Literature Review: HIV, Anxiety, Depression, and Emotional Health
VerifiedAdded on 2019/10/18
|38
|12852
|342
Report
AI Summary
This report presents a comprehensive literature review examining the intricate relationship between HIV/AIDS and mental health, specifically focusing on anxiety, depression, and related emotional distress experienced by patients. The review synthesizes findings from various sources, including studies on the neurobiological impact of HIV, the influence of treatment regimens, and the role of socioeconomic factors. It highlights the significance of social support and the detrimental effects of HIV-related stigma on patients' psychological well-being. The report discusses the impact of anxiety and depression on medication adherence and overall health outcomes. Furthermore, it emphasizes the need for psychosocial interventions and family-centered care to mitigate the burden of HIV and improve the quality of life for both patients and their families. The report also points out the gaps in current research and suggests directions for future investigations, particularly in identifying the underlying mechanisms of mental illness in HIV victims.
Does evidence suggest that HIV patients suffer from related emotions,
anxiety and depression?
Abstract
HIV infection has developed as one of the real difficulties of the current world. Regardless
of, awareness and education about this disease, a HIV patient is still thought to be a social
outcaste and is dealt with intensely by the group on the loose. HIV/AIDS has picked up
conspicuousness over the world as a developing general wellbeing issue. There is a complex
yet huge connection between psychological wellness and HIV/AIDS. HIV influences
psychological wellness by its direct neurobiological activity, the effect of having the ailment,
by its treatment including that for opportunistic infections and by its effect on the family. In
addition, the presence of multiple diseases due to suppression of immunity is an additional
variable that add to the unpredictability of evaluation, differential analysis and disease
management. The dissertation describes the searching of literature, review of literature and its
critique. The literature from diverse sources was collected, reviewed and the essentials of the
literature were collated. The outcome based on evidences was discussed for the effect of HIV
mediated anxiety, depression, or emotion on medication/therapy was discussed. The effect of
socioeconomic conditions on anxiety in HIV infected patients was elaborated along with the
possible factors that influence the lifespan of HIV victims. The disease has incurred
significant injury on communities, bringing about high dismalness and mortality. The
casualties of HIV convey the burden of being caretakers for individual who infected with
HIV while also stressing over their own particular wellbeing; be that as it may, little is
thought about how HIV/AIDS influences mental illness among patients. The patients who
reported more worry over being infected with HIV and more greater HIV-related stigma were
critically more inclined to report more prominent symptoms of anxiety and depression. These
1
anxiety and depression?
Abstract
HIV infection has developed as one of the real difficulties of the current world. Regardless
of, awareness and education about this disease, a HIV patient is still thought to be a social
outcaste and is dealt with intensely by the group on the loose. HIV/AIDS has picked up
conspicuousness over the world as a developing general wellbeing issue. There is a complex
yet huge connection between psychological wellness and HIV/AIDS. HIV influences
psychological wellness by its direct neurobiological activity, the effect of having the ailment,
by its treatment including that for opportunistic infections and by its effect on the family. In
addition, the presence of multiple diseases due to suppression of immunity is an additional
variable that add to the unpredictability of evaluation, differential analysis and disease
management. The dissertation describes the searching of literature, review of literature and its
critique. The literature from diverse sources was collected, reviewed and the essentials of the
literature were collated. The outcome based on evidences was discussed for the effect of HIV
mediated anxiety, depression, or emotion on medication/therapy was discussed. The effect of
socioeconomic conditions on anxiety in HIV infected patients was elaborated along with the
possible factors that influence the lifespan of HIV victims. The disease has incurred
significant injury on communities, bringing about high dismalness and mortality. The
casualties of HIV convey the burden of being caretakers for individual who infected with
HIV while also stressing over their own particular wellbeing; be that as it may, little is
thought about how HIV/AIDS influences mental illness among patients. The patients who
reported more worry over being infected with HIV and more greater HIV-related stigma were
critically more inclined to report more prominent symptoms of anxiety and depression. These
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
discoveries propose that mediations that decrease HIV-related stigma are probably going to
upgrade psychological function among the patients, which thus will enhance the patient's
personal satisfaction and prosperity. Diverse factors that contribute for mental illnesses
include gender, socioeconomic status, society and culture. In conclusion, studies have
reported depression, anxiety and emotional distress are being the most common psychiatric
morbidities among the afflicted individuals separately. No study dealt with the combination
of mental illnesses in HIV victims. It appears that no article describes the underlying
mechanisms of mental illness in HIV victims. In addition, there is a more requirement for
psychosocial support for HIV-influenced families inside the setting of growing HIV-related
services in healthcare system. The psychosocial mediations among HIV-influenced families
also upgrade the viability for the alleviation of disease manifestations and in order to decrease
the side effects of emotional sickness. A holistic approach to deal with HIV anticipation and
care (coordinated administrations that are family-engaged) that addresses the family's needs
(supporting guardians/parental figures, advancing family working, tending to physical and in
addition emotional well-being requirements, and offering money related support when
required) and additionally the wide scope of requirements for children (access to class,
physical wellbeing needs, advancement of psychological well-being), might be important to
decrease the burden the HIV infection and minimize the negative consequences of HIV
infection for present and future eras. Future research should focus the investigations to
identifying the underlying causes and mechanisms.
2
upgrade psychological function among the patients, which thus will enhance the patient's
personal satisfaction and prosperity. Diverse factors that contribute for mental illnesses
include gender, socioeconomic status, society and culture. In conclusion, studies have
reported depression, anxiety and emotional distress are being the most common psychiatric
morbidities among the afflicted individuals separately. No study dealt with the combination
of mental illnesses in HIV victims. It appears that no article describes the underlying
mechanisms of mental illness in HIV victims. In addition, there is a more requirement for
psychosocial support for HIV-influenced families inside the setting of growing HIV-related
services in healthcare system. The psychosocial mediations among HIV-influenced families
also upgrade the viability for the alleviation of disease manifestations and in order to decrease
the side effects of emotional sickness. A holistic approach to deal with HIV anticipation and
care (coordinated administrations that are family-engaged) that addresses the family's needs
(supporting guardians/parental figures, advancing family working, tending to physical and in
addition emotional well-being requirements, and offering money related support when
required) and additionally the wide scope of requirements for children (access to class,
physical wellbeing needs, advancement of psychological well-being), might be important to
decrease the burden the HIV infection and minimize the negative consequences of HIV
infection for present and future eras. Future research should focus the investigations to
identifying the underlying causes and mechanisms.
2
CHAPTER-1
1.1 Literature review
During past few decades, researchers have shown great interest in the phenomena of social
support, particularly in the context of health. According to reports (Maija & Bert, 2008), the
high quality or quantity of social networks have a decreased risk of mortality in comparison
to those who have low quantity or quality of social relationships. Especially the support is
needed for certain diseases like human immunodeficiency virus/acquired immune deficiency
syndrome (HIV/AIDS). HIV/AIDS is confined neither to any one class, community, religion,
age, gender, and group nor to a profession. Therefore, it is the major concern of health
psychologists to fight with AIDS because it is a major health problem of this century (Lefton,
1997). The AIDS is one of the most dreaded diseases that mainly impair body’s immune
system to fight bacteria, viruses, cancer, etc, (Lahey, 1997). Following exposure to HIV, the
person is vulnerable to germs that a normal immune system could destroy. HIV can be
transmitted through sexual/contact or from mother to child through the placenta or by transfer
of whole blood or blood product. However, it is important to note that social support in case
of AIDS is operationalized in several different ways. Most broadly, support can be
conceptualized in terms of the structural components (e.g. social integration). Despite of
marginal support from society, individual with HIV/AIDS experience the threat of major
negative life events and medical conditions. According to reports, the HIV/AIDS patients
could show diverse effects on individual health and wealth including, premature death,
physical disability and pain, loss of employment, social isolation, coasts of medical
treatment, anxiety for future of family members (Alpana & Ila, 2010). Early reports of
psychological responses of HIV infection revealed pervasive feelings of anxiety and
depression (Fleishman & Fugal, 1994). Depression is either mood of clinical syndrome, such
as emotional, motivational, cognitive, somatic or behavioral (Sarason & Sarason, 2000). The
3
1.1 Literature review
During past few decades, researchers have shown great interest in the phenomena of social
support, particularly in the context of health. According to reports (Maija & Bert, 2008), the
high quality or quantity of social networks have a decreased risk of mortality in comparison
to those who have low quantity or quality of social relationships. Especially the support is
needed for certain diseases like human immunodeficiency virus/acquired immune deficiency
syndrome (HIV/AIDS). HIV/AIDS is confined neither to any one class, community, religion,
age, gender, and group nor to a profession. Therefore, it is the major concern of health
psychologists to fight with AIDS because it is a major health problem of this century (Lefton,
1997). The AIDS is one of the most dreaded diseases that mainly impair body’s immune
system to fight bacteria, viruses, cancer, etc, (Lahey, 1997). Following exposure to HIV, the
person is vulnerable to germs that a normal immune system could destroy. HIV can be
transmitted through sexual/contact or from mother to child through the placenta or by transfer
of whole blood or blood product. However, it is important to note that social support in case
of AIDS is operationalized in several different ways. Most broadly, support can be
conceptualized in terms of the structural components (e.g. social integration). Despite of
marginal support from society, individual with HIV/AIDS experience the threat of major
negative life events and medical conditions. According to reports, the HIV/AIDS patients
could show diverse effects on individual health and wealth including, premature death,
physical disability and pain, loss of employment, social isolation, coasts of medical
treatment, anxiety for future of family members (Alpana & Ila, 2010). Early reports of
psychological responses of HIV infection revealed pervasive feelings of anxiety and
depression (Fleishman & Fugal, 1994). Depression is either mood of clinical syndrome, such
as emotional, motivational, cognitive, somatic or behavioral (Sarason & Sarason, 2000). The
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
feeling associated with a depressed mood includes disappointment, helplessness and
hopelessness (Comer, 1995). It indicates that patients with HIV can undergo for diverse complications in
terms of alterations in health condition due to the development of negative thoughts. Therefore, it is desired to
investigate the possible factors that contribute for such emotional distress. This section describes the search strategy
in brief and reviews of available literature.
1.2. Search strategy
The available and popular sources were used to search for the evidences. The sources, diverse online electronic
resources including BNI (British Nursing Index), CINAHL (Cumulative Index to Nursing and
Allied Health Literature), EMBASE (the Excerpta Medica database), Pubmed, The DARE
(Database of Abstracts of Reviews of Effects), HTA (Health Technology Assessment Database) and NHS
(Economic Evaluation Database). The search was made for past 30 years to collect the relevant
sources and link the evidences to the current context. In addition, the available textbooks
(pharmacology, nursing, health education) from the library were also searched for the
evidences. Satisfactory safety measures were made to channel the quest for the pertinent
sources. The keywords utilized for the pursuit incorporate "HIV/AIDS effect on emotion,
negative life occasions, premature death, physical disability, loss of employment, social
isolation, anxiety and depression etc. The outcome of the search for the relevant sources has
been depicted in subsequent sections.
1.3. Effect of HIV mediated anxiety on medication/therapy
Blank et al (2011) investigated the effect of the interventions from the community-based
advanced practice nurse (APN) to promote adherence to HIV and psychiatric treatment
regimens. The investigators conducted a randomized clinical trial utilizing 238 AIDS patients
with mental illnesses. The APNs who were involved in intervention for the patients are
assessed for the mental status and AIDS for 12 months. The intervention group showed a
4
hopelessness (Comer, 1995). It indicates that patients with HIV can undergo for diverse complications in
terms of alterations in health condition due to the development of negative thoughts. Therefore, it is desired to
investigate the possible factors that contribute for such emotional distress. This section describes the search strategy
in brief and reviews of available literature.
1.2. Search strategy
The available and popular sources were used to search for the evidences. The sources, diverse online electronic
resources including BNI (British Nursing Index), CINAHL (Cumulative Index to Nursing and
Allied Health Literature), EMBASE (the Excerpta Medica database), Pubmed, The DARE
(Database of Abstracts of Reviews of Effects), HTA (Health Technology Assessment Database) and NHS
(Economic Evaluation Database). The search was made for past 30 years to collect the relevant
sources and link the evidences to the current context. In addition, the available textbooks
(pharmacology, nursing, health education) from the library were also searched for the
evidences. Satisfactory safety measures were made to channel the quest for the pertinent
sources. The keywords utilized for the pursuit incorporate "HIV/AIDS effect on emotion,
negative life occasions, premature death, physical disability, loss of employment, social
isolation, anxiety and depression etc. The outcome of the search for the relevant sources has
been depicted in subsequent sections.
1.3. Effect of HIV mediated anxiety on medication/therapy
Blank et al (2011) investigated the effect of the interventions from the community-based
advanced practice nurse (APN) to promote adherence to HIV and psychiatric treatment
regimens. The investigators conducted a randomized clinical trial utilizing 238 AIDS patients
with mental illnesses. The APNs who were involved in intervention for the patients are
assessed for the mental status and AIDS for 12 months. The intervention group showed a
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
significant decrease in viral burden. The authors demonstrated that nursing interventions are
showing positive impact in disease reduction. However, there are no details pertaining to the
type of mental illness in detail. Most aspects are related to assessment of severity of AIDS.
The focus towards the etiology behind the HIV for the mental disorders is missing. It was
also evident from other reports (Vitiello et al., 2003) that the about 20.3% of HIV-infected
patients who receiving medical care are associated with anxiety and other psychotic disorders
(panic disorder, 12.3%; post-traumatic stress disorder, 10.4%; generalized anxiety disorder,
2.8%). Among the patients most patients are consuming psychotropics however, half of the
patients did not receive medication for depressive disorders. Kuo et al., (2014) reported the data from
a cross-sectional survey of families in HIV-endemic South Africa. The researchers studied the relationship between
HIV impacts and caregiver anxiety. The patients included in the study comprises of either not caring of children
orphaned by AIDS; caring for a child orphaned by AIDS but not living with HIV or dual HIV effects. The
outcome of the study (Kuo et al., 2014) suggests that it was not caring for a child orphaned by AIDS per se that
increased risk for anxiety. In addition, female patients appear to be of high risk of anxiety due to negative actions
towards coping responses to stress (Rudolph, 2002) and etiological differences. Equally age can also increase the
risk for anxiety due to an increase in chronic health conditions (Schoevers et al., 2005) and neurological
changes. Due to associated thinking, the patients with positive HIV can develop psychological distress leading to
development of anxiety for instance. The symptoms of anxiety have to be relieved in order to promote and sustain
the health of infected person. In another study, it was quoted that the South African children and adolescents living in
HIV/AIDS-affected families are at elevated risk of both symptoms of anxiety and depressive symptoms (Boyes &
Cluver, 2015). The investigators opined that the poverty and HIV/AIDS-related stigma are as additional risk factors
towards negative mental health outcomes. The study contains youths from high HIV-pervasive groups in South
Africa were met and caught up one year later. Familial HIV/AIDS at pattern appraisal was not specifically
connected with psychological wellness results 1 year later. However, the researchers opined that the usage and
thorough assessment of intense programs in South African people group may enhance emotional wellness results
5
showing positive impact in disease reduction. However, there are no details pertaining to the
type of mental illness in detail. Most aspects are related to assessment of severity of AIDS.
The focus towards the etiology behind the HIV for the mental disorders is missing. It was
also evident from other reports (Vitiello et al., 2003) that the about 20.3% of HIV-infected
patients who receiving medical care are associated with anxiety and other psychotic disorders
(panic disorder, 12.3%; post-traumatic stress disorder, 10.4%; generalized anxiety disorder,
2.8%). Among the patients most patients are consuming psychotropics however, half of the
patients did not receive medication for depressive disorders. Kuo et al., (2014) reported the data from
a cross-sectional survey of families in HIV-endemic South Africa. The researchers studied the relationship between
HIV impacts and caregiver anxiety. The patients included in the study comprises of either not caring of children
orphaned by AIDS; caring for a child orphaned by AIDS but not living with HIV or dual HIV effects. The
outcome of the study (Kuo et al., 2014) suggests that it was not caring for a child orphaned by AIDS per se that
increased risk for anxiety. In addition, female patients appear to be of high risk of anxiety due to negative actions
towards coping responses to stress (Rudolph, 2002) and etiological differences. Equally age can also increase the
risk for anxiety due to an increase in chronic health conditions (Schoevers et al., 2005) and neurological
changes. Due to associated thinking, the patients with positive HIV can develop psychological distress leading to
development of anxiety for instance. The symptoms of anxiety have to be relieved in order to promote and sustain
the health of infected person. In another study, it was quoted that the South African children and adolescents living in
HIV/AIDS-affected families are at elevated risk of both symptoms of anxiety and depressive symptoms (Boyes &
Cluver, 2015). The investigators opined that the poverty and HIV/AIDS-related stigma are as additional risk factors
towards negative mental health outcomes. The study contains youths from high HIV-pervasive groups in South
Africa were met and caught up one year later. Familial HIV/AIDS at pattern appraisal was not specifically
connected with psychological wellness results 1 year later. However, the researchers opined that the usage and
thorough assessment of intense programs in South African people group may enhance emotional wellness results
5
for HIV/AIDS-influenced youngsters and youths. In addition, the support from family appears to show some
influence towards the mitigation of infection. Some reports recommend supporting by family (Mohanan &
Kamath, 2009) so that the infected person can reduce the symptoms. Mohanan & Kamath (2009) assessed the
effect of family support on morbidity, mortality, quality of life, and economics in families with at least one HIV-
infected member, in developing countries. The authors utilized numerous databases including CENTRAL, the
Cochrane Database of Systematic Reviews, MEDLINE, AIDSLINE and CINAHL etc. No
trials found pertaining to the inclusion of family members for the support in the studies. It
indicates that there is an insufficient evidence to bring out the effect of family support in
reducing the morbidity and mortality of HIV-infected persons in developing countries.
1.4. Effect of HIV mediated depression on medication/therapy
Pence et al., (2015) investigated the impact of antidepressant efficacy in HIV care for the improvement of adherence
of antiretroviral therapy and depression morbidity. The pseudo-cluster randomized trial was conducted in HIV-
infected adults with major depressive disorder based on US infectious diseases clinics. The depression care
managers used systematic metrics to give HIV primary-care clinicians standardized antidepressant treatment
recommendations during 2010-2013. About 149 participants were randomized to intervention and 155 to usual
care. Diverse patients belonging to majorly men, Black, non-Hispanic, unemployed, and virally suppressed with
high baseline self-reported antiretroviral adherence and depressive severity were included. The outcome reveals that
there was significant improvement in depression. Mitzel et al., (2015) tested the role of depressive symptoms on
adherence of anti HIV-medication adherence. The study was conducted in 66 HIV-infected men who have sex
with men from an outpatient infectious disease clinic. The outcome reveals that the stigma-related experiences were
positively associated with depressive symptoms and negatively associated with adherence. These results highlight
the importance of treating depressive symptoms in interventions aiming to improve medication adherence among
HIV-infected patients. Turan et al., (1999) tried to fill the gap of the research by conducting the
study in women in association between internalized stigma and ART adherence. The multicenter cohort study
was based on questionnaires in 1168 women who were taking ART. Among the women, the minority woman
6
influence towards the mitigation of infection. Some reports recommend supporting by family (Mohanan &
Kamath, 2009) so that the infected person can reduce the symptoms. Mohanan & Kamath (2009) assessed the
effect of family support on morbidity, mortality, quality of life, and economics in families with at least one HIV-
infected member, in developing countries. The authors utilized numerous databases including CENTRAL, the
Cochrane Database of Systematic Reviews, MEDLINE, AIDSLINE and CINAHL etc. No
trials found pertaining to the inclusion of family members for the support in the studies. It
indicates that there is an insufficient evidence to bring out the effect of family support in
reducing the morbidity and mortality of HIV-infected persons in developing countries.
1.4. Effect of HIV mediated depression on medication/therapy
Pence et al., (2015) investigated the impact of antidepressant efficacy in HIV care for the improvement of adherence
of antiretroviral therapy and depression morbidity. The pseudo-cluster randomized trial was conducted in HIV-
infected adults with major depressive disorder based on US infectious diseases clinics. The depression care
managers used systematic metrics to give HIV primary-care clinicians standardized antidepressant treatment
recommendations during 2010-2013. About 149 participants were randomized to intervention and 155 to usual
care. Diverse patients belonging to majorly men, Black, non-Hispanic, unemployed, and virally suppressed with
high baseline self-reported antiretroviral adherence and depressive severity were included. The outcome reveals that
there was significant improvement in depression. Mitzel et al., (2015) tested the role of depressive symptoms on
adherence of anti HIV-medication adherence. The study was conducted in 66 HIV-infected men who have sex
with men from an outpatient infectious disease clinic. The outcome reveals that the stigma-related experiences were
positively associated with depressive symptoms and negatively associated with adherence. These results highlight
the importance of treating depressive symptoms in interventions aiming to improve medication adherence among
HIV-infected patients. Turan et al., (1999) tried to fill the gap of the research by conducting the
study in women in association between internalized stigma and ART adherence. The multicenter cohort study
was based on questionnaires in 1168 women who were taking ART. Among the women, the minority woman
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
showed significant suboptimal ART due to development of depressive symptoms. The authors explained the
probable causes of depression in minority community in general and female in particular contrasted with other
racial/ethnic gatherings. Another cross-sectional study (Medha et al., 2011) depicted the connections between social
bolster, HIV exposure, and melancholy among 340 country African American ladies with HIV ailment living in the
southeastern United States. Three parts of social backing (saw accessibility of bolster, wellsprings of accessible
backing, and fulfillment with accessible backing) were measured alongside HIV exposure and sadness. Seen
accessibility of backing and fulfillment with backing intervened the relationship between HIV divulgence and
sorrow. On the off chance that affirmed in longitudinal studies, these discoveries have suggestions for planning and
executing mediations supporting African American ladies with HIV ailment in revealing their HIV status fittingly,
especially to their youngsters.
1.5 Effect of HIV/AIDS on emotion
Without treatment, a large proportion of HIV-positive people live for a decade or more before the
virus begins to take a noticeable toll. In addition, there is a small proportion of people with HIV who
have immune systems that can naturally resist replication of the virus for an indefinite period of time
(Okulicz et al., 2009). Some people may have outdated concepts of the harm caused by HIV
because earlier antiretroviral drugs and combinations did not treat HIV effectively. However, the
discovery of new classes of antiretroviral in the late 1990s resulted in dramatic reductions in HIV-
related illnesses and deaths in high-income countries. For example, the age-adjusted HIV-related
death rate in the United States dropped from 17 per 100,000 people in 1995 to about five per 100,000
people by the end of the decade (Mocroft et al., 2002). Once the patient is diagnosed for the
positive HIV, can cause lot of emotional distress. Moneyham et al., (1997) investigated the
impact of psychological mediators of HIV-related stressors on emotional distress in 264 HIV
positive women. It appears that the effect of HIV-related stressors on emotional distress was indirect
through cognitive appraisal. The findings indicate that how HIV+ women think about HIV-related
stressors is an important factor that may account for individual variability in the ability to maintain a
7
probable causes of depression in minority community in general and female in particular contrasted with other
racial/ethnic gatherings. Another cross-sectional study (Medha et al., 2011) depicted the connections between social
bolster, HIV exposure, and melancholy among 340 country African American ladies with HIV ailment living in the
southeastern United States. Three parts of social backing (saw accessibility of bolster, wellsprings of accessible
backing, and fulfillment with accessible backing) were measured alongside HIV exposure and sadness. Seen
accessibility of backing and fulfillment with backing intervened the relationship between HIV divulgence and
sorrow. On the off chance that affirmed in longitudinal studies, these discoveries have suggestions for planning and
executing mediations supporting African American ladies with HIV ailment in revealing their HIV status fittingly,
especially to their youngsters.
1.5 Effect of HIV/AIDS on emotion
Without treatment, a large proportion of HIV-positive people live for a decade or more before the
virus begins to take a noticeable toll. In addition, there is a small proportion of people with HIV who
have immune systems that can naturally resist replication of the virus for an indefinite period of time
(Okulicz et al., 2009). Some people may have outdated concepts of the harm caused by HIV
because earlier antiretroviral drugs and combinations did not treat HIV effectively. However, the
discovery of new classes of antiretroviral in the late 1990s resulted in dramatic reductions in HIV-
related illnesses and deaths in high-income countries. For example, the age-adjusted HIV-related
death rate in the United States dropped from 17 per 100,000 people in 1995 to about five per 100,000
people by the end of the decade (Mocroft et al., 2002). Once the patient is diagnosed for the
positive HIV, can cause lot of emotional distress. Moneyham et al., (1997) investigated the
impact of psychological mediators of HIV-related stressors on emotional distress in 264 HIV
positive women. It appears that the effect of HIV-related stressors on emotional distress was indirect
through cognitive appraisal. The findings indicate that how HIV+ women think about HIV-related
stressors is an important factor that may account for individual variability in the ability to maintain a
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
sense of subjective well-being in the face of a devastating fatal disease. Numerous reports are not
available to link the emotional distress and their mechanisms. However on report (Wei et al., 2016)
describes the relation between stigma (discriminatory behaviors), stereotyped attitudes and
emotional behavior. The researchers utilized data from 790 children (age, 6-17 years) affected by HIV
for the analysis and mediation of the model. They found that a significant interaction between
perceived stigma and age suggested that negative emotions increase with age among those who
perceived a higher level of stigmatization. Asikhia & Mohangi (2015) reported the outcome of a
qualitative study utilizing 11 orphaned adolescent (5 boys and 6 girls aged between 15-18 years)
patients with AIDS. All the participants show that a high prevalence of psychological, behavioral and
emotional problems and lack of adequate support from the teachers. From the evidences it appear that
most patients are associated with a lack of support to get rid of the symptoms making the patients to
be emotional and psychological distress. Therefore there is need of adequate support from the
government in the disease management.
1.6. Effect of socioeconomic conditions on anxiety in HIV infected patients
Robinson et al., (2015) evaluated the effect of interventions aimed at sustaining and
improving employment in HIV+ persons utilizing a comprehensive search from 1981 until
December 2014. The evaluation has been done from randomized controlled trials or
controlled before-after studies. All the participants appear that they have undergone for
vocational training and antiretroviral therapy. No studies dealt with psychological
interventions. Among the studies, two studies compared employment outcomes of HIV+
persons on ART therapy to healthy controls. Three other studies compared HIV+ persons on
ART to HIV+ persons not yet on ART. Two studies indicated an increase in the likelihood of
employment over time due to the impact of ART for HIV+ persons compared to HIV+
person’s pre-ART. It indicates that there are no investigations associated with the assessment
of mental illnesses in HIV infected patients. Despite of low quality of interventions it was
8
available to link the emotional distress and their mechanisms. However on report (Wei et al., 2016)
describes the relation between stigma (discriminatory behaviors), stereotyped attitudes and
emotional behavior. The researchers utilized data from 790 children (age, 6-17 years) affected by HIV
for the analysis and mediation of the model. They found that a significant interaction between
perceived stigma and age suggested that negative emotions increase with age among those who
perceived a higher level of stigmatization. Asikhia & Mohangi (2015) reported the outcome of a
qualitative study utilizing 11 orphaned adolescent (5 boys and 6 girls aged between 15-18 years)
patients with AIDS. All the participants show that a high prevalence of psychological, behavioral and
emotional problems and lack of adequate support from the teachers. From the evidences it appear that
most patients are associated with a lack of support to get rid of the symptoms making the patients to
be emotional and psychological distress. Therefore there is need of adequate support from the
government in the disease management.
1.6. Effect of socioeconomic conditions on anxiety in HIV infected patients
Robinson et al., (2015) evaluated the effect of interventions aimed at sustaining and
improving employment in HIV+ persons utilizing a comprehensive search from 1981 until
December 2014. The evaluation has been done from randomized controlled trials or
controlled before-after studies. All the participants appear that they have undergone for
vocational training and antiretroviral therapy. No studies dealt with psychological
interventions. Among the studies, two studies compared employment outcomes of HIV+
persons on ART therapy to healthy controls. Three other studies compared HIV+ persons on
ART to HIV+ persons not yet on ART. Two studies indicated an increase in the likelihood of
employment over time due to the impact of ART for HIV+ persons compared to HIV+
person’s pre-ART. It indicates that there are no investigations associated with the assessment
of mental illnesses in HIV infected patients. Despite of low quality of interventions it was
8
expected to improve ART interventions outcomes of employment for the positive HIV
persons. Due to lack of high quality interventions, it is preferable to have adequate
randomized studies to assess the effectiveness of interventions for HIV+ persons.
1.7 Discussion
Numerous articles found from the PubMed search in comparison to other sources. However
few reports can be found in both the searches for instance PubMed and Cochrane. The
psychological disorders and alterations in mood are often comorbid with chronic illnesses
such as HIV leading to an increase the associated morbidity and mortality rates (Frasure-
Smith and Lesperance, 2005). The review was also extended towards available guidelines. It
was apparent from the guidelines that the guidance is recommending to diagnose the HIV
positive individuals for anxiety and depression using validated tools (Duncan et al., 2015).
Despite of describing the role of HIV on mental illnesses, the guidance (Duncan et al., 2015)
describes separately the aspects of strategies for individual diseases such as HIV, Kidney
diseases, mental illness and cardiovascular diseases. In addition, the reports (Bernard et al.,
2014) describe the diagnosis of HIV infection utilizing an algorithm (Fig-1) and are based on
testing of serum or plasma specimens. WHO (2016) even describing the general features of
disease including, signs and symptoms, transmission of disease; risk factors associated;
diagnosis and disease management. It appears that none of the source is describing the
underlying mechanisms involved in the development of emotional distress, anxiety and
depression in HIV infected patients. However, it was apartment from some of the sources the
personnel who were positive towards the HIV are associated with psychological distress.
9
persons. Due to lack of high quality interventions, it is preferable to have adequate
randomized studies to assess the effectiveness of interventions for HIV+ persons.
1.7 Discussion
Numerous articles found from the PubMed search in comparison to other sources. However
few reports can be found in both the searches for instance PubMed and Cochrane. The
psychological disorders and alterations in mood are often comorbid with chronic illnesses
such as HIV leading to an increase the associated morbidity and mortality rates (Frasure-
Smith and Lesperance, 2005). The review was also extended towards available guidelines. It
was apparent from the guidelines that the guidance is recommending to diagnose the HIV
positive individuals for anxiety and depression using validated tools (Duncan et al., 2015).
Despite of describing the role of HIV on mental illnesses, the guidance (Duncan et al., 2015)
describes separately the aspects of strategies for individual diseases such as HIV, Kidney
diseases, mental illness and cardiovascular diseases. In addition, the reports (Bernard et al.,
2014) describe the diagnosis of HIV infection utilizing an algorithm (Fig-1) and are based on
testing of serum or plasma specimens. WHO (2016) even describing the general features of
disease including, signs and symptoms, transmission of disease; risk factors associated;
diagnosis and disease management. It appears that none of the source is describing the
underlying mechanisms involved in the development of emotional distress, anxiety and
depression in HIV infected patients. However, it was apartment from some of the sources the
personnel who were positive towards the HIV are associated with psychological distress.
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
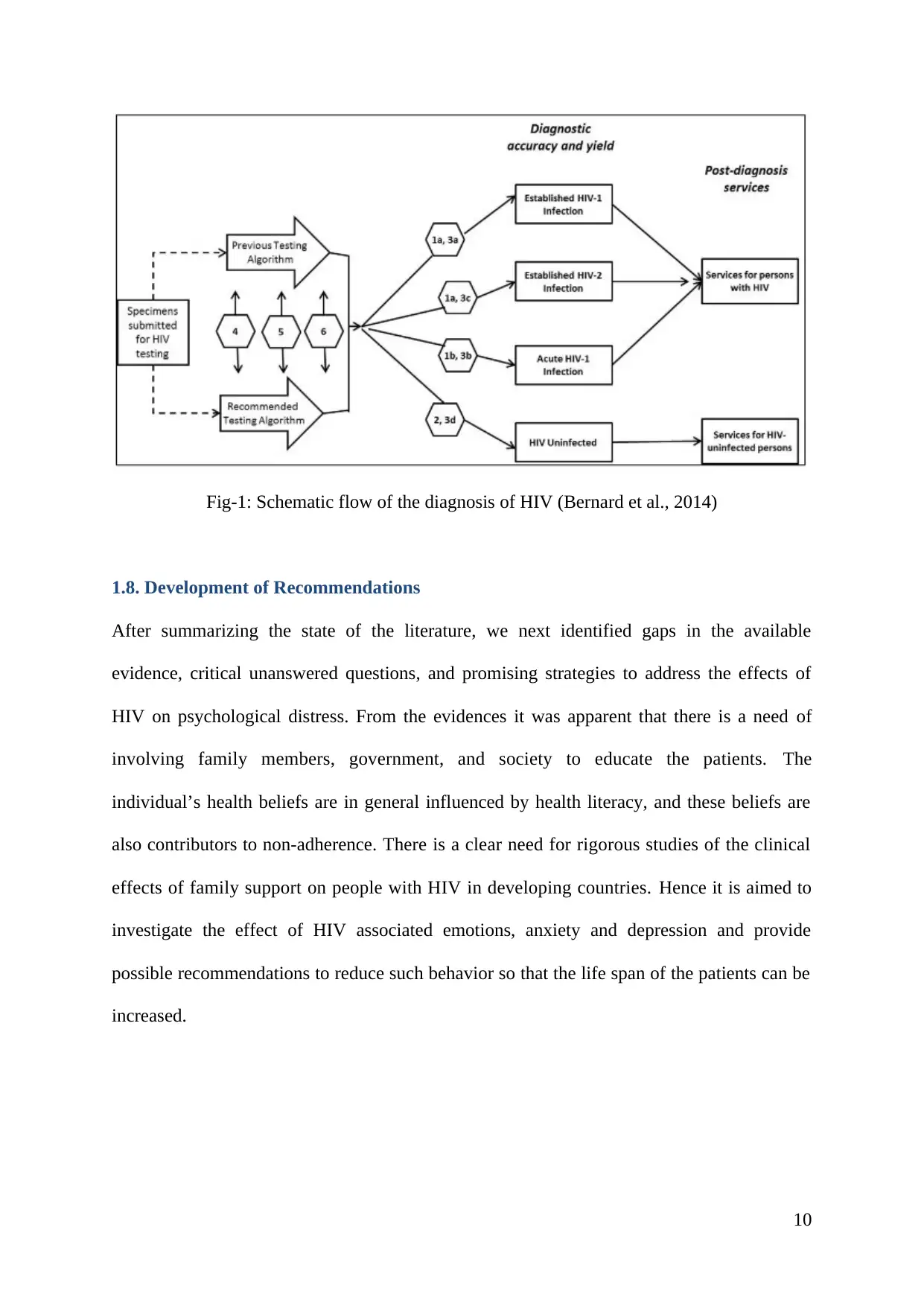
Fig-1: Schematic flow of the diagnosis of HIV (Bernard et al., 2014)
1.8. Development of Recommendations
After summarizing the state of the literature, we next identified gaps in the available
evidence, critical unanswered questions, and promising strategies to address the effects of
HIV on psychological distress. From the evidences it was apparent that there is a need of
involving family members, government, and society to educate the patients. The
individual’s health beliefs are in general influenced by health literacy, and these beliefs are
also contributors to non-adherence. There is a clear need for rigorous studies of the clinical
effects of family support on people with HIV in developing countries. Hence it is aimed to
investigate the effect of HIV associated emotions, anxiety and depression and provide
possible recommendations to reduce such behavior so that the life span of the patients can be
increased.
10
1.8. Development of Recommendations
After summarizing the state of the literature, we next identified gaps in the available
evidence, critical unanswered questions, and promising strategies to address the effects of
HIV on psychological distress. From the evidences it was apparent that there is a need of
involving family members, government, and society to educate the patients. The
individual’s health beliefs are in general influenced by health literacy, and these beliefs are
also contributors to non-adherence. There is a clear need for rigorous studies of the clinical
effects of family support on people with HIV in developing countries. Hence it is aimed to
investigate the effect of HIV associated emotions, anxiety and depression and provide
possible recommendations to reduce such behavior so that the life span of the patients can be
increased.
10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
CHAPTER-2: CRITIQUE OF LITERATURE
2.1. Literature review
The HIV infected victims fail to resist towards the attack of pathogenic and non-pathogenic
diseases. The complications of the patient are going to be increased. Therefore, the life span
is going to be reduced significantly if untreated. In view of the patient condition, by looking
to other patients, most HIV infected patients develop a kind of psychological distress. Most
researchers contributed for the identification of possible factors and their control towards
management of disease. However, there exist certain gaps in the literature. The gaps have
been identified and depicted in below sections. Late diagnosis and thus more severe illness at the time of
diagnosis can propel the older individuals and makes them to confuse towards for the development of symptoms of
HIV. The review of literature made utilizing diverse sources as depicted in preceding chapter.
A literature critique is an analysis of a piece of literature. The scope of a critique is to
examine each aspect of the work and involves breaking the literary piece apart into its
separate components and evaluating how they fit together to accomplish the piece's purpose.
The outcome of the literature along with positive and negative aspects is shown in this
chapter. The critique would help in developing the objectives and planning the research
further.
2.2. Effect of AIDS on Psychological disorders
2.2.1. Effect of HIV mediated anxiety on medication/therapy
The methods employed by Blank et al (2011) are based on randomized clinical trial in
numerous AIDS patients with mental illnesses. The intervention comprises for the assessment
of mental status and AIDS for a period of 12 months. The entire study duration is relatively
good and is based on clinical trials and showed a significant influence on the results. Despite
of positive influence, it appears that there exist certain limitations in the study. A generalized
11
2.1. Literature review
The HIV infected victims fail to resist towards the attack of pathogenic and non-pathogenic
diseases. The complications of the patient are going to be increased. Therefore, the life span
is going to be reduced significantly if untreated. In view of the patient condition, by looking
to other patients, most HIV infected patients develop a kind of psychological distress. Most
researchers contributed for the identification of possible factors and their control towards
management of disease. However, there exist certain gaps in the literature. The gaps have
been identified and depicted in below sections. Late diagnosis and thus more severe illness at the time of
diagnosis can propel the older individuals and makes them to confuse towards for the development of symptoms of
HIV. The review of literature made utilizing diverse sources as depicted in preceding chapter.
A literature critique is an analysis of a piece of literature. The scope of a critique is to
examine each aspect of the work and involves breaking the literary piece apart into its
separate components and evaluating how they fit together to accomplish the piece's purpose.
The outcome of the literature along with positive and negative aspects is shown in this
chapter. The critique would help in developing the objectives and planning the research
further.
2.2. Effect of AIDS on Psychological disorders
2.2.1. Effect of HIV mediated anxiety on medication/therapy
The methods employed by Blank et al (2011) are based on randomized clinical trial in
numerous AIDS patients with mental illnesses. The intervention comprises for the assessment
of mental status and AIDS for a period of 12 months. The entire study duration is relatively
good and is based on clinical trials and showed a significant influence on the results. Despite
of positive influence, it appears that there exist certain limitations in the study. A generalized
11
term of ‘mental illness’ is provided however no details are captured on the type of mental
illness in detail. An emphasis towards focus for the assessment of AIDS induced mental
illness should have been covered. The causes behind in the mental illness are missing. The
investigators even did not put additional efforts for the identification of mental illness in the
patients with AIDS. Certain reports describe the use of antipsychotic medication in HIV
infected patients. Among, the investigation performed by Vitiello et al., (2003) focused
mainly on the effectiveness of psychotropic medication on recovery of AIDS. The medical
intervention showed a decrease of disease intensity. However, the authors did not describe
the underlying reasons, why the psychotic symptoms are developed in those individuals. The
outcome of the study reported by Kuo et al., (2014) have covered a broad range of victims
with anxiety as one of the effect in AIDS patients from South African context. The report
gave an insight of how the caregivers are influencing psychologically. However, the
researchers are not addressed the impact of AIDS on patient’s perspective. Similar to other
reports, the investigators are not covered the factors contributing for anxiety and other
psychological disorders. The focus of other reports (Mohanan & Kamath, 2009) is based on
recommendations but not on the mechanism involved for the psychological distress in AIDS
patients.
2.2.2. Effect of HIV mediated depression on medication/therapy
According to the literature it appears that, AIDS patients and their caregivers can undergo depression. Therefore,
most physicians prescribe antipsychotic medication a part from the AIDS medication. Antidepressant efficacy in
HIV care have been evaluated by Pence et al., (2015), did not bring a significant improvement in HIV outcome
despite of following adequate assessment and statistics. The investigators evaluated the adherence of antiretroviral
therapy and depression morbidity. Except depression, no other psychological diseases such as anxiety have been
covered in the investigation. The study was also pseudo cluster randomization, a design most suits for in smaller
number of study participants (Melis et al., 2011). The sample size included is reasonably good however, the
12
illness in detail. An emphasis towards focus for the assessment of AIDS induced mental
illness should have been covered. The causes behind in the mental illness are missing. The
investigators even did not put additional efforts for the identification of mental illness in the
patients with AIDS. Certain reports describe the use of antipsychotic medication in HIV
infected patients. Among, the investigation performed by Vitiello et al., (2003) focused
mainly on the effectiveness of psychotropic medication on recovery of AIDS. The medical
intervention showed a decrease of disease intensity. However, the authors did not describe
the underlying reasons, why the psychotic symptoms are developed in those individuals. The
outcome of the study reported by Kuo et al., (2014) have covered a broad range of victims
with anxiety as one of the effect in AIDS patients from South African context. The report
gave an insight of how the caregivers are influencing psychologically. However, the
researchers are not addressed the impact of AIDS on patient’s perspective. Similar to other
reports, the investigators are not covered the factors contributing for anxiety and other
psychological disorders. The focus of other reports (Mohanan & Kamath, 2009) is based on
recommendations but not on the mechanism involved for the psychological distress in AIDS
patients.
2.2.2. Effect of HIV mediated depression on medication/therapy
According to the literature it appears that, AIDS patients and their caregivers can undergo depression. Therefore,
most physicians prescribe antipsychotic medication a part from the AIDS medication. Antidepressant efficacy in
HIV care have been evaluated by Pence et al., (2015), did not bring a significant improvement in HIV outcome
despite of following adequate assessment and statistics. The investigators evaluated the adherence of antiretroviral
therapy and depression morbidity. Except depression, no other psychological diseases such as anxiety have been
covered in the investigation. The study was also pseudo cluster randomization, a design most suits for in smaller
number of study participants (Melis et al., 2011). The sample size included is reasonably good however, the
12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 38
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.