Diabetic Foot Ulcers: An Evidence-Based Care and Nursing Approach
VerifiedAdded on 2023/04/07
|9
|2226
|342
Case Study
AI Summary
This case study examines the evidence-based care provided to an 80-year-old patient with a history of type 2 diabetes and bilateral diabetic foot ulcers. The report details the patient's assessment, including general signs of toxicity, fungal infections, skin fissures, and temperature variations, as well as a review of medical history and comorbidities such as hypertension, hyperlipidemia, and peripheral vascular disease. Wound assessment focuses on skin condition, vascular and neurological systems, and potential neuropathic deficits. Key nursing interventions discussed include multidisciplinary collaboration, wound debridement, infection control, revascularization, and ulcer offloading. The study emphasizes the importance of a multidisciplinary approach, nutritional care, and adherence to gold standard treatments to prevent amputation and improve patient outcomes. The report includes pictorial information on diabetic foot ulcers and references to relevant research.

Evidence-Based Care on Diabetic Foot Ulcers
University
Name
Tutor
Date
University
Name
Tutor
Date
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
Diabetic Foot Ulcer
Introduction
A diabetic foot ulcer is a serious disease characterized by ulceration associated with
neuropathy and peripheral artery disease of the lower limb among patients with diabetes. The
prevalence of diabetic foot ranges between 4%-10% among diabetic patients, with adverse
effects being observed among the elderly. About 5% of the diabetic patients with a history of
diabetic foot with ulceration while the overall life risks of complication development are
about 15%. Studies have estimated that 60%-80% of foot ulcers heal while 10-15% remains
activated and 5%-24% most likely progresses for limb amputation within 6-18 months after
initial evaluation (Lauterbach, Kostev & Kohlmann, 2010).
The occurrence of neuropathic wounds are highly likely to heal after 20 weeks, while
ulcers related to neuro ischemic often take the long and more likely lead to amputation
(Moxey et al., 2011)
Diabetic foot ulcers are currently responsible for more hospitalizations compared to
other diabetic complications. The risks associated with the ulceration of the foot ulceration
and amputation of limb increases with age. Ulcers foot prevention is evident, in view of
consideration of the harmful impact on the patient’s life quality and underlying economic
consequences on the health care system. It is a public health concern and its nursing often
involve a multidisciplinary team (Prompers et al., 2008).
Case study
This report is based on a case study involving 80 years old patient, with history of
diabetes type 2 NIDDM under regular drug management. The patient was admitted with
bilateral diabetic foot, with foul smell meaning from the right foot and previous history of
auto amputation of the 3rd toes as a result of gangrene. Examination reveals that the patient is
restless with pulse rate of 100/minute, temperature 37 degrees Celsius, BP of 130/85. Local
examination indicates gangrene of heel and auto amputation of the 3rd toes. The patient blood
sugar level ranges between fasting of 150mg% to 170mg%. The patient has prio amputation
history of amputation on the lower knee side. Further, stump reshaping was performed after
development of flap necrosis.
Diabetic Foot Ulcer
Introduction
A diabetic foot ulcer is a serious disease characterized by ulceration associated with
neuropathy and peripheral artery disease of the lower limb among patients with diabetes. The
prevalence of diabetic foot ranges between 4%-10% among diabetic patients, with adverse
effects being observed among the elderly. About 5% of the diabetic patients with a history of
diabetic foot with ulceration while the overall life risks of complication development are
about 15%. Studies have estimated that 60%-80% of foot ulcers heal while 10-15% remains
activated and 5%-24% most likely progresses for limb amputation within 6-18 months after
initial evaluation (Lauterbach, Kostev & Kohlmann, 2010).
The occurrence of neuropathic wounds are highly likely to heal after 20 weeks, while
ulcers related to neuro ischemic often take the long and more likely lead to amputation
(Moxey et al., 2011)
Diabetic foot ulcers are currently responsible for more hospitalizations compared to
other diabetic complications. The risks associated with the ulceration of the foot ulceration
and amputation of limb increases with age. Ulcers foot prevention is evident, in view of
consideration of the harmful impact on the patient’s life quality and underlying economic
consequences on the health care system. It is a public health concern and its nursing often
involve a multidisciplinary team (Prompers et al., 2008).
Case study
This report is based on a case study involving 80 years old patient, with history of
diabetes type 2 NIDDM under regular drug management. The patient was admitted with
bilateral diabetic foot, with foul smell meaning from the right foot and previous history of
auto amputation of the 3rd toes as a result of gangrene. Examination reveals that the patient is
restless with pulse rate of 100/minute, temperature 37 degrees Celsius, BP of 130/85. Local
examination indicates gangrene of heel and auto amputation of the 3rd toes. The patient blood
sugar level ranges between fasting of 150mg% to 170mg%. The patient has prio amputation
history of amputation on the lower knee side. Further, stump reshaping was performed after
development of flap necrosis.
3
Patient assessment
Patient assessment of the general signs of toxicity is necessary. Occurrences of
symptoms of sepsis are essential for active disease. Observation focuses on the fungal
infection, skin fissures, and deformity on the nails. Feeling of the temperature on the foot is
key in assessing patient temperature change. Cold temperature status reflects ischemia while
increased warmth-ness reflects redness and swelling suggesting the presence of acute
cellulitis presence (Miller et al., 2014).
Coupled with foot associated assessment on the patients, medical history data is often
considered. The condition of comorbid physiologic conditions and the contributing factors
are assessed. Some of the patient’s assessment includes diabetes mellitus, metabolic
disorders, deformity history, nutritional stage, renal disease, and autoimmune disorders.
Further, this patient has prior non-traumatic amputations thus is at a greater risk of
continuous amputation. Thus getting the patient history of surgical correction, previous
amputations, the presence of vascular surgery are often taken into considerations.
Patient history assessment is thus crucial in assessing the medical comorbidities,
previous history of complications and blood glucose levels. Obtaining glucose levels on the
patient is crucial in proving the primary clinical assessment of the general glycemia control of
the patient (Giovinco & Miler, 2015). Comorbidities needed urgent attention for the patient
includes hypertension, hyperlipidemia, peripheral vascular disease, visual impairment and
diabetic neuropathy (Miller et al., 2014).
Further subjective symptoms of the patients need to be addressed which indicate the
risks factors of any presence of peripheral neuropathy. These symptoms are further included
in the subjective assessments such as tingling, shooting pain, burning, and numbness which
causes concerns for peripheral neuropathy or intermittent symptoms.
Wound assessment
Physical assessment of diabetic foot ulcers on the skin type of musculoskeletal,
vascular, neurological systems and. Examination perfume don the dermatology often includes
inspection visually on skins of the feet and legs especially the lower sides (Tseng et al.,
2011). Notable observations entail skin peeling and skin maceration. The physical assessment
Patient assessment
Patient assessment of the general signs of toxicity is necessary. Occurrences of
symptoms of sepsis are essential for active disease. Observation focuses on the fungal
infection, skin fissures, and deformity on the nails. Feeling of the temperature on the foot is
key in assessing patient temperature change. Cold temperature status reflects ischemia while
increased warmth-ness reflects redness and swelling suggesting the presence of acute
cellulitis presence (Miller et al., 2014).
Coupled with foot associated assessment on the patients, medical history data is often
considered. The condition of comorbid physiologic conditions and the contributing factors
are assessed. Some of the patient’s assessment includes diabetes mellitus, metabolic
disorders, deformity history, nutritional stage, renal disease, and autoimmune disorders.
Further, this patient has prior non-traumatic amputations thus is at a greater risk of
continuous amputation. Thus getting the patient history of surgical correction, previous
amputations, the presence of vascular surgery are often taken into considerations.
Patient history assessment is thus crucial in assessing the medical comorbidities,
previous history of complications and blood glucose levels. Obtaining glucose levels on the
patient is crucial in proving the primary clinical assessment of the general glycemia control of
the patient (Giovinco & Miler, 2015). Comorbidities needed urgent attention for the patient
includes hypertension, hyperlipidemia, peripheral vascular disease, visual impairment and
diabetic neuropathy (Miller et al., 2014).
Further subjective symptoms of the patients need to be addressed which indicate the
risks factors of any presence of peripheral neuropathy. These symptoms are further included
in the subjective assessments such as tingling, shooting pain, burning, and numbness which
causes concerns for peripheral neuropathy or intermittent symptoms.
Wound assessment
Physical assessment of diabetic foot ulcers on the skin type of musculoskeletal,
vascular, neurological systems and. Examination perfume don the dermatology often includes
inspection visually on skins of the feet and legs especially the lower sides (Tseng et al.,
2011). Notable observations entail skin peeling and skin maceration. The physical assessment
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
show signs of autonomic neuropathy and dysfunction of the sudomotor (Schaper et al., 2012).
Diabetic patients are often at high risks of developing the disease of the peripheral
vascular area, thus assessment of the peripheral is necessary to assess blood circulation. Lack
of adequate limb perfusion related to vascular disease often affects the healing process, which
leads to unhealed chronic ulcers which are susceptible to infection (Lipsky et al., 2012). A
simple method of confirming arterial occlusion of the disease is assessing systolic blood
pressure on the arms and the ankles. This often carried out by assessing systolic pressure (Bus
et al., 2016).
Further, assessment of skin temperature on the hand back is intitated. Normal levels of
skin temperature often range between warm at the tibia to cool levels at the distal toes. The
temperature of the foot skin is measured with an infrared thermometer on the lower foot.
Increased temperature levels indicate to malfunction of the sudomotor and high risks of foot
ulceration (Shirazi, Nasiri & Yazdanpanah, 2016).
Physical assessment of the foot often assesses the perception of a pinprick, sensation of
the temperature, light sensation and pressure. Further neuropathic deficits can be assessed
using Neuropathy disability score with studies showing high predictive value (Neville,
Kayssi, Buecher & Stempel, 2016).
Nursing interventions
Potential evidence-based interventions for key nursing decisions for diabetic ulcers foot
entail a combination of clinical expertise and preferences of the patient and associated values
of care. key approaches for care as identified by Schaper et al., (2012) illustrated
identification of the at-risk foot, regular inspection, and examination, patient education,
routine footwear wearing and offering treatment management of pre-ulcerative observations.
Enhancing collaboration of multidisciplinary and holistic approach entails usage of well
organized multidisciplinary team which offering a coordinated nursing intervention approach.
Potential wound care actions
Case study management of diabetic foot ulcers is essential for wound healing recovery
process. The gold standard diabetic foot ulcer management entails wound debridement,
infection control, revascularization, and ulcers offloading. Debridement is performed to
show signs of autonomic neuropathy and dysfunction of the sudomotor (Schaper et al., 2012).
Diabetic patients are often at high risks of developing the disease of the peripheral
vascular area, thus assessment of the peripheral is necessary to assess blood circulation. Lack
of adequate limb perfusion related to vascular disease often affects the healing process, which
leads to unhealed chronic ulcers which are susceptible to infection (Lipsky et al., 2012). A
simple method of confirming arterial occlusion of the disease is assessing systolic blood
pressure on the arms and the ankles. This often carried out by assessing systolic pressure (Bus
et al., 2016).
Further, assessment of skin temperature on the hand back is intitated. Normal levels of
skin temperature often range between warm at the tibia to cool levels at the distal toes. The
temperature of the foot skin is measured with an infrared thermometer on the lower foot.
Increased temperature levels indicate to malfunction of the sudomotor and high risks of foot
ulceration (Shirazi, Nasiri & Yazdanpanah, 2016).
Physical assessment of the foot often assesses the perception of a pinprick, sensation of
the temperature, light sensation and pressure. Further neuropathic deficits can be assessed
using Neuropathy disability score with studies showing high predictive value (Neville,
Kayssi, Buecher & Stempel, 2016).
Nursing interventions
Potential evidence-based interventions for key nursing decisions for diabetic ulcers foot
entail a combination of clinical expertise and preferences of the patient and associated values
of care. key approaches for care as identified by Schaper et al., (2012) illustrated
identification of the at-risk foot, regular inspection, and examination, patient education,
routine footwear wearing and offering treatment management of pre-ulcerative observations.
Enhancing collaboration of multidisciplinary and holistic approach entails usage of well
organized multidisciplinary team which offering a coordinated nursing intervention approach.
Potential wound care actions
Case study management of diabetic foot ulcers is essential for wound healing recovery
process. The gold standard diabetic foot ulcer management entails wound debridement,
infection control, revascularization, and ulcers offloading. Debridement is performed to
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
remove the surface debris and underlying necrotic tissues. The removal of the debris
improves the healing process and production of granulation tissues. It is done by the surgical
process, biological methods, autolysis and enzymatic process (Lebrun, Tornic, Kirsner,
2010).
The offloading process of the ulcer area is crucial for the healing process. Both
retrospective and prospective studies have shown that increased levels of plantar pressures
contribute to plantar ulcers development. Inadequate offloading of the ulcers have been
shown to slow down the healing process. Benefits of ulcer offloading are increasing and have
been associated with recurrence risks of healed foot ulcer (Apelqvist et al., 2011).
Ulcers dressing offer a faster way of healing and reduced occurrence of infections. An
exception is when there is the presence of dry gangrene, in the necrotic area needs to be kept
dry so as to avoid infection and development of wet gangrene. A wound releases cytokines,
platelets, white blood cells, and growth factors. These factors aid in the healing process while
others produced by bacteria retards healing process.
The right dressing to be used needs to have free contamination from germs and has the
ability to clear excess exudation and toxic substance, while maintaining a cool environment,
has a permeability to allow to pass through (Game et al., 2012).
The potential outcomes of a multidisciplinary approach on the diabetic foot ulcers
patients are essential. The mechanism of the path physiology process entail multifactorial
factors such as neuropathy, ischemia, infection and abnormal foot structure. Thus with this
complex problem working in a multidisciplinary framework is essential. The role of experts
involved in the assessment of mechanical foot problems is key. Successful management often
involves recognizing the underlying etiology and its correction and preventing the
occurrence. Offloading care practices yield significant accelerations in healing times.
Offering reconstructive surgery becomes conservatory treatment in avoiding major
amputations and wounds on the neuropathic regions. Endpoints of the chronic foot often
result in a reduction of major amputations decreasing the occurrence of ulceration and
maintaining the integrity of the skin improving its function overall.
Further nutritional care for the patient is necessary. Nutrition management to manage
the underlying condition is critical as food intake can improve or lower the levels of glycemia
remove the surface debris and underlying necrotic tissues. The removal of the debris
improves the healing process and production of granulation tissues. It is done by the surgical
process, biological methods, autolysis and enzymatic process (Lebrun, Tornic, Kirsner,
2010).
The offloading process of the ulcer area is crucial for the healing process. Both
retrospective and prospective studies have shown that increased levels of plantar pressures
contribute to plantar ulcers development. Inadequate offloading of the ulcers have been
shown to slow down the healing process. Benefits of ulcer offloading are increasing and have
been associated with recurrence risks of healed foot ulcer (Apelqvist et al., 2011).
Ulcers dressing offer a faster way of healing and reduced occurrence of infections. An
exception is when there is the presence of dry gangrene, in the necrotic area needs to be kept
dry so as to avoid infection and development of wet gangrene. A wound releases cytokines,
platelets, white blood cells, and growth factors. These factors aid in the healing process while
others produced by bacteria retards healing process.
The right dressing to be used needs to have free contamination from germs and has the
ability to clear excess exudation and toxic substance, while maintaining a cool environment,
has a permeability to allow to pass through (Game et al., 2012).
The potential outcomes of a multidisciplinary approach on the diabetic foot ulcers
patients are essential. The mechanism of the path physiology process entail multifactorial
factors such as neuropathy, ischemia, infection and abnormal foot structure. Thus with this
complex problem working in a multidisciplinary framework is essential. The role of experts
involved in the assessment of mechanical foot problems is key. Successful management often
involves recognizing the underlying etiology and its correction and preventing the
occurrence. Offloading care practices yield significant accelerations in healing times.
Offering reconstructive surgery becomes conservatory treatment in avoiding major
amputations and wounds on the neuropathic regions. Endpoints of the chronic foot often
result in a reduction of major amputations decreasing the occurrence of ulceration and
maintaining the integrity of the skin improving its function overall.
Further nutritional care for the patient is necessary. Nutrition management to manage
the underlying condition is critical as food intake can improve or lower the levels of glycemia
6
in the body.
Combination of a multidisciplinary approach for ulcers diabetic care with a systematic
approach is essential for managing ischemia, foot and wound infection and helps in the
identification of dominant risks on the patient lifetime risks. The beneficial effects of
multidisciplinary are far-reaching. Enabling a focussed approach among the health care team,
patients and their family is essential in identifying patient needs and optimizing multifaceted
patient management and improving surveillance of patients. Research undertaken has
indicated that a coordinated care team approach lowers limb loss frequency among diabetic
patients (Krishnan et al., 2008).
Conclusion
Hence diabetic foot ulcers care is largely the focus of therapeutic challenge which
needs urgent needs on reviewing strategies and care burden through effective ways.
Prevention is critical so as to reduce and minimize morbidity and mortality rates and risks of
amputation. Case study assessment, foot examination, patient education, hygiene protocols
and wound care management offers significant progress on management aspect. Application
gold standards treatments need to be adhered to so as to prevent amputation stages. Thus
working through a multidisciplinary process is crucial in ensuring that all stakeholders
involved in the care process are involved in the treatment process. This, in turn, has a ripple
effect on the patient state and improve overall patient outcomes.
in the body.
Combination of a multidisciplinary approach for ulcers diabetic care with a systematic
approach is essential for managing ischemia, foot and wound infection and helps in the
identification of dominant risks on the patient lifetime risks. The beneficial effects of
multidisciplinary are far-reaching. Enabling a focussed approach among the health care team,
patients and their family is essential in identifying patient needs and optimizing multifaceted
patient management and improving surveillance of patients. Research undertaken has
indicated that a coordinated care team approach lowers limb loss frequency among diabetic
patients (Krishnan et al., 2008).
Conclusion
Hence diabetic foot ulcers care is largely the focus of therapeutic challenge which
needs urgent needs on reviewing strategies and care burden through effective ways.
Prevention is critical so as to reduce and minimize morbidity and mortality rates and risks of
amputation. Case study assessment, foot examination, patient education, hygiene protocols
and wound care management offers significant progress on management aspect. Application
gold standards treatments need to be adhered to so as to prevent amputation stages. Thus
working through a multidisciplinary process is crucial in ensuring that all stakeholders
involved in the care process are involved in the treatment process. This, in turn, has a ripple
effect on the patient state and improve overall patient outcomes.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

7
Annex
Diabetic foot ulcers pictorials information
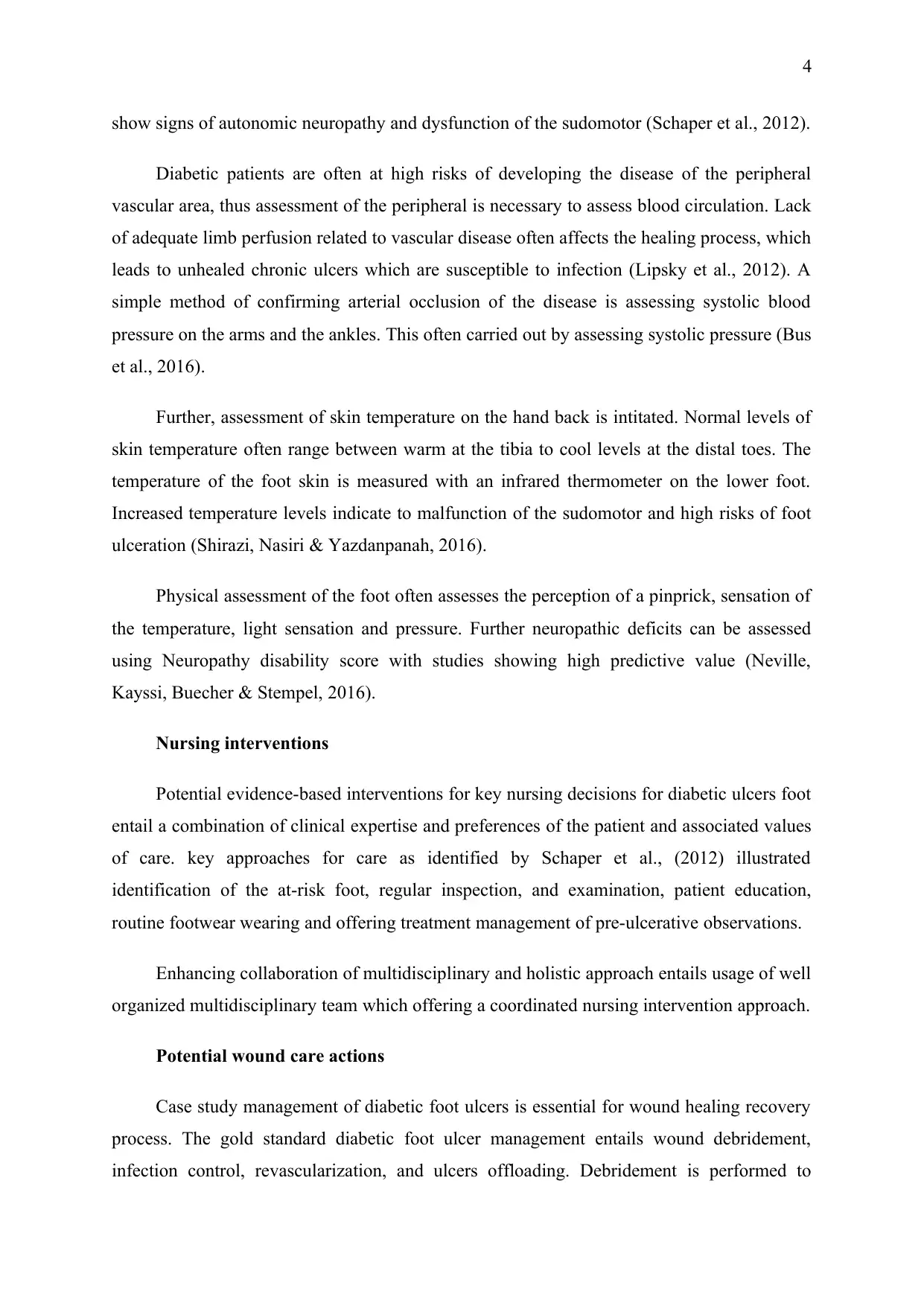
Figure 1 High risk gangrene and ulcer foot (Mishra et al.,2017)
Figure above illustrates a high risks diabetic ulcer foot patient with gangrene having
previous toe amputation.
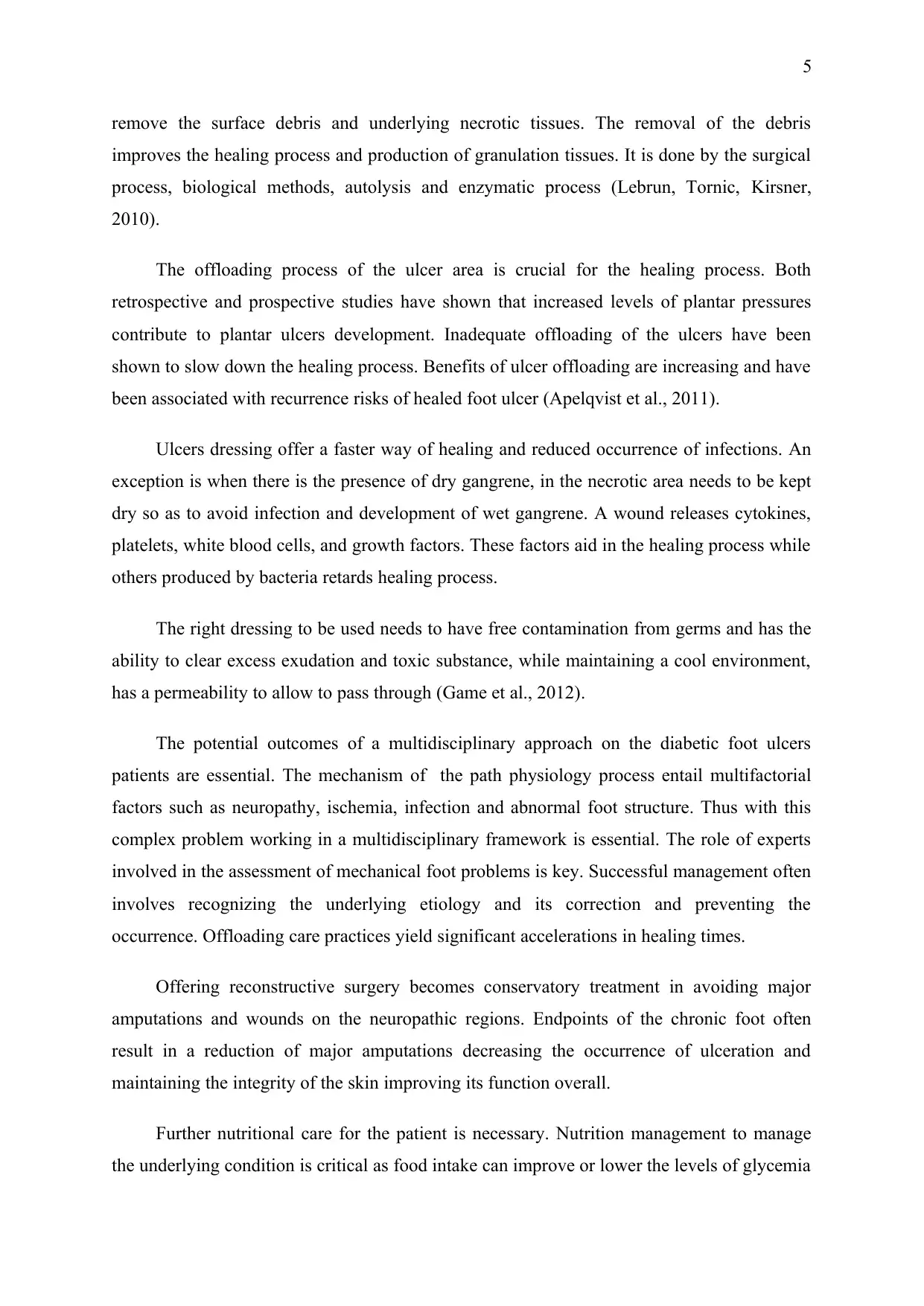
Figure 2 Hammer Toe defromity ulcer (Mishra et al, 2017)
Hammer toe condition of diabetic foot ulcer occasioned by weakened muscle son the
foot toe muscles
Annex
Diabetic foot ulcers pictorials information
Figure 1 High risk gangrene and ulcer foot (Mishra et al.,2017)
Figure above illustrates a high risks diabetic ulcer foot patient with gangrene having
previous toe amputation.
Figure 2 Hammer Toe defromity ulcer (Mishra et al, 2017)
Hammer toe condition of diabetic foot ulcer occasioned by weakened muscle son the
foot toe muscles
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
References
Apelqvist, J., Elgzyri, T., Larsson, J., Löndahl, M., Nyberg, P., & Thörne, J. (2011). Factors
related to outcome of neuroischemic/ischemic foot ulcer in diabetic patients. Journal
of vascular surgery, 53(6), 1582-1588.
Bus, S. A., Van Deursen, R. W., Armstrong, D. G., Lewis, J. E., Caravaggi, C. F., Cavanagh,
P. R., & International Working Group on the Diabetic Foot (IWGDF). (2016).
Footwear and offloading interventions to prevent and heal foot ulcers and reduce
plantar pressure in patients with diabetes: a systematic review. Diabetes/metabolism
research and reviews, 32, 99-118.
Game, F. L., Hinchliffe, R. J., Apelqvist, J., Armstrong, D. G., Bakker, K., Hartemann, A., ...
& Jeffcoate, W. J. (2012). A systematic review of interventions to enhance the healing
of chronic ulcers of the foot in diabetes. Diabetes/metabolism research and reviews,
28, 119-141.
Giovinco N., Miller J. D. (2015). A practical update to comprehensive screening in the high-
risk diabetic foot. Podiatry Management, February, 1
Krishnan, S., Nash, F., Baker, N., Fowler, D., & Rayman, G. (2008). Reduction in diabetic
amputations over 11 years in a defined UK population: benefits of multidisciplinary
team work and continuous prospective audit. Diabetes care, 31(1), 99-101.
Lauterbach, S., Kostev, K., & Kohlmann, T. (2010). Prevalence of diabetic foot syndrome
and its risk factors in the UK. Journal of wound care, 19(8), 333-337.
Lebrun, E., Tomic‐Canic, M., & Kirsner, R. S. (2010). The role of surgical debridement in
healing of diabetic foot ulcers. Wound repair and regeneration, 18(5), 433-438.
Lipsky, B. A., Berendt, A. R., Cornia, P. B., Pile, J. C., Peters, E. J., Armstrong, D. G., ... &
Pinzur, M. S. (2012). 2012 Infectious Diseases Society of America clinical practice
guideline for the diagnosis and treatment of diabetic foot infections. Clinical
infectious diseases, 54(12), e132-e173.
Miller, J. D., Carter, E., Shih, J., Giovinco, N. A., Boulton, A. J., Mills, J. L., & Armstrong,
D. G. (2014). How to do a 3-minute diabetic foot exam: this brief exam will help you
References
Apelqvist, J., Elgzyri, T., Larsson, J., Löndahl, M., Nyberg, P., & Thörne, J. (2011). Factors
related to outcome of neuroischemic/ischemic foot ulcer in diabetic patients. Journal
of vascular surgery, 53(6), 1582-1588.
Bus, S. A., Van Deursen, R. W., Armstrong, D. G., Lewis, J. E., Caravaggi, C. F., Cavanagh,
P. R., & International Working Group on the Diabetic Foot (IWGDF). (2016).
Footwear and offloading interventions to prevent and heal foot ulcers and reduce
plantar pressure in patients with diabetes: a systematic review. Diabetes/metabolism
research and reviews, 32, 99-118.
Game, F. L., Hinchliffe, R. J., Apelqvist, J., Armstrong, D. G., Bakker, K., Hartemann, A., ...
& Jeffcoate, W. J. (2012). A systematic review of interventions to enhance the healing
of chronic ulcers of the foot in diabetes. Diabetes/metabolism research and reviews,
28, 119-141.
Giovinco N., Miller J. D. (2015). A practical update to comprehensive screening in the high-
risk diabetic foot. Podiatry Management, February, 1
Krishnan, S., Nash, F., Baker, N., Fowler, D., & Rayman, G. (2008). Reduction in diabetic
amputations over 11 years in a defined UK population: benefits of multidisciplinary
team work and continuous prospective audit. Diabetes care, 31(1), 99-101.
Lauterbach, S., Kostev, K., & Kohlmann, T. (2010). Prevalence of diabetic foot syndrome
and its risk factors in the UK. Journal of wound care, 19(8), 333-337.
Lebrun, E., Tomic‐Canic, M., & Kirsner, R. S. (2010). The role of surgical debridement in
healing of diabetic foot ulcers. Wound repair and regeneration, 18(5), 433-438.
Lipsky, B. A., Berendt, A. R., Cornia, P. B., Pile, J. C., Peters, E. J., Armstrong, D. G., ... &
Pinzur, M. S. (2012). 2012 Infectious Diseases Society of America clinical practice
guideline for the diagnosis and treatment of diabetic foot infections. Clinical
infectious diseases, 54(12), e132-e173.
Miller, J. D., Carter, E., Shih, J., Giovinco, N. A., Boulton, A. J., Mills, J. L., & Armstrong,
D. G. (2014). How to do a 3-minute diabetic foot exam: this brief exam will help you
9
to quickly detect major risks and prompt you to refer patients to appropriate
specialists. Journal of Family Practice, 63(11), 646-654.
Mishra, S. C., Chhatbar, K. C., Kashikar, A., & Mehndiratta, A. (2017). Diabetic foot. Bmj,
359, j5064.
Moxey, P. W., Gogalniceanu, P., Hinchliffe, R. J., Loftus, I. M., Jones, K. J., Thompson, M.
M., & Holt, P. J. (2011). Lower extremity amputations—a review of global variability
in incidence. Diabetic Medicine, 28(10), 1144-1153.
Neville, R. F., Kayssi, A., Buescher, T., & Stempel, M. S. (2016). The diabetic foot. Current
problems in surgery, 53(9), 408-437.
Prompers, L., Huijberts, M., Schaper, N., Apelqvist, J., Bakker, K., Edmonds, M., ... &
Piaggesi, A. (2008). Resource utilisation and costs associated with the treatment of
diabetic foot ulcers. Prospective data from the Eurodiale Study. Diabetologia, 51(10),
1826.
Schaper, N. C., Andros, G., Apelqvist, J., Bakker, K., Lammer, J., Lepantalo, M., ... &
Hinchliffe, R. J. (2012). Diagnosis and treatment of peripheral arterial disease in
diabetic patients with a foot ulcer. A progress report of the International Working
Group on the Diabetic Foot. Diabetes/metabolism research and reviews, 28, 218-224.
Shirazi, A. A., Nasiri, M., & Yazdanpanah, L. (2016). Dermatological and musculoskeletal
assessment of diabetic foot: A narrative review. Diabetes & Metabolic Syndrome:
Clinical Research & Reviews, 10(2), S158-S164.
Tseng, C. L., Rajan, M., Miller, D. R., Lafrance, J. P., & Pogach, L. (2011). Trends in initial
lower extremity amputation rates among Veterans Health Administration health care
System users from 2000 to 2004. Diabetes Care, 34(5), 1157-1163.
to quickly detect major risks and prompt you to refer patients to appropriate
specialists. Journal of Family Practice, 63(11), 646-654.
Mishra, S. C., Chhatbar, K. C., Kashikar, A., & Mehndiratta, A. (2017). Diabetic foot. Bmj,
359, j5064.
Moxey, P. W., Gogalniceanu, P., Hinchliffe, R. J., Loftus, I. M., Jones, K. J., Thompson, M.
M., & Holt, P. J. (2011). Lower extremity amputations—a review of global variability
in incidence. Diabetic Medicine, 28(10), 1144-1153.
Neville, R. F., Kayssi, A., Buescher, T., & Stempel, M. S. (2016). The diabetic foot. Current
problems in surgery, 53(9), 408-437.
Prompers, L., Huijberts, M., Schaper, N., Apelqvist, J., Bakker, K., Edmonds, M., ... &
Piaggesi, A. (2008). Resource utilisation and costs associated with the treatment of
diabetic foot ulcers. Prospective data from the Eurodiale Study. Diabetologia, 51(10),
1826.
Schaper, N. C., Andros, G., Apelqvist, J., Bakker, K., Lammer, J., Lepantalo, M., ... &
Hinchliffe, R. J. (2012). Diagnosis and treatment of peripheral arterial disease in
diabetic patients with a foot ulcer. A progress report of the International Working
Group on the Diabetic Foot. Diabetes/metabolism research and reviews, 28, 218-224.
Shirazi, A. A., Nasiri, M., & Yazdanpanah, L. (2016). Dermatological and musculoskeletal
assessment of diabetic foot: A narrative review. Diabetes & Metabolic Syndrome:
Clinical Research & Reviews, 10(2), S158-S164.
Tseng, C. L., Rajan, M., Miller, D. R., Lafrance, J. P., & Pogach, L. (2011). Trends in initial
lower extremity amputation rates among Veterans Health Administration health care
System users from 2000 to 2004. Diabetes Care, 34(5), 1157-1163.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.