Global Burden of Disease Theory 2022
VerifiedAdded on 2022/09/18
|15
|4848
|56
AI Summary
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Running Head: Global Burden of Disease 0
Global Burden of Diseases
August 27
2019
Global Burden of Diseases
August 27
2019
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Global Burden of Disease 1
Global Burden of Diseases
Term Global Burden of Diseases is a systematic approach with the scientific efforts in
order to calculate the size of loss in health and its reasons were examined as diseases,
injuries, and risk factors defined under age, sex, and geography. According to the
concept of GBD the number of the deaths can be count for one time (Feigin, and Vos,
2019). In the first step the total numbers of deaths are counted in the whole year (Blyth,
Briggs, Schneider, Hoy, and March, 2019), whereas in the second step the cause of the
death is studied by the researchers in which they choose distinct types of methods.
Apart from comparing and comprehensive vision of the cause of premature death and
disability by the help of GBD different risk factors of the death estimation can be
examined. At present in the era of science and technology it is expected that the
scientists must cooperate with the demand with respect to health services and
resources (Chang, Skirbekk, Tyrovolas, Kassebaum, and Dieleman, 2019). The GBD is
performed so that the diseases with the complex pattern of the diseases and injuries
can be examined. The analysis is conduct on the basis of the incidence, prevalence,
and years lived with disability (YLDs). By the Global non-fatal burden age-
standardization rates are increasing consistently. According to the research it was
examined that due to YLDs premature mortality declines across the spectrum of
development. In order to fulfill the demand the scientists have to focus upon the choices
for the rules and system of health services. The approach of GBD is chosen by many
countries around the world in which Australia, India, Mauritius, Mexico, South Africa,
Thailand, Turkey, United States of America, World Health Organization, etc. are
included (Meier, et.al. , 2019) It is not easy to provide the effective and good quality of
health services to public or population without proper analysis of their symptoms. Before
1990s there was no any method in which comprehensive and comparative methods or
practices were available. Due to this reason the information of burden of diseases,
injuries and risks factors were unable to examine. To overcome from these issues
World Health Organization introduced Study of Global Burden of Disease in year of
1991. The major advantage of this study is that the analysis which is conducted with this
approach is consistent critically available for every condition (Naidoo, et. at., 2019).
1
Global Burden of Diseases
Term Global Burden of Diseases is a systematic approach with the scientific efforts in
order to calculate the size of loss in health and its reasons were examined as diseases,
injuries, and risk factors defined under age, sex, and geography. According to the
concept of GBD the number of the deaths can be count for one time (Feigin, and Vos,
2019). In the first step the total numbers of deaths are counted in the whole year (Blyth,
Briggs, Schneider, Hoy, and March, 2019), whereas in the second step the cause of the
death is studied by the researchers in which they choose distinct types of methods.
Apart from comparing and comprehensive vision of the cause of premature death and
disability by the help of GBD different risk factors of the death estimation can be
examined. At present in the era of science and technology it is expected that the
scientists must cooperate with the demand with respect to health services and
resources (Chang, Skirbekk, Tyrovolas, Kassebaum, and Dieleman, 2019). The GBD is
performed so that the diseases with the complex pattern of the diseases and injuries
can be examined. The analysis is conduct on the basis of the incidence, prevalence,
and years lived with disability (YLDs). By the Global non-fatal burden age-
standardization rates are increasing consistently. According to the research it was
examined that due to YLDs premature mortality declines across the spectrum of
development. In order to fulfill the demand the scientists have to focus upon the choices
for the rules and system of health services. The approach of GBD is chosen by many
countries around the world in which Australia, India, Mauritius, Mexico, South Africa,
Thailand, Turkey, United States of America, World Health Organization, etc. are
included (Meier, et.al. , 2019) It is not easy to provide the effective and good quality of
health services to public or population without proper analysis of their symptoms. Before
1990s there was no any method in which comprehensive and comparative methods or
practices were available. Due to this reason the information of burden of diseases,
injuries and risks factors were unable to examine. To overcome from these issues
World Health Organization introduced Study of Global Burden of Disease in year of
1991. The major advantage of this study is that the analysis which is conducted with this
approach is consistent critically available for every condition (Naidoo, et. at., 2019).
1
Global Burden of Disease 2
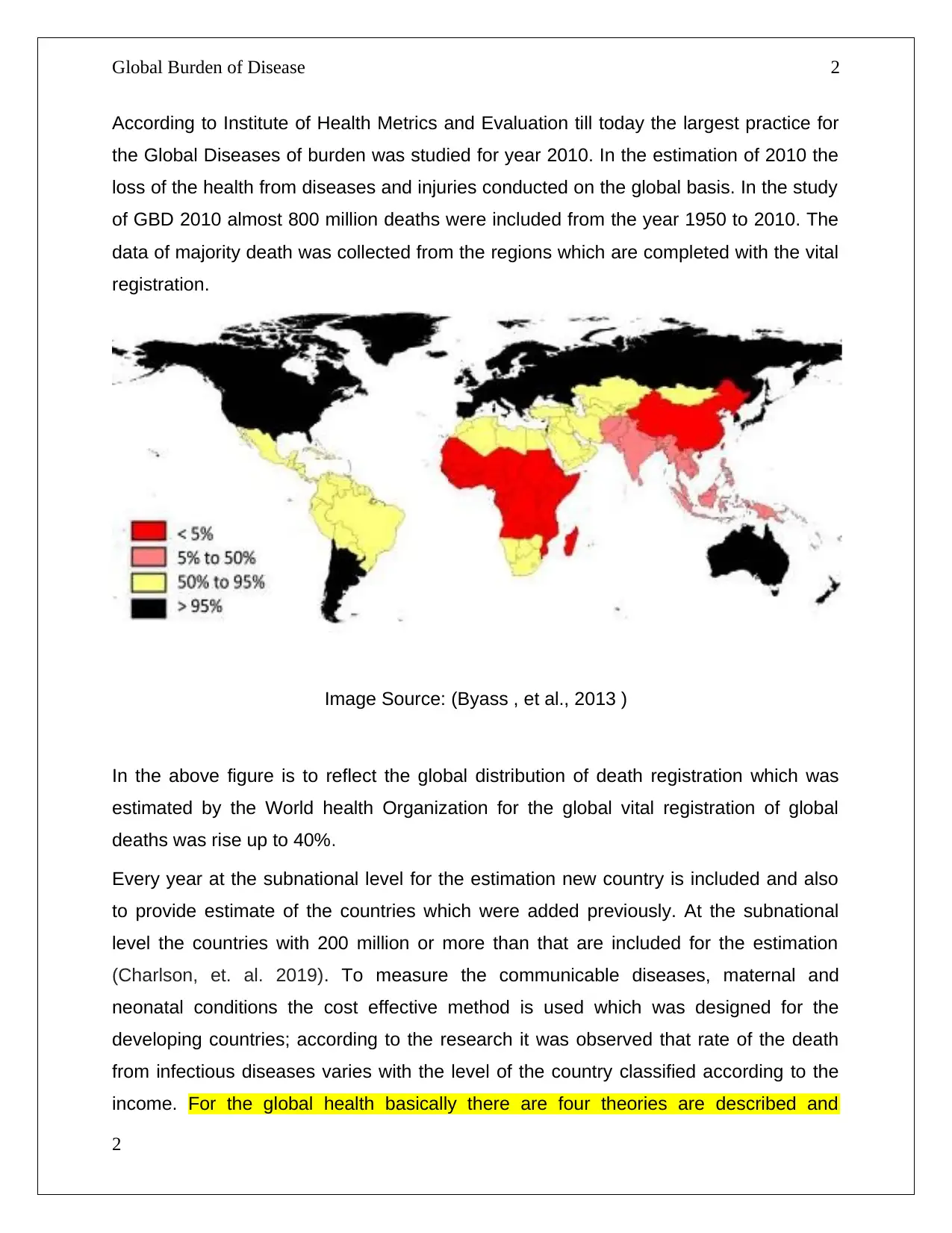
According to Institute of Health Metrics and Evaluation till today the largest practice for
the Global Diseases of burden was studied for year 2010. In the estimation of 2010 the
loss of the health from diseases and injuries conducted on the global basis. In the study
of GBD 2010 almost 800 million deaths were included from the year 1950 to 2010. The
data of majority death was collected from the regions which are completed with the vital
registration.
Image Source: (Byass , et al., 2013 )
In the above figure is to reflect the global distribution of death registration which was
estimated by the World health Organization for the global vital registration of global
deaths was rise up to 40%.
Every year at the subnational level for the estimation new country is included and also
to provide estimate of the countries which were added previously. At the subnational
level the countries with 200 million or more than that are included for the estimation
(Charlson, et. al. 2019). To measure the communicable diseases, maternal and
neonatal conditions the cost effective method is used which was designed for the
developing countries; according to the research it was observed that rate of the death
from infectious diseases varies with the level of the country classified according to the
income. For the global health basically there are four theories are described and
2
According to Institute of Health Metrics and Evaluation till today the largest practice for
the Global Diseases of burden was studied for year 2010. In the estimation of 2010 the
loss of the health from diseases and injuries conducted on the global basis. In the study
of GBD 2010 almost 800 million deaths were included from the year 1950 to 2010. The
data of majority death was collected from the regions which are completed with the vital
registration.
Image Source: (Byass , et al., 2013 )
In the above figure is to reflect the global distribution of death registration which was
estimated by the World health Organization for the global vital registration of global
deaths was rise up to 40%.
Every year at the subnational level for the estimation new country is included and also
to provide estimate of the countries which were added previously. At the subnational
level the countries with 200 million or more than that are included for the estimation
(Charlson, et. al. 2019). To measure the communicable diseases, maternal and
neonatal conditions the cost effective method is used which was designed for the
developing countries; according to the research it was observed that rate of the death
from infectious diseases varies with the level of the country classified according to the
income. For the global health basically there are four theories are described and
2
Global Burden of Disease 3
bunches of problems are explained with these theories. According to the first theory in
which the consequences are explained arises due to social action on the global health.
The theory was proposed by the sociologist Robert Merton in which all the intervention
related to society are included. In the second theory which was explained by the Peter
Berger and Thomas Luckmann reflects about the construction of the society by
considering the reality. While in the third theory which explains about the social suffering
and support through the framework that consists four potentially important implications
in health across the world (Hurwitz, Randhawa, Yu, Côté, and Haldeman, 2018).
In ancient time by analyzing the mortality of any person was the only method to study
the health of people. By the help of this method all the information related to health of
population and the comparison for the effectiveness is not possible to obtain in order to
improve the health. The measures of summaries which are define under Health-
Adjusted Life years are used in the burden of diseases for estimation. For determining
the HALYs generally in three steps it can be performed. In the first step description is
conducted over the associated health state and different condition of diseases. Another
step is used to develop some numerical figures or weighing the health state. In the final
step the values are combined which were observed in the previous step associated with
the health state and estimation of life expectancy. The above step consists of the
methods from which the final attempts can be analyzed with the effects. For the
measurement of HALYs two methods are commonly used which are described as
Quality-Adjusted Life Years (QALY) and Disability Adjusted Life Years (DALY). Term
QALY reflects the results of the health with the statistical values including quality and
quantity measures. By using QALY the estimation of the total year lived by an individual
as well as quality life spent by the same individual can be analyzed. When the
resources are limited QALY is used to identify the need of an intervention which is
known as quantity and quality of life so that area to use the resources can be
determined. Another method DALY designed by World Bank and Harvard University in
1990 to analyze the burden of disease and disability. This method helps to understand
the difference between the health of the population and ideal situation (Rehm, and
Shield, 2019).
3
bunches of problems are explained with these theories. According to the first theory in
which the consequences are explained arises due to social action on the global health.
The theory was proposed by the sociologist Robert Merton in which all the intervention
related to society are included. In the second theory which was explained by the Peter
Berger and Thomas Luckmann reflects about the construction of the society by
considering the reality. While in the third theory which explains about the social suffering
and support through the framework that consists four potentially important implications
in health across the world (Hurwitz, Randhawa, Yu, Côté, and Haldeman, 2018).
In ancient time by analyzing the mortality of any person was the only method to study
the health of people. By the help of this method all the information related to health of
population and the comparison for the effectiveness is not possible to obtain in order to
improve the health. The measures of summaries which are define under Health-
Adjusted Life years are used in the burden of diseases for estimation. For determining
the HALYs generally in three steps it can be performed. In the first step description is
conducted over the associated health state and different condition of diseases. Another
step is used to develop some numerical figures or weighing the health state. In the final
step the values are combined which were observed in the previous step associated with
the health state and estimation of life expectancy. The above step consists of the
methods from which the final attempts can be analyzed with the effects. For the
measurement of HALYs two methods are commonly used which are described as
Quality-Adjusted Life Years (QALY) and Disability Adjusted Life Years (DALY). Term
QALY reflects the results of the health with the statistical values including quality and
quantity measures. By using QALY the estimation of the total year lived by an individual
as well as quality life spent by the same individual can be analyzed. When the
resources are limited QALY is used to identify the need of an intervention which is
known as quantity and quality of life so that area to use the resources can be
determined. Another method DALY designed by World Bank and Harvard University in
1990 to analyze the burden of disease and disability. This method helps to understand
the difference between the health of the population and ideal situation (Rehm, and
Shield, 2019).
3
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Global Burden of Disease 4
DALY= Years of Life lost because of premature mortality (YLL) + Years Live with
disability (YLD)
YLL= N x L; Here N reflects the number of death and L stands for the standard life
expectancy.
The data which is required to calculate the burden of diseases includes Mortality,
Incidence of Diseases, Distribution of Health state, duration of health state, Weight
associated with every state in health. The calculation of the diseases is not easy to deal
and to avoid the issues or challenges the availability of the sources is important. Due to
lack of sources calculation in the burden of diseases for the developing countries is
difficult. To ensure about the data from different sources related with the different
countries are of same quality is one of the biggest challenge. By the help of QALY and
DALY the expectancy of the life can also be analyzed. In the analysis of chronic
diseases where the quality of life can be compromised but the survival of the individual
cannot by using the QALY difficulties can be observed (Caminade, McIntyre, and Jones,
2019). The dimensions on which the QALYs rely are age, context, and responsibilities
connected to the different stages of life due to which to quantify for the preventative
measures is difficult because there would be no any effect on the health outcome in
short-term. However instead of all these disadvantage QALY is the method which is
proffered for the comparison in interventions or across areas of diseases.
The patterns which are discussed here are geographical and demographic pattern
considered. The reasons for the change in the shifting patterns in the global burden of
diseases are Demographic changes and epidemiological changes related to the low
income countries. The low income countries burden of the non-communicable disease
will exceeds to 80% rather than the country with high income countries. With the
increase behavioral risks such as unhealthy diets, use of tobacco, and infectious
diseases get reduces rises in the countries of low income (Pishgar, et. al. 2018).
Increasing population at the same time amplifies the rate of increase in the shifting of
communicable diseases to non-communicable disease. The reduction in the fertility is
increase in the low income countries such as Bangladesh and Botswana. Due to this
4
DALY= Years of Life lost because of premature mortality (YLL) + Years Live with
disability (YLD)
YLL= N x L; Here N reflects the number of death and L stands for the standard life
expectancy.
The data which is required to calculate the burden of diseases includes Mortality,
Incidence of Diseases, Distribution of Health state, duration of health state, Weight
associated with every state in health. The calculation of the diseases is not easy to deal
and to avoid the issues or challenges the availability of the sources is important. Due to
lack of sources calculation in the burden of diseases for the developing countries is
difficult. To ensure about the data from different sources related with the different
countries are of same quality is one of the biggest challenge. By the help of QALY and
DALY the expectancy of the life can also be analyzed. In the analysis of chronic
diseases where the quality of life can be compromised but the survival of the individual
cannot by using the QALY difficulties can be observed (Caminade, McIntyre, and Jones,
2019). The dimensions on which the QALYs rely are age, context, and responsibilities
connected to the different stages of life due to which to quantify for the preventative
measures is difficult because there would be no any effect on the health outcome in
short-term. However instead of all these disadvantage QALY is the method which is
proffered for the comparison in interventions or across areas of diseases.
The patterns which are discussed here are geographical and demographic pattern
considered. The reasons for the change in the shifting patterns in the global burden of
diseases are Demographic changes and epidemiological changes related to the low
income countries. The low income countries burden of the non-communicable disease
will exceeds to 80% rather than the country with high income countries. With the
increase behavioral risks such as unhealthy diets, use of tobacco, and infectious
diseases get reduces rises in the countries of low income (Pishgar, et. al. 2018).
Increasing population at the same time amplifies the rate of increase in the shifting of
communicable diseases to non-communicable disease. The reduction in the fertility is
increase in the low income countries such as Bangladesh and Botswana. Due to this
4
Global Burden of Disease 5
reason the median age from year 1980-2015 increased from 17 years to 24 years
hence the number of the adults in the country also increases in the low income
countries so the burden of the non-communicable disease affects them
disproportionately (Zhou, et. al., 2019). In such countries the focus of the health care
system is based upon the acute care of the patients who are infected with the maternal
and neonatal diseases instead of providing the chronic treatments which is required for
the non-communicable disease. The health care system of the low income countries is
affected due to low or poor funding from the end of the government, on an average the
government in such countries invests 23 dollars on per person annually (Rieger,
Wagner, Mebratie, Alemu, and Bedi, 2019). It is very low in comparison to country with
the high income such as USA and UK where the government provides funding for per
person is 3860 dollars and 2695 dollars respectively. In the country with low and lower-
middle income the health facility and services are mostly purchased out of the pocket or
from donors. According to the study of year 2014 it was observed that in such countries
29.1% of the funding of the health was out of the pocket while 35.7% was financed by
the donors. For the poor households the medical services become expensive or
unavailable which were not available by the financing from the donors and insurance
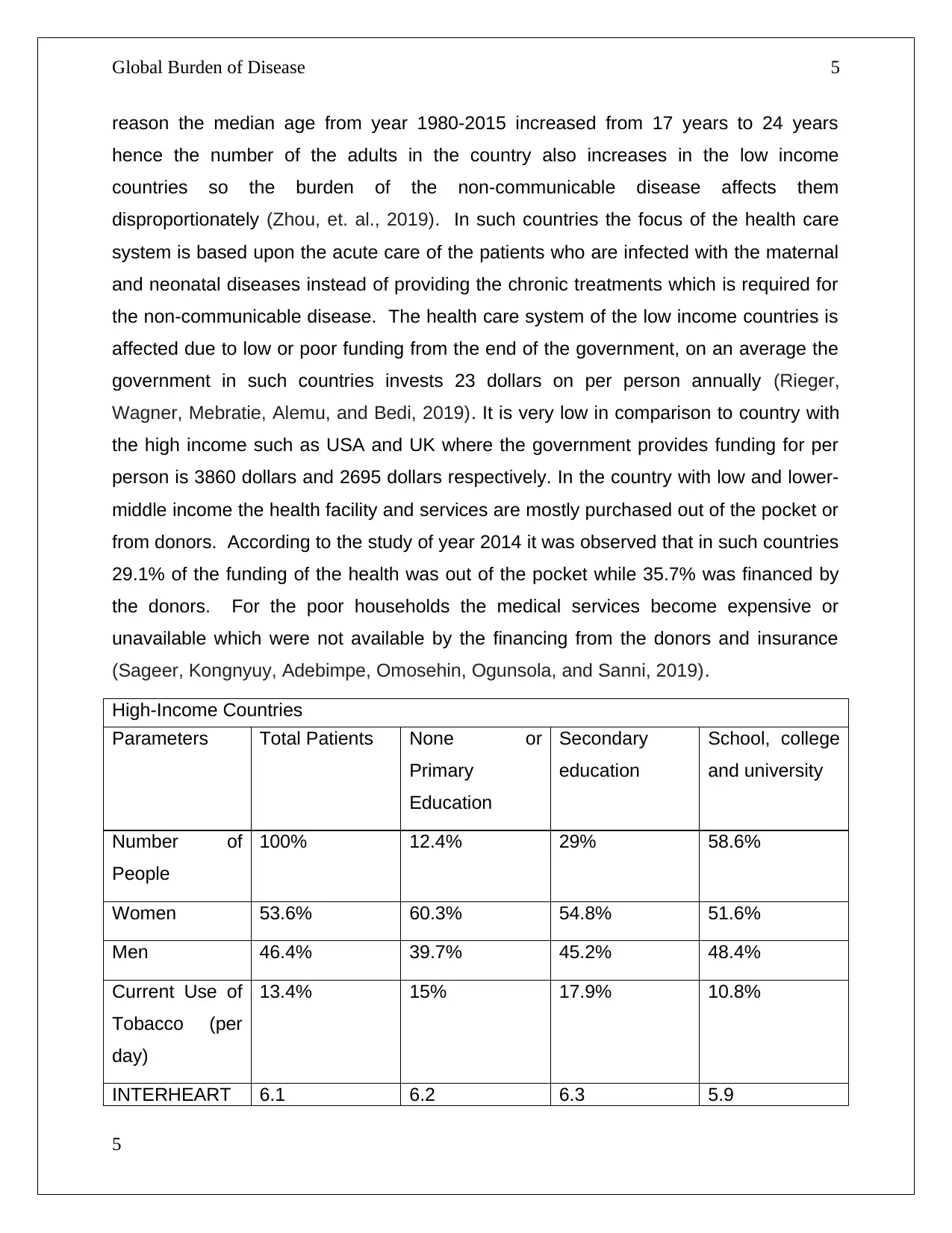
(Sageer, Kongnyuy, Adebimpe, Omosehin, Ogunsola, and Sanni, 2019).
High-Income Countries
Parameters Total Patients None or
Primary
Education
Secondary
education
School, college
and university
Number of
People
100% 12.4% 29% 58.6%
Women 53.6% 60.3% 54.8% 51.6%
Men 46.4% 39.7% 45.2% 48.4%
Current Use of
Tobacco (per
day)
13.4% 15% 17.9% 10.8%
INTERHEART 6.1 6.2 6.3 5.9
5
reason the median age from year 1980-2015 increased from 17 years to 24 years
hence the number of the adults in the country also increases in the low income
countries so the burden of the non-communicable disease affects them
disproportionately (Zhou, et. al., 2019). In such countries the focus of the health care
system is based upon the acute care of the patients who are infected with the maternal
and neonatal diseases instead of providing the chronic treatments which is required for
the non-communicable disease. The health care system of the low income countries is
affected due to low or poor funding from the end of the government, on an average the
government in such countries invests 23 dollars on per person annually (Rieger,
Wagner, Mebratie, Alemu, and Bedi, 2019). It is very low in comparison to country with
the high income such as USA and UK where the government provides funding for per
person is 3860 dollars and 2695 dollars respectively. In the country with low and lower-
middle income the health facility and services are mostly purchased out of the pocket or
from donors. According to the study of year 2014 it was observed that in such countries
29.1% of the funding of the health was out of the pocket while 35.7% was financed by
the donors. For the poor households the medical services become expensive or
unavailable which were not available by the financing from the donors and insurance
(Sageer, Kongnyuy, Adebimpe, Omosehin, Ogunsola, and Sanni, 2019).
High-Income Countries
Parameters Total Patients None or
Primary
Education
Secondary
education
School, college
and university
Number of
People
100% 12.4% 29% 58.6%
Women 53.6% 60.3% 54.8% 51.6%
Men 46.4% 39.7% 45.2% 48.4%
Current Use of
Tobacco (per
day)
13.4% 15% 17.9% 10.8%
INTERHEART 6.1 6.2 6.3 5.9
5
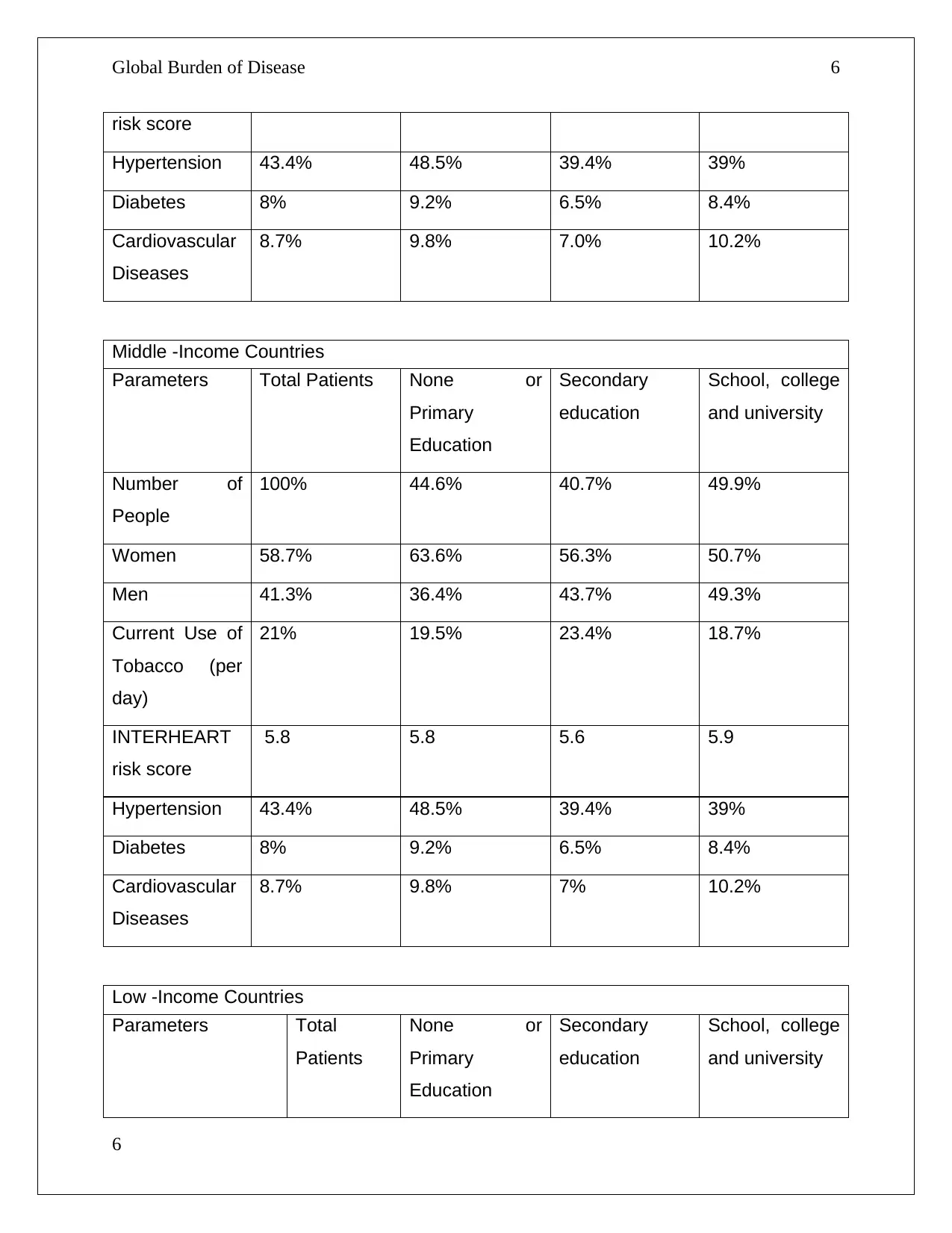
Global Burden of Disease 6
risk score
Hypertension 43.4% 48.5% 39.4% 39%
Diabetes 8% 9.2% 6.5% 8.4%
Cardiovascular
Diseases
8.7% 9.8% 7.0% 10.2%
Middle -Income Countries
Parameters Total Patients None or
Primary
Education
Secondary
education
School, college
and university
Number of
People
100% 44.6% 40.7% 49.9%
Women 58.7% 63.6% 56.3% 50.7%
Men 41.3% 36.4% 43.7% 49.3%
Current Use of
Tobacco (per
day)
21% 19.5% 23.4% 18.7%
INTERHEART
risk score
5.8 5.8 5.6 5.9
Hypertension 43.4% 48.5% 39.4% 39%
Diabetes 8% 9.2% 6.5% 8.4%
Cardiovascular
Diseases
8.7% 9.8% 7% 10.2%
Low -Income Countries
Parameters Total
Patients
None or
Primary
Education
Secondary
education
School, college
and university
6
risk score
Hypertension 43.4% 48.5% 39.4% 39%
Diabetes 8% 9.2% 6.5% 8.4%
Cardiovascular
Diseases
8.7% 9.8% 7.0% 10.2%
Middle -Income Countries
Parameters Total Patients None or
Primary
Education
Secondary
education
School, college
and university
Number of
People
100% 44.6% 40.7% 49.9%
Women 58.7% 63.6% 56.3% 50.7%
Men 41.3% 36.4% 43.7% 49.3%
Current Use of
Tobacco (per
day)
21% 19.5% 23.4% 18.7%
INTERHEART
risk score
5.8 5.8 5.6 5.9
Hypertension 43.4% 48.5% 39.4% 39%
Diabetes 8% 9.2% 6.5% 8.4%
Cardiovascular
Diseases
8.7% 9.8% 7% 10.2%
Low -Income Countries
Parameters Total
Patients
None or
Primary
Education
Secondary
education
School, college
and university
6
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
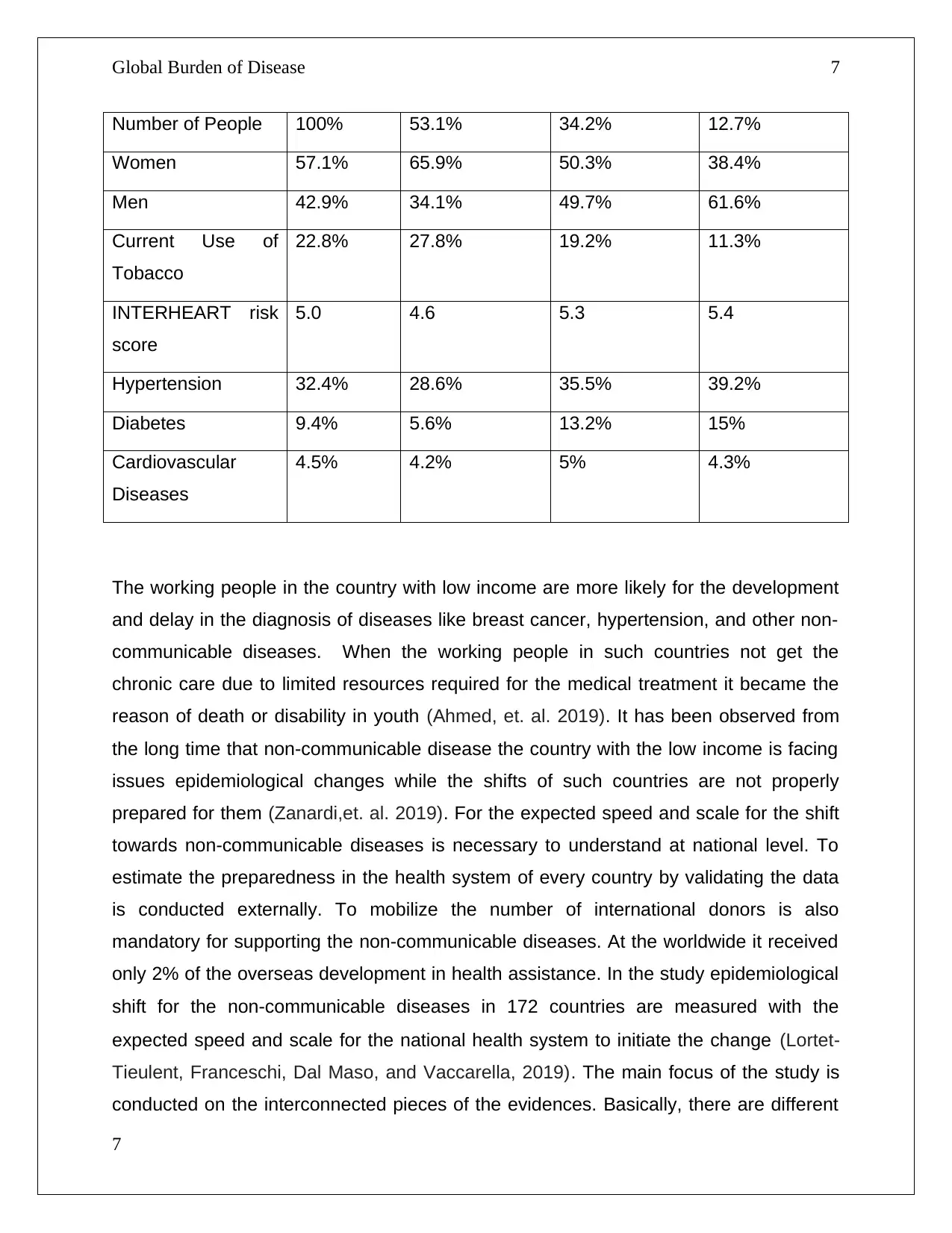
Global Burden of Disease 7
Number of People 100% 53.1% 34.2% 12.7%
Women 57.1% 65.9% 50.3% 38.4%
Men 42.9% 34.1% 49.7% 61.6%
Current Use of
Tobacco
22.8% 27.8% 19.2% 11.3%
INTERHEART risk
score
5.0 4.6 5.3 5.4
Hypertension 32.4% 28.6% 35.5% 39.2%
Diabetes 9.4% 5.6% 13.2% 15%
Cardiovascular
Diseases
4.5% 4.2% 5% 4.3%
The working people in the country with low income are more likely for the development
and delay in the diagnosis of diseases like breast cancer, hypertension, and other non-
communicable diseases. When the working people in such countries not get the
chronic care due to limited resources required for the medical treatment it became the
reason of death or disability in youth (Ahmed, et. al. 2019). It has been observed from
the long time that non-communicable disease the country with the low income is facing
issues epidemiological changes while the shifts of such countries are not properly
prepared for them (Zanardi,et. al. 2019). For the expected speed and scale for the shift
towards non-communicable diseases is necessary to understand at national level. To
estimate the preparedness in the health system of every country by validating the data
is conducted externally. To mobilize the number of international donors is also
mandatory for supporting the non-communicable diseases. At the worldwide it received
only 2% of the overseas development in health assistance. In the study epidemiological
shift for the non-communicable diseases in 172 countries are measured with the
expected speed and scale for the national health system to initiate the change (Lortet‐
Tieulent, Franceschi, Dal Maso, and Vaccarella, 2019). The main focus of the study is
conducted on the interconnected pieces of the evidences. Basically, there are different
7
Number of People 100% 53.1% 34.2% 12.7%
Women 57.1% 65.9% 50.3% 38.4%
Men 42.9% 34.1% 49.7% 61.6%
Current Use of
Tobacco
22.8% 27.8% 19.2% 11.3%
INTERHEART risk
score
5.0 4.6 5.3 5.4
Hypertension 32.4% 28.6% 35.5% 39.2%
Diabetes 9.4% 5.6% 13.2% 15%
Cardiovascular
Diseases
4.5% 4.2% 5% 4.3%
The working people in the country with low income are more likely for the development
and delay in the diagnosis of diseases like breast cancer, hypertension, and other non-
communicable diseases. When the working people in such countries not get the
chronic care due to limited resources required for the medical treatment it became the
reason of death or disability in youth (Ahmed, et. al. 2019). It has been observed from
the long time that non-communicable disease the country with the low income is facing
issues epidemiological changes while the shifts of such countries are not properly
prepared for them (Zanardi,et. al. 2019). For the expected speed and scale for the shift
towards non-communicable diseases is necessary to understand at national level. To
estimate the preparedness in the health system of every country by validating the data
is conducted externally. To mobilize the number of international donors is also
mandatory for supporting the non-communicable diseases. At the worldwide it received
only 2% of the overseas development in health assistance. In the study epidemiological
shift for the non-communicable diseases in 172 countries are measured with the
expected speed and scale for the national health system to initiate the change (Lortet‐
Tieulent, Franceschi, Dal Maso, and Vaccarella, 2019). The main focus of the study is
conducted on the interconnected pieces of the evidences. Basically, there are different
7
Global Burden of Disease 8
patterns exits between high, middle and low income countries. The chronic diseases
such as heart diseases and cancer are one of the most important risk factor. It is
identified that tobacco is one of the leading reason for both diseases in which 11% are
found as burden of diseases and 18% deaths in the high income countries. In the high
income countries other risk factors like alcohol, over weight and blood pressure found
as causes of lost year in healthy life; each factor affect the 6-7% of the total. In the
countries with middle income chronic diseases are the risk factors contributes in the
major reasons of death. Relatively in the low income countries there are less risk factor
are responsible for the death of people and loss in health year. Underweight is one the
major risk factor which is found as 10% of total burden of disease (Gibb, et. al. 2019).
In the demographic pattern the risk factors which are considered by age for burden of
diseases. These risks are underweight, under nutrition, unsafe water, smoke which
originates by the household usage of solid fuels and change in the climate. At older
ages chronic diseases such as cardiovascular disease and cancer are the reason in
most of the health burden of risk factors (Diao, McMillan, and Rodrik, 2019). The risks
which are associated with the diet both men and women are equally affected, in which
environment and unsafe sex plays role. If the addictive things are considered then it is
found that 75% of men are suffering from burden of diseases. In women the 80%
reason of the death is deficiency of iron also they are found to suffer from contraception
(Mokdad, et.al. 2019).
8
patterns exits between high, middle and low income countries. The chronic diseases
such as heart diseases and cancer are one of the most important risk factor. It is
identified that tobacco is one of the leading reason for both diseases in which 11% are
found as burden of diseases and 18% deaths in the high income countries. In the high
income countries other risk factors like alcohol, over weight and blood pressure found
as causes of lost year in healthy life; each factor affect the 6-7% of the total. In the
countries with middle income chronic diseases are the risk factors contributes in the
major reasons of death. Relatively in the low income countries there are less risk factor
are responsible for the death of people and loss in health year. Underweight is one the
major risk factor which is found as 10% of total burden of disease (Gibb, et. al. 2019).
In the demographic pattern the risk factors which are considered by age for burden of
diseases. These risks are underweight, under nutrition, unsafe water, smoke which
originates by the household usage of solid fuels and change in the climate. At older
ages chronic diseases such as cardiovascular disease and cancer are the reason in
most of the health burden of risk factors (Diao, McMillan, and Rodrik, 2019). The risks
which are associated with the diet both men and women are equally affected, in which
environment and unsafe sex plays role. If the addictive things are considered then it is
found that 75% of men are suffering from burden of diseases. In women the 80%
reason of the death is deficiency of iron also they are found to suffer from contraception
(Mokdad, et.al. 2019).
8
Global Burden of Disease 9
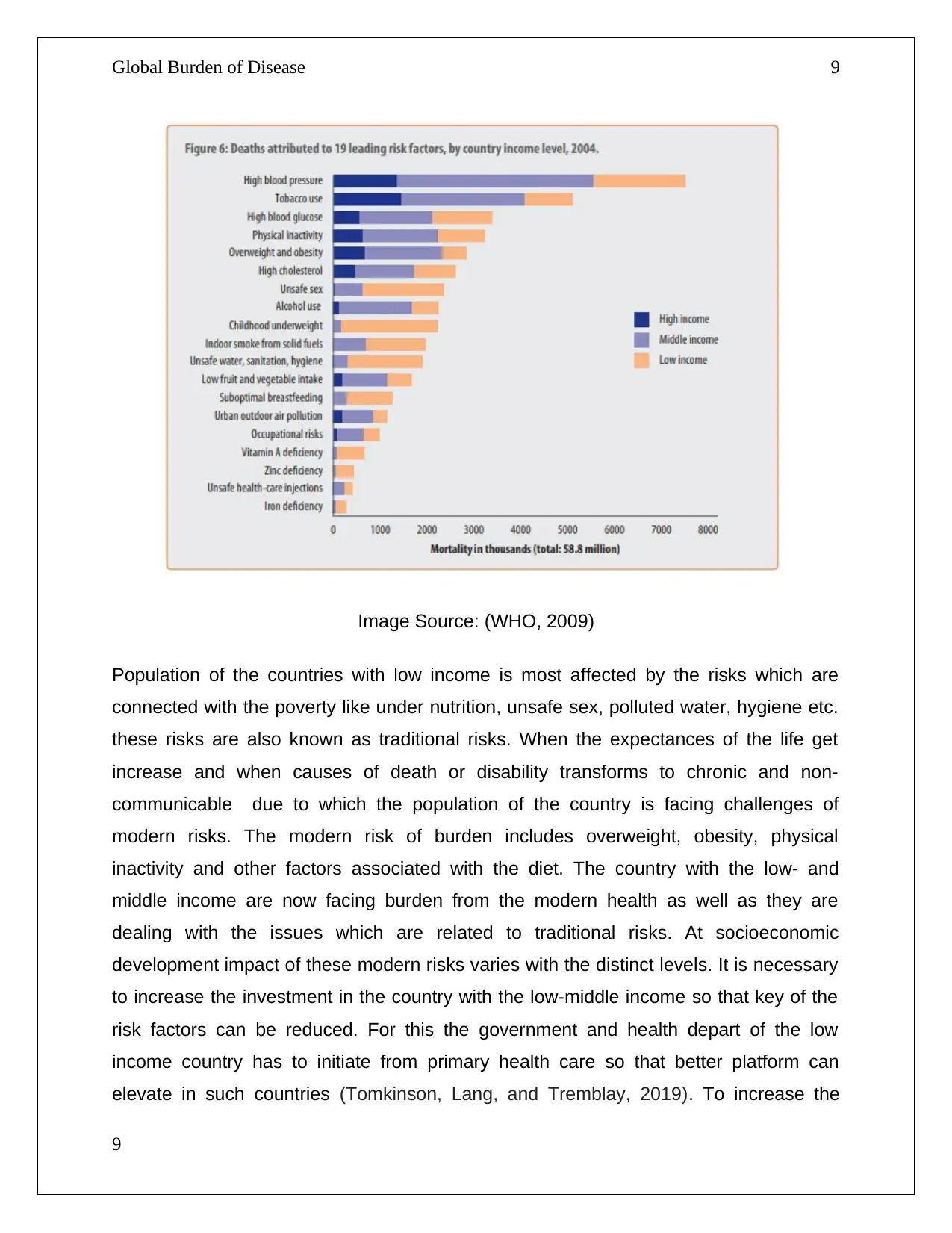
Image Source: (WHO, 2009)
Population of the countries with low income is most affected by the risks which are
connected with the poverty like under nutrition, unsafe sex, polluted water, hygiene etc.
these risks are also known as traditional risks. When the expectances of the life get
increase and when causes of death or disability transforms to chronic and non-
communicable due to which the population of the country is facing challenges of
modern risks. The modern risk of burden includes overweight, obesity, physical
inactivity and other factors associated with the diet. The country with the low- and
middle income are now facing burden from the modern health as well as they are
dealing with the issues which are related to traditional risks. At socioeconomic
development impact of these modern risks varies with the distinct levels. It is necessary
to increase the investment in the country with the low-middle income so that key of the
risk factors can be reduced. For this the government and health depart of the low
income country has to initiate from primary health care so that better platform can
elevate in such countries (Tomkinson, Lang, and Tremblay, 2019). To increase the
9
Image Source: (WHO, 2009)
Population of the countries with low income is most affected by the risks which are
connected with the poverty like under nutrition, unsafe sex, polluted water, hygiene etc.
these risks are also known as traditional risks. When the expectances of the life get
increase and when causes of death or disability transforms to chronic and non-
communicable due to which the population of the country is facing challenges of
modern risks. The modern risk of burden includes overweight, obesity, physical
inactivity and other factors associated with the diet. The country with the low- and
middle income are now facing burden from the modern health as well as they are
dealing with the issues which are related to traditional risks. At socioeconomic
development impact of these modern risks varies with the distinct levels. It is necessary
to increase the investment in the country with the low-middle income so that key of the
risk factors can be reduced. For this the government and health depart of the low
income country has to initiate from primary health care so that better platform can
elevate in such countries (Tomkinson, Lang, and Tremblay, 2019). To increase the
9
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Global Burden of Disease 10
resources is also mandatory for the low income nations so that the governance of the
country can provide the better facilities and support their health system. In these
countries the major deaths and disability are caused due to non-communicable
diseases but funding is very less which is based upon the income of their traditional
trends. For the epidemiological changes the world is the center point; the level of the
development in the countries is increasing with the time due to which the burden of the
communicable diseases is decreased while the expectancies of the people for their life
is also rising. However, by the development there are many positive changes can be
seen but the risk factors get worse.
The implications which were examined due to change in the pattern in global burden of
disease are discussed in the essay. For the health research and to making decision
about the investment in the health system and its interventions by the national and local
government through limited resources. The demand for the health care facilities and
services is increasing rapidly and constantly. Basically the three main uses of the study
of the GBD are that it is designed to compare the health of the people across the world
for a particular interval of time. Another use of the study is to help in understanding the
diseases and injuries which is responsible for the poor health for any specific
community, place or country. It is also can used to analyze the situation of their country
is improving or it is getting worse with the change in time. The other aim of the study is
to assess the information which is missing from the resources. Every individual can
understand whenever he/she is not well or not healthy also there are no methods are
available which can describe the specific reason of human health or the population
which is affected by the illness or any diseases. The method which explains about the
number of death is used to measure or to examine the health of people or any
community (Aizenman, Jinjarak, Nguyen, and Park, 2019).
The causes of the burden are transforming from the communicable disease to non-
communicable diseases. As it was observed in the study of 2015 the communicable
diseases were reason of the death of fewer people in which low respiratory infection,
diarrheal diseases, malaria and NTDs were included (Ryan, Carlson, Mordecai, and
Johnson, 2019). In the same year risk factors like Alzheimer’s disease, hypertensive
heart disease and other cancers were observed in as non-communicable disease. To
10
resources is also mandatory for the low income nations so that the governance of the
country can provide the better facilities and support their health system. In these
countries the major deaths and disability are caused due to non-communicable
diseases but funding is very less which is based upon the income of their traditional
trends. For the epidemiological changes the world is the center point; the level of the
development in the countries is increasing with the time due to which the burden of the
communicable diseases is decreased while the expectancies of the people for their life
is also rising. However, by the development there are many positive changes can be
seen but the risk factors get worse.
The implications which were examined due to change in the pattern in global burden of
disease are discussed in the essay. For the health research and to making decision
about the investment in the health system and its interventions by the national and local
government through limited resources. The demand for the health care facilities and
services is increasing rapidly and constantly. Basically the three main uses of the study
of the GBD are that it is designed to compare the health of the people across the world
for a particular interval of time. Another use of the study is to help in understanding the
diseases and injuries which is responsible for the poor health for any specific
community, place or country. It is also can used to analyze the situation of their country
is improving or it is getting worse with the change in time. The other aim of the study is
to assess the information which is missing from the resources. Every individual can
understand whenever he/she is not well or not healthy also there are no methods are
available which can describe the specific reason of human health or the population
which is affected by the illness or any diseases. The method which explains about the
number of death is used to measure or to examine the health of people or any
community (Aizenman, Jinjarak, Nguyen, and Park, 2019).
The causes of the burden are transforming from the communicable disease to non-
communicable diseases. As it was observed in the study of 2015 the communicable
diseases were reason of the death of fewer people in which low respiratory infection,
diarrheal diseases, malaria and NTDs were included (Ryan, Carlson, Mordecai, and
Johnson, 2019). In the same year risk factors like Alzheimer’s disease, hypertensive
heart disease and other cancers were observed in as non-communicable disease. To
10
Global Burden of Disease 11
inform policy making risk factors and burden of disease are useful in the projection of
future. By the help of current methods to analyze the burden of diseases for any
category is possible. To reduce the major projected reasons of burden the key
challenges arise by increasing the allocative and efficiency associated with technology
of the health system. For the developed countries like United States there is a strong
case for the investment in the health research in order to reduce the reasons of burden
of diseases which cannot be treated or prevented according to the health delivery
system globally and at national leve (Dolan, et.al., 2019)
11
inform policy making risk factors and burden of disease are useful in the projection of
future. By the help of current methods to analyze the burden of diseases for any
category is possible. To reduce the major projected reasons of burden the key
challenges arise by increasing the allocative and efficiency associated with technology
of the health system. For the developed countries like United States there is a strong
case for the investment in the health research in order to reduce the reasons of burden
of diseases which cannot be treated or prevented according to the health delivery
system globally and at national leve (Dolan, et.al., 2019)
11
Global Burden of Disease 12
Reference
Ahmed, S., Tholandi, M., Pedrana, A., Zazri, A., Parmawaty, N., Rahmanto, A. and Sethi, R., 2019.
Changes in obstetric case fatality and early newborn mortality rates in hospitals after the implementation
of the Expanding Maternal and Neonatal Survival program in Indonesia: Results from a health information
system. International Journal of Gynecology & Obstetrics, 144, pp.13-20.
Aizenman, J., Jinjarak, Y., Nguyen, H.T.K. and Park, D., 2019. Fiscal space and government-spending
and tax-rate cyclicality patterns: A cross-country comparison, 1960–2016. Journal of
Macroeconomics, 60, pp.229-252.
Blyth, F.M., Briggs, A.M., Schneider, C.H., Hoy, D.G. and March, L.M., 2019. The Global Burden of
Musculoskeletal Pain—Where to From Here?. American journal of public health, 109(1), pp.35-40.
Caminade, C., McIntyre, K.M. and Jones, A.E., 2019. Impact of recent and future climate change on
vector‐borne diseases. Annals of the New York Academy of Sciences, 1436(1), p.157.
Chang, A.Y., Skirbekk, V.F., Tyrovolas, S., Kassebaum, N.J. and Dieleman, J.L., 2019. Measuring
population ageing: an analysis of the Global Burden of Disease Study 2017. The Lancet Public
Health, 4(3), pp.e159-e167.
Charlson, F.J., Ferrari, A.J., Santomauro, D.F., Diminic, S., Stockings, E., Scott, J.G., McGrath, J.J. and
Whiteford, H.A., 2018. Global epidemiology and burden of schizophrenia: findings from the global burden
of disease study 2016. Schizophrenia bulletin, 44(6), pp.1195-1203.
Diao, X., McMillan, M. and Rodrik, D., 2019. The recent growth boom in developing economies: A
structural-change perspective. In The Palgrave Handbook of Development Economics, pp. 281-334.
Dolan, C.B., BenYishay, A., Grépin, K.A., Tanner, J.C., Kimmel, A.D., Wheeler, D.C. and McCord, G.C.,
2019. The impact of an insecticide treated bednet campaign on all-cause child mortality: A geospatial
impact evaluation from the Democratic Republic of Congo. PloS one, 14(2), p.e0212890.
Feigin, V.L. and Vos, T., 2019. Global burden of neurological disorders: from global burden of disease
estimates to actions. Neuroepidemiology, 52(1-2), pp.1-2.
Ferlay, J., Colombet, M., Soerjomataram, I., Mathers, C., Parkin, D.M., Piñeros, M., Znaor, A. and Bray,
F., 2019. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and
methods. International journal of cancer, 144(8), pp.1941-1953.
Gibb, H.J., Barchowsky, A., Bellinger, D., Bolger, P.M., Carrington, C., Havelaar, A.H., Oberoi, S., Zang,
Y., O’Leary, K. and Devleesschauwer, B., 2019. Estimates of the 2015 global and regional disease
burden from four foodborne metals–arsenic, cadmium, lead and methylmercury. Environmental
research, 174, pp.188-194.
12
Reference
Ahmed, S., Tholandi, M., Pedrana, A., Zazri, A., Parmawaty, N., Rahmanto, A. and Sethi, R., 2019.
Changes in obstetric case fatality and early newborn mortality rates in hospitals after the implementation
of the Expanding Maternal and Neonatal Survival program in Indonesia: Results from a health information
system. International Journal of Gynecology & Obstetrics, 144, pp.13-20.
Aizenman, J., Jinjarak, Y., Nguyen, H.T.K. and Park, D., 2019. Fiscal space and government-spending
and tax-rate cyclicality patterns: A cross-country comparison, 1960–2016. Journal of
Macroeconomics, 60, pp.229-252.
Blyth, F.M., Briggs, A.M., Schneider, C.H., Hoy, D.G. and March, L.M., 2019. The Global Burden of
Musculoskeletal Pain—Where to From Here?. American journal of public health, 109(1), pp.35-40.
Caminade, C., McIntyre, K.M. and Jones, A.E., 2019. Impact of recent and future climate change on
vector‐borne diseases. Annals of the New York Academy of Sciences, 1436(1), p.157.
Chang, A.Y., Skirbekk, V.F., Tyrovolas, S., Kassebaum, N.J. and Dieleman, J.L., 2019. Measuring
population ageing: an analysis of the Global Burden of Disease Study 2017. The Lancet Public
Health, 4(3), pp.e159-e167.
Charlson, F.J., Ferrari, A.J., Santomauro, D.F., Diminic, S., Stockings, E., Scott, J.G., McGrath, J.J. and
Whiteford, H.A., 2018. Global epidemiology and burden of schizophrenia: findings from the global burden
of disease study 2016. Schizophrenia bulletin, 44(6), pp.1195-1203.
Diao, X., McMillan, M. and Rodrik, D., 2019. The recent growth boom in developing economies: A
structural-change perspective. In The Palgrave Handbook of Development Economics, pp. 281-334.
Dolan, C.B., BenYishay, A., Grépin, K.A., Tanner, J.C., Kimmel, A.D., Wheeler, D.C. and McCord, G.C.,
2019. The impact of an insecticide treated bednet campaign on all-cause child mortality: A geospatial
impact evaluation from the Democratic Republic of Congo. PloS one, 14(2), p.e0212890.
Feigin, V.L. and Vos, T., 2019. Global burden of neurological disorders: from global burden of disease
estimates to actions. Neuroepidemiology, 52(1-2), pp.1-2.
Ferlay, J., Colombet, M., Soerjomataram, I., Mathers, C., Parkin, D.M., Piñeros, M., Znaor, A. and Bray,
F., 2019. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and
methods. International journal of cancer, 144(8), pp.1941-1953.
Gibb, H.J., Barchowsky, A., Bellinger, D., Bolger, P.M., Carrington, C., Havelaar, A.H., Oberoi, S., Zang,
Y., O’Leary, K. and Devleesschauwer, B., 2019. Estimates of the 2015 global and regional disease
burden from four foodborne metals–arsenic, cadmium, lead and methylmercury. Environmental
research, 174, pp.188-194.
12
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Global Burden of Disease 13
Hurwitz, E.L., Randhawa, K., Yu, H., Côté, P. and Haldeman, S., 2018. The Global Spine Care Initiative:
a summary of the global burden of low back and neck pain studies. European Spine Journal, 27(6),
pp.796-801.
Lortet‐Tieulent, J., Franceschi, S., Dal Maso, L. and Vaccarella, S., 2019. Thyroid cancer “epidemic” also
occurs in low‐and middle‐income countries. International journal of cancer, 144(9), pp.2082-2087.
Meier, T., Gräfe, K., Senn, F., Sur, P., Stangl, G.I., Dawczynski, C., März, W., Kleber, M.E. and
Lorkowski, S., 2019. Cardiovascular mortality attributable to dietary risk factors in 51 countries in the
WHO European Region from 1990 to 2016: a systematic analysis of the Global Burden of Disease
Study. European journal of epidemiology, 34(1), pp.37-55.
Mokdad, A.H., Mensah, G.A., Krish, V., Glenn, S.D., Miller-Petrie, M.K., Lopez, A.D. and Murray, C.J.,
2019. Global, regional, national, and subnational big data to inform health equity research: perspectives
from the Global Burden of Disease Study 2017. Ethnicity & disease, 29(Suppl 1), pp.159-172.
Naidoo, K.S., Fricke, T.R., Frick, K.D., Jong, M., Naduvilath, T.J., Resnikoff, S. and Sankaridurg, P.,
2019. Potential lost productivity resulting from the global burden of myopia: Systematic review, meta-
analysis, and modeling. Ophthalmology, 126(3), pp.338-346.
Pishgar, F., Ebrahimi, H., Moghaddam, S.S., Fitzmaurice, C. and Amini, E., 2018. Global, regional and
national burden of prostate cancer, 1990 to 2015: results from the global burden of disease study
2015. The Journal of urology, 199(5), pp.1224-1232.
Rehm, J. and Shield, K.D., 2019. Global Burden of Disease and the Impact of Mental and Addictive
Disorders. Current psychiatry reports, 21(2), p.10.
Rieger, M., Wagner, N., Mebratie, A., Alemu, G. and Bedi, A., 2019. The impact of the Ethiopian health
extension program and health development army on maternal mortality: A synthetic control
approach. Social Science & Medicine, 232, pp.374-381.
Ryan, S.J., Carlson, C.J., Mordecai, E.A. and Johnson, L.R., 2019. Global expansion and redistribution of
Aedes-borne virus transmission risk with climate change. PLoS neglected tropical diseases, 13(3),
p.e0007213.
Sageer, R., Kongnyuy, E., Adebimpe, W.O., Omosehin, O., Ogunsola, E.A. and Sanni, B., 2019. Causes
and contributory factors of maternal mortality: evidence from maternal and perinatal death surveillance
and response in Ogun state, Southwest Nigeria. BMC pregnancy and childbirth, 19(1), p.63.
Tomkinson, G.R., Lang, J.J. and Tremblay, M.S., 2019. Temporal trends in the cardiorespiratory fitness of
children and adolescents representing 19 high-income and upper middle-income countries between 1981
and 2014. Br J Sports Med, 53(8), pp.478-486.
Zanardi, D.M., Parpinelli, M.A., Haddad, S.M., Costa, M.L., Sousa, M.H., Leite, D.F. and Cecatti, J.G.,
2019. Adverse perinatal outcomes are associated with severe maternal morbidity and mortality: evidence
13
Hurwitz, E.L., Randhawa, K., Yu, H., Côté, P. and Haldeman, S., 2018. The Global Spine Care Initiative:
a summary of the global burden of low back and neck pain studies. European Spine Journal, 27(6),
pp.796-801.
Lortet‐Tieulent, J., Franceschi, S., Dal Maso, L. and Vaccarella, S., 2019. Thyroid cancer “epidemic” also
occurs in low‐and middle‐income countries. International journal of cancer, 144(9), pp.2082-2087.
Meier, T., Gräfe, K., Senn, F., Sur, P., Stangl, G.I., Dawczynski, C., März, W., Kleber, M.E. and
Lorkowski, S., 2019. Cardiovascular mortality attributable to dietary risk factors in 51 countries in the
WHO European Region from 1990 to 2016: a systematic analysis of the Global Burden of Disease
Study. European journal of epidemiology, 34(1), pp.37-55.
Mokdad, A.H., Mensah, G.A., Krish, V., Glenn, S.D., Miller-Petrie, M.K., Lopez, A.D. and Murray, C.J.,
2019. Global, regional, national, and subnational big data to inform health equity research: perspectives
from the Global Burden of Disease Study 2017. Ethnicity & disease, 29(Suppl 1), pp.159-172.
Naidoo, K.S., Fricke, T.R., Frick, K.D., Jong, M., Naduvilath, T.J., Resnikoff, S. and Sankaridurg, P.,
2019. Potential lost productivity resulting from the global burden of myopia: Systematic review, meta-
analysis, and modeling. Ophthalmology, 126(3), pp.338-346.
Pishgar, F., Ebrahimi, H., Moghaddam, S.S., Fitzmaurice, C. and Amini, E., 2018. Global, regional and
national burden of prostate cancer, 1990 to 2015: results from the global burden of disease study
2015. The Journal of urology, 199(5), pp.1224-1232.
Rehm, J. and Shield, K.D., 2019. Global Burden of Disease and the Impact of Mental and Addictive
Disorders. Current psychiatry reports, 21(2), p.10.
Rieger, M., Wagner, N., Mebratie, A., Alemu, G. and Bedi, A., 2019. The impact of the Ethiopian health
extension program and health development army on maternal mortality: A synthetic control
approach. Social Science & Medicine, 232, pp.374-381.
Ryan, S.J., Carlson, C.J., Mordecai, E.A. and Johnson, L.R., 2019. Global expansion and redistribution of
Aedes-borne virus transmission risk with climate change. PLoS neglected tropical diseases, 13(3),
p.e0007213.
Sageer, R., Kongnyuy, E., Adebimpe, W.O., Omosehin, O., Ogunsola, E.A. and Sanni, B., 2019. Causes
and contributory factors of maternal mortality: evidence from maternal and perinatal death surveillance
and response in Ogun state, Southwest Nigeria. BMC pregnancy and childbirth, 19(1), p.63.
Tomkinson, G.R., Lang, J.J. and Tremblay, M.S., 2019. Temporal trends in the cardiorespiratory fitness of
children and adolescents representing 19 high-income and upper middle-income countries between 1981
and 2014. Br J Sports Med, 53(8), pp.478-486.
Zanardi, D.M., Parpinelli, M.A., Haddad, S.M., Costa, M.L., Sousa, M.H., Leite, D.F. and Cecatti, J.G.,
2019. Adverse perinatal outcomes are associated with severe maternal morbidity and mortality: evidence
13
Global Burden of Disease 14
from a national multicentre cross-sectional study. Archives of gynecology and obstetrics, 299(3), pp.645-
654.
Zhou, M., Wang, H., Zeng, X., Yin, P., Zhu, J., Chen, W., Li, X., Wang, L., Wang, L., Liu, Y. and Liu, J.,
2019. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis
for the Global Burden of Disease Study 2017. The Lancet.
14
from a national multicentre cross-sectional study. Archives of gynecology and obstetrics, 299(3), pp.645-
654.
Zhou, M., Wang, H., Zeng, X., Yin, P., Zhu, J., Chen, W., Li, X., Wang, L., Wang, L., Liu, Y. and Liu, J.,
2019. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis
for the Global Burden of Disease Study 2017. The Lancet.
14
1 out of 15
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.