Health Assessment Assignment
VerifiedAdded on 2022/11/28
|13
|3357
|241
AI Summary
This Health Assessment Assignment discusses the patient's current health issues, previous hospitalizations, medication, and various patterns related to their health. It also explores the use of Gordon's Functional Assessment and nursing interventions to improve the patient's health outcome.
Contribute Materials
Your contribution can guide someone’s learning journey. Share your
documents today.
Health Assessment Assignment
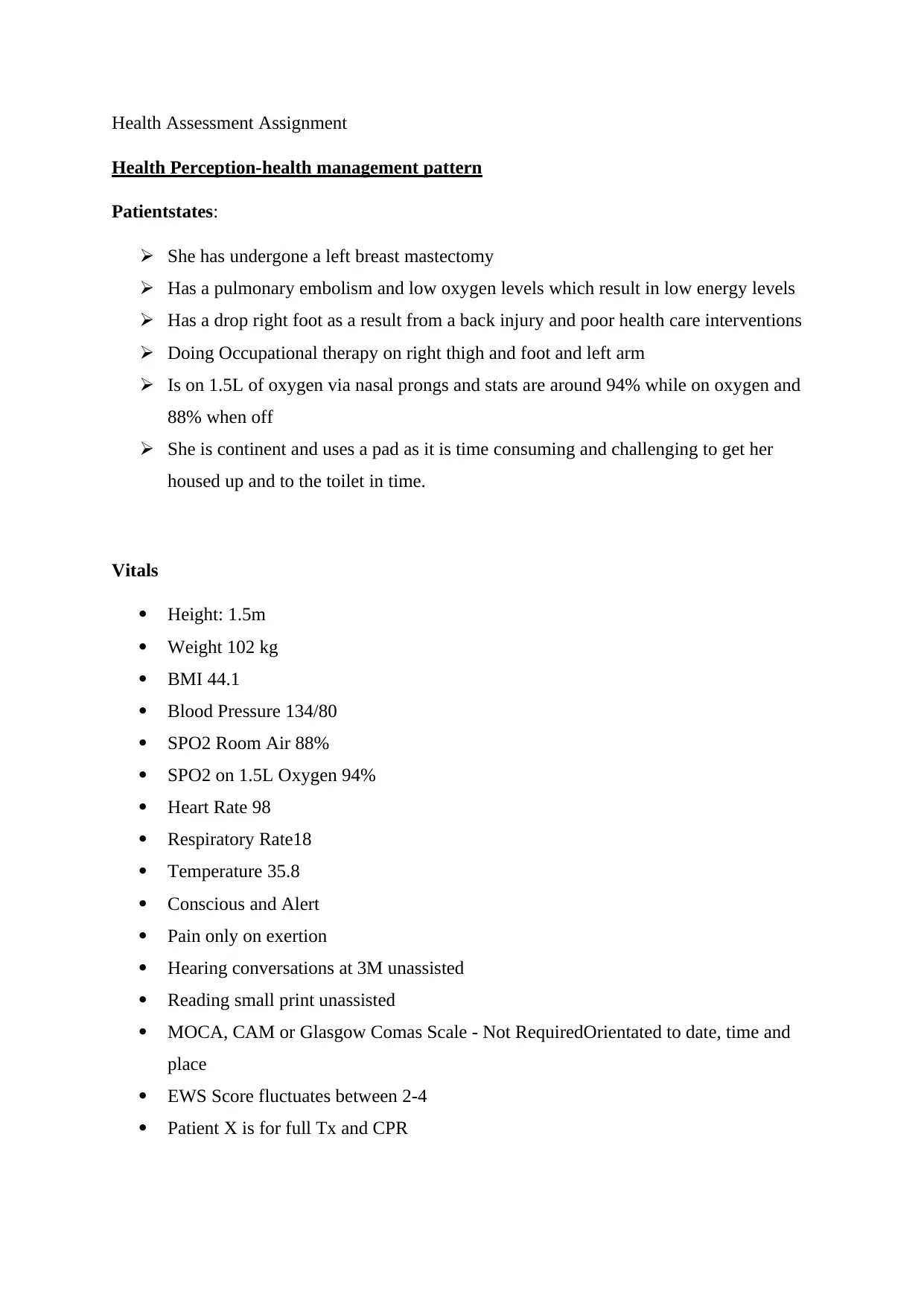
Health Perception-health management pattern
Patientstates:
She has undergone a left breast mastectomy
Has a pulmonary embolism and low oxygen levels which result in low energy levels
Has a drop right foot as a result from a back injury and poor health care interventions
Doing Occupational therapy on right thigh and foot and left arm
Is on 1.5L of oxygen via nasal prongs and stats are around 94% while on oxygen and
88% when off
She is continent and uses a pad as it is time consuming and challenging to get her
housed up and to the toilet in time.
Vitals
Height: 1.5m
Weight 102 kg
BMI 44.1
Blood Pressure 134/80
SPO2 Room Air 88%
SPO2 on 1.5L Oxygen 94%
Heart Rate 98
Respiratory Rate18
Temperature 35.8
Conscious and Alert
Pain only on exertion
Hearing conversations at 3M unassisted
Reading small print unassisted
MOCA, CAM or Glasgow Comas Scale - Not RequiredOrientated to date, time and
place
EWS Score fluctuates between 2-4
Patient X is for full Tx and CPR
Health Perception-health management pattern
Patientstates:
She has undergone a left breast mastectomy
Has a pulmonary embolism and low oxygen levels which result in low energy levels
Has a drop right foot as a result from a back injury and poor health care interventions
Doing Occupational therapy on right thigh and foot and left arm
Is on 1.5L of oxygen via nasal prongs and stats are around 94% while on oxygen and
88% when off
She is continent and uses a pad as it is time consuming and challenging to get her
housed up and to the toilet in time.
Vitals
Height: 1.5m
Weight 102 kg
BMI 44.1
Blood Pressure 134/80
SPO2 Room Air 88%
SPO2 on 1.5L Oxygen 94%
Heart Rate 98
Respiratory Rate18
Temperature 35.8
Conscious and Alert
Pain only on exertion
Hearing conversations at 3M unassisted
Reading small print unassisted
MOCA, CAM or Glasgow Comas Scale - Not RequiredOrientated to date, time and
place
EWS Score fluctuates between 2-4
Patient X is for full Tx and CPR
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
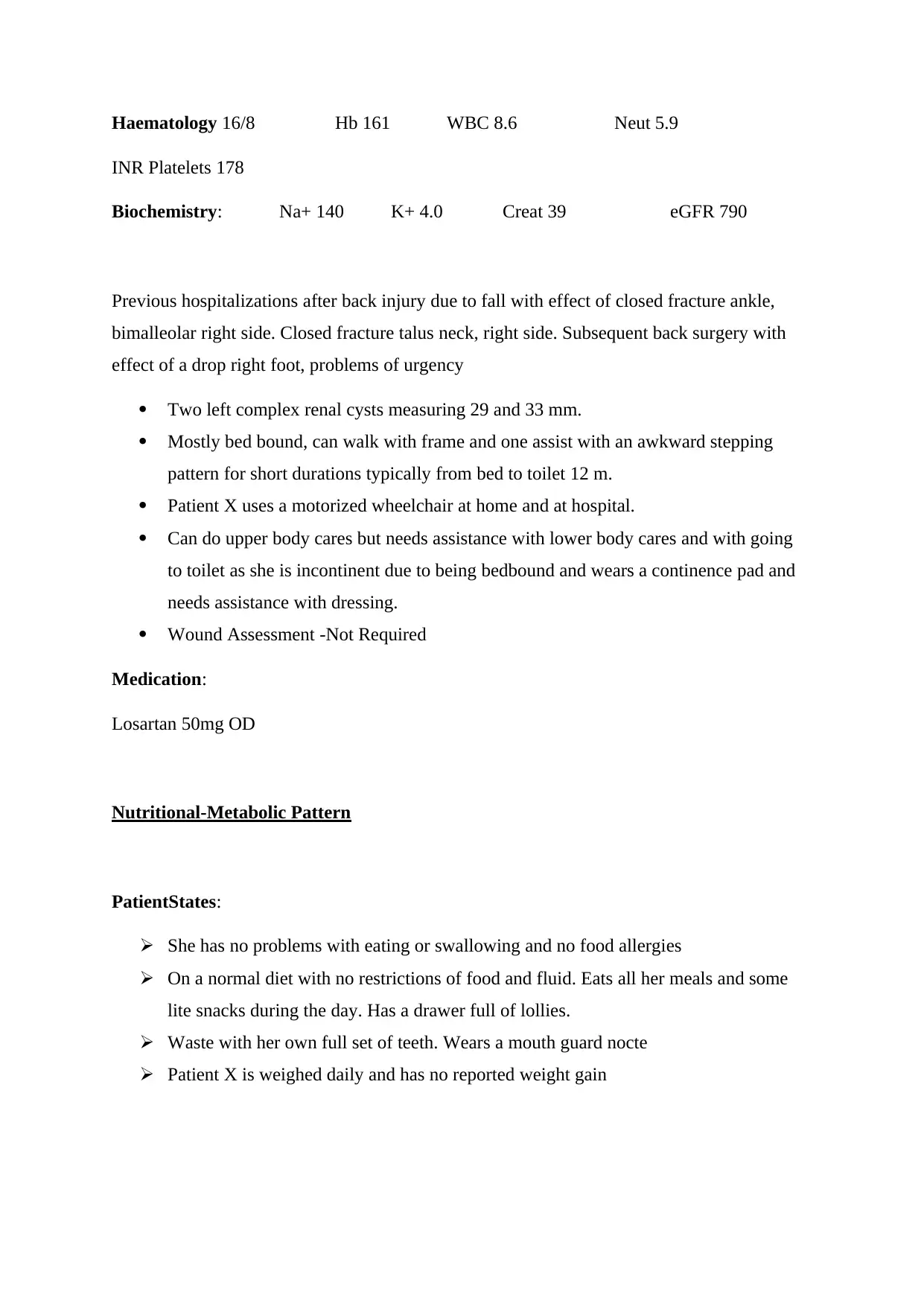
Haematology 16/8 Hb 161 WBC 8.6 Neut 5.9
INR Platelets 178
Biochemistry: Na+ 140 K+ 4.0 Creat 39 eGFR 790
Previous hospitalizations after back injury due to fall with effect of closed fracture ankle,
bimalleolar right side. Closed fracture talus neck, right side. Subsequent back surgery with
effect of a drop right foot, problems of urgency
Two left complex renal cysts measuring 29 and 33 mm.
Mostly bed bound, can walk with frame and one assist with an awkward stepping
pattern for short durations typically from bed to toilet 12 m.
Patient X uses a motorized wheelchair at home and at hospital.
Can do upper body cares but needs assistance with lower body cares and with going
to toilet as she is incontinent due to being bedbound and wears a continence pad and
needs assistance with dressing.
Wound Assessment -Not Required
Medication:
Losartan 50mg OD
Nutritional-Metabolic Pattern
PatientStates:
She has no problems with eating or swallowing and no food allergies
On a normal diet with no restrictions of food and fluid. Eats all her meals and some
lite snacks during the day. Has a drawer full of lollies.
Waste with her own full set of teeth. Wears a mouth guard nocte
Patient X is weighed daily and has no reported weight gain
INR Platelets 178
Biochemistry: Na+ 140 K+ 4.0 Creat 39 eGFR 790
Previous hospitalizations after back injury due to fall with effect of closed fracture ankle,
bimalleolar right side. Closed fracture talus neck, right side. Subsequent back surgery with
effect of a drop right foot, problems of urgency
Two left complex renal cysts measuring 29 and 33 mm.
Mostly bed bound, can walk with frame and one assist with an awkward stepping
pattern for short durations typically from bed to toilet 12 m.
Patient X uses a motorized wheelchair at home and at hospital.
Can do upper body cares but needs assistance with lower body cares and with going
to toilet as she is incontinent due to being bedbound and wears a continence pad and
needs assistance with dressing.
Wound Assessment -Not Required
Medication:
Losartan 50mg OD
Nutritional-Metabolic Pattern
PatientStates:
She has no problems with eating or swallowing and no food allergies
On a normal diet with no restrictions of food and fluid. Eats all her meals and some
lite snacks during the day. Has a drawer full of lollies.
Waste with her own full set of teeth. Wears a mouth guard nocte
Patient X is weighed daily and has no reported weight gain
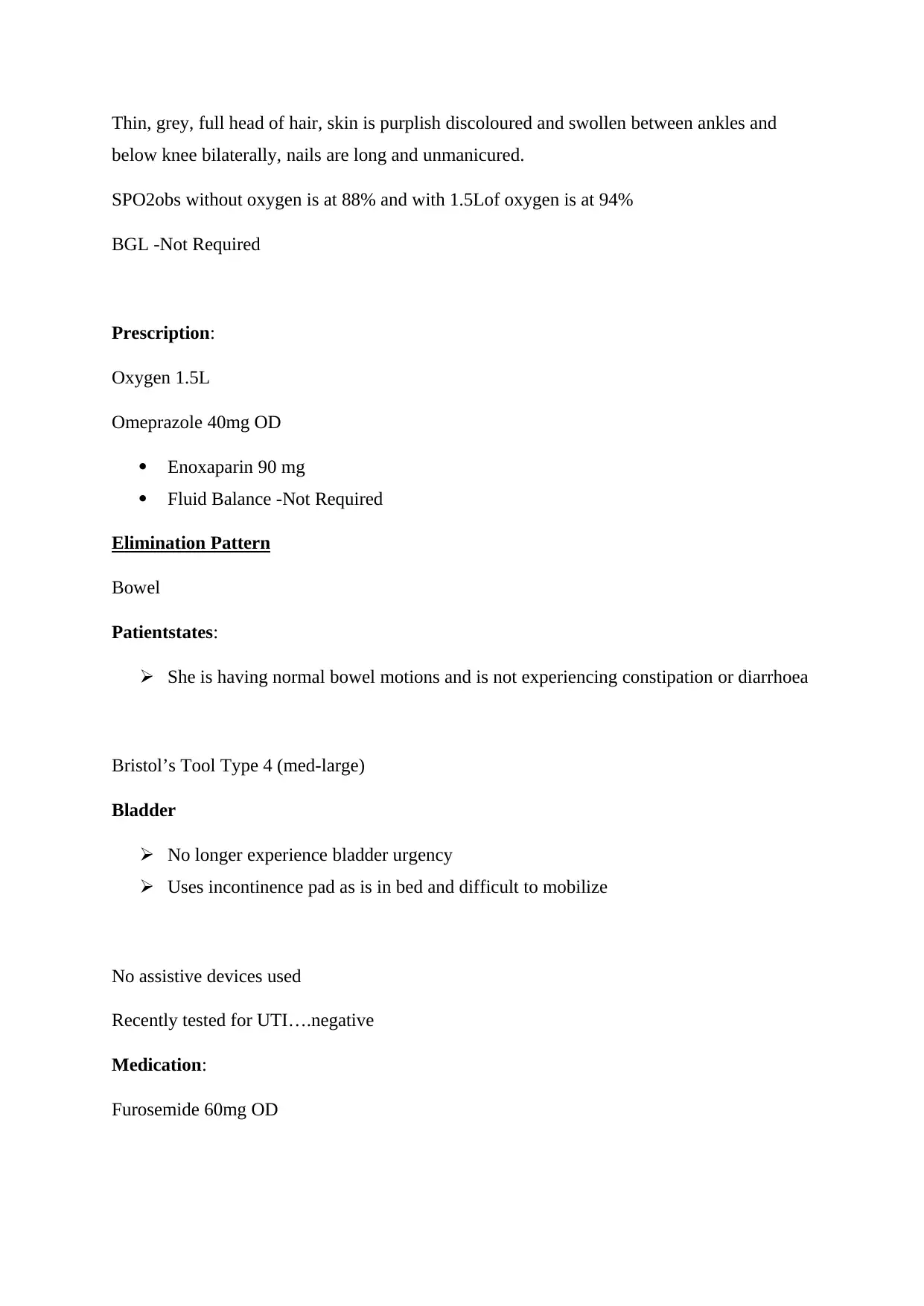
Thin, grey, full head of hair, skin is purplish discoloured and swollen between ankles and
below knee bilaterally, nails are long and unmanicured.
SPO2obs without oxygen is at 88% and with 1.5Lof oxygen is at 94%
BGL -Not Required
Prescription:
Oxygen 1.5L
Omeprazole 40mg OD
Enoxaparin 90 mg
Fluid Balance -Not Required
Elimination Pattern
Bowel
Patientstates:
She is having normal bowel motions and is not experiencing constipation or diarrhoea
Bristol’s Tool Type 4 (med-large)
Bladder
No longer experience bladder urgency
Uses incontinence pad as is in bed and difficult to mobilize
No assistive devices used
Recently tested for UTI….negative
Medication:
Furosemide 60mg OD
below knee bilaterally, nails are long and unmanicured.
SPO2obs without oxygen is at 88% and with 1.5Lof oxygen is at 94%
BGL -Not Required
Prescription:
Oxygen 1.5L
Omeprazole 40mg OD
Enoxaparin 90 mg
Fluid Balance -Not Required
Elimination Pattern
Bowel
Patientstates:
She is having normal bowel motions and is not experiencing constipation or diarrhoea
Bristol’s Tool Type 4 (med-large)
Bladder
No longer experience bladder urgency
Uses incontinence pad as is in bed and difficult to mobilize
No assistive devices used
Recently tested for UTI….negative
Medication:
Furosemide 60mg OD
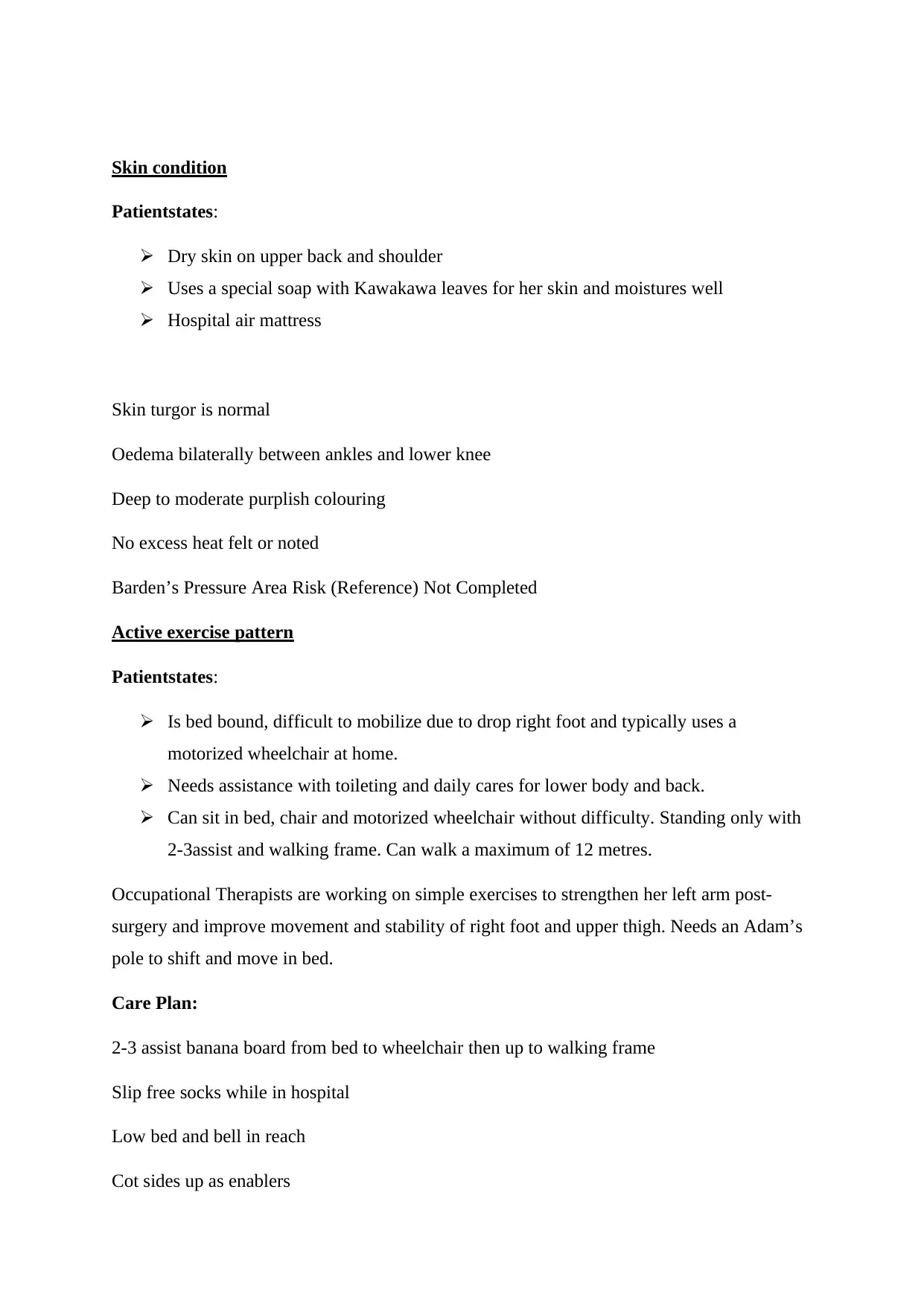
Skin condition
Patientstates:
Dry skin on upper back and shoulder
Uses a special soap with Kawakawa leaves for her skin and moistures well
Hospital air mattress
Skin turgor is normal
Oedema bilaterally between ankles and lower knee
Deep to moderate purplish colouring
No excess heat felt or noted
Barden’s Pressure Area Risk (Reference) Not Completed
Active exercise pattern
Patientstates:
Is bed bound, difficult to mobilize due to drop right foot and typically uses a
motorized wheelchair at home.
Needs assistance with toileting and daily cares for lower body and back.
Can sit in bed, chair and motorized wheelchair without difficulty. Standing only with
2-3assist and walking frame. Can walk a maximum of 12 metres.
Occupational Therapists are working on simple exercises to strengthen her left arm post-
surgery and improve movement and stability of right foot and upper thigh. Needs an Adam’s
pole to shift and move in bed.
Care Plan:
2-3 assist banana board from bed to wheelchair then up to walking frame
Slip free socks while in hospital
Low bed and bell in reach
Cot sides up as enablers
Patientstates:
Dry skin on upper back and shoulder
Uses a special soap with Kawakawa leaves for her skin and moistures well
Hospital air mattress
Skin turgor is normal
Oedema bilaterally between ankles and lower knee
Deep to moderate purplish colouring
No excess heat felt or noted
Barden’s Pressure Area Risk (Reference) Not Completed
Active exercise pattern
Patientstates:
Is bed bound, difficult to mobilize due to drop right foot and typically uses a
motorized wheelchair at home.
Needs assistance with toileting and daily cares for lower body and back.
Can sit in bed, chair and motorized wheelchair without difficulty. Standing only with
2-3assist and walking frame. Can walk a maximum of 12 metres.
Occupational Therapists are working on simple exercises to strengthen her left arm post-
surgery and improve movement and stability of right foot and upper thigh. Needs an Adam’s
pole to shift and move in bed.
Care Plan:
2-3 assist banana board from bed to wheelchair then up to walking frame
Slip free socks while in hospital
Low bed and bell in reach
Cot sides up as enablers
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
Hendrich’s Fall Risk – Not Completed
Sleep Rest Pattern
Patientstates:
For the most part sleeps well at night
Medication:
Risedronate 35 mg weekly Sunday
Cognitive-perceptual pattern
Patientstates
Does not use hearing aids or wears glasses.
Has adequate sensation of heat, cold and pain. No evidence of vertigo has adequate language
and memory and engaged in conversation easily and has adequate memory.
Self-perception-self-concept pattern
Patientstates:
Strong and resilient
Always the “rescuer” rarely rescued
Frustrated with her health situation and feels she has been robbed of her good health
and recovery after her fall and initial injury to back and neck. Feels there has been a
medical cover up to the poor care and failed proper assessment of her injuries leading
to further nerve damage and the right dropped foot.
She can no longer line dance, swim, get around and socialize and care for herself like
she used to.
Feel like the ACC and doctors have made statements about her health that are
incorrect and unsubstantiated which has led to her not getting the financial support,
Sleep Rest Pattern
Patientstates:
For the most part sleeps well at night
Medication:
Risedronate 35 mg weekly Sunday
Cognitive-perceptual pattern
Patientstates
Does not use hearing aids or wears glasses.
Has adequate sensation of heat, cold and pain. No evidence of vertigo has adequate language
and memory and engaged in conversation easily and has adequate memory.
Self-perception-self-concept pattern
Patientstates:
Strong and resilient
Always the “rescuer” rarely rescued
Frustrated with her health situation and feels she has been robbed of her good health
and recovery after her fall and initial injury to back and neck. Feels there has been a
medical cover up to the poor care and failed proper assessment of her injuries leading
to further nerve damage and the right dropped foot.
She can no longer line dance, swim, get around and socialize and care for herself like
she used to.
Feel like the ACC and doctors have made statements about her health that are
incorrect and unsubstantiated which has led to her not getting the financial support,
compensation and treatments she has needed to recover properly or that is due to her.
Her current and past health issues have increased her depression as she doesn’t live
the life she had or desires to have.
Role-relationship pattern
Single
Parent to adult children
Lives alone and independently
Retired
Interdependency with adult children and community carers for ADLs and various
needs
Dissatisfied with her role and relationships with children and her life as it is not what she
imagined it would be.
Sexuality-reproductive pattern
Patientstates:
Married, and divorced
Husband was an alcoholic and abusive
Post-menopausal
4-children by C-section (2-children in NZ and 1-in Australia).. All are adults and
living independent
Moved back to NZ after being in Australia for 28-years and raised 2-children on her
own with no financial support from ex
Thought that moving back to NZ she would have family support. She had no support
given to her by her family of origin.
1-male child predeceased at age of 23-years. Cause of PTSD and Depression
Her current and past health issues have increased her depression as she doesn’t live
the life she had or desires to have.
Role-relationship pattern
Single
Parent to adult children
Lives alone and independently
Retired
Interdependency with adult children and community carers for ADLs and various
needs
Dissatisfied with her role and relationships with children and her life as it is not what she
imagined it would be.
Sexuality-reproductive pattern
Patientstates:
Married, and divorced
Husband was an alcoholic and abusive
Post-menopausal
4-children by C-section (2-children in NZ and 1-in Australia).. All are adults and
living independent
Moved back to NZ after being in Australia for 28-years and raised 2-children on her
own with no financial support from ex
Thought that moving back to NZ she would have family support. She had no support
given to her by her family of origin.
1-male child predeceased at age of 23-years. Cause of PTSD and Depression
Coping-stress tolerance pattern
Patientstates:
Depression
PTSD
Patient X uses keeping overly busy as a distraction from emotional pain
Eating especially lollies to cope with boredom
Medication:
Escitalopram10mg OD
Cetirizine 10 mg OD
Paracetamol
Value-belief pattern
Patientstates:
ls an atheist.
Believes she is a good person who has gone through “hell”
Tries to be a good person….
Care Plan:
Daily assistance with care plans
Manage pain as needed
Communicate with clear explanations and maintain privacy and respect
Introduction
The primary responsibility of a nurse is to assess the patient’s health condition by
conducting appropriate assessments and collecting subjective and objective data that guides
the treatment process. Nurses use Gordon’s Functional Assessment to understand the
patient’s health condition by collecting information from all aspects that will help to deliver a
Patientstates:
Depression
PTSD
Patient X uses keeping overly busy as a distraction from emotional pain
Eating especially lollies to cope with boredom
Medication:
Escitalopram10mg OD
Cetirizine 10 mg OD
Paracetamol
Value-belief pattern
Patientstates:
ls an atheist.
Believes she is a good person who has gone through “hell”
Tries to be a good person….
Care Plan:
Daily assistance with care plans
Manage pain as needed
Communicate with clear explanations and maintain privacy and respect
Introduction
The primary responsibility of a nurse is to assess the patient’s health condition by
conducting appropriate assessments and collecting subjective and objective data that guides
the treatment process. Nurses use Gordon’s Functional Assessment to understand the
patient’s health condition by collecting information from all aspects that will help to deliver a
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
nursing care following a holistic approach. Nurses must possess the core competencies and
must have adequate skill set required to plan the intervention strategies. Nurse must be
culturally competent in order to facilitate an individualised care of the patient.
In this assignment The Gordon’s Functional Assessment (Gordon, 2016) will be used
to review Patient X current and previous health issues and how they relate to her current
status and recovery to be discharged and return home with community support services to
live her life independently. A discussion on two focus assessments and nursing interventions
on Patient X is included and evidence of nursing competencies 1.2 and 1.5 Nursing Council
of New Zealand 2016 will be explained.
Synopsis
Patient X is a 74-years 9-month old New Zealand European female, divorced mother
of 4-children. Patient currently has elected to undergo an elective mastectomy as she was
diagnosed with malignant neoplasm of upper-outer quadrant of breast and secondary and
unspecified malignant neoplasm of axillary and upper limb lymph nodes. Post-surgery she
has peripheral bilateral oedema, fluid overload, pulmonary embolism, and crackling bi-
laterally in base of both lungs. initial recovery transferred to rehabilitation ward to prepare for
discharge to rest home. Is in hospital for rehabilitation to strengthen muscles and heal from
complications from surgery with goal to return home with community supports in place or
increased to assist her with her independent living. Patient X is an ex-smoker for 10-years she
used to smoke40-50packs per year. She currently has asthma, without mention of COPD,
Hypertension, Renal Cysts, Depression, PTSD, pulmonary embolism, low SPO2 levels, and
Hiatus Hernia.
must have adequate skill set required to plan the intervention strategies. Nurse must be
culturally competent in order to facilitate an individualised care of the patient.
In this assignment The Gordon’s Functional Assessment (Gordon, 2016) will be used
to review Patient X current and previous health issues and how they relate to her current
status and recovery to be discharged and return home with community support services to
live her life independently. A discussion on two focus assessments and nursing interventions
on Patient X is included and evidence of nursing competencies 1.2 and 1.5 Nursing Council
of New Zealand 2016 will be explained.
Synopsis
Patient X is a 74-years 9-month old New Zealand European female, divorced mother
of 4-children. Patient currently has elected to undergo an elective mastectomy as she was
diagnosed with malignant neoplasm of upper-outer quadrant of breast and secondary and
unspecified malignant neoplasm of axillary and upper limb lymph nodes. Post-surgery she
has peripheral bilateral oedema, fluid overload, pulmonary embolism, and crackling bi-
laterally in base of both lungs. initial recovery transferred to rehabilitation ward to prepare for
discharge to rest home. Is in hospital for rehabilitation to strengthen muscles and heal from
complications from surgery with goal to return home with community supports in place or
increased to assist her with her independent living. Patient X is an ex-smoker for 10-years she
used to smoke40-50packs per year. She currently has asthma, without mention of COPD,
Hypertension, Renal Cysts, Depression, PTSD, pulmonary embolism, low SPO2 levels, and
Hiatus Hernia.
Assessment:
1. For patients with a lower pressure sore risk indicates a higher level of risk for
developing pressure ulcers. People having a pressure sore risk of 16 indicates a
moderate risk and therefore nurses must access the comorbidities and the medications
by monitoring perfusion and oxygenation of the patients and by evaluating nutritional
deficient of the patient. A higher rates of pressure ulcers is generally determined by
monitoring several comorbidities that act as risk factors for pressure sore including
obesity, Chronic Obstructive Pulmonary Disease, CHF, corticosteroid use and
Diabetes Mellitus. Therefore, nurses must first conduct health assessment of the
patient by following a Gordon’s functional Heath Patterns approach in order to
understand and access the patient’s health needs more comprehensively and
accurately and carry out effective intervention strategies to improve the health
outcome of the patient.Pressure ulcers develops as a result of compression in the
subcutaneous tissues and the capillaries of the skin that subsequently leads to tissue
necrosis (Bhattacharya & Mishra, 2015).Thus there is a need to keep the external
pressure less than 32 m Hg to prevent the development of pressure ulcers. Healthcare
professionals including nurse use risk assessment tools for accessing these risk factors
that includes the use of Braden Scale which is mostly used in the United States. The
scale has been designed to be used in adults that consist of 6 subscales- Sensory
perception, moisture, activity, mobility, nutrition, friction and shear which is based on
conceptual scheme that links the comorbidities or associated condition of the patient
(In.gov, 2019).
2. Nurses while working in clinical settings must possess adequate knowledge and skills
to understand and interpret the patient’s condition by monitoring the vitals through
assessments that helps to comprehensively understand and access the health needs of
the patients. Gordon’s functional health patterns helps in collecting data and
information about the patient’s health by accessing every details regarding the patient
from every aspect that helps to understand and access patent’s health needs
comprehensively and completely and helps the nurses to carry out appropriate
intervention strategies that will increase the health outcome of the patient and increase
the overall effectiveness of the care plan implanted by the nurse. One of the risk
1. For patients with a lower pressure sore risk indicates a higher level of risk for
developing pressure ulcers. People having a pressure sore risk of 16 indicates a
moderate risk and therefore nurses must access the comorbidities and the medications
by monitoring perfusion and oxygenation of the patients and by evaluating nutritional
deficient of the patient. A higher rates of pressure ulcers is generally determined by
monitoring several comorbidities that act as risk factors for pressure sore including
obesity, Chronic Obstructive Pulmonary Disease, CHF, corticosteroid use and
Diabetes Mellitus. Therefore, nurses must first conduct health assessment of the
patient by following a Gordon’s functional Heath Patterns approach in order to
understand and access the patient’s health needs more comprehensively and
accurately and carry out effective intervention strategies to improve the health
outcome of the patient.Pressure ulcers develops as a result of compression in the
subcutaneous tissues and the capillaries of the skin that subsequently leads to tissue
necrosis (Bhattacharya & Mishra, 2015).Thus there is a need to keep the external
pressure less than 32 m Hg to prevent the development of pressure ulcers. Healthcare
professionals including nurse use risk assessment tools for accessing these risk factors
that includes the use of Braden Scale which is mostly used in the United States. The
scale has been designed to be used in adults that consist of 6 subscales- Sensory
perception, moisture, activity, mobility, nutrition, friction and shear which is based on
conceptual scheme that links the comorbidities or associated condition of the patient
(In.gov, 2019).
2. Nurses while working in clinical settings must possess adequate knowledge and skills
to understand and interpret the patient’s condition by monitoring the vitals through
assessments that helps to comprehensively understand and access the health needs of
the patients. Gordon’s functional health patterns helps in collecting data and
information about the patient’s health by accessing every details regarding the patient
from every aspect that helps to understand and access patent’s health needs
comprehensively and completely and helps the nurses to carry out appropriate
intervention strategies that will increase the health outcome of the patient and increase
the overall effectiveness of the care plan implanted by the nurse. One of the risk
assessment used by the nurses is the Hendrick’s fall risk assessment. Considering the
patient’s age in this scenario, it is important to access the patient’s risk of falling.
Falls among older adults is common and occurs as a result of multifactorial etiology
including chronic diseases, acute conditions, comorbidities, mediations and as a
prodrome of other diseases or illnesses or as idiopathic phenomenon. Nurses must use
this tool to access their risk of falling and must include in their care strategy of
primary health care that helps to recognize the patients who are at risk of falling and
prevent falls in them through nursing interventions. The best available approach in the
acute care incorporate the use of Hendrick’s Fall Risk to determine the risk of falling
according to age, gender, emotional heath status, symptoms of dizziness or other
related diseases and also as adverse effects of some medications. Hendrick's Fall Risk
score at 4 indicates confusion, impulsivity and disorientation thereby increasing the
risk of fall.Therefore, nurses must assist the patient with ambulatory services and help
them in performing daily activities and promote the consumption of nutritional foods
(increasing intake of vitamin D foods) in order to prevent the risk of fall of the patient
(Vonnes & Wolf, 2017).Therefore, nurses must make sure that all the necessary items
are near the patients reach and a ringing bell is present near the patient’s bed so they
can always call or inform the healthcare staffs in case they need any help. The nurses
must be available to assist the patient when they are in need and must provide them
with care on priority basis. Since the patient has an increased chance of falling, the
patient must be properly monitored and accessed to prevent the chance of falling.
Nursing interventions should aim at preventing the chance of falling. The nurse can
make the patient wear non-slip socks to reduce the chance of falling. It is also
important for the nurse to educate the patient on the health condition so that they are
more cautious and are aware (Vonnes& Wolf, 2017). Nurse can also increase vitamin
D supplement in the patient’s diet and they must be screened for osteoporosis that
contributes to increase their risk of fall.
3. By conducting Gordon’s functional assessment the patient’s health needs and areas of
concern are determined and nursing interventions are implemented by identifying and
accessing those areas. To cope with her stress and emotional problems as a nurse one
must encourage verbalization of their feelings and perception, and fears for promoting
the resolution of fear and establish strategies of coping strategies effectively. She
must be supported to apply and use defences mechanism for relieving her anxiety.
The patient must be encouraged to have an attitude of realistic hope to deal with the
patient’s age in this scenario, it is important to access the patient’s risk of falling.
Falls among older adults is common and occurs as a result of multifactorial etiology
including chronic diseases, acute conditions, comorbidities, mediations and as a
prodrome of other diseases or illnesses or as idiopathic phenomenon. Nurses must use
this tool to access their risk of falling and must include in their care strategy of
primary health care that helps to recognize the patients who are at risk of falling and
prevent falls in them through nursing interventions. The best available approach in the
acute care incorporate the use of Hendrick’s Fall Risk to determine the risk of falling
according to age, gender, emotional heath status, symptoms of dizziness or other
related diseases and also as adverse effects of some medications. Hendrick's Fall Risk
score at 4 indicates confusion, impulsivity and disorientation thereby increasing the
risk of fall.Therefore, nurses must assist the patient with ambulatory services and help
them in performing daily activities and promote the consumption of nutritional foods
(increasing intake of vitamin D foods) in order to prevent the risk of fall of the patient
(Vonnes & Wolf, 2017).Therefore, nurses must make sure that all the necessary items
are near the patients reach and a ringing bell is present near the patient’s bed so they
can always call or inform the healthcare staffs in case they need any help. The nurses
must be available to assist the patient when they are in need and must provide them
with care on priority basis. Since the patient has an increased chance of falling, the
patient must be properly monitored and accessed to prevent the chance of falling.
Nursing interventions should aim at preventing the chance of falling. The nurse can
make the patient wear non-slip socks to reduce the chance of falling. It is also
important for the nurse to educate the patient on the health condition so that they are
more cautious and are aware (Vonnes& Wolf, 2017). Nurse can also increase vitamin
D supplement in the patient’s diet and they must be screened for osteoporosis that
contributes to increase their risk of fall.
3. By conducting Gordon’s functional assessment the patient’s health needs and areas of
concern are determined and nursing interventions are implemented by identifying and
accessing those areas. To cope with her stress and emotional problems as a nurse one
must encourage verbalization of their feelings and perception, and fears for promoting
the resolution of fear and establish strategies of coping strategies effectively. She
must be supported to apply and use defences mechanism for relieving her anxiety.
The patient must be encouraged to have an attitude of realistic hope to deal with the
Secure Best Marks with AI Grader
Need help grading? Try our AI Grader for instant feedback on your assignments.
feelings of helplessness. Since the patient has respiratory problems due to asthma, the
nurse must monitor her heart rhythm, observe chest movement including accessory
muscle and intercostal muscle refractions for evaluating the respiratory status of the
patient.
By Gordon’s functional assessment, the patient’s health concerns were
identified and the following medications were given to treat the health issues she was
facing-
The patient was given Escitalopram, which is an anti depressant drug and it
functions by affecting the chemicals in the brain that are unbalanced in people
suffering from depression or anxiety. To control the patients’s high blood pressure,
Losartan was given since it helps to protect the kidneys from getting damaged due to
diabetes. The patient also had osteoporosis, therefore, she was also given with
Risedronate Sodium weekly. Furosemide was also prescribed to treat the condition of
edema. Seretide was given to the patient to treat Chronic Obstructive Pulmonary
Disease (COPD).
4. Nursing Competency 1.2 demonstrates the principles of Treating of Waitangi to
nursing practice to ensure culturally safe nursing care (Tdhb.org.nz, 2019). It
promotes the principles that demonstrate culturally safe practices while caring for the
patients (Tdhb.org.nz, 2019). Nurses while working in clinical settings, often come
across situation where they care for people who are from diverse culture or ethnicity.
It evident that nurses struggle to meet the competencies that aims at delivering care
and promoting health of the patients irrespective of their cultural difference. One of
the common barriers to adopt cultural competence is language since in order to
facilitate the delivery of a high quality and a cultural safe care, an effective
communication is important to understand and connect. Considering the language
difference of two diverse cultures, the patient and the nurse, both finds difficult to
communicate, which must not be the scenario. The nurses should be culturally
competent and possess all the core skill set required to access patient’s needs and
provide the patient with a high quality care. If the patient was a non-Maori, the nurse
caring for that patient must be culturally competent to provide them an appropriate
care which is culturally safe.
Competency 1.5 demonstrates that nursing practice should be implemented in
a way that health consumer determines it as a culturally safe care when they are being
nurse must monitor her heart rhythm, observe chest movement including accessory
muscle and intercostal muscle refractions for evaluating the respiratory status of the
patient.
By Gordon’s functional assessment, the patient’s health concerns were
identified and the following medications were given to treat the health issues she was
facing-
The patient was given Escitalopram, which is an anti depressant drug and it
functions by affecting the chemicals in the brain that are unbalanced in people
suffering from depression or anxiety. To control the patients’s high blood pressure,
Losartan was given since it helps to protect the kidneys from getting damaged due to
diabetes. The patient also had osteoporosis, therefore, she was also given with
Risedronate Sodium weekly. Furosemide was also prescribed to treat the condition of
edema. Seretide was given to the patient to treat Chronic Obstructive Pulmonary
Disease (COPD).
4. Nursing Competency 1.2 demonstrates the principles of Treating of Waitangi to
nursing practice to ensure culturally safe nursing care (Tdhb.org.nz, 2019). It
promotes the principles that demonstrate culturally safe practices while caring for the
patients (Tdhb.org.nz, 2019). Nurses while working in clinical settings, often come
across situation where they care for people who are from diverse culture or ethnicity.
It evident that nurses struggle to meet the competencies that aims at delivering care
and promoting health of the patients irrespective of their cultural difference. One of
the common barriers to adopt cultural competence is language since in order to
facilitate the delivery of a high quality and a cultural safe care, an effective
communication is important to understand and connect. Considering the language
difference of two diverse cultures, the patient and the nurse, both finds difficult to
communicate, which must not be the scenario. The nurses should be culturally
competent and possess all the core skill set required to access patient’s needs and
provide the patient with a high quality care. If the patient was a non-Maori, the nurse
caring for that patient must be culturally competent to provide them an appropriate
care which is culturally safe.
Competency 1.5 demonstrates that nursing practice should be implemented in
a way that health consumer determines it as a culturally safe care when they are being
served. Therefore, nurses must ensure and promote culturally safe practices that
reflect the nurse’s values and beliefs related to the consumer’s culture, ethnicity and
other factors impacting the nursing care (Health.govt.nz, 2019). Nurses must conduct
assessment by aligning with culturally safe practices to ensure a quality outcome.
` I have delivered quality care through an individualised care approach and
implemented the intervention strategies by accessing the health needs of the patient
from every aspect to provide an enhanced nursing care. Models of care framework by
the New Zealand nurses organization states that nurses must maintain a person
centred model to care for achieving quality outcomes. The nurses must be engaged in
understanding and exploring the patient’s preference and values and support them and
their family for making clinical decisions (Nzno.org.nz, 2019). Therefore, I took the
necessary measures by accessing the patient’s needs and gave the appropriate
treatment necessary for her. Gordon’s Functional Health Assessment helped me to
understand the patient’s condition by collecting all the subjective and objective data
and helped me plan and develop the strategies that will increase the patient’s outcome.
reflect the nurse’s values and beliefs related to the consumer’s culture, ethnicity and
other factors impacting the nursing care (Health.govt.nz, 2019). Nurses must conduct
assessment by aligning with culturally safe practices to ensure a quality outcome.
` I have delivered quality care through an individualised care approach and
implemented the intervention strategies by accessing the health needs of the patient
from every aspect to provide an enhanced nursing care. Models of care framework by
the New Zealand nurses organization states that nurses must maintain a person
centred model to care for achieving quality outcomes. The nurses must be engaged in
understanding and exploring the patient’s preference and values and support them and
their family for making clinical decisions (Nzno.org.nz, 2019). Therefore, I took the
necessary measures by accessing the patient’s needs and gave the appropriate
treatment necessary for her. Gordon’s Functional Health Assessment helped me to
understand the patient’s condition by collecting all the subjective and objective data
and helped me plan and develop the strategies that will increase the patient’s outcome.
References:
Bhattacharya, S., & Mishra, R. K. (2015). Pressure ulcers: current understanding and newer
modalities of treatment. Indian journal of plastic surgery: official publication of the
Association of Plastic Surgeons of India, 48(1), 4. Doi: 10.4103/0970-0358.155260
Gordon, M. (2016). Manual of nursing diagnosis.. (13thed.) Burlington,MA: Jones and
Bartlett. Retrieved 17 September 2019, from https://books.google.co.in/books?
hl=en&lr=&id=t3W-BQAAQBAJ&oi=fnd&pg=PR3&dq=).
+Manual+of+nursing+diagnosis..+(13th+ed.)+Burlington,MA:+Jones+and+Bartlett.+
+&ots=TsU4K6CdJ_&sig=SU6fzjUm7VTZnIOSwVTXSBvuCe0&redir_esc=y#v=o
nepage&q&f=false
Health.govt.nz. (2019). Treaty of Waitangi principles. Retrieved 17 September 2019, from
https://www.health.govt.nz/our-work/populations/maori-health/he-korowai-oranga/
strengthening-he-korowai-oranga/treaty-waitangi-principles
In.gov. (2019). BRADEN SCALE – For Predicting Pressure Sore Risk. Retrieved 16
September 2019, from https://www.in.gov/isdh/files/Braden_Scale.pdf
Nursing Council of New Zealand. (2016). Competencies for registered nurses.
Wellington,NZ: Nursing Council of New Zealand
Nzno.org.nz. (2019). Retrieved 17 September 2019, from
https://www.nzno.org.nz/LinkClick.aspx?fileticket=TaToipIAm0Y%3D&portalid=0
Tdhb.org.nz. (2019). Retrieved 16 September 2019, from
https://www.tdhb.org.nz/services/nursing/documents/nursing-council-documents/
Competencies%20for%20registered%20nurses.pdf
Vonnes, C., & Wolf, D. (2017). Fall risk and prevention agreement: engaging patients and
families with a partnership for patient safety. BMJ Open Qual, 6(2), e000038. Doi:
10.1136/bmjoq-2017-000038
Bhattacharya, S., & Mishra, R. K. (2015). Pressure ulcers: current understanding and newer
modalities of treatment. Indian journal of plastic surgery: official publication of the
Association of Plastic Surgeons of India, 48(1), 4. Doi: 10.4103/0970-0358.155260
Gordon, M. (2016). Manual of nursing diagnosis.. (13thed.) Burlington,MA: Jones and
Bartlett. Retrieved 17 September 2019, from https://books.google.co.in/books?
hl=en&lr=&id=t3W-BQAAQBAJ&oi=fnd&pg=PR3&dq=).
+Manual+of+nursing+diagnosis..+(13th+ed.)+Burlington,MA:+Jones+and+Bartlett.+
+&ots=TsU4K6CdJ_&sig=SU6fzjUm7VTZnIOSwVTXSBvuCe0&redir_esc=y#v=o
nepage&q&f=false
Health.govt.nz. (2019). Treaty of Waitangi principles. Retrieved 17 September 2019, from
https://www.health.govt.nz/our-work/populations/maori-health/he-korowai-oranga/
strengthening-he-korowai-oranga/treaty-waitangi-principles
In.gov. (2019). BRADEN SCALE – For Predicting Pressure Sore Risk. Retrieved 16
September 2019, from https://www.in.gov/isdh/files/Braden_Scale.pdf
Nursing Council of New Zealand. (2016). Competencies for registered nurses.
Wellington,NZ: Nursing Council of New Zealand
Nzno.org.nz. (2019). Retrieved 17 September 2019, from
https://www.nzno.org.nz/LinkClick.aspx?fileticket=TaToipIAm0Y%3D&portalid=0
Tdhb.org.nz. (2019). Retrieved 16 September 2019, from
https://www.tdhb.org.nz/services/nursing/documents/nursing-council-documents/
Competencies%20for%20registered%20nurses.pdf
Vonnes, C., & Wolf, D. (2017). Fall risk and prevention agreement: engaging patients and
families with a partnership for patient safety. BMJ Open Qual, 6(2), e000038. Doi:
10.1136/bmjoq-2017-000038
1 out of 13
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
© 2024 | Zucol Services PVT LTD | All rights reserved.