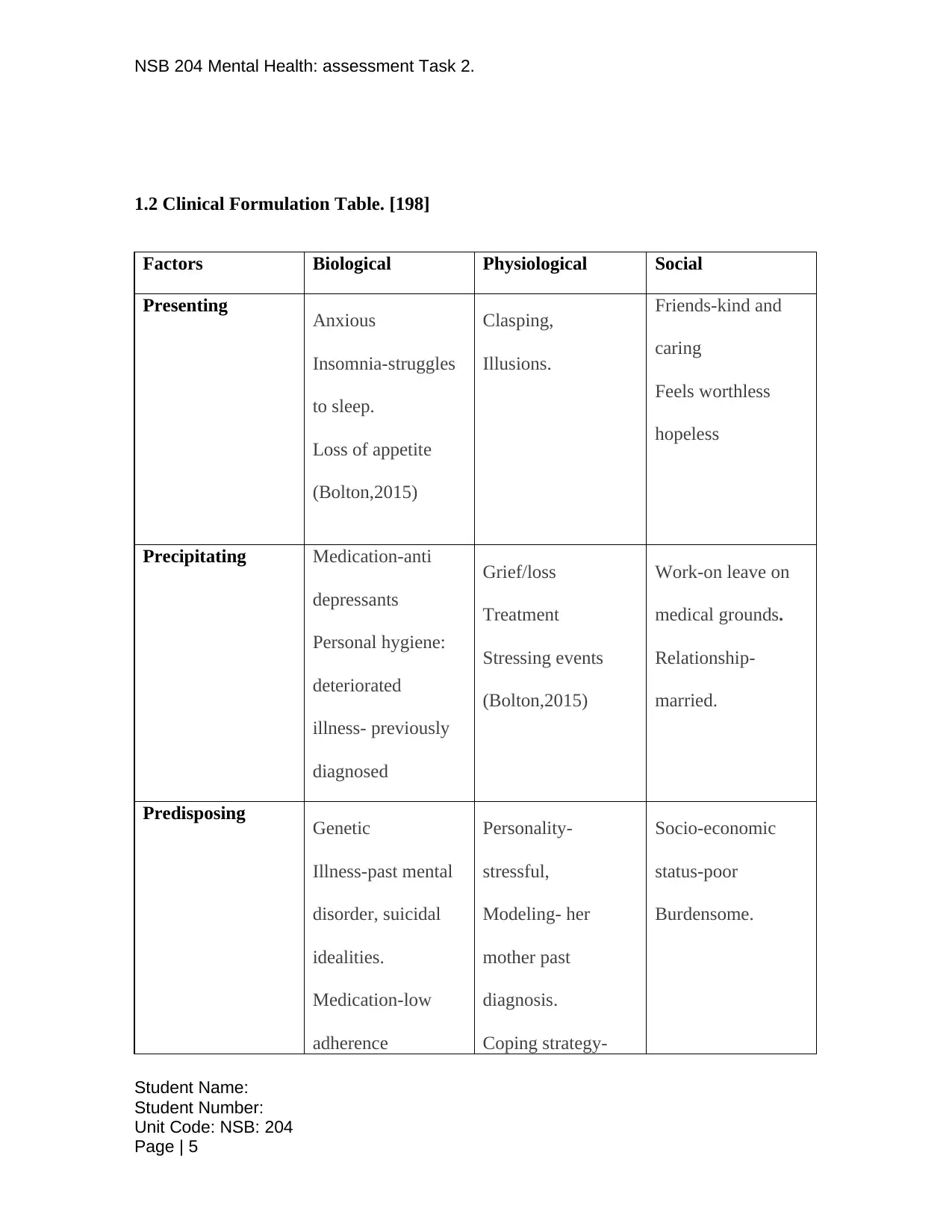
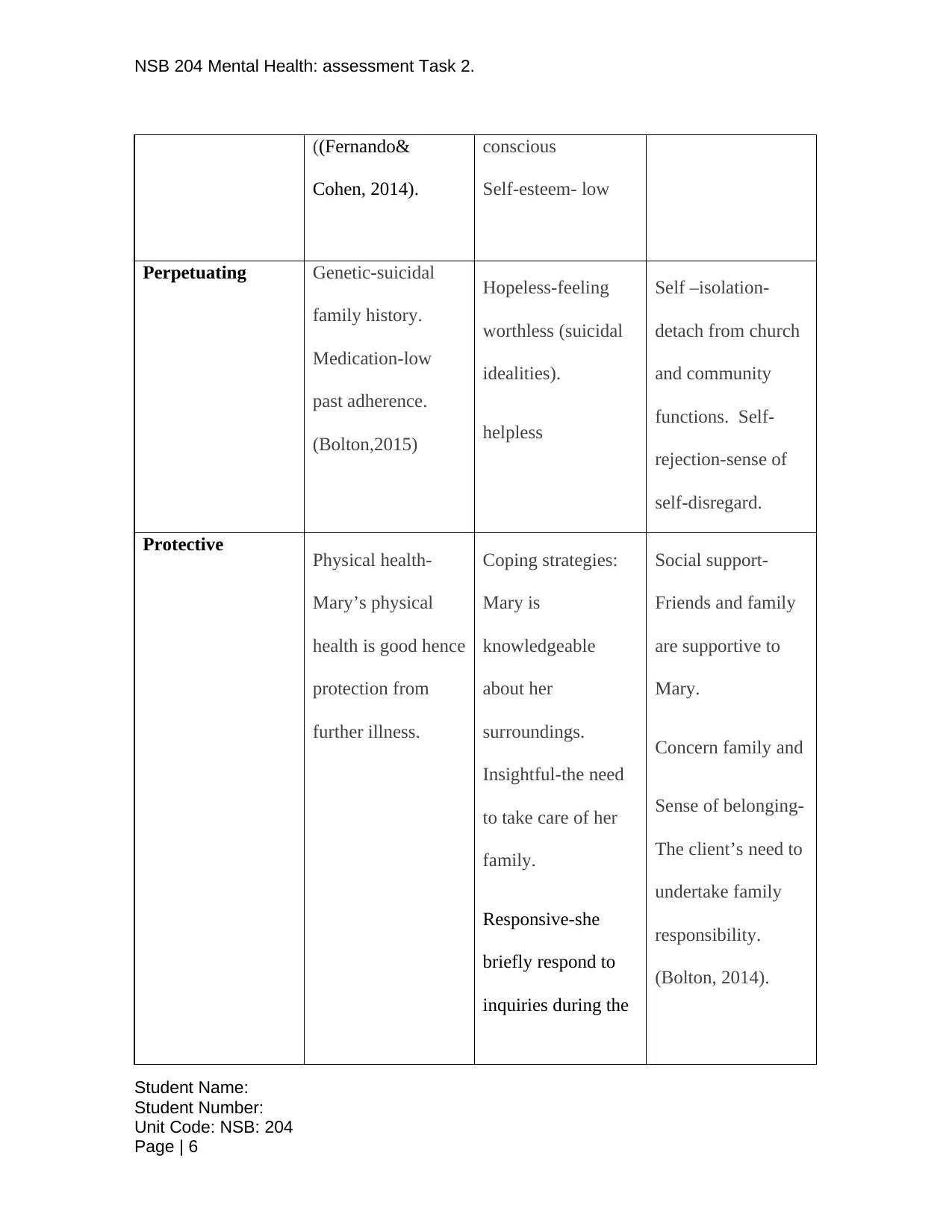
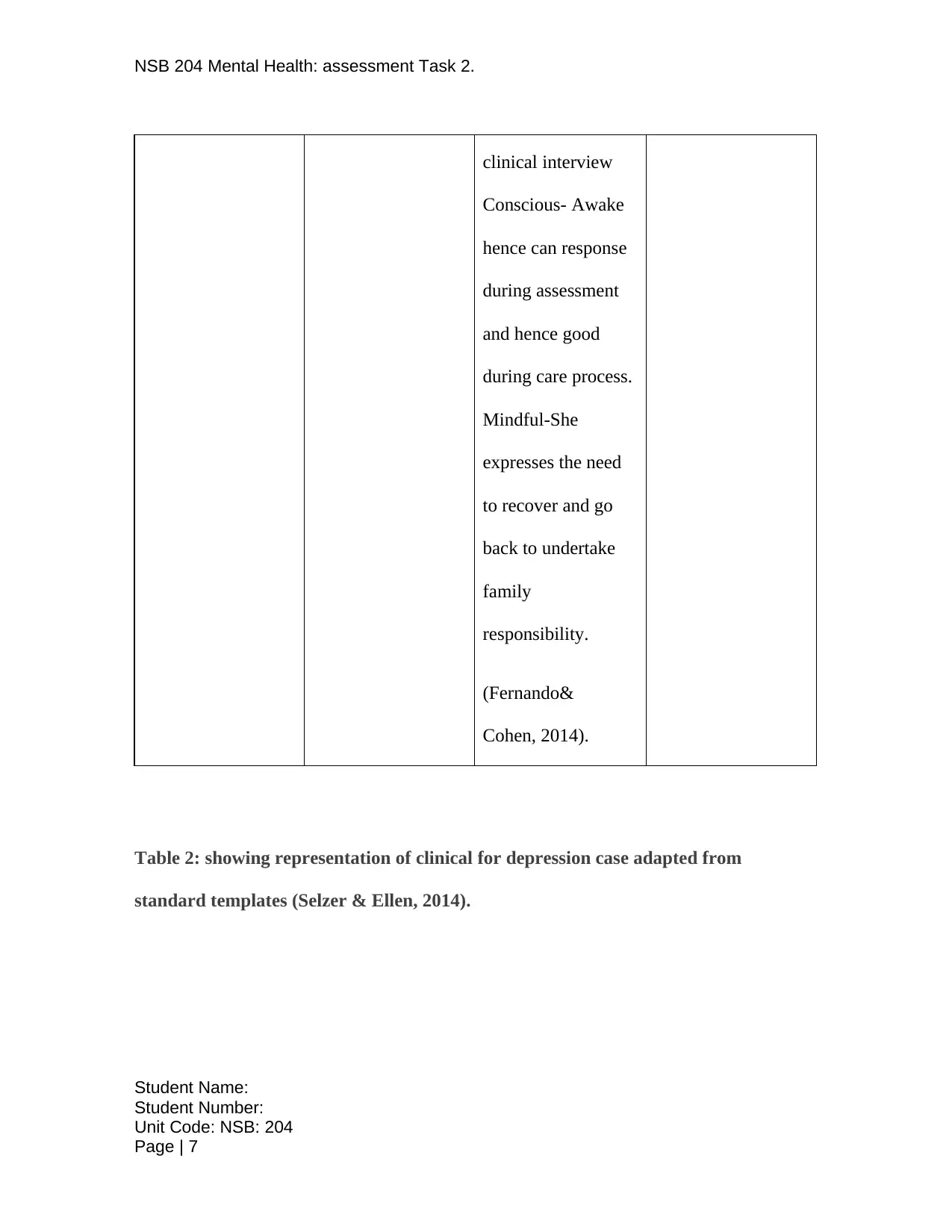
This report presents a detailed mental health assessment of a 41-year-old accountant, Mary, diagnosed with depression. It includes a Mental Status Examination (MSE) outlining her appearance, behavior, speech, mood, thought content, perception, cognition, emotions, insight, and judgment. A clinical formulation table provides biological, psychological, and social factors influencing her condition, along with precipitating, predisposing, and perpetuating factors, and protective elements. The report details plans for nursing care, including establishing a therapeutic relationship, promoting self-worth, communication skills, patient-centered care, and evidence-based practices. It also covers clinical handover procedures. Part 2 delves into therapeutic engagement, emphasizing the therapeutic nurse-client relationship, cultural safety, and recovery-oriented nursing care. The report highlights the importance of trust, empathy, and professional boundaries in the therapeutic relationship. It also addresses the significance of cultural sensitivity and the implementation of recovery-oriented models to support the client's journey towards wellness, emphasizing self-determination and shared decision-making.
1 out of 19
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.