MOD002801 - Age & Gender in Hypertension, Tachycardia Development
VerifiedAdded on 2023/04/07
|1
|1871
|336
Report
AI Summary
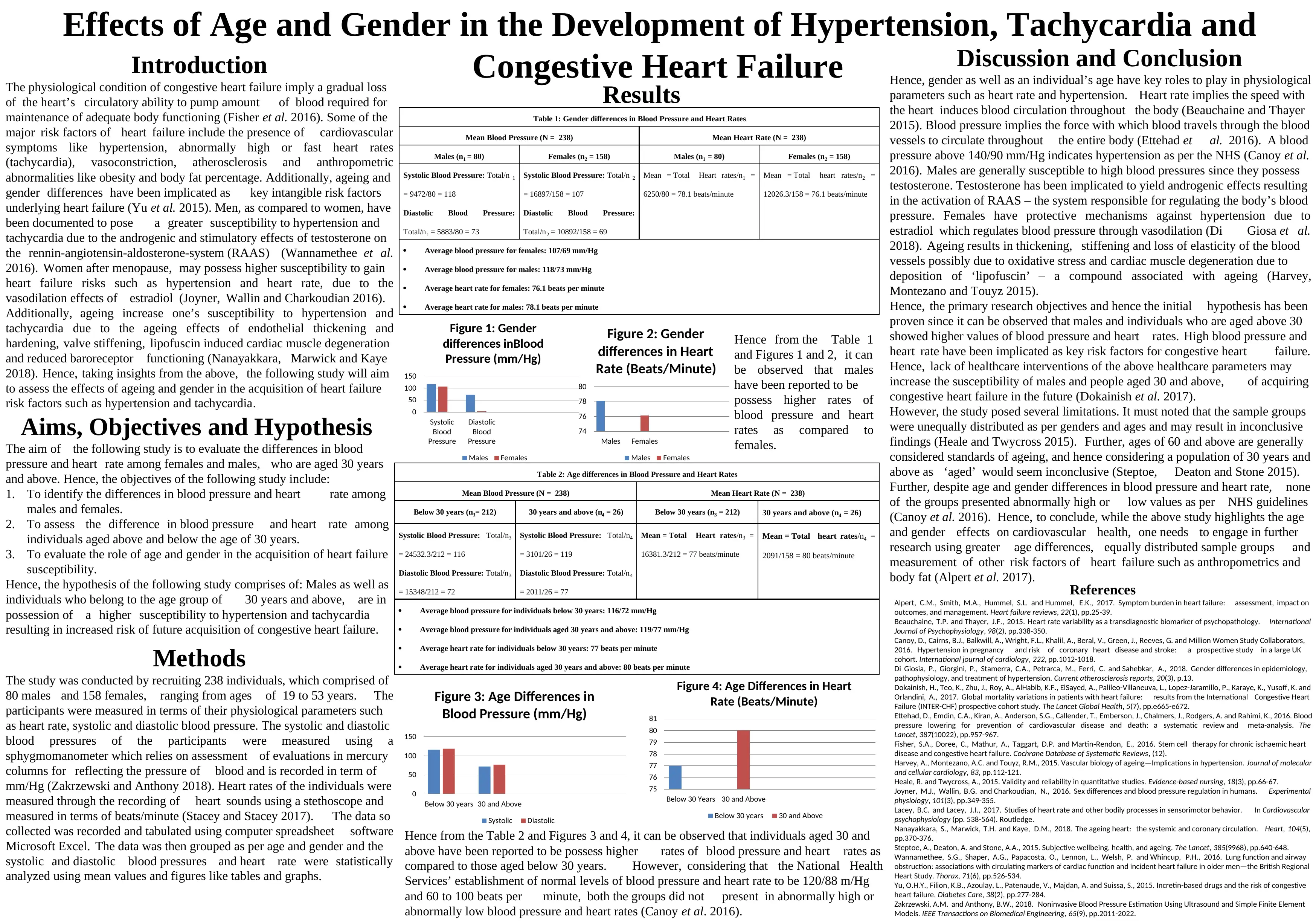
This report investigates the effects of age and gender on the development of hypertension and tachycardia, key risk factors for congestive heart failure. The study examines physiological parameters such as heart rate, systolic, and diastolic blood pressure in a group of 238 individuals, comprising 80 males and 158 females, aged between 19 and 53 years. The results indicate that males generally exhibit higher blood pressure and heart rates compared to females, and individuals aged 30 and above also show elevated levels compared to younger participants. While the findings support the hypothesis that age and gender influence cardiovascular health, the study acknowledges limitations such as unequal sample group sizes and the relatively young age range considered for the 'aged' group. The report concludes by emphasizing the need for further research with more balanced sample groups and a broader age range to comprehensively assess the impact of age and gender on heart failure risk.
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.