UTS - Epidemiology: Analysis of Cancer Death Rates in Australia & KSA
VerifiedAdded on 2023/06/14
|8
|2627
|90
Homework Assignment
AI Summary
This assignment provides a detailed analysis of cancer death rates in Australia and Saudi Arabia for the year 2012, including crude and age-specific death rates. It calculates and compares age-standardized death rates using the direct standardization method. The assignment also examines infant mortality rates based on birth weight, calculating risk ratios, absolute differences in incidence, and attributable fractions. Furthermore, it includes a case-control study investigating the association between smoking and human papillomavirus (HPV) infection of the cervix, utilizing chi-square tests to determine the statistical significance of the relationship, while considering confounding factors and effect modifiers such as the number of lifetime sexual partners. The assignment provides comprehensive tables and figures to support the analysis and findings.
Running head: EPIDEMIOLOGY
Epidemiology
Name of the Student:
Name of the University:
Author’s Note:
Epidemiology
Name of the Student:
Name of the University:
Author’s Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1EPIDEMIOLOGY
Table of Contents
Question 1....................................................................................................................................................................................................2
1...............................................................................................................................................................................................................2
1. a)......................................................................................................................................................................................................2
1. b)......................................................................................................................................................................................................2
1. c)......................................................................................................................................................................................................2
1. d)......................................................................................................................................................................................................3
2...............................................................................................................................................................................................................3
2. a)......................................................................................................................................................................................................3
2. b)......................................................................................................................................................................................................4
Question 2....................................................................................................................................................................................................4
1...............................................................................................................................................................................................................4
2...............................................................................................................................................................................................................5
3...............................................................................................................................................................................................................5
4...............................................................................................................................................................................................................5
5...............................................................................................................................................................................................................5
6...............................................................................................................................................................................................................5
7...............................................................................................................................................................................................................5
Question 3....................................................................................................................................................................................................5
1...............................................................................................................................................................................................................5
2...............................................................................................................................................................................................................6
3...............................................................................................................................................................................................................6
References:..................................................................................................................................................................................................7
Table of Contents
Question 1....................................................................................................................................................................................................2
1...............................................................................................................................................................................................................2
1. a)......................................................................................................................................................................................................2
1. b)......................................................................................................................................................................................................2
1. c)......................................................................................................................................................................................................2
1. d)......................................................................................................................................................................................................3
2...............................................................................................................................................................................................................3
2. a)......................................................................................................................................................................................................3
2. b)......................................................................................................................................................................................................4
Question 2....................................................................................................................................................................................................4
1...............................................................................................................................................................................................................4
2...............................................................................................................................................................................................................5
3...............................................................................................................................................................................................................5
4...............................................................................................................................................................................................................5
5...............................................................................................................................................................................................................5
6...............................................................................................................................................................................................................5
7...............................................................................................................................................................................................................5
Question 3....................................................................................................................................................................................................5
1...............................................................................................................................................................................................................5
2...............................................................................................................................................................................................................6
3...............................................................................................................................................................................................................6
References:..................................................................................................................................................................................................7
2EPIDEMIOLOGY
Question 1.
1.
Table 1: Crude and age-specific death rates due to cancer, Australia, 2012
Table 1: Crude and age-specific death rates due to cancer, Australia, 2012
Age group Deaths Total Population Death rate per 100,000 population
0-14 83 4293707 1.933061571
15-39 618 7986708 7.737856448
40-44 486 1573829 30.88010197
45-49 1017 1574299 64.60018078
50-54 1775 1541187 115.1709689
55-59 2687 1429322 187.9912294
60-64 4090 1304820 313.4531966
65-69 5174 1130258 457.7715884
70-74 5717 871194 656.2258234
75+ 21756 1436087 1514.95
Total 43403 23141411 187.5555471
Table 2: Crude and age-specific death rates due to cancer, Saudi Arabia, 2012
Table 1: Crude and age-specific death rates due to cancer, Saudi Arabia, 2012
Age group Deaths Total Population Death rate per 100,000 population
0-14 543 8134561 6.675221933
15-39 932 13600843 6.852516421
40-44 426 2261777 18.83474808
45-49 540 1709816 31.5823457
50-54 774 1200372 64.4800112
55-59 1084 812708 133.381239
60-64 1089 505266 215.5300376
65-69 1102 328827 335.130631
70-74 880 239961 366.7262597
75+ 1764 292226 603.6423864
Total 9134 29086357 31.40303889
1. a)
The crude death rate of Australia in 2012 = 187.556 (Roglic and Unwin 2010).
The crude death rate of Saudi Arabia in 2012 = 31.403.
1. b)
Table 3: The age-specific death rates are shown in the table of Australia and Saudi Arabia.
Age group Age-specific death rate in Australia
Age-specific death rate in Saudi
Arabia
0-14 1.933061571 6.675221933
15-39 7.737856448 6.852516421
40-44 30.88010197 18.83474808
45-49 64.60018078 31.5823457
50-54 115.1709689 64.4800112
55-59 187.9912294 133.381239
60-64 313.4531966 215.5300376
65-69 457.7715884 335.130631
70-74 656.2258234 366.7262597
75+ 1514.95 603.6423864
1. c)
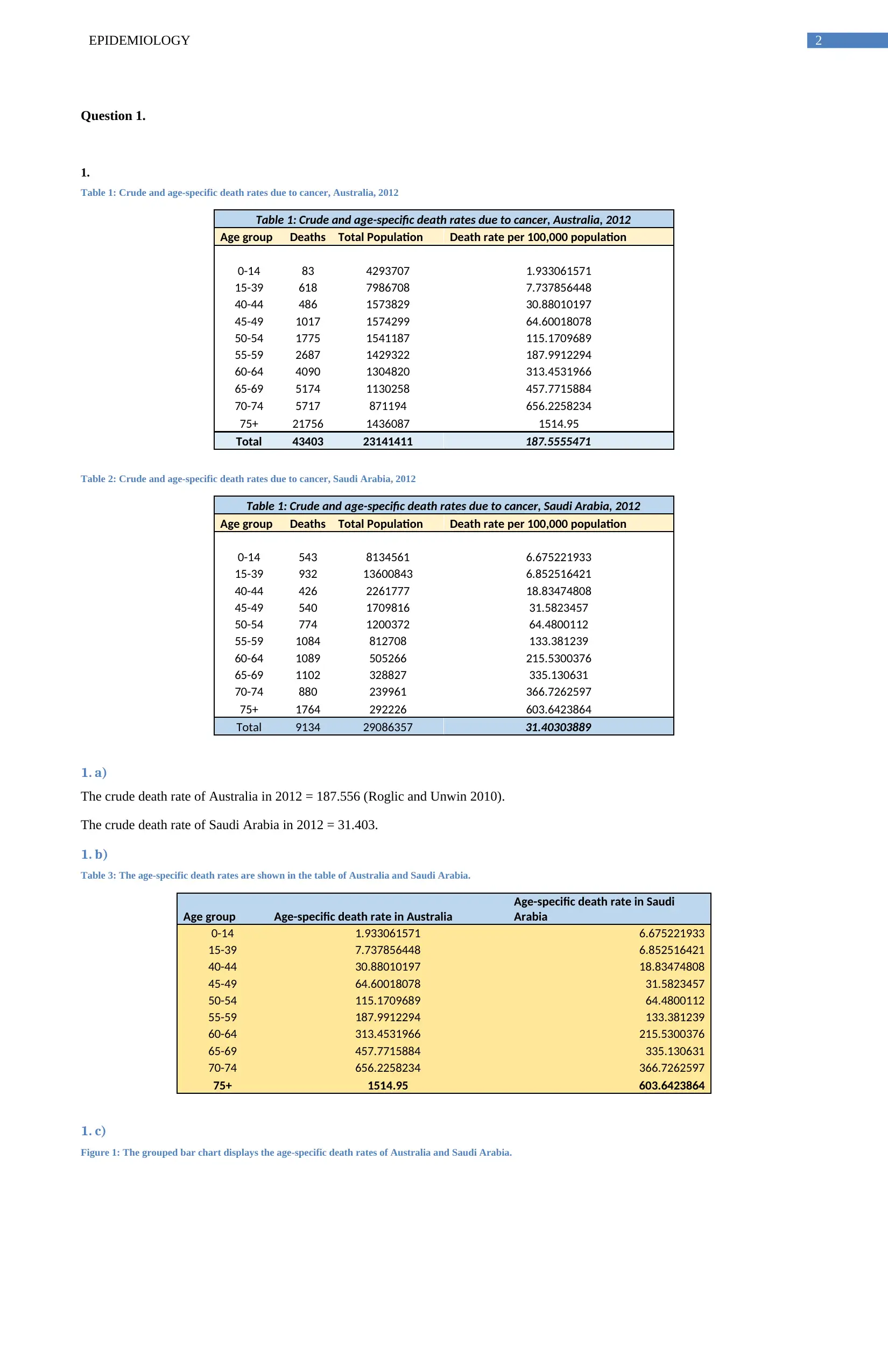
Figure 1: The grouped bar chart displays the age-specific death rates of Australia and Saudi Arabia.
Question 1.
1.
Table 1: Crude and age-specific death rates due to cancer, Australia, 2012
Table 1: Crude and age-specific death rates due to cancer, Australia, 2012
Age group Deaths Total Population Death rate per 100,000 population
0-14 83 4293707 1.933061571
15-39 618 7986708 7.737856448
40-44 486 1573829 30.88010197
45-49 1017 1574299 64.60018078
50-54 1775 1541187 115.1709689
55-59 2687 1429322 187.9912294
60-64 4090 1304820 313.4531966
65-69 5174 1130258 457.7715884
70-74 5717 871194 656.2258234
75+ 21756 1436087 1514.95
Total 43403 23141411 187.5555471
Table 2: Crude and age-specific death rates due to cancer, Saudi Arabia, 2012
Table 1: Crude and age-specific death rates due to cancer, Saudi Arabia, 2012
Age group Deaths Total Population Death rate per 100,000 population
0-14 543 8134561 6.675221933
15-39 932 13600843 6.852516421
40-44 426 2261777 18.83474808
45-49 540 1709816 31.5823457
50-54 774 1200372 64.4800112
55-59 1084 812708 133.381239
60-64 1089 505266 215.5300376
65-69 1102 328827 335.130631
70-74 880 239961 366.7262597
75+ 1764 292226 603.6423864
Total 9134 29086357 31.40303889
1. a)
The crude death rate of Australia in 2012 = 187.556 (Roglic and Unwin 2010).
The crude death rate of Saudi Arabia in 2012 = 31.403.
1. b)
Table 3: The age-specific death rates are shown in the table of Australia and Saudi Arabia.
Age group Age-specific death rate in Australia
Age-specific death rate in Saudi
Arabia
0-14 1.933061571 6.675221933
15-39 7.737856448 6.852516421
40-44 30.88010197 18.83474808
45-49 64.60018078 31.5823457
50-54 115.1709689 64.4800112
55-59 187.9912294 133.381239
60-64 313.4531966 215.5300376
65-69 457.7715884 335.130631
70-74 656.2258234 366.7262597
75+ 1514.95 603.6423864
1. c)
Figure 1: The grouped bar chart displays the age-specific death rates of Australia and Saudi Arabia.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3EPIDEMIOLOGY
0-14 15-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+
0
200
400
600
800
1000
1200
1400
1600
Age-specifi c death rates of Australia and Saudi Arabia
Age-specific death rate in Australia Age-specific death rate in Saudi Arabia
Age groups
Death Rates
1. d)
The grouped bar chart displays that-
The age specific death rates are greater for higher ages rather than lower ages in both the countries (Smink, Van Hoeken and Hoek
2012). The age specific death rates are higher in Australia rather than Saudi Arabia throughout all the age groups. The difference of
age specific death rates is prominent in the age group of 75+ years between Australia and Saudi Arabia. The rate is minimum in case
of children (0-14 years) in Saudi Arabia and maximum in case of old-aged (75+) persons in Australia.
2.
2. a)
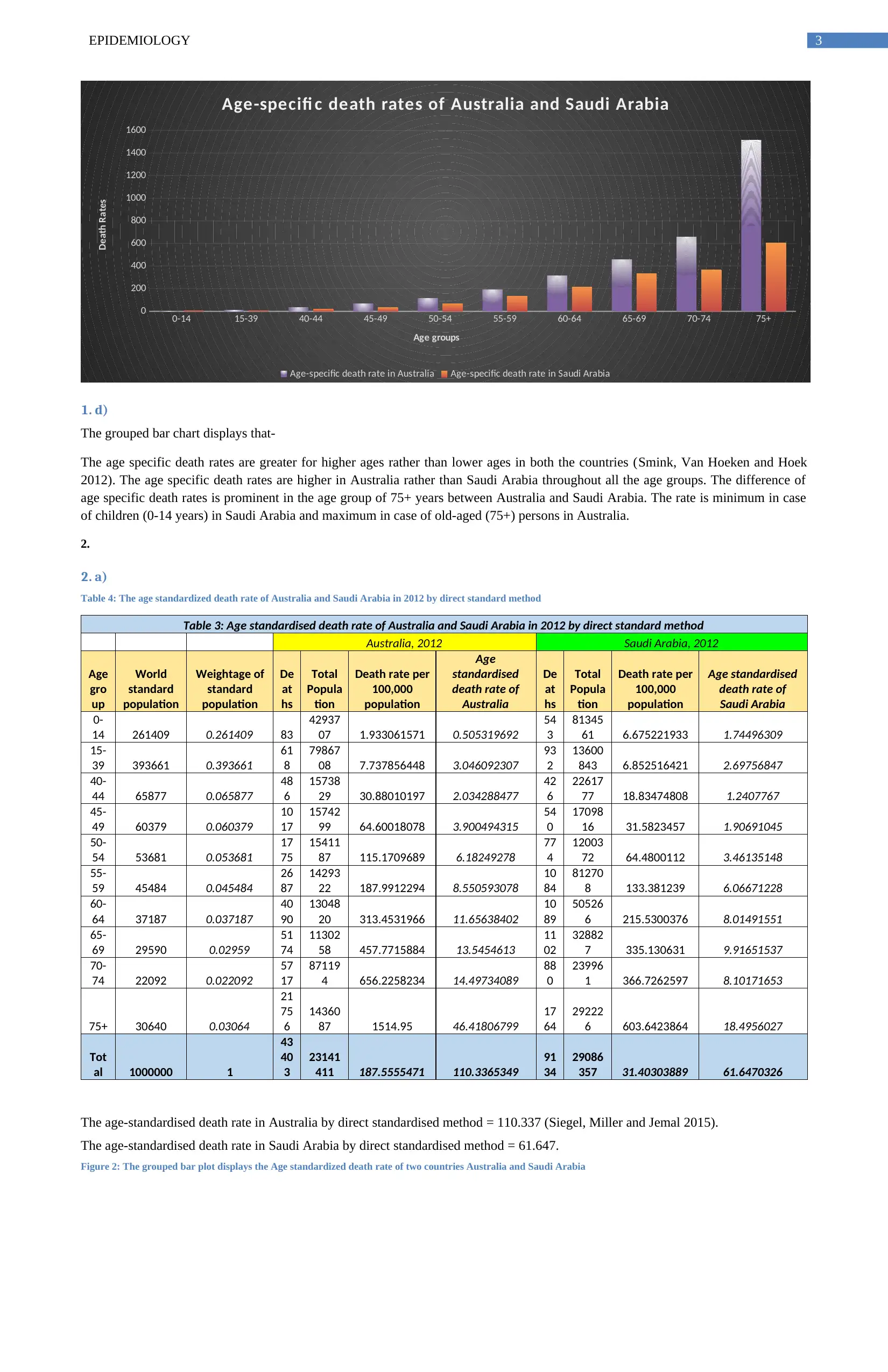
Table 4: The age standardized death rate of Australia and Saudi Arabia in 2012 by direct standard method
Table 3: Age standardised death rate of Australia and Saudi Arabia in 2012 by direct standard method
Australia, 2012 Saudi Arabia, 2012
Age
gro
up
World
standard
population
Weightage of
standard
population
De
at
hs
Total
Popula
tion
Death rate per
100,000
population
Age
standardised
death rate of
Australia
De
at
hs
Total
Popula
tion
Death rate per
100,000
population
Age standardised
death rate of
Saudi Arabia
0-
14 261409 0.261409 83
42937
07 1.933061571 0.505319692
54
3
81345
61 6.675221933 1.74496309
15-
39 393661 0.393661
61
8
79867
08 7.737856448 3.046092307
93
2
13600
843 6.852516421 2.69756847
40-
44 65877 0.065877
48
6
15738
29 30.88010197 2.034288477
42
6
22617
77 18.83474808 1.2407767
45-
49 60379 0.060379
10
17
15742
99 64.60018078 3.900494315
54
0
17098
16 31.5823457 1.90691045
50-
54 53681 0.053681
17
75
15411
87 115.1709689 6.18249278
77
4
12003
72 64.4800112 3.46135148
55-
59 45484 0.045484
26
87
14293
22 187.9912294 8.550593078
10
84
81270
8 133.381239 6.06671228
60-
64 37187 0.037187
40
90
13048
20 313.4531966 11.65638402
10
89
50526
6 215.5300376 8.01491551
65-
69 29590 0.02959
51
74
11302
58 457.7715884 13.5454613
11
02
32882
7 335.130631 9.91651537
70-
74 22092 0.022092
57
17
87119
4 656.2258234 14.49734089
88
0
23996
1 366.7262597 8.10171653
75+ 30640 0.03064
21
75
6
14360
87 1514.95 46.41806799
17
64
29222
6 603.6423864 18.4956027
Tot
al 1000000 1
43
40
3
23141
411 187.5555471 110.3365349
91
34
29086
357 31.40303889 61.6470326
The age-standardised death rate in Australia by direct standardised method = 110.337 (Siegel, Miller and Jemal 2015).
The age-standardised death rate in Saudi Arabia by direct standardised method = 61.647.
Figure 2: The grouped bar plot displays the Age standardized death rate of two countries Australia and Saudi Arabia
0-14 15-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+
0
200
400
600
800
1000
1200
1400
1600
Age-specifi c death rates of Australia and Saudi Arabia
Age-specific death rate in Australia Age-specific death rate in Saudi Arabia
Age groups
Death Rates
1. d)
The grouped bar chart displays that-
The age specific death rates are greater for higher ages rather than lower ages in both the countries (Smink, Van Hoeken and Hoek
2012). The age specific death rates are higher in Australia rather than Saudi Arabia throughout all the age groups. The difference of
age specific death rates is prominent in the age group of 75+ years between Australia and Saudi Arabia. The rate is minimum in case
of children (0-14 years) in Saudi Arabia and maximum in case of old-aged (75+) persons in Australia.
2.
2. a)
Table 4: The age standardized death rate of Australia and Saudi Arabia in 2012 by direct standard method
Table 3: Age standardised death rate of Australia and Saudi Arabia in 2012 by direct standard method
Australia, 2012 Saudi Arabia, 2012
Age
gro
up
World
standard
population
Weightage of
standard
population
De
at
hs
Total
Popula
tion
Death rate per
100,000
population
Age
standardised
death rate of
Australia
De
at
hs
Total
Popula
tion
Death rate per
100,000
population
Age standardised
death rate of
Saudi Arabia
0-
14 261409 0.261409 83
42937
07 1.933061571 0.505319692
54
3
81345
61 6.675221933 1.74496309
15-
39 393661 0.393661
61
8
79867
08 7.737856448 3.046092307
93
2
13600
843 6.852516421 2.69756847
40-
44 65877 0.065877
48
6
15738
29 30.88010197 2.034288477
42
6
22617
77 18.83474808 1.2407767
45-
49 60379 0.060379
10
17
15742
99 64.60018078 3.900494315
54
0
17098
16 31.5823457 1.90691045
50-
54 53681 0.053681
17
75
15411
87 115.1709689 6.18249278
77
4
12003
72 64.4800112 3.46135148
55-
59 45484 0.045484
26
87
14293
22 187.9912294 8.550593078
10
84
81270
8 133.381239 6.06671228
60-
64 37187 0.037187
40
90
13048
20 313.4531966 11.65638402
10
89
50526
6 215.5300376 8.01491551
65-
69 29590 0.02959
51
74
11302
58 457.7715884 13.5454613
11
02
32882
7 335.130631 9.91651537
70-
74 22092 0.022092
57
17
87119
4 656.2258234 14.49734089
88
0
23996
1 366.7262597 8.10171653
75+ 30640 0.03064
21
75
6
14360
87 1514.95 46.41806799
17
64
29222
6 603.6423864 18.4956027
Tot
al 1000000 1
43
40
3
23141
411 187.5555471 110.3365349
91
34
29086
357 31.40303889 61.6470326
The age-standardised death rate in Australia by direct standardised method = 110.337 (Siegel, Miller and Jemal 2015).
The age-standardised death rate in Saudi Arabia by direct standardised method = 61.647.
Figure 2: The grouped bar plot displays the Age standardized death rate of two countries Australia and Saudi Arabia
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4EPIDEMIOLOGY
0-14 15-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+
0
5
10
15
20
25
30
35
40
45
50
Age standardised death rate of two countries Australia and Saudi
Arabia
Age standardised death rate of Australia Age standardised death rate of Saudi Arabia
Age groups
Age standardised death rates
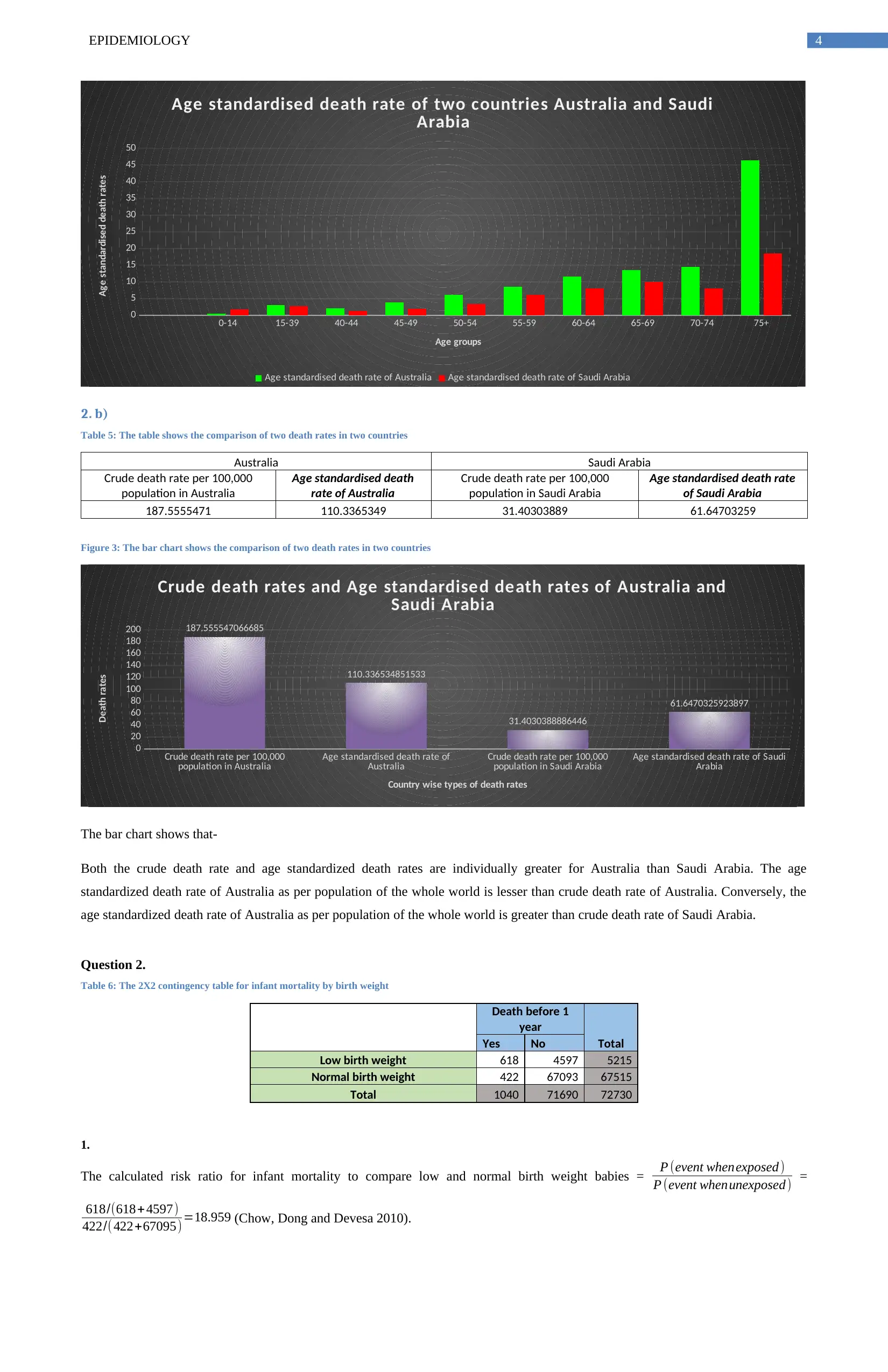
2. b)
Table 5: The table shows the comparison of two death rates in two countries
Australia Saudi Arabia
Crude death rate per 100,000
population in Australia
Age standardised death
rate of Australia
Crude death rate per 100,000
population in Saudi Arabia
Age standardised death rate
of Saudi Arabia
187.5555471 110.3365349 31.40303889 61.64703259
Figure 3: The bar chart shows the comparison of two death rates in two countries
Crude death rate per 100,000
population in Australia Age standardised death rate of
Australia Crude death rate per 100,000
population in Saudi Arabia Age standardised death rate of Saudi
Arabia
0
20
40
60
80
100
120
140
160
180
200 187.555547066685
110.336534851533
31.4030388886446
61.6470325923897
Crude death rates and Age standardised death rates of Australia and
Saudi Arabia
Country wise types of death rates
Death rates
The bar chart shows that-
Both the crude death rate and age standardized death rates are individually greater for Australia than Saudi Arabia. The age
standardized death rate of Australia as per population of the whole world is lesser than crude death rate of Australia. Conversely, the
age standardized death rate of Australia as per population of the whole world is greater than crude death rate of Saudi Arabia.
Question 2.
Table 6: The 2X2 contingency table for infant mortality by birth weight
Death before 1
year
TotalYes No
Low birth weight 618 4597 5215
Normal birth weight 422 67093 67515
Total 1040 71690 72730
1.
The calculated risk ratio for infant mortality to compare low and normal birth weight babies = P (event whenexposed )
P (event whenunexposed) =
618/(618+ 4597)
422/( 422+67095)=18.959 (Chow, Dong and Devesa 2010).
0-14 15-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+
0
5
10
15
20
25
30
35
40
45
50
Age standardised death rate of two countries Australia and Saudi
Arabia
Age standardised death rate of Australia Age standardised death rate of Saudi Arabia
Age groups
Age standardised death rates
2. b)
Table 5: The table shows the comparison of two death rates in two countries
Australia Saudi Arabia
Crude death rate per 100,000
population in Australia
Age standardised death
rate of Australia
Crude death rate per 100,000
population in Saudi Arabia
Age standardised death rate
of Saudi Arabia
187.5555471 110.3365349 31.40303889 61.64703259
Figure 3: The bar chart shows the comparison of two death rates in two countries
Crude death rate per 100,000
population in Australia Age standardised death rate of
Australia Crude death rate per 100,000
population in Saudi Arabia Age standardised death rate of Saudi
Arabia
0
20
40
60
80
100
120
140
160
180
200 187.555547066685
110.336534851533
31.4030388886446
61.6470325923897
Crude death rates and Age standardised death rates of Australia and
Saudi Arabia
Country wise types of death rates
Death rates
The bar chart shows that-
Both the crude death rate and age standardized death rates are individually greater for Australia than Saudi Arabia. The age
standardized death rate of Australia as per population of the whole world is lesser than crude death rate of Australia. Conversely, the
age standardized death rate of Australia as per population of the whole world is greater than crude death rate of Saudi Arabia.
Question 2.
Table 6: The 2X2 contingency table for infant mortality by birth weight
Death before 1
year
TotalYes No
Low birth weight 618 4597 5215
Normal birth weight 422 67093 67515
Total 1040 71690 72730
1.
The calculated risk ratio for infant mortality to compare low and normal birth weight babies = P (event whenexposed )
P (event whenunexposed) =
618/(618+ 4597)
422/( 422+67095)=18.959 (Chow, Dong and Devesa 2010).
5EPIDEMIOLOGY
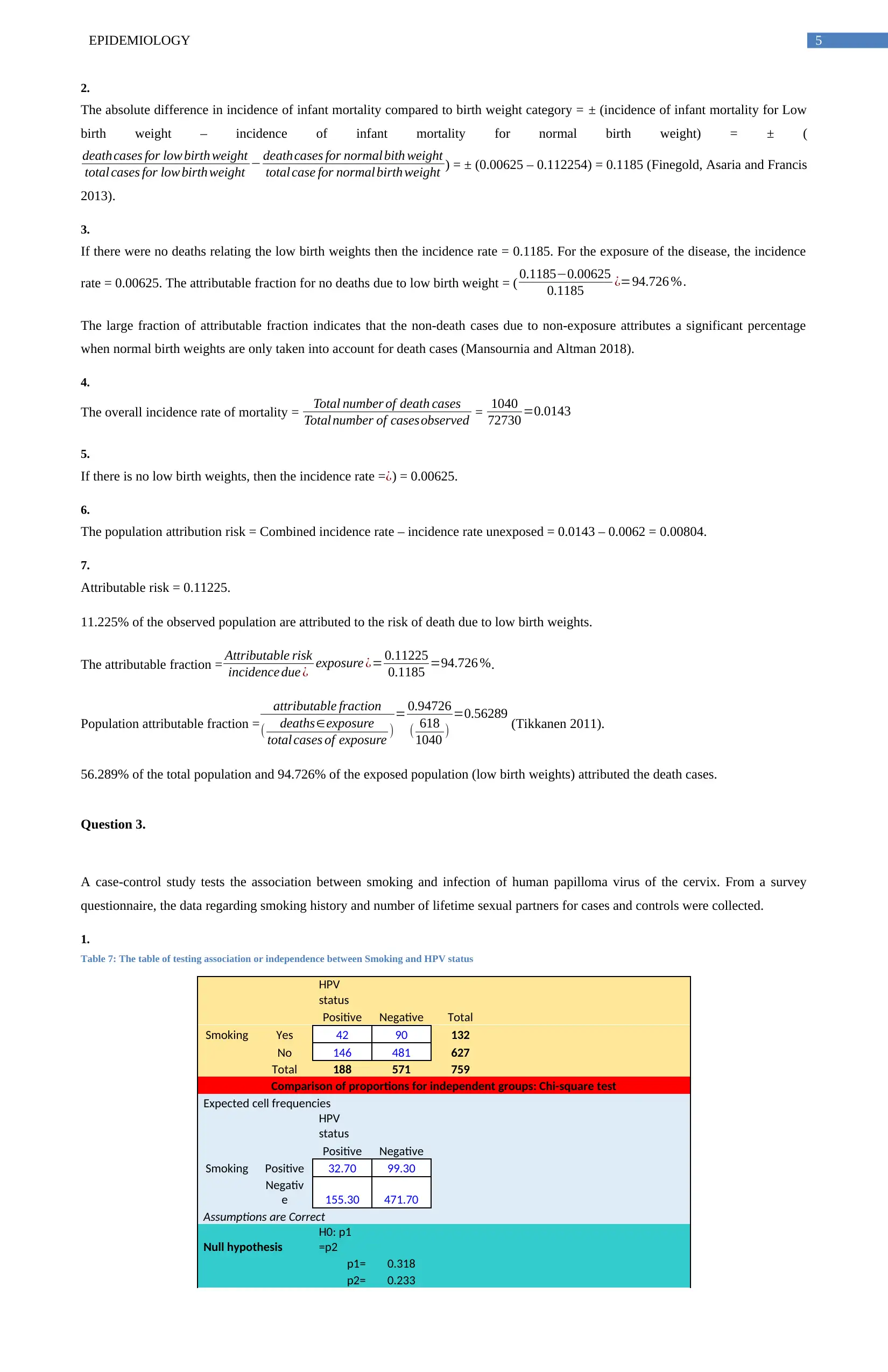
2.
The absolute difference in incidence of infant mortality compared to birth weight category = ± (incidence of infant mortality for Low
birth weight – incidence of infant mortality for normal birth weight) = ± (
death cases for low birth weight
total cases for low birth weight − deathcases for normal bith weight
total case for normal birth weight ) = ± (0.00625 – 0.112254) = 0.1185 (Finegold, Asaria and Francis
2013).
3.
If there were no deaths relating the low birth weights then the incidence rate = 0.1185. For the exposure of the disease, the incidence
rate = 0.00625. The attributable fraction for no deaths due to low birth weight = ( 0.1185−0.00625
0.1185 ¿=94.726 %.
The large fraction of attributable fraction indicates that the non-death cases due to non-exposure attributes a significant percentage
when normal birth weights are only taken into account for death cases (Mansournia and Altman 2018).
4.
The overall incidence rate of mortality = Total number of death cases
Total number of casesobserved = 1040
72730 =0.0143
5.
If there is no low birth weights, then the incidence rate = ¿) = 0.00625.
6.
The population attribution risk = Combined incidence rate – incidence rate unexposed = 0.0143 – 0.0062 = 0.00804.
7.
Attributable risk = 0.11225.
11.225% of the observed population are attributed to the risk of death due to low birth weights.
The attributable fraction = Attributable risk
incidence due ¿ exposure ¿= 0.11225
0.1185 =94.726 %.
Population attributable fraction =
attributable fraction
( deaths∈exposure
total cases of exposure )
= 0.94726
( 618
1040 )
=0.56289 (Tikkanen 2011).
56.289% of the total population and 94.726% of the exposed population (low birth weights) attributed the death cases.
Question 3.
A case-control study tests the association between smoking and infection of human papilloma virus of the cervix. From a survey
questionnaire, the data regarding smoking history and number of lifetime sexual partners for cases and controls were collected.
1.
Table 7: The table of testing association or independence between Smoking and HPV status
HPV
status
Positive Negative Total
Smoking Yes 42 90 132
No 146 481 627
Total 188 571 759
Comparison of proportions for independent groups: Chi-square test
Expected cell frequencies
HPV
status
Positive Negative
Smoking Positive 32.70 99.30
Negativ
e 155.30 471.70
Assumptions are Correct
Null hypothesis
H0: p1
=p2
p1= 0.318
p2= 0.233
2.
The absolute difference in incidence of infant mortality compared to birth weight category = ± (incidence of infant mortality for Low
birth weight – incidence of infant mortality for normal birth weight) = ± (
death cases for low birth weight
total cases for low birth weight − deathcases for normal bith weight
total case for normal birth weight ) = ± (0.00625 – 0.112254) = 0.1185 (Finegold, Asaria and Francis
2013).
3.
If there were no deaths relating the low birth weights then the incidence rate = 0.1185. For the exposure of the disease, the incidence
rate = 0.00625. The attributable fraction for no deaths due to low birth weight = ( 0.1185−0.00625
0.1185 ¿=94.726 %.
The large fraction of attributable fraction indicates that the non-death cases due to non-exposure attributes a significant percentage
when normal birth weights are only taken into account for death cases (Mansournia and Altman 2018).
4.
The overall incidence rate of mortality = Total number of death cases
Total number of casesobserved = 1040
72730 =0.0143
5.
If there is no low birth weights, then the incidence rate = ¿) = 0.00625.
6.
The population attribution risk = Combined incidence rate – incidence rate unexposed = 0.0143 – 0.0062 = 0.00804.
7.
Attributable risk = 0.11225.
11.225% of the observed population are attributed to the risk of death due to low birth weights.
The attributable fraction = Attributable risk
incidence due ¿ exposure ¿= 0.11225
0.1185 =94.726 %.
Population attributable fraction =
attributable fraction
( deaths∈exposure
total cases of exposure )
= 0.94726
( 618
1040 )
=0.56289 (Tikkanen 2011).
56.289% of the total population and 94.726% of the exposed population (low birth weights) attributed the death cases.
Question 3.
A case-control study tests the association between smoking and infection of human papilloma virus of the cervix. From a survey
questionnaire, the data regarding smoking history and number of lifetime sexual partners for cases and controls were collected.
1.
Table 7: The table of testing association or independence between Smoking and HPV status
HPV
status
Positive Negative Total
Smoking Yes 42 90 132
No 146 481 627
Total 188 571 759
Comparison of proportions for independent groups: Chi-square test
Expected cell frequencies
HPV
status
Positive Negative
Smoking Positive 32.70 99.30
Negativ
e 155.30 471.70
Assumptions are Correct
Null hypothesis
H0: p1
=p2
p1= 0.318
p2= 0.233
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6EPIDEMIOLOGY
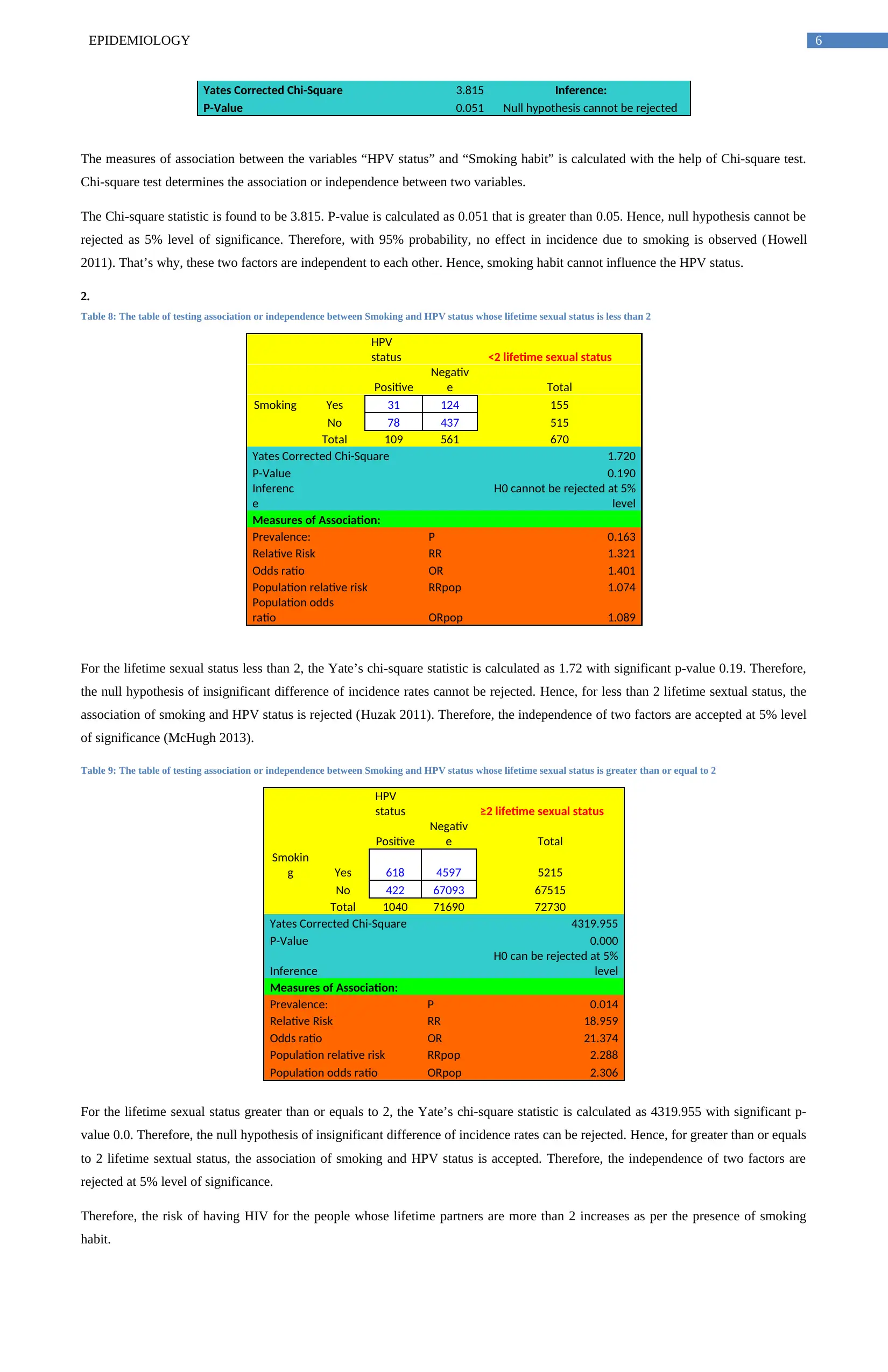
Yates Corrected Chi-Square 3.815 Inference:
P-Value 0.051 Null hypothesis cannot be rejected
The measures of association between the variables “HPV status” and “Smoking habit” is calculated with the help of Chi-square test.
Chi-square test determines the association or independence between two variables.
The Chi-square statistic is found to be 3.815. P-value is calculated as 0.051 that is greater than 0.05. Hence, null hypothesis cannot be
rejected as 5% level of significance. Therefore, with 95% probability, no effect in incidence due to smoking is observed (Howell
2011). That’s why, these two factors are independent to each other. Hence, smoking habit cannot influence the HPV status.
2.
Table 8: The table of testing association or independence between Smoking and HPV status whose lifetime sexual status is less than 2
HPV
status <2 lifetime sexual status
Positive
Negativ
e Total
Smoking Yes 31 124 155
No 78 437 515
Total 109 561 670
Yates Corrected Chi-Square 1.720
P-Value 0.190
Inferenc
e
H0 cannot be rejected at 5%
level
Measures of Association:
Prevalence: P 0.163
Relative Risk RR 1.321
Odds ratio OR 1.401
Population relative risk RRpop 1.074
Population odds
ratio ORpop 1.089
For the lifetime sexual status less than 2, the Yate’s chi-square statistic is calculated as 1.72 with significant p-value 0.19. Therefore,
the null hypothesis of insignificant difference of incidence rates cannot be rejected. Hence, for less than 2 lifetime sextual status, the
association of smoking and HPV status is rejected (Huzak 2011). Therefore, the independence of two factors are accepted at 5% level
of significance (McHugh 2013).
Table 9: The table of testing association or independence between Smoking and HPV status whose lifetime sexual status is greater than or equal to 2
HPV
status ≥2 lifetime sexual status
Positive
Negativ
e Total
Smokin
g Yes 618 4597 5215
No 422 67093 67515
Total 1040 71690 72730
Yates Corrected Chi-Square 4319.955
P-Value 0.000
Inference
H0 can be rejected at 5%
level
Measures of Association:
Prevalence: P 0.014
Relative Risk RR 18.959
Odds ratio OR 21.374
Population relative risk RRpop 2.288
Population odds ratio ORpop 2.306
For the lifetime sexual status greater than or equals to 2, the Yate’s chi-square statistic is calculated as 4319.955 with significant p-
value 0.0. Therefore, the null hypothesis of insignificant difference of incidence rates can be rejected. Hence, for greater than or equals
to 2 lifetime sextual status, the association of smoking and HPV status is accepted. Therefore, the independence of two factors are
rejected at 5% level of significance.
Therefore, the risk of having HIV for the people whose lifetime partners are more than 2 increases as per the presence of smoking
habit.
Yates Corrected Chi-Square 3.815 Inference:
P-Value 0.051 Null hypothesis cannot be rejected
The measures of association between the variables “HPV status” and “Smoking habit” is calculated with the help of Chi-square test.
Chi-square test determines the association or independence between two variables.
The Chi-square statistic is found to be 3.815. P-value is calculated as 0.051 that is greater than 0.05. Hence, null hypothesis cannot be
rejected as 5% level of significance. Therefore, with 95% probability, no effect in incidence due to smoking is observed (Howell
2011). That’s why, these two factors are independent to each other. Hence, smoking habit cannot influence the HPV status.
2.
Table 8: The table of testing association or independence between Smoking and HPV status whose lifetime sexual status is less than 2
HPV
status <2 lifetime sexual status
Positive
Negativ
e Total
Smoking Yes 31 124 155
No 78 437 515
Total 109 561 670
Yates Corrected Chi-Square 1.720
P-Value 0.190
Inferenc
e
H0 cannot be rejected at 5%
level
Measures of Association:
Prevalence: P 0.163
Relative Risk RR 1.321
Odds ratio OR 1.401
Population relative risk RRpop 1.074
Population odds
ratio ORpop 1.089
For the lifetime sexual status less than 2, the Yate’s chi-square statistic is calculated as 1.72 with significant p-value 0.19. Therefore,
the null hypothesis of insignificant difference of incidence rates cannot be rejected. Hence, for less than 2 lifetime sextual status, the
association of smoking and HPV status is rejected (Huzak 2011). Therefore, the independence of two factors are accepted at 5% level
of significance (McHugh 2013).
Table 9: The table of testing association or independence between Smoking and HPV status whose lifetime sexual status is greater than or equal to 2
HPV
status ≥2 lifetime sexual status
Positive
Negativ
e Total
Smokin
g Yes 618 4597 5215
No 422 67093 67515
Total 1040 71690 72730
Yates Corrected Chi-Square 4319.955
P-Value 0.000
Inference
H0 can be rejected at 5%
level
Measures of Association:
Prevalence: P 0.014
Relative Risk RR 18.959
Odds ratio OR 21.374
Population relative risk RRpop 2.288
Population odds ratio ORpop 2.306
For the lifetime sexual status greater than or equals to 2, the Yate’s chi-square statistic is calculated as 4319.955 with significant p-
value 0.0. Therefore, the null hypothesis of insignificant difference of incidence rates can be rejected. Hence, for greater than or equals
to 2 lifetime sextual status, the association of smoking and HPV status is accepted. Therefore, the independence of two factors are
rejected at 5% level of significance.
Therefore, the risk of having HIV for the people whose lifetime partners are more than 2 increases as per the presence of smoking
habit.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7EPIDEMIOLOGY
3.
Confounding happens when a factor is related with both the exposure and effect but does not remain on the causative pathway. Effect
modifier provides important information rather than being a “nuisance” (Nurmatov et al. 2012). The magnitude of the effect of the
exposure on an outcome would vary in accordance to the presence of a third factor.
The number of lifetime sexual partners would provide crucial information being a causative factor. Hence, the factor “The number of
lifetime sextual partners” is an effect modifier.
References:
Chow, W.H., Dong, L.M. and Devesa, S.S., 2010. Epidemiology and risk factors for kidney cancer. Nature Reviews Urology, 7(5),
p.245.
Finegold, J.A., Asaria, P. and Francis, D.P., 2013. Mortality from ischaemic heart disease by country, region, and age: statistics from
World Health Organisation and United Nations. International journal of cardiology, 168(2), pp.934-945.
Howell, D.C., 2011. Chi-square test: analysis of contingency tables. In International encyclopedia of statistical science (pp. 250-252).
Springer Berlin Heidelberg.
Huzak, M., 2011. Chi-Square Distribution. In International Encyclopedia of Statistical Science (pp. 245-246). Springer Berlin
Heidelberg.
Mansournia, M.A. and Altman, D.G., 2018. Population attributable fraction. BMJ, 360, p.k757.
McHugh, M.L., 2013. The chi-square test of independence. Biochemia medica: Biochemia medica, 23(2), pp.143-149.
Nurmatov, U., Nwaru, B.I., Devereux, G. and Sheikh, A., 2012. Confounding and effect modification in studies of diet and childhood
asthma and allergies. Allergy, 67(8), pp.1041-1059.
Roglic, G. and Unwin, N., 2010. Mortality attributable to diabetes: estimates for the year 2010. Diabetes research and clinical
practice, 87(1), pp.15-19.
Siegel, R.L., Miller, K.D. and Jemal, A., 2015. Cancer statistics, 2015. CA: a cancer journal for clinicians, 65(1), pp.5-29.
Smink, F.R., Van Hoeken, D. and Hoek, H.W., 2012. Epidemiology of eating disorders: incidence, prevalence and mortality
rates. Current psychiatry reports, 14(4), pp.406-414.
Tikkanen, M., 2011. Placental abruption: epidemiology, risk factors and consequences. Acta obstetricia et gynecologica
Scandinavica, 90(2), pp.140-149.
3.
Confounding happens when a factor is related with both the exposure and effect but does not remain on the causative pathway. Effect
modifier provides important information rather than being a “nuisance” (Nurmatov et al. 2012). The magnitude of the effect of the
exposure on an outcome would vary in accordance to the presence of a third factor.
The number of lifetime sexual partners would provide crucial information being a causative factor. Hence, the factor “The number of
lifetime sextual partners” is an effect modifier.
References:
Chow, W.H., Dong, L.M. and Devesa, S.S., 2010. Epidemiology and risk factors for kidney cancer. Nature Reviews Urology, 7(5),
p.245.
Finegold, J.A., Asaria, P. and Francis, D.P., 2013. Mortality from ischaemic heart disease by country, region, and age: statistics from
World Health Organisation and United Nations. International journal of cardiology, 168(2), pp.934-945.
Howell, D.C., 2011. Chi-square test: analysis of contingency tables. In International encyclopedia of statistical science (pp. 250-252).
Springer Berlin Heidelberg.
Huzak, M., 2011. Chi-Square Distribution. In International Encyclopedia of Statistical Science (pp. 245-246). Springer Berlin
Heidelberg.
Mansournia, M.A. and Altman, D.G., 2018. Population attributable fraction. BMJ, 360, p.k757.
McHugh, M.L., 2013. The chi-square test of independence. Biochemia medica: Biochemia medica, 23(2), pp.143-149.
Nurmatov, U., Nwaru, B.I., Devereux, G. and Sheikh, A., 2012. Confounding and effect modification in studies of diet and childhood
asthma and allergies. Allergy, 67(8), pp.1041-1059.
Roglic, G. and Unwin, N., 2010. Mortality attributable to diabetes: estimates for the year 2010. Diabetes research and clinical
practice, 87(1), pp.15-19.
Siegel, R.L., Miller, K.D. and Jemal, A., 2015. Cancer statistics, 2015. CA: a cancer journal for clinicians, 65(1), pp.5-29.
Smink, F.R., Van Hoeken, D. and Hoek, H.W., 2012. Epidemiology of eating disorders: incidence, prevalence and mortality
rates. Current psychiatry reports, 14(4), pp.406-414.
Tikkanen, M., 2011. Placental abruption: epidemiology, risk factors and consequences. Acta obstetricia et gynecologica
Scandinavica, 90(2), pp.140-149.
1 out of 8
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.