An In-depth Analysis of Health Care Expenditure Growth Drivers
VerifiedAdded on 2022/10/16
|14
|3936
|348
Essay
AI Summary
This essay delves into the multifaceted drivers of health care expenditure growth, examining the global landscape of healthcare spending. It explores the significant variations in health expenditure across high-income and resource-poor nations, highlighting the impact of economic development and fiscal policies. The essay analyzes key factors influencing healthcare costs, including income levels, technological advancements, and demographic shifts. It discusses various modeling approaches used to understand healthcare costs, emphasizing the role of per capita GDP and its elasticity. The study also considers the influence of population age structure, technological progress, and health system characteristics on expenditure patterns. Furthermore, it explores the relationship between government funding, social insurance schemes, and external resources, such as Official Development Aid, and their effects on healthcare spending. The essay underscores the need for efficient resource allocation and innovative funding sources to meet the growing demands of healthcare in developed and developing societies. The analysis provides a comprehensive overview of the complex interplay of factors shaping healthcare expenditure, offering valuable insights into global healthcare trends.

Running head: HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
Name of the Student
Name of the University
Author’s Note:
HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
Name of the Student
Name of the University
Author’s Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
Introduction:
Globally, the quantity of nations spending on health varies greatly. Health expenditure in high-
income countries per capita is over USD 3000 on average, compared with only USD 30 per
capita in resource poor nations. In 2008, per capita health expenditure in 64 nations fell below
USD 100 (Ke, Saksena, & Holly, 2011). The health costs of economic development are also
highly variable. Some nations spend more than 12 per cent of GDP on health and some spend
less than 3 per cent on health. Economists agree that most Western European countries are
currently operating health care systems that cannot be funded at all in future. Moreover, it may
not be far from the future. In general, Europe's fiscal balance and debt levels will be consolidated
in the next ten years. Europe is nearing frightening levels of public debt even if crisis-related
measures and developments are diminished. The European Commission has recently estimated
that by the end of this century, public debt in the EU may amount to up to 120 percent of GDP
(Ke et al., 2011). Only this would have depressing impacts on all kinds of government spending.
As spending rises even more rapidly when baby boom generation reaches medical age quickly,
any account of the future funding of healthcare is read carefully. There is a pressing need to find
methods of more effectively using resources and fresh sources of funding to meet growing
requirements for medical care in Europe and other matured societies with firm models for
finances (e.g. the United States). A comprehensive literature is available in OECD countries
about health expenditure and their development (Baltagi & Moscone, 2010). However, there is
comparatively little proof from developing nations, and the article aims to help fill this gap
through the exploration of information from 143 developing and developing nations. Healthcare
costs have been significantly increased for a long time. In the last two decades, the trend in
spending has continuously increased. For instance, over the last two years, each resident's
Introduction:
Globally, the quantity of nations spending on health varies greatly. Health expenditure in high-
income countries per capita is over USD 3000 on average, compared with only USD 30 per
capita in resource poor nations. In 2008, per capita health expenditure in 64 nations fell below
USD 100 (Ke, Saksena, & Holly, 2011). The health costs of economic development are also
highly variable. Some nations spend more than 12 per cent of GDP on health and some spend
less than 3 per cent on health. Economists agree that most Western European countries are
currently operating health care systems that cannot be funded at all in future. Moreover, it may
not be far from the future. In general, Europe's fiscal balance and debt levels will be consolidated
in the next ten years. Europe is nearing frightening levels of public debt even if crisis-related
measures and developments are diminished. The European Commission has recently estimated
that by the end of this century, public debt in the EU may amount to up to 120 percent of GDP
(Ke et al., 2011). Only this would have depressing impacts on all kinds of government spending.
As spending rises even more rapidly when baby boom generation reaches medical age quickly,
any account of the future funding of healthcare is read carefully. There is a pressing need to find
methods of more effectively using resources and fresh sources of funding to meet growing
requirements for medical care in Europe and other matured societies with firm models for
finances (e.g. the United States). A comprehensive literature is available in OECD countries
about health expenditure and their development (Baltagi & Moscone, 2010). However, there is
comparatively little proof from developing nations, and the article aims to help fill this gap
through the exploration of information from 143 developing and developing nations. Healthcare
costs have been significantly increased for a long time. In the last two decades, the trend in
spending has continuously increased. For instance, over the last two years, each resident's
2HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
healthcare spending in the US has been around $7,600 (Dieleman et al., 2016). It accounted for
approximately 16% of the nation's GDP. In reality, this figure is still the highest in the developed
countries. For instance, new medical technologies, treatments and medications can generate extra
expenditure on healthcare, particularly if they are not substituting or reducing current expenses
for one reason or another (Erixon & Van der Marel, 2011). However, it is not true that these new
or extra expenses explain the greater portion of general health care expenses. For example,
public services expenditure has in the last decades accounted for a steady comparative share of
OECD countries’ overall health care expenses. Indeed, pharmaceutical expenditure has
decreased relatively from 1970, although complete public health expenditure has risen quickly
over the previous 15 years (Erixon & Van der Marel, 2011). True, medical innovations such as
CT scanners have led to increasing healthcare expenses, while the general trend in the rates of
investment and healthcare development does not match the rates shown for general healthcare
expenditure development. In addition, when the expenses of particular components in healthcare
manufacturing are compared across nations, there is a considerable distinction in the degree of
capital contributions to healthcare manufacturing among nations of comparable stage of growth.
Moreover, for an industry of "Baumol disease characteristics," such as healthcare, incomes
should not be sufficient to follow a broad GDP growth trend; health tax revenues should instead
rise beyond the overall GDP trend to cover rising disease expenses (Hartwig, 2011). There are
clear trends for the European nations we studied in lagging productivity rates and greater actual
costs for healthcare.
In addition to a prediction on the scheme in terms of future development opportunities, this essay
will discuss present health care expenses in the world environment.
Discussion:
healthcare spending in the US has been around $7,600 (Dieleman et al., 2016). It accounted for
approximately 16% of the nation's GDP. In reality, this figure is still the highest in the developed
countries. For instance, new medical technologies, treatments and medications can generate extra
expenditure on healthcare, particularly if they are not substituting or reducing current expenses
for one reason or another (Erixon & Van der Marel, 2011). However, it is not true that these new
or extra expenses explain the greater portion of general health care expenses. For example,
public services expenditure has in the last decades accounted for a steady comparative share of
OECD countries’ overall health care expenses. Indeed, pharmaceutical expenditure has
decreased relatively from 1970, although complete public health expenditure has risen quickly
over the previous 15 years (Erixon & Van der Marel, 2011). True, medical innovations such as
CT scanners have led to increasing healthcare expenses, while the general trend in the rates of
investment and healthcare development does not match the rates shown for general healthcare
expenditure development. In addition, when the expenses of particular components in healthcare
manufacturing are compared across nations, there is a considerable distinction in the degree of
capital contributions to healthcare manufacturing among nations of comparable stage of growth.
Moreover, for an industry of "Baumol disease characteristics," such as healthcare, incomes
should not be sufficient to follow a broad GDP growth trend; health tax revenues should instead
rise beyond the overall GDP trend to cover rising disease expenses (Hartwig, 2011). There are
clear trends for the European nations we studied in lagging productivity rates and greater actual
costs for healthcare.
In addition to a prediction on the scheme in terms of future development opportunities, this essay
will discuss present health care expenses in the world environment.
Discussion:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
The literature describes several approaches to modelling healthcare costs. Some studies have
used domestic information while others have used macroeconomic aggregates. The review is
restricted to the latter research because of the scope of the research. Some past books depended
on cross-sectional technology while others used methods for panelling. The latter have been
based on static and dynamic models, often with distinct outcomes.
Income:
Revenue (per capita GDP) has been recognized as a significant explanation for the difference in
levels of overall health care expenditure and development in different nations. Cross-sectional
regressions of aggregate healthcare per capita GDP spending per capita in literature from OECD
countries have continuously demonstrated a considerably higher revenue elasticity of about 1.20
to 1.50 (Ke et al., 2011). Regressions of aggregate time series for different nations were mostly
comparable but had significant differences among nations. Likewise, a study used cross-sectional
data in 1997 in the worldwide literature and discovered, based on the information included, that
the income elasticity of health spending was between 1.133 and 1.275. OOP revenue elasticity
ranged from 0.884 to 1.033, while public health expenditure ranged from 1.069 to 1.194
(Musgrove et al. 2002). Gaag and Stimac have also used cross-sectional data from 175 nations in
2004 and have shown that the health expenses ' revenue elasticity is 1.09. They also reported the
outcomes by area and discovered that income elasticity in OECD countries ranged from 0.830 in
the Near East to 1.197 (Ke et al., 2011). The panel data accessibility has enabled the panel data
models to be evaluated for various periods of time. In several OECD countries, the income
elasticity based on cross-section data was discovered to be higher than that in line with past
outcomes. The outcome is vulnerable to the selection of the assumptions underlying the model,
however. In addition, certain writers acquired nearly one revenue elasticity under extra
The literature describes several approaches to modelling healthcare costs. Some studies have
used domestic information while others have used macroeconomic aggregates. The review is
restricted to the latter research because of the scope of the research. Some past books depended
on cross-sectional technology while others used methods for panelling. The latter have been
based on static and dynamic models, often with distinct outcomes.
Income:
Revenue (per capita GDP) has been recognized as a significant explanation for the difference in
levels of overall health care expenditure and development in different nations. Cross-sectional
regressions of aggregate healthcare per capita GDP spending per capita in literature from OECD
countries have continuously demonstrated a considerably higher revenue elasticity of about 1.20
to 1.50 (Ke et al., 2011). Regressions of aggregate time series for different nations were mostly
comparable but had significant differences among nations. Likewise, a study used cross-sectional
data in 1997 in the worldwide literature and discovered, based on the information included, that
the income elasticity of health spending was between 1.133 and 1.275. OOP revenue elasticity
ranged from 0.884 to 1.033, while public health expenditure ranged from 1.069 to 1.194
(Musgrove et al. 2002). Gaag and Stimac have also used cross-sectional data from 175 nations in
2004 and have shown that the health expenses ' revenue elasticity is 1.09. They also reported the
outcomes by area and discovered that income elasticity in OECD countries ranged from 0.830 in
the Near East to 1.197 (Ke et al., 2011). The panel data accessibility has enabled the panel data
models to be evaluated for various periods of time. In several OECD countries, the income
elasticity based on cross-section data was discovered to be higher than that in line with past
outcomes. The outcome is vulnerable to the selection of the assumptions underlying the model,
however. In addition, certain writers acquired nearly one revenue elasticity under extra
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
assumptions. Non - OECD panel data model literature has not examined the connection of
revenue with health spending directly.
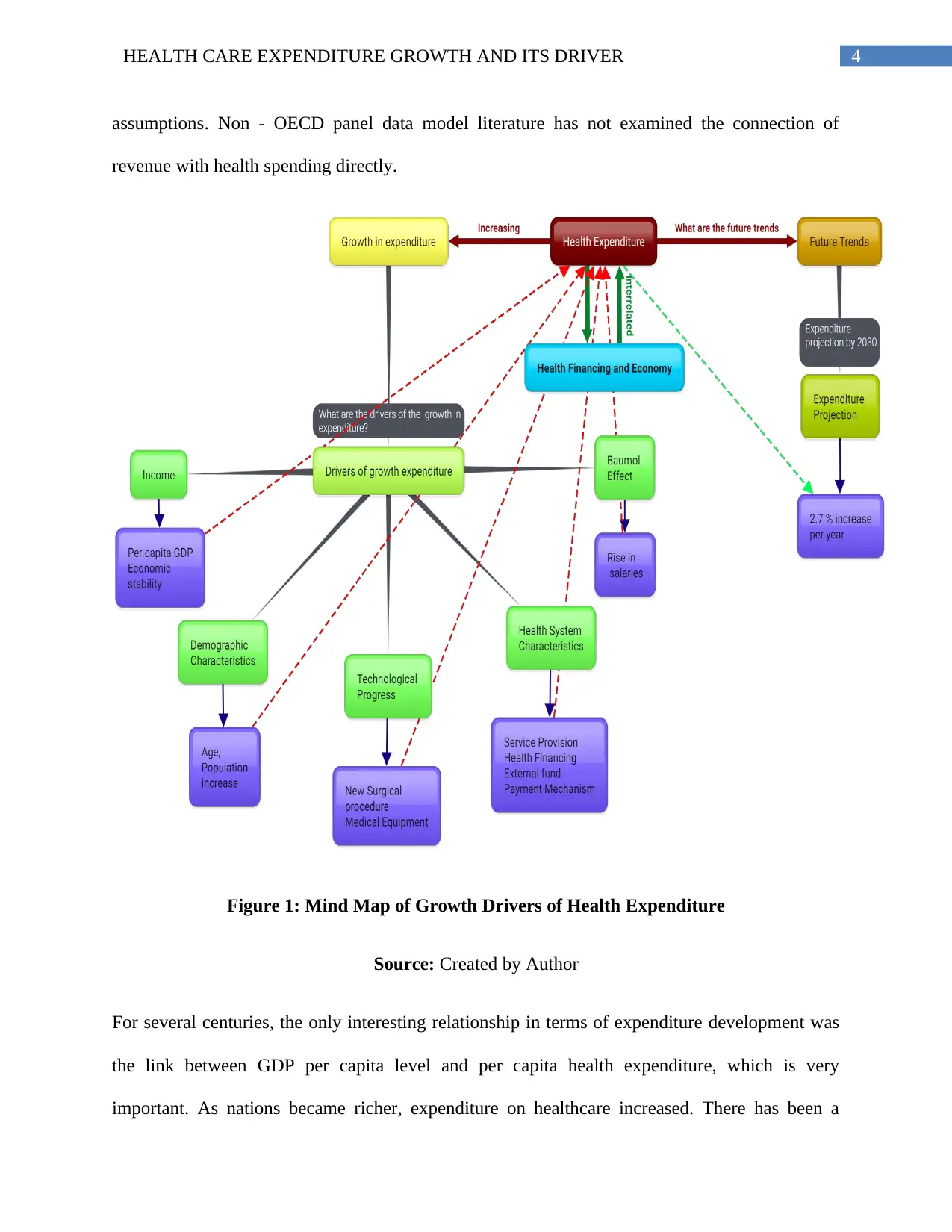
Figure 1: Mind Map of Growth Drivers of Health Expenditure
Source: Created by Author
For several centuries, the only interesting relationship in terms of expenditure development was
the link between GDP per capita level and per capita health expenditure, which is very
important. As nations became richer, expenditure on healthcare increased. There has been a
assumptions. Non - OECD panel data model literature has not examined the connection of
revenue with health spending directly.
Figure 1: Mind Map of Growth Drivers of Health Expenditure
Source: Created by Author
For several centuries, the only interesting relationship in terms of expenditure development was
the link between GDP per capita level and per capita health expenditure, which is very
important. As nations became richer, expenditure on healthcare increased. There has been a
5HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
considerably higher interest in understanding health expenditure beyond GDP and welfare
development over the last decade (Ke et al., 2011). However, it is reasonable to say that this
study is still in its infancy and lacks credible information in specific for quantitative research.
At this point, it is worth noting that the above literature focuses primarily on the direct impact of
GDP on healthcare costs. Indeed, the inverse cause, where GDP is a function of health spending,
has also a theoretical foundation, as was described in, for instance at Erdil and Yetkiner (Erdil &
Yetkiner 2009). One way to consider this inverse impact is to treat health together with education
as another element of human capital. The GDP is based on healthcare expenditure by at
minimum two mechanisms. First, if spending on healthcare can be seen as an investment in the
human capital and because an accumulation of human capital is a key cause of economic growth,
an increase in spending on healthcare should eventually bring about greater GDP. Secondly,
increased health care expenditure in conjunction with efficient health intervention improves the
supply of work and productivity, eventually increasing GDP (Ke et al., 2011).
Therefore, there can be and needs to be a concurrent causality in both directions. If GDP and
health care costs simultaneously determine each other, their connection has an issue of
endogeneity. If this occurs, then conventional methods of estimation that assume that GDP is
exogenous will generate inconsistent parameter estimates. But even if the causalities exist in both
directions, it seems logical to expect that it does not happen instantly, but with a delay of time.
For this reason, the Granger-causality test seems to be the best way to determine the possible
direction of causality between health care expenses and GDP. Their research shows that Granger
is significantly bi-directional in 46 nations. The pattern relies on the country's GDP level in cases
where there is a unique causality. Their analyses show that one-way causation generally extends
between GDP and health expenditure in nations with low and medium income, whilst the
considerably higher interest in understanding health expenditure beyond GDP and welfare
development over the last decade (Ke et al., 2011). However, it is reasonable to say that this
study is still in its infancy and lacks credible information in specific for quantitative research.
At this point, it is worth noting that the above literature focuses primarily on the direct impact of
GDP on healthcare costs. Indeed, the inverse cause, where GDP is a function of health spending,
has also a theoretical foundation, as was described in, for instance at Erdil and Yetkiner (Erdil &
Yetkiner 2009). One way to consider this inverse impact is to treat health together with education
as another element of human capital. The GDP is based on healthcare expenditure by at
minimum two mechanisms. First, if spending on healthcare can be seen as an investment in the
human capital and because an accumulation of human capital is a key cause of economic growth,
an increase in spending on healthcare should eventually bring about greater GDP. Secondly,
increased health care expenditure in conjunction with efficient health intervention improves the
supply of work and productivity, eventually increasing GDP (Ke et al., 2011).
Therefore, there can be and needs to be a concurrent causality in both directions. If GDP and
health care costs simultaneously determine each other, their connection has an issue of
endogeneity. If this occurs, then conventional methods of estimation that assume that GDP is
exogenous will generate inconsistent parameter estimates. But even if the causalities exist in both
directions, it seems logical to expect that it does not happen instantly, but with a delay of time.
For this reason, the Granger-causality test seems to be the best way to determine the possible
direction of causality between health care expenses and GDP. Their research shows that Granger
is significantly bi-directional in 46 nations. The pattern relies on the country's GDP level in cases
where there is a unique causality. Their analyses show that one-way causation generally extends
between GDP and health expenditure in nations with low and medium income, whilst the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
opposite goes with nations with elevated revenue. In comparison, the Hartwig assessment of
Granger-causality in a panel of 21 OECD countries found no proof to show that per capita GDP
development is caused by health expenditure (Hartwig 2008). If Granger causality's other
direction is tested, the findings actually support the hypothesis that GDP determine health
expenses with a favourable indication.
Population age structure:
Sometimes the epidemiological need is also integrated by multiple proxies as a covariant. HIV
seroprevalence was used as a proxy by Lu et al. and discovered that there had been no important
link to GDP overall public health expenditures (Lu et al. 2010). The rates of maternal mortality
in African nations, Murthy and Okunade discovered, are not associated with health expenses
(Murthy & Okunade, 2009).
Technological progress:
Progress in technology is also a main driver of health spending. The impact with each of the
other drivers is strongly linked. As the riches of a country rises, medical technology
developments usually increase the range of health care facilities, but are cost-effective. By
expanding life expectancy and altering morbidity patterns, new techniques affect demographic
change. The inefficient use of new techniques can, however, also boost health expenditure
without improving health conditions (Chandra and Skinner, 2012). Progress in technology was
seen as a major driver of health care. Several proxies are used according to the sort of model
under account for modifications in medical treatment technology. The surgical procedures and
the amount of particular medical devices and life expectance and infant death are examples of
such proxies in cross-section research. Studies have found that the amount and development of
opposite goes with nations with elevated revenue. In comparison, the Hartwig assessment of
Granger-causality in a panel of 21 OECD countries found no proof to show that per capita GDP
development is caused by health expenditure (Hartwig 2008). If Granger causality's other
direction is tested, the findings actually support the hypothesis that GDP determine health
expenses with a favourable indication.
Population age structure:
Sometimes the epidemiological need is also integrated by multiple proxies as a covariant. HIV
seroprevalence was used as a proxy by Lu et al. and discovered that there had been no important
link to GDP overall public health expenditures (Lu et al. 2010). The rates of maternal mortality
in African nations, Murthy and Okunade discovered, are not associated with health expenses
(Murthy & Okunade, 2009).
Technological progress:
Progress in technology is also a main driver of health spending. The impact with each of the
other drivers is strongly linked. As the riches of a country rises, medical technology
developments usually increase the range of health care facilities, but are cost-effective. By
expanding life expectancy and altering morbidity patterns, new techniques affect demographic
change. The inefficient use of new techniques can, however, also boost health expenditure
without improving health conditions (Chandra and Skinner, 2012). Progress in technology was
seen as a major driver of health care. Several proxies are used according to the sort of model
under account for modifications in medical treatment technology. The surgical procedures and
the amount of particular medical devices and life expectance and infant death are examples of
such proxies in cross-section research. Studies have found that the amount and development of
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
health expenditure were key to technological advances and variations in medical practice.
Technological progress was not regarded as a covariate by literature from non-OECD nations,
mostly because of an absence of credible technological progress information (Ke et al., 2011).
Health system characteristics:
Very few empirical studies have shown that the extent to which public funding for health care
spending is related to the degree of spending for health. In nations in OECD and in Eastern
European and Central Asian (ECA) nations (A. Wagstaff & Bank 2009), differences in spending
for health were considered between tax based and social insurance schemes. The OECD research
discovered that per capita health spending in nations where a social insurance system exists was
greater. The ECA research indicated that public health spending per capita in nations with social
insurance was greater than in nations that rely exclusively on general taxation. The connection
between external resources and domestic health expenditure in developing nations has recently
shown great interest. Gaag and Stimac discovered that while health-specific Official
Development Aid (ODA) has no important effect on complete health expenditure, health-specific
ODA has an elasticity of 0.138 compared to public health spending. Lu et al 2010 discovered a
favourable connection between health ODA channelling through the non-governmental industry
and overall public health expenditure, while it discovered an adverse correlation as channelled
through the governmental industry (Lu et al. 2010). Fee-for-service systems were generally more
expensive than capitation systems on average. In a research from the ECA nations, an increase in
government and private healthcare spending was connected with a change from funding clinics
to payment fees or patient payment systems via budgets. The ratio of hospital spending to
complete health care expenses is also strongly linked to health spending. The total supply of
doctors may have a positive effect on health expenditure. However, the Murthy and Okunade
health expenditure were key to technological advances and variations in medical practice.
Technological progress was not regarded as a covariate by literature from non-OECD nations,
mostly because of an absence of credible technological progress information (Ke et al., 2011).
Health system characteristics:
Very few empirical studies have shown that the extent to which public funding for health care
spending is related to the degree of spending for health. In nations in OECD and in Eastern
European and Central Asian (ECA) nations (A. Wagstaff & Bank 2009), differences in spending
for health were considered between tax based and social insurance schemes. The OECD research
discovered that per capita health spending in nations where a social insurance system exists was
greater. The ECA research indicated that public health spending per capita in nations with social
insurance was greater than in nations that rely exclusively on general taxation. The connection
between external resources and domestic health expenditure in developing nations has recently
shown great interest. Gaag and Stimac discovered that while health-specific Official
Development Aid (ODA) has no important effect on complete health expenditure, health-specific
ODA has an elasticity of 0.138 compared to public health spending. Lu et al 2010 discovered a
favourable connection between health ODA channelling through the non-governmental industry
and overall public health expenditure, while it discovered an adverse correlation as channelled
through the governmental industry (Lu et al. 2010). Fee-for-service systems were generally more
expensive than capitation systems on average. In a research from the ECA nations, an increase in
government and private healthcare spending was connected with a change from funding clinics
to payment fees or patient payment systems via budgets. The ratio of hospital spending to
complete health care expenses is also strongly linked to health spending. The total supply of
doctors may have a positive effect on health expenditure. However, the Murthy and Okunade

8HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
study of African countries found no relationship between the density of doctors and health
expenditure (Murthy & A. Okunade 2009).
Baumol effect:
The Baumol impact is that certain services tend to raise their comparative prices against other
products and services in the economy, reflecting the adverse productivity differential and wage
equalization across industries. In specific, health services prices will increase compared with
other prices because in high-productivity sectors salaries must maintain up with salaries. The
share of health care spending in GDP is expected to grow over time with price inelastic demand
(Hartwig 2008). Therefore, but not necessarily at their level, the Baumol effect can also be
significant in terms of increasing healthcare expenses, although it seems natural that the
healthcare expenses, which are a labour intensive good, in high salary economies will become
greater. However, it seems logical to ignore the Baumol effect as a phenomenon that primarily
impacts advanced economies in development studies.
Important explanatory variables for overall healthcare expenditure level and increase are: per
capita GDP, technological progress and variations in healthcare practice, as well as features of
the health systems. Recent studies acknowledge the significance of features of the health system
such as parameters for health funding, payment systems and provision of services. However, due
to information accessibility, the capacity to test these variables is restricted. This means that
certain significant factors may be missing from the assessment and therefore the econometric
findings should be interpreted carefully. Also, although incomes are strongly linked to health
care expenses, it is not evident what the conclusion is about income elasticity. While most
surveys tend to demonstrate that the elasticity of the revenue is higher than one, some trials
study of African countries found no relationship between the density of doctors and health
expenditure (Murthy & A. Okunade 2009).
Baumol effect:
The Baumol impact is that certain services tend to raise their comparative prices against other
products and services in the economy, reflecting the adverse productivity differential and wage
equalization across industries. In specific, health services prices will increase compared with
other prices because in high-productivity sectors salaries must maintain up with salaries. The
share of health care spending in GDP is expected to grow over time with price inelastic demand
(Hartwig 2008). Therefore, but not necessarily at their level, the Baumol effect can also be
significant in terms of increasing healthcare expenses, although it seems natural that the
healthcare expenses, which are a labour intensive good, in high salary economies will become
greater. However, it seems logical to ignore the Baumol effect as a phenomenon that primarily
impacts advanced economies in development studies.
Important explanatory variables for overall healthcare expenditure level and increase are: per
capita GDP, technological progress and variations in healthcare practice, as well as features of
the health systems. Recent studies acknowledge the significance of features of the health system
such as parameters for health funding, payment systems and provision of services. However, due
to information accessibility, the capacity to test these variables is restricted. This means that
certain significant factors may be missing from the assessment and therefore the econometric
findings should be interpreted carefully. Also, although incomes are strongly linked to health
care expenses, it is not evident what the conclusion is about income elasticity. While most
surveys tend to demonstrate that the elasticity of the revenue is higher than one, some trials
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
indicate that it is less than one. The results for revenue elasticity are in reality susceptible to the
selection of the underlying assumptions and the information used for estimating the model. It's
an empirical problem therefore.
Future trend and health expenditure projection:
Health expenditure for all OECD countries will continue to develop in the medium term. In the
lack of significant policy modifications, health expenditure per capita is expected to grow
slightly lower than it has done in the past, averaging 2.7 percent per year across the OECD from
2015-2030 (Lorenzoni, Marino, Morgan, & James, 2030). Health expenditure is expected to
output GDP in many situations and in a "base" situation to reach 10.2% on average.
Expenditures could reach up to 10.8% if cost containment strategies are ineffective and
increasing health systems expectations are not adequately managed (a scenario for' cost stress').
The development of health spending is anticipated to be slower with improved productivity and
efficient health promotion policies, although its GDP share is still predicted to rise to 9.6 percent
by 2030 (Lorenzoni et al., 2030). These numbers compare to 8.8% of GDP in 2015. In every
OECD nation, health spending as a share of GDP should rise, with major expectations in the
United States primarily due to population growth and coverage rises. The public health
expenditure is expected to increase slightly quicker than complete health expenditures, leading in
a 74.2 per cent increase to 77.4 percent in 2030. These findings are generally compatible with the
degree to which expenditure growth is achieved, although other cross-country projections model
public instead of complete health expenditure. The demographic impact in the basic situation
raises health spending by an OECD average of 0.7 percent per year. The predicted development
amounts to a quarter. Note that the demographic impact includes a 1.1-percent growth "pure age"
impact (Lorenzoni et al., 2030). This is tempered by a degree of reduction in morbidity that
indicate that it is less than one. The results for revenue elasticity are in reality susceptible to the
selection of the underlying assumptions and the information used for estimating the model. It's
an empirical problem therefore.
Future trend and health expenditure projection:
Health expenditure for all OECD countries will continue to develop in the medium term. In the
lack of significant policy modifications, health expenditure per capita is expected to grow
slightly lower than it has done in the past, averaging 2.7 percent per year across the OECD from
2015-2030 (Lorenzoni, Marino, Morgan, & James, 2030). Health expenditure is expected to
output GDP in many situations and in a "base" situation to reach 10.2% on average.
Expenditures could reach up to 10.8% if cost containment strategies are ineffective and
increasing health systems expectations are not adequately managed (a scenario for' cost stress').
The development of health spending is anticipated to be slower with improved productivity and
efficient health promotion policies, although its GDP share is still predicted to rise to 9.6 percent
by 2030 (Lorenzoni et al., 2030). These numbers compare to 8.8% of GDP in 2015. In every
OECD nation, health spending as a share of GDP should rise, with major expectations in the
United States primarily due to population growth and coverage rises. The public health
expenditure is expected to increase slightly quicker than complete health expenditures, leading in
a 74.2 per cent increase to 77.4 percent in 2030. These findings are generally compatible with the
degree to which expenditure growth is achieved, although other cross-country projections model
public instead of complete health expenditure. The demographic impact in the basic situation
raises health spending by an OECD average of 0.7 percent per year. The predicted development
amounts to a quarter. Note that the demographic impact includes a 1.1-percent growth "pure age"
impact (Lorenzoni et al., 2030). This is tempered by a degree of reduction in morbidity that
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
reduces the development of expenditure by 0.3 percent. Revenues are the main drivers, which
increase development by 1.5 per cent –equal to half the annual development in health
expenditure. Productivity limitations (the Baumol effect), which amounts to about one eighth of
the general development in expenditure, boost annual health expenditure by 0.4 per cent. Time-
specific impacts also boost the average annual health expenditures by 0.4 percent (Hartwig,
2008).
Conclusion:
The assessment of healthcare expenditure is essential for focusing on how healthcare expenditure
should be regulated. The increasing cost of health care is very important because of the fact that
the biggest expenditure is a comparatively tiny number of individuals. The system needs
adjustments and complete reorganization and is skewed in health care. Although current national
health expenditure has created more questions than answers, the system's future needs cannot be
ignored. Consequently, it is essential to have a healthcare system that reasonably accommodates
all actors. Nonetheless, a balance has been created with less fragile and pragmatic changes
between implementing a formidable health care plan and protecting egoistic political interests.
However, an appealing health system can still be achieved that can be funded from other sources.
The steady growth in healthcare expenses is a challenge for most industrialized countries. The
expenditure on nominal healthcare is growing not only, but also the share of GDP and
government spending is growing. In nations such as Germany, if policy does not change,
healthcare spending can expect to amount to more than 20 per cent of GDP for 15 or 20 years.
Although there is no such sharp rise in other nations, issues arise enough for us to examine
closely why healthcare expenses are rising and how healthcare can utilize resources in the future
more effectively. However, this is not in the interests of policy makers. In recent years, the major
reduces the development of expenditure by 0.3 percent. Revenues are the main drivers, which
increase development by 1.5 per cent –equal to half the annual development in health
expenditure. Productivity limitations (the Baumol effect), which amounts to about one eighth of
the general development in expenditure, boost annual health expenditure by 0.4 per cent. Time-
specific impacts also boost the average annual health expenditures by 0.4 percent (Hartwig,
2008).
Conclusion:
The assessment of healthcare expenditure is essential for focusing on how healthcare expenditure
should be regulated. The increasing cost of health care is very important because of the fact that
the biggest expenditure is a comparatively tiny number of individuals. The system needs
adjustments and complete reorganization and is skewed in health care. Although current national
health expenditure has created more questions than answers, the system's future needs cannot be
ignored. Consequently, it is essential to have a healthcare system that reasonably accommodates
all actors. Nonetheless, a balance has been created with less fragile and pragmatic changes
between implementing a formidable health care plan and protecting egoistic political interests.
However, an appealing health system can still be achieved that can be funded from other sources.
The steady growth in healthcare expenses is a challenge for most industrialized countries. The
expenditure on nominal healthcare is growing not only, but also the share of GDP and
government spending is growing. In nations such as Germany, if policy does not change,
healthcare spending can expect to amount to more than 20 per cent of GDP for 15 or 20 years.
Although there is no such sharp rise in other nations, issues arise enough for us to examine
closely why healthcare expenses are rising and how healthcare can utilize resources in the future
more effectively. However, this is not in the interests of policy makers. In recent years, the major
11HEALTH CARE EXPENDITURE GROWTH AND ITS DRIVER
approach has been to contain rises in health care expenditures to make public health accessible.
The concept of reducing spending development through the rationing of models that do not
sacrifice the quality of health care services is rather encouraging policymakers with so-called
cost-containment prospects. This is not a sustainable approach. Cost containment can have
marginal impacts only if such strategies go on along present lines by addressing fresh and extra
health care expenditure and not the bulk of total health service expenditure. In the health
industry, the government should instead tackle the inefficiencies. This would not only help to
contain rises in costs; it could also enhance the competitiveness and development of the health
industry. Projections of health spending demonstrate both cost containment policies ' potential
and restrictions. This is because people want better healthcare and technological advances extend
the range of healthcare that can be achieved. The challenge consists of how nations can further
push the borders of what healthcare systems can deliver to maximize value for money in a
financially sustainable way.
approach has been to contain rises in health care expenditures to make public health accessible.
The concept of reducing spending development through the rationing of models that do not
sacrifice the quality of health care services is rather encouraging policymakers with so-called
cost-containment prospects. This is not a sustainable approach. Cost containment can have
marginal impacts only if such strategies go on along present lines by addressing fresh and extra
health care expenditure and not the bulk of total health service expenditure. In the health
industry, the government should instead tackle the inefficiencies. This would not only help to
contain rises in costs; it could also enhance the competitiveness and development of the health
industry. Projections of health spending demonstrate both cost containment policies ' potential
and restrictions. This is because people want better healthcare and technological advances extend
the range of healthcare that can be achieved. The challenge consists of how nations can further
push the borders of what healthcare systems can deliver to maximize value for money in a
financially sustainable way.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.