Diagnostic Ultrasound: Indications, Patient Preparation, and Pathological Considerations
VerifiedAdded on 2023/06/05
|17
|3515
|115
AI Summary
This paper highlights the indications and the contra-indications that are related to the abdomen ultrasound. In addition to this the paper will also highlight the factors like patient preparation, patient care and the relevant anatomical and the physiological examinations. The likely outcome of the patient was that after conduction of the ultrasound, the patient was most likely to be diagnosed with kidney problems since he was experiencing pain in the right upper quadrant of the abdomen. Additionally it might be problems of liver cirrhosis or gall bladder as the patient showed deranged LFT results.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.

Running head: DIAGNOSTIC ULTRASOUND
DIAGNOSTIC ULTRASOUND
Name of the Student:
Name of the University:
Author Note:
DIAGNOSTIC ULTRASOUND
Name of the Student:
Name of the University:
Author Note:
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
1
DIAGNOSTIC ULTRASOUND
Executive Summary:
The abdominal ultrasound is an important method of diagnostics which is use for the
evaluation of the various structures of the abdomen which includes the livers, biliary tract, the
gall bladder along with the pancreas and the kidney. This paper therefore aims to highlight
the indications and the contra-indications that are related to the abdomen ultrasound. In
addition to this the paper will also highlight the factors like patient preparation, patient care
and the relevant anatomical and the physiological examinations. In association to abdomen
ultrasound the aspects like the examination protocols and the ultrasound machine that needs
to be used will also be discussed here in association with the alternative procedures and the
possible outcomes of the patient. The likely outcome of the patient was that after conduction
of the ultrasound, the patient was most likely to be diagnosed with kidney problems since he
was experiencing pain in the right upper quadrant of the abdomen. Additionally it might be
problems of liver cirrhosis or gall bladder as the patient showed deranged LFT results.
DIAGNOSTIC ULTRASOUND
Executive Summary:
The abdominal ultrasound is an important method of diagnostics which is use for the
evaluation of the various structures of the abdomen which includes the livers, biliary tract, the
gall bladder along with the pancreas and the kidney. This paper therefore aims to highlight
the indications and the contra-indications that are related to the abdomen ultrasound. In
addition to this the paper will also highlight the factors like patient preparation, patient care
and the relevant anatomical and the physiological examinations. In association to abdomen
ultrasound the aspects like the examination protocols and the ultrasound machine that needs
to be used will also be discussed here in association with the alternative procedures and the
possible outcomes of the patient. The likely outcome of the patient was that after conduction
of the ultrasound, the patient was most likely to be diagnosed with kidney problems since he
was experiencing pain in the right upper quadrant of the abdomen. Additionally it might be
problems of liver cirrhosis or gall bladder as the patient showed deranged LFT results.
2
DIAGNOSTIC ULTRASOUND
Table of Contents
Introduction................................................................................................................................3
Indications/contra-indications for examination..........................................................................3
Patient preparation.....................................................................................................................4
Patient care including communication, ethical and infection control considerations................5
Relevant anatomical and physiological considerations..............................................................6
3 - 5 pathological considerations for given patient presentation with likely ultrasound
appearances................................................................................................................................9
Procedure for examination/protocols and basic technical aspects...........................................12
Alternative procedures.............................................................................................................13
Possible or likely outcomes for the patient..............................................................................13
References................................................................................................................................14
DIAGNOSTIC ULTRASOUND
Table of Contents
Introduction................................................................................................................................3
Indications/contra-indications for examination..........................................................................3
Patient preparation.....................................................................................................................4
Patient care including communication, ethical and infection control considerations................5
Relevant anatomical and physiological considerations..............................................................6
3 - 5 pathological considerations for given patient presentation with likely ultrasound
appearances................................................................................................................................9
Procedure for examination/protocols and basic technical aspects...........................................12
Alternative procedures.............................................................................................................13
Possible or likely outcomes for the patient..............................................................................13
References................................................................................................................................14
3
DIAGNOSTIC ULTRASOUND
Introduction
The abdominal ultrasound is an important method of diagnostics which is use for the
evaluation of the various structures of the abdomen which includes the livers, biliary tract, the
gall bladder along with the pancreas and the kidney (Mouratev et al., 2013). The case
presented here shows that the patient who is a 54 old year gentleman s requesting to undergo
an abdomen ultrasound. The scenario shows that the referral indicates he is experiencing
severe right upper quadrant pain and the blood tests have indicated deranged LFTs. This
paper therefore aims to highlight the indications and the contra-indications that are related to
the abdomen ultrasound. In addition to this the paper will also highlight the factors like
patient preparation, patient care and the relevant anatomical and the physiological
examinations. In association to abdomen ultrasound the aspects like the examination
protocols and the ultrasound machine that needs to be used will also be discussed here in
association with the alternative procedures and the possible outcomes of the patient.
Indications/contra-indications for examination
The indications of abdomen ultrasound examination involve the conditions like
abdominal pain, the flank or back pain in association with the palpable abnormalities. The
conditions like abnormal laboratory values provide suggestions as indication for the
abdominal pathology. This leads to follow up of the abnormalities that are suspected along
with the search for a metastatic disease. Additionally some of the common indications for
abdominal ultrasound includes cholelithiasis in addition to nephroliathisis. In addition to this,
other indication involve pathology liver, in association with irritable bowel syndrome and
unspecified pathology gallbladder (Bohnhorst, 2013).
On the other hand the contra-indications of abdomen ultrasound examinations
involves conduction of ultrasound over the uterus during pregnancy. The contra indication
DIAGNOSTIC ULTRASOUND
Introduction
The abdominal ultrasound is an important method of diagnostics which is use for the
evaluation of the various structures of the abdomen which includes the livers, biliary tract, the
gall bladder along with the pancreas and the kidney (Mouratev et al., 2013). The case
presented here shows that the patient who is a 54 old year gentleman s requesting to undergo
an abdomen ultrasound. The scenario shows that the referral indicates he is experiencing
severe right upper quadrant pain and the blood tests have indicated deranged LFTs. This
paper therefore aims to highlight the indications and the contra-indications that are related to
the abdomen ultrasound. In addition to this the paper will also highlight the factors like
patient preparation, patient care and the relevant anatomical and the physiological
examinations. In association to abdomen ultrasound the aspects like the examination
protocols and the ultrasound machine that needs to be used will also be discussed here in
association with the alternative procedures and the possible outcomes of the patient.
Indications/contra-indications for examination
The indications of abdomen ultrasound examination involve the conditions like
abdominal pain, the flank or back pain in association with the palpable abnormalities. The
conditions like abnormal laboratory values provide suggestions as indication for the
abdominal pathology. This leads to follow up of the abnormalities that are suspected along
with the search for a metastatic disease. Additionally some of the common indications for
abdominal ultrasound includes cholelithiasis in addition to nephroliathisis. In addition to this,
other indication involve pathology liver, in association with irritable bowel syndrome and
unspecified pathology gallbladder (Bohnhorst, 2013).
On the other hand the contra-indications of abdomen ultrasound examinations
involves conduction of ultrasound over the uterus during pregnancy. The contra indication
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
4
DIAGNOSTIC ULTRASOUND
also involve ultrasound over the damaged skin or at the risk skin which might involve eczema
or skin rash. Other such contra indications involves over the excitable tissue that involves the
heart, exposed nerve and the carotid sinus (Sessa et al., 2015).
Patient preparation
The patient preparation for the abdomen ultrasound examination involves making the
patient wear loose fitting clothes. Any kind of jewellery and clothing needs to be removed
from the area which needs to be examined. The patient might be asked to wear a gown while
the examination takes place. The preparation of the patient needs to be taken according to the
type of ultrasound that the patient undergoes. Here the patient needs to be done a abdomen
ultrasound for the imaging of the liver, gallbladder, spleen, and pancreas, therefore the patient
needs to have a fat free meal on the evening prior to the examination is conducted. In addition
it needs to be ensured that eating is avoided before eight to 12 hours of the procedure is
conducted. This fasting is required since when food is taken, the gallbladder contracts and
discharges bile to help process the sustenance. On the off chance anything eaten inside 6 long
periods of the exam, the gallbladder may not look ordinary in the ultrasound pictures. The
patient will lie on an exam table. The sonographer will move the apparel far from the guts
and after that apply a warm gel to the territory. This gel enables the transducer to reach the
skin. The sonographer will then press the transducer against the skin and move it around to
take the pictures. If required, the radiologist may take more pictures after the sonographer is
finished. The exam ordinarily takes under 45 minutes. There is next to zero uneasiness amid
an ultrasound exam of the guts. The patient feels the sonographer apply warm gel to the guts.
One might feel slight weight as the transducer is moved over the skin (Bahner et al., 2013).
DIAGNOSTIC ULTRASOUND
also involve ultrasound over the damaged skin or at the risk skin which might involve eczema
or skin rash. Other such contra indications involves over the excitable tissue that involves the
heart, exposed nerve and the carotid sinus (Sessa et al., 2015).
Patient preparation
The patient preparation for the abdomen ultrasound examination involves making the
patient wear loose fitting clothes. Any kind of jewellery and clothing needs to be removed
from the area which needs to be examined. The patient might be asked to wear a gown while
the examination takes place. The preparation of the patient needs to be taken according to the
type of ultrasound that the patient undergoes. Here the patient needs to be done a abdomen
ultrasound for the imaging of the liver, gallbladder, spleen, and pancreas, therefore the patient
needs to have a fat free meal on the evening prior to the examination is conducted. In addition
it needs to be ensured that eating is avoided before eight to 12 hours of the procedure is
conducted. This fasting is required since when food is taken, the gallbladder contracts and
discharges bile to help process the sustenance. On the off chance anything eaten inside 6 long
periods of the exam, the gallbladder may not look ordinary in the ultrasound pictures. The
patient will lie on an exam table. The sonographer will move the apparel far from the guts
and after that apply a warm gel to the territory. This gel enables the transducer to reach the
skin. The sonographer will then press the transducer against the skin and move it around to
take the pictures. If required, the radiologist may take more pictures after the sonographer is
finished. The exam ordinarily takes under 45 minutes. There is next to zero uneasiness amid
an ultrasound exam of the guts. The patient feels the sonographer apply warm gel to the guts.
One might feel slight weight as the transducer is moved over the skin (Bahner et al., 2013).
5
DIAGNOSTIC ULTRASOUND
Patient care including communication, ethical and infection control
considerations
In terms of communication, while undertaking any ultrasound examination and
working as per privately concurred rehearse; the sonographer should get adequate verbal and
additionally composed data from the clinician to embrace effectively the examination asked
for. One should be aware of the need to utilize mediators as and when important to discuss
sufficiently with the patient. One should have the capacity to talk about the relative dangers
and advantages of the examination with the patient. One should clarify the filtering strategy
suitably to the patient. It is needed to acquire educated consent from the patient or their agent
being aware of his/her ability to understand know about the individual patient's extraordinary
needs including escorting and security amid the examination. One should be proficient and
understanding all through the examination and deal with the collaboration between the
patients (Callen & Norton, 2016).
As far as moral contemplations, substantial assent must be gotten before beginning
any ultrasound examination or methodology. Medicinal services experts who don't regard the
privilege of a patient to figure out the end result for their own body along these lines might be
at risk to lawful or disciplinary activity. The assent procedure is a continuum starting with the
alluding medicinal services proficient who asks for the ultrasound examination and
completion with the sonographer who does it. It is the obligation of the alluding proficient to
give adequate data to the patient to empower the last to agree to the ultrasound examination
being asked. It is the obligation of the sonographer to guarantee that the patient comprehends
the extent of the ultrasound examination preceding giving patient’s assent (Wax et al., 2014).
The absence of, or resistance to, cleaning and contamination control rules in the
ultrasound working environment could be in charge of the transmission of critical human
DIAGNOSTIC ULTRASOUND
Patient care including communication, ethical and infection control
considerations
In terms of communication, while undertaking any ultrasound examination and
working as per privately concurred rehearse; the sonographer should get adequate verbal and
additionally composed data from the clinician to embrace effectively the examination asked
for. One should be aware of the need to utilize mediators as and when important to discuss
sufficiently with the patient. One should have the capacity to talk about the relative dangers
and advantages of the examination with the patient. One should clarify the filtering strategy
suitably to the patient. It is needed to acquire educated consent from the patient or their agent
being aware of his/her ability to understand know about the individual patient's extraordinary
needs including escorting and security amid the examination. One should be proficient and
understanding all through the examination and deal with the collaboration between the
patients (Callen & Norton, 2016).
As far as moral contemplations, substantial assent must be gotten before beginning
any ultrasound examination or methodology. Medicinal services experts who don't regard the
privilege of a patient to figure out the end result for their own body along these lines might be
at risk to lawful or disciplinary activity. The assent procedure is a continuum starting with the
alluding medicinal services proficient who asks for the ultrasound examination and
completion with the sonographer who does it. It is the obligation of the alluding proficient to
give adequate data to the patient to empower the last to agree to the ultrasound examination
being asked. It is the obligation of the sonographer to guarantee that the patient comprehends
the extent of the ultrasound examination preceding giving patient’s assent (Wax et al., 2014).
The absence of, or resistance to, cleaning and contamination control rules in the
ultrasound working environment could be in charge of the transmission of critical human
6
DIAGNOSTIC ULTRASOUND
services related diseases between expert, machine and the patient. The ultrasound client may
disregard fundamental cleanliness safeguards, for example, sufficiently cleaning transducers
between patients, not utilizing transducer covers for specific examinations, not washing the
hands nor consistently cleaning the ultrasound machine console and transducer ropes, nor
taking suitable care and utilization of ultrasound coupling gel (O’Dochartaigh & Douma,
2015).
Relevant anatomical and physiological considerations
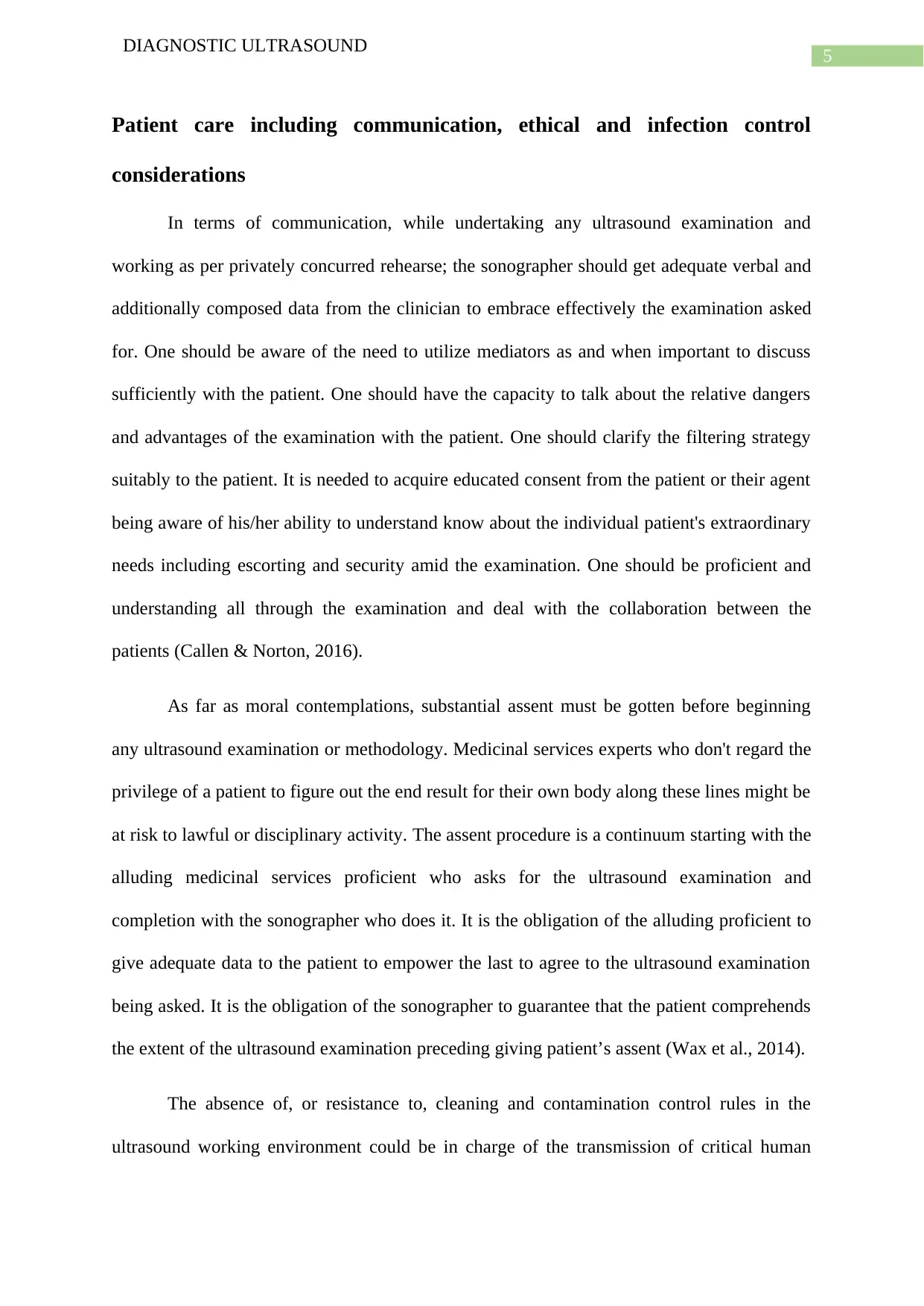
Liver- The examination begins with the patient in supine position and continues in left
lateral decubitus. For a good ultrasound "window" usually the patient needs to perform a
deep inspiration, to maintain it for a few seconds while the examiner scans the liver structure.
A convex transducer with variable frequency of 2-5 MHz is generally used, the frequency is
chosen according to the examined subject characteristics. If one is interested in details of
liver surface or in superficial areas of the liver, linear transducers with higher frequency (4-8
MHz) should be used (Ripollés et al., 2013).
DIAGNOSTIC ULTRASOUND
services related diseases between expert, machine and the patient. The ultrasound client may
disregard fundamental cleanliness safeguards, for example, sufficiently cleaning transducers
between patients, not utilizing transducer covers for specific examinations, not washing the
hands nor consistently cleaning the ultrasound machine console and transducer ropes, nor
taking suitable care and utilization of ultrasound coupling gel (O’Dochartaigh & Douma,
2015).
Relevant anatomical and physiological considerations
Liver- The examination begins with the patient in supine position and continues in left
lateral decubitus. For a good ultrasound "window" usually the patient needs to perform a
deep inspiration, to maintain it for a few seconds while the examiner scans the liver structure.
A convex transducer with variable frequency of 2-5 MHz is generally used, the frequency is
chosen according to the examined subject characteristics. If one is interested in details of
liver surface or in superficial areas of the liver, linear transducers with higher frequency (4-8
MHz) should be used (Ripollés et al., 2013).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
DIAGNOSTIC ULTRASOUND
Figure 1: US image of normal liver
Source: (eBook & Guide, 2018)
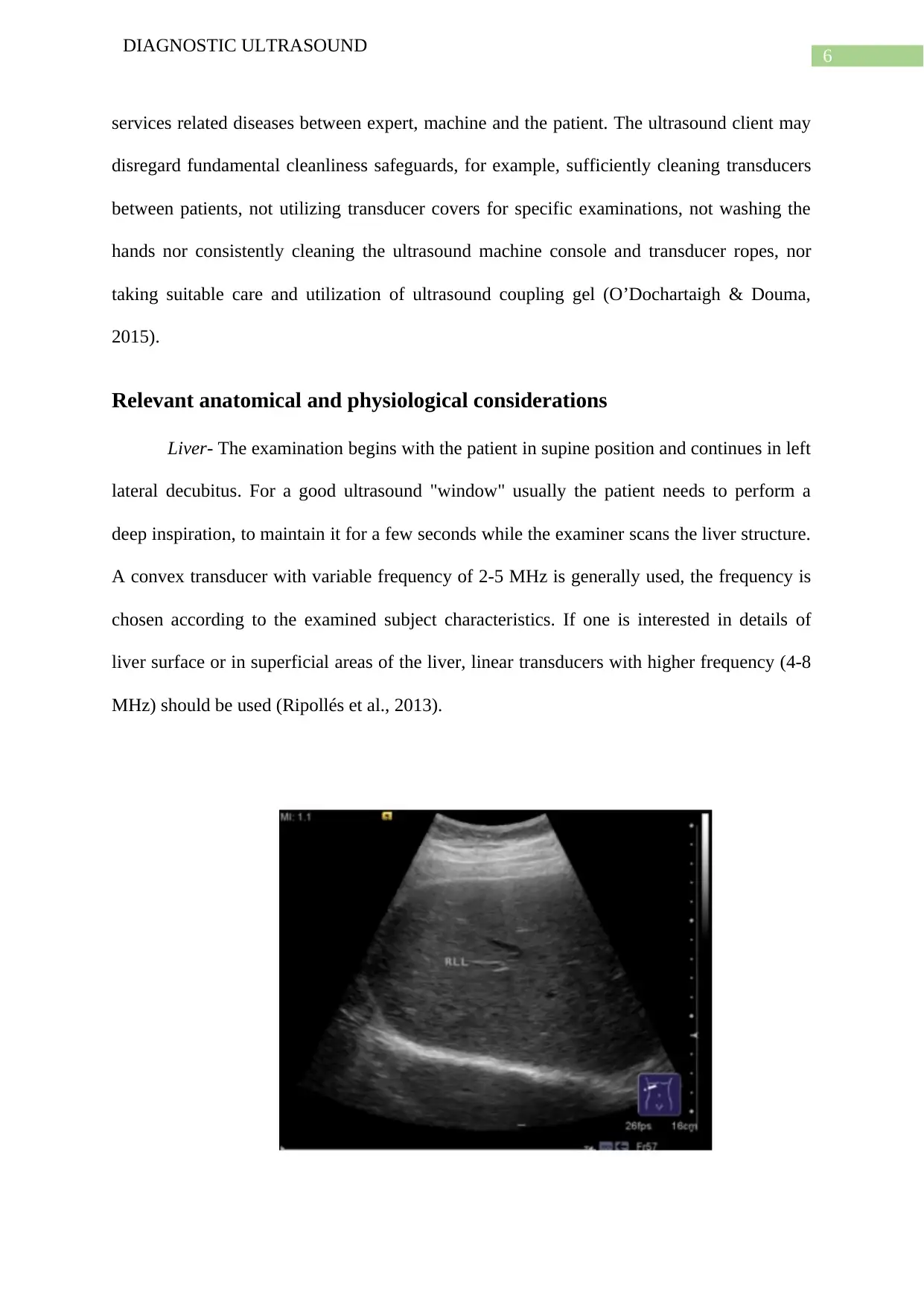
Gall bladder- The normal appearance of the gallbladder is of a pear shaped, anechoic
structure with well-defined hyperechoic wall. The normal diameters are generally smaller
than 8/3 cm, the maximum accepted ones are 10/4 cm, and higher values are suggestive for
hydrops. The normal gallbladder wall thickness is maximum 4 mm (Bourcier et al., 2014).
Figure 2: US of normal gall bladder
Source: (eBook & Guide, 2018)
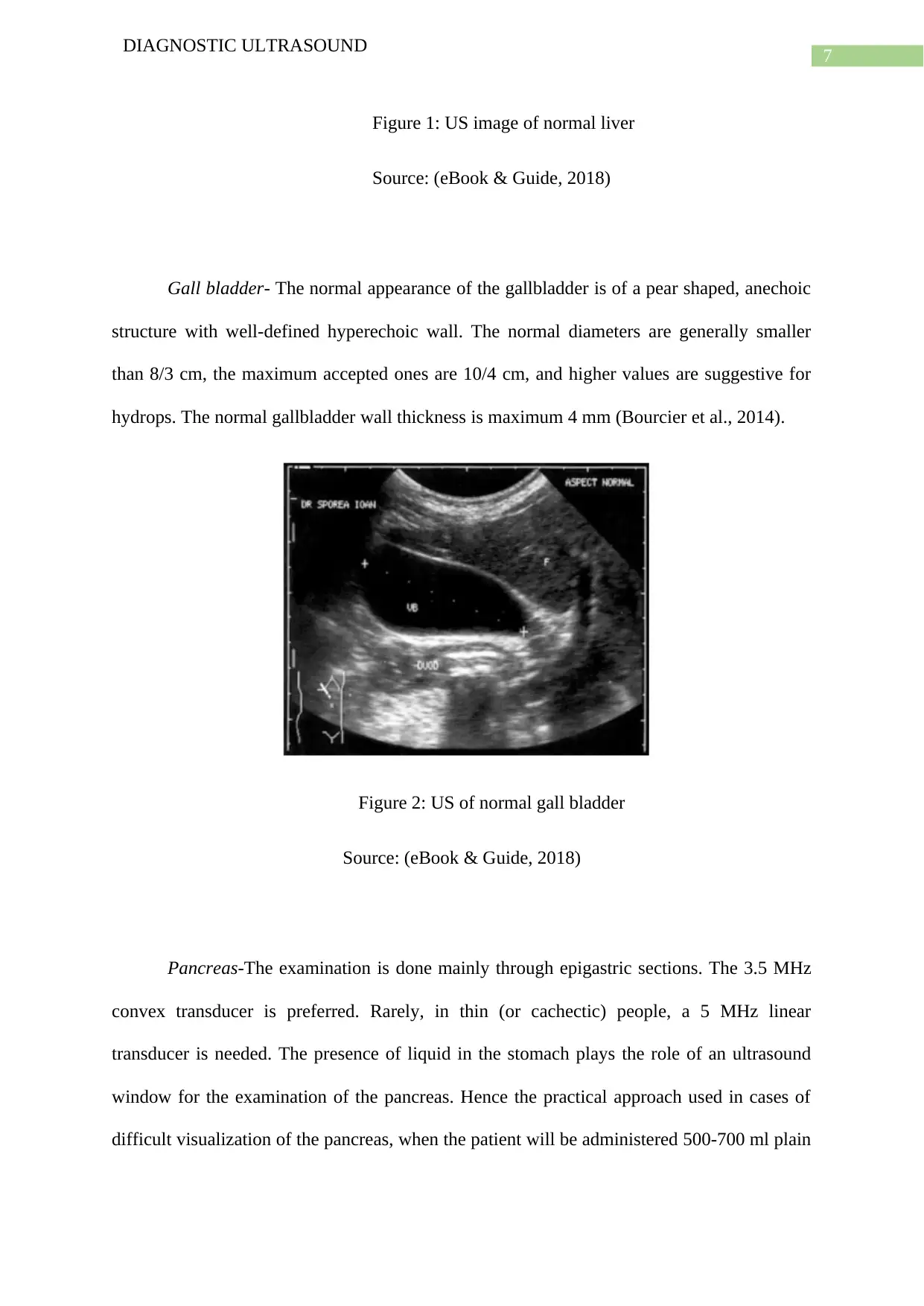
Pancreas-The examination is done mainly through epigastric sections. The 3.5 MHz
convex transducer is preferred. Rarely, in thin (or cachectic) people, a 5 MHz linear
transducer is needed. The presence of liquid in the stomach plays the role of an ultrasound
window for the examination of the pancreas. Hence the practical approach used in cases of
difficult visualization of the pancreas, when the patient will be administered 500-700 ml plain
DIAGNOSTIC ULTRASOUND
Figure 1: US image of normal liver
Source: (eBook & Guide, 2018)
Gall bladder- The normal appearance of the gallbladder is of a pear shaped, anechoic
structure with well-defined hyperechoic wall. The normal diameters are generally smaller
than 8/3 cm, the maximum accepted ones are 10/4 cm, and higher values are suggestive for
hydrops. The normal gallbladder wall thickness is maximum 4 mm (Bourcier et al., 2014).
Figure 2: US of normal gall bladder
Source: (eBook & Guide, 2018)
Pancreas-The examination is done mainly through epigastric sections. The 3.5 MHz
convex transducer is preferred. Rarely, in thin (or cachectic) people, a 5 MHz linear
transducer is needed. The presence of liquid in the stomach plays the role of an ultrasound
window for the examination of the pancreas. Hence the practical approach used in cases of
difficult visualization of the pancreas, when the patient will be administered 500-700 ml plain
8
DIAGNOSTIC ULTRASOUND
water or apple juice that will form an ultrasound window in the stomach (Mazzei et al.,
2013).
Figure 3: US of normal pancreas
Source: (eBook & Guide, 2018)
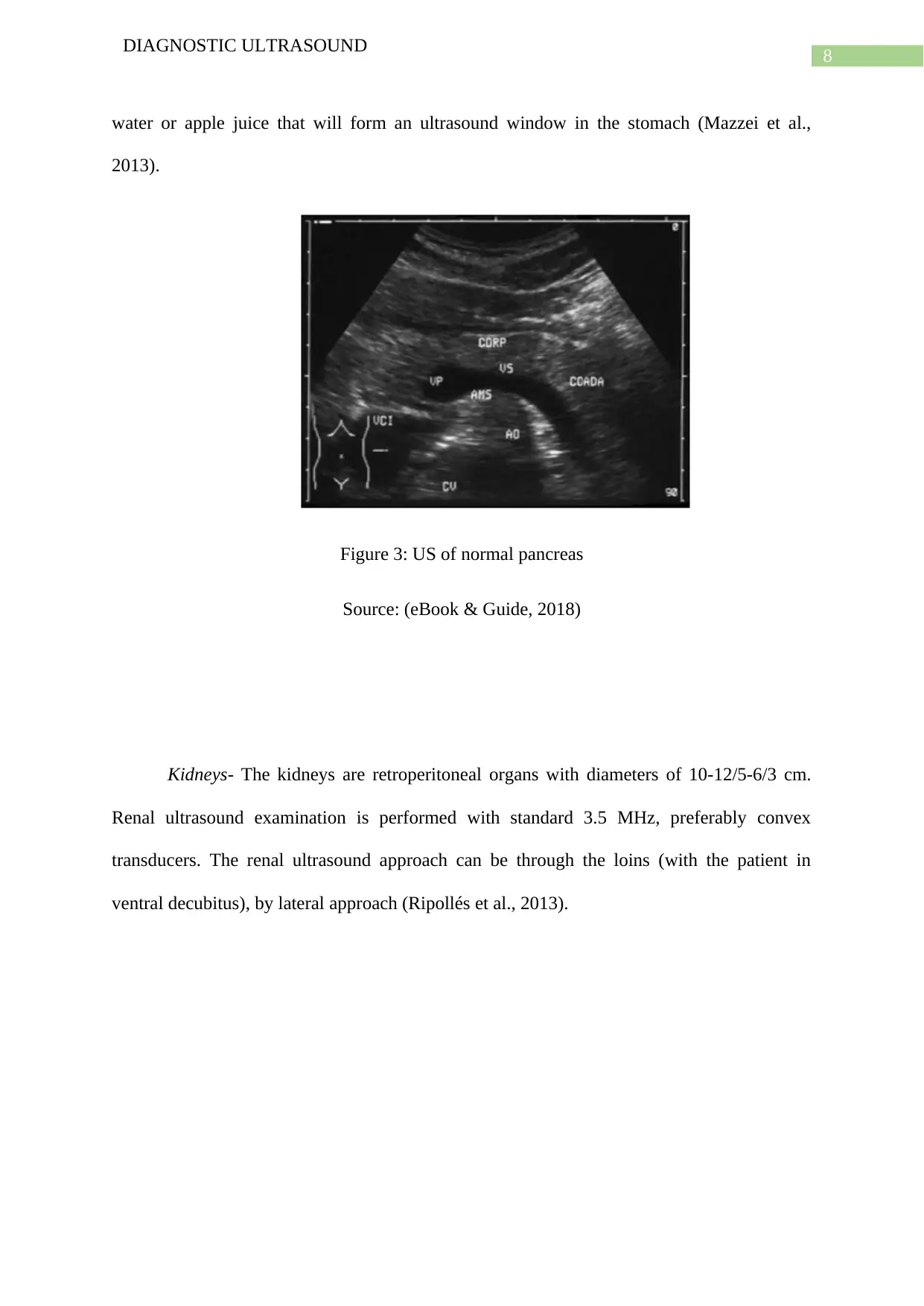
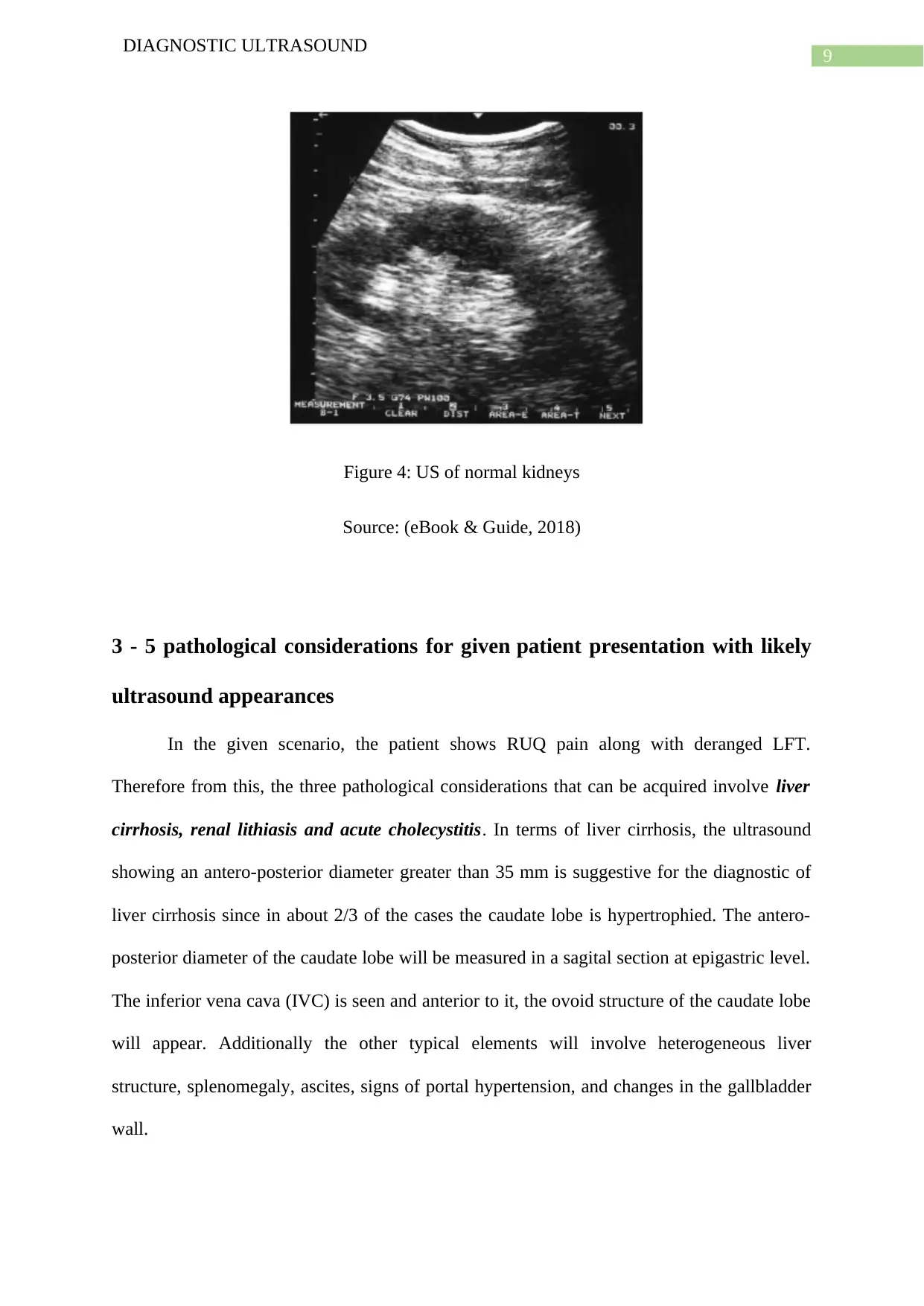
Kidneys- The kidneys are retroperitoneal organs with diameters of 10-12/5-6/3 cm.
Renal ultrasound examination is performed with standard 3.5 MHz, preferably convex
transducers. The renal ultrasound approach can be through the loins (with the patient in
ventral decubitus), by lateral approach (Ripollés et al., 2013).
DIAGNOSTIC ULTRASOUND
water or apple juice that will form an ultrasound window in the stomach (Mazzei et al.,
2013).
Figure 3: US of normal pancreas
Source: (eBook & Guide, 2018)
Kidneys- The kidneys are retroperitoneal organs with diameters of 10-12/5-6/3 cm.
Renal ultrasound examination is performed with standard 3.5 MHz, preferably convex
transducers. The renal ultrasound approach can be through the loins (with the patient in
ventral decubitus), by lateral approach (Ripollés et al., 2013).
9
DIAGNOSTIC ULTRASOUND
Figure 4: US of normal kidneys
Source: (eBook & Guide, 2018)
3 - 5 pathological considerations for given patient presentation with likely
ultrasound appearances
In the given scenario, the patient shows RUQ pain along with deranged LFT.
Therefore from this, the three pathological considerations that can be acquired involve liver
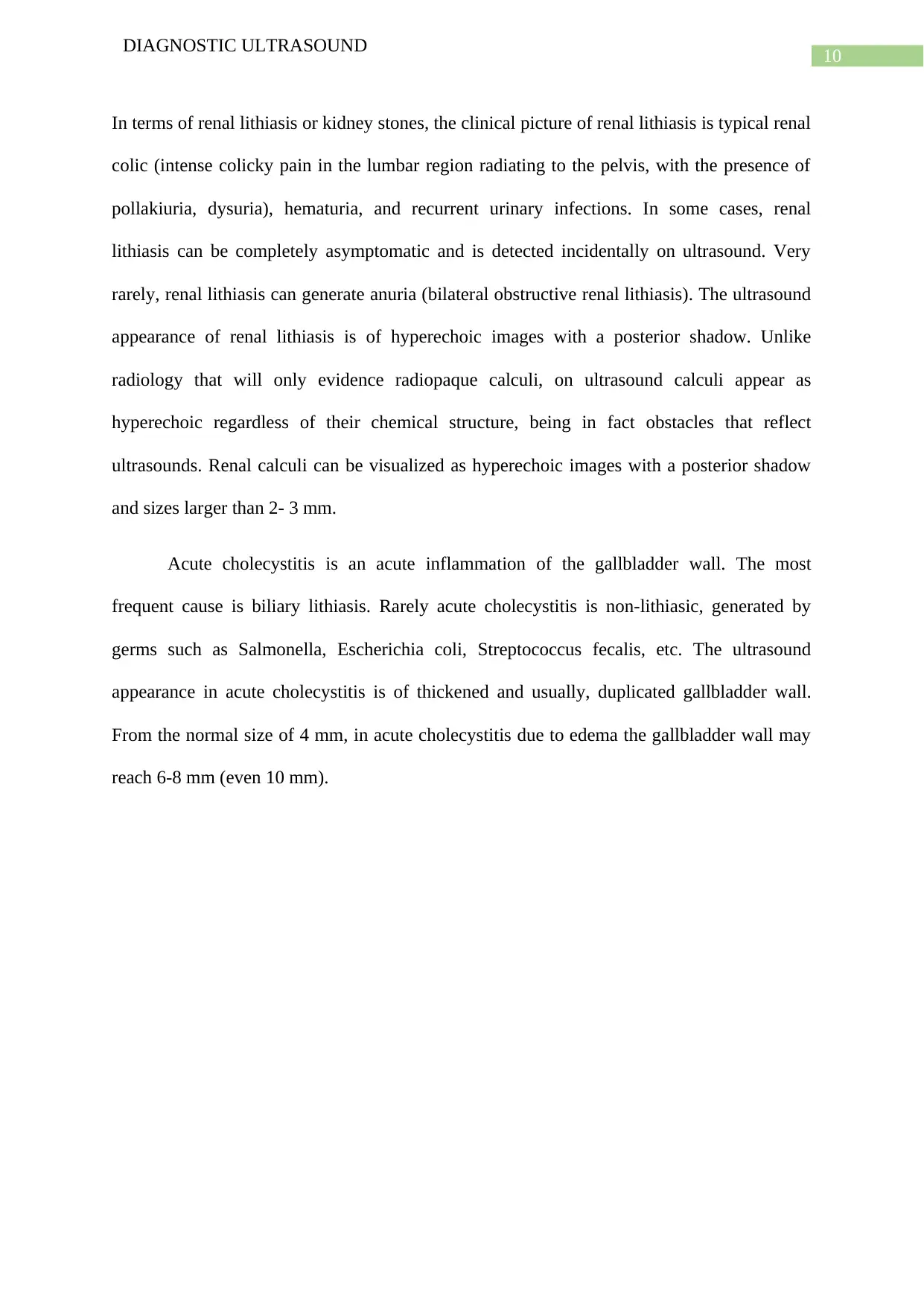
cirrhosis, renal lithiasis and acute cholecystitis. In terms of liver cirrhosis, the ultrasound
showing an antero-posterior diameter greater than 35 mm is suggestive for the diagnostic of
liver cirrhosis since in about 2/3 of the cases the caudate lobe is hypertrophied. The antero-
posterior diameter of the caudate lobe will be measured in a sagital section at epigastric level.
The inferior vena cava (IVC) is seen and anterior to it, the ovoid structure of the caudate lobe
will appear. Additionally the other typical elements will involve heterogeneous liver
structure, splenomegaly, ascites, signs of portal hypertension, and changes in the gallbladder
wall.
DIAGNOSTIC ULTRASOUND
Figure 4: US of normal kidneys
Source: (eBook & Guide, 2018)
3 - 5 pathological considerations for given patient presentation with likely
ultrasound appearances
In the given scenario, the patient shows RUQ pain along with deranged LFT.
Therefore from this, the three pathological considerations that can be acquired involve liver
cirrhosis, renal lithiasis and acute cholecystitis. In terms of liver cirrhosis, the ultrasound
showing an antero-posterior diameter greater than 35 mm is suggestive for the diagnostic of
liver cirrhosis since in about 2/3 of the cases the caudate lobe is hypertrophied. The antero-
posterior diameter of the caudate lobe will be measured in a sagital section at epigastric level.
The inferior vena cava (IVC) is seen and anterior to it, the ovoid structure of the caudate lobe
will appear. Additionally the other typical elements will involve heterogeneous liver
structure, splenomegaly, ascites, signs of portal hypertension, and changes in the gallbladder
wall.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
10
DIAGNOSTIC ULTRASOUND
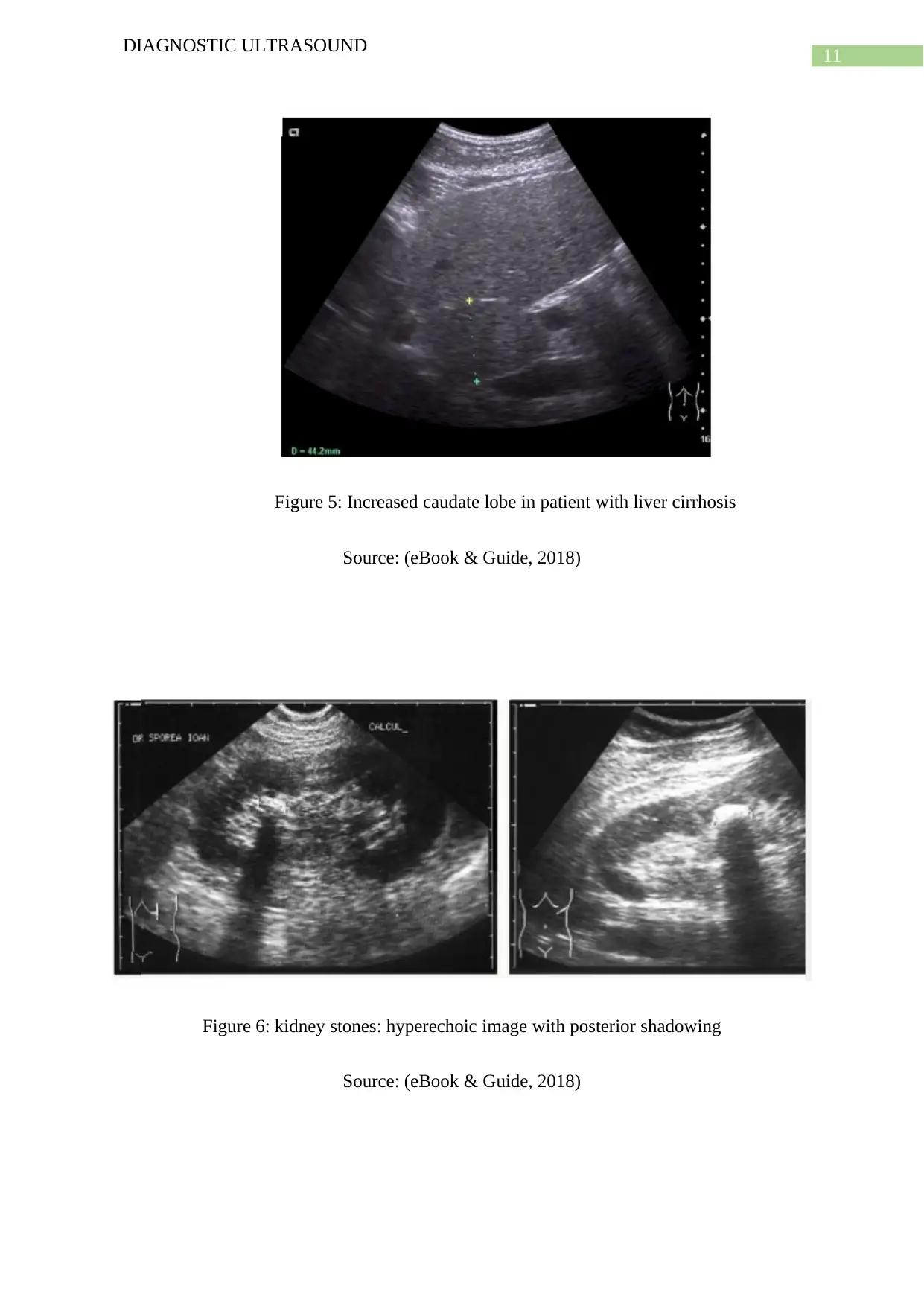
In terms of renal lithiasis or kidney stones, the clinical picture of renal lithiasis is typical renal
colic (intense colicky pain in the lumbar region radiating to the pelvis, with the presence of
pollakiuria, dysuria), hematuria, and recurrent urinary infections. In some cases, renal
lithiasis can be completely asymptomatic and is detected incidentally on ultrasound. Very
rarely, renal lithiasis can generate anuria (bilateral obstructive renal lithiasis). The ultrasound
appearance of renal lithiasis is of hyperechoic images with a posterior shadow. Unlike
radiology that will only evidence radiopaque calculi, on ultrasound calculi appear as
hyperechoic regardless of their chemical structure, being in fact obstacles that reflect
ultrasounds. Renal calculi can be visualized as hyperechoic images with a posterior shadow
and sizes larger than 2- 3 mm.
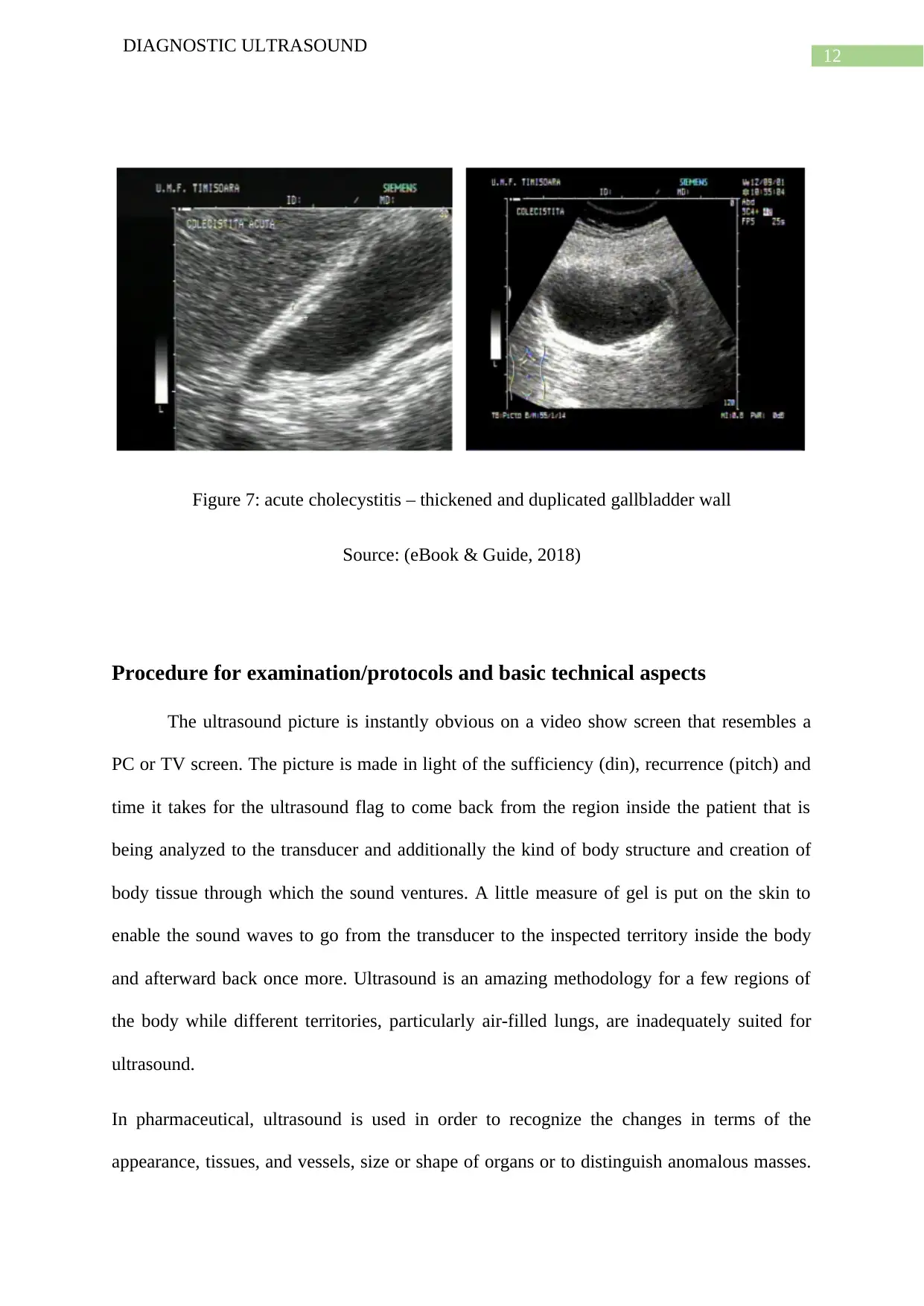
Acute cholecystitis is an acute inflammation of the gallbladder wall. The most
frequent cause is biliary lithiasis. Rarely acute cholecystitis is non-lithiasic, generated by
germs such as Salmonella, Escherichia coli, Streptococcus fecalis, etc. The ultrasound
appearance in acute cholecystitis is of thickened and usually, duplicated gallbladder wall.
From the normal size of 4 mm, in acute cholecystitis due to edema the gallbladder wall may
reach 6-8 mm (even 10 mm).
DIAGNOSTIC ULTRASOUND
In terms of renal lithiasis or kidney stones, the clinical picture of renal lithiasis is typical renal
colic (intense colicky pain in the lumbar region radiating to the pelvis, with the presence of
pollakiuria, dysuria), hematuria, and recurrent urinary infections. In some cases, renal
lithiasis can be completely asymptomatic and is detected incidentally on ultrasound. Very
rarely, renal lithiasis can generate anuria (bilateral obstructive renal lithiasis). The ultrasound
appearance of renal lithiasis is of hyperechoic images with a posterior shadow. Unlike
radiology that will only evidence radiopaque calculi, on ultrasound calculi appear as
hyperechoic regardless of their chemical structure, being in fact obstacles that reflect
ultrasounds. Renal calculi can be visualized as hyperechoic images with a posterior shadow
and sizes larger than 2- 3 mm.
Acute cholecystitis is an acute inflammation of the gallbladder wall. The most
frequent cause is biliary lithiasis. Rarely acute cholecystitis is non-lithiasic, generated by
germs such as Salmonella, Escherichia coli, Streptococcus fecalis, etc. The ultrasound
appearance in acute cholecystitis is of thickened and usually, duplicated gallbladder wall.
From the normal size of 4 mm, in acute cholecystitis due to edema the gallbladder wall may
reach 6-8 mm (even 10 mm).
11
DIAGNOSTIC ULTRASOUND
Figure 5: Increased caudate lobe in patient with liver cirrhosis
Source: (eBook & Guide, 2018)
Figure 6: kidney stones: hyperechoic image with posterior shadowing
Source: (eBook & Guide, 2018)
DIAGNOSTIC ULTRASOUND
Figure 5: Increased caudate lobe in patient with liver cirrhosis
Source: (eBook & Guide, 2018)
Figure 6: kidney stones: hyperechoic image with posterior shadowing
Source: (eBook & Guide, 2018)
12
DIAGNOSTIC ULTRASOUND
Figure 7: acute cholecystitis – thickened and duplicated gallbladder wall
Source: (eBook & Guide, 2018)
Procedure for examination/protocols and basic technical aspects
The ultrasound picture is instantly obvious on a video show screen that resembles a
PC or TV screen. The picture is made in light of the sufficiency (din), recurrence (pitch) and
time it takes for the ultrasound flag to come back from the region inside the patient that is
being analyzed to the transducer and additionally the kind of body structure and creation of
body tissue through which the sound ventures. A little measure of gel is put on the skin to
enable the sound waves to go from the transducer to the inspected territory inside the body
and afterward back once more. Ultrasound is an amazing methodology for a few regions of
the body while different territories, particularly air-filled lungs, are inadequately suited for
ultrasound.
In pharmaceutical, ultrasound is used in order to recognize the changes in terms of the
appearance, tissues, and vessels, size or shape of organs or to distinguish anomalous masses.
DIAGNOSTIC ULTRASOUND
Figure 7: acute cholecystitis – thickened and duplicated gallbladder wall
Source: (eBook & Guide, 2018)
Procedure for examination/protocols and basic technical aspects
The ultrasound picture is instantly obvious on a video show screen that resembles a
PC or TV screen. The picture is made in light of the sufficiency (din), recurrence (pitch) and
time it takes for the ultrasound flag to come back from the region inside the patient that is
being analyzed to the transducer and additionally the kind of body structure and creation of
body tissue through which the sound ventures. A little measure of gel is put on the skin to
enable the sound waves to go from the transducer to the inspected territory inside the body
and afterward back once more. Ultrasound is an amazing methodology for a few regions of
the body while different territories, particularly air-filled lungs, are inadequately suited for
ultrasound.
In pharmaceutical, ultrasound is used in order to recognize the changes in terms of the
appearance, tissues, and vessels, size or shape of organs or to distinguish anomalous masses.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
13
DIAGNOSTIC ULTRASOUND
The examples include tumours. Ultrasound examination involves a transducer that sends the
sound waves into the body in addition to getting the reverberating waves. In the scenario
where the transducer is pressed against the skin of the patient, it develops coordinates of little
beats which are quiet and cause high-recurrence sound waves into the body. The sound waves
bob off inside organs, tissues and the liquids, which in turn cause the recipient in the
transducer records to develop minor changes in the sound's pitch and bearing. The developed
mark waves then repairs in a split and in a second is estimated and shown by a PC, which
thus makes an ongoing picture on the screen. At least one edge of the moving pictures is
commonly caught as still pictures. Short video circles of the pictures may likewise be spared.
Doppler ultrasound, an uncommon use of ultrasound, measures the heading and speed of
platelets as they travel through vessels. The development of platelets causes an adjustment in
pitch of the reflected sound waves which is known as the Doppler impact. A PC is involved
in gathering the procedures the sounds and making of charts or shading pictures that speak to
the stream of blood through the veins (Joshi et al., 2013).
Alternative procedures
Ultrasound is required to be done all together decide if a lady is at an adequately early
gestational age with the end goal that mifepristone– misoprostol has a high possibility of
success. Previous explore has demonstrated a high connection between's pregnancy dating
dictated by clinician and that controlled by sonography. It was found that reports of LMP and
physical examination, as opposed to ultrasound, to decide qualification for restorative end of
pregnancy would have brought about 1.6% of ladies getting medicinal end of pregnancy at a
gestational age past the customary cut‐off for early therapeutic end of pregnancy conventions
(Koenig et al., 2014).
DIAGNOSTIC ULTRASOUND
The examples include tumours. Ultrasound examination involves a transducer that sends the
sound waves into the body in addition to getting the reverberating waves. In the scenario
where the transducer is pressed against the skin of the patient, it develops coordinates of little
beats which are quiet and cause high-recurrence sound waves into the body. The sound waves
bob off inside organs, tissues and the liquids, which in turn cause the recipient in the
transducer records to develop minor changes in the sound's pitch and bearing. The developed
mark waves then repairs in a split and in a second is estimated and shown by a PC, which
thus makes an ongoing picture on the screen. At least one edge of the moving pictures is
commonly caught as still pictures. Short video circles of the pictures may likewise be spared.
Doppler ultrasound, an uncommon use of ultrasound, measures the heading and speed of
platelets as they travel through vessels. The development of platelets causes an adjustment in
pitch of the reflected sound waves which is known as the Doppler impact. A PC is involved
in gathering the procedures the sounds and making of charts or shading pictures that speak to
the stream of blood through the veins (Joshi et al., 2013).
Alternative procedures
Ultrasound is required to be done all together decide if a lady is at an adequately early
gestational age with the end goal that mifepristone– misoprostol has a high possibility of
success. Previous explore has demonstrated a high connection between's pregnancy dating
dictated by clinician and that controlled by sonography. It was found that reports of LMP and
physical examination, as opposed to ultrasound, to decide qualification for restorative end of
pregnancy would have brought about 1.6% of ladies getting medicinal end of pregnancy at a
gestational age past the customary cut‐off for early therapeutic end of pregnancy conventions
(Koenig et al., 2014).

14
DIAGNOSTIC ULTRASOUND
Possible or likely outcomes for the patient
The likely outcome of the patient was that after conduction of the ultrasound, the patient was
most likely to be diagnosed with kidney problems since he was experiencing pain in the right
upper quadrant of the abdomen. Additionally it might be problems of liver cirrhosis or gall
bladder as the patient showed deranged LFT results.
DIAGNOSTIC ULTRASOUND
Possible or likely outcomes for the patient
The likely outcome of the patient was that after conduction of the ultrasound, the patient was
most likely to be diagnosed with kidney problems since he was experiencing pain in the right
upper quadrant of the abdomen. Additionally it might be problems of liver cirrhosis or gall
bladder as the patient showed deranged LFT results.
15
DIAGNOSTIC ULTRASOUND
References
Bahner, D. P., Adkins, E. J., Hughes, D., Barrie, M., Boulger, C. T., & Royall, N. A. (2013).
Integrated medical school ultrasound: development of an ultrasound vertical
curriculum. Critical ultrasound journal, 5(1), 6.
Bohnhorst, B. (2013). Usefulness of abdominal ultrasound in diagnosing necrotising
enterocolitis. Archives of Disease in Childhood-Fetal and Neonatal Edition, 98(5),
F445-F450.
Bourcier, J. E., Paquet, J., Seinger, M., Gallard, E., Redonnet, J. P., Cheddadi, F., ... &
Geeraerts, T. (2014). Performance comparison of lung ultrasound and chest x-ray for
the diagnosis of pneumonia in the ED. The American journal of emergency
medicine, 32(2), 115-118.
Callen, P. W., & Norton, M. E. (2016). The obstetric ultrasound
examination. Ultrasonography in obstetrics and gynecology, 1-17.
Joshi, N., Lira, A., Mehta, N., Paladino, L., & Sinert, R. (2013). Diagnostic accuracy of
history, physical examination, and bedside ultrasound for diagnosis of extremity
fractures in the emergency department: a systematic review. Academic Emergency
Medicine, 20(1), 1-15.
Koenig, S., Chandra, S., Alaverdian, A., Dibello, C., Mayo, P. H., & Narasimhan, M. (2014).
Ultrasound assessment of pulmonary embolism in patients receiving CT pulmonary
angiography. Chest, 145(4), 818-823.
DIAGNOSTIC ULTRASOUND
References
Bahner, D. P., Adkins, E. J., Hughes, D., Barrie, M., Boulger, C. T., & Royall, N. A. (2013).
Integrated medical school ultrasound: development of an ultrasound vertical
curriculum. Critical ultrasound journal, 5(1), 6.
Bohnhorst, B. (2013). Usefulness of abdominal ultrasound in diagnosing necrotising
enterocolitis. Archives of Disease in Childhood-Fetal and Neonatal Edition, 98(5),
F445-F450.
Bourcier, J. E., Paquet, J., Seinger, M., Gallard, E., Redonnet, J. P., Cheddadi, F., ... &
Geeraerts, T. (2014). Performance comparison of lung ultrasound and chest x-ray for
the diagnosis of pneumonia in the ED. The American journal of emergency
medicine, 32(2), 115-118.
Callen, P. W., & Norton, M. E. (2016). The obstetric ultrasound
examination. Ultrasonography in obstetrics and gynecology, 1-17.
Joshi, N., Lira, A., Mehta, N., Paladino, L., & Sinert, R. (2013). Diagnostic accuracy of
history, physical examination, and bedside ultrasound for diagnosis of extremity
fractures in the emergency department: a systematic review. Academic Emergency
Medicine, 20(1), 1-15.
Koenig, S., Chandra, S., Alaverdian, A., Dibello, C., Mayo, P. H., & Narasimhan, M. (2014).
Ultrasound assessment of pulmonary embolism in patients receiving CT pulmonary
angiography. Chest, 145(4), 818-823.
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
16
DIAGNOSTIC ULTRASOUND
Mazzei, M. A., Guerrini, S., Squitieri, N. C., Cagini, L., Macarini, L., Coppolino, F., ... &
Volterrani, L. (2013). The role of US examination in the management of acute
abdomen. Critical ultrasound journal, 5(S1), S6.
Mouratev, G., Howe, D., Hoppmann, R., Poston, M. B., Reid, R., Varnadoe, J., ... &
DeMarco, P. (2013). Teaching medical students ultrasound to measure liver size:
comparison with experienced clinicians using physical examination alone. Teaching
and learning in medicine, 25(1), 84-88.
O’Dochartaigh, D., & Douma, M. (2015). Prehospital ultrasound of the abdomen and thorax
changes trauma patient management: A systematic review. Injury, 46(11), 2093-2102.
Ripollés, T., Martínez-Pérez, M. J., Paredes, J. M., Vizuete, J., García-Martínez, E., &
Jiménez-Restrepo, D. H. (2013). Contrast-enhanced ultrasound in the differentiation
between phlegmon and abscess in Crohn's disease and other abdominal
conditions. European journal of radiology, 82(10), e525-e531.
Sessa, B., Trinci, M., Ianniello, S., Menichini, G., Galluzzo, M., & Miele, V. (2015). Blunt
abdominal trauma: role of contrast-enhanced ultrasound (CEUS) in the detection and
staging of abdominal traumatic lesions compared to US and CE-MDCT. La
radiologia medica, 120(2), 180-189.
Wax, J., Minkoff, H., Johnson, A., Coleman, B., Levine, D., Helfgott, A., ... & Benson, C.
(2014). Consensus report on the detailed fetal anatomic ultrasound examination:
indications, components, and qualifications. Journal of Ultrasound in
Medicine, 33(2), 189-195.
eBook, &., & Guide), A. (2018). Abdominal Ultrasound (Full Guide) – "The" Med Student
Ultrasound eBook. Retrieved from http://lluultrasound.org/home/ebook/original-
abdominal/
DIAGNOSTIC ULTRASOUND
Mazzei, M. A., Guerrini, S., Squitieri, N. C., Cagini, L., Macarini, L., Coppolino, F., ... &
Volterrani, L. (2013). The role of US examination in the management of acute
abdomen. Critical ultrasound journal, 5(S1), S6.
Mouratev, G., Howe, D., Hoppmann, R., Poston, M. B., Reid, R., Varnadoe, J., ... &
DeMarco, P. (2013). Teaching medical students ultrasound to measure liver size:
comparison with experienced clinicians using physical examination alone. Teaching
and learning in medicine, 25(1), 84-88.
O’Dochartaigh, D., & Douma, M. (2015). Prehospital ultrasound of the abdomen and thorax
changes trauma patient management: A systematic review. Injury, 46(11), 2093-2102.
Ripollés, T., Martínez-Pérez, M. J., Paredes, J. M., Vizuete, J., García-Martínez, E., &
Jiménez-Restrepo, D. H. (2013). Contrast-enhanced ultrasound in the differentiation
between phlegmon and abscess in Crohn's disease and other abdominal
conditions. European journal of radiology, 82(10), e525-e531.
Sessa, B., Trinci, M., Ianniello, S., Menichini, G., Galluzzo, M., & Miele, V. (2015). Blunt
abdominal trauma: role of contrast-enhanced ultrasound (CEUS) in the detection and
staging of abdominal traumatic lesions compared to US and CE-MDCT. La
radiologia medica, 120(2), 180-189.
Wax, J., Minkoff, H., Johnson, A., Coleman, B., Levine, D., Helfgott, A., ... & Benson, C.
(2014). Consensus report on the detailed fetal anatomic ultrasound examination:
indications, components, and qualifications. Journal of Ultrasound in
Medicine, 33(2), 189-195.
eBook, &., & Guide), A. (2018). Abdominal Ultrasound (Full Guide) – "The" Med Student
Ultrasound eBook. Retrieved from http://lluultrasound.org/home/ebook/original-
abdominal/
1 out of 17



Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.