Progress of EHR Adoption in US Emergency and Outpatient Departments
VerifiedAdded on 2023/06/13
|8
|2976
|233
Report
AI Summary
This report, based on data from the National Hospital Ambulatory Medical Care Survey (NHAMCS) from 2006 to 2011, examines the adoption of Electronic Health Records (EHR) in hospital emergency departments (EDs) and outpatient departments (OPDs) in the United States. It highlights a significant increase in EHR usage, with 84% of EDs and 73% of OPDs using EHR systems by 2011. The adoption of basic EHR systems with specific functionalities also rose substantially in both departments. The report further analyzes the progress in meeting Stage 1 Meaningful Use objectives, driven by the HITECH Act of 2009, noting improvements in areas such as drug interaction warnings, prescription ordering, and patient problem list maintenance. However, it also points out that only a small percentage of departments had EHR technology supporting a comprehensive set of Meaningful Use objectives, indicating ongoing challenges in fully implementing EHR systems.
NCHS Data Brief ■ No. 187 ■ February 2015
u.s. department of health and human services
centers for disease control and prevention
national center for health statistics
Progress With Electronic Health Record Adoption Among
Emergency and Outpatient Departments:
United States, 2006–2011
Eric Jamoom, Ph.D., M.P.H., M.S.; and Esther Hing, M.P.H.
Key findings
Data from the 2006–
2011 National Hospital
Ambulatory Medical Care
Survey
● In 2011, 84% of hospital
emergency departments (EDs)
used an electronic health record
(EHR) system.
● Adoption of a basic EHR
system with a specific set
of functionalities by EDs
increased from 19% in 2007 to
54% in 2011.
● In 2011, 73% of hospital
outpatient departments (OPDs)
used an EHR system, up from
29% in 2006.
● Adoption of a basic EHR
system with a specific set
of functionalities by OPDs
increased from 9% in 2007 to
57% in 2011.
● From 2007 through 2011,
adoption of Stage 1 Meaningful
Use objectives by EDs and
OPDs increased.
● In 2011, 14% of EDs
and 16% of OPDs had EHR
technology able to support
nine Stage 1 Meaningful Use
objectives.
The Health Information Technology for Economic and Clinical Health
(HITECH) Act of 2009 provides incentive payments to eligible hospitals and
providers that demonstrate the meaningful use of a certified electronic health
record (EHR) system (1,2). This report describes the adoption of EHRs in
hospital emergency departments (EDs) and outpatient departments (OPDs)
from 2006 through 2011 using the National Hospital Ambulatory Medical
Care Survey (NHAMCS).
Keywords: health information technology • National Hospital Ambulatory
Medical Care Survey
Use of an EHR system in EDs increased from 2006 through
2011.
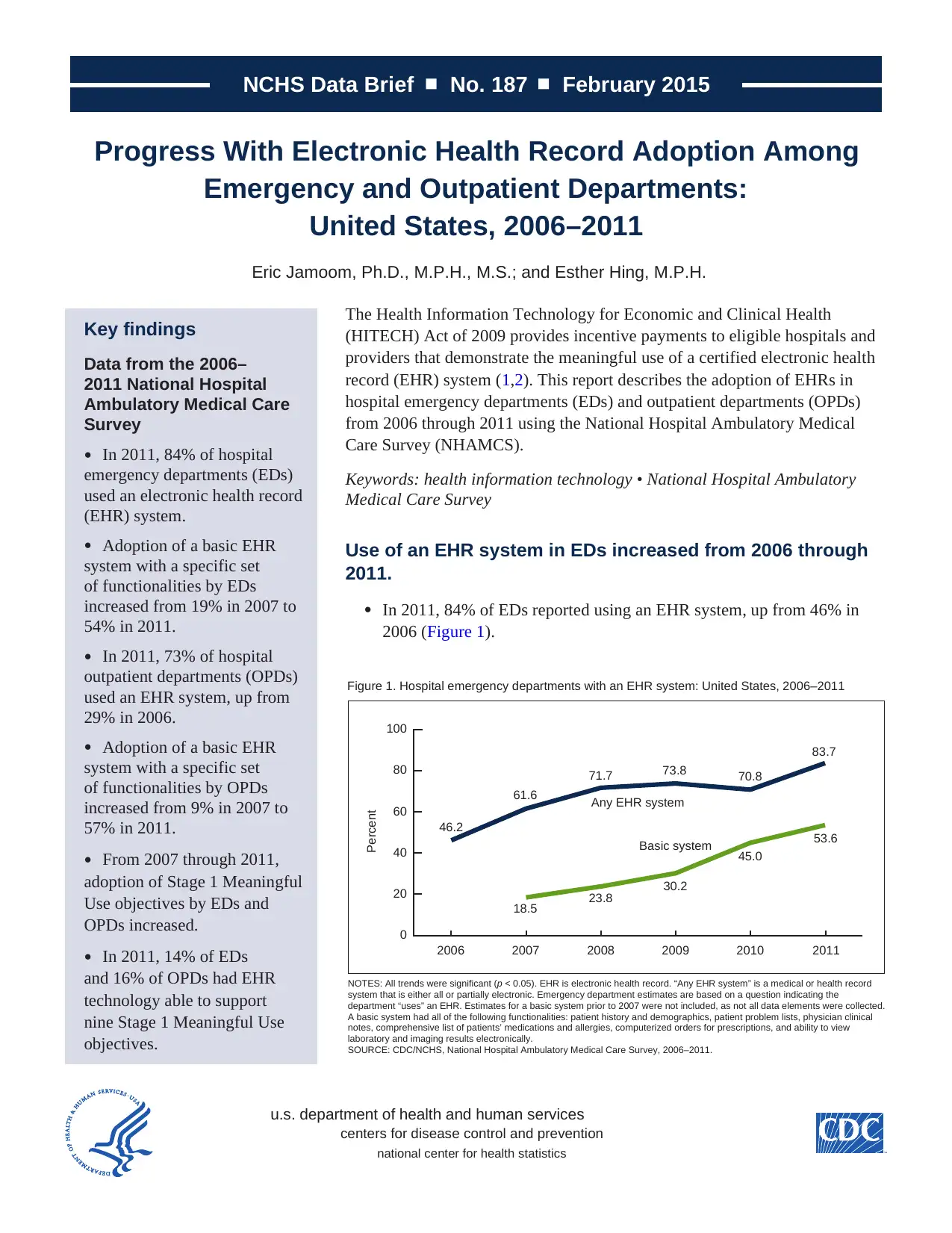
● In 2011, 84% of EDs reported using an EHR system, up from 46% in
2006 (Figure 1).
Figure 1. Hospital emergency departments with an EHR system: United States, 2006–2011
NOTES: All trends were significant (p < 0.05). EHR is electronic health record. “Any EHR system” is a medical or health record
system that is either all or partially electronic. Emergency department estimates are based on a question indicating the
department “uses” an EHR. Estimates for a basic system prior to 2007 were not included, as not all data elements were collected.
A basic system had all of the following functionalities: patient history and demographics, patient problem lists, physician clinical
notes, comprehensive list of patients’ medications and allergies, computerized orders for prescriptions, and ability to view
laboratory and imaging results electronically.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2006–2011.
Percent
0
20
40
60
80
100
201120102009200820072006
46.2
61.6
71.7 73.8 70.8
83.7
18.5 23.8
30.2
45.0
53.6
Any EHR system
Basic system
u.s. department of health and human services
centers for disease control and prevention
national center for health statistics
Progress With Electronic Health Record Adoption Among
Emergency and Outpatient Departments:
United States, 2006–2011
Eric Jamoom, Ph.D., M.P.H., M.S.; and Esther Hing, M.P.H.
Key findings
Data from the 2006–
2011 National Hospital
Ambulatory Medical Care
Survey
● In 2011, 84% of hospital
emergency departments (EDs)
used an electronic health record
(EHR) system.
● Adoption of a basic EHR
system with a specific set
of functionalities by EDs
increased from 19% in 2007 to
54% in 2011.
● In 2011, 73% of hospital
outpatient departments (OPDs)
used an EHR system, up from
29% in 2006.
● Adoption of a basic EHR
system with a specific set
of functionalities by OPDs
increased from 9% in 2007 to
57% in 2011.
● From 2007 through 2011,
adoption of Stage 1 Meaningful
Use objectives by EDs and
OPDs increased.
● In 2011, 14% of EDs
and 16% of OPDs had EHR
technology able to support
nine Stage 1 Meaningful Use
objectives.
The Health Information Technology for Economic and Clinical Health
(HITECH) Act of 2009 provides incentive payments to eligible hospitals and
providers that demonstrate the meaningful use of a certified electronic health
record (EHR) system (1,2). This report describes the adoption of EHRs in
hospital emergency departments (EDs) and outpatient departments (OPDs)
from 2006 through 2011 using the National Hospital Ambulatory Medical
Care Survey (NHAMCS).
Keywords: health information technology • National Hospital Ambulatory
Medical Care Survey
Use of an EHR system in EDs increased from 2006 through
2011.
● In 2011, 84% of EDs reported using an EHR system, up from 46% in
2006 (Figure 1).
Figure 1. Hospital emergency departments with an EHR system: United States, 2006–2011
NOTES: All trends were significant (p < 0.05). EHR is electronic health record. “Any EHR system” is a medical or health record
system that is either all or partially electronic. Emergency department estimates are based on a question indicating the
department “uses” an EHR. Estimates for a basic system prior to 2007 were not included, as not all data elements were collected.
A basic system had all of the following functionalities: patient history and demographics, patient problem lists, physician clinical
notes, comprehensive list of patients’ medications and allergies, computerized orders for prescriptions, and ability to view
laboratory and imaging results electronically.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2006–2011.
Percent
0
20
40
60
80
100
201120102009200820072006
46.2
61.6
71.7 73.8 70.8
83.7
18.5 23.8
30.2
45.0
53.6
Any EHR system
Basic system
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
NCHS Data Brief ■ No. 187 ■ February 2015
■ 2 ■
● Adoption of a basic EHR system by hospital EDs increased from 19% in 2007 to 54% in
2011.
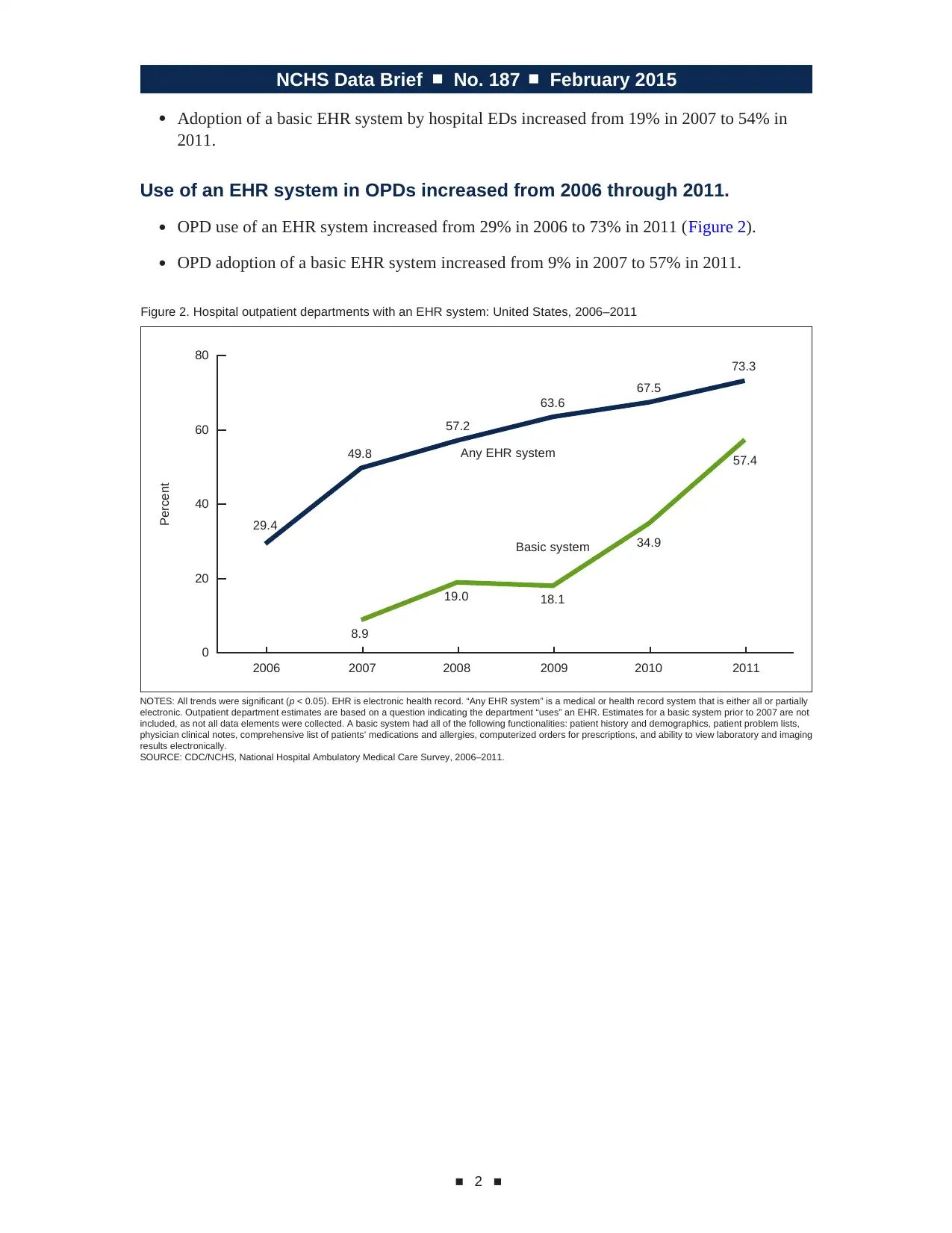
Use of an EHR system in OPDs increased from 2006 through 2011.
● OPD use of an EHR system increased from 29% in 2006 to 73% in 2011 (Figure 2).
● OPD adoption of a basic EHR system increased from 9% in 2007 to 57% in 2011.
Percent
Figure 2. Hospital outpatient departments with an EHR system: United States, 2006–2011
NOTES: All trends were significant (p < 0.05). EHR is electronic health record. “Any EHR system” is a medical or health record system that is either all or partially
electronic. Outpatient department estimates are based on a question indicating the department “uses” an EHR. Estimates for a basic system prior to 2007 are not
included, as not all data elements were collected. A basic system had all of the following functionalities: patient history and demographics, patient problem lists,
physician clinical notes, comprehensive list of patients’ medications and allergies, computerized orders for prescriptions, and ability to view laboratory and imaging
results electronically.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2006–2011.
29.4
49.8
57.2
63.6
67.5
73.3
8.9
19.0 18.1
34.9
57.4
0
20
40
60
80
2006 2007 2008 2009 2010 2011
Any EHR system
Basic system
■ 2 ■
● Adoption of a basic EHR system by hospital EDs increased from 19% in 2007 to 54% in
2011.
Use of an EHR system in OPDs increased from 2006 through 2011.
● OPD use of an EHR system increased from 29% in 2006 to 73% in 2011 (Figure 2).
● OPD adoption of a basic EHR system increased from 9% in 2007 to 57% in 2011.
Percent
Figure 2. Hospital outpatient departments with an EHR system: United States, 2006–2011
NOTES: All trends were significant (p < 0.05). EHR is electronic health record. “Any EHR system” is a medical or health record system that is either all or partially
electronic. Outpatient department estimates are based on a question indicating the department “uses” an EHR. Estimates for a basic system prior to 2007 are not
included, as not all data elements were collected. A basic system had all of the following functionalities: patient history and demographics, patient problem lists,
physician clinical notes, comprehensive list of patients’ medications and allergies, computerized orders for prescriptions, and ability to view laboratory and imaging
results electronically.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2006–2011.
29.4
49.8
57.2
63.6
67.5
73.3
8.9
19.0 18.1
34.9
57.4
0
20
40
60
80
2006 2007 2008 2009 2010 2011
Any EHR system
Basic system
NCHS Data Brief ■ No. 187 ■ February 2015
■ 3 ■
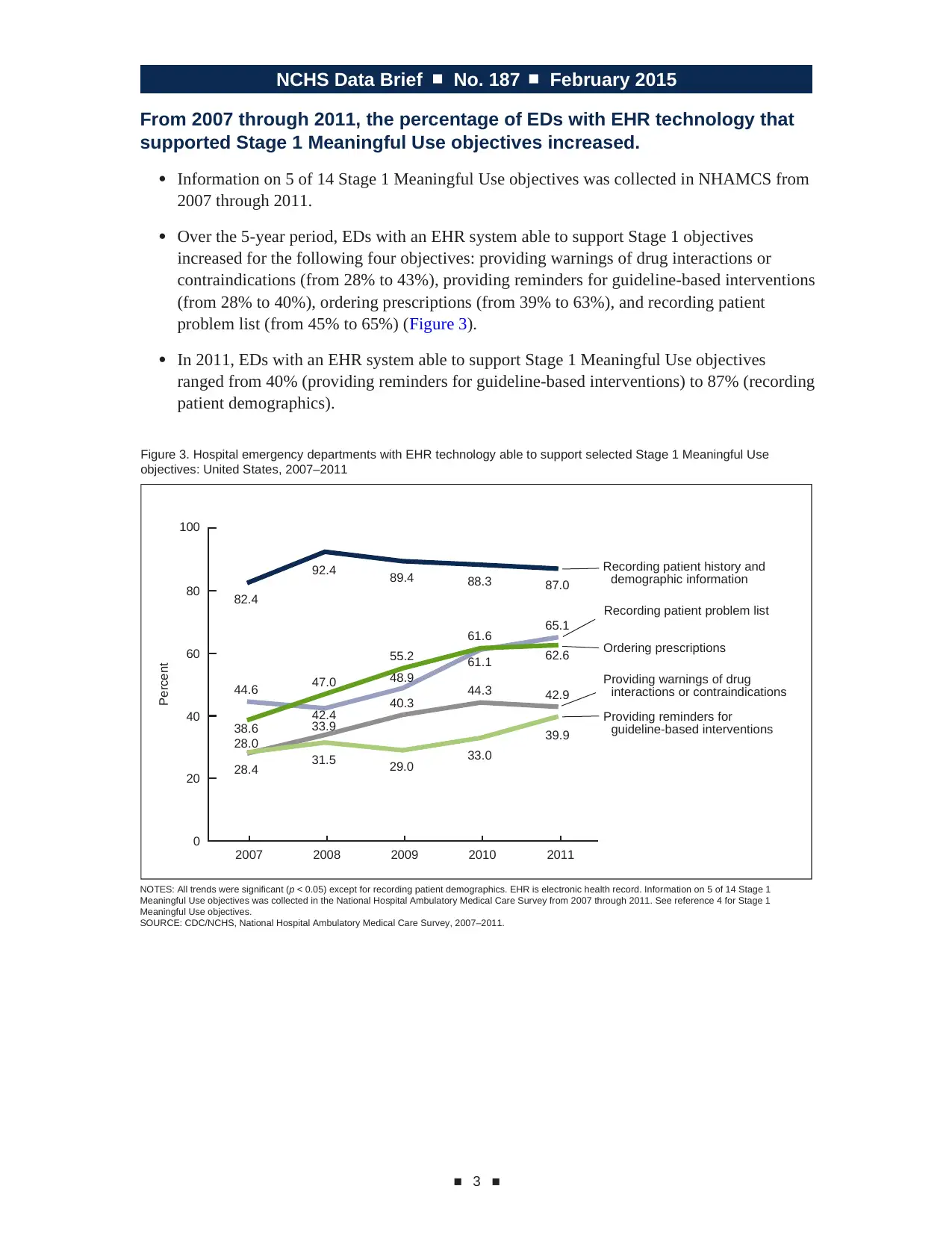
From 2007 through 2011, the percentage of EDs with EHR technology that
supported Stage 1 Meaningful Use objectives increased.
● Information on 5 of 14 Stage 1 Meaningful Use objectives was collected in NHAMCS from
2007 through 2011.
● Over the 5-year period, EDs with an EHR system able to support Stage 1 objectives
increased for the following four objectives: providing warnings of drug interactions or
contraindications (from 28% to 43%), providing reminders for guideline-based interventions
(from 28% to 40%), ordering prescriptions (from 39% to 63%), and recording patient
problem list (from 45% to 65%) (Figure 3).
● In 2011, EDs with an EHR system able to support Stage 1 Meaningful Use objectives
ranged from 40% (providing reminders for guideline-based interventions) to 87% (recording
patient demographics).
Percent
Figure 3. Hospital emergency departments with EHR technology able to support selected Stage 1 Meaningful Use
objectives: United States, 2007–2011
NOTES: All trends were significant (p < 0.05) except for recording patient demographics. EHR is electronic health record. Information on 5 of 14 Stage 1
Meaningful Use objectives was collected in the National Hospital Ambulatory Medical Care Survey from 2007 through 2011. See reference 4 for Stage 1
Meaningful Use objectives.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2007–2011.
82.4
92.4 89.4 88.3 87.0
44.6
42.4
48.9
65.1
38.6
47.0
55.2
61.6
61.1 62.6
28.0
33.9
40.3 44.3 42.9
28.4 31.5 29.0 33.0
39.9
0
20
40
60
80
100
2007 2008 2009 2010 2011
Recording patient history and
demographic information
Recording patient problem list
Ordering prescriptions
Providing warnings of drug
interactions or contraindications
Providing reminders for
guideline-based interventions
■ 3 ■
From 2007 through 2011, the percentage of EDs with EHR technology that
supported Stage 1 Meaningful Use objectives increased.
● Information on 5 of 14 Stage 1 Meaningful Use objectives was collected in NHAMCS from
2007 through 2011.
● Over the 5-year period, EDs with an EHR system able to support Stage 1 objectives
increased for the following four objectives: providing warnings of drug interactions or
contraindications (from 28% to 43%), providing reminders for guideline-based interventions
(from 28% to 40%), ordering prescriptions (from 39% to 63%), and recording patient
problem list (from 45% to 65%) (Figure 3).
● In 2011, EDs with an EHR system able to support Stage 1 Meaningful Use objectives
ranged from 40% (providing reminders for guideline-based interventions) to 87% (recording
patient demographics).
Percent
Figure 3. Hospital emergency departments with EHR technology able to support selected Stage 1 Meaningful Use
objectives: United States, 2007–2011
NOTES: All trends were significant (p < 0.05) except for recording patient demographics. EHR is electronic health record. Information on 5 of 14 Stage 1
Meaningful Use objectives was collected in the National Hospital Ambulatory Medical Care Survey from 2007 through 2011. See reference 4 for Stage 1
Meaningful Use objectives.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2007–2011.
82.4
92.4 89.4 88.3 87.0
44.6
42.4
48.9
65.1
38.6
47.0
55.2
61.6
61.1 62.6
28.0
33.9
40.3 44.3 42.9
28.4 31.5 29.0 33.0
39.9
0
20
40
60
80
100
2007 2008 2009 2010 2011
Recording patient history and
demographic information
Recording patient problem list
Ordering prescriptions
Providing warnings of drug
interactions or contraindications
Providing reminders for
guideline-based interventions
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
NCHS Data Brief ■ No. 187 ■ February 2015
■ 4 ■
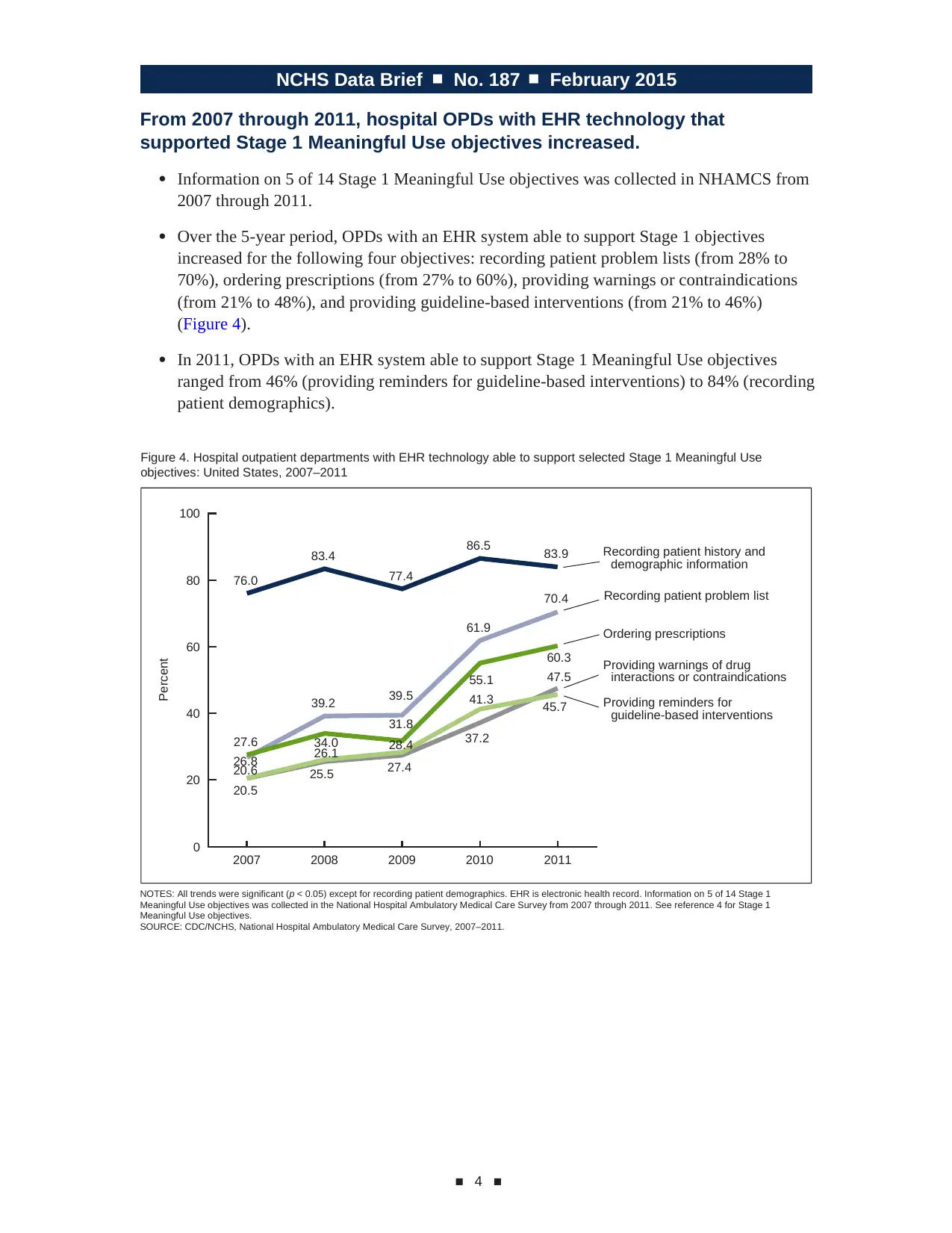
From 2007 through 2011, hospital OPDs with EHR technology that
supported Stage 1 Meaningful Use objectives increased.
● Information on 5 of 14 Stage 1 Meaningful Use objectives was collected in NHAMCS from
2007 through 2011.
● Over the 5-year period, OPDs with an EHR system able to support Stage 1 objectives
increased for the following four objectives: recording patient problem lists (from 28% to
70%), ordering prescriptions (from 27% to 60%), providing warnings or contraindications
(from 21% to 48%), and providing guideline-based interventions (from 21% to 46%)
(Figure 4).
● In 2011, OPDs with an EHR system able to support Stage 1 Meaningful Use objectives
ranged from 46% (providing reminders for guideline-based interventions) to 84% (recording
patient demographics).
Percent
Figure 4. Hospital outpatient departments with EHR technology able to support selected Stage 1 Meaningful Use
objectives: United States, 2007–2011
NOTES: All trends were significant (p < 0.05) except for recording patient demographics. EHR is electronic health record. Information on 5 of 14 Stage 1
Meaningful Use objectives was collected in the National Hospital Ambulatory Medical Care Survey from 2007 through 2011. See reference 4 for Stage 1
Meaningful Use objectives.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2007–2011.
0
20
40
60
80
100
2007 2008 2009 2010 2011
Recording patient history and
demographic information
Recording patient problem list
Ordering prescriptions
Providing warnings of drug
interactions or contraindications
Providing reminders for
guideline-based interventions
76.0
83.4
77.4
86.5 83.9
39.2 39.5
61.9
70.4
27.6 34.0
31.8
55.1
60.3
47.5
26.8
20.6
26.1 28.4
41.3
20.5
25.5 27.4
37.2
45.7
■ 4 ■
From 2007 through 2011, hospital OPDs with EHR technology that
supported Stage 1 Meaningful Use objectives increased.
● Information on 5 of 14 Stage 1 Meaningful Use objectives was collected in NHAMCS from
2007 through 2011.
● Over the 5-year period, OPDs with an EHR system able to support Stage 1 objectives
increased for the following four objectives: recording patient problem lists (from 28% to
70%), ordering prescriptions (from 27% to 60%), providing warnings or contraindications
(from 21% to 48%), and providing guideline-based interventions (from 21% to 46%)
(Figure 4).
● In 2011, OPDs with an EHR system able to support Stage 1 Meaningful Use objectives
ranged from 46% (providing reminders for guideline-based interventions) to 84% (recording
patient demographics).
Percent
Figure 4. Hospital outpatient departments with EHR technology able to support selected Stage 1 Meaningful Use
objectives: United States, 2007–2011
NOTES: All trends were significant (p < 0.05) except for recording patient demographics. EHR is electronic health record. Information on 5 of 14 Stage 1
Meaningful Use objectives was collected in the National Hospital Ambulatory Medical Care Survey from 2007 through 2011. See reference 4 for Stage 1
Meaningful Use objectives.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2007–2011.
0
20
40
60
80
100
2007 2008 2009 2010 2011
Recording patient history and
demographic information
Recording patient problem list
Ordering prescriptions
Providing warnings of drug
interactions or contraindications
Providing reminders for
guideline-based interventions
76.0
83.4
77.4
86.5 83.9
39.2 39.5
61.9
70.4
27.6 34.0
31.8
55.1
60.3
47.5
26.8
20.6
26.1 28.4
41.3
20.5
25.5 27.4
37.2
45.7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
NCHS Data Brief ■ No. 187 ■ February 2015
■ 5 ■
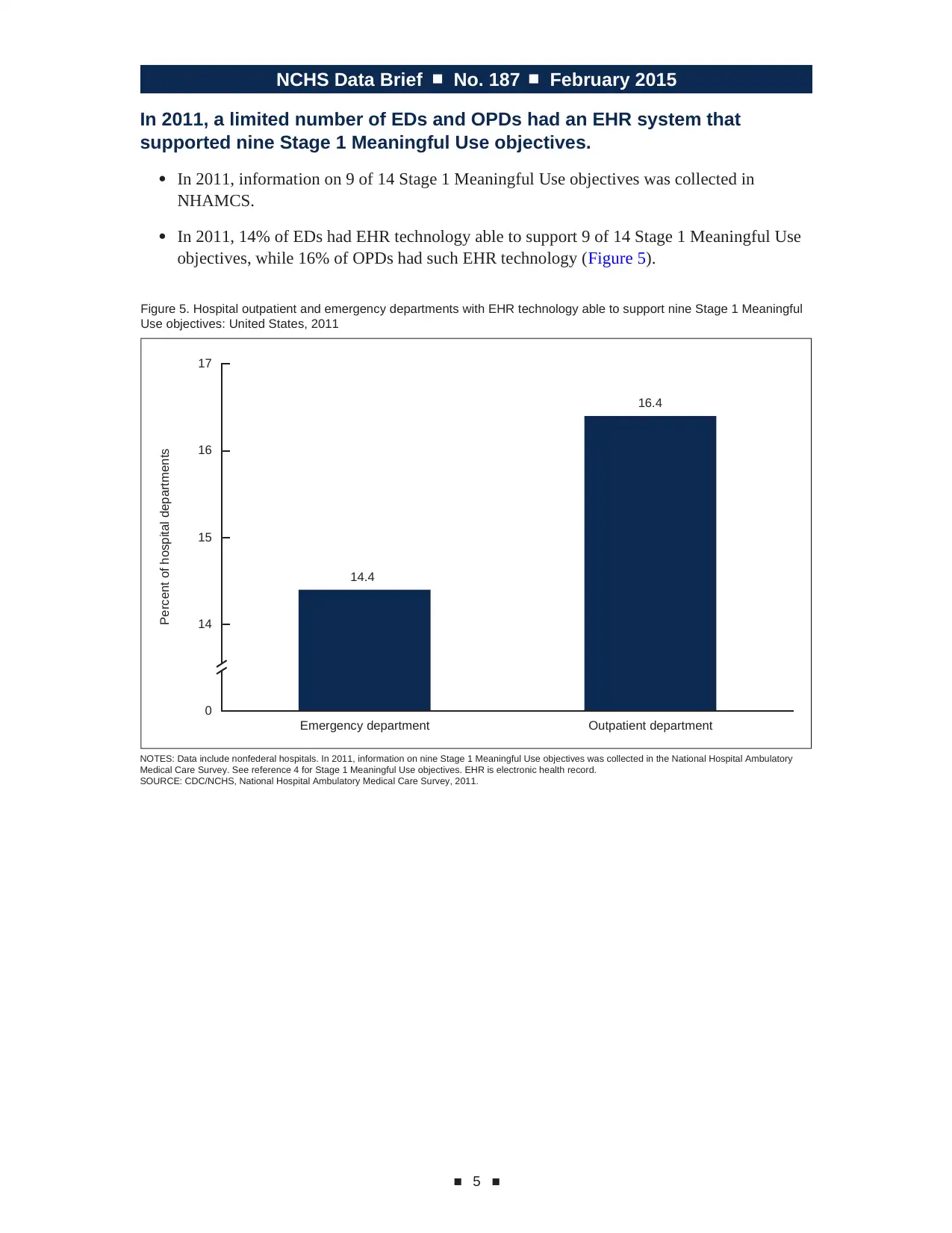
In 2011, a limited number of EDs and OPDs had an EHR system that
supported nine Stage 1 Meaningful Use objectives.
● In 2011, information on 9 of 14 Stage 1 Meaningful Use objectives was collected in
NHAMCS.
● In 2011, 14% of EDs had EHR technology able to support 9 of 14 Stage 1 Meaningful Use
objectives, while 16% of OPDs had such EHR technology (Figure 5).
Percent of hospital departments
Figure 5. Hospital outpatient and emergency departments with EHR technology able to support nine Stage 1 Meaningful
Use objectives: United States, 2011
NOTES: Data include nonfederal hospitals. In 2011, information on nine Stage 1 Meaningful Use objectives was collected in the National Hospital Ambulatory
Medical Care Survey. See reference 4 for Stage 1 Meaningful Use objectives. EHR is electronic health record.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2011.
14.4
16.4
0
14
15
16
17
Emergency department Outpatient department
■ 5 ■
In 2011, a limited number of EDs and OPDs had an EHR system that
supported nine Stage 1 Meaningful Use objectives.
● In 2011, information on 9 of 14 Stage 1 Meaningful Use objectives was collected in
NHAMCS.
● In 2011, 14% of EDs had EHR technology able to support 9 of 14 Stage 1 Meaningful Use
objectives, while 16% of OPDs had such EHR technology (Figure 5).
Percent of hospital departments
Figure 5. Hospital outpatient and emergency departments with EHR technology able to support nine Stage 1 Meaningful
Use objectives: United States, 2011
NOTES: Data include nonfederal hospitals. In 2011, information on nine Stage 1 Meaningful Use objectives was collected in the National Hospital Ambulatory
Medical Care Survey. See reference 4 for Stage 1 Meaningful Use objectives. EHR is electronic health record.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2011.
14.4
16.4
0
14
15
16
17
Emergency department Outpatient department
NCHS Data Brief ■ No. 187 ■ February 2015
■ 6 ■
Summary
Adoption of EHRs by hospital EDs and OPDs has increased. From 2006 through 2011, use of
EHR systems increased significantly. In 2011, 84% of EDs and 73% of OPDs used an EHR
system.
From 2007 through 2011, the percentage of hospitals reporting having an EHR system that met
the criteria for a basic system increased among EDs (from 19% to 54%) and OPDs (from 9% to
57%).
The HITECH Act of 2009 gave hospitals monetary incentives to adopt EHR systems. To receive
incentive payments through the Centers for Medicare & Medicaid Services, hospitals had to meet
federal standards of “meaningful use” of EHRs in three stages. Payments for Stage 1 of the EHR
Incentive Programs began in fiscal year 2011, and payments for Stage 2 began in fiscal year 2014.
From 2007 through 2011, five EHR Stage 1 core set objectives for demonstrating meaningful use
were consistently collected in NHAMCS. Four of these five objectives increased significantly
in both EDs and OPDs from 2007 through 2011. In 2011, information on 9 of the 14 Stage 1
Meaningful Use objectives was collected in NHAMCS. Using 2011 data, the year with the
most complete data on hospital readiness to meet Stage 1 core set objectives for demonstrating
meaningful use, this report found that 14% of EDs and 16% of OPDs had EHR technology able to
support nine Stage 1 core set objectives.
This study is limited in that its estimate of hospital readiness for Stage 1 Meaningful Use
objectives overestimates hospital readiness because NHAMCS only measures 9 of 14 objectives,
and hospital departments are limited to EDs and OPDs. To receive Meaningful Use incentive
payments, hospitals have to meet 14 core set objectives and 5 of 10 menu set objectives.
Definitions
Basic system: A system that had all of the following functionalities: patient history and
demographics, patient problem lists, physician clinical notes, comprehensive list of patients’
medications and allergies, computerized orders for prescriptions, and ability to view laboratory
and imaging results electronically (3).
Demonstrating meaningful use: The Medicare and Medicaid EHR Incentive Programs provide
incentive payments to hospitals as they demonstrate meaningful use of certified EHR technology.
The Centers for Medicare & Medicaid Services established the objectives for meaningful use in
three stages that hospitals must meet in order to receive an incentive payment (4). From 2011
through 2012, hospitals could receive incentive payments if they demonstrated 14 of the Stage
1 core objectives for meaningful use, and 5 of 10 menu set objectives. The full list of Stage 1
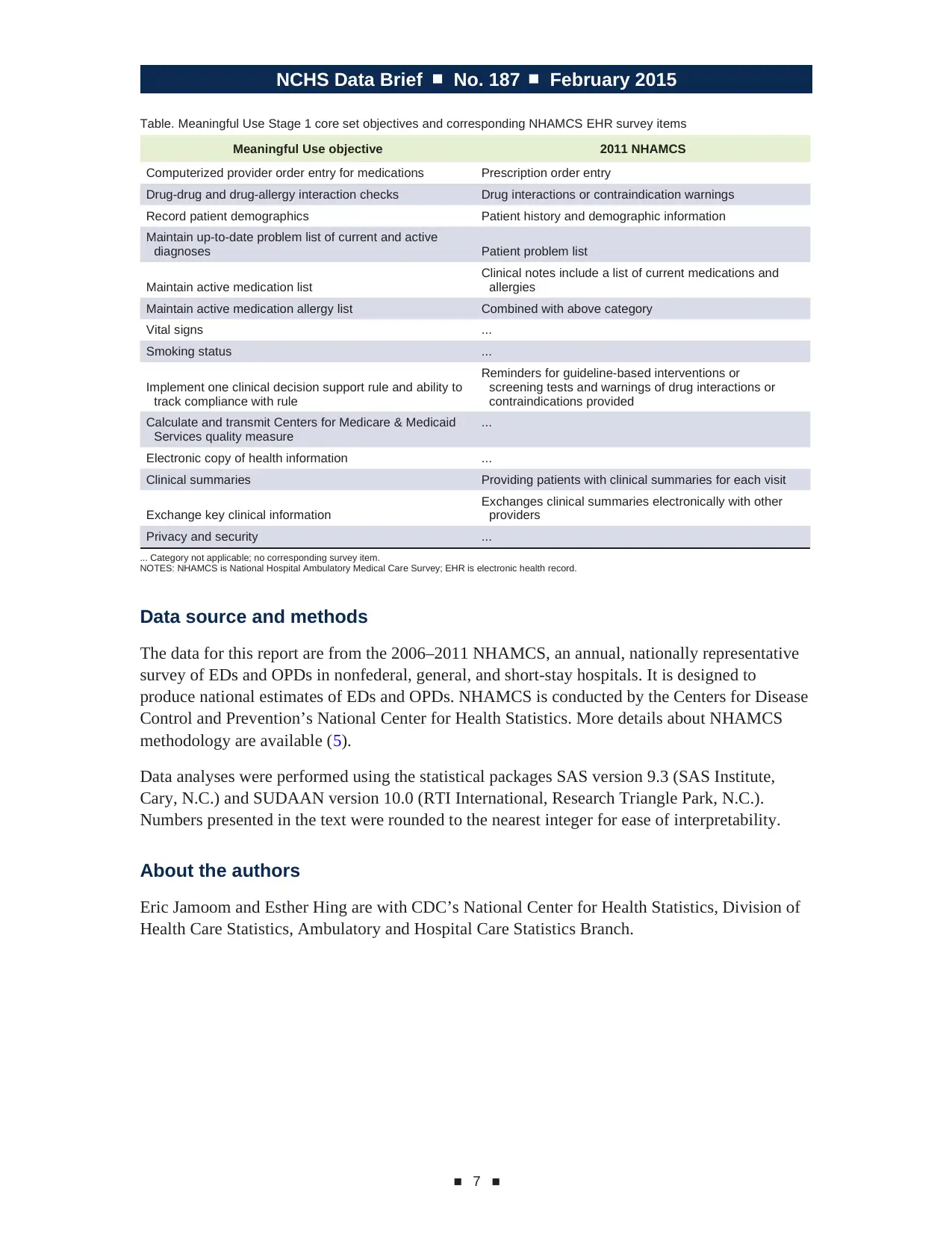
objectives and measures is published (1,2). The Table presents Stage 1 Meaningful Use core set
objectives and corresponding 2011 NHAMCS EHR survey items.
■ 6 ■
Summary
Adoption of EHRs by hospital EDs and OPDs has increased. From 2006 through 2011, use of
EHR systems increased significantly. In 2011, 84% of EDs and 73% of OPDs used an EHR
system.
From 2007 through 2011, the percentage of hospitals reporting having an EHR system that met
the criteria for a basic system increased among EDs (from 19% to 54%) and OPDs (from 9% to
57%).
The HITECH Act of 2009 gave hospitals monetary incentives to adopt EHR systems. To receive
incentive payments through the Centers for Medicare & Medicaid Services, hospitals had to meet
federal standards of “meaningful use” of EHRs in three stages. Payments for Stage 1 of the EHR
Incentive Programs began in fiscal year 2011, and payments for Stage 2 began in fiscal year 2014.
From 2007 through 2011, five EHR Stage 1 core set objectives for demonstrating meaningful use
were consistently collected in NHAMCS. Four of these five objectives increased significantly
in both EDs and OPDs from 2007 through 2011. In 2011, information on 9 of the 14 Stage 1
Meaningful Use objectives was collected in NHAMCS. Using 2011 data, the year with the
most complete data on hospital readiness to meet Stage 1 core set objectives for demonstrating
meaningful use, this report found that 14% of EDs and 16% of OPDs had EHR technology able to
support nine Stage 1 core set objectives.
This study is limited in that its estimate of hospital readiness for Stage 1 Meaningful Use
objectives overestimates hospital readiness because NHAMCS only measures 9 of 14 objectives,
and hospital departments are limited to EDs and OPDs. To receive Meaningful Use incentive
payments, hospitals have to meet 14 core set objectives and 5 of 10 menu set objectives.
Definitions
Basic system: A system that had all of the following functionalities: patient history and
demographics, patient problem lists, physician clinical notes, comprehensive list of patients’
medications and allergies, computerized orders for prescriptions, and ability to view laboratory
and imaging results electronically (3).
Demonstrating meaningful use: The Medicare and Medicaid EHR Incentive Programs provide
incentive payments to hospitals as they demonstrate meaningful use of certified EHR technology.
The Centers for Medicare & Medicaid Services established the objectives for meaningful use in
three stages that hospitals must meet in order to receive an incentive payment (4). From 2011
through 2012, hospitals could receive incentive payments if they demonstrated 14 of the Stage
1 core objectives for meaningful use, and 5 of 10 menu set objectives. The full list of Stage 1
objectives and measures is published (1,2). The Table presents Stage 1 Meaningful Use core set
objectives and corresponding 2011 NHAMCS EHR survey items.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
NCHS Data Brief ■ No. 187 ■ February 2015
■ 7 ■
Table. Meaningful Use Stage 1 core set objectives and corresponding NHAMCS EHR survey items
Meaningful Use objective 2011 NHAMCS
Computerized provider order entry for medications Prescription order entry
Drug-drug and drug-allergy interaction checks Drug interactions or contraindication warnings
Record patient demographics Patient history and demographic information
Maintain up-to-date problem list of current and active
diagnoses Patient problem list
Clinical notes include a list of current medications and
Maintain active medication list allergies
Maintain active medication allergy list Combined with above category
Vital signs ...
Smoking status ...
Reminders for guideline-based interventions or
Implement one clinical decision support rule and ability to screening tests and warnings of drug interactions or
track compliance with rule contraindications provided
Calculate and transmit Centers for Medicare & Medicaid ...
Services quality measure
Electronic copy of health information ...
Clinical summaries Providing patients with clinical summaries for each visit
Exchanges clinical summaries electronically with other
Exchange key clinical information providers
Privacy and security ...
... Category not applicable; no corresponding survey item.
NOTES: NHAMCS is National Hospital Ambulatory Medical Care Survey; EHR is electronic health record.
Data source and methods
The data for this report are from the 2006–2011 NHAMCS, an annual, nationally representative
survey of EDs and OPDs in nonfederal, general, and short-stay hospitals. It is designed to
produce national estimates of EDs and OPDs. NHAMCS is conducted by the Centers for Disease
Control and Prevention’s National Center for Health Statistics. More details about NHAMCS
methodology are available (5).
Data analyses were performed using the statistical packages SAS version 9.3 (SAS Institute,
Cary, N.C.) and SUDAAN version 10.0 (RTI International, Research Triangle Park, N.C.).
Numbers presented in the text were rounded to the nearest integer for ease of interpretability.
About the authors
Eric Jamoom and Esther Hing are with CDC’s National Center for Health Statistics, Division of
Health Care Statistics, Ambulatory and Hospital Care Statistics Branch.
■ 7 ■
Table. Meaningful Use Stage 1 core set objectives and corresponding NHAMCS EHR survey items
Meaningful Use objective 2011 NHAMCS
Computerized provider order entry for medications Prescription order entry
Drug-drug and drug-allergy interaction checks Drug interactions or contraindication warnings
Record patient demographics Patient history and demographic information
Maintain up-to-date problem list of current and active
diagnoses Patient problem list
Clinical notes include a list of current medications and
Maintain active medication list allergies
Maintain active medication allergy list Combined with above category
Vital signs ...
Smoking status ...
Reminders for guideline-based interventions or
Implement one clinical decision support rule and ability to screening tests and warnings of drug interactions or
track compliance with rule contraindications provided
Calculate and transmit Centers for Medicare & Medicaid ...
Services quality measure
Electronic copy of health information ...
Clinical summaries Providing patients with clinical summaries for each visit
Exchanges clinical summaries electronically with other
Exchange key clinical information providers
Privacy and security ...
... Category not applicable; no corresponding survey item.
NOTES: NHAMCS is National Hospital Ambulatory Medical Care Survey; EHR is electronic health record.
Data source and methods
The data for this report are from the 2006–2011 NHAMCS, an annual, nationally representative
survey of EDs and OPDs in nonfederal, general, and short-stay hospitals. It is designed to
produce national estimates of EDs and OPDs. NHAMCS is conducted by the Centers for Disease
Control and Prevention’s National Center for Health Statistics. More details about NHAMCS
methodology are available (5).
Data analyses were performed using the statistical packages SAS version 9.3 (SAS Institute,
Cary, N.C.) and SUDAAN version 10.0 (RTI International, Research Triangle Park, N.C.).
Numbers presented in the text were rounded to the nearest integer for ease of interpretability.
About the authors
Eric Jamoom and Esther Hing are with CDC’s National Center for Health Statistics, Division of
Health Care Statistics, Ambulatory and Hospital Care Statistics Branch.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
NCHS Data Brief ■ No. 187 ■ February 2015
First Class mail
Postage & Fees Paid
CdC/NCHs
Permit No. g-284
References
1. Blumenthal D, Tavenner M. The “meaningful use” regulation for
electronic health records. N Engl J Med 363(6):501–4. 2010.
2. Hing E, Hall MJ, Ashman JJ. Use of electronic medical records by
ambulatory care providers: United States, 2006. National health statistics
reports; no 22. Hyattsville, MD: National Center for Health Statistics. 2010.
Available from: http://www.cdc.gov/nchs/data/nhsr/nhsr022.pdf.
3. Hsiao CJ, Hing E, Socey TC, Cai B. Electronic health record systems and
intent to apply for meaningful use incentives among office-based physician
practices: United States, 2001–2011. NCHS data brief, no 79. Hyattsville,
MD: National Center for Health Statistics. 2011. Available from: http://www.
cdc.gov/nchs/data/databriefs/db79.htm.
4. Centers for Medicare & Medicaid Services. EHR incentive programs:
The official web site for the Medicare and Medicaid electronic health
records (EHR) incentive programs. Available from: https://www.cms.gov/
Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.
html?redirect=/ehrincentiveprograms.
5. NCHS. National Hospital Ambulatory Medical Care Survey. Public-use
data file documentation, 2001–2010. Available from: ftp://ftp.cdc.gov/pub/
Health_Statistics/NCHS/Dataset_Documentation/NHAMCS/.
Suggested citation
Jamoom E, Hing E. Progress with electronic
health record adoption among emergency
and outpatient departments: United States,
2006–2011. NCHS data brief, no 187.
Hyattsville, MD: National Center for Health
Statistics. 2015.
Copyright information
All material appearing in this report is in
the public domain and may be reproduced
or copied without permission; citation as to
source, however, is appreciated.
National Center for Health
Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Nathaniel Schenker, Ph.D., Deputy Director
Jennifer H. Madans, Ph.D., Associate
Director for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director
For e-mail updates on NCHS publication
releases, subscribe online at:
http://www.cdc.gov/nchs/govdelivery.htm.
For questions or general information
about NCHS:
Tel: 1–800–CDC–INFO (1–800–232–4636)
TTY: 1–888–232–6348
Internet: http://www.cdc.gov/nchs
Online request form: http://www.cdc.gov/info
ISSN 1941–4927 Print ed.
ISSN 1941–4935 Online ed.
DHHS Publication No. 2015–1209
CS253963
U.S. Department of
HealtH & HUman ServiceS
Centers for Disease Control and Prevention
National Center for Health Statistics
3311 Toledo Road, Room 5419
Hyattsville, MD 20782–2064
OffiCial BuSiNeSS
PeNalTy fOR PRivaTe uSe, $300
For more NCHS Data Briefs, visit:
http://www.cdc.gov/nchs/products/databriefs.htm.
First Class mail
Postage & Fees Paid
CdC/NCHs
Permit No. g-284
References
1. Blumenthal D, Tavenner M. The “meaningful use” regulation for
electronic health records. N Engl J Med 363(6):501–4. 2010.
2. Hing E, Hall MJ, Ashman JJ. Use of electronic medical records by
ambulatory care providers: United States, 2006. National health statistics
reports; no 22. Hyattsville, MD: National Center for Health Statistics. 2010.
Available from: http://www.cdc.gov/nchs/data/nhsr/nhsr022.pdf.
3. Hsiao CJ, Hing E, Socey TC, Cai B. Electronic health record systems and
intent to apply for meaningful use incentives among office-based physician
practices: United States, 2001–2011. NCHS data brief, no 79. Hyattsville,
MD: National Center for Health Statistics. 2011. Available from: http://www.
cdc.gov/nchs/data/databriefs/db79.htm.
4. Centers for Medicare & Medicaid Services. EHR incentive programs:
The official web site for the Medicare and Medicaid electronic health
records (EHR) incentive programs. Available from: https://www.cms.gov/
Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.
html?redirect=/ehrincentiveprograms.
5. NCHS. National Hospital Ambulatory Medical Care Survey. Public-use
data file documentation, 2001–2010. Available from: ftp://ftp.cdc.gov/pub/
Health_Statistics/NCHS/Dataset_Documentation/NHAMCS/.
Suggested citation
Jamoom E, Hing E. Progress with electronic
health record adoption among emergency
and outpatient departments: United States,
2006–2011. NCHS data brief, no 187.
Hyattsville, MD: National Center for Health
Statistics. 2015.
Copyright information
All material appearing in this report is in
the public domain and may be reproduced
or copied without permission; citation as to
source, however, is appreciated.
National Center for Health
Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Nathaniel Schenker, Ph.D., Deputy Director
Jennifer H. Madans, Ph.D., Associate
Director for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director
For e-mail updates on NCHS publication
releases, subscribe online at:
http://www.cdc.gov/nchs/govdelivery.htm.
For questions or general information
about NCHS:
Tel: 1–800–CDC–INFO (1–800–232–4636)
TTY: 1–888–232–6348
Internet: http://www.cdc.gov/nchs
Online request form: http://www.cdc.gov/info
ISSN 1941–4927 Print ed.
ISSN 1941–4935 Online ed.
DHHS Publication No. 2015–1209
CS253963
U.S. Department of
HealtH & HUman ServiceS
Centers for Disease Control and Prevention
National Center for Health Statistics
3311 Toledo Road, Room 5419
Hyattsville, MD 20782–2064
OffiCial BuSiNeSS
PeNalTy fOR PRivaTe uSe, $300
For more NCHS Data Briefs, visit:
http://www.cdc.gov/nchs/products/databriefs.htm.
1 out of 8
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.