South Australian Aboriginal Children: SSB Consumption Health Programme
VerifiedAdded on 2020/05/03
1
Paraphrase This Document
Health promotion programme for the reduction of children’s consumption of sugar sweetened
beverages (SSB) among South Australian Aboriginal and Torres Strait Islander children.
Description:
In this health promotion programme, educational intervention will be provided to the children
and parents of South Australian Aboriginal and Torres Strait Islander. It is evident that health
promotion programmes through educational intervention will be useful in improving health
of the people. Health education will be provided at schools and restriction on the
consumption of SSB will be implemented among these children. Quantity and frequency of
SSB consumption will be recorded. Body weight and body mass index of children will be
measured. This programme will be implemented for 24 months. This programme will be
beneficial in reducing obesity in children.
2
Consumption of Sugar-sweetened beverages (SSB) is rising as global health concern and
multiple adverse effects are associated with its consumption. Abundant evidence is available
in the form of systemic reviews and meta analysis to establish exposure and effect
relationship between SSB and obesity. Moreover, it has been observed that SSB is the
autonomous risk factor for metabolic disease like type 2 diabetes and cardiovascular disease
and few cancers and dental caries (Te Morenga et al., 2012; Malik et al., 2013). As
consumption of SSB is associated with multiple health issues, its magnitude is high on health
and well-being of the person (Malik et al., 2010). Consumption of SSBs is more in
Aboriginal and Torres Strait Islander people as compared to the other population.
Along with obesity, there is high prevalence of metabolic disease in these people. A research
project entitled ‘Next Step’ identified association between food choices and exposure to
diseases as priority research area. This project is applicable throughout Australia and more
emphasis is given to Aboriginal and Torres Strait Islander people. This project has more
importance because it is a community driven project and importance has been given to the
needs and interests of Aboriginal and Torres Strait Islander people (King and Brown, 2015).
Comprehensive intervention for SSB consumption, need to be planned which address at
multiple levels because there is widespread availability of SSB and it is in high demand
specifically in the children. As a result, there high magnitude of negative health impact of
SSB and it is difficult to control by planning small scale or localised intervention. It is
evident that people in the lower socio-economic status are more vulnerable to adverse health
conditions as compared to the people in high-socioeconomic status (Pampel et al., 2010).
Aboriginal and Torres Strait Islander people belongs to low socio-economic class as
compared to non-indigenous people. In these people, adverse health conditions might be due
to more exposure to behavioural and environmental health risk factors, poor living conditions
and inadequate education. Cultural aspects and racism also have major impact on the health
inequalities among indigenous and non-indigenous people in Australia. Hence, for these
people community driven intervention need to be carried out (AHMAC, 2015).
As compared to the global context prevalence of obesity is more in Indigenous children. One
of the prominent reason observed for increased prevalence of obesity is consumption of
refined carbohydrates like SSB (Singh et al., 2010). There is a biological link between the
obesity and consumption of SSB. These SSBs overcome the homeostatic regulatory system
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Hence, Australian Dietary Guidelines recommend to limit consumption of SSB in the form
soft drink and cordial. Australian Medical Association and Public Health Association of
Australia also addressed importance of intervention to limit consumption of SSB.
Intervention measures include heavy taxation of soft drinks, channelling of revenue from sale
of soft drinks to preventive measures, ban on sale of soft drinks in schools, ban on promotion
and advertising of soft drinks to the children. These efforts are in line with the international
trials for reduction in SSB consumption. However, there is scarcity of literature for
description of SSB consumption based on source, demographic and other dietary habits
(NHMRC, 2013; AHMAC, 2015).
National Children's Nutrition and Physical Activity Survey (NCNPAS) conducted survey
among 4,487 children aged between 2 and 16 years. In this survey, it was concluded that SSB
intake is high in Australian children and it is the need of hour to implement public health
intervention. In this survey, it was observed that supermarkets are the primary source of SSB.
Most of these children consumed these beverages at the home. Inadequate education of
parents and children about the health consequences of SSB consumption are mainly
responsible for more consumption of SSB among Aboriginal and Torres Strait Islander
children. SSB contributed approximately 4 % energy in children of age between 2 – 3years
old and approximately 7.5 % energy in children between 14-16 years old. Independence in
the children of age 14-16 years old is mainly responsible for more consumption of SSB, even
though it is evident that approximately 75 % of the children used to consume SSB at home.
Previous interventions mainly focused on the fast food for assessing consumption of SSB.
Due to recent findings, focus of the intervention should be diverted towards SSB
consumption in supermarket and consumption at home. There is variation among children of
different age group for SSB consumption. Children in age group between 2- 3 years prefers
to drink sweetened juice and 2 - 5 years prefers to drink sweetened fruit punch and fruit
juice. Consumption of SSB at the critical phase of growth and development can have major
impact on the health of child for the rest of life (Hafekost et al., 2011; NCNPAS, 2007).
A survey was conducted among Indigenous children and in this survey, it was found that
approximately 65 % Indigenous children are consuming soft drinks containing SSB and out
of this approximately 55 % children are consuming these drinks at home. 85 % of these SSB
drinks are purchased from supermarkets. Both parents and children were incorporated in this
survey and children between age group 11 – 16 years were the target group. Data was
4
Paraphrase This Document
lead to augmentation of cases of obesity in Indigenous children. Based on this hypothesis,
protocol was developed to carry out actual health promotion programme. Our hypothesis
exhibited similar response to 2007 Australian National, Children’s Nutrition and Physical
Activity Survey.
Following are the sample of questions from the survey:
1. How much amount of SSB is present in the soft-drinks ?
2. Whether parents are accompanying children while drinking SSB containing soft-
drinks ?
3. What is frequency of purchase of soft drinks from supermarkets?
4. What is frequency of soft drink consumption at home ?
5
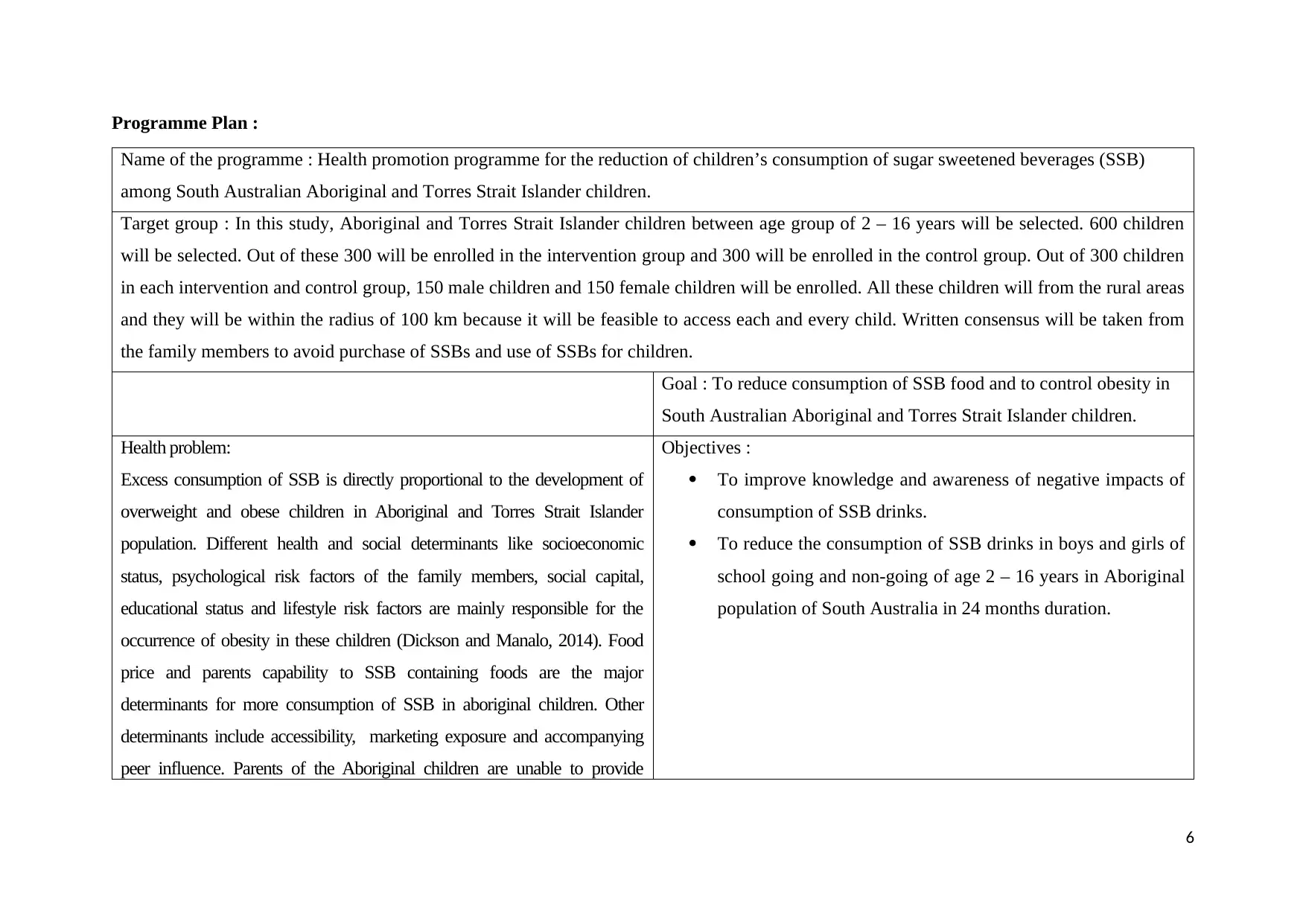
Name of the programme : Health promotion programme for the reduction of children’s consumption of sugar sweetened beverages (SSB)
among South Australian Aboriginal and Torres Strait Islander children.
Target group : In this study, Aboriginal and Torres Strait Islander children between age group of 2 – 16 years will be selected. 600 children
will be selected. Out of these 300 will be enrolled in the intervention group and 300 will be enrolled in the control group. Out of 300 children
in each intervention and control group, 150 male children and 150 female children will be enrolled. All these children will from the rural areas
and they will be within the radius of 100 km because it will be feasible to access each and every child. Written consensus will be taken from
the family members to avoid purchase of SSBs and use of SSBs for children.
Goal : To reduce consumption of SSB food and to control obesity in
South Australian Aboriginal and Torres Strait Islander children.
Health problem:
Excess consumption of SSB is directly proportional to the development of
overweight and obese children in Aboriginal and Torres Strait Islander
population. Different health and social determinants like socioeconomic
status, psychological risk factors of the family members, social capital,
educational status and lifestyle risk factors are mainly responsible for the
occurrence of obesity in these children (Dickson and Manalo, 2014). Food
price and parents capability to SSB containing foods are the major
determinants for more consumption of SSB in aboriginal children. Other
determinants include accessibility, marketing exposure and accompanying
peer influence. Parents of the Aboriginal children are unable to provide
Objectives :
To improve knowledge and awareness of negative impacts of
consumption of SSB drinks.
To reduce the consumption of SSB drinks in boys and girls of
school going and non-going of age 2 – 16 years in Aboriginal
population of South Australia in 24 months duration.
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
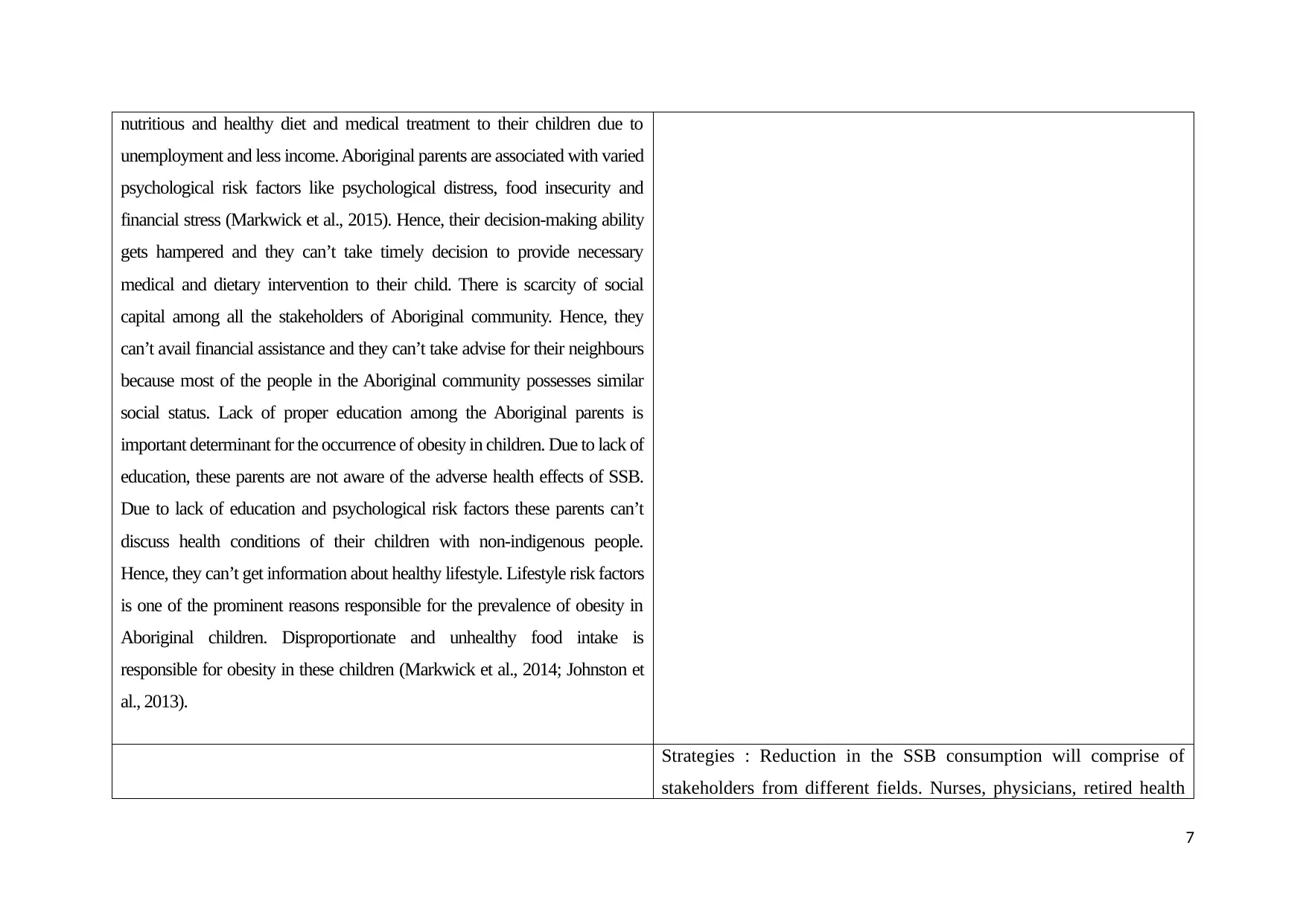
unemployment and less income. Aboriginal parents are associated with varied
psychological risk factors like psychological distress, food insecurity and
financial stress (Markwick et al., 2015). Hence, their decision-making ability
gets hampered and they can’t take timely decision to provide necessary
medical and dietary intervention to their child. There is scarcity of social
capital among all the stakeholders of Aboriginal community. Hence, they
can’t avail financial assistance and they can’t take advise for their neighbours
because most of the people in the Aboriginal community possesses similar
social status. Lack of proper education among the Aboriginal parents is
important determinant for the occurrence of obesity in children. Due to lack of
education, these parents are not aware of the adverse health effects of SSB.
Due to lack of education and psychological risk factors these parents can’t
discuss health conditions of their children with non-indigenous people.
Hence, they can’t get information about healthy lifestyle. Lifestyle risk factors
is one of the prominent reasons responsible for the prevalence of obesity in
Aboriginal children. Disproportionate and unhealthy food intake is
responsible for obesity in these children (Markwick et al., 2014; Johnston et
al., 2013).
Strategies : Reduction in the SSB consumption will comprise of
stakeholders from different fields. Nurses, physicians, retired health
7
Paraphrase This Document
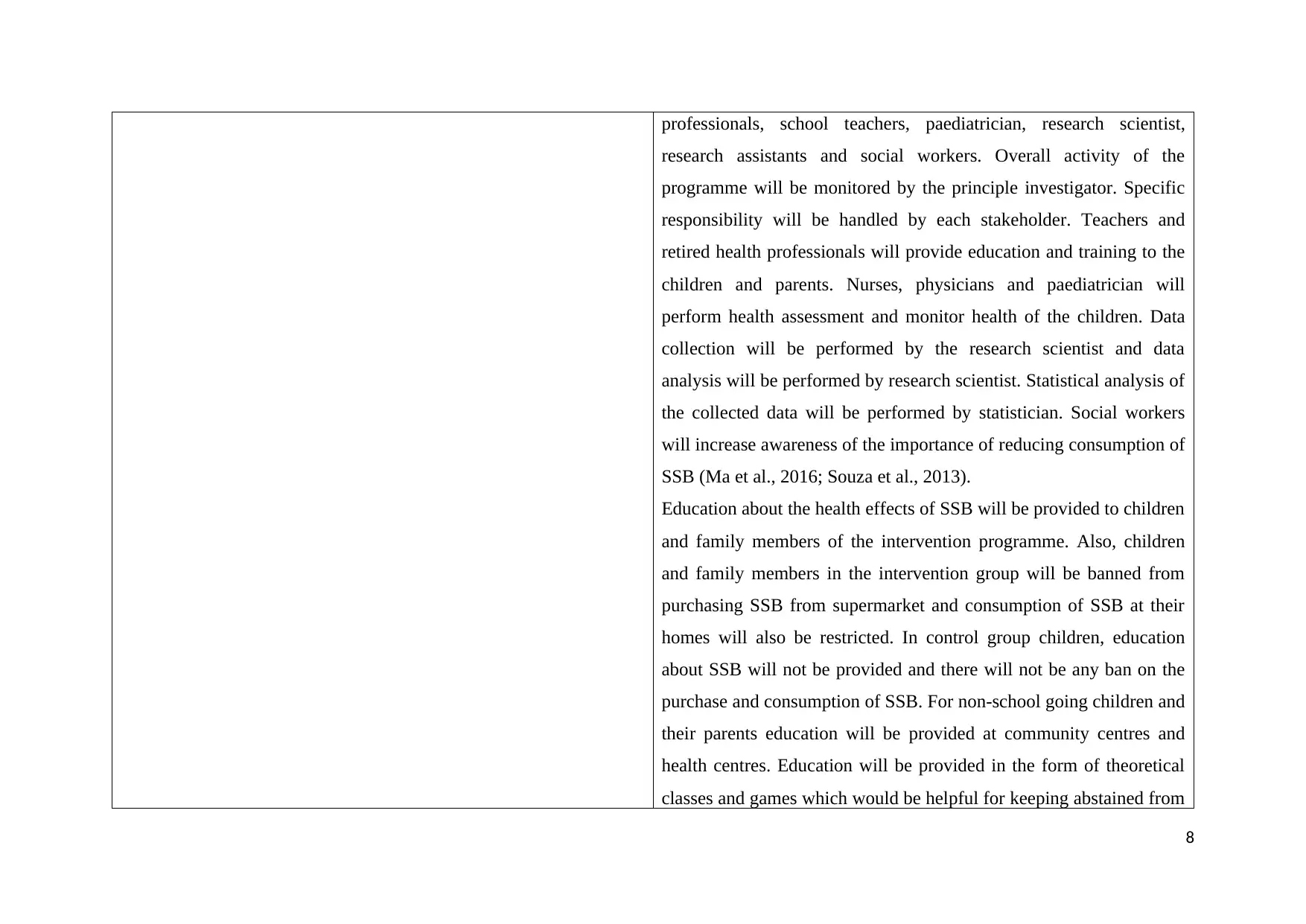
research assistants and social workers. Overall activity of the
programme will be monitored by the principle investigator. Specific
responsibility will be handled by each stakeholder. Teachers and
retired health professionals will provide education and training to the
children and parents. Nurses, physicians and paediatrician will
perform health assessment and monitor health of the children. Data
collection will be performed by the research scientist and data
analysis will be performed by research scientist. Statistical analysis of
the collected data will be performed by statistician. Social workers
will increase awareness of the importance of reducing consumption of
SSB (Ma et al., 2016; Souza et al., 2013).
Education about the health effects of SSB will be provided to children
and family members of the intervention programme. Also, children
and family members in the intervention group will be banned from
purchasing SSB from supermarket and consumption of SSB at their
homes will also be restricted. In control group children, education
about SSB will not be provided and there will not be any ban on the
purchase and consumption of SSB. For non-school going children and
their parents education will be provided at community centres and
health centres. Education will be provided in the form of theoretical
classes and games which would be helpful for keeping abstained from
8
Educational and health promotion programme will comprise of
(Rauba et al., 2017):
Development of school wellness committee comprising of
‘sugar free’ lesson plan.
Posters displaying ‘sugar free life’ in cafeteria of the school.
Lessons will be presented to teachers during weekly staff get-
together and in parents meeting. Suggestions from the parents
and teachers will be considered for improvement in the
programme.
Lessons will comprise of information about the adverse health
conditions related to the SSB, lifestyle measures to prevent
development of obesity, healthy diet formula for the children
and alternative drinks for SSB like real fruit juice.
Letters comprising of instructions to avoid purchase and use
of SSB will be sent to home of each student.
Special seminars will be arranged by nutritionist.
Weekly 4 X 45 min. lessons will be arranged.
Weekly 1 X 60 min. lesson will be planned of lifestyle
modifications.
Students will be advised to take part sports with more physical
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Discounts will be provided for the bottles of real fruit juices in
the cafeteria.
Surveys will be conducted for parents and students to assess
improvement in the awareness of sugar free life. Based on the
outcome of the surveys, necessary modifications in the
programme will be implemented.
Weekly once home delivery of healthy drinks like real fruit
juice.
Children in both intervention group and control group will be
monitored for consumption of amount of SSBs and types of SSBs for
one year. All the enrolled children will also be assessed for obesity.
Body weight and body mass index will be evaluated for assessment of
obesity for 24 months.
Data collection:
Dara related to amount of SSB consumption, type of SSB, body
weight and body mass index will be collected. Semi-structured
interviews will be conducted for parents of the children for amount
and quality of SSB consumption. Semi-structured interviews have the
option of slight modification in the framework of questions.
Questionnaires will be prepared based on the validated questions
10
Paraphrase This Document
in the field. Data related to food consumption will be collected over
the phone by enquiring with parents. Research assistance will collect
data for food consumption. Data related to body weight and body
mass index will be measured and recorded by nurses and other
healthcare professionals. Body weight and body mass index data will
be collected at designated healthcare centres.
Data analysis:
Collected data will be stored in Microsoft Excel and mean and
standard deviation will be calculated for this data. Compiled data will
be verified and reviewed by research assistance and research scientist
respectively. For each children data will be stored in coded form to
maintain confidentiality of the data. Data will be presented in the
form of tables and graphs and these will be prepared separately for
intervention group and control group. Power calculation will be done
for statistical significance. Mean difference between intervention
group and control will calculated. Within each group, data will be
calculated and presented for boys and girls separately. Statistical
analysis will be performed by using SPSS 18.0 software (SPSS Inc.,
Chicago, IL, USA). For comparison intervention group and control;
and boys and girls of the same group, either ‘t’ test or one-way
repeated measures ANOVA will be implemented. Post hoc
11

implementing Tukey test and Pearson’s coefficients (Petrie and Sabin,
2016).
12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Health promotion theory:
Life course Health Development model (LCHDM) is applicable in this intervention of
reduction in SSB consumption in indigenous children. This is based on the development of
health throughout lifetime. This evolution of health is specific for certain period. This
intervention is specifically designed for children below 16 years. Hence, LCHDM is more
relevant to this SSB consumption reduction programme. Growth, development and health of
children specifically dependent on the health status of the children in the childhood.
Unhealthy food and condition like obesity in childhood can adversely affect that particular
person in adulthood. Embedding component of LCHDM specifically focused on integrating
concept experiences for improving structure and functioning of the person. This embedding
concept can be applicable for improving educational and nutritional status of the children.
This concept is helpful in policy development for health promotion. According to LCHDM,
assessment of the individual can be performed throughout life because negative impacts of
nutrition and health can be extended throughout life. In this intervention also, SSB food can
influence obesity in adulthood also. According to LCHDM, functional trajectory assessment
is an important component. SSB induced obesity in children can adversely affect functional
activity of children (Halfon et al., 2014; Cheng and Solomon, 2014).
Policy and principles :
WHO in 2002 recommended to implement Obesity and diet related chronic disease
prevention policy. More than 100 countries are implementing this policy and there is positive
outcome are evident as a result of implementation of this policy. This policy is useful in
establishing relationship between diet, physical activity and nutrition based chronic disease
like obesity. Obesity mainly occurs due more energy consumption in the form of foods like
SSB and less energy expenditure decline in physical activity. This policy includes activities
like food based dietary guidelines, nutritional counselling and food labelling. Promotion of
health-related messages through different media proved most useful strategy for the
implementation of this policy. Promotion of fruits and vegetable consumption and regulation
on sale of high energy food for children proved fruitful in controlling diet induced chromic
disease like obesity in children. Implementation of this policy in school based interventions
proved beneficial in controlling obesity in children. School based interventions include
banning unhealthy food vending machines in the schools, surveys to identify children with
13
Paraphrase This Document
products in schools (Malik et al., 2013; Ogata and Hayes, 2014). In this programme policies
related to social support and social determinant of health will be addressed. This health
promotion programme will be carried out on evidence based research and socially and
culturally appropriate methods will be implemented (Visagie and Schneider, 2014).
Ottawa Charter for Health Promotion:
Ottawa Charter for Health Promotion was adopted at international health conference.
National developments in Indigenous health promotion is the part of Ottawa Charter. Healthy
life to all the Indigenous people can be provided by affording nutritious food and ensuring
optimum physical activity. There is a provision for providing community-controlled health
services to Indigenous people in culturally appropriate manner. For the promotion of health
among Indigenous people, Aboriginal community-controlled health services (ACCHSs) was
established in 1971 in Sydney. According to Ottawa Charter, health promotion is
augmentation in control over and improvement in health. There should be complete physical,
mental and social well-being of the individual or group of individuals. In this health
promotion programme also, efforts will be taken to provide complete management of the
children with obesity to enable their proper growth. Health promotion is not the mere
responsibility of healthcare sector, however other stakeholders should also contribute to
change life-style of the people to enable health promotion. In this health promotion
programme, there is need of contribution from other stakeholders like teachers, family
members and social workers for the reduction of SSB consumption in the children (Potvin
and Jones, 2011; Roden and Jarvis, 2012).
Research on similar interventions:
Australian Health Survey estimated that consumption of SSB is approximately 50 % in
Aboriginal and Torres Strait Islander people and it is approximately 34 % in non-indigenous
people (ABS, 2013). Obesity trend is similar to the SSB consumption among Aboriginal and
Torres Strait Islander people and non-indigenous people. Aboriginal and Torres Strait
Islander people exhibited more obesity as compared to the non-indigenous people.
Approximately 66 % adults and 30 % children are associated with obesity in Aboriginal and
Torres Strait Islander population (2015). In addition to this occurrence of non-communicable
diseases is also more in indigenous people as compared to the non-indigenous people. Next
step, a community driven research project was implemented in collaboration with South
14
is mainly responsible for the poor health of Indigenous children and it should be projected as
national health issue. It is evident from the studies, Aboriginal people and children and
people are less educated and less employed. Hence, they are living in poor housing
conditions. These are responsible for the less knowledge about the adverse health effects of
SSB food in Indigenous people and children. It has been established that early food choices
of child can lead to later life food preferences. Parents control over child’s food choices can
result in the lesser consumption of SSB drinks by the child. Public health strategies in the
form of health education to the parents can effectively reduce consumption of SSB drinks.
Variations in the consumption of SSB drinks among children of various age groups warrants
age specific intervention to reduce SSB consumption (Fiorito et al., 2010). High consumption
of SSB drinks is directly proportional to the poor dietary education and lesser physical
activities (Ranjit et al., 2010).
15
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Evaluation of health promotion programmes designed for the children’s is necessary because
implementation of the wrong programme can impact health of the children for life-long.
Reduction in the consumption of SSB consumption will be implemented in the Indigenous
children of Australia. This health promotion programme will be implemented according to
the socio-ecological model of health and health-promotion principles. This programme will
be specifically targeted towards children; however, parents will also be incorporated in the
programme. Hence, this programme will bring overall improvement in the health of the
society. This programme will bring changes in the physical, social and economic aspects of
the of Indigenous children and their parents and improvements in the behavioural aspects
(Nakkash et al., 2012).
For evaluation of the successful decrement in the consumption of SSB, data will be collected
in the form of survey and interview. Data related to SSB consumption will be collected prior
to and after completion of the health promotion programme. Data related to sales of SSB will
be collected from the school canteen and home of children. Impact outcome will be
evaluated based on the by asking questions to the children and parents. Questions will be
asked related to the amount of SSB consumption and change in behaviour of the children
(Wallace et al., 2014).
16
Paraphrase This Document
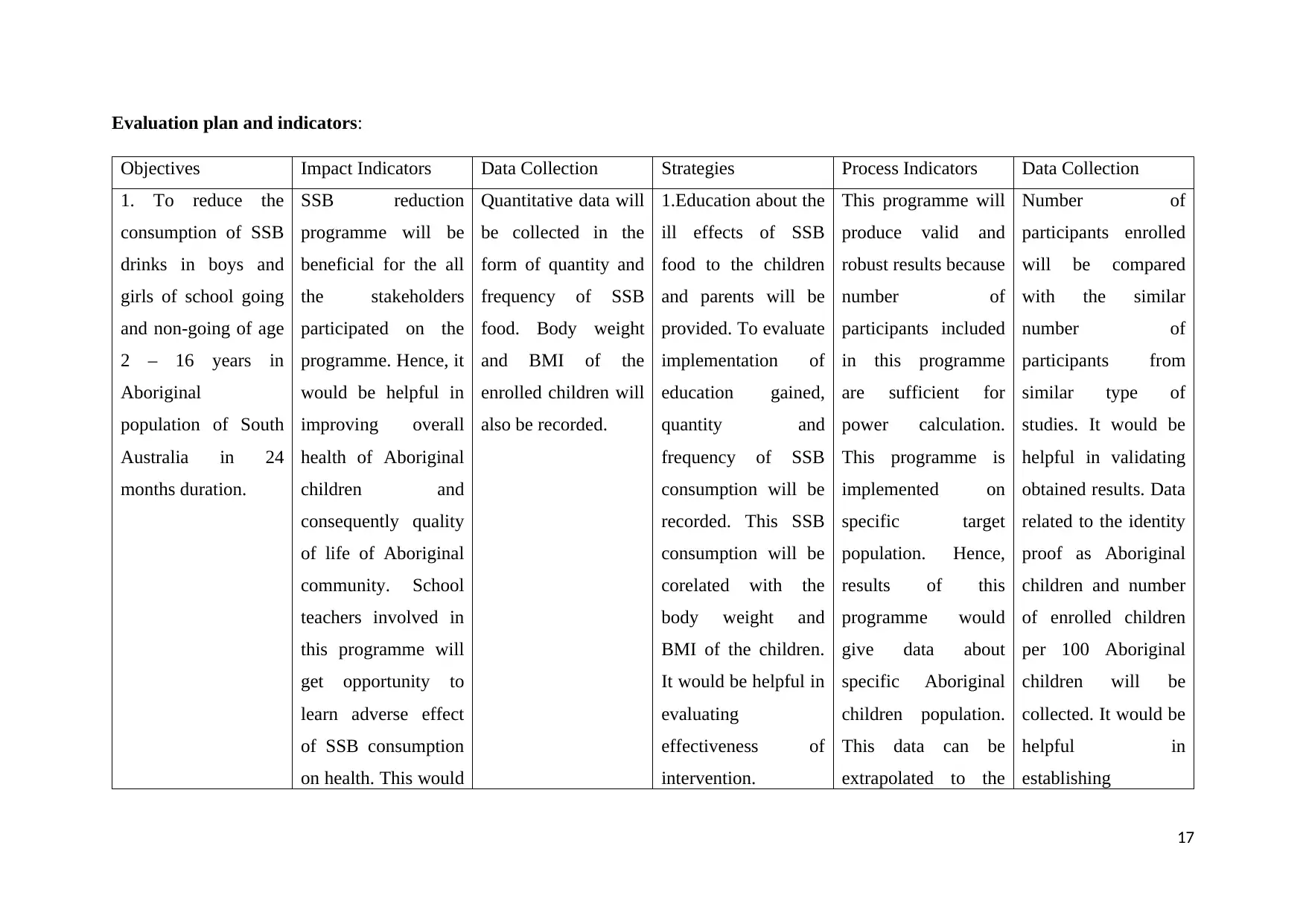
Objectives Impact Indicators Data Collection Strategies Process Indicators Data Collection
1. To reduce the
consumption of SSB
drinks in boys and
girls of school going
and non-going of age
2 – 16 years in
Aboriginal
population of South
Australia in 24
months duration.
SSB reduction
programme will be
beneficial for the all
the stakeholders
participated on the
programme. Hence, it
would be helpful in
improving overall
health of Aboriginal
children and
consequently quality
of life of Aboriginal
community. School
teachers involved in
this programme will
get opportunity to
learn adverse effect
of SSB consumption
on health. This would
Quantitative data will
be collected in the
form of quantity and
frequency of SSB
food. Body weight
and BMI of the
enrolled children will
also be recorded.
1.Education about the
ill effects of SSB
food to the children
and parents will be
provided. To evaluate
implementation of
education gained,
quantity and
frequency of SSB
consumption will be
recorded. This SSB
consumption will be
corelated with the
body weight and
BMI of the children.
It would be helpful in
evaluating
effectiveness of
intervention.
This programme will
produce valid and
robust results because
number of
participants included
in this programme
are sufficient for
power calculation.
This programme is
implemented on
specific target
population. Hence,
results of this
programme would
give data about
specific Aboriginal
children population.
This data can be
extrapolated to the
Number of
participants enrolled
will be compared
with the similar
number of
participants from
similar type of
studies. It would be
helpful in validating
obtained results. Data
related to the identity
proof as Aboriginal
children and number
of enrolled children
per 100 Aboriginal
children will be
collected. It would be
helpful in
establishing
17
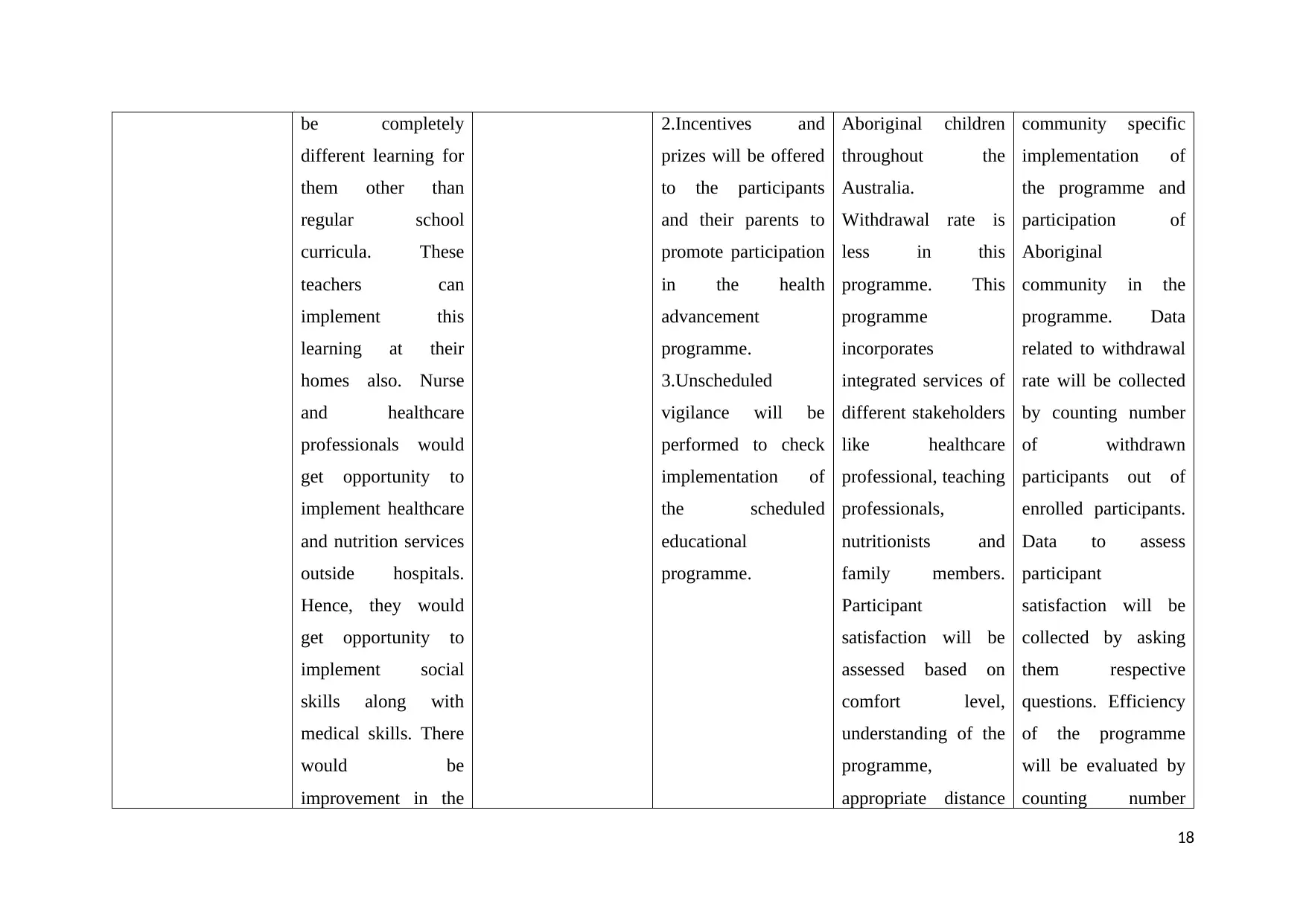
different learning for
them other than
regular school
curricula. These
teachers can
implement this
learning at their
homes also. Nurse
and healthcare
professionals would
get opportunity to
implement healthcare
and nutrition services
outside hospitals.
Hence, they would
get opportunity to
implement social
skills along with
medical skills. There
would be
improvement in the
2.Incentives and
prizes will be offered
to the participants
and their parents to
promote participation
in the health
advancement
programme.
3.Unscheduled
vigilance will be
performed to check
implementation of
the scheduled
educational
programme.
Aboriginal children
throughout the
Australia.
Withdrawal rate is
less in this
programme. This
programme
incorporates
integrated services of
different stakeholders
like healthcare
professional, teaching
professionals,
nutritionists and
family members.
Participant
satisfaction will be
assessed based on
comfort level,
understanding of the
programme,
appropriate distance
community specific
implementation of
the programme and
participation of
Aboriginal
community in the
programme. Data
related to withdrawal
rate will be collected
by counting number
of withdrawn
participants out of
enrolled participants.
Data to assess
participant
satisfaction will be
collected by asking
them respective
questions. Efficiency
of the programme
will be evaluated by
counting number
18
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
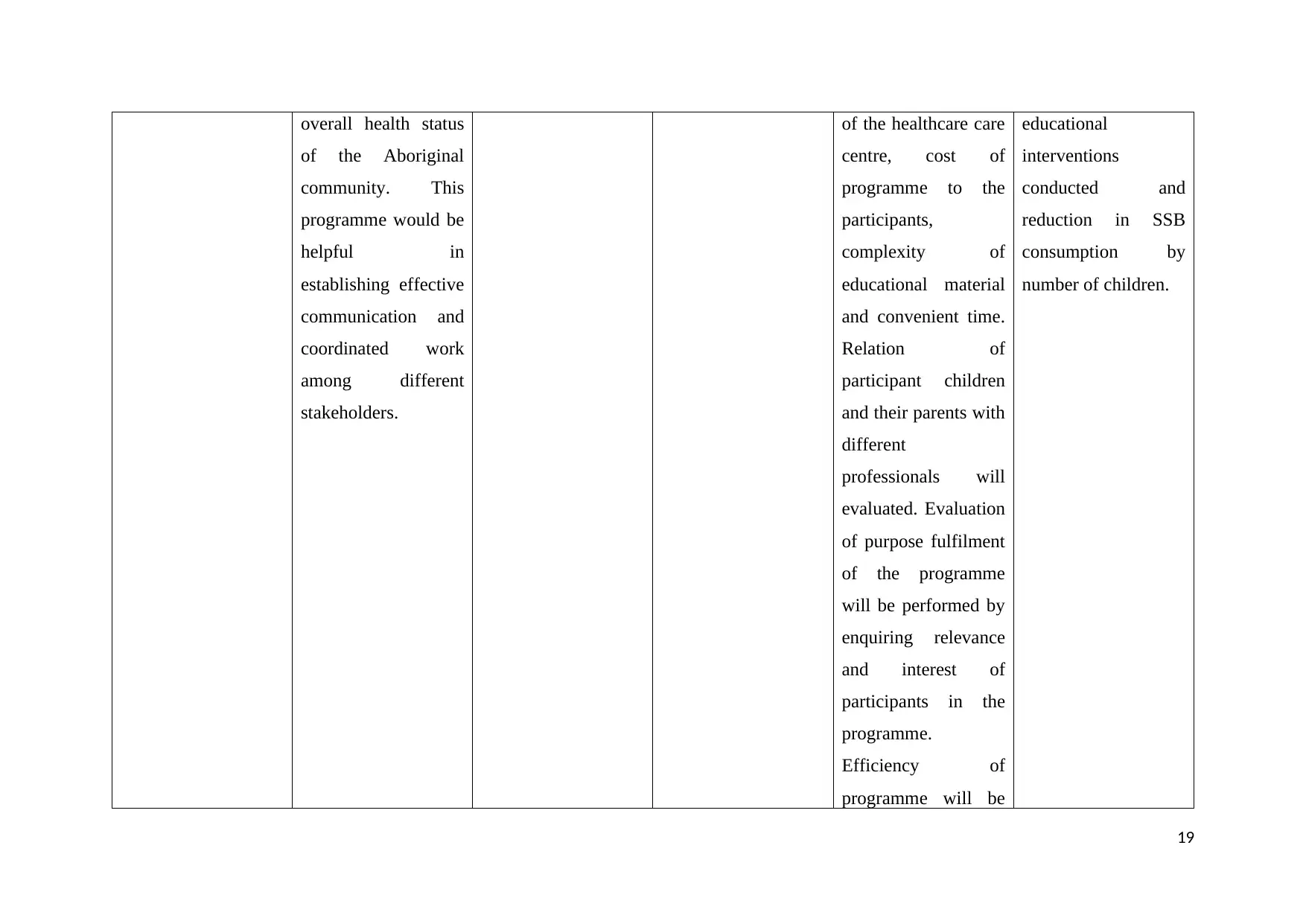
of the Aboriginal
community. This
programme would be
helpful in
establishing effective
communication and
coordinated work
among different
stakeholders.
of the healthcare care
centre, cost of
programme to the
participants,
complexity of
educational material
and convenient time.
Relation of
participant children
and their parents with
different
professionals will
evaluated. Evaluation
of purpose fulfilment
of the programme
will be performed by
enquiring relevance
and interest of
participants in the
programme.
Efficiency of
programme will be
educational
interventions
conducted and
reduction in SSB
consumption by
number of children.
19
Paraphrase This Document
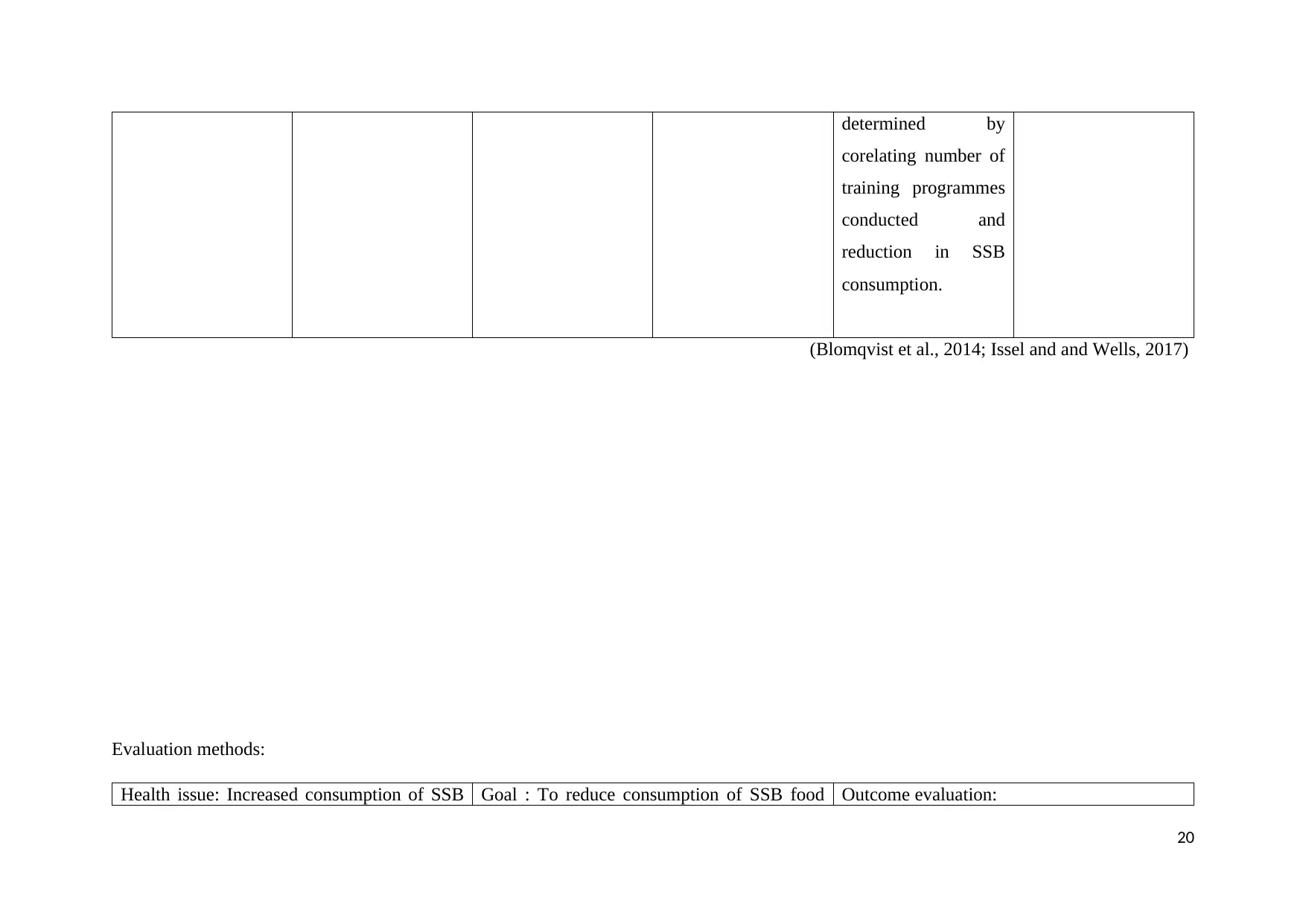
corelating number of
training programmes
conducted and
reduction in SSB
consumption.
(Blomqvist et al., 2014; Issel and and Wells, 2017)
Evaluation methods:
Health issue: Increased consumption of SSB Goal : To reduce consumption of SSB food Outcome evaluation:
20
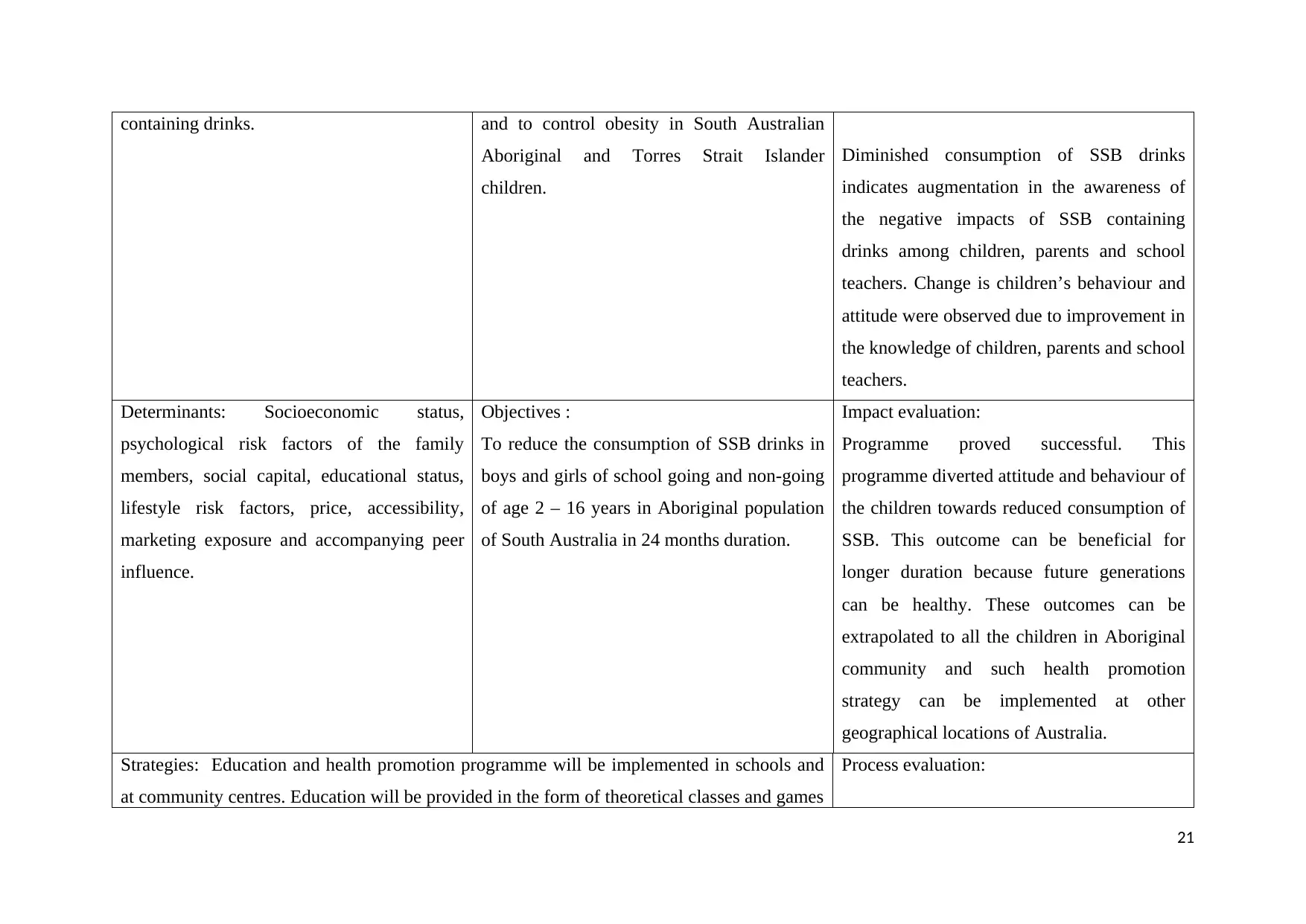
Aboriginal and Torres Strait Islander
children.
Diminished consumption of SSB drinks
indicates augmentation in the awareness of
the negative impacts of SSB containing
drinks among children, parents and school
teachers. Change is children’s behaviour and
attitude were observed due to improvement in
the knowledge of children, parents and school
teachers.
Determinants: Socioeconomic status,
psychological risk factors of the family
members, social capital, educational status,
lifestyle risk factors, price, accessibility,
marketing exposure and accompanying peer
influence.
Objectives :
To reduce the consumption of SSB drinks in
boys and girls of school going and non-going
of age 2 – 16 years in Aboriginal population
of South Australia in 24 months duration.
Impact evaluation:
Programme proved successful. This
programme diverted attitude and behaviour of
the children towards reduced consumption of
SSB. This outcome can be beneficial for
longer duration because future generations
can be healthy. These outcomes can be
extrapolated to all the children in Aboriginal
community and such health promotion
strategy can be implemented at other
geographical locations of Australia.
Strategies: Education and health promotion programme will be implemented in schools and
at community centres. Education will be provided in the form of theoretical classes and games
Process evaluation:
21
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
family members in the intervention group will be banned from purchasing SSB from
supermarket and consumption of SSB at their homes will also be restricted. ‘Sugar free’
lesson plan will be incorporated in the school curricula. Posters displaying ‘sugar free life’ in
cafeteria of the school. Discounts will be provided for the bottles of real fruit juices in the
cafeteria. Weekly once home delivery of healthy drinks like real fruit juice.
Every aspect and each step of programme
should be assessed to establish relationship
between steps implemented in the programme
and its respective outcome. It would be
helpful evaluating whether implemented
strategies are useful in achieving objectives
of the programme. This programme also
would be helpful in validating process of the
programme, so that it can be implemented at
other population and geographical areas.
22
Paraphrase This Document
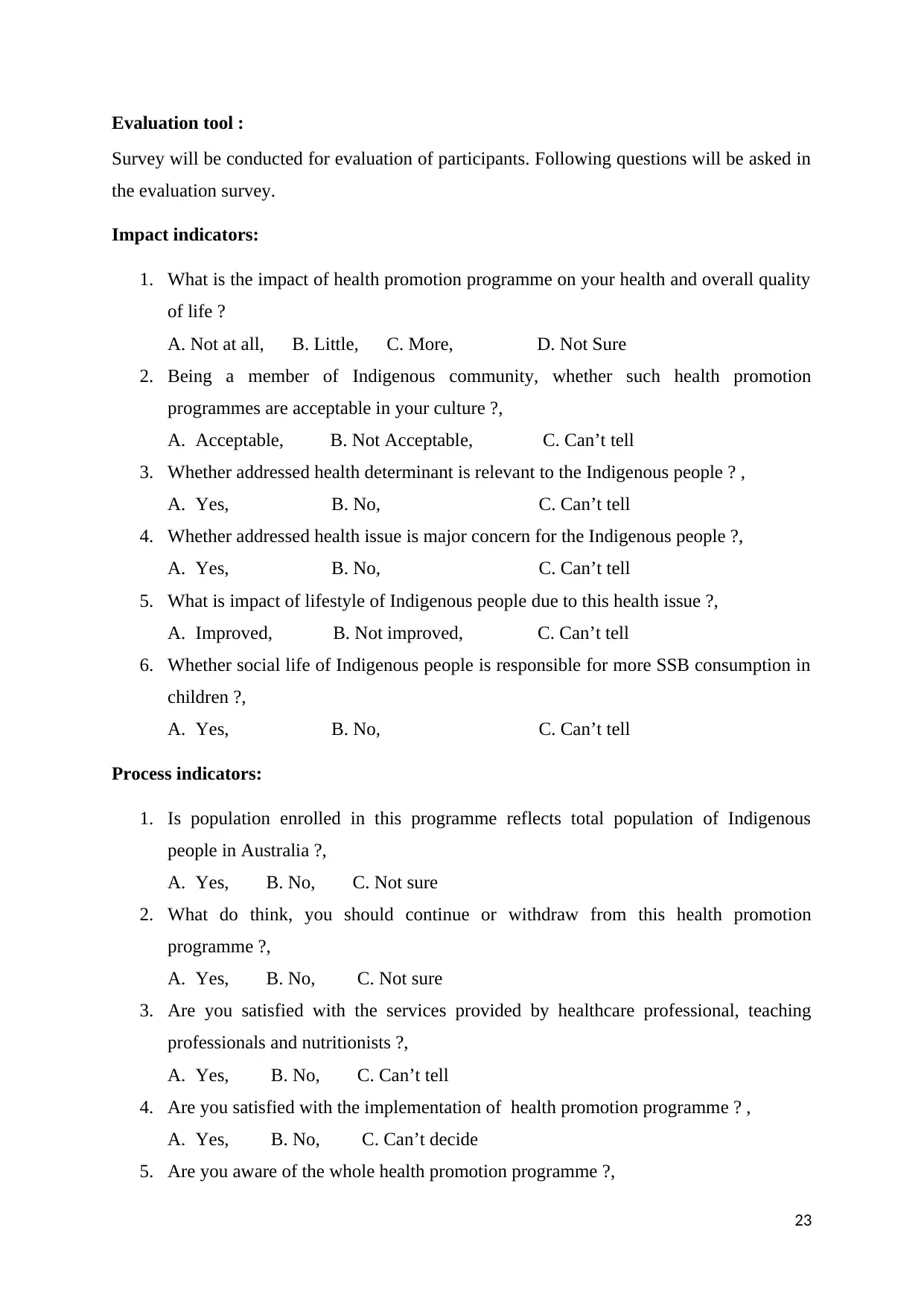
Survey will be conducted for evaluation of participants. Following questions will be asked in
the evaluation survey.
Impact indicators:
1. What is the impact of health promotion programme on your health and overall quality
of life ?
A. Not at all, B. Little, C. More, D. Not Sure
2. Being a member of Indigenous community, whether such health promotion
programmes are acceptable in your culture ?,
A. Acceptable, B. Not Acceptable, C. Can’t tell
3. Whether addressed health determinant is relevant to the Indigenous people ? ,
A. Yes, B. No, C. Can’t tell
4. Whether addressed health issue is major concern for the Indigenous people ?,
A. Yes, B. No, C. Can’t tell
5. What is impact of lifestyle of Indigenous people due to this health issue ?,
A. Improved, B. Not improved, C. Can’t tell
6. Whether social life of Indigenous people is responsible for more SSB consumption in
children ?,
A. Yes, B. No, C. Can’t tell
Process indicators:
1. Is population enrolled in this programme reflects total population of Indigenous
people in Australia ?,
A. Yes, B. No, C. Not sure
2. What do think, you should continue or withdraw from this health promotion
programme ?,
A. Yes, B. No, C. Not sure
3. Are you satisfied with the services provided by healthcare professional, teaching
professionals and nutritionists ?,
A. Yes, B. No, C. Can’t tell
4. Are you satisfied with the implementation of health promotion programme ? ,
A. Yes, B. No, C. Can’t decide
5. Are you aware of the whole health promotion programme ?,
23
6. Do you understand educational complexities in this health promotion programme ?
(Hodges and Videto, 2011).
A. Understood, B. Not-understood, C. Partially understood
(Hodges and Videto,
2011).
24
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Australian Bureau of Statistics. (2013). Australian Aboriginal and Torres Strait Islander
Health Survey: First Results, Australia, 2012–13. Canberra: Australia Bureau of Statistics,
2013. Retrieved from http://www.abs.gov.au/ausstats/abs@.nsf/mf/4727.0.55.001 on
31.10.2017.
Australian Bureau of Statistics. (2015). Australian Health survey: nutrition first results-Foods
and Nutrients, 2011–12. Table 18: Consumption of Sweetened Beverages. Canberra:
Australian Bureau of Statistics, 2015. Retrieved from
http://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/4364.0.55.007Main+Features12011-
12.on 31.10.2017.
Australian Health Ministers’ Advisory Council. (2015). Aboriginal and Torres Strait Islander
Health Performance Framework 2014 Report. Canberra: AHMAC, 2015. Retrieved from
https://www.pmc.gov.au/sites/default/files/publications/Aboriginal_and_Torres_Strait_Island
er_HPF_2014%20-%20edited%2016%20June2015.pdf. On 31.10.2017.
Avery A, Bostock L, McCullough F. (2015). A systematic review investigating interventions
that can help reduce consumption of sugar-sweetened beverages in children leading to
changes in body fatness. J Hum Nutr Diet. 28(1), pp. 52-64.
Blomqvist P, Ojala E, Kettunen T, Poskiparta M, Kasila K. (2014). Community-based oral
health promotion practices targeted at children and adolescents in Finland--developing an
assessment tool. Community Dent Oral Epidemiol. 42(3), pp. 245-53.
Cheng TL, Solomon BS. (2014). Translating Life Course Theory to clinical practice to
address health disparities. Matern Child Health J. 18(2), pp. 389-95.
Dickson M, Manalo G. (2014). The beyond borders initiative: Aboriginal, Torres Strait
Islander and international public health students: engaging partners in cross-cultural learning.
Educ Health (Abingdon). 27(2), pp. 132-7.
Fiorito LM, Marini M, Mitchell DC, Smiciklas-Wright H, Birch LL. (2010). Girls’ early
sweetened carbonated beverage intake predicts different patterns of beverage and nutrient
intake across childhood and adolescence. J Am Diet Assoc. 110(4), pp. 543-550.
Hafekost, K., Mitrou, F., Lawrence, D., and Zubrick, S. R. (2011). Sugar sweetened
beverage consumption by Australian children: Implications for public health strategy. BMC
Public Health. 11: 950. doi: 10.1186/1471-2458-11-950.
Halfon N, Larson, K, Lu, M, Tullis, E, Russ S. (2014). Lifecourse health development: past,
present and future. Maternal and Child Health Journal, 18(2), pp. 344-65.
Health Council of South Australia, 2015. Retrieved from
http://ahcsa.org.au/app/uploads/2014/11/AHCSA_Next_Steps_2015.pdf on 31.10.2017.
Hodges BC, Videto, D M. (2011). Assessment and Planning in Health Programs. Jones &
Bartlett.
25
Paraphrase This Document
sweetened beverage consumption will reduce the prevalence of obesity and obesity-related
diseases. Obes Rev. 14, pp. 606–19.
Issel L M, Wells R. (2017). Health Program Planning and Evaluation. Jones & Bartlett
Learning.
Johnston L, Doyle J, Morgan B, Atkinson-Briggs S, Firebrace B, Marika M, Reilly R, Cargo
M, Riley T, Rowley K. (2013). A review of programs that targeted environmental
determinants of Aboriginal and Torres Strait Islander health. Int J Environ Res Public Health.
10(8), 3518-42.
King R, Brown A. (2015). Next steps for Aboriginal Health Research: exploring how
research can improve the health and wellbeing of aboriginal people in South Australia.
Adelaide: Aboriginal .
Ma Y, He FJ, Yin Y, Hashem KM, MacGregor GA. (2016). Gradual reduction of sugar in
soft drinks without substitution as a strategy to reduce overweight, obesity, and type 2
diabetes: a modelling study. Lancet Diabetes Endocrinol. 4(2), pp. 105-14.
Markwick A, Ansari Z, Sullivan M, McNeil J. (2015). Social determinants and psychological
distress among Aboriginal and Torres Strait islander adults in the Australian state of Victoria:
a cross-sectional population based study. Soc Sci Med. 128, pp. 178-87.
Markwick A, Ansari Z, Sullivan M, Parsons L, McNeil J. (2014). Inequalities in the social
determinants of health of Aboriginal and Torres Strait Islander People: a cross-sectional
population-based study in the Australian state of Victoria. Int J Equity Health. 13(1):91. doi:
10.1186/s12939-014-0091-5.
Malik VS, Pan A, Willett WC, et al. (2013). Sugar-sweetened beverages and weight gain in
children and adults: a systematic review and metaanalysis. Am J Clin Nutr. 98, pp. 1084–102.
Malik VS, Popkin BM, Bray GA, et al. (2010). Sugar-sweetened beverages and risk of
metabolic syndrome and type 2 diabetes: a metaanalysis. Diabetes Care. 33, pp. 2477–83.
Malik VS, Willett WC, Hu FB. (2013). Global obesity: trends, risk factors and policy
implications. Nat Rev Endocrinol. 9(1), pp. 13-27.
NHMRC. (2013). Australian dietary guidelines. Canberra: National Health and Medical
Research Council, 2013. Retrieved from
https://www.nhmrc.gov.au/guidelines-publications/n29-n30-n31-n32-n33-n34. On
31.10.2017.
National Children's Nutrition and Physical Activity Survey (NCNPAS). (2007). The 2007
Australian National Children’s Nutrition and Physical Activity Survey. Retrieved from
https://www.health.gov.au/internet/main/publishing.nsf/Content/8F4516D5FAC0700ACA25
7BF0001E0109/$File/childrens-nut-phys-survey.pdf on 31.10.2017.
Nakkash RT, Alaouie H, Haddad P, El Hajj T, Salem H, Mahfoud Z, Afifi RA. (2012).
Process evaluation of a community-based mental health promotion intervention for refugee
children. Health Educ Res. 27(4), pp. 595-607.
26
guidance for healthy children ages 2 to 11 years. J Acad Nutr Diet. 114(8), pp. 1257-76.
Pampel F C, Krueger, P M, Denney, J T. (2010). Socioeconomic Disparities in Health
Behaviors. Annu Rev Sociol, 36, pp. 349–370.
Petrie, A., and Sabin, C. (2009). Medical Statistics at a Glance. John Wiley & Sons.
Potvin L, Jones CM. (2011). Twenty-five years after the Ottawa Charter: the critical role of
health promotion for public health. Can J Public Health. 102(4), pp. 244-8
Ranjit N, Evans MH, Byrd-Williams C, Evans AE, Hoelscher DM. (2010). Dietary and
activity correlates of sugar-sweetened beverage consumption among adolescents. Pediatrics.
126(4), pp. :e754-761.
Rauba J, Tahir A, Milford B, Toll A, Benedict V, Wang C, Chehab L, Sanborn T. (2017).
Reduction of Sugar-Sweetened Beverage Consumption in Elementary School Students Using
an Educational Curriculum of Beverage Sugar Content. Glob Pediatr Health.
4:2333794X17711778. doi: 10.1177/2333794X17711778.
Roden J, Jarvis L. (2012). Evaluation of the health promotion activities of paediatric nurses:
is the Ottawa Charter for Health Promotion a useful framework? Contemp Nurse. 41(2), pp.
271-84.
Singh GM, Micha R, Khatibzadeh S, et al. (2015). Estimated global, regional, and national
disease burdens related to sugar-sweetened beverage consumption in 2010. Circulation. 132,
pp. 639–66.
Souza RA, Mediano MF, Souza Ade M, Sichieri R. (2013). Reducing the use of sugar in
public schools: a randomized cluster trial. Rev Saude Publica. 47(4), pp. 666-74.
Te Morenga L, Mallard S, Mann J. (2012). Dietary sugars and body weight: systematic
review and meta-analyses of randomised controlled trials and cohort studies. BMJ. 346,
p.e7492.
Zoellner JM, Hedrick VE, You W, Chen Y, Davy BM, Porter KJ, Bailey A, Lane H,
Alexander R, Estabrooks PA. (2016). Effects of a behavioral and health literacy intervention
to reduce sugar-sweetened beverages: a randomized-controlled trial. Int J Behav Nutr Phys
Act. 13:38. doi: 10.1186/s12966-016-0362-1.
Visagie S, Schneider M. (2014). Implementation of the principles of primary health care in a
rural area of South Africa. Afr J Prim Health Care Fam Med. 6(1), pp. E1-E10.
Wallace LM, Brown KE, Hilton S. (2014). Planning for, implementing and assessing the
impact of health promotion and behaviour change interventions: a way forward for health
psychologists. Health Psychol Rev. 8(1), pp. 8-33.
27
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
© 2024 | Zucol Services PVT LTD | All rights reserved.