Importance of Hand Hygiene in Controlling Hospital Acquired Infections
VerifiedAI Summary
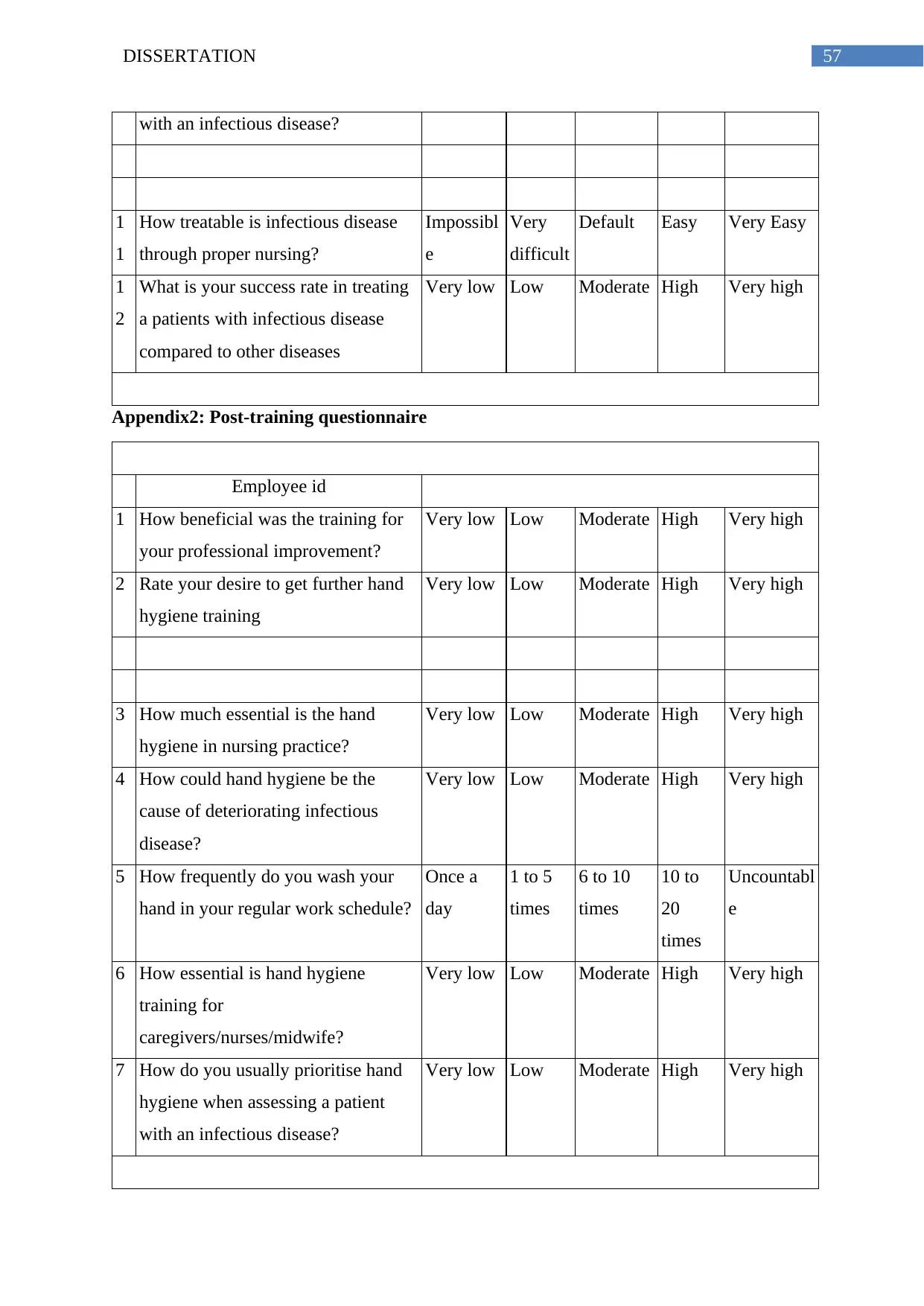
This dissertation explores the importance of hand hygiene in controlling hospital acquired infections. It discusses the high morbidity and mortality rates associated with these infections and the role of hand hygiene in preventing their transmission. The research aims to evaluate the existing perception of hand hygiene among care professionals and investigate the effectiveness of an awareness workshop in changing their perceptions. The study also aims to assess the changes in perception and behavior after the training program on hand hygiene. The literature review section provides an overview of the existing research on hand hygiene and its implications for infection control.
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)