Epidemiology Assignment: Principles, Practices, and Analysis
VerifiedAdded on 2023/01/16
|8
|1707
|61
Homework Assignment
AI Summary
This document presents a comprehensive solution to an epidemiology assignment, covering various aspects of public health and statistical analysis. The assignment includes calculations and interpretations of crude, age-specific, and standardized incidence rates for prostate cancer in two cities, comparing their population structures and disease prevalence. It also explores prevalence and incidence rates of cervical cancer, analyzing data from screening programs and calculating person-year incidence. Furthermore, the assignment delves into a quantitative study on the relationship between alcohol consumption and coronary heart disease, determining the risk among heavy drinkers and calculating the percentage of preventable cases. Finally, it provides a comparative analysis of health statistics for Australia, India, and Nigeria, examining mortality rates, life expectancy, and healthy life expectancy to assess the overall public health levels of each country. The solution demonstrates an understanding of epidemiological principles and their practical application in analyzing health data and drawing meaningful conclusions.

Running head: EPIDEMIOLOGY PRACTICES AND PRINCIPLES
EPIDEMIOLOGY PRACTICES AND PRINCIPLES
Name of the Student
Name of the University
Author’s Note:
EPIDEMIOLOGY PRACTICES AND PRINCIPLES
Name of the Student
Name of the University
Author’s Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1EPIDEMIOLOGY PRACTICES AND PRINCIPLES
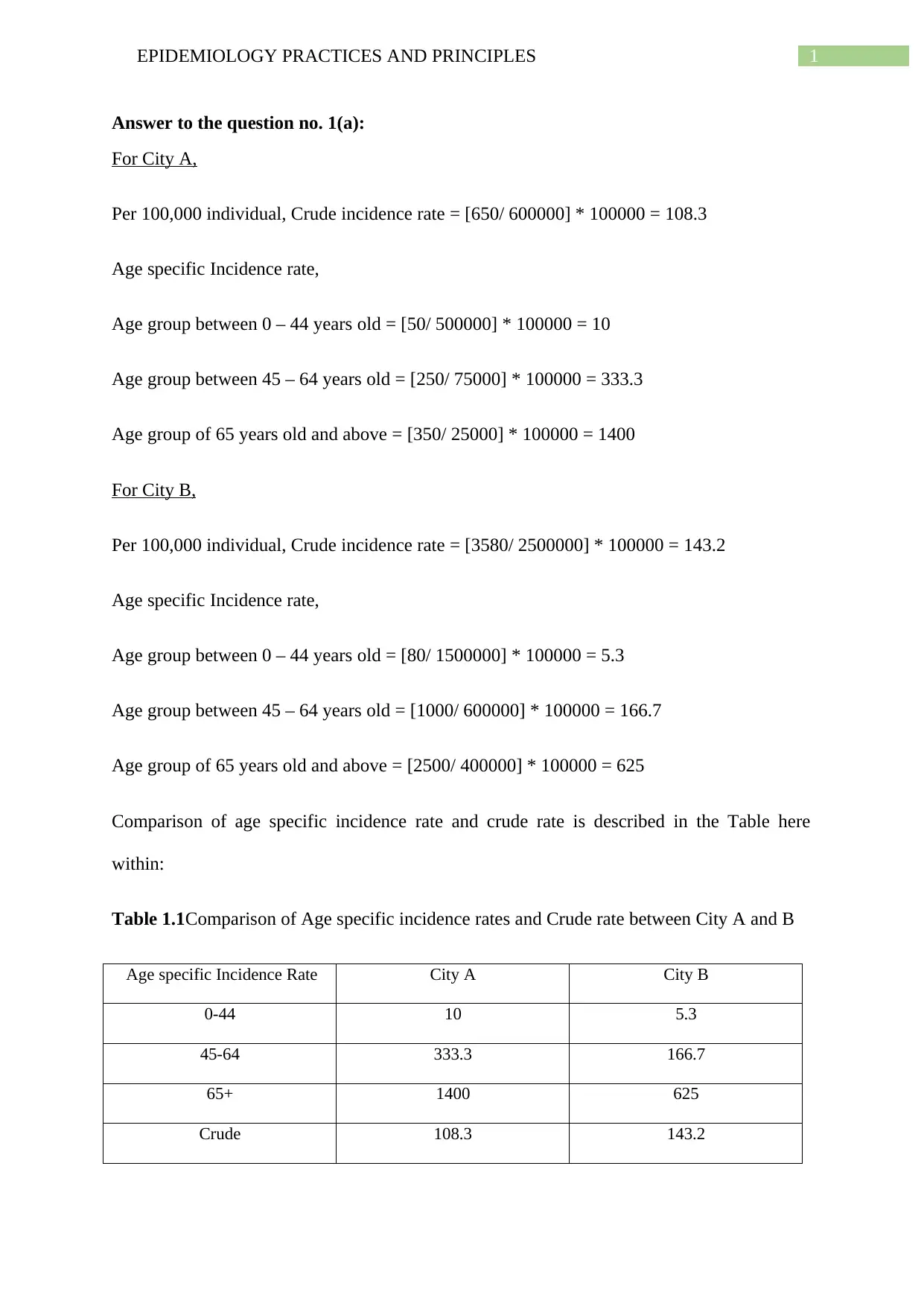
Answer to the question no. 1(a):
For City A,
Per 100,000 individual, Crude incidence rate = [650/ 600000] * 100000 = 108.3
Age specific Incidence rate,
Age group between 0 – 44 years old = [50/ 500000] * 100000 = 10
Age group between 45 – 64 years old = [250/ 75000] * 100000 = 333.3
Age group of 65 years old and above = [350/ 25000] * 100000 = 1400
For City B,
Per 100,000 individual, Crude incidence rate = [3580/ 2500000] * 100000 = 143.2
Age specific Incidence rate,
Age group between 0 – 44 years old = [80/ 1500000] * 100000 = 5.3
Age group between 45 – 64 years old = [1000/ 600000] * 100000 = 166.7
Age group of 65 years old and above = [2500/ 400000] * 100000 = 625
Comparison of age specific incidence rate and crude rate is described in the Table here
within:
Table 1.1Comparison of Age specific incidence rates and Crude rate between City A and B
Age specific Incidence Rate City A City B
0-44 10 5.3
45-64 333.3 166.7
65+ 1400 625
Crude 108.3 143.2
Answer to the question no. 1(a):
For City A,
Per 100,000 individual, Crude incidence rate = [650/ 600000] * 100000 = 108.3
Age specific Incidence rate,
Age group between 0 – 44 years old = [50/ 500000] * 100000 = 10
Age group between 45 – 64 years old = [250/ 75000] * 100000 = 333.3
Age group of 65 years old and above = [350/ 25000] * 100000 = 1400
For City B,
Per 100,000 individual, Crude incidence rate = [3580/ 2500000] * 100000 = 143.2
Age specific Incidence rate,
Age group between 0 – 44 years old = [80/ 1500000] * 100000 = 5.3
Age group between 45 – 64 years old = [1000/ 600000] * 100000 = 166.7
Age group of 65 years old and above = [2500/ 400000] * 100000 = 625
Comparison of age specific incidence rate and crude rate is described in the Table here
within:
Table 1.1Comparison of Age specific incidence rates and Crude rate between City A and B
Age specific Incidence Rate City A City B
0-44 10 5.3
45-64 333.3 166.7
65+ 1400 625
Crude 108.3 143.2
2EPIDEMIOLOGY PRACTICES AND PRINCIPLES
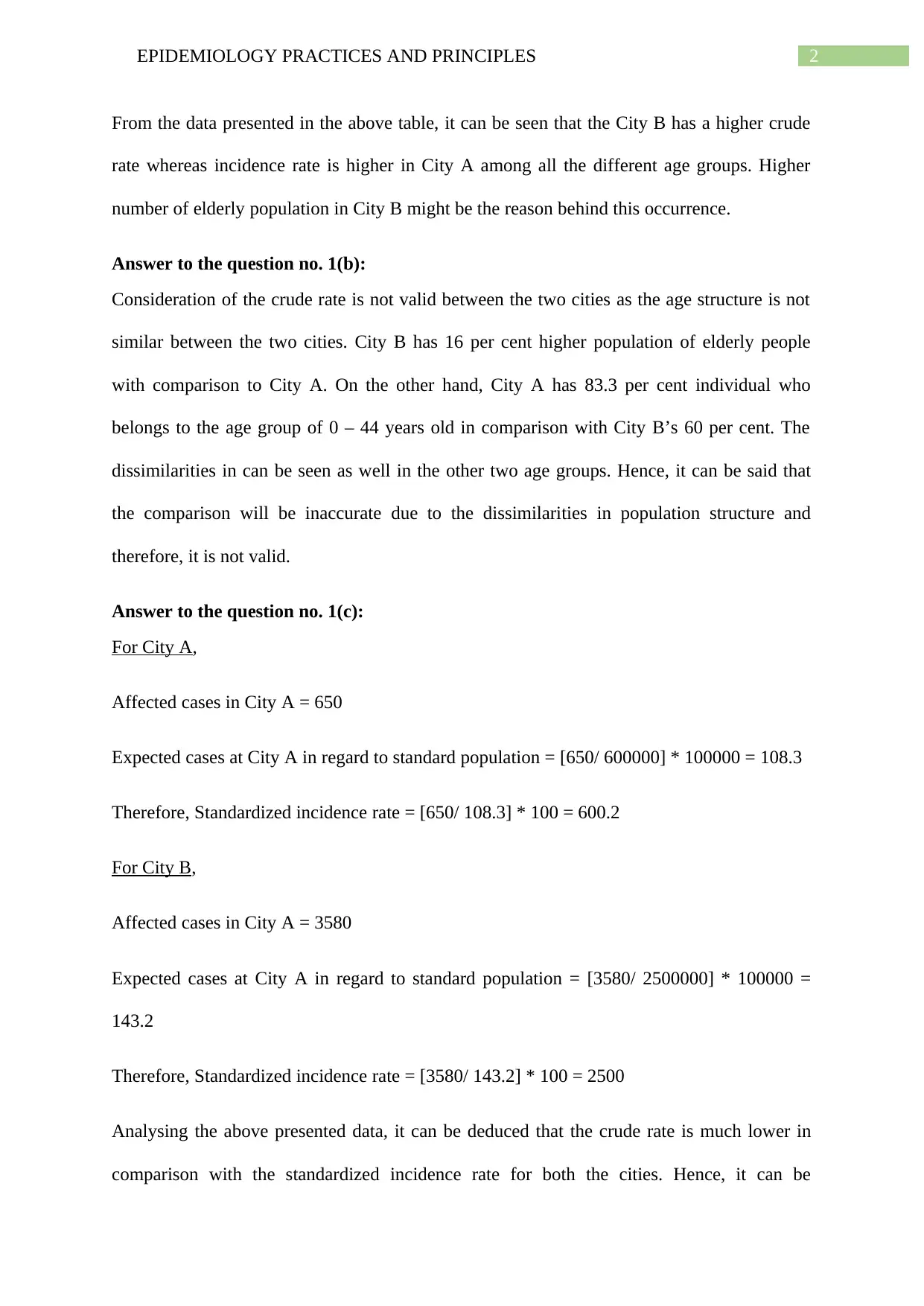
From the data presented in the above table, it can be seen that the City B has a higher crude
rate whereas incidence rate is higher in City A among all the different age groups. Higher
number of elderly population in City B might be the reason behind this occurrence.
Answer to the question no. 1(b):
Consideration of the crude rate is not valid between the two cities as the age structure is not
similar between the two cities. City B has 16 per cent higher population of elderly people
with comparison to City A. On the other hand, City A has 83.3 per cent individual who
belongs to the age group of 0 – 44 years old in comparison with City B’s 60 per cent. The
dissimilarities in can be seen as well in the other two age groups. Hence, it can be said that
the comparison will be inaccurate due to the dissimilarities in population structure and
therefore, it is not valid.
Answer to the question no. 1(c):
For City A,
Affected cases in City A = 650
Expected cases at City A in regard to standard population = [650/ 600000] * 100000 = 108.3
Therefore, Standardized incidence rate = [650/ 108.3] * 100 = 600.2
For City B,
Affected cases in City A = 3580
Expected cases at City A in regard to standard population = [3580/ 2500000] * 100000 =
143.2
Therefore, Standardized incidence rate = [3580/ 143.2] * 100 = 2500
Analysing the above presented data, it can be deduced that the crude rate is much lower in
comparison with the standardized incidence rate for both the cities. Hence, it can be
From the data presented in the above table, it can be seen that the City B has a higher crude
rate whereas incidence rate is higher in City A among all the different age groups. Higher
number of elderly population in City B might be the reason behind this occurrence.
Answer to the question no. 1(b):
Consideration of the crude rate is not valid between the two cities as the age structure is not
similar between the two cities. City B has 16 per cent higher population of elderly people
with comparison to City A. On the other hand, City A has 83.3 per cent individual who
belongs to the age group of 0 – 44 years old in comparison with City B’s 60 per cent. The
dissimilarities in can be seen as well in the other two age groups. Hence, it can be said that
the comparison will be inaccurate due to the dissimilarities in population structure and
therefore, it is not valid.
Answer to the question no. 1(c):
For City A,
Affected cases in City A = 650
Expected cases at City A in regard to standard population = [650/ 600000] * 100000 = 108.3
Therefore, Standardized incidence rate = [650/ 108.3] * 100 = 600.2
For City B,
Affected cases in City A = 3580
Expected cases at City A in regard to standard population = [3580/ 2500000] * 100000 =
143.2
Therefore, Standardized incidence rate = [3580/ 143.2] * 100 = 2500
Analysing the above presented data, it can be deduced that the crude rate is much lower in
comparison with the standardized incidence rate for both the cities. Hence, it can be
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3EPIDEMIOLOGY PRACTICES AND PRINCIPLES
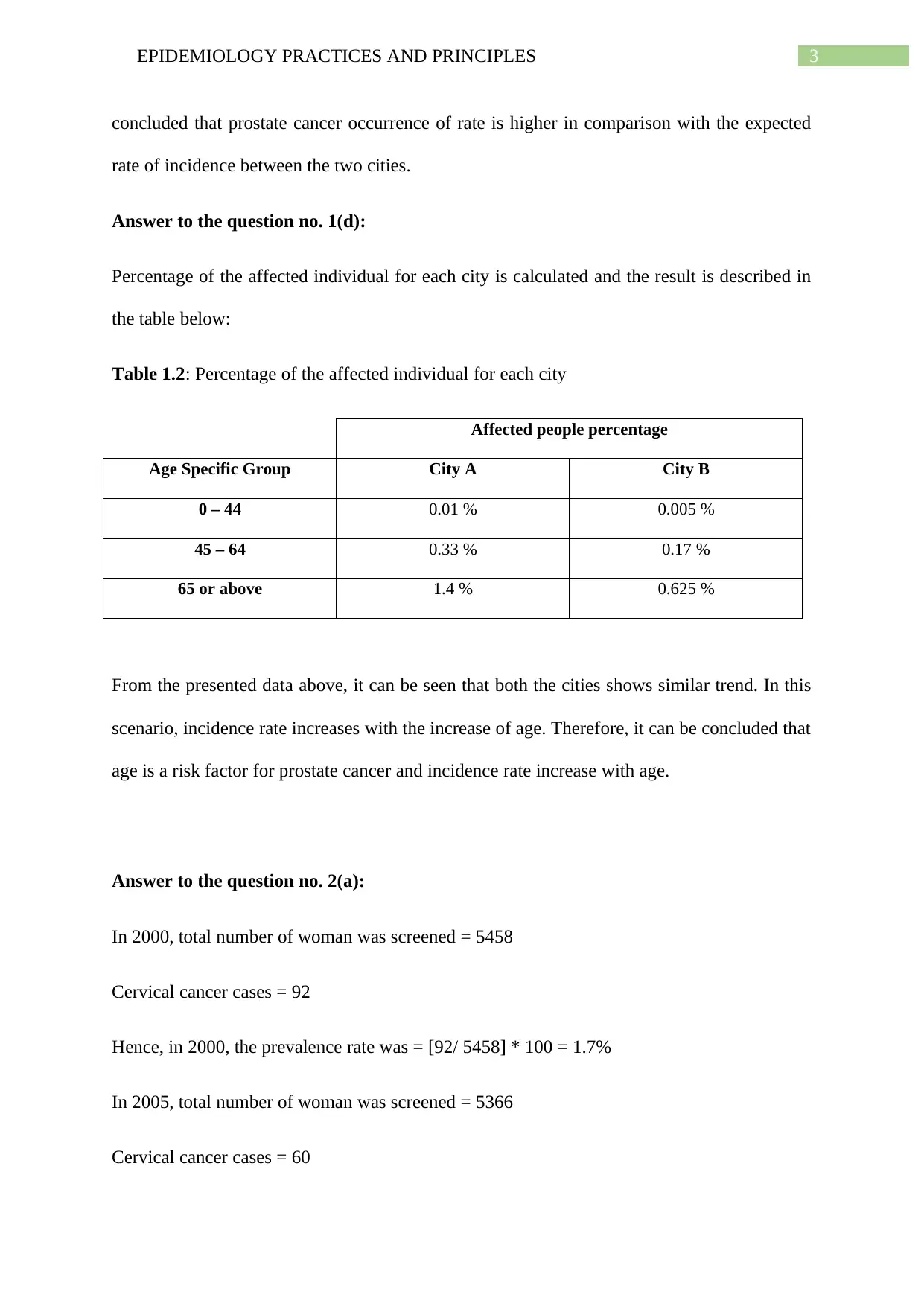
concluded that prostate cancer occurrence of rate is higher in comparison with the expected
rate of incidence between the two cities.
Answer to the question no. 1(d):
Percentage of the affected individual for each city is calculated and the result is described in
the table below:
Table 1.2: Percentage of the affected individual for each city
Affected people percentage
Age Specific Group City A City B
0 – 44 0.01 % 0.005 %
45 – 64 0.33 % 0.17 %
65 or above 1.4 % 0.625 %
From the presented data above, it can be seen that both the cities shows similar trend. In this
scenario, incidence rate increases with the increase of age. Therefore, it can be concluded that
age is a risk factor for prostate cancer and incidence rate increase with age.
Answer to the question no. 2(a):
In 2000, total number of woman was screened = 5458
Cervical cancer cases = 92
Hence, in 2000, the prevalence rate was = [92/ 5458] * 100 = 1.7%
In 2005, total number of woman was screened = 5366
Cervical cancer cases = 60
concluded that prostate cancer occurrence of rate is higher in comparison with the expected
rate of incidence between the two cities.
Answer to the question no. 1(d):
Percentage of the affected individual for each city is calculated and the result is described in
the table below:
Table 1.2: Percentage of the affected individual for each city
Affected people percentage
Age Specific Group City A City B
0 – 44 0.01 % 0.005 %
45 – 64 0.33 % 0.17 %
65 or above 1.4 % 0.625 %
From the presented data above, it can be seen that both the cities shows similar trend. In this
scenario, incidence rate increases with the increase of age. Therefore, it can be concluded that
age is a risk factor for prostate cancer and incidence rate increase with age.
Answer to the question no. 2(a):
In 2000, total number of woman was screened = 5458
Cervical cancer cases = 92
Hence, in 2000, the prevalence rate was = [92/ 5458] * 100 = 1.7%
In 2005, total number of woman was screened = 5366
Cervical cancer cases = 60
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4EPIDEMIOLOGY PRACTICES AND PRINCIPLES
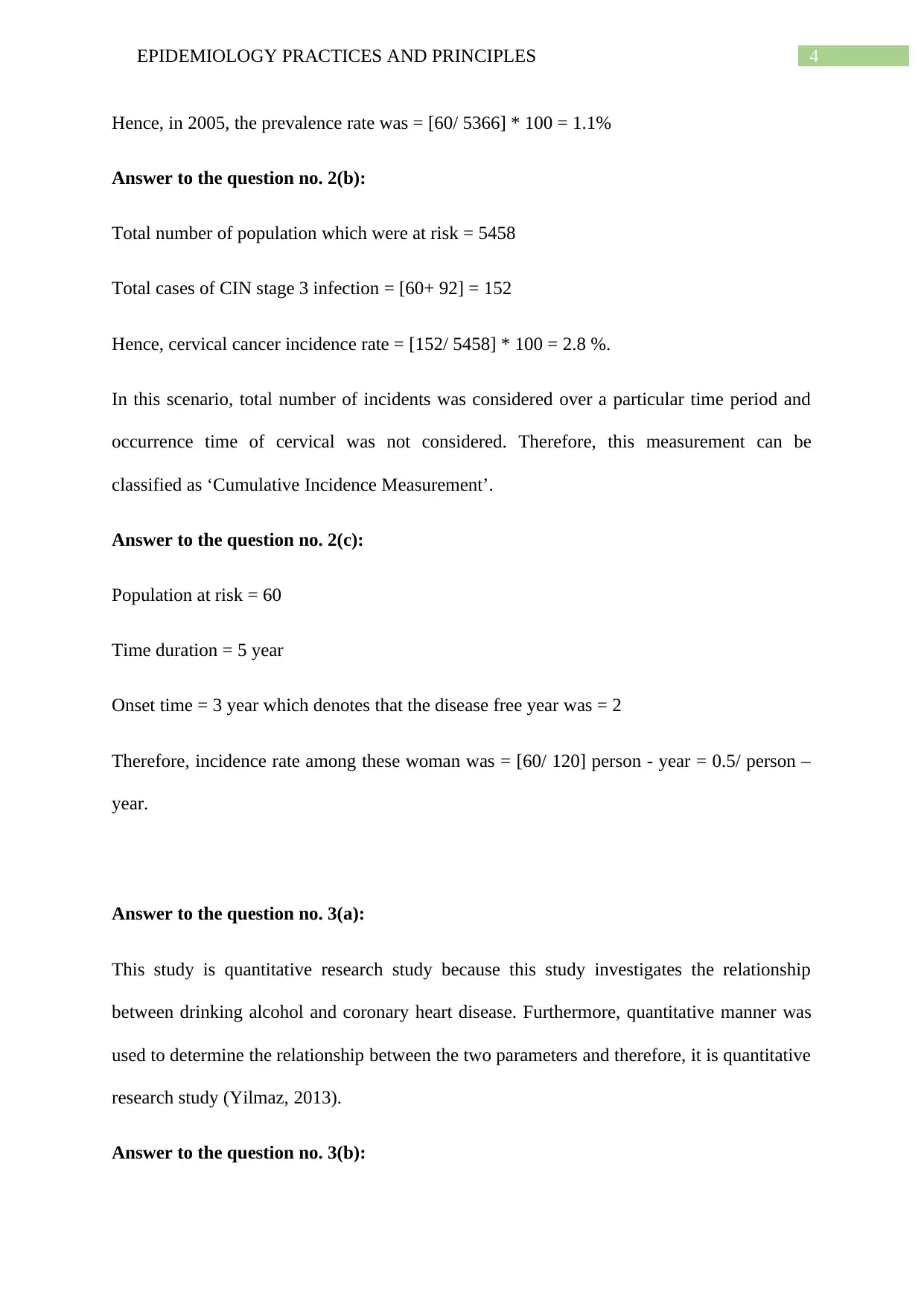
Hence, in 2005, the prevalence rate was = [60/ 5366] * 100 = 1.1%
Answer to the question no. 2(b):
Total number of population which were at risk = 5458
Total cases of CIN stage 3 infection = [60+ 92] = 152
Hence, cervical cancer incidence rate = [152/ 5458] * 100 = 2.8 %.
In this scenario, total number of incidents was considered over a particular time period and
occurrence time of cervical was not considered. Therefore, this measurement can be
classified as ‘Cumulative Incidence Measurement’.
Answer to the question no. 2(c):
Population at risk = 60
Time duration = 5 year
Onset time = 3 year which denotes that the disease free year was = 2
Therefore, incidence rate among these woman was = [60/ 120] person - year = 0.5/ person –
year.
Answer to the question no. 3(a):
This study is quantitative research study because this study investigates the relationship
between drinking alcohol and coronary heart disease. Furthermore, quantitative manner was
used to determine the relationship between the two parameters and therefore, it is quantitative
research study (Yilmaz, 2013).
Answer to the question no. 3(b):
Hence, in 2005, the prevalence rate was = [60/ 5366] * 100 = 1.1%
Answer to the question no. 2(b):
Total number of population which were at risk = 5458
Total cases of CIN stage 3 infection = [60+ 92] = 152
Hence, cervical cancer incidence rate = [152/ 5458] * 100 = 2.8 %.
In this scenario, total number of incidents was considered over a particular time period and
occurrence time of cervical was not considered. Therefore, this measurement can be
classified as ‘Cumulative Incidence Measurement’.
Answer to the question no. 2(c):
Population at risk = 60
Time duration = 5 year
Onset time = 3 year which denotes that the disease free year was = 2
Therefore, incidence rate among these woman was = [60/ 120] person - year = 0.5/ person –
year.
Answer to the question no. 3(a):
This study is quantitative research study because this study investigates the relationship
between drinking alcohol and coronary heart disease. Furthermore, quantitative manner was
used to determine the relationship between the two parameters and therefore, it is quantitative
research study (Yilmaz, 2013).
Answer to the question no. 3(b):
5EPIDEMIOLOGY PRACTICES AND PRINCIPLES
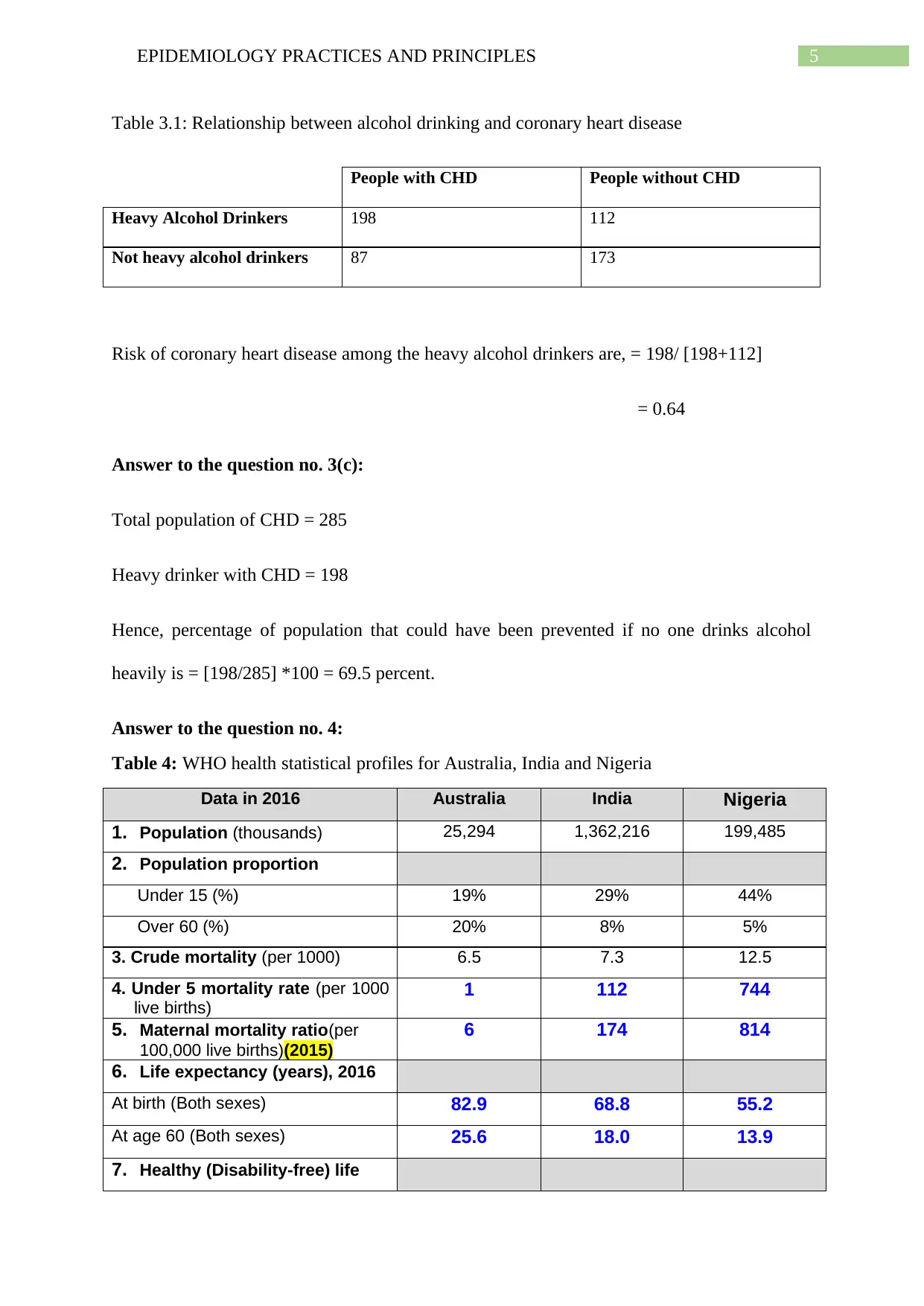
Table 3.1: Relationship between alcohol drinking and coronary heart disease
People with CHD People without CHD
Heavy Alcohol Drinkers 198 112
Not heavy alcohol drinkers 87 173
Risk of coronary heart disease among the heavy alcohol drinkers are, = 198/ [198+112]
= 0.64
Answer to the question no. 3(c):
Total population of CHD = 285
Heavy drinker with CHD = 198
Hence, percentage of population that could have been prevented if no one drinks alcohol
heavily is = [198/285] *100 = 69.5 percent.
Answer to the question no. 4:
Table 4: WHO health statistical profiles for Australia, India and Nigeria
Data in 2016 Australia India Nigeria
1. Population (thousands) 25,294 1,362,216 199,485
2. Population proportion
Under 15 (%) 19% 29% 44%
Over 60 (%) 20% 8% 5%
3. Crude mortality (per 1000) 6.5 7.3 12.5
4. Under 5 mortality rate (per 1000
live births)
1 112 744
5. Maternal mortality ratio(per
100,000 live births)(2015)
6 174 814
6. Life expectancy (years), 2016
At birth (Both sexes) 82.9 68.8 55.2
At age 60 (Both sexes) 25.6 18.0 13.9
7. Healthy (Disability-free) life
Table 3.1: Relationship between alcohol drinking and coronary heart disease
People with CHD People without CHD
Heavy Alcohol Drinkers 198 112
Not heavy alcohol drinkers 87 173
Risk of coronary heart disease among the heavy alcohol drinkers are, = 198/ [198+112]
= 0.64
Answer to the question no. 3(c):
Total population of CHD = 285
Heavy drinker with CHD = 198
Hence, percentage of population that could have been prevented if no one drinks alcohol
heavily is = [198/285] *100 = 69.5 percent.
Answer to the question no. 4:
Table 4: WHO health statistical profiles for Australia, India and Nigeria
Data in 2016 Australia India Nigeria
1. Population (thousands) 25,294 1,362,216 199,485
2. Population proportion
Under 15 (%) 19% 29% 44%
Over 60 (%) 20% 8% 5%
3. Crude mortality (per 1000) 6.5 7.3 12.5
4. Under 5 mortality rate (per 1000
live births)
1 112 744
5. Maternal mortality ratio(per
100,000 live births)(2015)
6 174 814
6. Life expectancy (years), 2016
At birth (Both sexes) 82.9 68.8 55.2
At age 60 (Both sexes) 25.6 18.0 13.9
7. Healthy (Disability-free) life
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
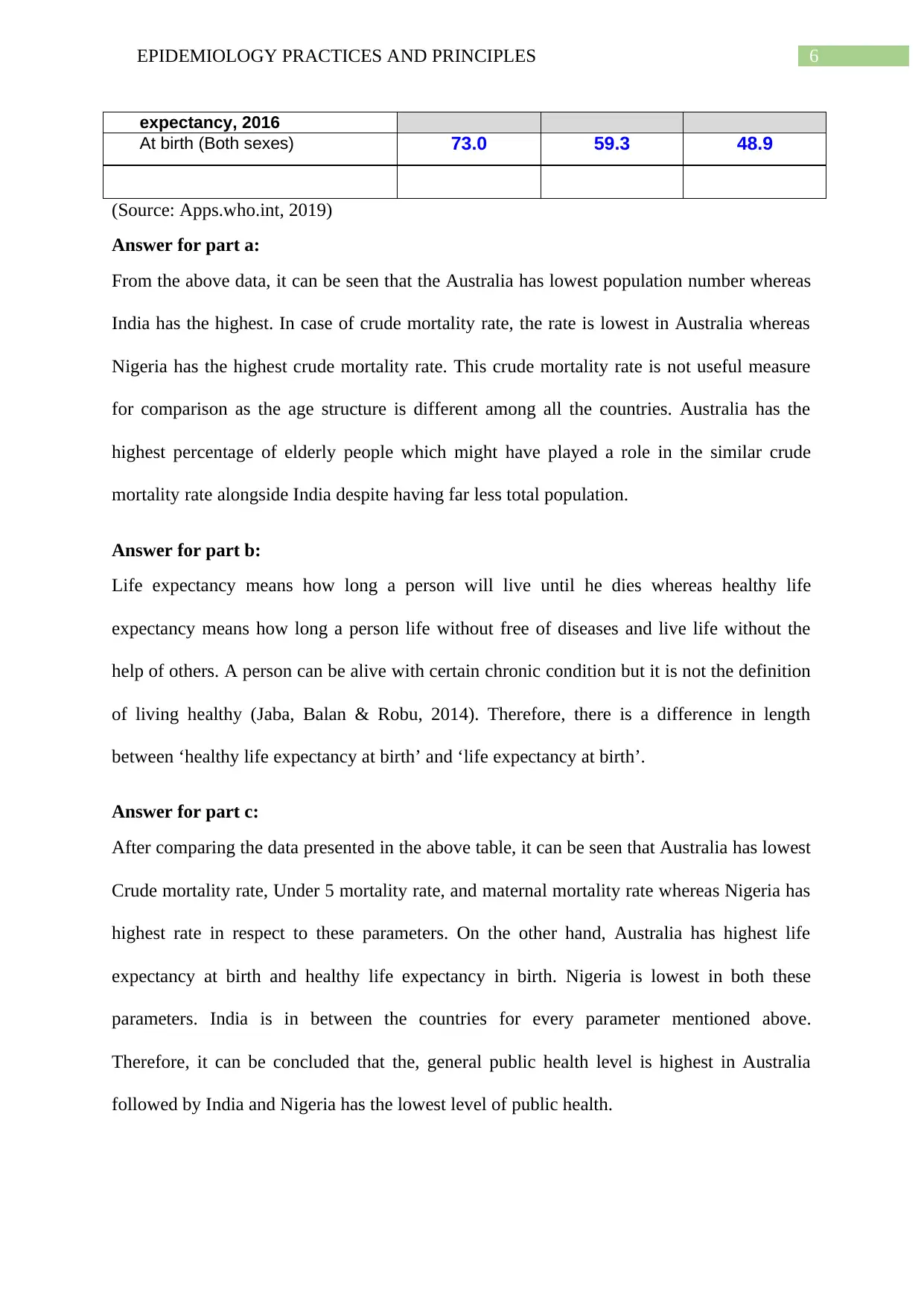
6EPIDEMIOLOGY PRACTICES AND PRINCIPLES
expectancy, 2016
At birth (Both sexes) 73.0 59.3 48.9
(Source: Apps.who.int, 2019)
Answer for part a:
From the above data, it can be seen that the Australia has lowest population number whereas
India has the highest. In case of crude mortality rate, the rate is lowest in Australia whereas
Nigeria has the highest crude mortality rate. This crude mortality rate is not useful measure
for comparison as the age structure is different among all the countries. Australia has the
highest percentage of elderly people which might have played a role in the similar crude
mortality rate alongside India despite having far less total population.
Answer for part b:
Life expectancy means how long a person will live until he dies whereas healthy life
expectancy means how long a person life without free of diseases and live life without the
help of others. A person can be alive with certain chronic condition but it is not the definition
of living healthy (Jaba, Balan & Robu, 2014). Therefore, there is a difference in length
between ‘healthy life expectancy at birth’ and ‘life expectancy at birth’.
Answer for part c:
After comparing the data presented in the above table, it can be seen that Australia has lowest
Crude mortality rate, Under 5 mortality rate, and maternal mortality rate whereas Nigeria has
highest rate in respect to these parameters. On the other hand, Australia has highest life
expectancy at birth and healthy life expectancy in birth. Nigeria is lowest in both these
parameters. India is in between the countries for every parameter mentioned above.
Therefore, it can be concluded that the, general public health level is highest in Australia
followed by India and Nigeria has the lowest level of public health.
expectancy, 2016
At birth (Both sexes) 73.0 59.3 48.9
(Source: Apps.who.int, 2019)
Answer for part a:
From the above data, it can be seen that the Australia has lowest population number whereas
India has the highest. In case of crude mortality rate, the rate is lowest in Australia whereas
Nigeria has the highest crude mortality rate. This crude mortality rate is not useful measure
for comparison as the age structure is different among all the countries. Australia has the
highest percentage of elderly people which might have played a role in the similar crude
mortality rate alongside India despite having far less total population.
Answer for part b:
Life expectancy means how long a person will live until he dies whereas healthy life
expectancy means how long a person life without free of diseases and live life without the
help of others. A person can be alive with certain chronic condition but it is not the definition
of living healthy (Jaba, Balan & Robu, 2014). Therefore, there is a difference in length
between ‘healthy life expectancy at birth’ and ‘life expectancy at birth’.
Answer for part c:
After comparing the data presented in the above table, it can be seen that Australia has lowest
Crude mortality rate, Under 5 mortality rate, and maternal mortality rate whereas Nigeria has
highest rate in respect to these parameters. On the other hand, Australia has highest life
expectancy at birth and healthy life expectancy in birth. Nigeria is lowest in both these
parameters. India is in between the countries for every parameter mentioned above.
Therefore, it can be concluded that the, general public health level is highest in Australia
followed by India and Nigeria has the lowest level of public health.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7EPIDEMIOLOGY PRACTICES AND PRINCIPLES
References:
Apps.who.int. (2019). GHO | By category | Mortality and global health estimates. Retrieved
from http://apps.who.int/gho/data/node.main.686?lang=en
Jaba, E., Balan, C. B., & Robu, I. B. (2014). The relationship between life expectancy at birth
and health expenditures estimated by a cross-country and time-series
analysis. Procedia Economics and Finance, 15, 108-114.
Yilmaz, K. (2013). Comparison of quantitative and qualitative research traditions:
Epistemological, theoretical, and methodological differences. European Journal of
Education, 48(2), 311-325.
References:
Apps.who.int. (2019). GHO | By category | Mortality and global health estimates. Retrieved
from http://apps.who.int/gho/data/node.main.686?lang=en
Jaba, E., Balan, C. B., & Robu, I. B. (2014). The relationship between life expectancy at birth
and health expenditures estimated by a cross-country and time-series
analysis. Procedia Economics and Finance, 15, 108-114.
Yilmaz, K. (2013). Comparison of quantitative and qualitative research traditions:
Epistemological, theoretical, and methodological differences. European Journal of
Education, 48(2), 311-325.
1 out of 8